module 15 cardiovascular system blood, lymphatic...
TRANSCRIPT

587
Objective 1. Characterize the properties of the blood that make it a connective tissue, and
describe the general functions of the blood.
Blood is one component of the
cardiovascular system, the others being the
heart and blood vessels. As the body’s
transport medium, the blood provides a
means to transport oxygen, carbon dioxide,
hormones, and nutrients. The blood also
contains most of the cells, proteins, and
chemicals required to initiate and support
resistance to diseases. Body temperature
and pH are also regulated by the blood.
Because the blood has access to the entire
body, disorders and diseases associated with
the blood are not localized disorders.
All connective tissues share similar properties; they have cells and an extracellular matrix.
Blood fits these parameters. The blood contains various types of cells and cell fragments,
suspended in an extracellular matrix called the plasma.
The blood has three basic functions: transportation, regulation, and protection. Each of the
individual components of the blood has a specific function. Together, they provide a very
efficient means of delivering nutrients and removing wastes to and from all areas of body.
Every cell in the body requires a continuous supply of oxygen and nutrients. Restricting
the blood supply to a tissue, even for a short period of time, will result in some amount of
cellular death. This is exactly what happens in the majority of heart attacks and strokes; the
blood supplies to the heart and brain become blocked and the cells are injured or die.
Assignment: Tortora, p. 690 or Wiley Plus – 19.1 Functions and Properties of Blood
Module 15
Cardiovascular System
Blood, Lymphatic System & Immunity

588
Objective 2. Describe the physical characteristics of the blood.
The blood has a number of physical characteristics that give it its functional properties.
Assignment: Tortora, p. 690 or Wiley Plus – 19.1 Functions and Properties of Blood
Property Characteristic
Viscosity Thicker than water due to solutes, colloids, and suspended formed
elements
Temperature 38o C (100.4o F)
pH Slightly alkaline, 7.35-7.45
Color Variable shades of red depending on the amount of oxygen present
Volume 4-6 liters depending on gender and body mass

589
Objective 3. Identify and describe the components of whole blood.
Blood has two main components, the formed
elements (mostly cells) and plasma. The
term formed elements sounds like a weird
term for the cellular components of the
blood, but it is accurate. The formed
elements consist of the red blood cells
(RBCs), the white blood cells (WBCs) and
the platelets (thrombocytes). The reason
they are called formed elements is because
of the platelets; they aren’t cells; they are
fragments of cells.
When a tube of whole blood is spun in a
centrifuge, the denser cells will sink to the
bottom of the tube, and it leaves the less
dense plasma on top. The formed elements
account for about 45% of the total volume,
plasma 55%. It is very rare for a patient to
receive a whole-blood transfusion. They
always get one or more of the components,
whether it is RBCs, plasma, or platelets,
depending on their need.
When a person donates
blood, the laboratory will
spin the bag in a specially
designed centrifuge to
separate the blood
components.
Blood plasma is a clear,
yellow liquid. It is 92%
water and 8% solutes. The
majority of the solutes (7%
of the 8%) are plasma
proteins.
Assignment: Tortora, pp. 691-693 or Wiley Plus – 19.1 Functions and Properties of Blood

590
Objective 3 (continued). Identify and describe the components of whole blood.
There are many types of plasma proteins, and they have individual functions, frequently as
carrier molecules, but collectively, they contribute to the osmotic balance of the blood. The
hepatocytes of the liver produce the majority of the plasma proteins. They include the
albumins (54%), the globulins (38%) and fibrinogen (7%), a clotting protein. The remaining
1% of plasma is made up of miscellaneous solutes: electrolytes, nutrients, gases, hormones,
and waste products.
One of the important types of globulins are the gamma globulins. These are also known as
immunoglobulins or antibodies. These plasma proteins are produced in response to organic
molecules that the body recognizes as foreign. They serve as flags for the immune system,
so it knows what needs to be destroyed.
As previously mentioned, the formed elements consist of the red blood cells, white blood
cells, and platelets. Each of these along with the immune system will be addressed in detail
later in this module.
591
Objective 4. Define and describe hematopoiesis (hemopoiesis).
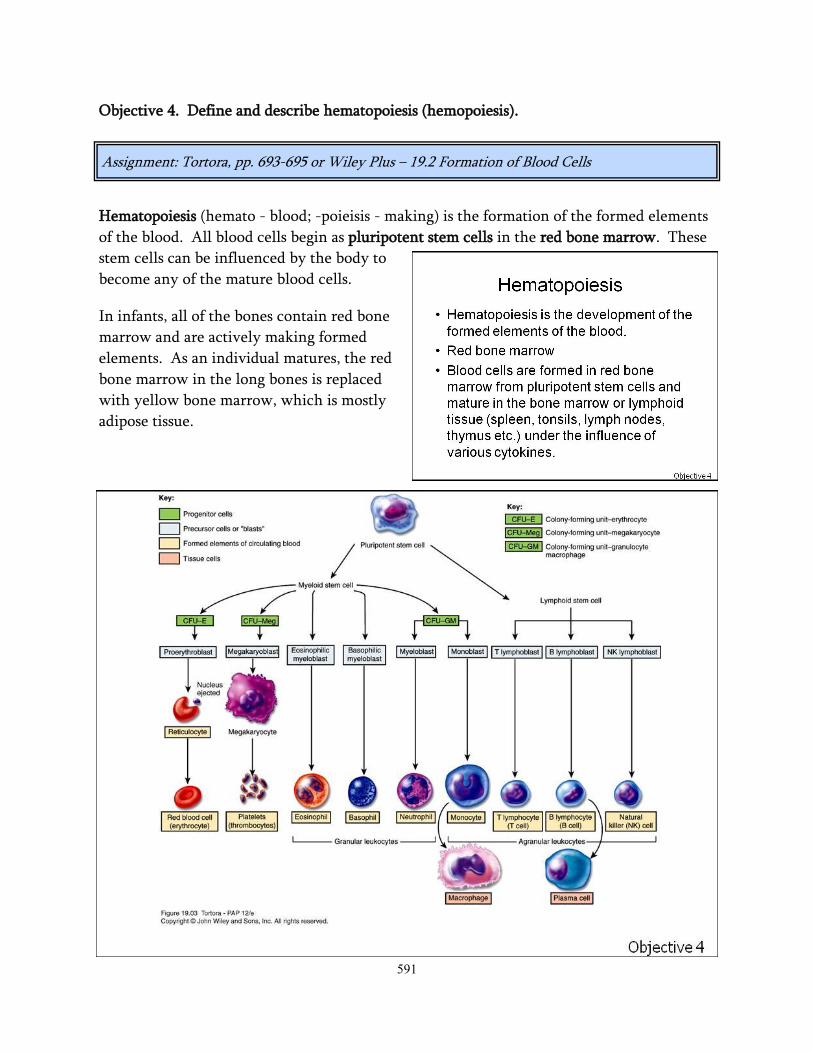
Hematopoiesis (hemato - blood; -poieisis - making) is the formation of the formed elements
of the blood. All blood cells begin as pluripotent stem cells in the red bone marrow. These
stem cells can be influenced by the body to
become any of the mature blood cells.
In infants, all of the bones contain red bone
marrow and are actively making formed
elements. As an individual matures, the red
bone marrow in the long bones is replaced
with yellow bone marrow, which is mostly
adipose tissue.
Assignment: Tortora, pp. 693-695 or Wiley Plus – 19.2 Formation of Blood Cells

592
Objective 4 (continued). Define and describe hematopoiesis (hemopoiesis).
Proliferation and maturation of blood cells depends on specific cytokines, chemical signals
from one group of cells to stimulate another. Under the influence of these cytokines
(growth factors, colony-stimulating factors, and interleukins) cells differentiate into the
various cell types. The stem cells differentiate into either the myeloid group of the
lymphoid group. The names indicate where the cells are formed and mature. The
immature myeloid (bone marrow) cells differentiate and become red blood cells, platelets,
and many types of white blood cells. The lymphoid cells mature in the lymphatic system
and give rise to a specific group of white blood cells called lymphocytes.
Cytokines Effect
Erythropoietin (EPO) Increases number of early red blood cells in the
bone marrow
Thrombopoietin (TPO) Increases the formation of platelets
Colony-stimulating factors (CSFs)
and interleukins
Increases the production and differentiation of
white blood cells.

593
Objective 5. Describe the structure and function of the red blood cells (RBCs).
Red blood cells have characteristics that make them perfect transporters of oxygen: they are
biconcave discs, they demonstrate reversible-deformity, they don’t consume the oxygen
they carry, and they lack a nucleus. Each of these properties is important to the appropriate
function of the RBC.
Their biconcave shape gives them a high surface-to-volume ratio, thus allowing them to
carry a great deal of oxygen in relation to their size. Think of this shape as a donut, but the
hole in the middle doesn’t go all the way through.
Red cells lack mitochondria, so they don’t
produce ATP by oxidative metabolism; they
utilize glycolysis to stay alive. So, they use
glucose for energy, but they transport all of
the oxygen they pick up. This is like a
person carrying around a candy bar and not
eating it. Most people couldn’t do it.
RBCs are required to squeeze through really small spaces, specifically blood capillaries. As
they pass through these small spaces, they become almost torpedo-like, but when they
come out the other side, they revert back to their biconcave shape.
Because a RBC lacks a nucleus, it allows all of the cytoplasmic space to carry oxygen.
Before the nucleus is lost, it provides the instructions to produce hemoglobin, the oxygen-
carrying molecule of the red cell.
Red cells live for approximately 120 days. This isn’t too bad due to the fact that they are
constantly damaged from squeezing through small spaces, and they don’t have a nucleus or
any organelles to repair any damage that takes place. If red cells are damaged, they are
removed from the circulation by phagocytic white blood cells, the spleen, and the liver.
Assignment: Tortora, pp. 695-696 or Wiley Plus – 19.3 Red Blood Cells

594
Objective 6. Identify the components of the hemoglobin molecule and describe its
function.
As previously mentioned, hemoglobin is the
oxygen-carrying molecule of the red blood
cell. There are approximately 280 million
hemoglobin molecules in each red cell. One
hemoglobin molecule consists of two main
components, heme and globin. Globin is a
protein that is made up of four-polypeptide
chains, two alpha chains and two beta
chains. Each polypeptide chain has a heme
molecule bound to it. Heme is a ringed
molecule with one iron (Fe2+) atom at the
center. The iron atom is the binding site for
oxygen; each Fe2+ can pick up one oxygen molecule (O2) at the lungs. So, if there are 280
million hemoglobin molecules in a red cell and each hemoglobin molecule has four hemes,
and each heme can pick up one oxygen molecule, one red cell can carry 1.1 billion oxygen
atoms. The total amount of hemoglobin in the blood ranges from 14-16 g/dl.
At the lungs, hemoglobin
has a high affinity for
oxygen; it wants to pick it up
and hold on to it. At the
tissue level, hemoglobin has
a lower affinity for oxygen.
Hemoglobin wants to let go
of oxygen, thereby allowing
it to diffuse into the cells. It
doesn’t do any good to pick
up oxygen and just hold on
to in the blood. Hemoglobin
also picks up a little bit of
CO2 from the tissues to
transport back to the lungs
and be exhaled.
Assignment: Tortora, pp. 696-697 or Wiley Plus – 19.3 Red Blood Cells

595
Objective 7. Describe the process of erythropoiesis.
Erythropoiesis is part of
hematopoiesis, specifically
relating to the production
and maturation of red blood
cells.
Red cells are produced
continuously (approximately
2 million per second) to keep
up with red cell destruction.
The average person has 4.00-
6.00 x 106 RBCs/mm3 of
blood. If the number of red
cells lost exceeds the
number made, hypoxemia
(too little oxygen in the
blood) will result. In this case,
the lack of oxygen is not due
to problems with breathing;
there just aren’t enough red
cells to transport the
available oxygen around the
body. The decreased
amount of oxygen is
detected in the kidneys and
the kidneys secrete
erythropoietin (EPO), a
hormone to increase the rate
of erythropoiesis. EPO
increases the development of
red cells in the bone
marrow.
Assignment: Tortora, p. 698 or Wiley Plus – 19.3 Red Blood Cells

596
Objective 7 (continued). Describe the process of erythropoiesis.
Early red cells are large, they have a nucleus, very little cytoplasm, and they lack
hemoglobin. As a red cell matures, it becomes smaller, increases its hemoglobin content,
and loses its nucleus. The loss of the nucleus results in the red cell gaining its biconcave
shape, but it isn’t mature yet; it still contains some mitochondria, ribosomes, and
endoplasmic reticulum. This almost-mature red cell is called a reticulocyte. These
reticulocytes are released into the blood stream and will mature over the next 1-2 days.
Normally, 0.5-1.5% of circulating red blood cells are reticulocytes. If this percentage
increases, a person has a high rate of erythropoiesis. If it goes down, they have a low rate.
Physicians will try to determine why the person is making more or less than normal.
The relative amount of red cells in the blood can be measured by determining a patient’s
hematocrit (Hct). The Hct is the % of a patient’s whole blood that is occupied by red blood
cells. This averages about 45%, a little higher in men and a little lower in women.

597
Objective 8. Define terms associated with increased or decreased numbers of red cells, and
describe examples of these changes.
Polycythemia is the presence of too many red blood cells. Polycythemia can manifest as a
primary or secondary disease. Primary polycythemia is also known as polycythemia vera
(PV). It is an abnormality of the bone marrow causing an overproduction of red blood cells,
and it may also result in an increase of white cells and platelets. The biggest problem with
PV is that it increases the viscosity of the blood which can make the heart work harder and
increase the likelihood of clotting.
Secondary polycythemia is an increase in red cell numbers due to another condition. Any
stimulus that causes hypoxemia can cause the bone marrow to increase the production of
red cells. Examples include smoking, sleep apnea, prolonged exposure to low atmospheric
oxygen, or heart disease.
Assignment: Tortora, pp. 693, 711 or Wiley Plus – 19.2 Formation of Blood Cells & 19.8 Blood Groups and Blood Types (Disorders: Homeostatic Imbalances)

598
Objective 8 (continued). Define terms associated with increased or decreased numbers of
red cells, and describe examples of these changes.
Anemia is a decrease in the
normal number of red blood
cells. The various forms of
anemia are classified based
on the size of the red cells
(microcytic, normocytic, and
macrocytic), the amount of
hemoglobin in the red blood
cell (hypochromic and
normochromic) and the
cause of the low red cell
numbers.
Anemia Examples
Type Size Amt. of
Hemoglobin Cause
Hemorrhagic anemia Normocytic Normochromic Bleeding
Iron deficiency anemia Microcytic Hypochromic Lack of iron
Pernicious anemia Macrocytic Normochromic Vitamin B12 deficiency
Hemolytic anemia Normocytic Normochromic Destruction of RBCs
Aplastic anemia Normocytic Normochromic Bone marrow failure

599
Objective 9. Define leukocyte, and identify the various types of white blood cells normally
present in the blood.
Leukocyte is another term for a white blood cell. White blood cells (WBCs) are very
different from red cells: they have nuclei, they are larger, they don’t have hemoglobin, and
there are different types with unique functions. There are fewer white cells circulating in
the blood stream than red cells. A normal white blood cell count is 5.0-10.0 x 103 WBCs/
mm3.
WBCs can be separated into
two groups based on the
presence of cytoplasmic
granules. They are the
granulocytes (granular
leukocytes) and the
agranulocytes (agranular
leukocytes). These granules
are visible under a
microscope when the cells
are stained.
The granulocytic group
includes three specific
WBCs: neutrophils,
eosinophils, and basophils.
The names of these cells
come from their staining
characteristics. The granules
of an eosinophil stain red
with an eosin stain. The
granules of a basophil stain
dark purple, and the
granules of a neutrophils
stain somewhere in the
middle.
The agranulocytes do
contain some cytoplasmic
granules but they are much
less prominent and they don’t stain as well and their granulocytic counterparts.
Lymphocytes and monocytes are included in this group.
Assignment: Tortora, pp. 699-701 or Wiley Plus – 19.4 White Blood Cells

600
Objective 10. Define and describe conditions related to leukocytosis and leukopenia.
Leukocytosis is an increase in the number of white blood cells. Leukocytosis is a normal
physiologic response, up to a certain point. An individual wants their white cell numbers to
increase as a response to diseases or conditions. Any disruption of homeostasis can cause an
increase in white cell numbers. Common causes would be bacterial infections, viruses,
parasites, stress, temperature extremes, etc.
An increase in white blood cell numbers above 40,000 WBCs/mm3 is never a normal
response. An individual can have a severe bacterial pneumonia and their white count will
not increase to that degree. Levels above 40,000 would indicate an abnormal proliferation
of white cells. Frequently this is one of the various types of leukemia. Leukemia is a cancer
of the blood-forming cells, most often the white cells. Can an individual have leukemia of
early, precursor, red cells or platelets? Yes, but these are rare. In some leukemia cases,
white cell numbers can increase above 300,000 WBCs/mm3.
Leukopenia is a decrease in white cell numbers, and it is never a normal response. There
isn’t a normal physiological reason for a person’s white count to go down. Causes can
include: AIDS, chemotherapy, or bone marrow failure (aplastic anemia).
Assignment: Tortora, pp. 700-701 or Wiley Plus – 19.4 White Blood Cells
601
Objective 11. Describe the basic functions of the individual white blood cells.
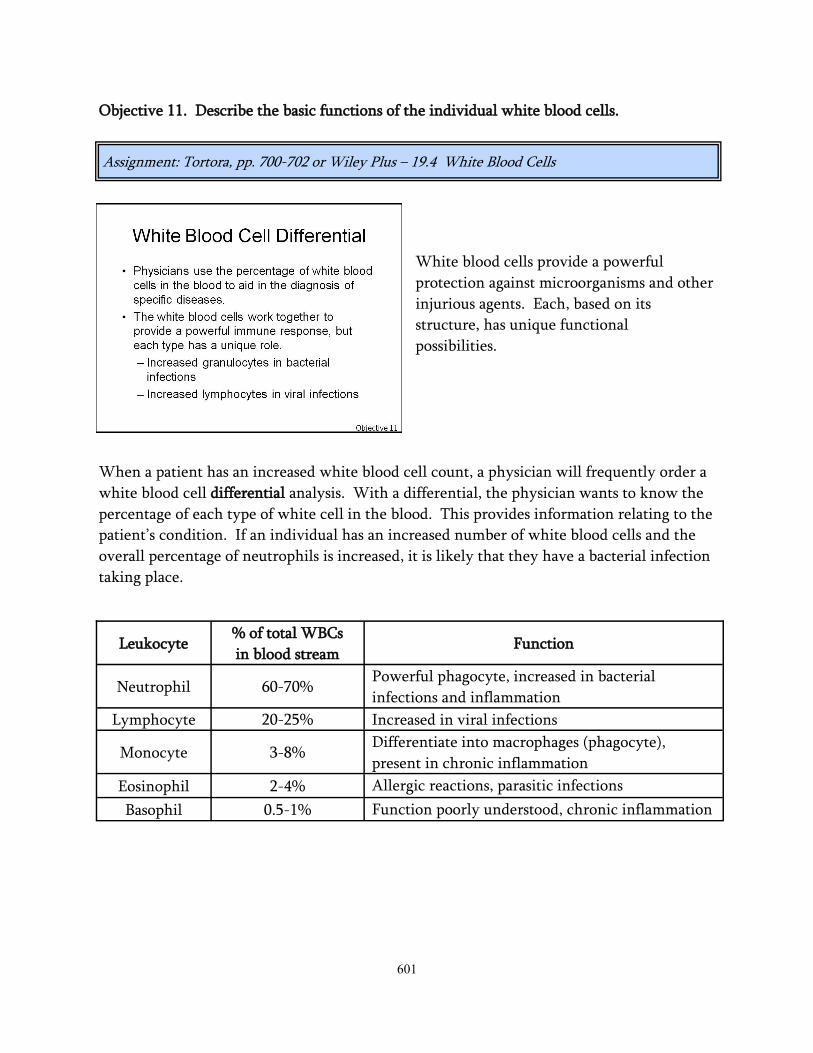
White blood cells provide a powerful
protection against microorganisms and other
injurious agents. Each, based on its
structure, has unique functional
possibilities.
When a patient has an increased white blood cell count, a physician will frequently order a
white blood cell differential analysis. With a differential, the physician wants to know the
percentage of each type of white cell in the blood. This provides information relating to the
patient’s condition. If an individual has an increased number of white blood cells and the
overall percentage of neutrophils is increased, it is likely that they have a bacterial infection
taking place.
Assignment: Tortora, pp. 700-702 or Wiley Plus – 19.4 White Blood Cells
Leukocyte % of total WBCs
in blood stream Function
Neutrophil 60-70% Powerful phagocyte, increased in bacterial
infections and inflammation
Lymphocyte 20-25% Increased in viral infections
Monocyte 3-8% Differentiate into macrophages (phagocyte),
present in chronic inflammation
Eosinophil 2-4% Allergic reactions, parasitic infections
Basophil 0.5-1% Function poorly understood, chronic inflammation

602
Objective 11 (continued). Describe the basic functions of the individual white blood cells.

603
Objective 12. Describe the production and function of platelets.
Platelets, also called thrombocytes, are cytoplasmic fragments of large cells in the bone
marrow called megakaryocytes. These cells are 10-15 times larger than a red cell, and due
to their size, they don’t escape the bone marrow and show up in the blood stream. An
individual megakaryocyte can release 2000-5000 platelets. The normal range for platelets in
the blood is 150-400 x 103/mm3.
Platelets have a very short
lifespan, approximately 5-9
days. Platelets help limit
blood loss by forming a
platelet plug and releasing
chemicals to encourage
vasoconstriction and activate
the clotting process.
Assignment: Tortora, pp. 701-702 or Wiley Plus – 19.5 Platelets

604
Objective 13. Define hemostasis and describe the three mechanisms that contribute to
hemostasis.
The term hemostasis, not to be confused
with homeostasis, has a Greek origin,
meaning blood stagnation. It is very
complex process which when activated
causing a cessation of bleeding. There are
three mechanisms involved: vascular spasm,
platelet plug formation, and coagulation.
Vascular spasm is the constriction of
damaged blood vessels. This limits the
amount of blood lost. The vascular
constriction is due to chemicals released from platelets, damage to the smooth muscle of the
vessels, and pain receptor reflexes.
Platelets are very active in the hemostatic process. Think of them as little bags of
procoagulant chemicals. Platelets form a plug through a three-step process. First, the
platelets adhere to the wall of the blood vessel. Second, the platelets release their chemical
contents. This encourages further vasoconstriction and recruitment of other platelets.
Lastly, due to chemical
release, the activated and
newly-recruited platelets
become sticky. The
clumping of platelets is
called platelet aggregation.
With the activation of
enough platelets, a loose
platelet plug is formed.
Assignment: Tortora, pp. 703-705 or Wiley Plus – 19.7 Hemostasis

605
Objective 13 (continued). Define hemostasis and describe the three mechanisms that
contribute to hemostasis.
Everyone witnesses this
event sometime in their life,
some more than others.
When someone cuts
themselves shaving, it is
common practice to place a
piece of toilet paper over the
cut. This keeps blood off
their clothing and it makes
an attempt at stopping the
bleeding. Because the
individual is usually in a
hurry, (that is why they cut
themselves in the first place)
they remove the toilet paper prior to going out into public. They are disappointed to find
out that they begin bleeding again. What happened to the platelets? They are on the toilet
paper, so there isn’t an intact platelet plug. Now, that is embarrassing.
The last mechanism in hemostasis is coagulation. An easy way to think of coagulation is
taking that which is liquid (plasma) and make it a solid (clot) or at least a semi-solid.

606
Coagulation is a complex series of enzymatic
reactions that occur in a stepwise or
cascading fashion. Think of the steps as
dominos standing next to each other, ready
to fall, and when injury occurs, it tips over
the first domino. Just like tipping over the
dominos, all of the dominos have to be in
place to get to the end. If one is removed, it
stops. The dominos in this game are called
clotting or coagulation factors. Once one is
activated, the new active form stimulates
the next factor, which activates the next,
and so on. Most of these factors are
synthesized by the liver and they are
enumerated with Roman numerals (factors
I, III, IV, X, VIII, etc.).
There are two separate pathways to activate
coagulation, and they merge to form a common pathway. A person may ask, why are there
so many? The presence of two pathways attempts to guarantee that bleeding stops. Each of
the pathways is activated in a slightly
different fashion, and the name gives a hint
to their activator.
The extrinsic pathway is activated by
damage outside of the vessel, specifically
tissue. A tissue protein called tissue factor
(TF) or tissue thromboplastin is released
from the damaged tissue into the blood
vessels. The extrinsic pathway has fewer
steps and occurs rapidly.
The intrinsic pathway is activated by
substances within or associated with the vessel. Exposed vascular collagen, damaged
endothelium, or activated platelets are all potent coagulation activators.
Objective 14. Describe the process of coagulation: stimuli, pathways, and products.
Assignment: Tortora, pp. 704-707 or Wiley Plus – 19.7 Hemostasis
607
Objective 14 (continued). Describe the process of coagulation: stimuli, pathways, and
products.
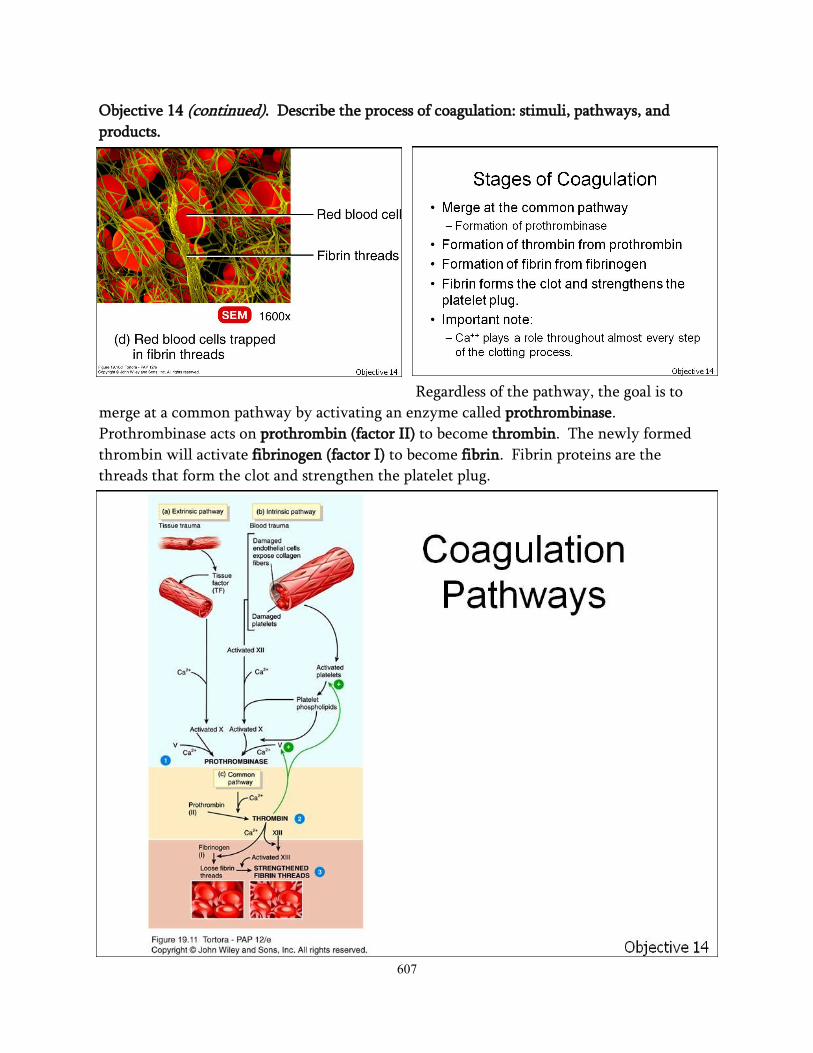
Regardless of the pathway, the goal is to
merge at a common pathway by activating an enzyme called prothrombinase.
Prothrombinase acts on prothrombin (factor II) to become thrombin. The newly formed
thrombin will activate fibrinogen (factor I) to become fibrin. Fibrin proteins are the
threads that form the clot and strengthen the platelet plug.

608
There are a number of cofactors that must be present for clotting factor synthesis and for
coagulation to occur. Vitamin K is a cofactor in the synthesis of clotting factors II, VII, IX,
and X. The mineral calcium is required as a cofactor for almost every step of the
coagulation process. So, a person with vitamin K deficiency or a reduced amount of blood
calcium would have difficulty clotting.
Understanding coagulation helps one
understand the difference between plasma
and serum. Plasma is the liquid portion of
unclotted blood. Serum is the liquid portion
of clotted blood. If a sample of blood hasn’t
been allowed to clot, it still has available,
yet-to-be-activated, clotting factors;
therefore it is plasma. If the sample has
clotted, the clotting factors have been
utilized, so it is serum. This is why a patient
is given plasma, not serum. They don’t
want to limit their ability to clot.
If the clot is stationary, it is
called a thrombus. If it is a
clot that is moving in the
blood stream, it is an
embolus. To complicate
things a little, if it was a
thrombus that detached and
is now moving, it is often
called a thromboembolus.
Objective 14 (continued). Describe the process of coagulation: stimuli, pathways, and
products.
609
Objective 15. Compare the fibrinolytic system with the process of coagulation.
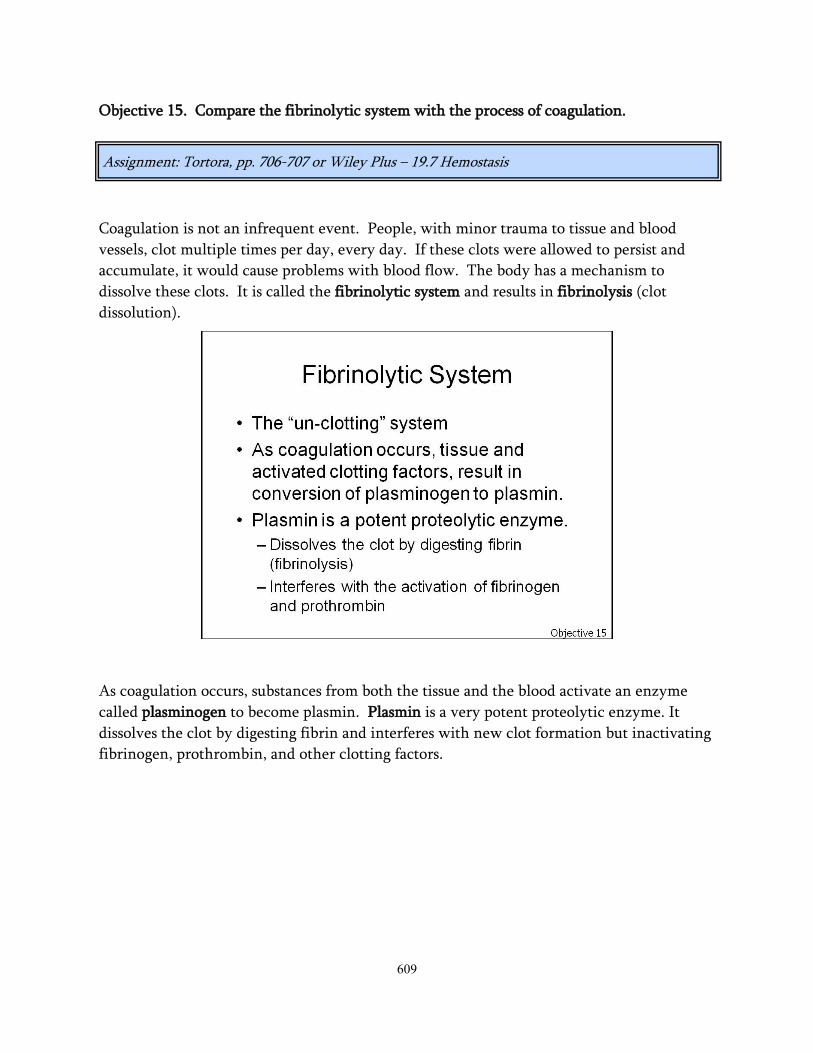
Coagulation is not an infrequent event. People, with minor trauma to tissue and blood
vessels, clot multiple times per day, every day. If these clots were allowed to persist and
accumulate, it would cause problems with blood flow. The body has a mechanism to
dissolve these clots. It is called the fibrinolytic system and results in fibrinolysis (clot
dissolution).
As coagulation occurs, substances from both the tissue and the blood activate an enzyme
called plasminogen to become plasmin. Plasmin is a very potent proteolytic enzyme. It
dissolves the clot by digesting fibrin and interferes with new clot formation but inactivating
fibrinogen, prothrombin, and other clotting factors.
Assignment: Tortora, pp. 706-707 or Wiley Plus – 19.7 Hemostasis
610
Objective 16. Relate the use of anticoagulants and thrombolytics to the coagulation process.
If someone has, or is prone to forming, clots they are often given anticoagulants. These are
commonly referred to as blood-thinners. They do not change the viscosity of the blood,
and they don’t decrease a person’s hematocrit, so they are not blood-thinners. They do
however inhibit coagulation, so the correct term is anticoagulant.
There are a number of anticoagulants. Some are used for therapeutic reasons and some for
specimen collection. The common goal is to inhibit the coagulation process.
Warfarin is not just used in people. It is used as a pesticide, specifically a rodenticide to
control mouse and rat populations. D-Con® is a common brand people use. It is not a
mouse poison, it is a mouse anticoagulant. The mouse consumes enough over time until
they have a lethal dose. Without the ability to clot, they will simply bleed to death.
It is important to inhibit clotting in high-risk individuals, but what if the person has already
formed clots? What can be done for them? Thrombolytics are medications used to dissolve
clots that are already present.
Assignment: Tortora, p. 707 or Wiley Plus – 19.7 Hemostasis
Anticoagulant Examples
Anticoagulant Use
Heparin Administered intravenously to a stroke or heart attack victim,
also used in surgery and dialysis
Coumadin® (warfarin) Oral medication used to inhibit clotting in high-risk patients
EDTA Present in blood-draw tubes used for blood counts
Sodium Citrate Present in blood collection bags for blood donations
Aspirin Inhibits platelet aggregation

611
Objective 17. Describe the development and identification of the ABO and Rh blood
groups.
Red blood cells, like all other cells contain
genetically-determined cellular markers.
These markers provide a cell’s signature.
Through this signature, cells can be
identified. A person inherits genes from
their parents that dictate which markers will
appear on their on their cells, in this case
specifically red cells. Two of the major
blood groups appear from this process, the
ABO and Rh systems. Many other blood
groups exist, but they will not be addressed
in this course.
When a person is blood typed, their cells are
evaluated for the presence or absence of
specific markers. These markers, because
they can react with products of the immune
system, are called antigens. The immune
system can make specific antibodies to these
antigens.
The ABO blood group is the most important
blood group system to consider. A person’s
ABO blood type simply identifies the
presence or absence of A and B antigens on
their red cells, due to the inheritance of
certain genes. Both a father and mother will
pass an ABO blood-type gene to their
offspring. The choices are A, B, or O. If a
person inherits the A gene from at least one
parent, they will have A antigens on their
cells. If they inherit the B gene from at least
one parent, they will have B antigens on
their cells. If they inherit both genes, one
from each parent, they will have both A and
B antigens on their cells.
Assignment: Tortora, pp. 708-709 or Wiley Plus – 19.8 Blood Groups and Blood Types

612
Objective 17 (continued). Describe the development and identification of the ABO and Rh
blood groups.
Lastly, if they don’t inherit
either the A or B gene, they
will be identified as having
the O blood type. The
reason for this expression is
because the A and B genes
are dominant genes. That
means a person will
demonstrate the antigens on
their cells if they inherit the
genes. So, the possible blood
types within the ABO group
are: A, B, AB, and O.
To make things a little more
confusing, a person will
have antibodies in their plasma to the A or B antigens they lack. So, if a person lacks the A
antigen on their cells, they will have A antibodies in their plasma. A lack of B antigens will
result in the presence of B antibodies in their plasma. A person with the O blood type lacks
both antigens, so they will have both A and B antibodies in their plasma. This is why a
person’s blood type must be considered when a patient needs a blood transfusion. If type-A
blood is given to a type-B person, the A antibodies will flag the red cells for destruction by
the immune system.
A person isn’t born with A
and B antibodies, but they
are formed shortly after
birth (within six months).
Research doesn’t know what
causes this, but the current
theory is that the immune
system reacts with
something in the
environment that appears, to
the immune system, like A
and/or B antigen.
613
Objective 17 (continued). Describe the development and identification of the ABO and Rh
blood groups.
The cause must be something along this line because, as a rule, the immune system will
only react to something it sees and recognizes as foreign. So, it has to see A antigen or at
least something that looks like it to form A antibodies.
The Rh blood type is a little easier to understand. It is determined simply by the presence
or absence of the Rh antigen on red cells. If a person inherits the Rh gene from either
parent, they will have the antigen, so they are Rh-positive. If they don’t inherit it, they will
be Rh-negative.
Another important aspect of this system is that individuals don’t make antibodies to the Rh
antigen unless the immune system sees it. So, unless an Rh-negative person sees Rh-
positive blood, they will not have any Rh antibody.
Inherited Gene(s) Antigens on RBCs Antibodies in the Plasma
A gene A antigens B antibodies
B gene B antigens A antibodies
A and B genes A and B antigens no A or B antibodies
Neither A or B genes Neither A or B A and B antibodies

614
Objective 18. Describe the considerations of the ABO and Rh blood groups with blood
transfusions.
When a person needs a blood transfusion, the
blood groups must be considered. In the
medical laboratory, there are many blood groups
they have to be considered, but this discussion
will be restricted to the ABO and Rh systems.
The most important thing to remember is that
the immune system will only react to that which
it sees. If there is nothing to see, the immune
system won’t care. This is like a child hiding
candy in their room. If mom and dad can’t see it,
there isn’t a problem. If they find it, there are
likely consequences.
If a person has a low red count and hematocrit, and they are struggling to oxygenate, a physician
will order a blood transfusion. To understand blood-compatibility, it is important to understand
99% of the blood transfusions are just red blood cells. It is very rare for a person to receive whole
blood.
In a blood transfusion, RBCs from a generous donor are
given to a needy recipient. With this in mind, two things
have to be considered. One, what antigens are on the
donor’s cells, and two, what antibodies are in the recipient’s
plasma. When receiving blood, the patient doesn’t want to
see any antigens they haven’t seen before or any antigen to
which they already have antibodies, or the newly transfused red cells will be flagged for destruction
by the immune system. This cellular destruction is called a transfusion reaction. To avoid this
problem, the medical laboratory will put donor red cells and recipient plasma in a tube to check for
compatibility before the patient is given the red cells. If it doesn’t work in a tube, it won’t work in
the patient.
The O blood type is commonly referred to as the
universal donor. This is because there isn’t any
A or B antigen on the red blood cells; therefore,
there isn’t anything for the immune system to
see. The AB blood type is called the universal
recipient because they don’t have any A or B
antibodies in their plasma. Their system already
knows what A and B antigens look like, so they
aren’t foreign to them. As an example, an A
patient can receive type-A or type-O blood. A
patient who is type B, can have B or O.
Assignment: Tortora, pp. 709-710 or Wiley Plus – 19.8 Blood Groups and Blood Types
Blood Type Compatible Blood
A A or O
B B or O
AB A, B, AB, or O
O Only O
615
Objective 19. Describe the interactions of the blood groups that cause hemolytic disease of
the newborn (HDN).
Hemolytic disease of the newborn is caused by a blood incompatibility between a fetus and
an expectant mother. Hemolytic of course means that red blood cells are being destroyed.
In this situation, the mother is producing an antibody against antigens on her child’s red
cells.
Normally, the mother and baby’s blood
don’t come into contact with one another.
But, if some of baby’s blood gets into mom’s
circulation, the mother can make antibodies
to any foreign antigens her immune system
sees. The most common opportunity for
this to take place is during delivery. As the
placenta separates, a sample of baby’s blood
can enter the mother’s circulation. Now,
any antigens present on the newborn’s cells
can encourage an immune response. This
does not cause a problem for this particular child because the mother and baby are no
longer attached by the umbilical cord. But, it may be a problem for later children.
Here is an important concept to help understand this disorder. To provide immune
protection for a developing fetus, a mother will produce and transport antibodies to her
child. This can protect baby from various diseases during pregnancy. The good thing is
that baby gets antibodies from its mother; the bad thing is that a baby gets antibodies from
its mother. If an antibody is designed to protect the child, that is a good thing. If it is an
antibody that targets any of the baby’s cells,
that isn’t good. The problem is that the
placenta can’t tell the difference.
There are different classes of antibodies.
One of these types is called immunoglobulin
G or IgG antibodies. This class is the one
that is actively transported across the
placenta. These classes will be discussed in
more detail later in the unit.
Assignment: Tortora, p. 710 or Wiley Plus – 19.8 Blood Groups and Blood Types

616
Objective 19 continued). Describe the interactions of the blood groups that cause
hemolytic disease of the newborn (HDN).
Here is an example of the scenario. If a
mother is Rh-negative, and the baby is Rh-
positive, her child has an antigen on its cells
that she doesn’t. How did the baby get it? It
was dad’s fault. The father gave the child
the gene to be Rh-positive. If the mother is
exposed to the child’s red cells, she will
likely make an Rh-antibody. Now, if she
gets pregnant again and the next child is Rh-
positive, she has a pre-formed antibody
against the fetus’ red cells. Her antibody can
cross the placenta and target the fetus’ red cells.
Can medical science keep the mother from
forming an Rh antibody? Well, it does. An
Rh-negative mother, who delivers an Rh-
positive child, is given a shot of Rhogam®.
Rhogam® is a dose of Rh-antibody. Wait,
the physician didn’t want her to get an Rh-
antibody. The key is that the antibody from
the injection wasn’t developed by her
immune system. If they can give her an Rh-
antibody that helps get rid of the Rh-
positive cells without her immune system
seeing them, the cells are gone, and she
never develops Rh-antibody of her own.
What if the Rh types from the previous example are reversed? What if the mother is Rh-
positive and the baby is Rh-negative. This isn’t a problem, but why? The baby is Rh-
negative; therefore there isn’t an Rh antigen to see, and if there was, who cares. Mom is Rh
-positive. She already has the Rh antigen. The immune system doesn’t make antibody to
antigen it doesn’t recognize as foreign, and the Rh antigen isn’t foreign to her.
OK, here is another question. How can a mother who is blood-type A have a baby with
type- B blood? An A person has B antibodies, and they’ve had them for the majority of
their life. The answer is in the antibodies. The A and B antibodies a person produces are
not IgGs, they are IgMs (different class). Therefore they are not transported across the
placenta and therefore not usually an issue.

617
Objective 20. Describe the structure and primary functions of the lymphatic system.
The lymphatic system is a system throughout the body made up of lymphatic vessels and
supporting organs that drain excess interstitial fluid, transport dietary lipids, and facilitate
immune responses.
The lymphatic system includes: lymphatic
fluid, lymphatic capillaries, vessels, trunks,
ducts, lymph nodes and nodules, red bone
marrow, the thymus gland, and the spleen.
Lymphatic vessels are a little different from
blood vessels. Blood vessels contain blood
that circulates to and from the heart. The
lymphatic vessels carry lymphatic fluid
(lymph) one way, from the tissue, back into
the blood stream.
Lymph vessels begin as small lymphatic capillaries that are located throughout the body in
the interstitial spaces. Lymphatic capillaries have overlapping endothelium that allows
interstitial fluid in, but not out. If pressure in the interstitial space is high, fluid flows in; if
it is low, the flaps close and fluid doesn’t enter. The lymphatic capillaries are held in place
by anchoring filaments. These are specialized fibers arising from the capillaries that extend
into the tissue.
As lymphatic capillaries converge, they form larger lymphatic vessels. Lymphatic vessels
have thin walls and valves to encourage one-way fluid movements.
Lymph nodes are present at intervals along
the lymphatic vessels. The lymph nodes
provide an opportunity for the lymphatic
fluid to come into contact with the immune
system. It is like a specialized sampling
process. The immune system gets a
continuous flow of information about what
is taking place in the body.
Assignment: Tortora, p. 832 or Wiley Plus – 22.1 Lymphatic System Structure and Function

618
Objective 21. Compare plasma, interstitial fluid, and lymphatic fluid (lymph).
Plasma is filtered by the capillary walls to form interstitial fluid. Most of the interstitial
fluid is reabsorbed back into the blood stream. Any excess fluid is drained from the tissue
through the lymphatic capillaries. On an average day, 20 liters of fluid passes from the
blood into the interstitial space; 17 liters are
reabsorbed back into the capillaries. The
lymphatic vessels drain the remaining three
liters.
Because proteins are too large to easily pass
through the capillary walls, the plasma
contains a much higher amount of protein
than interstitial fluid and lymph. Lymphatic
fluid is essentially just drainage from the
tissue, so it is identical to interstitial fluid.
Assignment: Tortora, p. 834 or Wiley Plus – 22.1 Lymphatic System Structure and Function
619
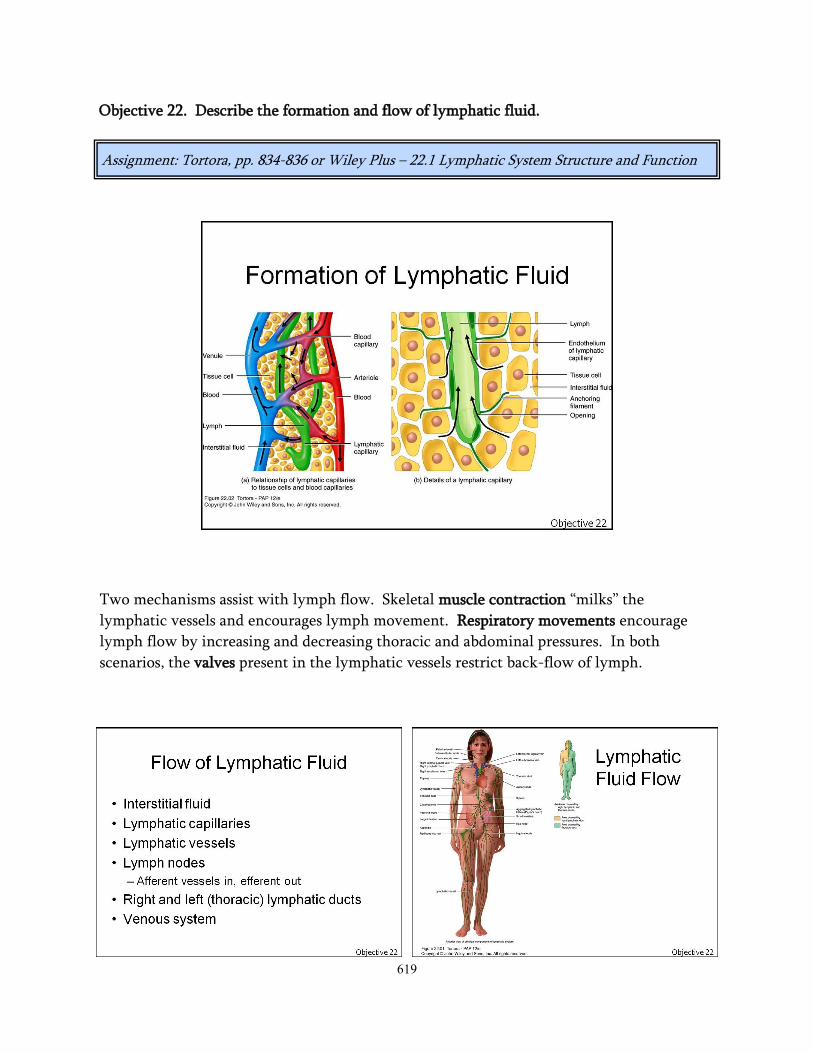
Objective 22. Describe the formation and flow of lymphatic fluid.
Two mechanisms assist with lymph flow. Skeletal muscle contraction “milks” the
lymphatic vessels and encourages lymph movement. Respiratory movements encourage
lymph flow by increasing and decreasing thoracic and abdominal pressures. In both
scenarios, the valves present in the lymphatic vessels restrict back-flow of lymph.
Assignment: Tortora, pp. 834-836 or Wiley Plus – 22.1 Lymphatic System Structure and Function

620
Flow of Fluids
1. Plasma in the blood
vessels
2. Interstitial fluid
3. Lymphatic capillaries
4. Lymphatic vessels
5. Lymphatic ducts
6. Back into the blood
stream
Objective 22 (continued). Describe the formation and flow of lymphatic fluid.

621
The secondary lymphatic organs and tissues
are sites where the majority of immune
responses take place. Lymph nodes and the
spleen are secondary lymphatic organs;
lymphatic nodules are secondary lymphatic
tissue. The difference is the presence or
absence of a capsule. Lymph nodes have a
connective tissue capsule, nodules do not.
Examples of lymphatic nodules include the
Peyer’s patches in the intestinal tract,
portions of the appendix, and the tonsils
(pharyngeal, adenoid and palatine).
Objective 23. Differentiate primary from secondary lymphatic organs/structures.
The primary lymphatic organs are the
locations where stem cells divide to produce
cells for immune functions. As these cells
mature, they become immunocompetent,
which means they can facilitate an immune
response. The primary lymphatic organs are
the bone marrow and the thymus gland.
Stem cells in the bone marrow divide to
produce both B lymphocytes and T
lymphocytes. B lymphocytes will remain in
the bone marrow to mature. T lymphocytes
will leave as pre-T lymphocytes and migrate
to the thymus gland to become
immunocompetent.
The thymus gland is located in the
mediastinum between the sternum and the
aorta. In infants, the thymus gland is
approximately 70 g. It will remain
approximately this size until after puberty
when connective and adipose tissue will
replace the thymic cells. By the time an
individual reaches old age, the thymus will
only weigh about 3 g, but it will continue to
release some mature T cells.
Assignment: Tortora, pp. 836-837 or Wiley Plus – 22.1 Lymphatic System Structure and Function

622
Objective 24. Describe the locations, structure, and function of lymph nodes.
Lymph nodes are bean-shaped lymphatic organs and are anywhere from 1 to 25 mm in
length. There are approximately 600 lymph nodes in the body, and they occur at intervals
along the lymphatic vessels. There are regions in the body where the lymph nodes are
group together more prominently: cervical, submandibular, axillary, and inguinal.
A lymph node is surrounded by a connective
tissue capsule. Extensions of the capsule
(trabeculae) divide the node into
compartments. There are two regions of a
lymph node, the cortex and the medulla.
Both regions contain large numbers of white
blood cells and macrophages. The types of
cells present in each region differ slightly.
The lymph node is the location where the
immune system gets a sample of the
interstitial fluid. It would be cumbersome
and costly to test every drop of water that passed through a water-purification facility, but
samples are checked on a regular basis. The lymph nodes in the body act as a sampling
system.
Lymph flows into a node through afferent lymphatic vessels. The lymph flows through the
cortex, where it comes into
contact with large
populations of B
lymphocytes, dendritic cells,
and macrophages. The lymph
continues to flow through
the node into the medulla.
There it is exposed to more B
lymphocytes, plasma cells
(activated B cells), and more
macrophages. The lymph
will then exit the lymph
node through efferent
vessels.
Assignment: Tortora, pp. 837-838 or Wiley Plus – 22.1 Lymphatic System Structure and Function

623
Objective 25. Contrast innate and adaptive immunity.
Innate immunity consists of a number of different cellular and chemical barriers which
non-specifically protect the body and respond to pathogenic organisms. In addition to
being non-specific, innate immunity is non-adaptive, meaning that the response doesn’t
change from exposure to exposure. Components of innate immunity include: the skin and
mucous membranes, cilia, antimicrobial chemicals, phagocytes, inflammation, and fever.
In contrast with innate immunity the adaptive immune response is specific, adaptive, and
generates memory. Components of adaptive immunity include: T lymphocytes, B
lymphocytes, plasma cells, and antibodies. The ability to respond against specific invaders
is the main function of adaptive immunity.
Assignment: Tortora, pp. 842 & 846 or Wiley Plus – 22.3 Innate Immunity

624
Objective 26. Compare the lines of defense associated with innate immunity.
There are two lines of defense associated with innate immunity. If the first barrier is
compromised, the second takes over, and to guarantee a response, the adaptive immunity
takes over.
The chemical and physical barriers of the
first line of defense include: mucus, mucus-
coated hairs, cilia, the lacrimal apparatus,
salivary glands, the flow of urine, vaginal
secretions, defecation, vomiting, sebaceous
secretions, perspiration, and gastric fluids.
Each of these barriers protects the various
external openings of the body.
The second line of defense includes a large
number of internal defenses. As part of this
line, the body produces natural antimicrobial
substances like interferons, complement, and
iron-binding proteins to decrease microbial
growth.
Non-specific phagocytes and natural killer
cells are part of this line. Natural killer (NK)
cells are actually a type of lymphocyte. They
make up 5-10% of our circulating
lymphocytes. There role is to release
chemicals from their granules to either
induce apoptosis or cause lysis of a targeted cell.
Assignment: Tortora, pp. 842-846 or Wiley Plus – 22.3 Innate Immunity
625
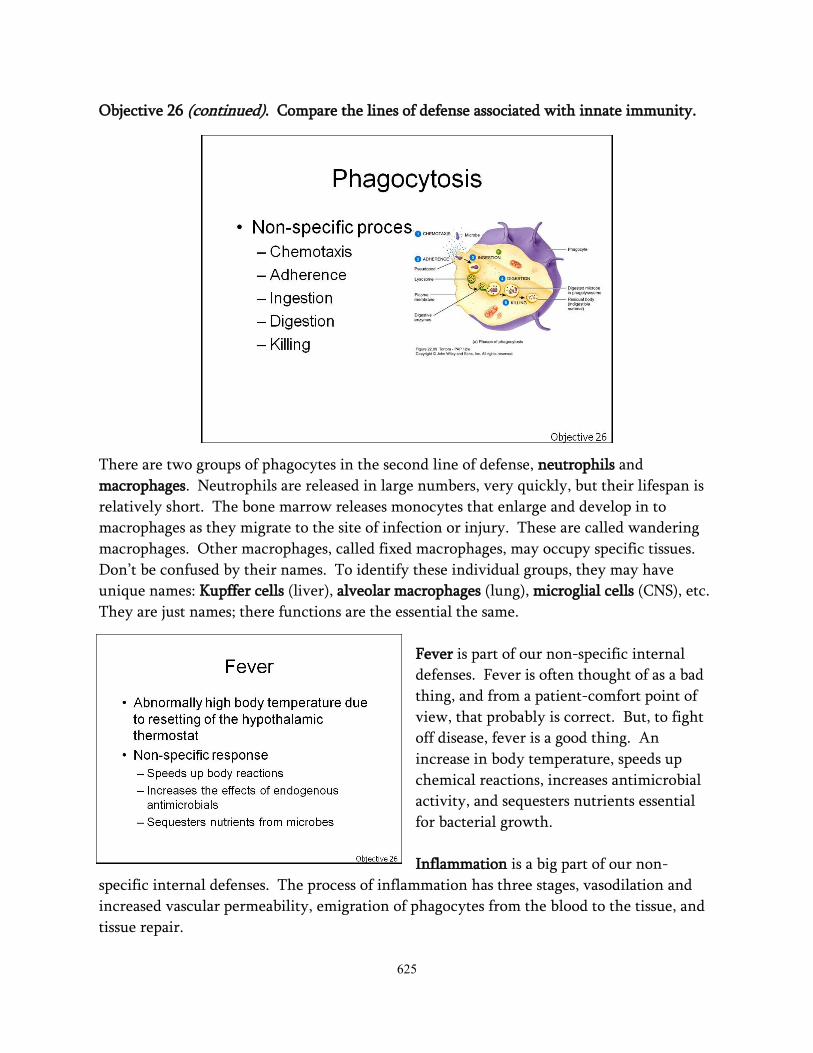
Objective 26 (continued). Compare the lines of defense associated with innate immunity.
There are two groups of phagocytes in the second line of defense, neutrophils and
macrophages. Neutrophils are released in large numbers, very quickly, but their lifespan is
relatively short. The bone marrow releases monocytes that enlarge and develop in to
macrophages as they migrate to the site of infection or injury. These are called wandering
macrophages. Other macrophages, called fixed macrophages, may occupy specific tissues.
Don’t be confused by their names. To identify these individual groups, they may have
unique names: Kupffer cells (liver), alveolar macrophages (lung), microglial cells (CNS), etc.
They are just names; there functions are the essential the same.
Fever is part of our non-specific internal
defenses. Fever is often thought of as a bad
thing, and from a patient-comfort point of
view, that probably is correct. But, to fight
off disease, fever is a good thing. An
increase in body temperature, speeds up
chemical reactions, increases antimicrobial
activity, and sequesters nutrients essential
for bacterial growth.
Inflammation is a big part of our non-
specific internal defenses. The process of inflammation has three stages, vasodilation and
increased vascular permeability, emigration of phagocytes from the blood to the tissue, and
tissue repair.
626
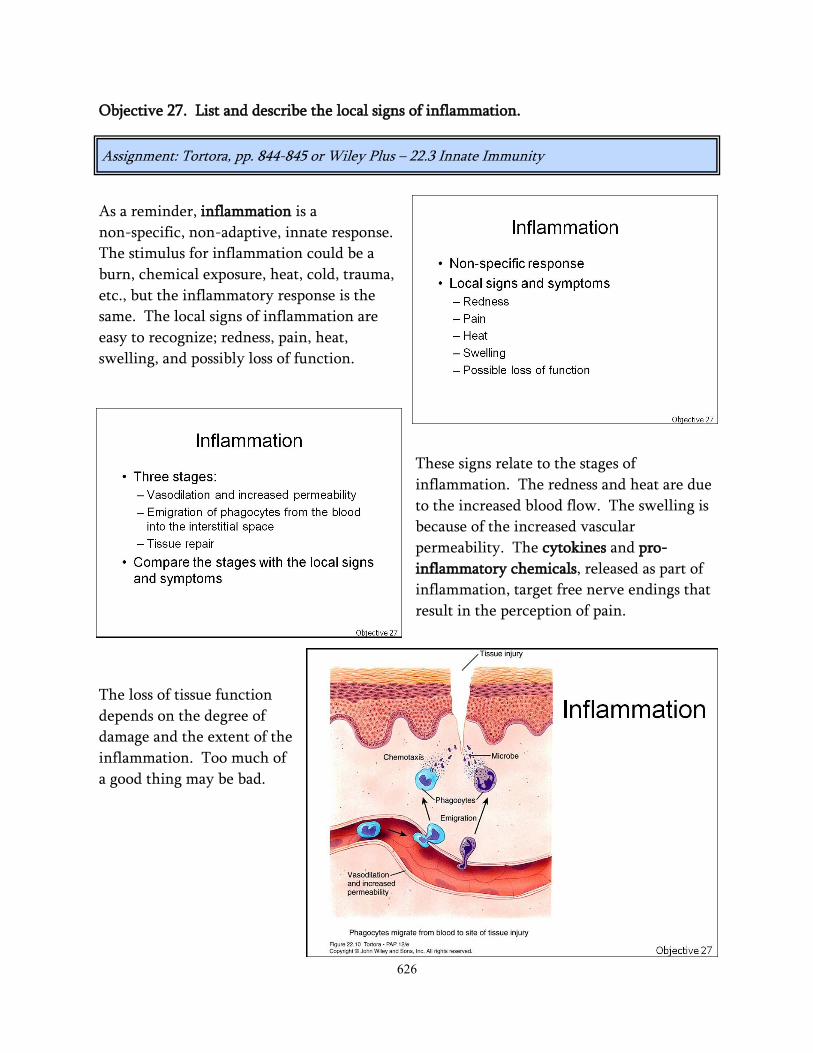
Objective 27. List and describe the local signs of inflammation.
As a reminder, inflammation is a
non-specific, non-adaptive, innate response.
The stimulus for inflammation could be a
burn, chemical exposure, heat, cold, trauma,
etc., but the inflammatory response is the
same. The local signs of inflammation are
easy to recognize; redness, pain, heat,
swelling, and possibly loss of function.
These signs relate to the stages of
inflammation. The redness and heat are due
to the increased blood flow. The swelling is
because of the increased vascular
permeability. The cytokines and pro-
inflammatory chemicals, released as part of
inflammation, target free nerve endings that
result in the perception of pain.
The loss of tissue function
depends on the degree of
damage and the extent of the
inflammation. Too much of
a good thing may be bad.
Assignment: Tortora, pp. 844-845 or Wiley Plus – 22.3 Innate Immunity

627
Objective 28. Define the term antigen and relate its characteristics to the adaptive immune
system.
A substance that is recognized as foreign and reacts with product of the immune system is
an antigen. An adaptive response to an antigen demonstrates specificity and memory. Both
of these characteristics will be described in
detail.
There are four main characteristics that
determine the antigenicity of substance:
recognition as foreign, structural
complexity, size, organic in nature.
Recognition as foreign is the most important
of the three. A potential antigen could fit
all of the others, but if the body deems it as
part of itself, it will leave it alone.
If a molecule fits all of the criteria, except
for size (<10,000 mw), it is referred to as a hapten. A hapten doesn’t trigger an immune
response, unless it binds to another molecule, now it is big enough.
If a pathogen is large enough, it may have multiple sites that can react with the immune
system. These sites are called antigenic determinants or epitopes.
Assignment: Tortora, pp. 846-849 or Wiley Plus – 22.4 Adaptive Immunity
628
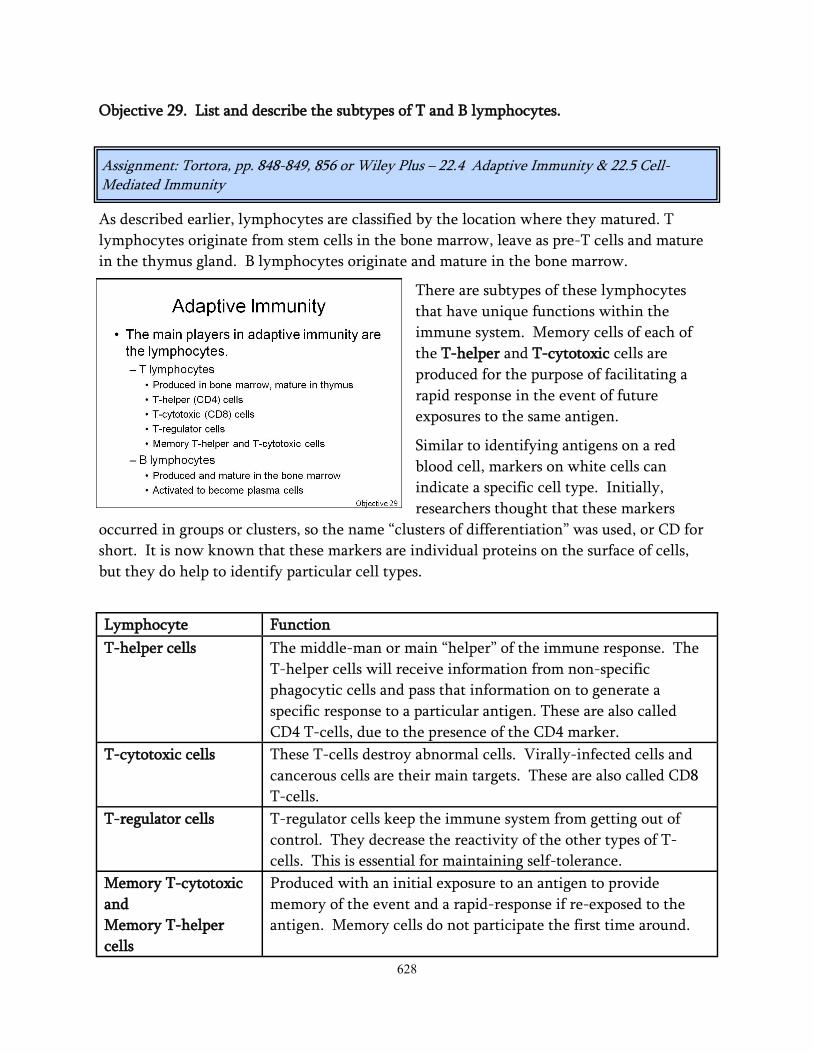
Objective 29. List and describe the subtypes of T and B lymphocytes.
As described earlier, lymphocytes are classified by the location where they matured. T
lymphocytes originate from stem cells in the bone marrow, leave as pre-T cells and mature
in the thymus gland. B lymphocytes originate and mature in the bone marrow.
There are subtypes of these lymphocytes
that have unique functions within the
immune system. Memory cells of each of
the T-helper and T-cytotoxic cells are
produced for the purpose of facilitating a
rapid response in the event of future
exposures to the same antigen.
Similar to identifying antigens on a red
blood cell, markers on white cells can
indicate a specific cell type. Initially,
researchers thought that these markers
occurred in groups or clusters, so the name “clusters of differentiation” was used, or CD for
short. It is now known that these markers are individual proteins on the surface of cells,
but they do help to identify particular cell types.
Assignment: Tortora, pp. 848-849, 856 or Wiley Plus – 22.4 Adaptive Immunity & 22.5 Cell-Mediated Immunity
Lymphocyte Function
T-helper cells The middle-man or main “helper” of the immune response. The
T-helper cells will receive information from non-specific
phagocytic cells and pass that information on to generate a
specific response to a particular antigen. These are also called
CD4 T-cells, due to the presence of the CD4 marker.
T-cytotoxic cells These T-cells destroy abnormal cells. Virally-infected cells and
cancerous cells are their main targets. These are also called CD8
T-cells.
T-regulator cells T-regulator cells keep the immune system from getting out of
control. They decrease the reactivity of the other types of T-
cells. This is essential for maintaining self-tolerance.
Memory T-cytotoxic
and
Memory T-helper
cells
Produced with an initial exposure to an antigen to provide
memory of the event and a rapid-response if re-exposed to the
antigen. Memory cells do not participate the first time around.

629
Each of these cells responds
to a specific antigen because
they have antigen receptors
for it. T-cells and B-cells
can respond to all antigens
presented to the immune
system, and because these
cells are spread throughout
the body, they are
constantly ready for any
exposure to specific
antigens. It sounds
impossible that the body can
respond to all potential
antigens, but the shuffling
genes (genetic
recombination) during
lymphocyte production give
the cell its specificity. Then
if one cell, specific to a
particular antigen, is active,
many copies of that cell can
be produced.
Objective 30. Compare cell-mediated and antibody-mediated immunity.
Cell-mediated and antibody-mediated
immunity are the two types of adaptive
immunity. Both mechanisms are triggered
by exposure to specific antigens.
In cell mediated immunity, T-cytotoxic cells
are activated directly against abnormal cells,
such as cancer cells or even tissue
transplants. In antibody-mediated
immunity, B-lymphocytes are activated to
become plasma cells, which produce and
secrete specific antibodies. Because T-
helper cells are the middle-men of adaptive
immunity, they are a part of both cell-
mediated and antibody-mediated immunity.
Assignment: Tortora, pp. 848, 856 or Wiley Plus – 22.4 Adaptive Immunity & 22.5 Cell-Mediated Immunity

630
Objective 31. Describe the major histocompatibility complex (MHC).
The major histocompatibility complex
(MHC) is a group of genes that codes for a
group of transmembrane proteins on the
surface of cells, sometimes called MHC
molecules or human leukocyte antigens
(HLA). Originally, they were thought to
exist only on leukocytes, so the name HLA
fit. Now it is known that they are present
on all nucleated cells.
These molecules are very important in the processing and presentation of antigen. They
allow a cell to respond to an antigen directly or to present the antigen to the rest of the
immune system.
There are two major types of MHC
molecules, class-I and class-II. MHC class-I
molecules are present on all body cells,
except red blood cells. MHC class-II
molecules are demonstrated on the surface
of antigen-presenting cells (APC).
Assignment: Tortora, pp. 850-852 or Wiley Plus – 22.4 Adaptive Immunity

631
Objective 32. List and describe the general steps of antigen processing and presentation.
Phagocytes are a very important part of the innate immune response, but if every antigen
were simply disposed of by phagocytes, components of the adaptive immune response would
very seldom get information about what took place. Therefore, there wouldn’t be a cell-
mediated or antibody response or memory. This requires cells that initially detect the
antigen to present it to the rest of the immune system. These cells are called antigen-
presenting cells (APCs).
APCs are commonly phagocytes, but B cells can present antigen. Antigen processing and
presentation differs slightly depending on whether or not the antigen was present outside of
the body cells (exogenous) or inside (endogenous). Examples of endogenous antigens include
viral proteins within virally-infected cells, toxins from intracellular bacteria, and abnormal
proteins in cancer cells.
Assignment: Tortora, pp. 850-851 or Wiley Plus – 22.4 Adaptive Immunity

632
Objective 32 (continued). List and describe the general steps of antigen processing and
presentation.
Once an antigen is presented on the surface
of an APC, it can now be recognized by the
adaptive immune response. This is where
the T-cell middle-man comes in. An
inactive T-helper cell, specific for the
antigen, will bind with its T-cell receptor to
the presented antigen on the APC. This will
activate the T-cell. The activated T-cell will
proliferate (increase its numbers) and
differentiate (mature). This process is called
clonal selection. Through this process the
active T-helper cells and T-memory cells are
produced.
An inactive T-cytotoxic cell will bind to
MHC class-I presented antigen infected
body cells. With the assistance
(costimulation) of the T-helper cells, the
cytotoxic cell becomes active. Through
clonal selection, a population of active T-
cytotoxic cells and memory T-cytotoxic cells
are produced.

633
Objective 32 (continued). List and describe the general steps of antigen processing and
presentation.
Lastly is the activation of B-cells; they can
be activated by two different mechanisms,
direct antigen attachment to B-cell
receptors or stimulation by activated T-
helper cells. Some new B-cell clones will
become B-memory cells, others will mature
into plasma cells and secrete antibodies
specific to the particular antigen.
Steps in Antigen Processing and Presentation
Exogenous Antigens Endogenous Antigens
Ingestion of the antigen Digestion of the antigen into fragments
Digestion of the antigen into fragments Synthesis of MHC class-I molecules
Synthesis of MHC class-II molecules Binding of fragments to class-I molecules
Vesicular packaging of class-II molecules Vesicular packaging of class-I molecules
Fusion of fragment and class-II vesicles
Insertion of the antigen-MHC class-I
complexes in the plasma membrane for
recognition
Binding of fragments to class-II molecules
Insertion of the antigen-MHC class-II
complexes in the plasma membrane for
recognition

634
Objective 33. Describe the role of cytokines in the immune response.
Cytokines are chemical signals from one cell
that influences another. These chemicals act
as small protein hormones to control cellular
growth and maturation. Each type of
cytokine has a cellular origin and specific
function. For example, erythropoietin is a
cytokine from the kidneys increases the
number and activity of red cell precursors in
the bone marrow. With modern research
techniques, the list of known cytokines is
becoming very large.
Assignment: Tortora, p. 852 or Wiley Plus – 22.4 Adaptive Immunity
Common Groups of Cytokines
Interleukins Cytokines between white blood cells
Interferon Anti-viral properties and stimulators of the immune
system
Tumor-necrosis factor (TNF) Produced by macrophages to encourage inflammation.

635
Objective 34. Describe the basic structure of antibodies and their actions in the immune
response.
Antibodies are commonly called gamma globulins, as well as immunoglobulins (Ig). They
have a specific structure that provides for their specificity. A general antibody consists of 4
polypeptide chains, two long (heavy chains) and two short (light chains). Disulfide bonds
link the chains together. This simple arrangement gives the antibody a characteristic Y-
shape. Most antibodies are one Y-shaped unit (monomer), but some can contain multiple
units (dimer and pentamer).
There are two main regions of an antibody,
the constant region and the variable region.
The variable region consists of the distal
segments of the heavy and light chains and
forms the antigen-binding site. This region
gives the antibody its specificity. The
constant region differs slightly for the
different classes of antibodies.
Assignment: Tortora, pp. 857-858 or Wiley Plus – 22.6 Antibody-mediated Immunity

636
Objective 34 (continued). Describe the basic structure of antibodies and their actions in the
immune response.
Antibodies don’t destroy anything directly, but they act as a great flagging system for the
immune system. Maybe a better statement is that they signal antigen for destruction, and
they disable antigen.
Antibody Action Result
Neutralizing antigen Neutralizes toxins and binds to viruses to restrict their binding
to host cells
Immobilizing bacteria Restricts the spread of motile bacteria by binding to cilia or
flagella
Agglutinating and
precipitating antigen
Multiple antigen-binding sites can result in one antibody
binding to 2 or more antigen, causing agglutination, binding
may cause soluble antigen to become insoluble
Activating complement Antigen/antibody complexes initiate the classical complement
pathway
Enhance phagocytosis Opsonize (flag) for phagocytosis
637
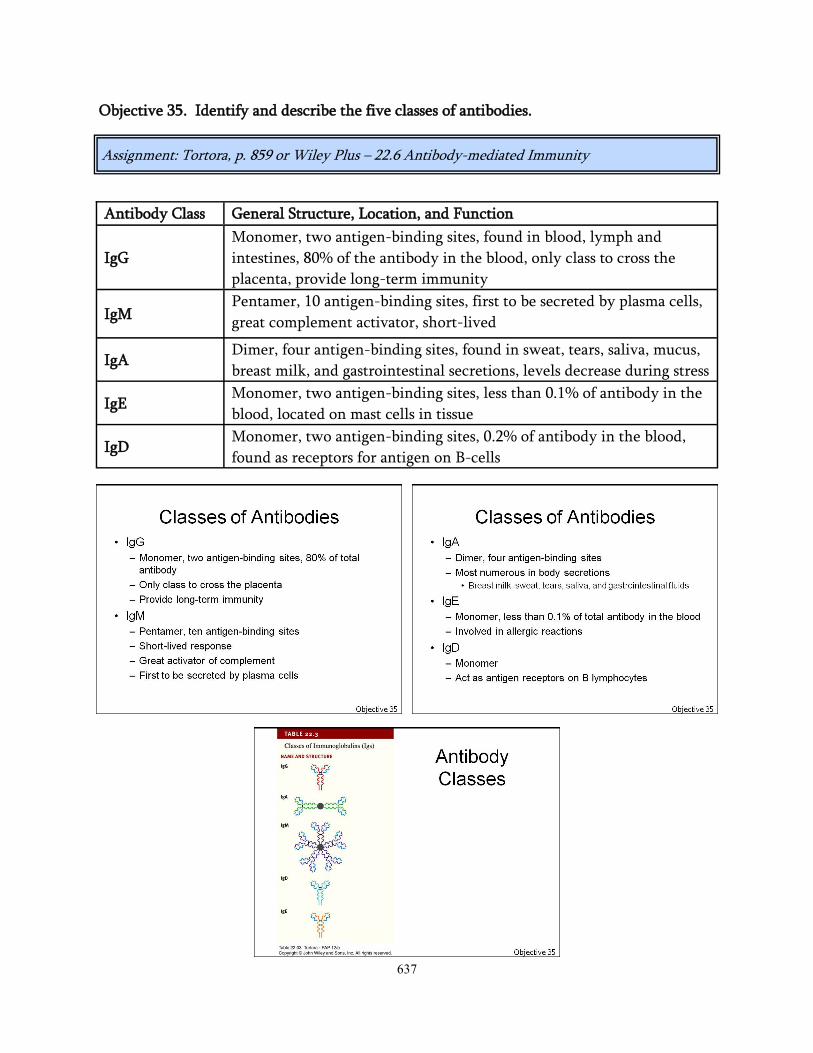
Objective 35. Identify and describe the five classes of antibodies.
Assignment: Tortora, p. 859 or Wiley Plus – 22.6 Antibody-mediated Immunity
Antibody Class General Structure, Location, and Function
IgG
Monomer, two antigen-binding sites, found in blood, lymph and
intestines, 80% of the antibody in the blood, only class to cross the
placenta, provide long-term immunity
IgM Pentamer, 10 antigen-binding sites, first to be secreted by plasma cells,
great complement activator, short-lived
IgA Dimer, four antigen-binding sites, found in sweat, tears, saliva, mucus,
breast milk, and gastrointestinal secretions, levels decrease during stress
IgE Monomer, two antigen-binding sites, less than 0.1% of antibody in the
blood, located on mast cells in tissue
IgD Monomer, two antigen-binding sites, 0.2% of antibody in the blood,
found as receptors for antigen on B-cells

638
Objective 36. List and describe ways to acquire adaptive immunity.
Adaptive immunity can be acquired in a
number of different ways: actively or
passively, and naturally or artificially.
Active acquisition of immunity means that
someone’s immune system was stimulated,
and they generated a cell and antibody-
mediated response as well as memory.
Passive immunity simply means the
products of immunity were given to them,
without any effort of their own. Active
immunity provides long-term immunity.
Passive is a short-lived response, the
acquired cells die or the antibodies are
eventually lost.
Active immunity is like baking a pie. An
individual pulls out the recipe book, makes
the crust and filling, and bakes the pie.
Using the same illustration, passive
immunity is simply buying a pie. The end
result is the same, there is a pie, but with
active immunity, memory is gained, and
immune products can be made over and
over again.
Assignment: Tortora, p. 861 or Wiley Plus – 22.6 Antibody-mediated Immunity
Acquiring Adaptive Immunity
Method Result
Naturally-acquired active immunity Immune products acquired following
exposure to antigen
Naturally-acquired passive immunity
Transfer of antibody from non-medical
source; IgG through the placenta, IgA
through breast milk
Artificially-acquired active immunity
Immune products acquired through
vaccination; antigens given that are
immunogenic but not pathogenic
Artificially-acquired passive immunity Prepared injection of antibody
639
Objective 37. Describe the components of the complement system and its role in
immunity.
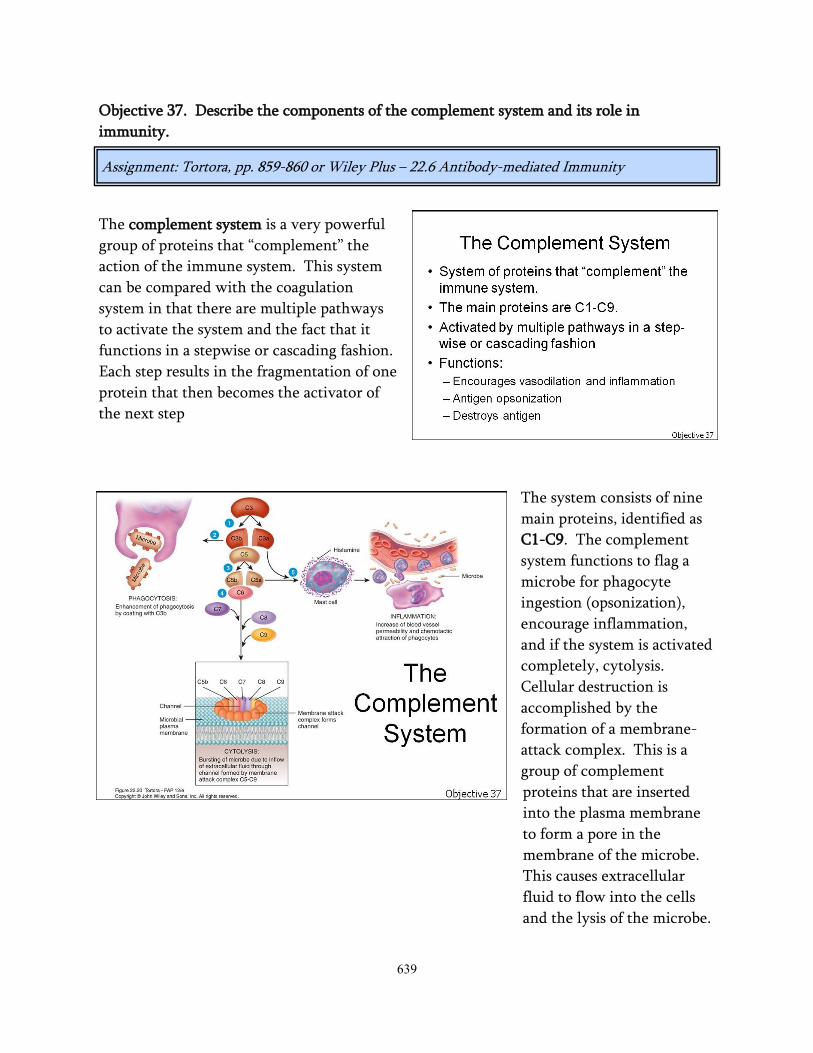
The complement system is a very powerful
group of proteins that “complement” the
action of the immune system. This system
can be compared with the coagulation
system in that there are multiple pathways
to activate the system and the fact that it
functions in a stepwise or cascading fashion.
Each step results in the fragmentation of one
protein that then becomes the activator of
the next step
The system consists of nine
main proteins, identified as
C1-C9. The complement
system functions to flag a
microbe for phagocyte
ingestion (opsonization),
encourage inflammation,
and if the system is activated
completely, cytolysis.
Cellular destruction is
accomplished by the
formation of a membrane-
attack complex. This is a
group of complement
proteins that are inserted
into the plasma membrane
to form a pore in the
membrane of the microbe.
This causes extracellular
fluid to flow into the cells
and the lysis of the microbe.
Assignment: Tortora, pp. 859-860 or Wiley Plus – 22.6 Antibody-mediated Immunity

640
Objective 38. Contrast the primary and secondary immune responses.
The differences between the primary and secondary immune responses illustrate the ability
of the immune system to demonstrate memory. The primary immune response is the
sequence of events and outcomes of the immune response with an initial exposure to an
antigen. The secondary response relates to second or subsequent exposures.
The indicator for an
antibody-mediated response
is an antibody titer. A titer
is a test that detects the
relative amount of antibody.
To understand an antibody
titer, it might be easy to
relate it to making
lemonade. When someone
makes lemonade, they add a
particular amount of
lemonade power to water.
If they add more water, it
decreases the concentration.
If they keep adding water,
they will eventually not be
able to even taste a hint of lemon. If the lemonade was initially very concentrated, they
would add a great deal of water before they couldn’t taste any lemon.
This is how antibody titers work. A clinical laboratorian will take a patient’s plasma and
determine whether or not there is any of a particular type of antibody. If there is, they will
dilute it and determine if they can still detect any antibody. If they can, they dilute it
again, and so on.
If a patient has an antibody titer of 256, their plasma was diluted 256 times before there
wasn’t any detectable antibody. The higher the number, the greater the concentration of
antibody there was originally in the plasma.
Assignment: Tortora, p. 861 or Wiley Plus – 22.6 Antibody-mediated Immunity

641
Objective 38 (continued). Contrast the primary and secondary immune responses.
There are two main differences between the primary and secondary immune responses:
time and antibody titer.
The first time the immune system recognizes an antigen, it takes a short period of time for
antigen processing, presentation, and antibody production. This period lasts approximately
5-7 days. Initially, the plasma cells will produce a population of IgM antibodies, followed
by a population of IgG. The goal of the primary response is to provide an initial antibody-
mediated response and produce a population of memory cells.
Because the primary response generates memory cells, the secondary response is immediate.
The antigen can be taken care of before a person even becomes symptomatic. Time to
process and present antigen is not necessary. There is an immediate increase in IgM
antibodies, followed quickly by a large, long-lasting increase in the amount of IgG
antibodies. This is one of the main reasons to provide booster shots for various
vaccinations.

642
Objective 39. Define self-recognition and self-tolerance and relate the terms to
autoimmune disease.
To keep from destroying oneself, the immune system must have two characteristics, self-
recognition and self-tolerance. Self-recognition is the ability to recognize one’s own
cellular markers. If a person’s immune system didn’t know what they look like, the
immune system would not able to recognize anything foreign.
Self-tolerance means to leave oneself alone. If any T or B cells have self-reactive antigen
receptors, they are either inactivated or deleted from the population.
A failure of self-recognition or self-tolerance would result in the development of
autoimmune diseases. Either scenario would result in the immune system’s perceiving that
various autoantigens were foreign and should be destroyed.
Assignment: Tortora, pp. 862, 867-868 or Wiley Plus – 22.7 Self-Recognition and Self-Tolerence & 22.9 Aging and the Immune System (Disorders: Homeostatic Imbalances)

643
Objective 40. Describe the effects of aging on the immune system.
It’s not a secret that individuals are more susceptible to infections and the development of
cancers as they age. This is due to a decreased function of the immune system. The thymus
atrophies as a person ages; this leads to lower T-cell numbers and a slower response. Due to
the lack of T-cells available to coordinate activities, the B-cell response is also slower. With
a slower immunological response, it is important that the elderly are properly vaccinated
against various infections.
The elderly have a similar quantity of antibodies as a middle-aged population, but a much
larger percentage of the antibodies are autoimmune antibodies. This is due to a lifetime of
slow and subtle cellular changes which can result in a decrease of self-tolerance.
Assignment: Tortora, p. 864 or Wiley Plus – 22.9 Aging and the Immune System