mrs. jones has pain - knowing & doing wo videos
TRANSCRIPT
Mrs. Jones Has Pain: How Will You
Know and What Will You Do?
Palliative Care for People with Dementia: Why Comfort Matters
April 29, 2015
Carol O. Long, PhD, RN, FPCN, FAAN
Principal, Capstone Healthcare
Adjunct Faculty, Arizona State University College of Nursing
Alzheimer’s Association, NYC Chapter; Center to Advance Palliative Care (CAPC),
Quality Care Committee (QCC) 1199SIEU Conference
Learning Objectives
1. Describe processes for assessing pain in persons with advanced dementia
2. Identify when behaviors suggest that a person with dementia is in pain
3. Present key clinical management strategies for addressing pain in persons with advanced dementia

Meet Mrs. Jones! • 86 yo, advanced AD
• Resident of Happy Valley Nursing Facility for 4 years
• Becoming less mobile
• No current “complaints” of pain; largely non-verbal
• History: arthritis, surgeries, MVA; acetaminophen (Tylenol®)
© Capstone Healthcare 2015
What Do We Know About Pain?
• Definition: “Pain is whatever the person says it is, experienced whenever they say they are experiencing it” (McCaffery & Pasero, 1999)
• Pain is a silent epidemic! • 100 million people suffer from chronic pain
(IOM, 2011) • 25-56% of adults in the community (Herr et al.,
2011) • 45-85% of US nursing home residents report
pain (Herr et al., 2011; IOM, 2011)
© Capstone Healthcare 2015

What Do We Know About Pain and Dementia?
• 50% of people in nursing homes have some level of cognitive impairment
• Older adults in nursing homes and those with cognitive impairment or dementia often live with pain that is undetected, undertreated or poorly managed
(Fink & Gates, & Montgomery, 2015)
© Capstone Healthcare 2015

What Do We Know About Pain and Dementia?
• Tolerance to acute pain possibly increases but pain threshold does not change – people with dementia sense even low levels of pain
• Absence of vital sign changes in people with dementia experiencing acute pain does not mean absence of pain
© Capstone Healthcare 2015
What Do We Know About Pain and Dementia?
• Cognitive impairment may alter response to pain therapies – people with dementia may require more analgesic (Benedetti et al., 2004, 2006)
• Pain does negatively affects cognitive function (Morrison et al., 2003)
• Summary: There is no empirical evidence that dementia results in the loss of ability to feel pain…Just the ability to report!
© Capstone Healthcare 2015
Challenges to Pain Assessment
in Dementia 1. Person with dementia concerns:
▫ “Do you have pain?” ▫ Older adults describe pain as discomfort, hurting or
aching and they may under-report their pain ▫ Discomfort / pain from constipation, cold, hunger,
and fatigue ▫ Increased affective pain and emotional distress
from difficulty managing everyday activities related to the disease state
▫ Pre-existing conditions: arthritis, disc compression, neuropathies, and more…
© Capstone Healthcare 2015

Challenges to Pain Assessment
in Dementia 2. Staff & organizational concerns:
▫ Concerns over use of opioids and potential delirium
▫ Lack of consistent staff can be a problem or caregivers may not „know‟ the person
▫ Reluctance to use opioids without a clear diagnosis
▫ Psychotropics mask pain symptoms
▫ Staff may forget what risk factors are present that may precipitate pain and behaviors that suggest pain
2. Family concerns: ▫ Fear of opioids
▫ Do not understand or know pain behaviors
© Capstone Healthcare 2015

General Principles
• We need to rethink how we come to know if a person with dementia has pain through behaviors
• Don‟t use: “No complaints of pain” / Pain is the 5th Vital Sign
• Adopt: Assume Pain is Present (APP) when behaviors emerge that suggest pain
• Pain is everyone‟s responsibility: Team effort is necessary
• Use evidence-based guidelines and tools to assess and address
• Pain is NOT a normal consequence of aging!
SEE: http://prc.coh.org/elderly.asp, http://www.geriatricpain.org
© Capstone Healthcare 2015

The Hierarchy of Pain Assessment
Guidelines
1. Attempt to elicit self-report from person. If the person is unable to self-report, document.
2. Identify pathologic conditions or procedures that may cause pain.
3. List the person‟s behaviors that may indicate pain.
4. Identify behaviors that caregivers and others knowledgeable about the person think may indicate pain.
5. Make a plan to address pain – analgesic trial
(Herr et al., 2011; Pasero & McCaffery, 2011)
© Capstone Healthcare 2015
Assess Pain
1. Investigate what may be causing the pain
▫ Complete physical examination
▫ Review medical history: Consider common pain etiologies in older adults (e.g. arthritis, UTI, fracture, etc.)
▫ Check on basic needs: physical, social, psychological, environmental, spiritual and person‟s life story/biography
© Capstone Healthcare 2015

Assess Pain 2. Complete and document a comprehensive pain
assessment & use evidence-based assessment tools. Secure as much information as possible:
1. Location – use a body chart
2. Character of pain (nociceptive vs. neuropathic vs. mixed)
3. Duration – how long has pain been a problem
4. Pattern (intermittent, constant, mixed), type of pain (acute or chronic/persistant)
5. Frequency – how often?
6. Associated symptoms
7. Modifying factors: what makes pain worse or better?
8. Analgesic medication history
9. How does pain affect function?
10. Intensity (Use appropriate rating scale)
© Capstone Healthcare 2015

• Grimacing
• Calling out
• Bracing
• Guarding
• Rubbing
• Changes in activity level
• Sleeplessness
• Reluctance to move
• Withdrawal
• Decreased appetite
• Increased or new behaviors
Assess Pain
Obvious Less Obvious
Ask: What are the behaviors that are new or escalating? What is this person trying to communicate to me through their dementia-related behaviors?
© Capstone Healthcare 2015

Assess Pain
3. Use evidence-based assessment tools to ascertain intensity of pain:
▫ Self-report tools: ask if the person has pain! Then try to obtain pain intensity rating. 3 tools.
▫ Behavioral observation assessment tools: List behaviors that suggest pain. Used for individuals who are unable to self-report. Total score is derived – cannot be used to calibrate intensity. 3 tools.
© Capstone Healthcare 2015

Self-Report Tools
1. Numeric Rating Scale (NRS)
0 1 2 3 4 5 6 7 8 9 10 No Pain Mild Pain Moderate Worst Possible
Pain Pain
Ask if the person has pain. Then ask …“On a scale of 0 to 10, with 0 meaning no pain and 10 meaning the worst pain you can imagine, how much pain are you having now?” Ask them to point to the number on the scale.
© Capstone Healthcare 2015

Self-Report Tools
2. FACES Pain Scale-Revised (FPS-R) The FPS-R is a self-report tool that a person may prefer over a NRS; often due to the pictures of 6 faces that range from happy to sad and distressed.
• Ask the person if they have pain. Then ask…“The faces show how much pain or discomfort someone is feeling. The face on the left shows no pain. Each face shows more and more pain and the last face shows the worst pain possible. Point to the face that shows how bad your pain is right NOW.”
• Scoring: Score the chosen face as 0, 2, 4, 6, 8 or 10, counting left to right with 0 = “no pain” and 10 = “worst pain possible”
(IASP, 2012)
© Capstone Healthcare 2015

Self-Report Tools
3. Verbal Descriptor Scale (VDS) – Pain Thermometer
© Capstone Healthcare 2015
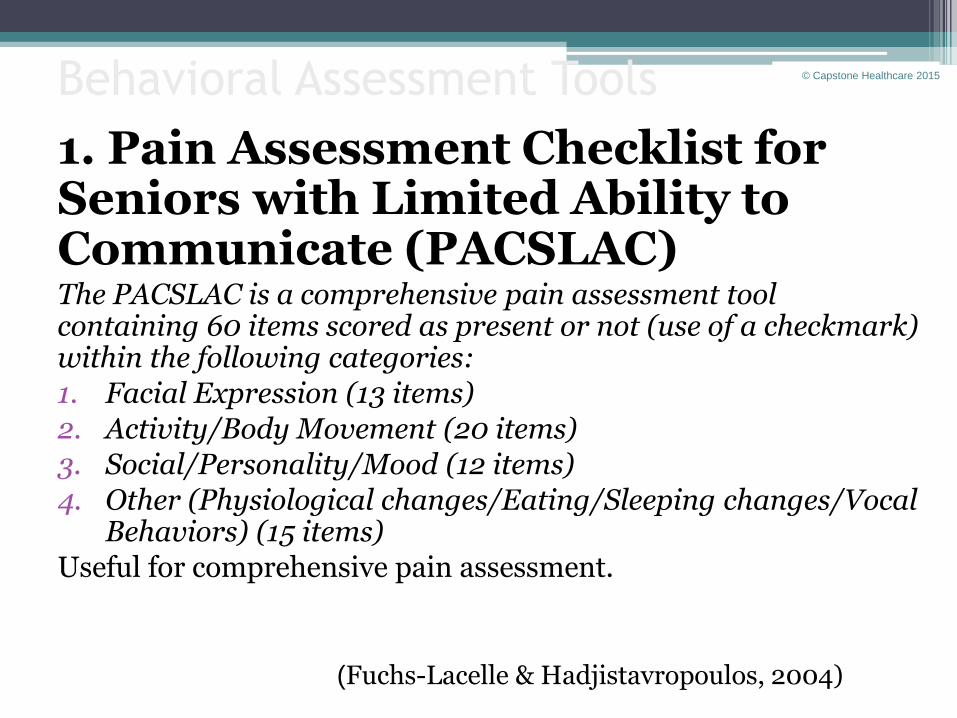
Behavioral Assessment Tools
1. Pain Assessment Checklist for Seniors with Limited Ability to Communicate (PACSLAC) The PACSLAC is a comprehensive pain assessment tool containing 60 items scored as present or not (use of a checkmark) within the following categories:
1. Facial Expression (13 items)
2. Activity/Body Movement (20 items)
3. Social/Personality/Mood (12 items)
4. Other (Physiological changes/Eating/Sleeping changes/Vocal Behaviors) (15 items)
Useful for comprehensive pain assessment.
(Fuchs-Lacelle & Hadjistavropoulos, 2004)
© Capstone Healthcare 2015
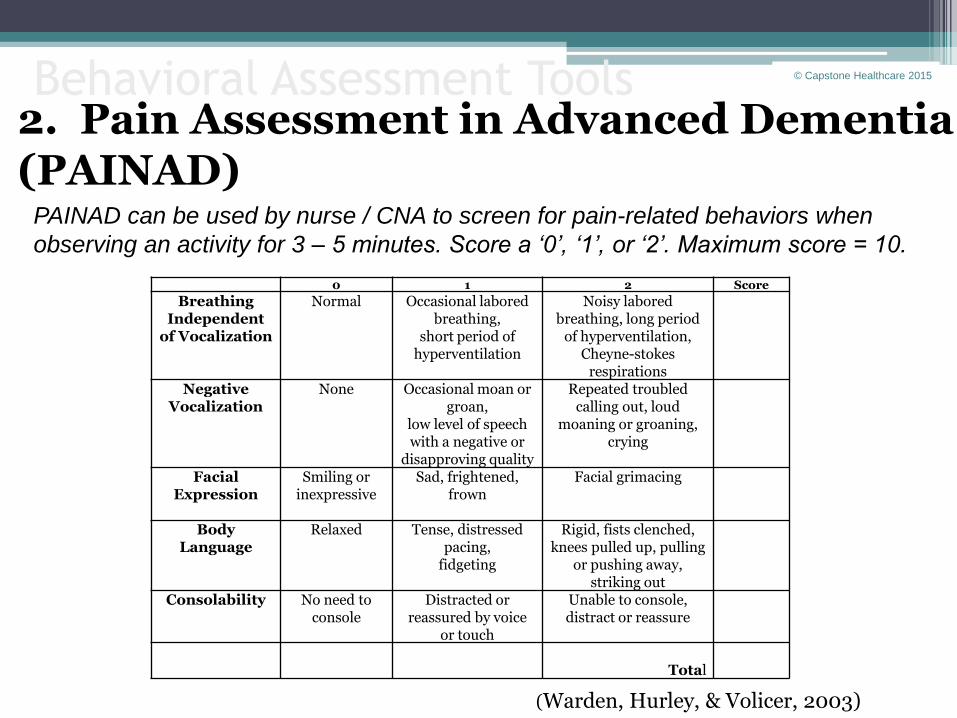
Behavioral Assessment Tools
(Warden, Hurley, & Volicer, 2003)
2. Pain Assessment in Advanced Dementia (PAINAD)
0 1 2 Score
Breathing Independent
of Vocalization
Normal Occasional labored breathing,
short period of hyperventilation
Noisy labored breathing, long period
of hyperventilation, Cheyne-stokes
respirations
Negative Vocalization
None Occasional moan or groan,
low level of speech with a negative or
disapproving quality
Repeated troubled calling out, loud
moaning or groaning, crying
Facial Expression
Smiling or inexpressive
Sad, frightened, frown
Facial grimacing
Body Language
Relaxed Tense, distressed pacing,
fidgeting
Rigid, fists clenched, knees pulled up, pulling
or pushing away, striking out
Consolability No need to console
Distracted or reassured by voice
or touch
Unable to console, distract or reassure
Total
PAINAD can be used by nurse / CNA to screen for pain-related behaviors when
observing an activity for 3 – 5 minutes. Score a ‘0’, ‘1’, or ‘2’. Maximum score = 10.
© Capstone Healthcare 2015

Behavioral Assessment Tools 3. Checklist of Nonverbal Pain Indicators (CNPI) Ask if the person has pain…Then observe the person for the following behaviors at rest and during movement. Score a „0‟ if the behavior was not observed, „1‟ if occurred briefly during activity or at rest. Total number of indicators is summed with movement, at rest and overall. No cut-off score.
(Feldt, 2000)
Behavior With Movement
At Rest
1. Vocal complaints: nonverbal (Sighs, gasps, moans, groans, cries)
2. Facial grimaces/winces (Furrowed brow, narrowed eyes, clenched teeth, tightened lips, jaw drop, distorted expressions)
3. Bracing (Clutching or holding onto
furniture, equipment, or affected area during movement)
4. Restlessness (Constant or intermittent
shifting of position, rocking, intermittent or constant hand motions, inability to keep still)
5. Rubbing (Massaging affected area)
6. Vocal complaints: verbal (Words
expressing discomfort or pain [e.g. „ouch‟, „that hurts‟];cursing during movement; exclamations of protest [e.g. „stop‟, „that‟s enough‟])
Subtotal Scores
Total Score
© Capstone Healthcare 2015
Does Mrs. Jones have pain?
• The evening shift CNAs are worried about Mrs. Jones…her behavior has changed.
• Could she have pain? How will you know and communicate it?
© Capstone Healthcare 2015

Address Pain
When addressing pain… Connect the assessment with the intervention and goals of care 1. Address unmet needs 2. Use nonpharmacologic interventions 3. Add pharmacologic interventions
a. start with serial trial intervention or analgesic trial for chronic/persistent pain
b. aggressively manage acute pain
© Capstone Healthcare 2015
1. Address Unmet Needs
• Therapeutic communication • Positioning and repositioning • Movement / ambulation • Toileting • Hunger and thirst • Ambulation • Milieu: heat / cold room • Sensory-stimulating or sensory-calming
activities • A hug!
2. Use Nonpharmacologic Interventions
Physical Psychological*
• Massage
• Heat/cold
• Gentle Vibration
• Positioning
• Exercise
• Sensory-integrated measures: use 5 senses
• Distraction
• Relaxation
• Music
• Comfort Foods
• Imagery
• Controlled Breathing * Individual responses vary based on abilities
© Capstone Healthcare 2015
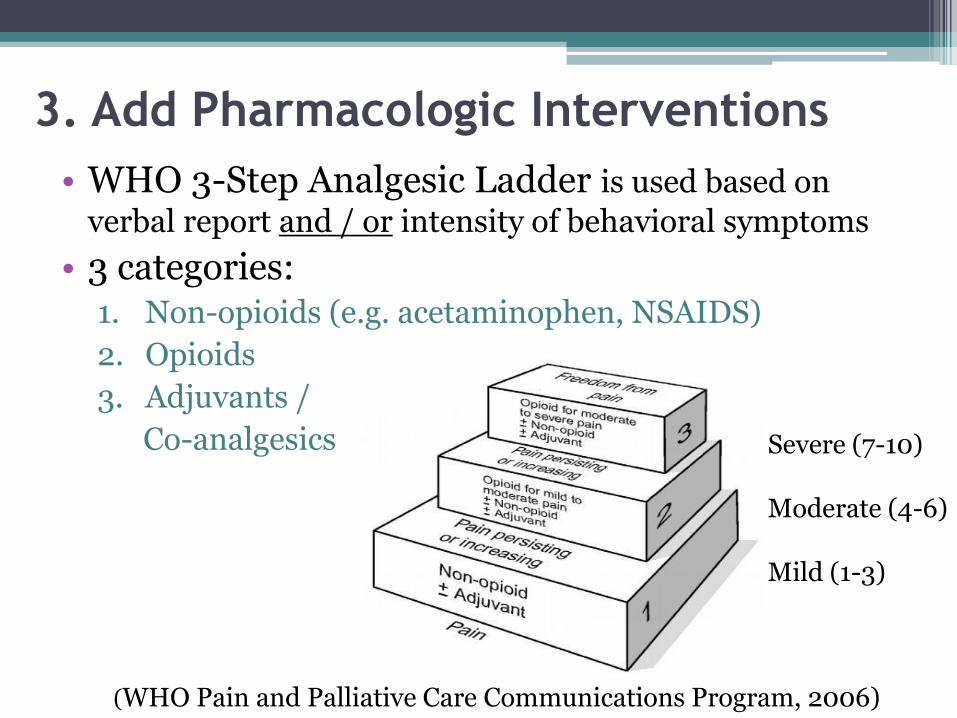
3. Add Pharmacologic Interventions
• WHO 3-Step Analgesic Ladder is used based on
verbal report and / or intensity of behavioral symptoms
• 3 categories: 1. Non-opioids (e.g. acetaminophen, NSAIDS)
2. Opioids
3. Adjuvants /
Co-analgesics
(WHO Pain and Palliative Care Communications Program, 2006)
Severe (7-10) Moderate (4-6) Mild (1-3)
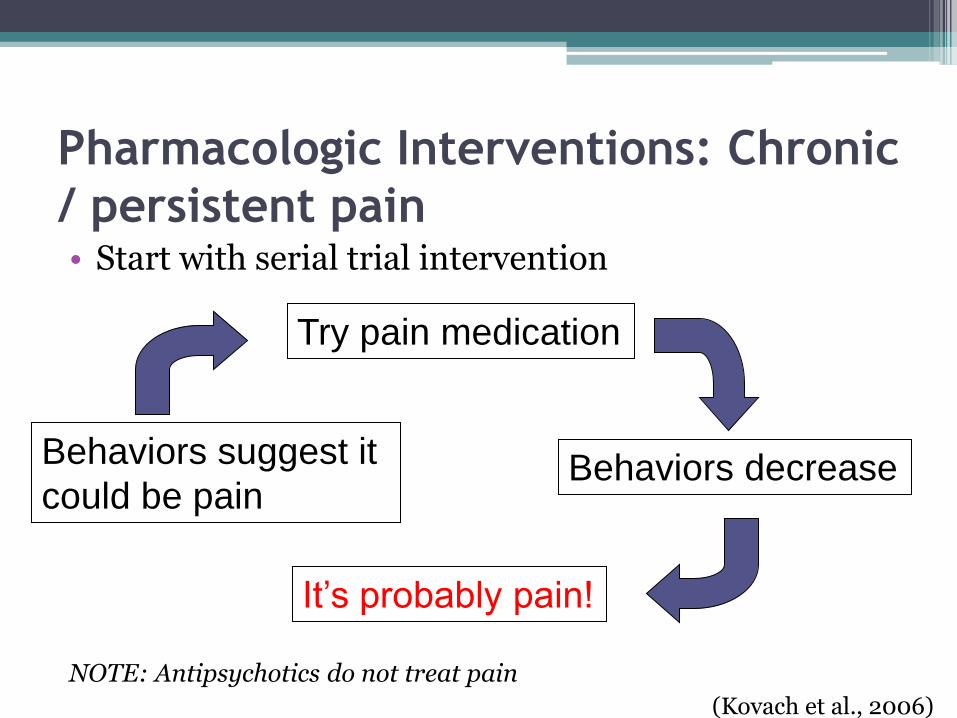
Pharmacologic Interventions: Chronic
/ persistent pain • Start with serial trial intervention
NOTE: Antipsychotics do not treat pain
Try pain medication
Behaviors decrease
It’s probably pain!
Behaviors suggest it
could be pain
(Kovach et al., 2006)

Pharmacologic Interventions
Medication Principles:
1. Initiate: Start low, go slow (except with acute pain) and titrate to effect while managing any side effects
2. If unable to report: schedule it! NO p.r.n. and document results
p.r.n. = person receives nothing!
3. Pain medication/analgesic + non-pharmacologic intervention is always considered

Now what will you do?
© Capstone Healthcare
2015
Communicate - Plan - Execute

Summary
• Assess pain
▫ Pain in the 5th Vital Sign – make it visible!
▫ 3 self-report tools
▫ 3 behavioral observation tools + common behaviors
▫ 5-step hierarchy
• Address pain
▫ 3 elements: address unmet need, nonpharm and pharmacologic management
▫ WHO 3-Step Analgesic Ladder
▫ Communication is essential
© Capstone Healthcare 2015

THANK-YOU!
Questions?
www.linkedin.com/in/carollongphd
Carol O. Long, PhD, RN, FPCN, FAAN E-mail: [email protected]
© Capstone Healthcare 2015
Selected References • Alzheimer‟s Association. Facts and Figures 2015
• American Geriatrics Society (AGS) Panel on Pharmacological Management of Persistent Pain in Older Persons. (2009). The pharmacological management of persistent pain in older persons. Journal of the American Geriatrics Society, 57(8), 1131-1346. doi: 10.1111/j.1532-5415.2009.02376.x.
• Benedetti, F., Arduino, C., Vighetti, S., Asteggiano, G., Tarenzi, L., & Rainero, I. (2004). Pain reactivity in Alzheimer patients with different degrees of cognitive impairment and brain electrical activity deterioration. Pain, 111(1-2), 22-29.
• Benedetti, F., Arduino, C., Costa, S., Vighetti, S., Tarenzi, L., Rainero, I., & Asteggiano, G. (2006). Loss of expectation-related mechanisms in Alzheimer's disease makes analgesic therapies less effective. Pain, 121(1-2), 133-144.
• City of Hope Pain Resource Center. A State of the Art Review for Assessment of Pain in Nonverbal Older Adults. Retrieved April 20, 2015 from http://prc.coh.org/pain-noa.htm
• Feldt, K. S. (2000). The Checklist of Nonverbal Pain Indicators (CNPI). Pain Management Nursing, 1(1), 13-21.
• Fink, R.M., Gates, R.A. & Montgomery (2015). Pain assessment. In: B. R. Ferrell, N. Coyle, & J. Paice (Eds.), Oxford textbook of palliative nursing, 4th edition (Chapter 6). New York, NY: Oxford University Press.
• Fuchs-Lacelle, S., & Hadjistavropolous, T. (2004). Development and preliminary validation of the pain assessment checklist for seniors with limited ability to communicate (PACSLAC). Pain Management Nursing, 5(1), 37-49.
• Herr K. A, Mobily P. R. (1993). Comparison of selected pain assessment tools for use with the elderly. Applied Nursing Research, 6(1), 39-46.
• Herr, K., Coyne, P. J., McCaffery, M., Manworren, R., & Merkel, S. (2011). Pain assessment in the patient unable to self-report: position statement with clinical practice recommendations. Pain Management Nursing, 12(4), 230-250.
• Institute of Medicine (IOM). (2011). Relieving pain in America: A blueprint for transforming prevention, care, education, and research. Washington, DC: The National Academies Press.
Selected References (cont)
Selected References (cont)
• International Association for the Study of Pain (IASP). (2001). Faces pain scale- revised. Retrieved October 8, 2014 from: http://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1519
• Kovach CR, Noonan PE, Schlidt AM, Reynolds S, Wells T. The Serial Trial Intervention: an innovative approach to meeting needs of people with dementia. J Gerontol Nurs. 2006;32:18-36.
• Morrison, R. S., Magaziner, J., Gilbert, M., Koval, K. J., McLaughlin, M. A., Orosz, G., et al. (2003). Relationship between pain and opioid analgesics on the development of delirium following hip fracture. Journals of the Gerontology Series: A Biological Science and Medical Sciences, 58(1), 76-81.
• Pasero, C., & McCaffery, M. (2011). Pain assessment and pharmacologic management. New York, NY: Mosby Elsevier.
• Warden, V., Hurley, A. C., & Volicer, L. (2003). Development and psychometric evaluation of the pain assessment in advanced dementia (PAINAD) scale. Journal of the American Medical Directors Association, 4(1), 9-15.
• World Health Organization. (1996). Cancer pain relief: With a guide to opioid availability, 2nd edition. Geneva, Switzerland: Author. Retrieved October 9, 2014 from http://www.who.int/cancer/palliative/painladder/en/