comparison of elisa and iif for detection of ana...
TRANSCRIPT

237
INTRODUCTION
Connective tissue diseases are a group ofdisorders that involve multiple body systemsand exhibit a wide spectrum of clinicalmanifestations.1 They share certain commonfeatures which include inflammation of skin,joints and other structures rich in connectivetissue along with altered patterns ofimmunoregulation such as production ofautoantibodies and abnormalities of cellmediated immunity.2 The term “auto-immunerheumatic disease” (ARD) is preferable to theolder term “connective tissue disease” because
the clinical effects of ARD are not limited toconnective tissues only.3 The diagnosis of ARDis arrived at taking into consideration severalclinical and laboratory criteria because thesediseases are not organ-specific and have nosingle pathognomonic finding. Each ARD maybe associated with different autoantibody types.Presence of these autoantibodies in a person isused as an aid to the diagnosis of autoimmunediseases. Anti-nuclear antibodies (ANA) refersto immunoglobulins that react against differentautologous nuclear [eg. anti-double strandeddeoxyribonucleic acid (dsDNA), anti-soluble
Original Article:Comparison of enzyme linked immunosorbant assaay (ELISA) with indirect
immunofluorescence for detection of anti-nuclear antibodyG.L.S. Sumanth Kumar,1 Abhijit Chaudhury,1 Anju Verma,1 Usha Kalawat,1
B.V. Ramana,1 B. Siddhartha Kumar2
Department of 1Microbiology, 2Division of Rheumatology, Department of Medicine, Sri Venkateswara Institute ofMedical Sciences, Tirupati
ABSTRACTBackground: Detection of antinuclear antibody (ANA) is used as one of the diagnostic criteria for autoimmunerheumatic diseases (ARD). Both indirect immunofluorescence (IIF) and enzyme linked immunosorbant assay (ELISA)methods are used for this purpose. However, there are lack of data comparing these two tests from India.Methods: We prospectively studed 294 patients clinically suspected to be having ARD between April 2012 andSeptember 2013. They were tested for ANA by IIF and ELISA methods. Representative samples positive by both thetests were processed again by a line immunoassay test to detect the specific antinuclear antibodies. Considering the IIFresults as the ‘gold standard’, the utility of ELISA for ANA detection was analyzed.Results: Of the 294 samples processed, 181 (61.5%) were from female patients. By IIF 30% of samples in males and40.3% sample in females tested positive. We found ELISA to have a poor sensitivity (45.8%) but good specificity(99.5%). The positive predictive value for ELISA were 98% and negative predictive value 76.2% respectively. Fortyfour samples positive by both IIF and ELISA were tested by Western blot to detect individual autoantibodies. Of these,only 24 samples showed the presence of one or more bands, while the remaining 20 (45.4%) were negative by lineimmunoassay. In our study anti-nuclear ribonucleoprotein/Smith was the most common ANA detected.Conclusions: The poor sensitivity raises concerns regarding the practice of initial screening for ANA by ELISA. Key Words: Anti nuclear antibody, ELISA, Indirect immunofluorescence, Line immunoassaySumanth Kumar GLS, Chaudhury A, Verma A, Kalawat U, Ramana BV, Siddhartha Kumar B. Comparison of enzyme linkedimmunosorbant assaay (ELISA) with indirect immunofluorescence for detection of anti-nuclear antibody. J Clin Sci Res2014;3:237-42. DOI: http://dx.doi.org/10.15380/2277-5706.JCSR.14.056.
Corresponding author: Dr AbhijitChaudhury, Professor and Head, Departmentof Microbiology, Sri Venkateswara Instituteof Medical Sciences, Tirupati, India.e-mail: [email protected]
Received: 22 September, 2014.
Comparison of ELISA and IIF for detection of ANA Sumanth Kumar et al
Online accesshttp://svimstpt.ap.nic.in/jcsr/oct-dec14_files/4oa414.pdf
DOI: http://dx.doi.org/10.15380/2277-5706.JCSR.14.056

238
substance A or Sjogren’s Syndrome A/Robert(SSA/Ro), and cytoplasmic components[aminoacyl transfer nibonucleic acid (tRNA)synthetase (Jo-1), mitochondria, etc].4 ThusANA usually target specific antigens in thenuclear part of the cells, and can sometimesshow affinity against all types of subcellularstructures and cell organelles, including thecytoplasm, nucleoli, or cell surfaces. ANA canbe detected in several ARDs. Although a batteryof laboratory tools are available for detectingANA, indirect immunofluorescence anti-nuclear antibody (IIF) test, fluorescent anti-nuclear antibody (FANA) test and enzymeimmunoassay (EIA) / enzyme linkedimmunosorbent assay (ELISA) are commonlyused in day-to-day practice. IIF test is currentlyconsidered to be the gold standard for detectingANA in clinical practice. By using humanepithelial -2(HEp-2) cells as the substrate, IIFtest permits the detection of antibodies to morethan 30 different nuclear and cytoplasmicantigens comprising more than 50autoantibodies.5
Because of the ease of performing the test ANAdetection by ELISA has often been used forscreening purposes. Other main methods usedfor detection of specific antibodies include gelprecipitation assays, passive haemagglutina-tion, Western blot, multiple immunoassay, flowcytometry and antigen microassay.6
This study was undertaken to assen usefulnessof ELISA for detecting ANA compared to thegold standard of indirect immunofluorescenttest and identification of specific importantant inuclear autoant ibodies by lineimmunoassay.
MATERIALS AND METHODS
We prospectively studied 294 patients clinicallysuspected to have ARD who presented to theRheumatology Clinic at the Sri VenkateswaraInstitute of Medical Sciences (SVIMS),Tirupati, whose samples were submitted to the
Department of Microbiology SVIMS Tirupati,for testing for ANA during the period April2012 to September 2013. The study wasapproved by the Institutional EthicalCommittee.
All the serum samples were kept at –20 oCuntil they were processed and were tested byindirect immunofluoresence antinuclear anti-body test (Aeskuslides ANA HEp-2, AeskuDiagnostics, Germany) and ELISA wasperformed using Auto StatTM Anti-NuclearAntibody (ANA) screen (Hycor BiomedicalInc.USA). For ELISA, serum samples showingANA concentration greater than 23 IU/mL weretaken as positive as recommended by the kitmanufacturer. Representative samples positiveby both the tests were processed again by lineimmunoassay test to detect the specificantinuclear antibodies using Euroline ANAProfile 3 (Euroimmun, Germany). It cansimultaneously detect antibodies to nuclearribonucleoprotein / Smith (nRNP / Sm), Smith(Sm), soluble substance A or Sjogren’ssyndrome A, Robert-52 (SSA, Ro-52) , solublesubstance B or Sjogren’s syndrome B (SSB),DNA topoisomerase 1 or scleroderma-70 (Scl-70), polymyositis-scleroderma (PM-Scl),proliferating cell nuclear antigen (PCNA),cytoplasmic histidyl tRNA synthetase (Jo-1),centromere protein-B (CENP-B), doublestranded deoxyribonucleic acid (dsDNA),nucleosomes, histones, ribosomal protein-P,anti-mitochondrial antibodies (AMA-M2).Thekit manufacturers’ instructions were followedfor all the tests. The sensitivity, specificity,positive predictive value (PPV) and thenegative predictive value (NPV) of ELISA werecalculated considering IIF as the “goldstandard”.
RESULTS
Of the 294 samples studied, 113 (38.4%) wereobtained from male patients and 181 (61.5%)were from female patients. Among males, 34
Comparison of ELISA and IIF for detection of ANA Sumanth Kumar et al
239
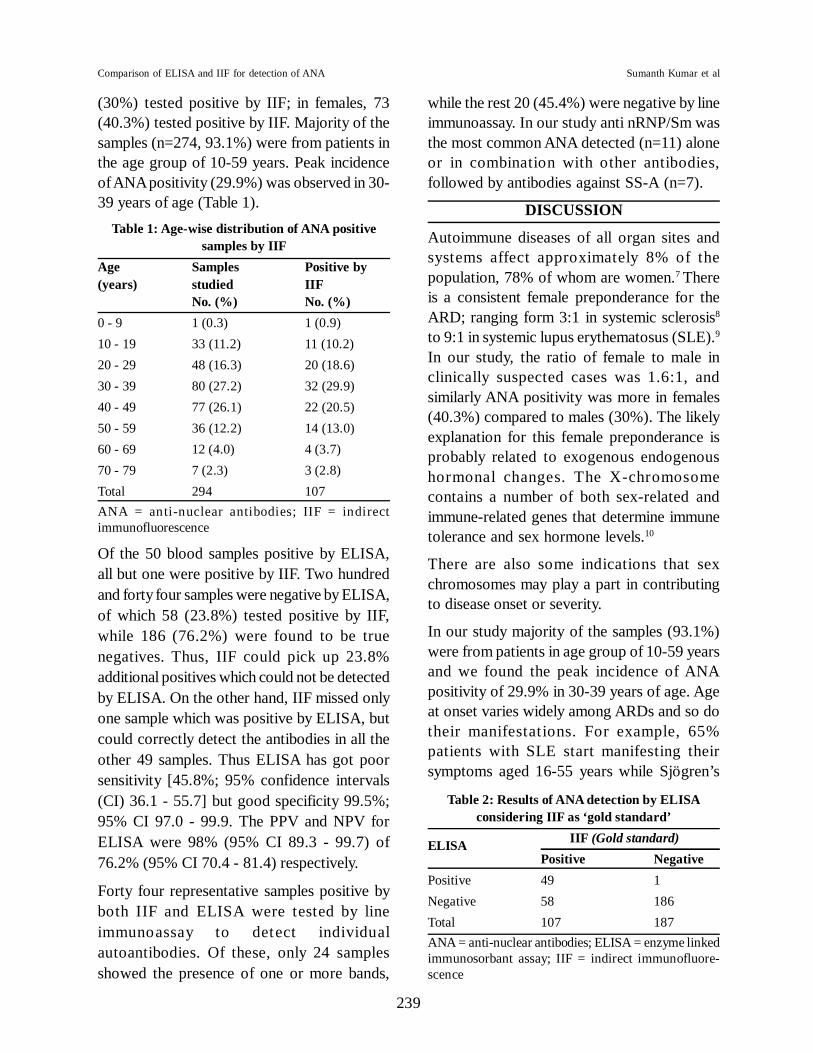
(30%) tested positive by IIF; in females, 73(40.3%) tested positive by IIF. Majority of thesamples (n=274, 93.1%) were from patients inthe age group of 10-59 years. Peak incidenceof ANA positivity (29.9%) was observed in 30-39 years of age (Table 1).
Table 1: Age-wise distribution of ANA positivesamples by IIF
Age Samples Positive by(years) studied IIF
No. (%) No. (%)0 - 9 1 (0.3) 1 (0.9)10 - 19 33 (11.2) 11 (10.2)20 - 29 48 (16.3) 20 (18.6)30 - 39 80 (27.2) 32 (29.9)40 - 49 77 (26.1) 22 (20.5)50 - 59 36 (12.2) 14 (13.0)60 - 69 12 (4.0) 4 (3.7)70 - 79 7 (2.3) 3 (2.8)Total 294 107ANA = anti-nuclear antibodies; IIF = indirectimmunofluorescence
Of the 50 blood samples positive by ELISA,all but one were positive by IIF. Two hundredand forty four samples were negative by ELISA,of which 58 (23.8%) tested positive by IIF,while 186 (76.2%) were found to be truenegatives. Thus, IIF could pick up 23.8%additional positives which could not be detectedby ELISA. On the other hand, IIF missed onlyone sample which was positive by ELISA, butcould correctly detect the antibodies in all theother 49 samples. Thus ELISA has got poorsensitivity [45.8%; 95% confidence intervals(CI) 36.1 - 55.7] but good specificity 99.5%;95% CI 97.0 - 99.9. The PPV and NPV forELISA were 98% (95% CI 89.3 - 99.7) of76.2% (95% CI 70.4 - 81.4) respectively.
Forty four representative samples positive byboth IIF and ELISA were tested by lineimmunoassay to detect individualautoantibodies. Of these, only 24 samplesshowed the presence of one or more bands,
while the rest 20 (45.4%) were negative by lineimmunoassay. In our study anti nRNP/Sm wasthe most common ANA detected (n=11) aloneor in combination with other antibodies,followed by antibodies against SS-A (n=7).
DISCUSSION
Autoimmune diseases of all organ sites andsystems affect approximately 8% of thepopulation, 78% of whom are women.7 Thereis a consistent female preponderance for theARD; ranging form 3:1 in systemic sclerosis8
to 9:1 in systemic lupus erythematosus (SLE).9
In our study, the ratio of female to male inclinically suspected cases was 1.6:1, andsimilarly ANA positivity was more in females(40.3%) compared to males (30%). The likelyexplanation for this female preponderance isprobably related to exogenous endogenoushormonal changes. The X-chromosomecontains a number of both sex-related andimmune-related genes that determine immunetolerance and sex hormone levels.10
There are also some indications that sexchromosomes may play a part in contributingto disease onset or severity.
In our study majority of the samples (93.1%)were from patients in age group of 10-59 yearsand we found the peak incidence of ANApositivity of 29.9% in 30-39 years of age. Ageat onset varies widely among ARDs and so dotheir manifestations. For example, 65%patients with SLE start manifesting theirsymptoms aged 16-55 years while Sjögren’s
Table 2: Results of ANA detection by ELISAconsidering IIF as ‘gold standard’
ELISA IIF (Gold standard)Positive Negative
Positive 49 1Negative 58 186Total 107 187ANA = anti-nuclear antibodies; ELISA = enzyme linkedimmunosorbant assay; IIF = indirect immunofluore-scence
Comparison of ELISA and IIF for detection of ANA Sumanth Kumar et al

240
syndrome is considered to be more prevalentin women between ages 45 and 50.11
In our study we evaluated the performance ofELISA in the detection of ANA considering IIFas ‘gold standard’. The sensitivity andspecificity of ELISA in our study were 45.8%and 99.5% respectively. A study fromBangladesh12 found low sensitivity of 55%with ELISA, when compared with IIF for ANAdetection in childhood SLE cases which iscomparable with our study. However, in anotherstudy13 four ANA ELISA kits were evaluatedand a high sensitivity ranging from 90% to 97%and specificities ranging from 36% to 94% wereobserved when compared to IIF in patient withSLE. One explanation for the high sensitivityobserved in this study13 may be the use ofclinically defined samples. Another study14
reported the performance of five ELISA kitsand comparing them with IIF and found thatthe sensitivity and specificity of differentELISA kits ranged from 69.5% to 97.7% and81.4% to 97.9% respectively. We found asimilar high specificity for ELISA in our study.An explanation for low sensitivity in our studymay be due to the use of imported kits whichgave a high cut-off concentration levels todifferentiate a positive and a negative sample.It appears logical that whenever imported kitsare used it may be necessary to define a cut offconcentration based on local population studies.The other more likely explanation may be dueto the limited number of antigens used in theELISA which may not reflect the autoantibodypatterns of the local population. There may alsobe racial and/or ethnic differences in theautoantibody patterns found in differentpopulation groups.15
We found that ELISA had a PPV and NPV of98% and 76.2% respectively. A PPV and NPVof 100% and 69% respectively were reportedfor ELISA in one study.12 However, a PPV andNPV of ELISA as 35.8% and 96.4%respectively were reported in another study.13
This difference may be due to differences instudy population and the inclusion criteria usedin these studies.12,13
The ELISA test formats use a cocktail of 10-14 antigens, depending on the commercial kitused. The antigens used may be native orrecombinant.13 Almost all the kits containdisrupted human epithelial -2 (HEp-2) cells tosupply the same antigenic sites found in HEp-2 IIF test. The use of this component remainscontroversial since some argue that it increasessensitivity while others maintain that it lowersspecificity. On the other hand, IIF test formatsuse HEp-2 cells which contain high concen-tration of nuclear and cytoplasmic antigenswhich results in higher sensitivity. Thus it isunderstandable that ELISA with its limitedcontent of antigens may fail to detect certainantibodies which can be detected by IIF.
We studied 44 representative samples by lineimmunoassay method to detect specific ANAs.Among these 44 samples, 24 (54.5%) weredetected positive for ANA showing either singletype or a combination of two or more. In ourstudy anti nRNP/Sm was the most commonANA detected (13 out of 44, 29.5%) and ANAagainst SS-A antigen being the second ( 8 outof 44, 18.1%). The Sm and nRNP antigens aretargets for autoant ibodies in SLE, andconsidered specific for this condition. 17
However, Sm autoantibodies appear in only20%-30% of SLE patients while nRNPantibodies are found in 30%-40% cases.Further, while anti-Sm is highly specific forSLE, anti-nRNP is relatively non-specific andmay appear in various other conditions.18 Sinceboth these autoantibodies are detected in thesame band in the line immunoassay test,isolated presence of these bands in the absenceof other SLE specific bands like anti-dsDNAmay not be significant. The SS-A band, whichwas the second most common band patternobserved in our study is found in a variety ofARDs, particularly SLE and Sjögern
Comparison of ELISA and IIF for detection of ANA Sumanth Kumar et al

241
syndrome.17 Co-relation with other bandpatterns is equally important in theinterpretation of SS-A band like nRNP/Sm.Remaining 20 of the 44 samples did not showany banding by line immunoassay though theywere positive by IIF. Probably these serumsamples had some antibodies other than themost common ones coated on the strips usedin line assay. The same issue was addressed inanother study19 and the authors reported that17.2% samples which were positive for ANAby IIF were negative by line immunoassaymethod. Hence, though by line assay we coulddifferentiate ANA, it may sometimes miss thedetection of rare ANAs. In our study line assayshowed positivity for nRNP/Sm, SS-A, SS-B,dsDNA, AMA-M2, and nucleosomes in onesample, and nRNP/Sm, Sm, dsDNA, andnucleosomes in another sample. This showsthat this method has the advantage to detectpatients with overlap syndrome, giving moreinformation about the ANA present in thepatient sample than IIF, which needs greaterexpertise to detect different patterns of ANAin a single sample.
ELISA has gained popularity since by thismethod ANA assay can be performed on amultiplex platform, with larger number ofsamples in a quicker time and at a much lowercost. Moreover, IIF has a subjectiveinterpretation which depends on the experienceof the person performing the test while ELISAformat has objective well defined parameters.For these reasons, ELISA is increasinglygaining popularity as an initial screening test,followed by confirmation of positive samplesby IIF-ANA. However, low sensitivity andpropensity for false-negative ELISA resultsraises concerns regarding the practice of usingELISA method for the detection of ANA as theinitial screening method.
REFERENCES1. Doherty M, Ralston SH. Musculoskeletal diseases.
In: Colledge NR, Walker BR, Ralston SH, editors.
Davidson’s Principles and Practice of Medicine,21st edition. New York: Chruchill Livingstone;2010.p.1053-1129.
2. Fauci AS, Langford CA. SLE, RA, and otherconnective tissue diseases. In: Fauci AS,Braunwald E, Kasper DL, Hauser SL, Lango DL,Jameson JL, et al. editors. Harrison’s principlesof internal medicine. 17th edition. Philadelphia:McGrawHill; 2009.p.885-91.
3. Shipley M, Rahman A, O’Gradiagh D, ConwayR. Rheumatology and bone disease. In: Kumar P,Clark M, editors. Kumar & Clark’s clinicalmedicine, 8th edition. New York: SaundersElsevier; 2012.p.493-560.
4. Tan EM. Autoantibodies to nuclear antigens(ANA): their immunobiology and medicine. AdvImmunol 1982;33:167-240.
5. Bradwell AR, Hughes RG, Karim AR.Immunofluorescent antinuclear antibody tests. In:Detrick B, Hamilton RG, Folds JD, editors. Manualof molecular and clinical laboratory immunology,7th edition. Washington, DC: ASM press;2006.p.995-1006.
6. Kumar Y, Bhatia A, Minz RW. Antinuclearantibodies and their detection methods in diagnosisof connective tissue diseases: a journey revisited.Diagn Pathol 2009;4:1.
7. Fairweather D, Frisancho-Kiss S, Rose NR. Sexdifferences inautoimmune disease from apathological perspective. Am J Pathol2008;173:600-9.
8. Chifflot H, Fautrel B, Sordet C, Chatelus E, SibiliaJ. Incidence and prevalence of systemic sclerosis:a systematic literature review. Semin ArthritisRheum 2008;37:223-35.
9. D’Cruz DP, Khamashta MA, Hughes GR.Systemic lupus erythematosus. Lancet2007;369:587-96.
10. Oliver JE, Silman AJ. Why are women predisposedto autoimmune rheumatic diseases? Arthritis ResTher 2009;11:252.
11. Amador-Patarroyo MJ, Rodriguez-Rodriguez A,and Montoya-Ortiz G. How Does Age at onsetinfluence the outcome of autoimmune Diseases?Autoimmune Diseases 2012, doi:10.1155/2012/251730.
12. Dipti TR, Azam MS, Sattar MH, Rahman SA.Detection of anti-nuclear antibody byimmunofluorescence assay and enzymeimmunoassay in childhood systemic lupus
Comparison of ELISA and IIF for detection of ANA Sumanth Kumar et al
242
erythematosus: experience from Bangladesh. IntJ Rheum Dis 2012;15:121-5.
13. Copple SS, Sawitzke AD, Wilson AM, Tebo AE,Hill HR. Enzyme linked immunosorbent assayscreening then indirect immunofluorescenceconfirmation of antinuclear antibodies: a statisticalanalysis. Am J Clin Pathol 2011;135:678-84.
14. Jaskowski TD, Schroder C, Martins TB, MouritsenCL, Litwin CM, Hill HR. Screening for antinuclearantibodies by enzyme immunoassay. Am J ClinPathol 1996;105:468-73.
15. Pisetsky DS. Antinuclear antibodies in healthypeople: the tip of autoimmunity’s iceberg? ArthritisRes Ther 2011,13:109.
16. Gniewek RA, Stites DP, McHugh TM, HiltonJF, Nakagawa M. Comparison of antinuclearantibody testing methods: immunofluorescence
assay versus enzyme immunoassay. Clin DiagnLab Immunol 1997;4:185-8.
17. Kavanaugh A, Tomar R, Reveille J, Solomon DH,Hamburger HA. Guidelines for clinical use of theantinuclear antibody test and tests for specificautoantibodies to nuclear antigens. Arch PatholLab Med 2000;124:71-81.
18. Peng SL, Craft JE Antinuclear antibodies. In:Firestein GS, Budd RC, Gabriel SE, McInnes IB,O’dell JR, editors. Kelley’s textbook ofrheumatology. 9th edition. Philadelphia: SaundersElsevier; 2013.p.789-803.
19. Sebastian W, Roy A, Kini U, Mullick S.Correlation of antinuclear antibodyimmunofluorescence patterns with immune profileusing line immunoassay in the Indian scenario.Indian J Pathol Microbiol 2010;53:427-32.
Comparison of ELISA and IIF for detection of ANA Sumanth Kumar et al