mha 2015 fall regional meetings -...
TRANSCRIPT

MHA 2015 Fall Regional MeetingsStrategies to Reduce Harms and Infections

Workgroup and Discussion Time
What is your priority harm/infection opportunity?
Debrief
PDCA

Welcome and Agenda
Introductions
Missouri harms and infections data review
Infection prevention focus areas: sepsis, hand hygiene, antimicrobial stewardship programming
Shared best practices
Workshop activity
Networking!!!

Missouri’s Performance
Q4CY2013 Q1CY2014 Q2CY2014 Q3CY2014 Q4CY2014 Q1CY2015
Total Infections 1323 1381 1366 1117 1146 1198
0
200
400
600
800
1000
1200
1400
1600
NU
MB
ER
OF I
NFE
CT
ION
S
STATE LEVEL NUMBER OF INFECTIONS FROM Q4CY2013 -Q1CY2015
9.4%
Q4CY2013 Q1CY2014 Q2CY2014 Q3CY2014 Q4CY2014 Q1CY2015
Total Harm 667 630 564 582 324 352
0
100
200
300
400
500
600
700
800
NU
MB
ER
OF H
AR
M E
VE
NT
S
REPORTING TIMEFRAME
STATE LEVEL RAW DATA FOR TOTAL HARM FROM Q4CY2013-Q1CY2015
42%
0
50
100
150
200
250
0
5
10
15
20
25
30
DV
T R
AT
E
TOTAL HARM BY OUTCOME MEASURE
Falls & Trauma Death Rate in Low Mortality DRG's
Pressure Rates DVT Rate
Falls = 38% increase


HAI Overview
Every day, 1 in 25 hospital patients suffer from at least one health care-associated infection
An estimate of 4,037 people died in Missouri hospitals because of an HAI in 2014
Pay-for-Performance
HAC Reduction Program penalty
VBP reimbursement
Costly
Substandard/not evidence based care

Link between HAI and Handwashing
Difficult to prove but studies with increasing hand hygiene show decreased infection rates


Key Structures to Hand Hygiene Programs
Successful hand hygiene educational programs should incorporate:
reinforcement of hand hygiene messages
knowledge of health care workers’ perceived importance of hand hygiene and its role in prevention of HAIs
monitoring and feedback of hand hygiene practices
practical education tools
role modeling by senior staff
supportive infrastructure and management

Meet Infection Control Barbie, Ami
Links to Hand WashingResources
Centers for Disease Control and Prevention
Institute for Healthcare Improvement
The Joint Commission
World Health Organization

Trending: Sepsis

Update
Effective October 1, 2015, CMS will enforce its new bundle measure for severe sepsis and septic shock as part of the Hospital Inpatient Quality Reporting (Hospital IQR) program
The new bundle is based on two time periods:
the first three hours of diagnosis
six hours of diagnosis
the clock starts as soon as presumed or confirmed severe sepsis is documented by diagnosis or criteria are met.

Sepsis Bundle Project: New CMS Guidelines
New measure beginning with 10/1/2015 discharges
Collected for CMS
Process measure
Added to align with CY 2015 IPPS Final Rule
Includes SEP-1 – Early Management Bundle, Severe Sepsis/Septic Shock
63 new data elements
Improvement noted as an increase in the rate

SEP Initial Patient Population
Population determined using five data elements
ICD-10-CM Principal Diagnosis Code
ICD-10-CM Other Diagnosis Code
Admission Date
Birthdate
Discharge Date

SEP Initial Patient Population
Patients admitted to the hospital for acute inpatient care with a PDC or ODC for sepsis as defined in Appendix A, Table 4.01
Age > or = to 18 years
LOS < or = to 120 days

SEP Sampling
Option of sampling quarterly or monthly
Hospitals selecting sample cases must ensure that the population and sample size meets the conditions

SEP Sampling
Quarterly Sample Size Based on Hospital’s Initial Patient Population Size for the Sepsis Measure

SEP Sampling
Monthly Sample Size Based on Hospital’s Initial Patient Population Size for the Sepsis Measure

It’s all about the lactate
Lactate Level
(mmol/L)
AssociatedMortality
Rate
≥ 4.0 27%
2.5-4.0 7%
<2.5 <5%

Surviving Sepsis Campaign

TO BE COMPLETED WITHIN 3 HOURS OF TIME OF PRESENTATION*:
1. Measure lactate level
2. Obtain blood cultures prior to administration of antibiotics
3. Administer broad spectrum antibiotics
4. Administer 30ml/kg crystalloid for hypotension or lactate ≥4mmol/L
* “Time of presentation” is defined as the time of triage in the emergency department or, if presenting from another care venue, from the earliest chart annotation consistent with all elements of severe sepsis or septic shock ascertained through chart review.
Surviving Sepsis Campaign, 2015.
Surviving Sepsis Bundle (update 2015)

Surviving Sepsis Bundle (update 2015)
TO BE COMPLETED WITHIN 6 HOURS OF TIME OF PRESENTATION:
5. Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation) to maintain a mean arterial pressure (MAP) ≥65mmHg
6. In the event of persistent hypotension after initial fluid administration (MAP < 65 mm Hg) or if initial lactate was ≥4 mmol/L, re-assess volume status and tissue perfusion and document findings (next slide)
7. Re-measure lactate if initial lactate elevated.
Surviving Sepsis Campaign, 2015.

DOCUMENT REASSESSMENT OF VOLUME STATUS AND TISSUE PERFUSION WITH
EITHER:
Repeat focused exam (after initial fluid resuscitation) by licensed independent practitioner including vital signs, cardiopulmonary, capillary refill, pulse, and skin findings.
OR TWO OF THE FOLLOWING:
Measure CVP
Measure ScvO2
Bedside cardiovascular ultrasound
Dynamic assessment of fluid responsiveness with passive leg raise or fluid challenge
Surviving Sepsis Bundle (update 2015)

Sepsis
Remains a serious, and growing, challenge
Rising Volumes Poor Outcomes Extreme Costs
2xHospitalizations for sepsis more than
doubled in the past decade
65% Percentage of sepsis
patients over 65
17%Increase in sepsis
inpatient hospital death rates in past decade
40-70% Mortality rates for septic
shock
700Patients die of severe
sepsis daily
$25,000Average cost per sepsis
case
6x Direct cost of treating
sepsis patient is six-fold higher than non-sepsis
patient
1Most costly reason for hospitalization in 2009
Sepsis Solutions International 2006The Advisory Board Group Company, 2014

Infections Inflammatory Response Progression
SIRS
• Temp >38° or <36°C, HR >90, RR >20 or PaCO2 <32, WBCs >12,000 or <4,000 or >10% bands
Sepsis
• SIRS + Infection
Severe Sepsis
• Sepsis + End Organ Damage
Septic Shock
• Severe Sepsis + Hypotension
(Systemic Inflammatory Response Syndrome)

Progress lags despite 13 year campaign
Surviving sepsis campaign yet to curb rising sepsis mortality rates
Increase in sepsis inpatient hospital death rates in the past decade
Physicians who follow pediatric sepsis guidelines
Physicians who adhere to 6-hour sepsis resuscitation bundle
17%
19%
31%
The Advisory Board Group Company, 2014

Many Hurdles Along Path to Delivering Sepsis Care
TriageEarly
ResuscitationOngoing
Management
Suspect sepsis Screen for sepsis Identify positive
screens Inform physician Kick-off 6 hr bundle Order sepsis panel
Draw cultures and lactate
Give antibiotics Collect test results Alert ICU or RRT Central line
insertion EGDT monitoring
ICU/Floor transfer Hand-off remaining
bundle steps Repeat lactate Collect culture
results Adjust antibiotics
47%Fail to order lactate with blood culture
50%Fail to administer
antibiotics within 6 hrs
72%Fail to document specific microbe
The Advisory Board Group Company, 2014

4-Tier Process for Severe Sepsis Program Implementation
Measuring Success and
CI
Implementation of the Sepsis
Bundle
Early Screening with Tools and Triggers
Organizational Consensus that Severe Sepsis Must be Managed
Early and Aggressively
Sepsis Solutions International 2006
Tier 1: Organizational Consensus and Support
Define Sepsis Program Goal and aligned with organizational goals
Identify Executive sponsor
Collect Baseline Data—essential step
Develop sepsis team(do we have all the right people here?) and schedule monthly (minimum) meetings for at least 6 months
Complete Team Charter
Identify nursing and physician champions in ED and ICU and ensure champions attend team meeting
Begin to define action plan and timeline for program development and implementation
Measuring Success and
CI
Implementation of the Sepsis
Bundle
Early Screening with Tools and Triggers
Organizational Consensus that Severe Sepsis Must be Managed
Early and Aggressively
Sepsis Solutions International 2006

Tier 1: Challenges and Barriers
Scheduling meetings and consistent attendance
Time
Skipping key steps
Charter
Communication plan (accountability)
Align within organization
Baseline data
Sepsis Solutions International 2006

Tier 2: Screening for Severe Sepsis
Define the Disease Continuum
Sepsis: presence of infection (suspected or confirmed) with systemic manifestations of infection
Severe Sepsis: Sepsis-induced tissue hypoperfusion or organ dysfunction
Septic Shock: Hypotension that persists despite adequate fluid resuscitation
Sepsis Solutions International 2006
Measuring Success and
CI
Implementation of the Sepsis
Bundle
Early Screening with Tools and Triggers
Organizational Consensus that Severe Sepsis Must be Managed
Early and Aggressively

Tier 2: Screening for Severe Sepsis
Develop screening process for ED, rapid response team and ICU (eventually housewide)
Develop audit process to evaluate compliance and effectiveness
Ensure screening process has clear “next steps” defined for nursing staff
Sepsis Solutions International 2006

Tier 3: Sepsis Bundle Implementation
Develop easy to use order sets (ED and ICU should be the same), organized by bundle
Order sets approved by appropriate medical and nursing leadership/committees
Identify resistance and barriers to bundle implementation and develop solutions
Ex: ability to get lactate quickly
Identify equipment needs and make capital requests
Develop triggers/processes to alert staff when time to move from first 3 hrs to shock bundle
Define educational plan for all staff
Develop implementation plan
Measuring Success and
CI
Implementation of the Sepsis
Bundle
Early Screening with Tools and Triggers
Organizational Consensus that Severe Sepsis Must be Managed
Early and Aggressively
Sepsis Solutions International 2006

Tier 3: Sepsis Bundle Implementation
Hospital resources often focus on planning phase and then back off after implementation.
The implementation phase is the most critical.
Frequent rounds by project champion recommended on unit to support staff and answer questions.
Defined resources for bedside nurse
Project champion has pager to be available 24/7 initially
Clinical nurse champions identified on each ICU unit and ED to be resources to bedside staff (these staff should be members of the sepsis team/committee
from the beginning)Sepsis Solutions International 2006

Tier 3: Sepsis Bundle Implementation
Identify who will oversee the implementation and the expectations of that person(sepsis nurse or program coordinator)
Define ICU/ED resources for staff that they can call at any time for questions and assistance
Create rounding schedule and process
Should begin as daily in the ICU and ED
Keep master list of all patients who go on the bundles (and those who should have but didn’t if possible)
Do real time interventions to ensure patients get the evidence based practices
Define follow up process for review and evaluate missed opportunities
Sepsis Solutions International 2006

Tier 4: Measure Success and Continuous Improvement
Define outcome and process data elements that will be collected
Develop and implement a data collection process
Revise and update goals and action plan as needed
Execute implementation plan
Measuring Success and
CI
Implementation of the Sepsis
Bundle
Early Screening with Tools and Triggers
Organizational Consensus that Severe Sepsis Must be Managed
Early and Aggressively
Sepsis Solutions International 2006

Tier 4: Measure Success and Continuous Improvement
Data Collection
Patient Log
Define how will find all patients that receive the bundles
Real time data collection is optimal—then used as checklist to ensure patient receives all appropriate interventions
Outcome
Mortality (ICU and Hosp)
Hosp LOS
Cost per case (total and direct)
Process
SSC database
Data elements that measure process achievement of the 3 & 6 hour bundles & outcome measures of the 6hrs
Sepsis Solutions International 2006
Strategies for Keeping Sepsis Front and Center
Align team with clinical and quality structures in organization
Sepsis program/goals part of hospital quality plan
Reporting progress and data quarterly to executive leadership
Report to hospital board annually
Standing agenda item on department meetings
Communication plan – includes flyers, newsletters, postings in units etc.
Code sepsis
Real time data measurement and feedback
Sepsis Solutions International 2006

Question
Where is your sepsis recognition priority
ED/EMS
Critical Care
Floors

Case Study 1Establishing an Emergency Department Sepsis Screen at St. Claire
Regional Medical Center, Kentucky

Discovering a Need at St. Claire Regional Medical Center
Chart reviews of patients with primary diagnosis of sepsis for the months of January-March 2012.
42 patients with primary diagnosis of sepsis.
21 patients met SIRS criteria at triage
13 of those 21 patients met SIRS criteria based on vital signs alone.
Only 3 of those 21 patients had the established sepsis order set initiated.
Bailey, P. (2014). St Claire Regional Medical Center.

Next Step at St. Claire Sepsis screening tool created and added into ED
triage assessment.
Performed on every adult patient upon arrival to emergency department.
If patient meets the criteria, the Triage Sepsis order set is initiated by the nurse and the patient is flagged on the tracker.
Bailey, P. (2014). St Claire Regional Medical Center.

Triage Sepsis Order Set at St. Claire
CBC
CMP
Magnesium
PTT, PT/INR
Lactate
Troponin
BNP
Blood culture x 2
CXR - portable
EKG
IV initiation and normal saline bolus
Bedside telemetry, non-invasive blood pressure, and continuous pulse oximetry monitoring
Bailey, P. (2014). St Claire Regional Medical Center.

Post-Intervention Data at St. Claire
Screening initiated on January 15th, 2013
235 positive screens from January 15th,2013 through June 30th, 2013
113 (48% of patients with positive screen) met criteria for diagnosis of sepsis
Main sources
Sepsis of urinary origin
Sepsis of pulmonary origin
Bailey, P. (2014). St Claire Regional Medical Center.

Case Study 2Reducing Sepsis Mortality at Wake Health

Case Study at Wake Forest: A Gradual Rollout to the Floors, ED, and ICU
Stepwise Approach Allows Initiative Refinement Along the Way
The Advisory Board Group Company, 2014

Wake Health’s Barriers to Optimal Sepsis Care Reflect Industry-wide Challenges
Multidisciplinary Staff Meeting to Uncover Barriers to
Optimal Sepsis Care at Wake Health
Meeting Attendees
Performance improvement experts
Faculty and house staff from medical, surgery, and neurology departments
ICU physicians
Respiratory therapy leaders
Frontline nurses
Pharmacists
Rapid response team
Barriers Identified
Guidelines not consistently followed in time-sensitive window
Responsibilities for identifying and treating sepsis in rapid timeframe not well-defined
Lack of education on sepsis and sepsis initiative among frontline staff
Clinicians took often take ad-hoc approach to screening and miss diagnoses
The Advisory Board Group Company, 2014

Reducing Sepsis Mortality at Wake Health Eight Tactics for Promoting Consistent, High-Quality Sepsis Care
IFormalize
Identification
1. Inpatient early warning sepsis screen
2. Acuity-sensitive ICU sepsis trigger
IIAccelerate Treatment
3. Simplified sepsis bundle
4. Top-of-license sepsis roles
5. Rapid response sepsis kit
6. Comfort care decision prompt
IIIHardwire
Accountability
7. Real-time protocol checklist
8. Phased bundle adherence accountability
The Advisory Board Group Company, 2014

Wake Health Roadmap
I: Formalize Identification
(Immersion Project coming Fall 2015!)

Definition of “Code Sepsis” at Wake Health
A patient emergency requiring immediate action for the treatment of potential sepsis and septic shock.
Early identification, communication, and intervention for patients with sepsis
Implementing the sepsis bundle (including antibiotics) within one hour
Signaling Initiative Importance with a Brand
“Code Sepsis” Logo
The Advisory Board Group Company, 2014

Wake Health Addresses Barriers to Identification
Barriers to Early Identification
Subtle symptoms often fly under the radar
Floor nurses not exposed to many sepsis cases
Nurses reluctant to sound alarm because of false positive
All clinicians extremely busy
Site of Care
Screen Used
Provider Responsible for Screening
Screening Frequency
Inpatient Floor
Early Warning System
Nursing assistant checks vitals and RN patient alertness
• Every 4 hours for first 24 hours
• If patient is stable after 24 hours, every hours
• Is EWS is between 5-7, every four hours
ICU SIRS and “snooze criteria”
Bedside nurse • Upon ICU admission• Every 12 hours as
needed
ED EWS RN During ED triage
Sepsis Identification Process Across Inpatient Floor, ED, and ICU
The Advisory Board Group Company, 2014

Sepsis Screen Tells Nurses When to Sound the Alarm
Early Warning Score Criteria
Used on inpatient floors and EDThe Advisory Board Group Company, 2014

“Post-Snooze Phase”
Nurses conduct sepsis screen every 12 hours or as needed: if positive for SIRES nurse draws lactate: if abnormal lactate and/or potential infection, nurse calls “Code Sepsis”
Sepsis Trigger in ICU Reduces False AlarmsICU sepsis screen accounts for high acuity
“Snooze Phase”
Patients expected to meet SIRS criteria, but not have sepsis: nurses do not trigger sepsis alert
Patient Timeline in ICU
Hitting the “Snooze” to Reduce False Alarms
“The sepsis trigger needs to be like an alarm clock when you hit the snooze alarm. ICU patients will meet SIRS criteria for a period of time and it shouldn’t always trigger an alert.”
ICU Physician, Wake Forest Baptist Health
The Advisory Board Group Company, 2014

Complete “Snooze” CriteriaLength of Time per “Snooze” Based on Diagnosis
“Snooze” time must elapse before triggering a sepsis alert for patient who meet SIRS Criteria
If a patient is… Snooze them for…
On ABX for Sepsis 96 hrs from new ABX start/change in ABX
Post-Arrest Hypothermia Protocol Patients
72 hours from arrival to facility
DNR/Comfort Care Permanent, unless order changed
Trauma Patient 48 hours from arrival to facility
Patient has CT Surgery 48 hours from return to unit
AMI patients (including STEMIs) 48 hours from return to unit
TAVR Value 24 hours from return to unit
Intracranial bleed 24 hours from arrival to ED
Surgery 24 hours from return to unit
The Advisory Board Group Company, 2014

Wake Health Roadmap
II: Accelerate Treatment

Rapid Treatment Crucial to Reduce Mortality
Impact of Compliance with 6-hour Sepsis Bundle on Hospital Mortality
The Advisory Board Group Company, 2014

Drawing the Link from Staff Activities to Mortality
The Advisory Board Group Company, 2014

Simplifying Guidelines to a Four-Component Bundle
Simplified, Time-Sensitive Sepsis Resuscitation Bundle at Wake
Forest Health
1. Measure serum lactate
2. Obtain blood cultures prior to antibiotic administration
3. Administer broad-spectrum antibiotics within one hour
4. Fluid resuscitation if MAP<65 or elevated lactate
The Advisory Board Group Company, 2014

Defined Roles Expedite Sepsis Care on the Floor
Initial Sepsis Care Actions and Parties Responsible at Wake Health
For Inpatient Floor Code Sepsis
The Advisory Board Group Company, 2014

Pharmacists
Pharmacist monitors timing between Code Sepsis page and receiving antibiotic order from physician; follows up with first-call provider if order is not received in a timely manner
Once a physician verbally confirms sepsis and site of infection to pharmacist over the phone, pharmacist places order for appropriate broad-spectrum antibiotics
Pharmacist delivers antibiotics directly to Code Sepsis patient’s bedside
Empowering Staff to Practice at Top-of-License
Rapid Response Nurses
All rapid response nurses have critical care experience and are highly regarded by the medical staff
Nurses take lactate tests to stat lab and draw blood culture for Code Sepsis patients
Physicians agreed to pass on these responsibilities to RNs after data showed physicians were not consistently doing lactate tests
The Advisory Board Group Company, 2014

Rapid Response Sepsis Kit Supply List
Minimizing Time Wasted on Gathering SuppliesSepsis kit ensures all necessary supplies are quickly available to RRT
The Advisory Board Group Company, 2014

Sample Treatment Decision Tree Before Calling RRT
When Curative Treatment is Not the Goal
Physician Feedback Prompts Mandated
Comfort Care Decisions
Physician feedback reveals providers occasionally choosing not to deliver sepsis bundle because it does not align with patient care goal of comfort care
Wake Health trains first call physicians to consider patient care goals before initiating sepsis bundle
Physicians may opt out of Rapid Response Team trigger if patient and family decide to pursue palliative care or hospice
The Advisory Board Group Company, 2014

Wake Health Roadmap
III: Hardwire Accountability

Driving Bundle Compliance, Real-TimeRapid Responses Sepsis Screening Tool at Wake Health
The Advisory Board Group Company, 2014

Tiered Monitoring Efforts Instill Accountability
Stages of the Sepsis Bundle Accountability Strategy at Wake Health
The Advisory Board Group Company, 2014
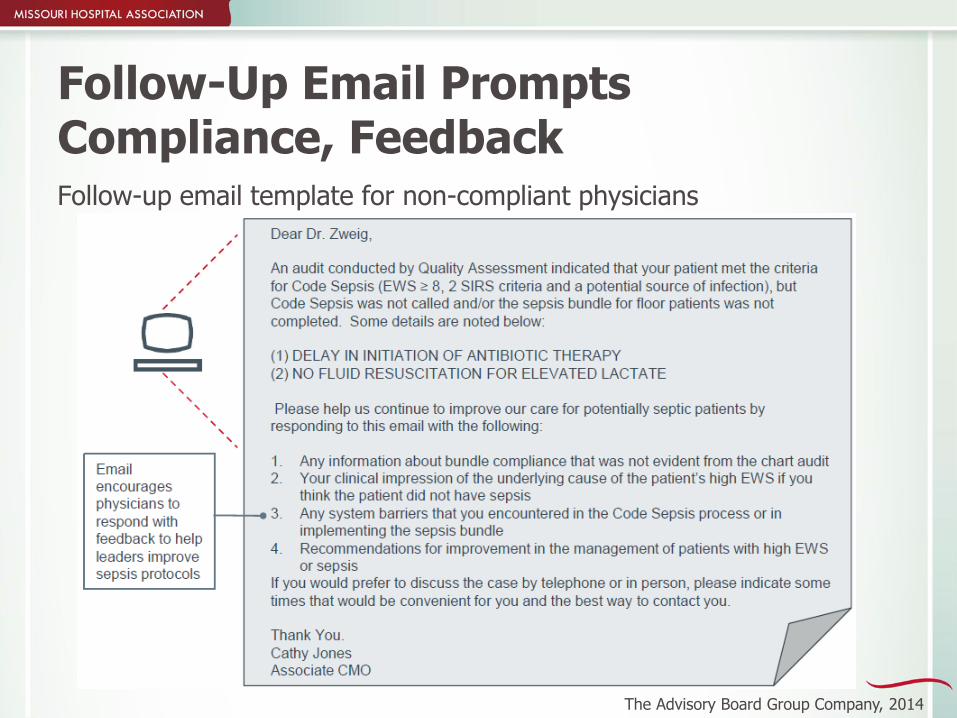
Follow-Up Email Prompts Compliance, FeedbackFollow-up email template for non-compliant physicians
The Advisory Board Group Company, 2014

Recognizing Physicians for Bundle Adherence
CMO-signed email reinforces sepsis as organization-wide priority
Thank-you email template for compliant physicians
The Advisory Board Group Company, 2014

Wake Health’s Across-the-Board Improvement
The Advisory Board Group Company, 2014

Key Takeaways from Wake Health
Make it a team effort: optimal sepsis care relies on a systematized, team approach (even if physicians know how to treat sepsis).
Approach non-adherence to the sepsis bundle as an opportunity to solicit feedback from clinicians on what barriers are standing in their way.
Getting clinicians comfortable with giving antibiotics to patients without confirmation of infection is a significant challenge, but critical to ensuring timely antibiotic administration.
Senior leadership involvement is a must to signal organizational commitment and promote accountability.
The Advisory Board Group Company, 2014

Packet Resources
Advisory Board 10 Imperatives to Reduce Sepsis Mortality
Surviving Sepsis Campaign Bundle

Questions?
Jessica Rowden, RN, BSN, MHA
Clinical Quality Improvement Manager
Missouri Hospital Association
(573) 893-3700, ext. 1391

MHA FALL REGIONAL MEETINGS September 24, 2015
Clinical Excellence: Reducing Patient Harm &
Infections
Dennis Manley, RN, HRM, CPHQ
Chief Nursing Officer
Mercy Hospital Joplin
73

EF5 Tornado Impact on Mercy Hospital
Direct Hit
Windows and Walls blown out
Portions of roof pulled off
Building infrastructure severely damaged
Generators destroyed
All communication lost
Water, sprinkler, gas and sewer pipes disrupted
Liquid O2 tanks damaged
Massive debris throughout building
74

EF5 Tornado Impact on Mercy Hospital 86 Medical Staff Member’s Offices
destroyed or severely damaged
Medical Office building on property
heavily damaged
Rehab building heavily damaged
– some generator power
Helicopter destroyed
Disaster trailer destroyed
75

76

Take-Aways You do what you practice/drill
Evaluate drills/responses to improve your plan Drill until you fail Add patient slippers/shoes to your weather plan
When under storm watches announce periodically to keep staff informed.
Know your contacts Local EOC-Coalition
Strong community group that plan and drill together State level positions Hospital Association
Store emergency response supplies where you will need to use them
77

Take-Aways continuedMake emergency supplies easily portable
Grab bags at locations throughout facilityPaper and pen
Record where patients are evacuatedGloves Flashlights & batteries
Consider marking rooms that have been searched and evacuated
Establish communications as rapidly as possible –especially with other key sites Cell phone # - texting
78

Take-Aways continued Respond to disaster situations with name badge
Educate
Security needs increase rapidly
Take care of yourself, your staff and their families Employee Assistant Program (EAP) – debriefing
Consider your staffing needs for Day #1 through?
79

Storm Hardening
High Performance Windows
Safety Laminated
Greater than 140 mph rated
Greater than 250 mph rated
80

81
Storm Hardening
Durable Exterior Skin Precast concrete exterior
No metal panels
No plastered exteriors
Poured concrete roof
No ballast
No metal decking
Hurricane-grade entry doors
Reinforced Penthouse
Designed for high impact/high wind
82

Storm Hardening
Protected interiors Hallway safe zones
Heavy-duty storm doors
Reinforced walls
Additional ceiling supports
Ante room and storm doors at hallway ends
Emergency storage next to stairwells
Battery-powered lighting
83

Storm Hardening
Power on Generator partially buried in reinforced concrete structure
All fuel tanks buried – 96 hours of run time
Two independent power feeds from different power stations
All utilities connect to building via underground tunnel
All critical care ventilator and bassinets on uninterrupted
power sources
Function for 2 hours
84

1 85
86
Completion Date: March 2015
Dennis Manley, RN, HRM, CPHQ
Chief Nursing Office
Mercy Hospital– Joplin, MO

Antibiotic/Antimicrobial Stewardship

Goal #2:
Reduce health care costs without adversely affecting the quality of care
Stewardship Program Goals
Goal #1:
Optimize clinical outcomes while minimizing the unintended consequences of antimicrobial use

Antibiotic Resistance
Antibiotic resistance is not a new phenomenon
Within 10 years of penicillin’s discovery in 1928, group A streptococci and pneumococci had already developed modes of resistance
What is new?
the growing magnitude of the problem
the speed with which new resistant pathogens are emerging
the decline in new antibiotic research and development

Antibiotic Resistance
At least some clinical isolates of many pathogenic bacterial species are now resistant to most antibiotics
Most new antibiotic developments have failed to expand on the “golden era” of antibiotics
Poses a significant patient safety and public health issue

• Patient harm, morbidity, mortality
• Cost of care• Cross-transmission
Stats
In a survey of 505 acute care hospitals, 78% had evidence of redundant antibiotic usage
Antibiotic exposure is the single most important risk factor for the development of C. difficile
Antibiotic Resistance
Root-Causes
Prescribing incorrectly
Over-prescribing
Unnecessarily prescribing
Outside Pressures and Future Pay-for-Performance??
Antibiotic stewardship programs currently voluntary
CDC urging CMS to “put teeth” to it and include as part of pay-for-performance
“10 x ’20 initiative,” a call to action to develop 10 new antimicrobial drugs by the year 2020 (IDSA)
Strategies to Address Antimicrobial Resistance Act (H.R. 2400 known as STAAR) — introduced in May 2009

Educating providers on use and resistance
Guidelines for management of common infection syndromes
Computer decision support
Specific improvement interventions
Components of an AR Program*
Leadership commitment
Accountability via an interprofessional team with a designated leader
Designated pharmacy leader
Tracking of antibiotic use
Regular reporting on antibiotic use and resistance
*2014 CDC Core Elements of Hospital Antibiotic Stewardship Programs and 2007 Guidelines for Developing an Institutional Program to Enhance Antimicrobial Stewardship

Ensure the “Basics”
Anderson DJ, Kaye KS. Controlling antimicrobial resistance in the hospital. Infect Dis Clin North Am. 2009; 23:847-64, vii-viii.
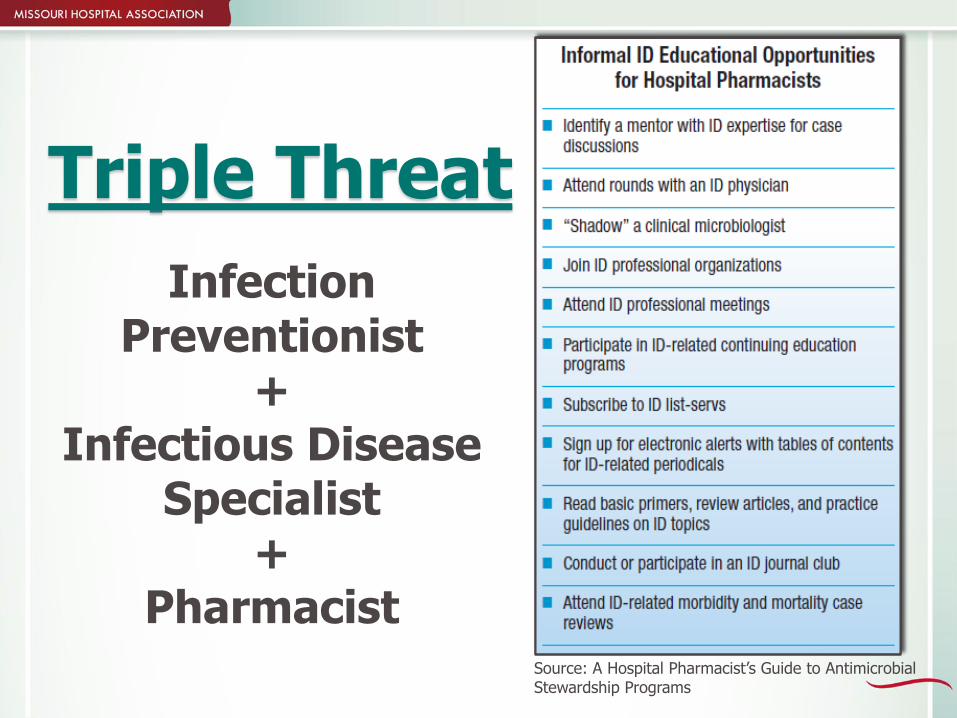
Infection Preventionist
+Infectious Disease
Specialist+
Pharmacist
Triple Threat
Source: A Hospital Pharmacist’s Guide to AntimicrobialStewardship Programs

Recommended Strategies
• Hard stops• Care
bundles• Antibiotic
“timeouts”• Committee
structure• Antibiotic
cycling• Education
feedback strategies High Reliability Organization Principles!!


Data Needed!
Measurement methodology is not exact
Example: defined daily doses
Health care informatics focus areas and goal
Hospitals can measure antimicrobial use, track changes in antimicrobial use and resistance over time, compare to similar institutions, and provide data to regional and national databases to allow largescale tracking of trends
Encourage reporting through NHSN (HIDI Group)
Source: A Hospital Pharmacist’s Guide to AntimicrobialStewardship Programs

Quality – Finance Link: ASP Program Return on Investment• Calculation of anticipated savings may
be based on current use and practices and estimates of the impact of proposed interventions. Such calculations may be useful in obtaining initial support for the development of an ASP.
• Calculation of actual savings can be based on the results of specific patient-level interventions or on aggregate data for the entire hospital/facility from pre-and post-intervention periods. Such calculations may be one method of demonstrating the value of the ASP and justifying requests for additional financial support (e.g., personnel resources) for the program.

Associated Savings
Reduced LOS
Reduced incidence of C. difficile
Reductions in rates of antibiotic resistance among health care facility–associated pathogens
Reduced incidence of toxicity
Cost Savings Opportunities
Direct Savings
IV:PO Conversions
Reductions in use of high-cost antimicrobials
Reductions in performing therapeutic drug monitoring (TDM) lab tests
Reduction in overall antimicrobial use
Population Health Implications
Care Coordination
Cross-transmission among hospitals, LTC, and the community
Lack of systemic control of antibiotic use across domains of care
Increase in outpatient and LTC setting antibiotic usage
Population Health Implications
Antibiotic use in animal medicine/food animal production
Antibiotic use in agriculture for food production
Growing body of evidence noting link between antibiotic use in food/animals to antibiotic resistance in humans
Includes the direct acquisition of resistant pathogens through the food supply as well as the transfer of resistance genes to human bacterial populations
Recommendations to decrease/eliminate use

ASP Resources
CDC
IDSA
LeadStewardship.org
APIC
SHEA
ASHP
Society of Infectious Disease Pharmacists
The Ohio State University
UCLA Health System
The Nebraska Medical Center

ASP Resources

Workgroup and Discussion Time
What is your priority harm/infection opportunity?
Debrief
PDCA

MHA Upcoming Events
Awaiting HEN 2.0 contract award
What’s Up Wednesday?
First Wednesday of the month, 12-1 pm
HEN 2.0 and Immersion Projects Kick-Off
Oct. 15, Columbia
Immersion Project registration by Oct. 31
– Introductory webinars – Sept. 23 and 30
Transparency Initiative Update – Sept. 25 and Nov.10
MHA Convention and Trade Show – Nov. 4-6
Quarterly Quality Webinar – Nov. 18

MHA:SQI - http://web.mhanet.com/strategic-quality/
Leslie Porth, Ph.D., R.N.
Division Vice President of Strategic Quality
Improvement
Triple Aim
Population Health
Oversight of division (Quality Improvement,
Quality Works, Emergency
Preparedness)
MONL
Alison Williams, R.N., BSN, MBA-
HCM
Vice President of Clinical Quality Improvement
Dana Downing, B.S., MBA-H,
CPHQ
Vice President of Quality Program
Development
National quality measures
Quality outcome transparency
Electronic clinical quality measures
MBQIP grant lead
MOAHQ
Jessica Rowden, R.N., BSN, MHA
Clinical Quality Improvement
Manager
Clinical quality SME
Data management and analytics
HEN/AHRQ grant projects
TeamSTEPPS
Host of WUW|LNL
MOAHQ
MONL
Cheryl Eads
Executive Assistant of Quality Improvement
Provides support to the SQI team
Coordinates webinars, conference calls and
meetings
Distributes correspondence and
communication
Assists in maintaining reports
[email protected]/893-3700x1305
[email protected]/893-3700x1326
[email protected]/893-3700x1314
[email protected]/893-3700x1391
[email protected]/893-3700x1382
Clinical quality SME
Oversight of Quality Improvement
Grant management
Collaborative management
Patient & Family Engagement
MONL
MOAHQ