morgagni’s hernia gowrinath et al case report: morgagni’s hernia...
TRANSCRIPT

195
INTRODUCTION
Foramen of Morgani (sternocostal hiatus) is atriangular space located between the muscularfibres of the xiphisternum and the costal marginfibres that insert on central tendon ofhemidiaphragm. This potential space of hernialies just posterolateral to the sternum at the levelof seventh rib on either side of the xiphoidprocess. Herniation through right sternocostalhiatus is called Morgagni’s hernia (MH) andherniation through left sternocostal hiatus iscalled as Larrey’s hernia.1 MH is the leastcommon form of congenital diaphragmatichernia and majority of cases in adults aredetected incidentally on chest radiographs takenfor other indications.2 The exactpathophysiology of MH is unclear but it ispostulated that the small foramen of Morgagniis enlarged with prolonged or sudden increasein int ra-abdominal pressure allowingabdominal organs into thoracic cavity. 3
Respiratory disease as a predisposing factor ofMH in adults is infrequent.4 We report MH asan incidental finding in a middle aged womanwith bronchial asthma during preoperativescreening for cataract surgery.
CASE REPORT
A 59-year-old otherwise asymptomatic womanwas detected to have on abnormal chestradiograph while being worked up for pre-operative evaluation for cataract surgery andwas referred to us for evaluation. There was nohistory of trauma. Medical history revealedbronchial asthma for the past 30 years withperiodic acute exacerbations during rainyseasons. Patient had been using inhaled drugsregularly for the last 10 years only. Patient’sobstetric history showed normal vaginaldelivery 38 years ago. On physical examination,her body mass index (BMI) was 19.2 kg/m2.Except for the presence of cataract, physicalexamination was normal. Laboratoryinvestigations revealed haemoglobin of 10.8g/dL, total leukocyte count 9,200/mm3 with adifferential of 60% polymorphs,28%lymphocytes and 10% eosinophils. Bloodbiochemistry was normal. Postero-anteriorchest radiograph showed a right paracardiacopacity (Figure 1) and right lateral chestradiograph (Figure 2) showed the opacity in theperidiaphragmatic area of anteriormediastinum. Cardiac evaluation was normal.
Case Report:Morgagni’s hernia in a woman with bronchial asthma
K. Gowrinath,1 B.E.Panilkumar2
Departments of 1Pulmonary Medicine, 2Radiology and Imaging SciencesNarayana Medical College, Nellore
ABSTRACTA 59-year-old, other wise asymptomatic lady known to have bronchial asthma was found to have an anterior mediastinalmass on a chest radiograph incidentally obtained as a part of pre-operative work-up for cataract surgery. Computedtomography of the chest confirmed the diagnosis of Morgagni’s hernia.
Key words: Morgagni hernia, Mediastinal mass, Bronchial asthmaGowrinath K, Panilkumar BE. Morgagni’s hernia in a woman with bronchial asthma. J Clin Sci Res 2014;3:195-7.
Corresponding author: Dr. K.Gowrinath,Professor and Head, Department ofPulmonary Medicine, Narayana MedicalCollege, Nellore, India. e-mail:[email protected]
Received: 20 September, 2013.
Morgagni’s hernia Gowrinath et al
Online accesshttp://svimstpt.ap.nic.in/jcsr/jul-sep14_files/3cr314.pdf
DOI: http://dx.doi.org/10.15380/2277-5706.JCSR.13.057
196
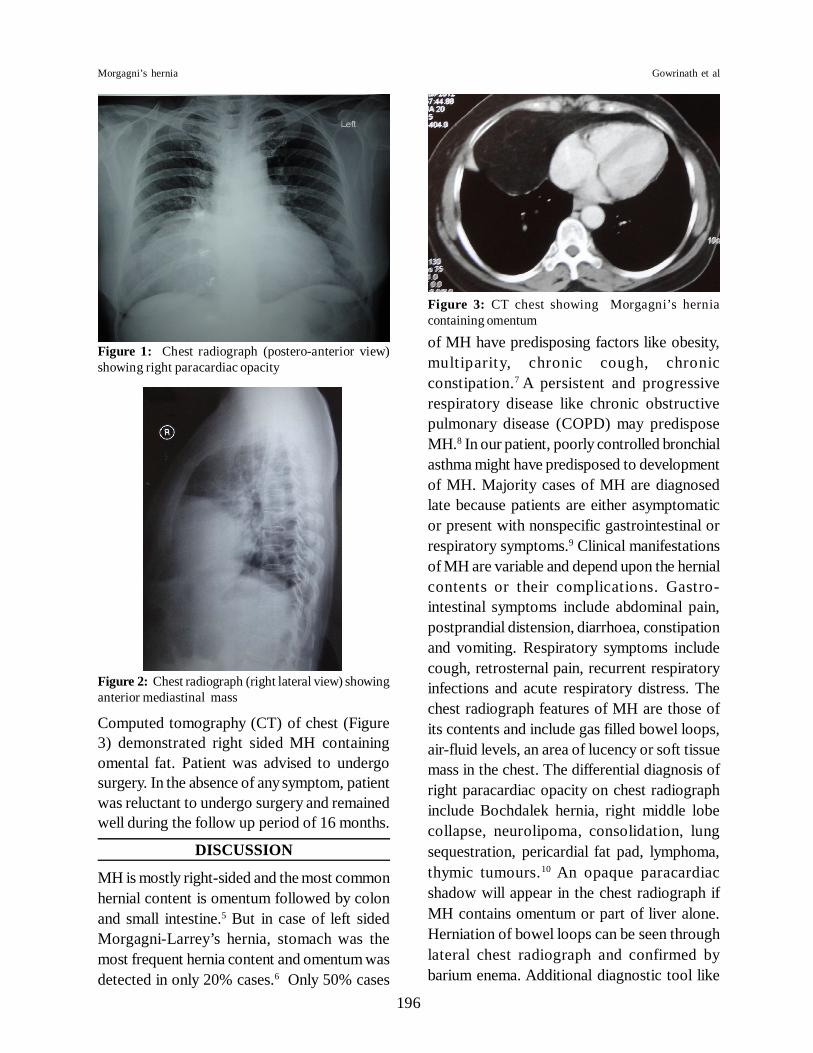
Computed tomography (CT) of chest (Figure3) demonstrated right sided MH containingomental fat. Patient was advised to undergosurgery. In the absence of any symptom, patientwas reluctant to undergo surgery and remainedwell during the follow up period of 16 months.
DISCUSSION
MH is mostly right-sided and the most commonhernial content is omentum followed by colonand small intestine.5 But in case of left sidedMorgagni-Larrey’s hernia, stomach was themost frequent hernia content and omentum wasdetected in only 20% cases.6 Only 50% cases
of MH have predisposing factors like obesity,multiparity, chronic cough, chronicconstipation.7 A persistent and progressiverespiratory disease like chronic obstructivepulmonary disease (COPD) may predisposeMH.8 In our patient, poorly controlled bronchialasthma might have predisposed to developmentof MH. Majority cases of MH are diagnosedlate because patients are either asymptomaticor present with nonspecific gastrointestinal orrespiratory symptoms.9 Clinical manifestationsof MH are variable and depend upon the hernialcontents or their complications. Gastro-intestinal symptoms include abdominal pain,postprandial distension, diarrhoea, constipationand vomiting. Respiratory symptoms includecough, retrosternal pain, recurrent respiratoryinfections and acute respiratory distress. Thechest radiograph features of MH are those ofits contents and include gas filled bowel loops,air-fluid levels, an area of lucency or soft tissuemass in the chest. The differential diagnosis ofright paracardiac opacity on chest radiographinclude Bochdalek hernia, right middle lobecollapse, neurolipoma, consolidation, lungsequestration, pericardial fat pad, lymphoma,thymic tumours.10 An opaque paracardiacshadow will appear in the chest radiograph ifMH contains omentum or part of liver alone.Herniation of bowel loops can be seen throughlateral chest radiograph and confirmed bybarium enema. Additional diagnostic tool like
Figure 1: Chest radiograph (postero-anterior view)showing right paracardiac opacity
Figure 2: Chest radiograph (right lateral view) showinganterior mediastinal mass
Figure 3: CT chest showing Morgagni’s herniacontaining omentum
Morgagni’s hernia Gowrinath et al

197
CT of the chest is required if the MH containsomentum or liver alone. CT is the mostsensitive diagnostic method of MH and maydemonstrate the extent, contents as well as itsanatomic location.11 Fatty lesion like omentalmass in the right cardiophrenic angle throughCT scan has to be differentiated from prominentepicardial fat pad, lipoma, liposarcoma andthymolipoma and this is possible if linear softtissue opacities which represent omentalvessels are visible within the fatty lesion.12 ThisCT finding helped us to diagnose hernia contentas omentum. Magnetic resonance imaging(MRI) is a non-invasive technique that candiagnose fatty lesions within MH well13 but thistechnique is rarely done now in view of its highcost, time consuming nature and requirementof skilled personell. Surgery is recommendedin all cases of MH to avoid life threateningcomplications in future. If MH containsomentum alone, surgery is advised if thesymptoms are recurrent and troublesome.14 Ourpatient has been under regular follow-up as shewas not ready to undergo surgery citing noproblem with her MH.
REFERENCES1. Hoyos DA. Foramen of morgagni hernia. In:
Shields TW, Locicero III Jr, Reed CE, Feins RHeditors. General thoracic surgery. 7th ed.Philadelphia: Lippincott and WilliamWilkins;2009.p.719-24.
2. Wolloch Y, Grunebaum M, Glanz I, Dintsman M.Symptomatic retrosternal (Morgagni) hernia. AmJ Surg 1974;127:601-5.
3. Colakoglu O, Haciyanli M, Soyturk M, ColakogluG, Simsek I. Morgagni hernia in adult: atypical
presentations and diagnostic difficulties. Turk JGastroenterol 2005;16:114-6.
4. Vassileva CM, Shabosky J, Boley T, Hazelrigg S.Morgagni hernia presenting as right middle lobecompression. Ann Thorac Cardiovasc Surg2012;18:79-81.
5. Ambrogi V, Forcella D, Gatti A,Vanni G,MineoTC. Transthoracic repair of Morgagni’s hernia. a-20- year experience from open to vedio-assistedapproach. Surg Endosc 2007;21:587-91.
6. Abraham V, Myla Y, Verghese S, Chandran BS.Morgagni-Larrey hernia- a Review of 20 cases.Indian J Surg 2012;74:391-5.
7. Aghajinzadah M, Khadem S, Jahrouri SK, GorabiHE, Ebrahimi H, Maafi AA. Clinical presentationand operative repair of Morgagni hernia. InteractCardiovasc Thorac Surg 2012;15:608-11.
8. Yadav RK, Sukhija S. Morgagni hernia. Indian JChest Dis Allied Sci 2001;43:163-4.
9. Lin ST,Moss DM, Henderson SO. A case ofMorgagni hernia presenting as pneumonia. JEmerg Med 1997;15:297-301.
10. Pineda V, Andreu J, Cáceres J, Merino X, VaronaD, Domínguez-Oronoz R . Lesions ofcardiophrenic space: findings at cross sectionalimaging. Radiographics 2007;27:19-32.
11. Minneci PC, Deans KJ, Kim P,Mathisen DJ.Foramen of Morgagni hernia: changes in diagnosisand treatment. Ann Thorac Surg 2004;77:1956-9.
12. Gossios KJ, Tatsis CK, Lykouri A,Constantopoulos SH. Omental herniation throughthe foramen of Morgagni. Diagnosis with chestcomputed tomography. Chest 1991;100:1469-70.
13. Kamiya N, Yokoi K, Miyazawa N, Hishinuma S,Ogata Y, Katayama N. Morgagni hernia diagnosedby MRI. Surg Today 1996;26:446-8.
14. Loong TP, Kocher HM. Clinical presentation ofoperative repair and hernia of Morgagni. PostgradMed J 2005;81:41-4.
Morgagni’s hernia Gowrinath et al