morphine with adjuvant ketamine vs. higher …library.tasmc.org.il/ · induction of the...
TRANSCRIPT

DOI 10.1378/chest.08-0246 published online August 27, 2008; Chest
Shoshana Chazan and Avi A. Weinbroum Nachum Nesher, Margaret P. Ekstein, Yoseph Paz, Nissim Marouani,
ANALGESIAIMMEDIATE POST-THORACOTOMYHIGHER DOSES OF MORPHINE ALONE FOR MORPHINE WITH ADJUVANT KETAMINE VS.
http://chestjournal.org/cgi/content/abstract/chest.08-0246v1services can be found online on the World Wide Web at: The online version of this article, along with updated information and
to refer to the final, typeset version when it is available. advisedeffect to CHEST Papers In Press online publications. Readers are
or in the print version apply with full force andhttp://www.chestjournal.org/(DOI) and date of initial online publication. Any disclaimers set forth at CHEST Papers In Press articles must include the digital object identifierpriority; they are indexed by PubMed from initial publication. Citations to version. CHEST Papers In Press are citable and establish publication(substantive and/or non-substantive) that do not appear in this manuscript subsequently appear in typeset form may contain changes and correctionsnot yet copyedited, formatted, or typeset, and the version that will appeared in the printed or online issues of the Journal. These papers arebeen peer reviewed and accepted for publication but have not yet CHEST Papers In Press contains articles in manuscript form that have
). ISSN: 0012-3692. http://www.chestjournal.org/misc/reprints.shtml(copyright holder reproduced or distributed without the prior written permission of the60062. All rights reserved. No part of this article or PDF may be American College of Chest Physicians, 3300 Dundee Road, Northbrook ILIt has been published monthly since 1935. Copyright 2007 by the CHEST is the official journal of the American College of Chest Physicians.
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

1
MORPHINE WITH ADJUVANT KETAMINE VS. HIGHER DOSES OF MORPHINE 1
ALONE FOR IMMEDIATE POST-THORACOTOMY ANALGESIA 2
3
Nachum Nesher, MD,1 Margaret P. Ekstein, MD,2 Yoseph Paz, MD,3 Nissim Marouani, 4
MD,4 Shoshana Chazan, RN,5 and Avi A. Weinbroum, MD6 5
1Department of Cardiothoracic Surgery, email: [email protected] 6
2Department of Anesthesia and Intensive Care Medicine, email: 7
3Department of Cardiothoracic Surgery, email: [email protected] 9
4Acute Pain Service Department of Anesthesia and Intensive Care Medicine, email: 10
5Acute Pain Service Department of Anesthesia and Intensive Care Medicine, email: 12
6Chief Post-Anesthesia Care Unit, Professor Department of Anesthesia and Intensive Care 14
Medicine, email: [email protected] 15
Tel Aviv Sourasky Medical Center and the Sackler Faculty of Medicine, Tel Aviv University, 16
Tel Aviv, Israel. 17
18
Corresponding author: Avi A. Weinbroum, MD 19
Professor of Anesthesiology and CCM 20
Director, Post-Anesthesia Care Unit 21
Tel Aviv Sourasky Medical Center 22
6 Weizman Street, Tel Aviv 64239, Israel 23
Tel: 972-3-6973237; Fax 972-3-6925749 24
E-mail: [email protected] 25
Abstract: 267 wordsArticle: 2676 words
Page 1 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

2
Parts of this study were presented at the Euroanaesthesia 2003 Meeting, Glasgow, Scotland 26
and at the 5th International Congress on Coronary Artery Disease, 2003, Florence, Italy. 27
No financial support was received for this clinical trial. 28
Page 2 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

3
ABSTRACT 29
Background: Thoracotomy is associated with severe pain. We hypothesized that the 30
concomitant use of a subanesthetic dose of ketamine plus a ⅔-standard morphine dose might 31
provide more effective analgesia with fewer side effects than a standard morphine dose for 32
early pain control. 33
Methods: We conducted a 6-month randomized, double blind study in patients undergoing 34
thoracotomy for minimally invasive direct coronary artery bypass or for lung tumor resection. 35
After extubation, when objectively awake (≥5/10 VAS) and complaining of pain (≥5/10 36
VAS), patients were connected to a PCIA delivering 1.5mg morphine/bolus (MO group) or 37
1.0mg morphine+5mg ketamine/bolus (MK group), with a 7-minute lockout time. Rescue 38
intramuscular diclofenac 75mg was available. Follow-up lasted 4h. 39
Results: Forty-one patients completed the study. MO patients (n=20) used 6.8±1.9 40
(mean±SD) and 5.5±3.6 mg/h morphine during h 1 and 2, respectively; MK patients (n=21) 41
used 3.7±1.2 and 2.8±2.3 mg/h, respectively (P<0.01). The 4-h activation rate of the device 42
was double in the MOs than the MKs (66 ± 54 vs. 28 ± 20, P<0.001). The maximal self- 43
rated pain score was 5.6±1.0 for the MO vs. 3.7±0.7 for the MK group (P<0.01). Four MO 44
patients vs. one MK required diclofenac; 6 MO but no MK patients had SpO2 <94% on a 45
FiO2=0.4 (P<0.01); two MO patients required re-intubation. PaCO2 was higher in the MO 46
group (40±6 vs. 33±5 mmHg, P<0.05). Heart rate, blood pressure and incidence of 47
nausea/vomiting were similar; no ketamine-related hallucinations were detected. 48
Conclusions: Subanesthetic ketamine combined with a 35%-lower morphine dose provided 49
equivalent pain control compared to the standard morphine dose alone, with fewer adverse 50
side effects and a 45%-reduction in morphine consumption. 51
52
Registered at this site ClinicalTrials.gov; Registration number NCT00625911 53
Page 3 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

4
KEY WORDS: thoracotomy, analgesia, minimally invasive direct coronary artery bypass 54
(MIDCAB), lung tumor, pain, postoperative, morphine, ketamine 55
56
Page 4 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

5
ABBREVIATION LIST 57
ANOVA, analysis of variance 58
ASA, American Society of Anesthesiologists 59
BMI, body mass index 60
CICU, cardiac intensive care unit 61
EF, ejection fraction 62
FEV1/FVC, forced expiratory volume (in one second)/forced vital capacity 63
FiO2, fraction of inspired oxygen 64
IQR, inter-quarterly ratio 65
IV, intravenous 66
MIDCAB, minimally invasive direct coronary artery bypass 67
MK group, morphine 1.0 mg + 5 mg ketamine /bolus 68
MO group, morphine 1.5 mg/bolus 69
NMDA, N-methyl-D-aspartate 70
NSAIDs, non-steroidal anti-inflammatory drugs 71
PaCO2, arterial blood partial pressure of carbon dioxide 72
PACU, post-anesthesia care unit 73
PCIA, patient-controlled intravenous analgesia 74
PONV, postoperative nausea and/or vomiting 75
SpO2, pulse-derived arterial blood oxygen saturation 76
VAS, visual analogue scale 77
Page 5 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
6
INTRODUCTION 78
Thoracotomy, whether performed for the resection of lung tumor or for minimally invasive 79
direct coronary artery bypass, MIDCAB, surgery, is associated with severe and sometimes 80
uncontrolled, debilitating pain.1,2 Catecholamine release in response to nociceptive stimuli3 is 81
associated with undesirable hemodynamic consequences as well as disturbances in 82
respiratory, endocrine, metabolic4 and immune function.5 These changes may increase the 83
rate of complications, prolong hospitalization and augment cost.4-6 Importantly, if the acute 84
pain is not effectively controlled, it may evolve into severe chronic pain.7 85
Postoperative pain that is uncontrollable despite the administration of considerable 86
amounts of IV morphine could suggest tolerance to the drug.8-10 The administration of large 87
amounts of morphine to the awakening patient may cause respiratory and hemodynamic 88
depression.11,12 These effects may be especially serious when they follow lung lobectomy2 or 89
when they occur in patients with poor left ventricular function.13,14 For these reasons, 90
supplementation of morphine with non-narcotics (adjuvant agents) may be a way of 91
effectively controlling pain while reducing the incidence of adverse events.15,16 92
Ketamine, a noncompetitive NMDA-receptor antagonist, was shown to enhance 93
opioid-induced antinociception,17 to reduce hyperalgesia and to prevent morphine-induced 94
resistance 18,19 and, when combined with morphine, to lower post operative morphine 95
consumption.20 Given that subanesthetic (≤500 mcg/kg) doses of ketamine seldom produce 96
undesired hemodynamic alterations (e.g., elevated heart rate and blood pressure),21 we 97
hypothesized that by combining a subanesthetic dose of ketamine with morphine, we could 98
effectively control pain, while reducing postoperative morphine demand and drowsiness, with 99
an acceptable level of adverse side effects. The primary end point was pain VAS that was 100
used to calculate the sample size (see statistical paragraph); the secondary parameters 101
measured were morphine consumption, PCA activation, and side effects. 102
Page 6 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

7
103
PATIENTS AND METHODS 104
After the Ethics Committee of the Tel-Aviv Sourasky Medical Center approved this study’s 105
protocol, 44 patients scheduled for elective MIDCAB or for lung resection via thoracotomy 106
during a 6-month period (September 2001- March 2002) were enrolled in the study. They all 107
gave their informed, written consent to participate in this double blind study and were 108
randomly assigned to one of two groups according to their national ID number. Patients were 109
eligible for the study if they had been referred for a first time isolated coronary bypass and if 110
their surgeon considered them candidates for a MIDCAB procedure, or if they were to 111
undergo lung surgery. Exclusion criteria were ASA physical class ≥3, emergency operations, 112
Q-wave myocardial infarct occurring during the previous 3 weeks, or poor left ventricular 113
function (e.g., EF <30% by echocardiography or angiography). Other exclusion criteria were: 114
a BMI >35 kg/m2, past or current neuropathy or psychological disturbances, the use of 115
psychiatric medications, including anti-depressants and anti-psychotic agents, chronic liver or 116
renal failure requiring dialysis, a FEV1/FVC <70%, allergy to ketamine, morphine or 117
NSAIDs, clotting abnormalities, a platelets count <70000/mm3, a white blood count 118
<3000>14000/mm3, uncontrolled diabetes mellitus or fasting blood glucose >250 g/dl, 119
evidence of sepsis or infection up to one week prior to randomization. There was no age 120
restriction. 121
Anesthesia protocol 122
General anesthesia was administrated by the same anesthetist and no regional block was used. 123
Induction of the standardized anesthesia consisted of IV midazolam 2 mg, propofol 1 mg/kg, 124
medium-dose fentanyl (5-15 mcg/kg) and pancuronium (0.1mg/kg) to facilitate endotracheal 125
intubation. Anesthesia was maintained by repeated doses of fentanyl and pancuronium when 126
deemed necessary. All patients were ventilated in a volume-controlled mode with a tidal 127
Page 7 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
8
volume of 6 ml/kg and received oxygen enriched with isoflurane (0.4-0.8% inspired 128
concentration). Neuromuscular relaxation was reversed pharmacologically at the end of 129
surgery. When the patients resumed spontaneous respiration, responded adequately to orders 130
and demonstrated negative inspiratory force of at least 20 cmH2O or vital capacity greater 131
than 20cc/kg, their tracheas were extubated. Patients who were not extubated in the operating 132
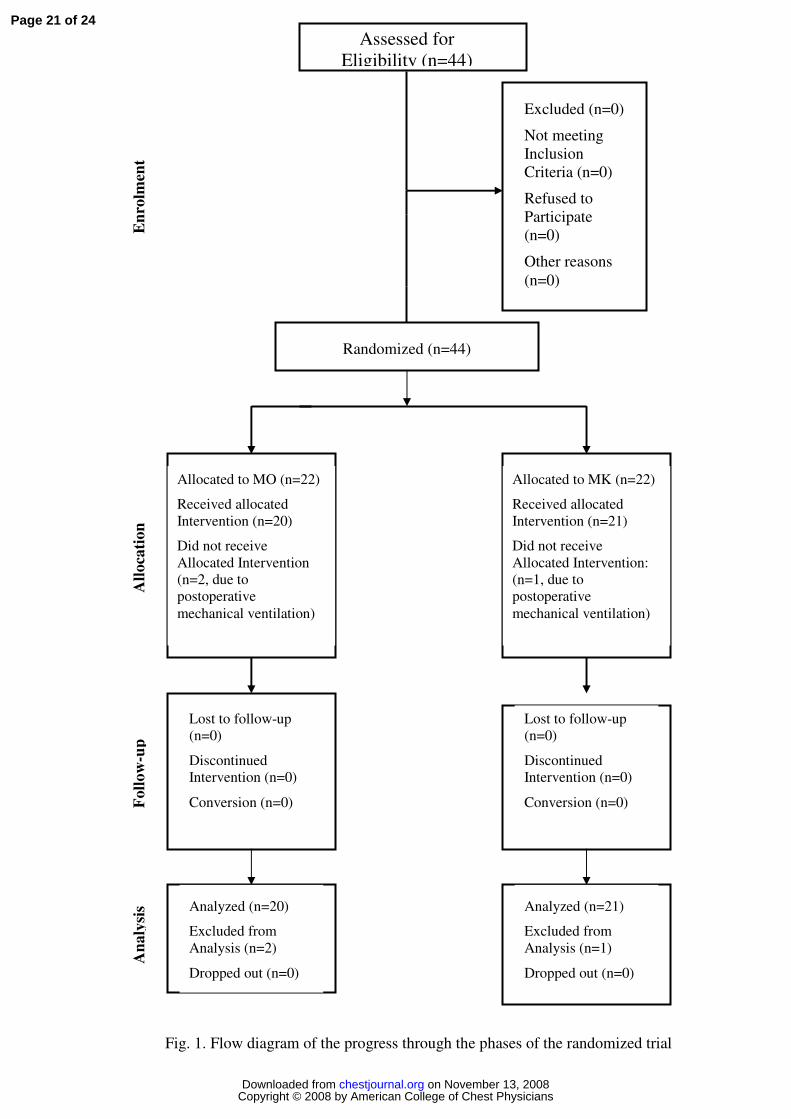
room were excluded from the study (see “allocation” boxes in CONSORT Statement, Fig. 1). 133
The postoperative monitoring included the measurements of heart rate by a 5-lead 134
electrocardiograph, invasive systolic and diastolic blood pressures, respiratory rate, and SpO2, 135
(AS/3™, Datex-Ohmeda®, Helsinki, Finland). 136
Postoperative analgesia protocol 137
All patients were transferred to the PACU where postoperative follow-up started. They 138
received IV analgesics (per patient request) starting from when their pain was score was 139
≥5/10 on a 0-10 VAS, see below) and when the attending physician determined that the 140
patient was in an acceptable cognitive state (≥5/10 VAS). A cutoff pain score was chosen on 141
the basis of previous experience in acute pain control.2,13 Drug injections consisted of either 142
1.5 mg morphine plus saline (group MO) or 1 mg morphine plus 5 mg ketamine (group MK). 143
A blinded anesthesiologist prepared the separate syringes based on the randomization list and 144
administered the first dose, after which the PCIA device was turned on. The device was 145
preset to deliver similar boluses whenever the patient activated it, controlled by a 7-minute 146
lockout period. If the protocol was ineffective to reduce pain VAS by ≥2 levels or patients 147
reported no satisfaction of the treatment within 30 minutes of treatment, a rescue dose of 148
intramuscular diclofenac 75 mg was available by the nurses. 149
One of two designated PACU nurses, who were blinded to the drug assignment, 150
assessed the variables listed below for each patient during the entire stay in the PACU. VAS 151
scores were assessed every 15 minutes: 152
Page 8 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

9
• Subjective pain intensity was patient self-rated, based on a VAS graded from “no 153
pain”=0 to “worst possible pain”=10. 154
• A patient’s subjective level of wakefulness was assessed by a self-rated VAS, from 155
1=heavily sedated to 10=fully awake. If patients were asleep, they were awakened to 156
obtain their rating; the data of patients unable to cooperate were excluded at that time 157
point. 158
• An SpO2-derived value of 94%, with 40% oxygen by facemask, was the lowest limit 159
allowed for arterial oxygenation, otherwise a 100% oxygen mask was placed and the 160
various patient's data from that time point were not recorded. 161
• Untoward effects (e. g., nausea, vomiting or any distress) were recorded by the nurse 162
and treated as indicated (e. g., metoclopramide 10 mg IV for nausea or vomiting). 163
Nurses specifically asked patients if hallucinations occurred and reported them. 164
Reintubation in the psotoeprative period, if necessary, was decided by the blinded PACU 165
attending physician based on clinical and laboratory data. 166
Patients were kept for 4 h in the PACU and then were transferred to the CICU for further 167
observation; no further data were collected thereafter. 168
Statistical analysis 169
The analyses were performed at the Statistical Laboratory of the School of Mathematics, Tel- 170
Aviv University, using the SPSS Release for Windows, Version 11.01 (Chicago, IL, 2002). A 171
pre-study power table where delta (representing the mean difference in pain score recorded in 172
a pilot study)=2.1, alpha=0.05 and power=0.97 resulted in the need for a minimum of 15 173
patients in each group. The demographic data (age, weight) and background characteristics 174
(baseline heart and respiratory rates, SpO2, systolic and diastolic blood pressures), the ASA 175
physical class, duration of surgery and intraoperative drug dosages, as well as fluid and blood 176
administration, were compared using one-way analysis of variance (ANOVA). Patients’ 177
Page 9 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

10
gender and intra-group procedure distributions were analyzed using the Fisher exact test. The 178
rates of the hourly demands of the PCIA devices were square rooted in order to obtain their 179
normal distribution; the results were then analyzed by one-way ANOVA with repeated 180
measures. The number of times the patients received a rescue drug and the rate of side effects 181
were also analyzed using the Fisher exact test. The effects of type of analgesia on the 182
patients’ self-rated pain and grade of wakefulness (VAS's), as well as the hourly amounts of 183
analgesic use were also analyzed using the ANOVA with repeated measures. The ANOVA 184
tests were always followed by the post-hoc Tukey’s Honest Significant Difference method. 185
All values are expressed as mean ± standard deviation (SD), with significance defined as 186
P≤0.05. 187
188
RESULTS 189
Out of 62 screened patients, 44 fulfilled the study criteria for randomization. Three of them 190
subsequently dropped out after surgery because they required continuous ventilation 191
(CONSORT statement, Fig. 1); no MIDCAB patient was converted to an on-pump procedure. 192
The demographic, anesthesia and surgical data were similar between the two drug study 193
groups (Table 1); intraoperative blood replacement and fluid infusion were similar as well 194
(data not shown). Baseline (immediately before starting study drug administration) vital 195
signs, patients’ self-rated pain intensity (Fig. 2) and wakefulness scores (data not shown) 196
were also similar between the groups. 197
Overall, the amounts of analgesics that were requested by the patients to alleviate pain 198
were found to be associated with the drug regimen. The MK group required 45% of the total 199
amount of morphine used by the MO group (P<0.001), ranges being 16-19 mg/4h, and 200
applied the PCIA more frequently (66 ± 54 vs. 28 ± 20, P<0.001, Fig. 3). The MO group 201
Page 10 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

11
requested more diclofenac per the protocol (P=NS) than the MK group (Table 1); in all cases 202
the rescue treatment was effective. 203
The subjectively evaluated pain intensity (VAS) during the 4-h PACU stay was 204
significantly (P<0.001) lower for the MK group compared to their MO counterparts (Fig. 2), 205
despite the larger amount of morphine that had been administered to the latter group. The 206
subjectively rated wakefulness scores for the MK group were also better (p<0.05) than those 207
for the MO group (Table 1). 208
All the recorded respiratory parameters were better in the MK group compared to the 209
MO group (Table 1): none of the MK patients had an SpO2 <94% with 40% oxygen by 210
facemask, but 6 of the MO patients did at one time point each (P<0.01): SpO2 values 211
improved better in the former than in the latter (Table 1) and PaCO2 were also lower in the 212
former. Two of the latter group subsequently required re-intubation and mechanical 213
ventilation for a period of 5-6 hours due to clinical respiratory distress associated with an 214
increase in heart rate and systolic blood pressure. The mean 4-h-respiratory rate was also 215
better in the MK group than in the MO group (Table 1). Finally, 1 h after the drugs were first 216
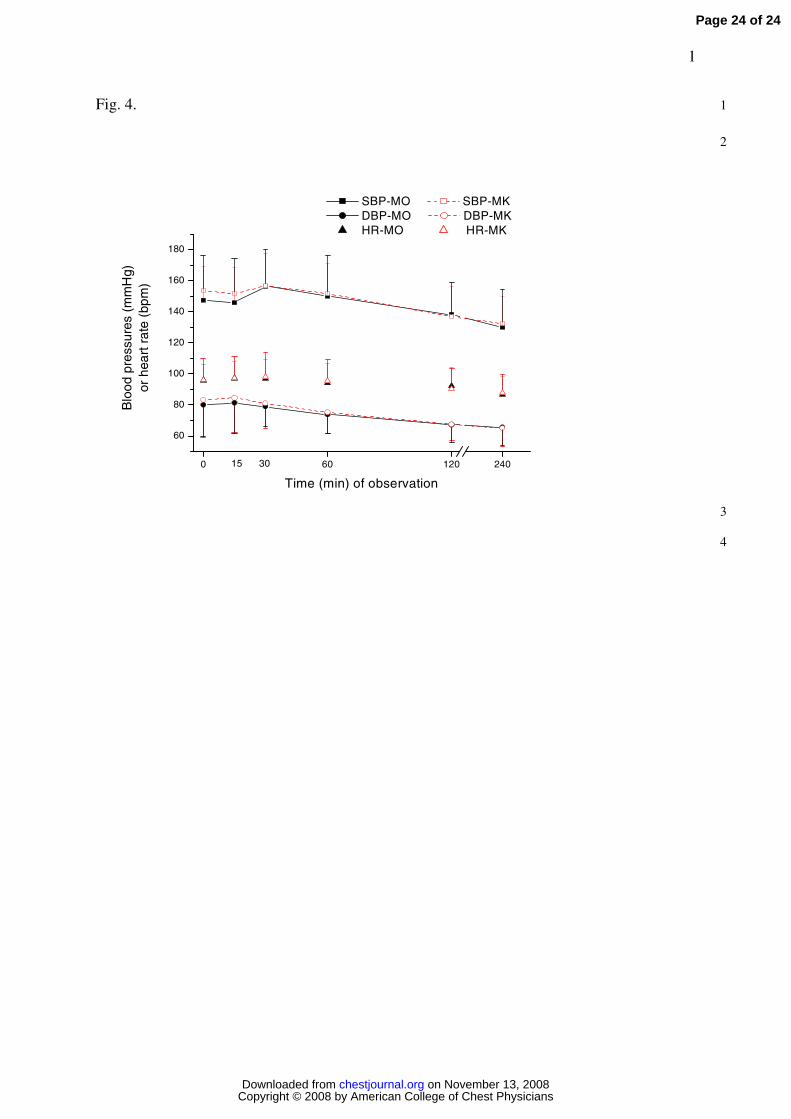
injected, heart rate and blood pressures in both groups decreased and stabilized for the rest of 217
the study period: interestingly, they were almost identical in both study groups (Fig. 4). 218
The incidence of PONV was similar between the groups (Table 1); all incidents were 219
short-lived and responded well to appropriate therapy. One MK patient reported a sensation 220
of lightheadedness that resolved spontaneously in <4 minutes, and at no time did any patients 221
report hallucinations or postoperative confusion. 222
None of the study patients in either group were kept in the PACU for more than the 223
protocol dictated period and all were transferred to the ward after fulfilling PACU discharge 224
criteria. All the study patients were later discharged from the CICU uneventfully according to 225
the cardiothoracic departmental discharge policies. 226
Page 11 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
12
227
DISCUSSION 228
Our study demonstrates that the administration of an IV subanesthetic dose (5 mg/bolus) of 229
ketamine combined with ⅔ of the standard (1.5 mg) morphine dose provided lower subjective 230
measures of pain (by >2 points on a scale of 1-10) than the standard morphine dose alone 231
during the immediate (4 h) post-thoracotomy period. The combined protocol was also 232
associated with remarkably stable hemodynamic conditions and better respiratory parameters 233
than the MO group. These objective effects were associated with a better self-rated level of 234
wakefulness, similar PONV, and insignificant ketamine specific side effects. 235
Postoperative pain ranks among the major problems of surgical patients, especially 236
after thoracotomy.2,22 During the last few years, evaluation of intense pain associated with 237
thoracotomy has become a subject of considerable interest, since both lung resection and 238
MIDCAB share the properties of newly evolving minimally invasive and “fast-tracking” 239
surgical techniques.23 240
Ketamine hydrochloride is a well known general dissociative anesthetic and a short 241
acting analgesic with antagonist activity at the NMDA receptor. Morphine and other opioids 242
produce antinociception via mu receptor agonistic activity and by the activation of the 243
monoaminergic descending pathways at the spinal level,10 they also activate the NMDA 244
receptor, resulting in hyperalgesia and development of tolerance to opioids.3,10 If tolerance is 245
one of the explanations for severe postoperative pain small doses of ketamine added to 246
morphine could treat pain better than morphine alone.8,10 247
If given alone, ketamine in small doses (<250 mcg/kg IV) may seldom induce a 248
change in level of consciousness lasting a few minutes because of the large plasma 249
concentration that develops immediately after the injection.24 Whereas the plasma half-life of 250
ketamine is only 15-20 minutes, the analgesic effect of the MK combination was evident and 251
Page 12 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

13
clinically stable throughout the 4-h observation period. The drug combination dose that was 252
used in this study allowed for a prompt reduction of pain and a morphine sparing effect. 253
These current results are supported by our previous data25 that demonstrated the beneficial 254
combination of ketamine and morphine in patients suffering from severe postoperative pain 255
that was resistant to morphine. 256
Heart rate and blood pressure are negatively affected by large morphine doses given 257
within a short period of time, but most importantly, respiratory rate, oxygenation and 258
adequate ventilation may drastically worsen because of the increased sedation.4,12 We 259
observed such events in several individuals in the MO group. On the other hand, the ketamine 260
dose of anesthesia is known to increase heart rate and blood pressure due to its pro-adrenergic 261
effect: our MK patients did not exhibit these reactions, either because of the very low 262
ketamine dose and/or because of its combination with morphine. The evidence of almost 263
identical pulse rates and blood pressures in both groups is, therefore, promising, especially in 264
the MIDCAB subgroup of patients of this study. 265
Reducing postoperative pain enhances the ability to breathe deeply and cough 266
effectively. All these features lead to better oxygenation and a probable preservation of 267
positive myocardial oxygen balance. 268
Ketamine alone may produce drowsiness;21,26 our MK patients, however, self-rated 269
themselves more awake than their MO counterparts, supporting the findings of an earlier 270
report.25 Short lived hallucinations are the most frequently mentioned side effect of ketamine, 271
especially if administered at doses ≥500 mcg/kg.27,28 Some reports indicated that up to 30% 272
of the patients receiving IV anesthesia doses of ketamine (0.5-1.5 mg/kg) experienced 273
unpleasant dreams or acute psychosis-like symptoms.29 In our current MK study group, there 274
were no reports of hallucinations or bad dreams, a finding we consider to be due to the small 275
intermittent dosage.25 276
Page 13 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

14
This study is limited by the short duration of follow up. The results of this study 277
cannot be extrapolated to imply that improving pain for the initial 4 postoperative h has long- 278
term effects on pain control or overall recovery. Nevertheless, effective initial pain control is 279
an important factor among other determinants of safe recovery and patient satisfaction. Also, 280
the specific cohort of coronary bypass patients presented here was managed with the "fast 281
track" mode of immediate awakening and extubation, the success of this approach is 282
dependent, among other things, on level of pain, wakefulness and adequate pulmonary 283
function. Indeed, the ketamine+morphine group fared significantly better in all of these 284
parameters. Another limitation is the theoretical difference between the incisions used for the 285
MIDCAB vs. the lung lobectomy. MIDCAB’s were performed via an anterolateral incision, 286
with the patients lying in the supine position, whereas lung resections were performed via a 287
more lateral incision, with the patients positioned more laterally. However, both types of 288
incision were similarly represented in both study groups. One other potential limitation to the 289
analysis of our data is the possibility of inter-observer variability between the PACU nurses 290
who collected the data. To minimize variability, there were only 2 dedicated nurses in the 291
PACU who assumed responsibility for the study patients. 292
In conclusion, immediate (4 h) postoperative subanesthetic doses of ketamine added 293
to ⅔ the standard dose of morphine provided equivalent analgesia with a better safety profile 294
compared to that obtained by a standard dose of morphine alone, in patients undergoing 295
thoracotomy for lung tumor resection or MIDCAB. The MK patients were hemodynamically 296
stable and there were signs of less respiratory depression compared to the MO group. MK 297
patients self-rated their wakefulness as being better than the MO patients. We recommend 298
additional studies to confirm our findings so that this promising drug protocol can be 299
considered safe for use in postoperative pain control of pulmonary and cardiac patients. 300
301
Page 14 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
15
Acknowledgment: The authors thank Esther Eshkol, MA (institutional medical copyeditor, 302
Tel Aviv Sourasky Medical Center) for editorial assistance, and the nursing staff of the 303
PACU for their collaboration and dedication. 304
Page 15 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
16
REFERENCES 305
1 Mehta Y, Swaminathan M, Mishra Y, et al. A comparative evaluation of intrapleural and 306
thoracic epidural analgesia for postoperative pain relief after minimally invasive direct 307
coronary artery bypass surgery. J Cardiothorac Vasc Anesth 1998; 12:162-5. 308
2 Soto RG, Fu ES. Acute pain management for patients undergoing thoracotomy. Ann Thorac 309
Surg 2003; 75:1349-57. 310
3 Phillips WJ, Currier BL. Analgesic pharmacology: II. Specific analgesics. J Am Acad 311
Orthop Surg 2004; 12:221-33. 312
4 Fleron MH, Weiskopf RB, Bertrand M, et al. A comparison of intrathecal opioid and 313
intravenous analgesia for the incidence of cardiovascular, respiratory, and renal 314
complications after abdominal aortic surgery. Anesth Analg 2003; 97:2-12. 315
5 Beilin B, Shavit Y, Trabekin E, et al. The effects of postoperative pain management on 316
immune response to surgery. Anesth Analg 2003; 97:822-7. 317
6 Polomano RC, Dunwoody CJ, Krenzischek DA, Rathmell JP. Perspective on pain 318
management in the 21st century. J PeriAnesth Nurs 2008; 23(Suppl 1):S4-14. 319
7 Bruce J, Drury N, Poobalan AS, et al. The prevalence of chronic chest and leg pain 320
following cardiac surgery: a historical cohort study. Pain 2003; 104:265-73. Erratum in: Pain 321
2004; 112:413. 322
8 Mao J, Price DD, Mayer DJ. Mechanisms of hyperalgesia and morphine tolerance: a 323
current view of their possible interactions. Pain 1995; 62:259-74. 324
9 Mao J, Price DD, Mayer DJ. Experimental mononeuropathy reduces the antinociceptive 325
effects of morphine: implications for common intracellular mechanisms involved in morphine 326
tolerance and neuropathic pain. Pain 1995; 61:353-64. 327
10 Mao J. Opioid tolerance and neuroplasticity. Novartis Found Symp 2004; 261:181-6; 328
discussion 187-93. 329
Page 16 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
17
11 Rothbard RL, Schreiner BF, Yu PN. Hemodynamic and respiratory effects of dezocine, 330
ciramadol, and morphine. Clin Pharmacol Ther 1985; 38:84-8. 331
12 Pena BM, Krauss B. Adverse events of procedural sedation and analgesia in a pediatric 332
emergency department. Ann Emerg Med 1999; 34:483-91. 333
13 Dowling R, Thielmeier K, Ghaly A, et al. Improved pain control after cardiac surgery: 334
results of a randomized, double-blind, clinical trial. J Thorac Cardiovasc Surg 2003; 335
126:1271-8. 336
14 Yorke J, Wallis M, McLean B. Patients' perceptions of pain management after cardiac 337
surgery in an Australian critical care unit. Heart Lung 2004; 33:33-41. 338
15 Hynninen MS, Cheng DC, Hossain I, et al. Non-steroidal anti-inflammatory drugs in 339
treatment of postoperative pain after cardiac surgery. Can J Anaesth 2000; 47:1182-7. 340
16 Lahtinen P, Kokki H, Hendolin H, et al. Propacetamol as adjunctive treatment for 341
postoperative pain after cardiac surgery. Anesth Analg 2002; 95:813-9. 342
17 Oye I, Paulsen O, Maurset A. Effects of ketamine on sensory perception: evidence for a 343
role of N-methyl-D-aspartate receptors. J Pharmacol Exp Ther 1992; 260:1209-13. 344
18 Stubhaug A, Breivik H, Eide PK, et al. Mapping of punctuate hyperalgesia around a 345
surgical incision demonstrates that ketamine is a powerful suppressor of central sensitization 346
to pain following surgery. Acta Anaesthesiol Scand 1997; 41:1124-32. 347
19 Javery KB, Ussery TW, Steger HG, et al. Comparison of morphine and morphine with 348
ketamine for postoperative analgesia. Can J Anaesth 1996; 43:212-5. 349
20 Laulin JP, Maurette P, Corcuff JB, et al. The role of ketamine in preventing fentanyl- 350
induced hyperalgesia and subsequent acute morphine tolerance. Anesth Analg 2002; 351
94:1263-9. 352
21 Fortin D, Adams R, Gallez A. A blood-brain barrier disruption model eliminating the 353
hemodynamic effect of ketamine. Can J Neurol Sci 2004; 31:248-53. 354
Page 17 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

18
22 Hawkes CA, Dhileepan S, Foxcroft D. Early extubation for adult cardiac surgical patients. 355
Cochrane Database Syst Rev 2003; 4:CD003587. 356
23 Pande RU, Nader ND, Donias HW, et al. REVIEW: Fast-Tracking Cardiac Surgery. Heart 357
Surg Forum 2003; 6:244-8. 358
24 Guillou N, Tanguy M, Seguin P, et al. The effects of small-dose ketamine on morphine 359
consumption in surgical intensive care unit patients after major abdominal surgery. Anesth 360
Analg 2003; 97:843-7. 361
25 Weinbroum AA. A single small dose of postoperative ketamine provides rapid and 362
sustained improvement in morphine analgesia in the presence of morphine-resistant pain. 363
Anesth Analg 2003; 96:789-95. 364
26 Krystal JH, Karper LP, Seibyl JP, et al. Subanesthetic effects of the noncompetitive 365
NMDA antagonist, ketamine, in humans. Psychotomimetic, perceptual, cognitive, and 366
neuroendocrine responses. Arch Gen Psychiatry 1994; 51:199-214. 367
27 Hartvig P, Larsson E, Joachimsson PO. Postoperative analgesia and sedation following 368
pediatric cardiac surgery using a constant infusion of ketamine. J Cardiothorac Vasc Anesth 369
1993; 7:148-53. 370
28 Green SM, Nakamura R, Johnson NE. Ketamine sedation for pediatric procedures: Part 1, 371
A prospective series. Ann Emerg Med 1990; 19:1024-32. 372
29 Lofwall MR, Griffiths RR, Mintzer MZ. Cognitive and subjective acute dose effects of 373
intramuscular ketamine in healthy adults. Exp Clin Psychopharmacol 2006; 14:439-49. 374
Page 18 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

19
Table 1. Demographic, intraoperative and 4h-postoperative data (mean ± SD or absolute 375
numbers). 376
Parameter Morphine
(n=20)
Morphine+Ketamine
(n=21)
P-values
Age (years)* 58 ± 12 61 ± 11 0.41
Weight (kg)* 73 ± 8 76 ± 14 0.4
Male/Female* 13/9 10/12 0.16
MIDCAB/lung surgery (n)* 7/15 6/16 0.25
Duration of surgery (h)* 3.1 ± 1.3 3.5 ± 1.0 0.28
MO 1st-h consumption (mg) 6.8 ± 1.9 3.7 ± 1.2 0.0001
MO 2nd-h consumption (mg) 5.5 ± 3.6 2.8 ± 2.3 0.008
Diclofenac consumption (n) 4 1 0.14
Maximal pain (VAS 0-10)** 5.6 ± 1.0 3.7 ± 0.7 0.0001
90-min arterial blood pCO2 (mm Hg) 40 ± 6 33 ± 5 0.0003
SpO2 changes over 90min (%)*** 1.0±1.0 4.5±1.0 0.0001
Respiratory rate (breaths/minute) 19 ± 1 13 ± 1 0.0001
Wakefulness score (VAS 1-10) 1.2 ±3.2 1.2±5.5 0.0001
Incidence of PONV (n) 3 1 0.24
*Including data of the excluded (2 MO and 1 MK) patients; statistical analyses followed the 377
intent-to-analyze format. **Collected before patient's discharge. ***Difference between 378
baseline and 90-min values. 379
Page 19 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

20
Figure legends. 380
Fig. 1. CONSORT statement of the study. 381
382
Fig. 2. Four-hour pain trends (mean ± SD). 383
VAS, visual analogue scale. 384
*P<0.001 (by ANOVA with repeated measures). 385
386
Fig. 3. Square-rooted number of PCIA device applications (median and IQR). 387
*P<0.0001 (by ANOVA with repeated measures). 388
389
Fig. 4. Four-hour hemodynamics (systolic and diastolic blood pressures and heart rate) (mean 390
± SD). 391
392
Page 20 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
Excluded (n=0)
Not meetingInclusionCriteria (n=0)
Refused to Participate (n=0)
Other reasons(n=0)
Assessed forEligibility (n=44)
Randomized (n=44)
Allocated to MO (n=22)
Received allocated Intervention (n=20)
Did not receive Allocated Intervention(n=2, due topostoperativemechanical ventilation)
Allocated to MK (n=22)
Received allocated Intervention (n=21)
Did not receive Allocated Intervention:(n=1, due to postoperative mechanical ventilation)
Lost to follow-up (n=0)
Discontinued Intervention (n=0)
Conversion (n=0)
Lost to follow-up (n=0)
Discontinued Intervention (n=0)
Conversion (n=0)
Analyzed (n=20)
Excluded fromAnalysis (n=2)
Dropped out (n=0)
Analyzed (n=21)
Excluded fromAnalysis (n=1)
Dropped out (n=0)
Ana
lysi
sF
ollo
w-u
pA
lloca
tion
Enr
olm
ent
Fig. 1. Flow diagram of the progress through the phases of the randomized trial
Page 21 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

1
Fig. 2. 1
0 15 30 45 60 75 90 105 120 135 150 165 180 195 210 225 240
0
1
2
3
4
5
6
7
8
9
10
*
Morphine (MO)Morphine+Ketamine (MK)
Pai
nV
AS
(0-1
0)
Time (min) of observation
2
Page 22 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

Fig. 3.
0
2
4
6
8
10
12
14
16
MO PatientsMK Patients
*
Squ
are-
Roo
ted
Num
ber
of D
evic
e A
pplic
atio
ns
Study Groups
Page 23 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from
1
Fig. 4. 1
2
0 60 120 240
60
80
100
120
140
160
180
15 30
SBP-MO SBP-MK DBP-MO DBP-MK HR-MO HR-MK
Blo
od p
ress
ures
(m
mH
g)or
hea
rt r
ate
(bpm
)
Time (min) of observation
3
4
Page 24 of 24
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from

DOI 10.1378/chest.08-0246 published online August 27, 2008; Chest
Chazan and Avi A. Weinbroum Nachum Nesher, Margaret P. Ekstein, Yoseph Paz, Nissim Marouani, Shoshana
MORPHINE ALONE FOR IMMEDIATE POST-THORACOTOMY ANALGESIAMORPHINE WITH ADJUVANT KETAMINE VS. HIGHER DOSES OF
This information is current as of November 13, 2008
& ServicesUpdated Information
http://chestjournal.orgfigures, can be found at: Updated information and services, including high-resolution
Open Access Freely available online through CHEST open access option
Permissions & Licensing
http://chestjournal.org/misc/reprints.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://chestjournal.org/misc/reprints.shtml
Information about ordering reprints can be found online:
Email alerting servicesign up in the box at the top right corner of the online article. Receive free email alerts when new articles cite this article
Images in PowerPoint format
online article figure for directions. for teaching purposes in PowerPoint slide format. See any Figures that appear in CHEST articles can be downloaded
Copyright © 2008 by American College of Chest Physicians on November 13, 2008 chestjournal.orgDownloaded from