mortality and morbidity in obese patients undergoing ... · mortality and morbidity in obese...
TRANSCRIPT

Mortality and Morbidity in obese patients
undergoing anesthesia
and
Preoperative preparation
Pr Philippe CUVILLON
Pôle ARDU, CHU Nîmes

Adiposity
P / T2
Body Mass Index
BMI= Weight (kg) /Height² (m²)
Adolphe Quetelet. Edinburgh Medical Journal 1817

Mortality and obese patients
Assurance program : 1950-60
Moderate < 18,5
Very low 18,5 – 24,9
low 25 – 29,9
moderate 30 – 34,9
High
Very high
Super obese
35 – 39,9
40
> 50

Abdominal adiposity
0
2
4
6
8
10
12
14
16
18
20
I II III IV
Abdominal visceral fat
Cardiac CancerAll causes
Circulation 2016 Feb 16;133(7):639-49.

WHO (Worl Hearth Organization) 1997
Obesity is a « disease »


Obesity and cancer

Male : 1,75 m
Weight : 259 Kg
Age = 23 years
max : 296 kg
HTA
OAS (Apnea)
Heart failure
Obesity
BMI = 85kg/m²
Frequence
= 30-50 %
Frequence
= 30-70 %
Frequence
= 20-40 %
Frequence
= 20-30 %
Case n°1.
Stroke

Preoperative evaluation
• Perioperative outcomes
and surgery
SurgeryNon bariatric
Bariatric
0
2
4
6
8
10
12
14
16
18
20
I II III IV
Abdominal visceral fat
Cardiac CancerAll causes

Dindo D et coll. 2003;361:2032- 2035.
6336 consecutive patients
9% obese including, 4% with BMI > 35
Non bariatric surgery

General elective surgery

General elective surgery


Obesity, diabetes and smoking are important determinants of resource utilization in liver resection:
a multicenter analysis of 1029 patients. Gedaly R et al. Ann Surg 2009; 249:414-9.

23 studies (13 prospective, 10 retrospective): 106 119 patients
Admission : 15 of 2549 (0.59%) : pain, nausea, and dysphagia
Readmission (30-days) : 0.55% (12 of 2181 pts) : dysphagia +++
Super obese (BMI> 50):
more comorbidities, significantly longer operating times: 74 vs 81 min
The predictors of increased mortality:
BMI, ASA, type of procedure (i.e., Laparoscopic Roux-en-Y Gastric
Bypass versus LAGB), operative time.
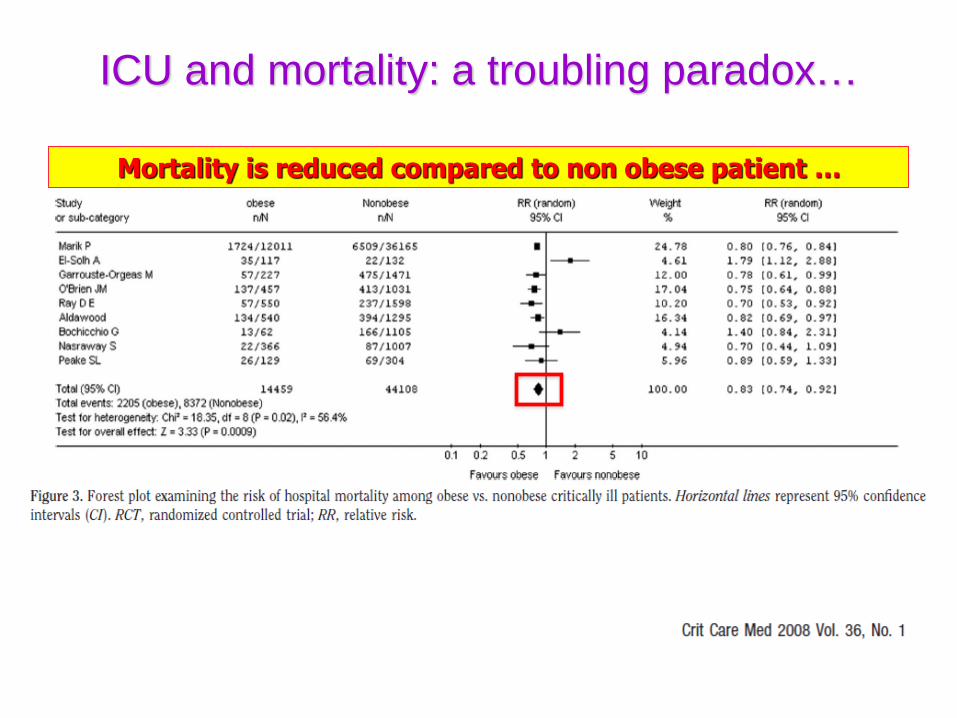
ICU and mortality: a troubling paradox…
Mortality is reduced compared to non obese patient …

• Mortality : 0.3 %
• Complications Death
– P. Emboli and DTV: 0.3 % 50 %
– Cardiac Failure: 0.4 % 15 %
– Anastomotic leak: 0.6 to 6 % 15-30 %
– Hemorhage: 3% <low
– Parietal infection ans abscess: 1.6 % <low
– Respiratory AE, pneumonia: 4-5 % 11-15 %
Br J Anaesth. 1981, 53:811-816,
Obese Surg. 2016, May
Bariatric surgery


113,898 patients overal postdischarge complication: 3.2%- wound infection (49.4%)
- reoperation (30.7%)
- urinary tract infection (16.9%),
- shock/sepsis (12.4%)
- organ space surgical-site infection (11.0%)
Open gastric bypass: greatest postdischarge complication 8.5%.
The factors associated most strongly with increased odds of postdischarge
complications: body mass index ≥ 50, use of steroids, procedure type,
predischarge complication, prolonged duration of stay, and prolonged operative
time.
Surgery 2015
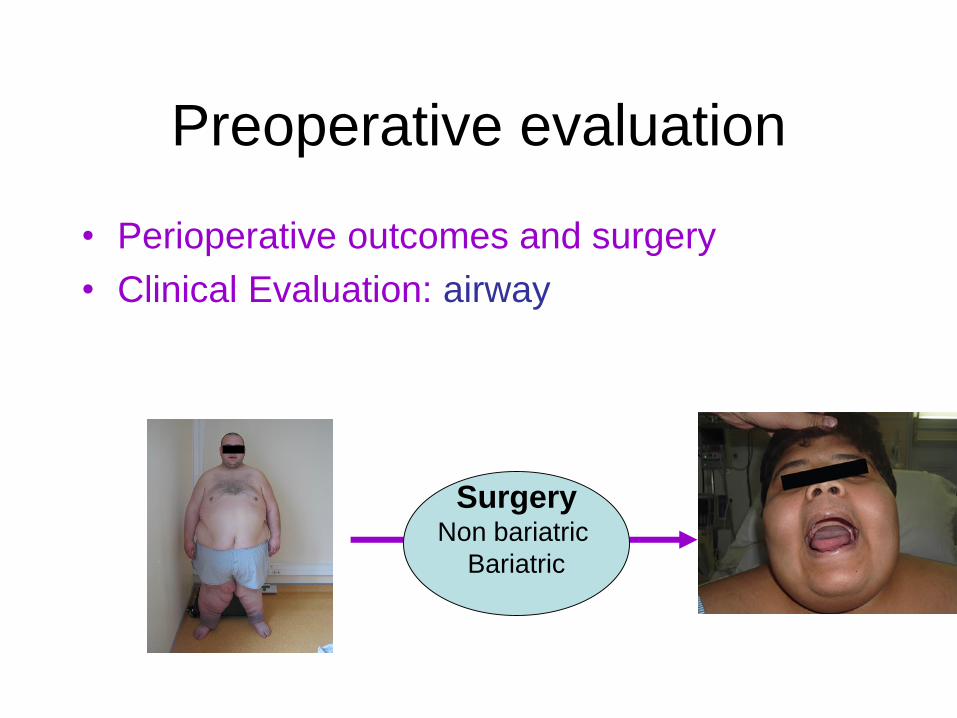
Preoperative evaluation
• Perioperative outcomes and surgery
• Clinical Evaluation: airway
SurgeryNon bariatric
Bariatric

Operating room, difficult intubation : 8% vs 5% non obese

grade I grade II grade III grade IV
Classification Mallampati
Classification Cormack AndLehane(laryngoscopie)
Facile DifficileIntubation
SCORE DE MALLAMPATI


Prediction of Difficult Tracheal IntubationTime for a Paradigm Change
Anesthesiology 2002Olivier Langeron, M.D., Ph.D.,* Philippe Cuvillon, M.D.,† Cristina Ibanez-Esteve,
M.D.,‡François Lenfant, M.D., Ph.D.,§ Bruno Riou, M.D., Ph.D.,‖ Yannick Le
Manach, M.D., Ph.D.#
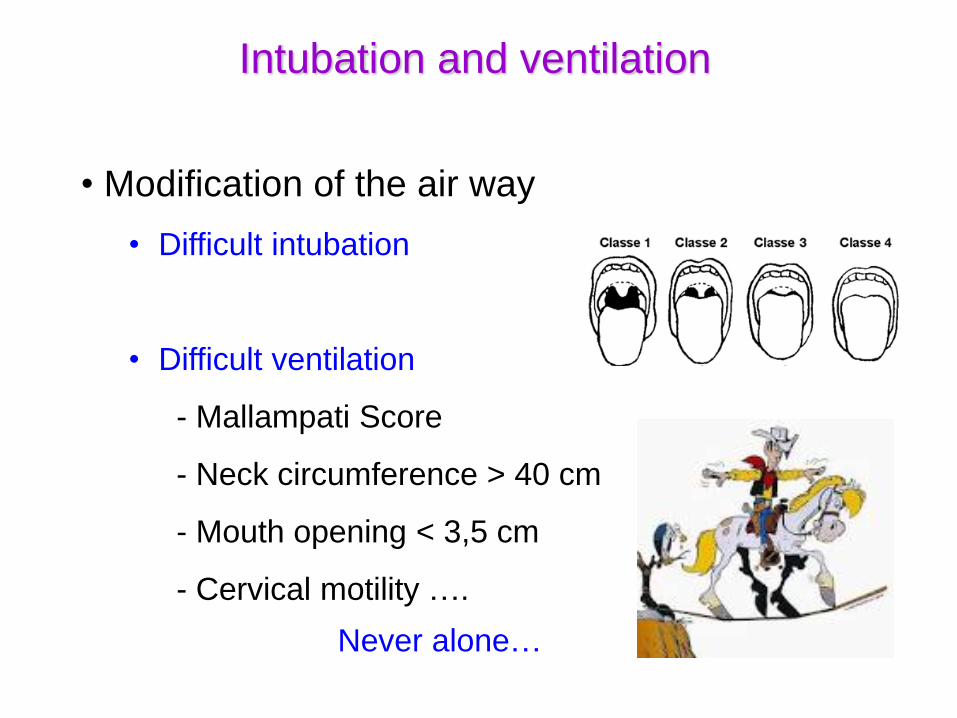
Intubation and ventilation
• Modification of the air way
• Difficult intubation
• Difficult ventilation
- Mallampati Score
- Neck circumference > 40 cm
- Mouth opening < 3,5 cm
- Cervical motility ….
Never alone…

Neck circumference as a predictor of difficult intubation and
difficult mask ventilation in morbidly obese patients: A
prospective observational study Eur J Anaesth 2016
Riad, Waleed; Vaez, Mercedeh N.; Raveendran, Ravi; Tam, Amanda D.;
Quereshy, Fayez A.; Chung, Frances; Wong, David T.
PATIENTS: A total of 104 morbidly obese surgical patients
(BMI ≥40 kg m−2) were included in the study. 88 patients were
women and 16 were men. Exclusions were known difficult
airway and emergency surgery.
Male sex (P = 0.004) and BMI more than 50 kg m−2 (P = 0.031)
were independent predictors of difficult mask ventilation.
• Modification of the air way
• Difficult intubation
• Difficult ventilation
• Inhalation and regurgitation
- Gastric paresis (diabetic)
- By pass surgery
Never alone…
Intubation and ventilation



Preoperative evaluation
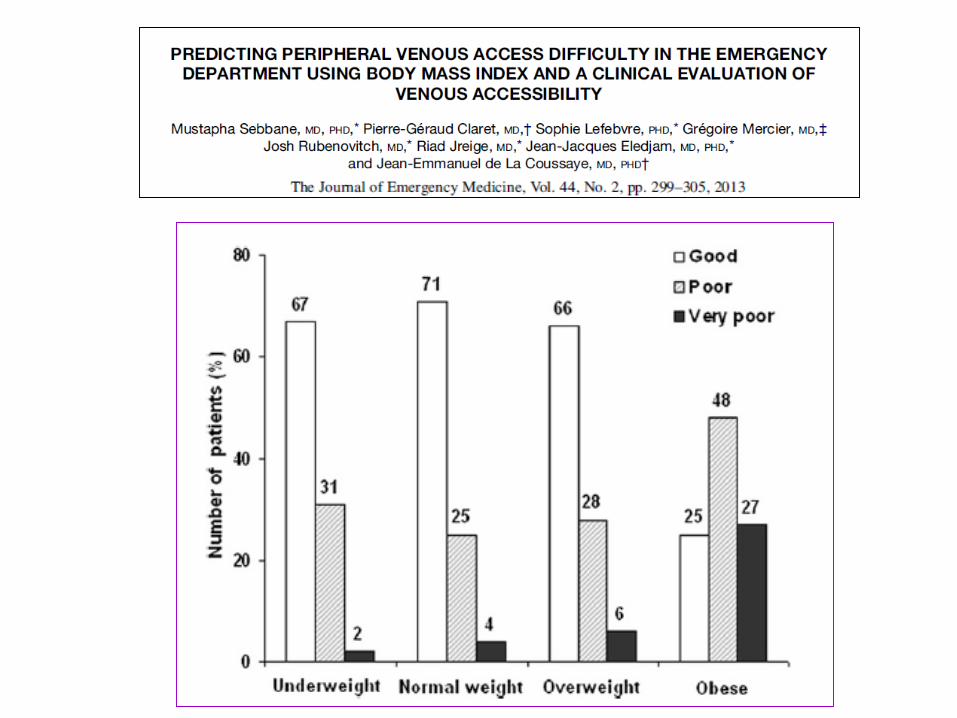
• Perioperative outcomes and surgery
• Clinical Evaluation: Venous access
SurgeryNon bariatric
Bariatric
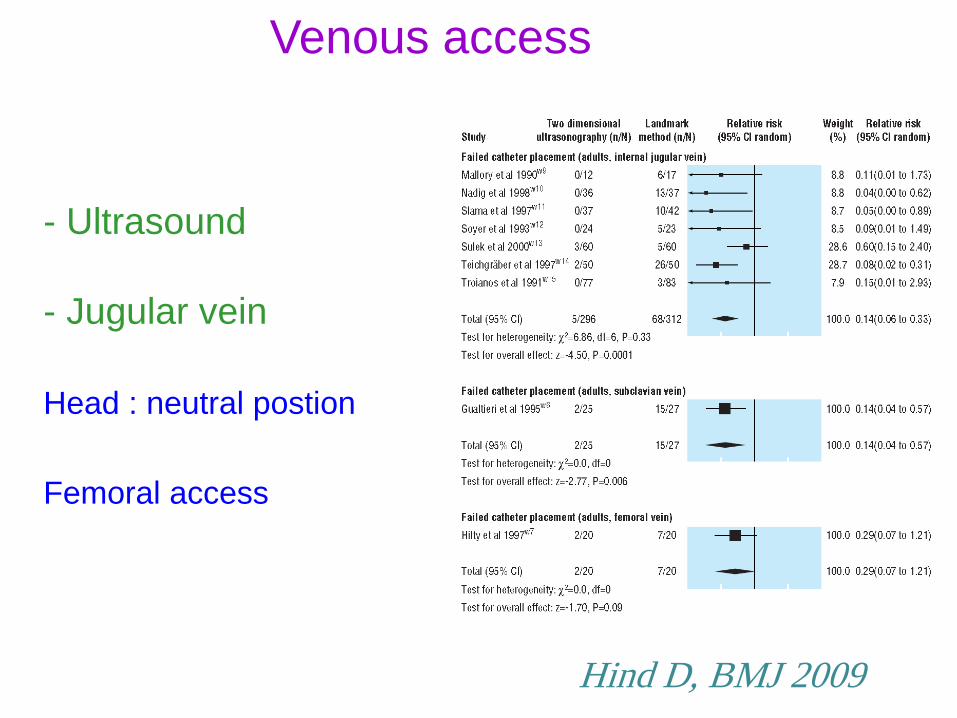
Venous access
- Ultrasound
- Jugular vein
Head : neutral postion
Femoral access
Hind D, BMJ 2009

Fujiki M, Obes Surg 2008
Head : neutral position
VJI
Venous access

Preoperative evaluation
• Perioperative outcomes and surgery
• Clinical Evaluation: Labs
SurgeryNon bariatric
Bariatric

Labs• Chemistry, liver function, renal function
• Lipid Profile
• CBC
• Iron Profile- TIBC, total iron, saturation
• B-1, B-12 levels
• HbA1c
• H-Pylori
• Drug Screen (optional)

Preoperative evaluation
• Perioperative outcomes and surgery
• Clinical Evaluation: cardiac evaluation
SurgeryNon bariatric
Bariatric

Cardiac dysfunction and obesity

Except for bariatric surgery, few data are available regarding
the morbidity and mortality associated with severe obesity and
specific surgical procedures.



There are 6 known risk factors for perioperative cardiovascular
morbidity in the general population according to the Revised
Cardiac Risk Index
These include:
- high-risk surgery, such as emergency surgical
procedures or major thoracic, abdominal, or vascular
surgery
- history of CHD
- history of congestive heart failure
- history of cerebrovascular disease
- preoperative treatment with insulin
- preoperative serum creatinine levels >2.0 mg/dL
Risk Class/ complication rate
Class I Zero 0.4%
Class II One 0.9%
Class III Two 6.6%
Class IV Three 11.0%

Obese patients with no CHD risk factors who are referred
for elective surgery may not require further testing.
On the other hand, patients with ≥3 CHD risk factors or
diagnosed CHD may require additional noninvasive
testing if the results will change management.
If significant coronary artery disease is found, surgery
could be delayed to allow the institution and titration of
appropriate medical therapy, such as statin or β-blocker
therapy, or even coronary revascularization in appropriate
patients with severe 3-vessel or left main disease

Preoperative evaluation
• Perioperative outcomes and surgery
• Clinical Evaluation: cardiac evaluation
SurgeryNon bariatric
Bariatric
Clinical
evaluation
Dyspnea
HTA
ECG
US echography






Preoperative evaluation
• Perioperative outcomes and surgery
• Clinical Evaluation: Pulmonary Function
SurgeryNon bariatric
Bariatric
Obstructive Sleep Apnea
(testing and treatment).
• Asthma.
• Smokers.

Obstructive Sleep Apnea incidence
IOSA-defined as an apnea/hypopnea index (AHI) ≥ 5.0 events/h
Study 1: 1 089 patients for bariatric surgery
OSA was 74 % J Brazil Pneumol 2015
Study 2: 120 patients (Canada) Obes Surg 2015
BMI 35-39.9 kg/m2 : 71 %.
BMI 40-40.9 kg/m2) : 74 %
Superobese (BMI 50-59.9 kg/m2): 77 %
> BMI 60 kg/m2: 95 %
Pulmonary complication after surgery : Chest 2016 Jan;149(1):84-91

• Pulmonary evaluation
– Spirometry (effect of β2 agonist)
– Polysomnography showed an obstructive
sleep apnea-hypopnea syndrome
(OSAHS)
• STOP-BANG questionnaire
OUI
OUI NON
OK pour la
chirurgie
24 heures
post-
opératoires
en
chambre
Snoring (ronflemment)
Tired (fatigue diurne)
Observed (apnées observées)
Blood Pressure (HTA)
BMI > 35
Age > 50
Neck tour de cou > 40 cm
Gender (homme)
Venir avec
l’appareillage
OK pour la
chirurgie
24 heures
post-
opératoires
en soins
continus
SAS
appareillé
NONSAHOS
connu
OUI NONSAS
diagnostiqué
Exploration nécessaireContacter pneumologue référent
OUIOUI NONSAS
appareillé
OUI
OK pour la
chirurgie
24 heures
post-
opératoires
en soins
continus
Venir avec
l’appareillage
≥ 3
facteurs de
risque
Ventilation en
pression positive
pendant 4 à 6
semaines
NON
6 weeks before surgery
3-4h / night


Film 4
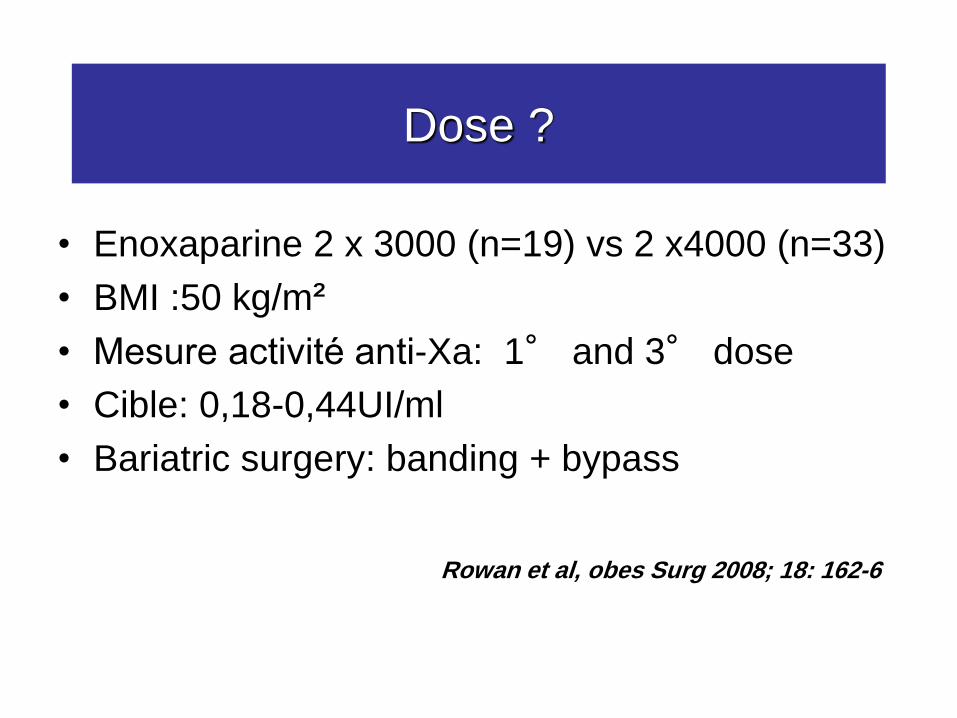
Dose ?
• Enoxaparine 2 x 3000 (n=19) vs 2 x4000 (n=33)
• BMI :50 kg/m²
• Mesure activité anti-Xa: 1° and 3° dose
• Cible: 0,18-0,44UI/ml
• Bariatric surgery: banding + bypass
Rowan et al, obes Surg 2008; 18: 162-6

Dose ?
• Pic 3è dose
• Cible atteinte 42% pour 4000UI
Mais chirurgie non homogène,
Groupes successifs, 1è dose J-1 ou J0
Quelle thromboprophylaxie ?
Adaptation posologique
• Enoxaparine 2x4000(n=24) vs 2x6000(n=16)
• BMI 50 kg/m²
• Chirurgie bariatrique: banding ou bypass
• Cible: 0,18-0,44
• Mesure anti-Xa 1è et 3è dose
Simone et al Surg Endosc 2008
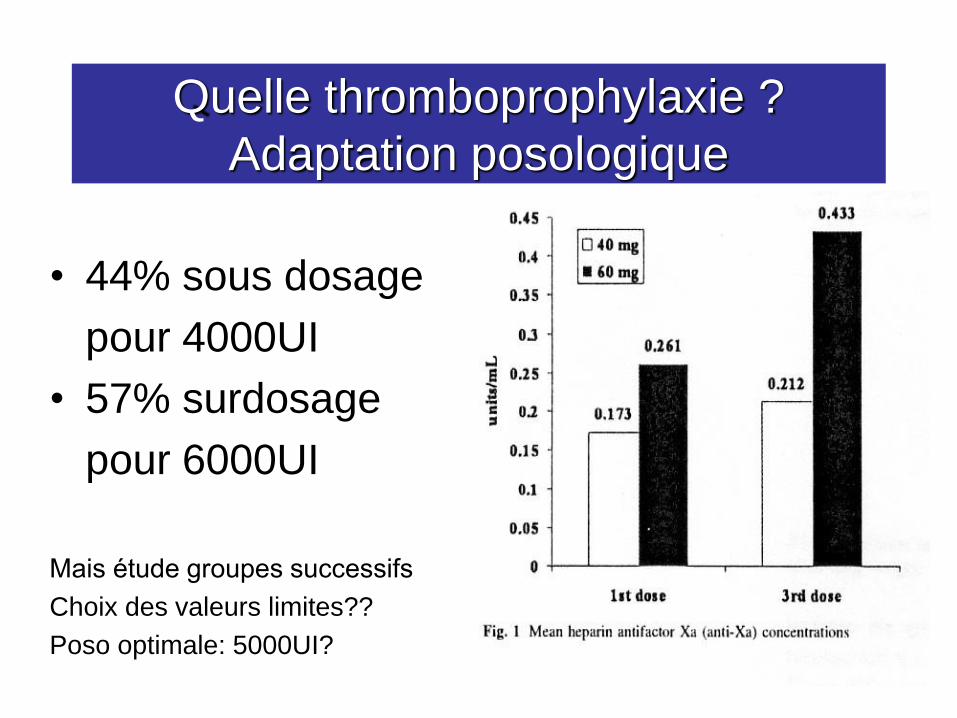
Quelle thromboprophylaxie ?
Adaptation posologique
• 44% sous dosage
pour 4000UI
• 57% surdosage
pour 6000UI
Mais étude groupes successifs
Choix des valeurs limites??
Poso optimale: 5000UI?

Preoperative evaluation
• Perioperative outcomes and surgery
• Clinical Evaluation
– airway (intubation, ventilation)
– Labs
– Cardiac evaluation (physical status)
– Pulmonary evaluation (OSA and B2)
– Venous access
– DTV and EP