monthly conference calls compendium july 2013 may · pdf filemonthly conference calls...
TRANSCRIPT

Monthly Conference Calls Compendium
July 2013 – May 2014
Strategies
Janet Gingold, MD, MPH
CIzQIDS Project QI Coach

These slides were compiled for the conference calls for the
Quality Improvement Technical Support program of the
Comparison of Immunization Quality Improvement
Dissemination Strategies (CIzQIDS) project, June 2013-June
2014 to stimulate discussions about strategies for improving
immunization delivery.
Immunization recommendations are subject to change as new
data becomes available. Users are advised to check for
updates of recommendations.
2
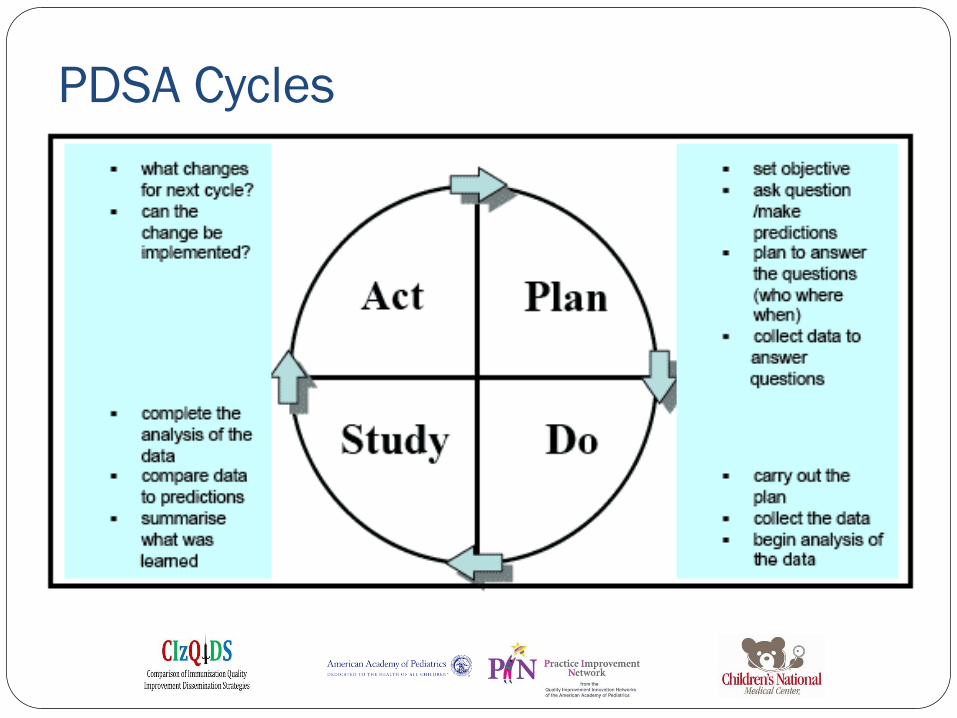
PDSA Cycles

Steps in developing improvements
Step 1: Diagnostic journey
In depth review of performance
Step 2: Prioritization
Identify high-impact improvement issues
Step 3: Organizing the work
Define people and resources needed
Step 4: Work planned
Focused and clearly defined action
Step 5: Learning and recalibration

Example 1: The Common Theme
Problem to address: Missed opportunities result in low
immunization compliance rates
Change to test: Assess immunization status at every visit
Measurement of effect: Percent of visits where review of
immunization status is documented
Anticipated problems
Getting the complete immunization record
Ensuring that “decider” has necessary training and resources
Suggestions (white board)

Example 2: Different ways to chart your course

Example 3 GOAL CURRENT
PRACTICE-
Well Check visits
Intervention: Change
in immunization
practice
Test
intervention
or Task
Timeline
To Improve
documentation
practices in our
clinic
(NextGen) and
state
(Immprint).
1. Nurse check Immprint and
NextGen.
2. Provider will review
NextGen records and will
decide which immunizations
are due for visit.
3. Nurses will notify provider if
any records are missing in
Nextgen but are present in
Immprint.
4. Provider will order shots in
NextGen. 5.
Nurse will give shots.
6. Nurse documents shots in
NextGen and Immprint and she
will bill immunizations in
NextGen.
On patients >=2mo to <=18mo
attending clinic for well check
visits on Wed-Th-frid for 2 weeks:
1.The day before visit, Nurse will
check Immprint and Nextgen to
check for immunization status and
if outside records are need to be
obtained from another
clinic/hospital.
2. Nurse will print Immprint and
NextGen immunization records
and will give them to provider on
day of patient 's visit.
3. Provider will check NextGen
and Immprint printed records to
see which immunizations are due
at that visit.
4. Provider will order shots in
NextGen.
5. Nurse will give ordered shots.
6. Nurse will document shots in
NextGen and Immprint and she
will bill immunizations in
NextGen or she will documented
parent refusal to immunizations in
both systems.
Test
Will review
immunization
records for all
patients who met
criteria for
intervention and we
will assess:
1. Percentage of pts
who got incomplete
or no intervention.
2. Reason for each
case of this
happening.
Aug 15 to Aug 30th
To Improve printed material/aids to
informed/educate families about
immunizations
1. Currently there are no printed nor audio-visual education
materials related to immunizations are available in waiting rooms
and very limited availability in patient rooms.
1) Will display posters, handouts, booklets and videos containing
educational material regarding immunizations.
Task Will need to obtain supplies to display printed
materials (booklet/handout holders).
Timeline depends on availability if these supplies
Provide information to parents about
free immunization reminder
(internet/mobile app)."Vaccination
reminder-Pediatric On call)
Currently there are no automatic media immunization reminders
available to our patients.
1) We will display information about where to find and download
this app using printed materials to be displayed in our waiting rooms
and pt rooms. 2). When possible,
personal assistance by clinic staff will be provided to parents
/guardians to help set up app in their mobile phones.
Task Will need to obtain supplies to display printed
materials (booklet/handout holders).
Timeline depends on availability if these supplies
What are we
already doing? What will
we do
differently?
How will
we measure
the effect?
When?
Who?
Why?

GOAL CURRENT PRACTICE-
Well Check visits
Intervention: Change in
immunization practice
Test
intervention or
Task
Timeline
To Improve documentation practices in
our clinic (NextGen) and state
(Immprint).
1. Nurse check Immprint and NextGen.
2. Provider will review NextGen records and will decide
which immunizations are due for visit.
3. Nurses will notify provider if any records are missing in
Nextgen but are present in Immprint.
4. Provider will order shots in NextGen. 5.
Nurse will give shots. 6.
Nurse documents shots in NextGen and Immprint and she will
bill immunizations in NextGen.
On patients >=2mo to <=18mo attending clinic for well check
visits on Wed-Th-frid for 2 weeks:
1.The day before visit, Nurse will check Immprint and Nextgen to
check for immunization status and if outside records are need to be
obtained from another clinic/hospital.
2. Nurse will print Immprint and NextGen immunization records
and will give them to provider on day of patient 's visit.
3. Provider will check NextGen and Immprint printed records to see
which immunizations are due at that visit.
4. Provider will order shots in NextGen.
5. Nurse will give ordered shots. 6. Nurse
will document shots in NextGen and Immprint and she will bill
immunizations in NextGen or she will documented parent refusal to
immunizations in both systems.
Test
Will review immunization records for all
patients who met criteria for
intervention and we will assess:
1. Percentage of pts who got incomplete
or no intervention. 2.
Reason for each case of this happening.
Aug 15 to Aug 30th
To Improve
printed
material/aids to
informed/educat
e families about
immunizations
1. Currently there are no
printed nor audio-visual
education materials related
to immunizations are
available in waiting rooms
and very limited availability
in patient rooms.
1) Will display posters,
handouts, booklets and videos
containing educational
material regarding
immunizations.
Task Will need to obtain
supplies to display
printed materials
(booklet/handout
holders).
Timeline depends on
availability if these
supplies
Provide
information to
parents about
free
immunization
reminder
(internet/mobile
app)."Vaccinatio
n reminder-
Pediatric On call)
Currently there are no
automatic media
immunization reminders
available to our patients.
1) We will display information
about where to find and
download this app using
printed materials to be
displayed in our waiting
rooms and pt rooms.
2). When possible, personal
assistance by clinic staff will
be provided to parents
/guardians to help set up app
in their mobile phones.
Task Will need to obtain
supplies to display
printed materials
(booklet/handout
holders).
Timeline depends on
availability if these
supplies 8
“Yes, and…”
Thinking about and
planning for future
PDSA cycles

What’s next? Continue PDSA cycles!
• Implement your plan • Measure its effect • Analyze the results • Discuss with your team
• Use what you learn to
develop a new plan • Check in with coach as
needed
9
Breakthrough
Results
Theories,
hunches,
& best practices
A P S D
A P S D
A P S D
A P S D

Addressing Administrative Barriers
Do you have trouble with your supply of VFC vaccines?
How do you deal with seasonal fluctuations in vaccine supply
and demand? Any tips about how to estimate need in advance
and expedite orders from VFC?

Follow up: Immunization assessment
How do providers respond to having the immunization status
assessment available at the beginning of the visit?
How is this information used?
Does it result in more attention to immunizations in the
treatment plan and improved delivery of immunizations?
11

How to get providers to use the
information better
Design a prompt that requires response
When, where, and how to present the prompt
Increase responsibility of nursing staff
Reminder during treatment plan/exit process
Give shots under standing orders
What works for you?
12

Influenza Vaccine for Health Care
Workers CDC recommends that health care workers get annual flu vaccine
During the 2010-2011 season, an estimated 63.5% of health care workers got flu shots
Where employers required flu vaccine, coverage rates were 98%
More health care workers got flu shots if Vaccine was offered on site Vaccine was offered free of charge Vaccine was available on multiple days
Health care workers who don’t get flu shots were less likely to believe Flu shots are safe and effective Flu shots are worth the time and effort Flu is a significant threat to self/others
13

Influenza Vaccine for Health Care
Workers CDC recommends that health care workers get annual flu vaccine
During the 2010-2011 season, an estimated 63.5% of health care workers got flu shots
Where employers required flu vaccine, coverage rates were 98%
More health care workers got flu shots if Vaccine was offered on site Vaccine was offered free of charge Vaccine was available on multiple days
Health care workers who don’t get flu shots were less likely to believe Flu shots are safe and effective Flu shots are worth the time and effort Flu is a significant threat to self/others
14

Walking the walk
22%
44%
11%
11%
11%
Which best describes your
position regarding your own influenza immunization for
2013-2014
Already had it
Have a plan to get it soon
Intend to; no plan yet
Don't intend to
No answer
1. Don’t be a vector
2. Protect the vulnerable
3. Model vaccine-acceptance
4. Promote vaccine awareness
5. Establish pro-vaccine culture
Talking the talk
Flu shots
don’t cause
flu
We all have a
responsibility to decrease
the chance that we will
spread a preventable
disease to someone else
Of course! I had mine as
soon as I could to build up
my immunity before flu
season starts
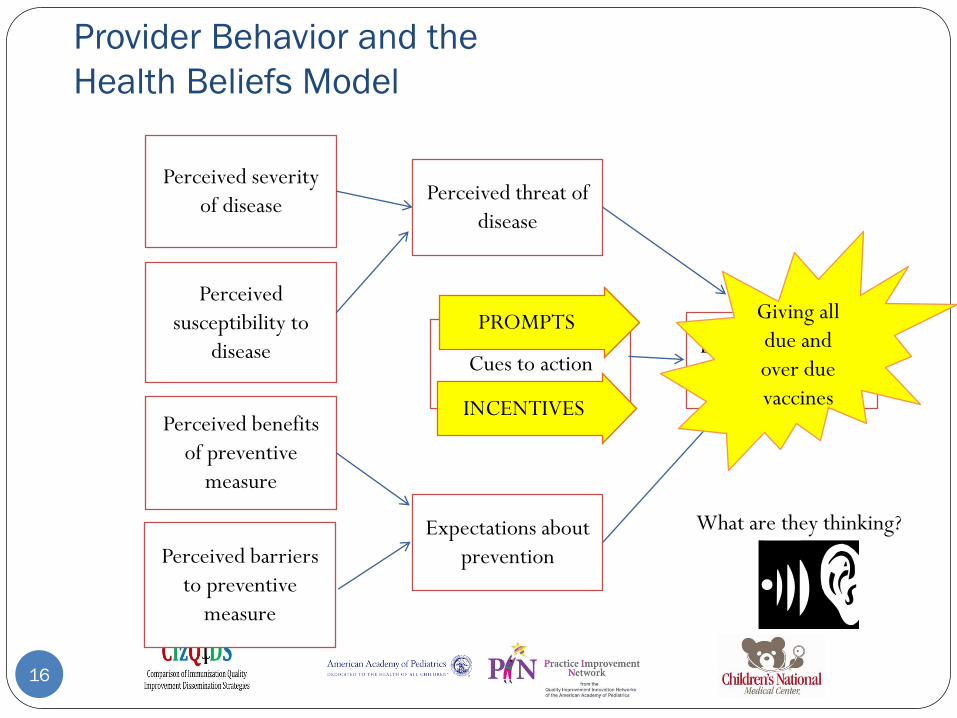
Provider Behavior and the
Health Beliefs Model
16
Perceived severity
of disease
Likeliness of taking
preventive measure
Perceived threat of
disease
Perceived benefits
of preventive
measure
Perceived
susceptibility to
disease Cues to action
Perceived barriers
to preventive
measure
Expectations about
prevention
Giving all
due and
over due
vaccines
PROMPTS
What are they thinking?
INCENTIVES

Training providers and staff to do
things differently
What resources or trainings
have been helpful?
Do reminders work?
Do incentives work?
Does seeing the results of
chart reviews work?
Studies show:
Provider reports of what they
think they do don’t match what
they actually do.
Missed opportunity are more
highly correlated with
difference in motivation than
with difference in knowledge.

Remind and Recall:
What works for you?
Here’s the list of patients
who are overdue for shots
according the state
registry. How should we contact
them? Can we afford a
mailing? Do we have time
to call them all?
What about email?

Building Remind and Recall Systems
Registry
training
EMR tools Registry
tools
Old
fashioned
“tickler”
postcards

When you send a message out into the deep,
how do you know if anybody hears it?

What are you measuring to see if it’s
working?
How many messages go out?
How many messages get received?
How many recipients respond to the message?
How easy is it for the recipient to make an appointment or
come in when they get the “cue to action”?
What message works best?
Cues work best if they contain all the information the recipient
needs to respond as desired
Number to call; best time to call; walk-in times

Robert Tremaine Hall, JD Bob Hall is currently the Associate Director of the
Washington, DC office of the American Academy of
Pediatrics. His work is focused on federal advocacy related
to children's health, specifically in the areas of access to
care; health care financing; Medicaid/CHIP; quality and
system reform; and pediatric practice.
He has chaired the AAPs Children’s Health Group, which was involved in reauthorizing the
Children’s Health Insurance Program in 2007-2009 and now focuses on health reform
implementation and its impact on children. Mr. Hall serves as the Academy’s staff lead on
health reform efforts and has presented across the country on health reform’s likely impact
on children.
Prior to joining the AAP, he served as Legislative Counsel to Senator Mark Drayton of
Minnesota, managing portfolios related to health care, labor, immigration, social security
and Medicare prescription drug coverage. He holds a BA in political science from
Haverford, a Masters in Public Affairs from the Lyndon B. Johnson School of Public Affairs
and a Juris Doctorate from the University of Texas School of Law in Austin.

Immunizations and the ACA
No copays for preventive care, including immunizations
Increased administration fees under Medicaid
Less need for referrals to FQHCs and RHCs once more have
private coverage through exchanges?

In states with Medicaid expansion, more might be
eligible for VFC
In some states, coverage of previously underinsured
through exchanges might mean purchasing more
private stock
Section 317 funds will not be used for individuals who
have any form of insurance
VFC and Section 317

Exchanges
Vary from state to state
All must offer preventive care benefits with no copay
How to get information about contracting with exchange
plans in your state

Other issues
Transition to adulthood for Medicaid patients and foster
children
Health insurance for small businesses
Other questions?

Plan-do-STUDY-act
27
Analyze your
observations
Share your ideas
about the factors
that contributed to
the outcome
Study how the
pieces fit together.

It usually takes multiple short cycles to get from where
you are to where you want to go
Breakthrough
Results
Theories,
hunches,
& best practices
A P S D
A P S D
A P S D
A P S D

An example: Developing a form for
vaccine refusers Plan Wanted: A form for consistent, easily
documentable communication of consequences
of vaccine refusal
Do Work with team to develop form; collect
feedback from providers
Study Consider feedback from multiple
providers
Act Adjust form based on feedback
Plan Determine how well parents understand
the form
Do One provider tries out form with parents
with different viewpoints; collects feedback
Study Consider feedback from multiple parents
Act Adjust form based on feedback and try with
more providers/parents

Follow through
Plan Make form available in “patient instructions” part of
EMR
Do Upload form; inform providers about availability; track
usage; after one week, review charts with ICD 9 code for
vaccine refusal to see how many were given form; ask
providers for further feedback
Study
Act

Meningitis Outbreak in Princeton
7 cases of meningitis due to N. meningitidis Serogroup B since
March 2013.
Meningococcal Vaccines currently approved for use in US cover
Serogroups A, C, Y and W-135, but not B.
University Trustees, CDC, FDA considering possibility of
importing different vaccine that is in use in Europe and Australia
that includes Serogroup B
As of Tuesday, FDA has approved import of vaccine for use there

Dealing with shortages
How do you find out about shortages?
from your local vaccines rep?
from the VFC program?
CDC website? http://www.cdc.gov/vaccines/vac-
gen/shortages/default.htm
Consider signing up for CDC email updates or updates from
your state immunization program.
Dealing with shortages
Do you keep track of patients who miss vaccines due to
shortages and call them when they come in?
If so, how?
When you have vaccine shortages, how do you
distribute triage the smaller supply?
What groups get priority?
Do you outreach to priority groups?
If so, how?

Selling parents on timely immunization
Marketing principle: Audience segmentation
Message should be targeted to the needs of the segment of
the population you are talking to.
Wrong message for that segment might be
counterproductive
You need to know something about the thinking of the
person you are talking to

Categories of parents:
Positions on vaccination
Percentages may vary greatly from place to place and from practice to practice

Hot off the press
Opel et al analyzed videotaped vaccine-related
discussions during 111 well-child visits involving 16
providers from 9 practices in the Seattle area.
Parents were categorized as vaccine-hesitant or not
based on responses to a questionnaire completed
before the visit about vaccine attitudes.
Videotapes were examined for specific types of
communications and relationships between
communications and vaccine acceptance were
explored.
Opel DJ, Heritage J, Taylor JA, Mangione-Smith R, Salas HS, DeVere B, Zhou C,
Robinson JD. The Architecture of Provider-Parent Vaccine Discussions at Health Supervision Visits. Pediatrics 2013; 132(6):1-10
36

How are vaccination conversations
initiated?
Participatory
Provide parents with relatively more decision-
making latitude
“Are we going to do shots today?”
“What do you want to do about shots?”
“You’re still declining shots?”
Presumptive
Presupposes that parents will vaccinate the child
“Well, we have to do some shots”
“We’ll do three shots and an oral vaccine today, okay?”
37

Make a prediction
Which approach will get vaccine-hesitant parents
to accept vaccination?
Participatory
Presumptive
Neither one will work better than the other
38

What would YOU do?
When parents voice resistance, what do you do?
Accept parent’s position
Offer a mitigated plan (fewer, later…)
Continue pursuit of initial plan
39

What did the study find?
40
Most pediatricians used presumptive format.
Participatory format was used more often with hesitant parents.
Provider use of participatory initiation formats was associated with a
significantly increased odds of parental resistance.
When parents resisted recommendations, half of providers pursued their
original recommendation.
After initial resistance, 9 of 19 (47%) of parents accepted the provider’s
vaccine recommendation immediately after provider pursued it.
Conclusion: How you start the conversation affects vaccine
acceptance. Despite initial resistance, many parents are
persuadable.

Quality improvement for
essential components of care:
Training resources for staff
Staff with varying skills require regular training
for consistent immunization delivery
In-house training course
Teaching tools and resources
EZIZ online modules
AAP Immunization training guide
CDC Vaccine Storage and Handling Toolkit

Staff training: What do you do?
Is regular immunization training required By your state?
By your organization?
Do staff get educational activities paid for by your organization?
Do you do in-house training?
Do you go to conferences?
Have you used on-line training modules?
Have you used trainers from your VFC program?

Training staff to screen for
contraindications What screening tool do you use?
How long does it take to complete the questionnaire?
Who does what, when?
How is the data entered into the medical record?
What if there is a “yes” response?
Who decides what to do?
What’s the process?
Do valid contraindications get entered in progress note,
problem list….
Any problems with this process?
Recommended solutions for these problems?

Categories of parents:
Positions on vaccination
Percentages may vary greatly from place to place and from practice to practice.
Vaccine communication needs to be tailored to parent’s position and cognitive style.

Alison Singer
Alison Singer is Co-Founder and President of the Autism Science
Foundation which supports autism research by providing funding and
other assistance to scientists and organizations conducting, facilitating,
publicizing and disseminating autism research.
Founded by parents of children with autism, ASF also provides
information about autism to the general public and serves to increase
awareness of autism spectrum disorders and the needs of individuals and
families affected by autism. The organization adheres to rigorous scientific
standards and values.
Alison has served on the Federal Interagency Autism Coordinating
Committee and the AAP’s New York State Immunization Coalition, and
played a significant role in the passage of the Combatting Autism Act of
2006. She is a frequent spokesperson on issues related to autism and
autism research.

New 4-step Framework for
Communicating Science: Making the
CASE for Vaccines
Corroborate: Acknowledge the parents’ concern and find some
point on which you can agree. Set the tone for a respectful,
successful talk.
About Me: Describe what you have done to build your
knowledge base and expertise
Science: Describe what the science says
Explain/Advise: Give your advice to patient, based on the
science
© 2009 Autism Science
Foundation, Inc. All Rights
Reserved.

Top Three Parent Concerns about
Vaccines
Vaccines Cause Autism
The diseases are not so bad (better to fight them naturally)
Too Many Too Soon (let’s slow down the schedule)
© 2009 Autism Science
Foundation, Inc. All Rights
Reserved.

© 2009 Autism Science
Foundation, Inc. All Rights
Reserved.
I heard on TV that vaccines cause autism
Corroborate: There’s certainly been a lot of coverage on television about vaccines
and autism so I can understand why you have questions
About Me: I always want to make sure I’m up to date on the latest information so
that I can do what’s best for my patients, so I’ve researched this thoroughly. In fact, I
just returned from a professional conference…
Science: The scientific evidence does not support a causal link. The CDC, the AAP,
the NIH, the IOM (etc) all reviewed the data and all reached the same conclusion.
Dozens of studies have been done. None show a link. In fact, the latest autism science
indicates…
Explain/Advise: Vaccines are critical to maintaining health and wellbeing. They
prevent diseases that cause real harm. Choosing not to vaccinate does not protect
children for autism, but does leave them open to diseases. Kids need these vaccines.

Corroborate: I can understand why you might feel that way. Hey, I had chicken pox
myself
About Me: The vaccine program has been so successful that the vaccine-preventable
diseases have become pretty rare in this country. However, from what I learned during my
training, I know that these diseases can have very serious consequences, even in otherwise
healthy children. The first time I saw a kid with meningitis, I knew we need to do
everything possible to prevent the spread of contagious diseases. We all need to get
immunized so that we don’t spread things to other people who might get serious
complications. I make sure I’m immunized to protect my family and my patients from
diseases I might be exposed to. You never know when you might be exposed or which of
your contacts might be particularly vulnerable.
Science: These diseases have come back in areas where vaccination rates are low. 5
children have died of HIB. Five cases of mumps have been diagnosed in NYC. 9 California
babies died this year of pertussis.
Explain: We care about our patients and we want to give you the best possible
protection against preventable disease. We all need to be vaccinated.
© 2009 Autism
Science Foundation,
Inc. All Rights
Reserved.
Measles isn’t so bad.
I had chicken pox and I was fine.

Corroborate: Kids today certainly get more shots than kids did years ago
About Me: Our practice follows the CDC schedule because it is carefully designed
to protect children at the time they are most vulnerable to disease. I recently returned
from a meeting, or I served on a committee that reviewed the schedule…
Science: Although kids get more shots today, they actually receive fewer antigens
than when they got fewer shots, because technology has enabled us to make vaccines
that have only the part of the cell that induces immune response. Plus, the
immunological challenge from a vaccine is nothing compared to what kids fight off
every day. An ear infection is a bigger immunological challenge. “Drop in the ocean”
Explain: We want all the kids in our practice to be immunized so that they have the
greatest chance for a long, healthy life. My own children are fully vaccinated.
© 2009 Autism Science
Foundation, Inc. All Rights
Reserved.
I want to spread out the shots so they won’t overwhelm
my child’s immune system

Making the
CASE for
Vaccines
© 2009 Autism Science
Foundation, Inc. All Rights
Reserved.
Corroborate: Acknowledge the parents’ concern
and find some point on which you can agree. This sets the right tone.
About Me: Describe what you have done to build
your knowledge base and expertise.
Science: Describe what the science says
Explain/Advise: Give advice to patient, based on
the science
Don’t expect me to
believe that vaccines
don’t cause autism if
you can’t tell me
what does cause
autism.

New Evidence and Current Scientific
Thinking about Causes of Autism Clinical heterogeneity
Genetics
More common in boys
Twin studies (more concordance in MZ twins than DZ twins)
Family studies
Multiple single genes, copy-number variants
Epigenetics
Possible gene-environment interaction
In utero exposures (valproate, thalidomide, terbutaline)
Organophosphates, PCBs, polycyclic aromatic hydrocarbons
“Multiple hits” might affect developing neuronal connectivity
“synaptopathy”
“failure to prune”

Main ideas about autism
Multiple causes
Causative events occur before MMR is given
“Refusing MMR vaccine will not protect your child from
autism, but will leave your child vulnerable to serious,
preventable diseases.”

New VISs
HIB and Td now have
updated VIS
statements
New content:
Problems that
could happen
after any vaccine
Because this is a
change to the adverse
effects section, you
should use the new
version now.

Legally Required Documentation

News: NYC requires flu shots for
kids in daycare and preschool
Four kids died of flu
last year
Tots are vectors,
transmitting virus
through population

California VPDs
Pertussis: In 2013, there were 2372 reported cases of pertussis in CA (twice as many as in
2012)
First infant death since 2010 recently reported in Latino infant
80% of infant pertussis deaths in CA since 1990 have been in Latino infants while 50% of
births in CA are to Latina mothers.
Overall incidence of pertussis in children <2 is greater in Latinos than in other ethnic
groups
Measles
15 cases in CA residents in 6 counties (5 mo-44 yrs old) so far in 2014 as of 2/21
Travelers (3 to Philippines, 2 to India) and people exposed to them
Most not vaccinated, 7 intentionally with PBE
Berkeley student riding BART
More cases expected: Contagious for 8 days, 4 days before and 4 days after the rash;
incubation period 7-18 days

Cultural Concerns What ethnic or religious groups do you
serve?
Have members of these groups expressed
particular concerns about immunizations?
How do you corroborate and address
these concerns?

Improving Cultural Competency (National Initiative for Children’s Healthcare Quality)
Provide and adequately fund interpreter services.
Implement a system to link bi- or multi-lingual staff with LEP patients.
Visibly and accessibly provide information about patients’ right to receive language
assistance in multi-lingual signage throughout the system.
Visibly and accessibly list local options for interpretation (e.g., telephone
interpreters, in person interpreters, etc.).
Identify cultural/linguistic barriers to care in order to help patients navigate the
healthcare system.
Identify pertinent demographic information that will assure referral settings are
knowledgeable of specific patient needs (e.g., preferred language, need for
interpreter).
Use a “navigator” program for new immigrants.
Incorporate language/interpreter needs at time of scheduling and when designing
visits.

Findings from a focus group study
(Shui et al, 2005)
Participants were “very concerned” about vaccine safety and their
children were fully vaccinated
Major factors influencing concerns
Lack of information
Mistrust of medical community and government
Major factors convincing them to have child immunized:
Social norms
Laws requiring immunization
Fear of consequences of not immunizing
Mistrust
You really don’t know what’s happening and here these people (Tuskegee study)
were guinea pigs and I just don’t want my children to be part of that
They give you all these papers…but they never tell you what exactly is inside the
shot
Are they getting the same shots as the Caucasian children are getting? They might try
out the black shot on you.
How do I know they’re not just telling me this so I can get these shots so they can get
their money?
EMR-IIS Interface
“We have been waiting years for the state’s vaccine registry to
communicate bi-directionally with our EMR. I think with state
budget cuts this is not in the near future but it would save us so
much nursing staff time. Are there any practices that have
successfully accomplished this information exchange?”

Sustaining Improvement: Which response
reinforces performance of immunization
assessments?
Let them know it’s helpful
Share the data so they can see their progress
GRRRRRR.
Another
item on the
problem list
Good catch. Let’s
see if we can get
him caught up
today. Thanks!

Lynn Cramer, RN
Chief Administrative Officer, Eden Park Pediatrics,
Lancaster, PA
Certified Pediatric Nurse with 25 years of pediatric nursing
experience and 15 years of management experience
Served as member of the AAP’s Practice Management On-
line Editorial Advisory Board
Management consultant for AAP’s Pediatric Practice
Management Leadership Team

National Vaccine Advisory Committee
Standard # 10 states: Persons who administer vaccines and staff who manage or
support vaccine administration are knowledgeable and
receive ongoing education.
Health care professionals or others who administer vaccinations should be
knowledgeable and receive continuing education in vaccine storage and handling,
the recommended vaccine schedule, contraindications, and administration
techniques; treatment and reporting of adverse events; vaccine benefit and risk
communication; and vaccination record maintenance and accessibility. With
appropriate training and in accordance with state law/regulation/policy, people
other than physicians and nurses may administer vaccines.
In addition, other staff should receive training and
continuing education related to their specific roles and
responsibilities that affect vaccination services

Scheduling Strategies to Keep Children’s
Immunizations Up to Date
Schedulers, nurses and checkin staff will think of every office visit
as an opportunity to immunize
Inform the Families
Patients/Families will have the information on standard vaccine schedule
presented to them at every opportunity.
Handout a laminated schedule for review at every visit
Website Immunization Schedules to Display on your website Insert this link:
http://www.cdc.gov/vaccines/schedules/syndicate.html
Increase availability and Opportunity
Prompts to staff to give vaccines at every patient interaction ( EHR Flags
Postings Templates)
Huddle Sheets for pre-visit planning

Strategies and Processes that are Effective
for Reminder Recall
Use of an IIS, or immunization registry, is a powerful tool
Use it to flag records of patients ahead of time behind in their
immunizations
More easily track a patient’s immunizations
Verify whether vaccinations were given by an alternative
provider
Recall patients who are behind in their immunizations
When there is a no-show nurses recall three!
Use of templates, plan of care, EHR programs, Practice
Management Systems to generate recall lists

QI Cycle: Identify, Plan, Implement, and
Reassess Workflow Changes that will Increase
Immunization Rates
Huddle sheet
Standing orders:
Standing orders include office policies, procedures, and orders
to provide recommended immunizations to patients.
For example, a standing order might be in place to instruct health care
personnel (as allowed by the state) to give a specific vaccine to all patients
for whom the vaccine is recommended based on the immunization
schedule. Standing orders should include procedures for vaccinating
eligible children and contraindications.
To access sample standing orders for vaccines, visit:
http://www.immunize.org/standing-orders


What’s wrong with this picture?

A better prompt
After upgrading eClinical Works
MA writes a sticky note for each visit about when last WCC was
and whether/which shots are needed
Provider responds by checking box in template about whether
shots are up-to-date
Test: Count the charts with the box checked

Stockwell M S et al. CLIN PEDIATR 2014;53:420-427

Stockwell M S et al. CLIN PEDIATR 2014;53:420-427 Copyright © by SAGE Publications
Table 3. Factors Associated With Missing an Immunization Visit on Multivariable Regression.

The Prius Effect
Given real-time
feedback about fuel
consumption,
drivers learn to drive
for greater fuel-
efficiency.
Happy Earth Day


Does feedback improve your
performance?
That which we measure,
we tend to improve
True
False
It depends

What happens in your
organization?
Who decides what to measure?
Is it clinically relevant?
How is the data collected?
How are findings presented?
Who has access to the findings?
Does performance affect income?

From the literature
Strong scientific evidence exists that assessment and feedback of
vaccination coverage information to providers are effective in
improving vaccination coverage.
The specific characteristics of assessment and feedback
interventions (e.g., content, intensity, use of incentives, or
benchmarking) that contribute most to effectiveness cannot be
determined from available data;
A variety of assessment and feedback interventions have been
consistently effective in a wide range of contexts.
Task Force on Community Preventive Services, 2000. Reviews of Evidence Regarding Interventions to Improve
Vaccination Coverage in Children, Adolescents, and Adults. Am J Prev Med 2000;18(1S)
Putting feedback in context
Basis for comparison
Others in practice
Mean performance of larger group
Goal based on wider objective (achieving herd immunity)
“Achievable benchmarks”
Benchmark is the level of performance of the top 10% of physicians for a
specific indicator

Identify area where improvement is needed
Document performance and describe current practice environment
Identify other practices providing similar services
Identify top performers for indicator of interest
Study the leaders: What makes them different?
Identify actions that lower performers can take to become more like
higher performers
Benchmarking

How might benchmarks and means affect
motivation of teams at different performance
levels?
0
10
20
30
40
50
60
70
80
90
100
Bas
e
Aug Sep
Oct
Nov
Dec Jan
Feb
Mar
ch
Pe
rce
nt
Team A
Team B
Group mean
Benchmark

AHRQ 2012: Feedback should
Address the goals and needs of target audience
Use performance measures that are perceived as relevant and
actionable
Use sound methods and make them transparent
Provide timely data (monthly, or at least quarterly)
Include benchmarks for comparison to peers and normative standards
Provide access to patient-level data
Enable physicians to correct patient-level data
Have built-in capacity to view performance trends (run charts)
Be part of quality improvement program that allows clinicians to
discuss challenges and solutions with peers

What next?
A nurse manager is assigned responsibility for coordinating
quality improvement efforts aimed at improving immunization
rates
She does a chart review, which indicates deficiencies in
documenting immunization assessments, giving vaccines during
sick visits and documenting reasons that vaccines aren’t given
She prepares a written report describing how the charts were
selected and the percent of all charts with various deficiencies.
She sends the report to all providers along with a list of relevant
best practices from the National Vaccine Advisory Committee
Two months later, she repeats the audit, finding no significant
change

What are the key barriers inhibiting the use of feedback by
individual physicians?
How might these barriers be overcome?
What kind of feedback is useful?

When giving feedback
Act as a facilitator of improvement, not an auditor
Provide guidance as to how performance can be improved
Use both quantitative and qualitative findings
In-person feedback is more effective than other kinds
Ask for feedback while giving feedback
How do you think you're doing?
What do you need help with?
What are you getting from me that you find valuable?
What am I doing that gets in the way?
What do you need from me?

Example: Feedback in action
“The new dashboards are helpful, but based on feedback
from the physicians we are still missing some patients in
acute care. The number is lower, but could still be
improved. The physicians say they get busy thinking about
the acute problem and sometimes don't get back to the
vaccines.”

The Feedback Sandwich
1. Start on something positive
2. Get into the meat
3. End on something positive
Be careful that the meat doesn’t get
lost in the bun

Criticism is better received when it’s invited; unsolicited negative feedback provokes
annoyance and might be discounted.
Criticism is more effective when it is perceived as coming from someone with
authority and qualifications to give it.
Criticism can be perceived as a threat to one’s livelihood or even self-worth
Negative Emotions interfere with effectiveness
Who asked
you?
Who are you to
tell me what to do?
They think I’m
scum. I guess
they’re right.
Does that mean
I’m going to be
fired?
Try saying
I appreciate that feedback.
Tell me more.
Help me understand that.
What can I do to change that?
Thank you.

Make it Actionable Encourage provider/staff to
develop their own solutions
Encourage setting incremental
realistic goals
Focus on 2-3 areas of improvement
Encourage development of a plan
Who will do what by when?
Actionable examples

So what should I DO about it?
Set SMART goals
S – Specific
M – Measurable
A – Attainable
R – Relevant
T – Time-bound
Plan Do
Study Act

What would you do?
Suppose an administrator in your large organization decided
that it would be more efficient if all appointments were made
off- site by personnel totally outside your control.
Shortly after this change goes into effect, you see two
children who can’t get their shots at their scheduled well-
visit because they are a week short of their birthdays.
Headlines we appreciate
U.S. Cites End to C.I.A. Ruses Using Vaccines
The New York Times, May 20
CIA: Vaccination programs won’t be used as cover
The Washington Post, May 20

Number of rotavirus-positive laboratory reports in
England, 2009/2010 - 2013/2014
England added rotavirus to vaccine schedule in 2013. The vaccine is estimated to prevent three rotavirus
deaths, 13,000 rotavirus admissions, 27,000 rotavirus emergency visits and 74,000 rotavirus GP
consultations in children aged <5 years, and lead to annual savings of over £11 million, each year.
Authors estimate 375 fewer RVGE admissions for every additional intussusception admission, and 88
fewer RVGE deaths for every additional intussusception death. The estimated benefits of Rotarix®
vaccination would greatly exceed the potential risk in England.
Clark A, Jit M, Andrews N,
Atchinson C, Edmunds J,
Sanderson C (2014).
Evaluating the potential risks
and benefits of infant rotvirus
vaccination in England. Vaccine.
Doi.org/10.1016/jvaccine.201
4.04.082

This study looked at immunized children
who had seizures during the first 2 years
of life and compared those who got
immunization on time with those who
had delayed immunizations. Each child
was his/her own control.
No association between timing of
vaccination and occurrence of post-
vaccination seizures in first year.
Risk of seizure 7-10 days after vaccination
was greater when MMR and varicella
were delayed past 15 months.
Hambridge SJ, Newcomer SR, Narwaney KJ, Glanz JM et al
Pediatrics 2014; 133:e1492-e1499
Data from Vaccine Safety Datalink

New Vaccines on the Horizon
Meningococcus Type B vaccine
Already in use in Europe, Australia and Canada
Has been safe and effective in Princeton and UC Santa Barbara in
response to recent outbreaks
Might be approved for use in US on expedited schedule
HPV 9
HPV in use now protects against 4 strains
Adding 5 more strains would protect against an additional 4000
HPV-associated cancers each year
Might be approved soon

A penny for your thoughts
Personal Belief Exemption Documentation: What do you do?
How do state requirements affect your practice?
How do you provide information about risks and benefits and ensure parental
understanding of the information you provide?
Do you have a “standard curriculum” for parents?
How do you document this in the medical record?
Should Personal Belief Exemptions be permanent? How often do you revisit this
question with parents?
In the event of an outbreak at a local school, could you generate a list of
vulnerable children who should be isolated?

What do you think?
In a community where there are a relatively high number of parents
who don’t want to vaccinate their children, would it be a good idea
to have group meetings for discussion?
How would you “control the message”?

If we don’t administer vaccines that are due, we
document the reason why in the chart
0
5
10
15
20
Base Aug Sep Oct Nov Dec Jan Feb Mar Apr May
Nu
mb
er
of
pra
cti
ces
No
Partly
Yes
0
0.5
1
1.5
2
Base Aug Sep Oct Nov Dec Jan Feb Mar Apr May
QIT
S M
ean
ite
m s
co
re
no=0
partly=1
yes=2
