mha: strategic quality
TRANSCRIPT

MHA: Strategic Quality What’s Up Wednesday|Lunch and LearnYour clinical quality, process improvement resource
Jessica Rowden, MHA, BSN, R.N., CPHQ
Director of Clinical Quality
http://web.mhanet.com/strategic-quality/
1

Housekeeping
Interactive networking platform
Press *1
Type questions in the question box feature of the webinar platform
Please fill out the evaluation
Give feedback
Offer suggestions of what would be beneficial to your organization
Be a featured hospital speaker!
2

February Topics
Opioid Prescribing Recommendations and Tracking
Mercy Hospital: Disposable ECGs decrease sternal wounds
Equity
Qualaris
Transparency
Immersion project
HEN 2.0
Upcoming events
3

Opioid Prescribing Recommendations
4

Opioid Recommendations Goal to reduce opioid painkiller misuse and abuse
Six organizations:
5
o Missouri Academy of Family Physicians
o Missouri Hospital Association
o Missouri Association of Osteopathic Physicians and Surgeons
o Missouri Dental Association
o Missouri College of Emergency Physicians
o Missouri State Medical Association
Policy recommendations
A focused pain assessment prior to determination of treatment plan
Diagnoses based on evidence-based guidelines
Non-narcotic treatment of symptomatic, non-traumatic tooth pain should be utilized when possible
Treatment of chronic pain should begin with an attempt to contact the primary opioid
Opioid analgesic prescriptions for chronic conditions limited to no more than 72 hours
Limit the prescription to the shortest duration needed that effectively controls the patient’s pain until follow-up care accessed
6

Policy recommendations
ED physicians and providers should not provide prescriptions for controlled substances that are claimed to be lost or destroyed
ED physicians and providers should not prescribe long-acting or controlled release opioids
ED staff should counsel patients on proper use, storage, and disposal of narcotic medications
Health care providers should encourage policies that allow providers to prescribe and dispense naloxone to public health, law enforcement and family as an antidote for opioid overdoses
7

Disposable ECG Leads to
Decrease Sternal Wound
Infections
Elizabeth Boyle RN, BSN, CCRN, MS
Kara Battig RN, BSN, CCRN-CSC

Introduction
• In coronary artery bypass graft (CABG) patients, post-operative
sternal wound infections are a costly and potentially deadly
complication.
– Superficial sternal wound infection (SSWI)
– Deep sternal wound infection (DSWI)

• Complications of sternal wound infections:– Accumulate an average of 20 additional hospital days and cost
the hospital an estimated 2.8 times the amount of money of an
uncomplicated CABG procedure.
– A DSWI increases the mortality risk from 5.4% for an
uncomplicated procedure to as high as 28.6% at the 1.5 year
mark.

• A number of studies have highlighted the role of reusable ECG
leads in the spread of infection.
• The use of single-patient, disposable ECG leads eliminated the
pathway for bacterial spread from one patient to the next.
Reusable Single-Use

Methods
• Retrospective chart audit was conducted, using all
cardiothoracic surgery patients who had undergone a
CABG procedure.
– From July 2012-June 2013, all patients were recovered using
reusable Phillips 5 Lead Set Grabber AAMI leads.
– From July 2013-June 2014, all patients were given Covidien ™
Kendall ™ DL Disposable Cable and Lead Wire System single-
patient use leads.

Results
July 2012-June 2013
• 289 CABG patients.
• Total of six developed
sternal wound infections:
– Two SSWIs
– Four DSWIs
July 2013-June 2014
• 268 CABG patients.
• Total of three sternal
wounds:
– Three SSWIs
– ZERO DSWIs
• Cultures of those three
SSWIs revealed a S.
Aureus colonization.

• The total number of infections was decreased by
half with the utilization of disposable ECG leads.
• The incidence of DSWI was completely
eliminated.

0
1
2
3
4
5
6
7
July 2012-June 2013 July 2013-June 2014
Total Number of Infections
Number of Infections
Linear (Number of Infections)

0
1
2
3
4
5
July 2012-June 2013 (Non-DisposableLeads)
July 2013-June 2014 (Disposable Leads)
Number of Deep Sternal Wound Infections (DSWI)
Number of Deep Infections
Cost Avoidance
• The average DSWI costs hospitals an average of 2.8
times the cost the hospital makes on an uncomplicated
CABG.
• The price for all the disposable ECG leads for the
projected number of CABG cases in 2015 is $12,909.
• After collaboration with the Mercy Finance Department
and a retrospective study of the cost Mercy incurred
related to sternal wound infections, it was determined
that there was a cost avoidance of:
$263,545/year

(400,000)
(300,000)
(200,000)
(100,000)
0
100,000
200,000
300,000
400,000
Cost of Infectionfor Reuseable
Leads
Cost of Infectionfor Disposable
Leads
Cost of Leads perYear
Cost Avoidancefor 2015
Cost Avoidance for Mercy Hospital
Dollars
Discussion
• Cultures of remaining superficial sternal wound
infections yielded growth of S. Aureus, a common
organism usually found on the surface of the skin.
• This conclusion presents an opportunity for further
education and study.

Conclusion
• With the utilization of disposable ECG
leads, deep sternal wound infections have
been completely eliminated.
• By continuing the use of disposable leads
in our cardiothoracic surgical patients, we
will be able to decrease the number of
surgical site infections and therefore
decrease the length of stay, cost incurred
by the hospital, and patient mortality rates.

References
Barnett, T. E. (2007). The not-so-hidden costs of surgical site infections. AORN journal, 86(2), 249-258.
Brown, D. Q. (2011). Disposable vs reusable electrocardiography leads in development of and cross-contamination by
resistant bacteria. Critical Care Nurse, 31 (3), 62-68.
Head, C. (2014, June 7-9, 2014). Taking the lead with disposable ECG leads: preventing chest incision surgical site
infections. American Journal of Infection Control, 42, 534.
Horan, T. C., Jarvis, W. R., Mangram, A. J., Pearson, M. L., & Silver, L. C. (1999). Guideline for prevention of surgical
site infection, 1999.
Gummert, J. F., Barten, M. J., Hans, C., Kluge, M., Doll, N., Walther, T., ... Diegeler, A. (2002). Mediastinitis and cardiac
surgery--an updated risk factor analysis in 10,373 consecutive adult patients. Thoracic Cardiovascular Surgery,
41(), 1-5.
Roger, V. L., Go, A. S., Lloyd-Jones, D. M., Adams, R. J., Berry, J. D., Brown, T. M., ... & Wylie-Rosett, J. (2011). Heart
disease and stroke statistics—2011 update a report from the American Heart Association. Circulation, 123(4), e18-
e209.
Singh, K., Anderson, E., & Garrett Harper, J. (2011). Overview and managment of sternal wound infection. Seminars in
Plastic Surgery, 25 (1), 25-33.

Equity
22
Equity Assessment
The #123forEquity Pledge to Act Campaign asks every hospital leader to commit to the following:
Sign the pledge
Take action
Tell others
Information has been sent to hospital CEOs
Upcoming webinars
Data analysis comparing discharge records to census
Scripts to assist hospitals
23
Equity of Care: A Toolkit for Eliminating Health Care Disparities

Equity Assessment
Polling time!
Going Beyond REaL Data Collection: Collecting Social Determinants of Health
HRET Webinar: February 23, 11 a.m. to noon
Click here to register.
24

Qualaris
25

Qualaris Stats
30 hospitals have launched the software
16 hospitals collecting data
14 hospitals launched but not yet collecting data
6 hospitals that have asked for more information, but have not launched
8 hospitals which have opted out of using the tools altogether
85 hospitals which have not contacted us at all
Rolling registration and more information here
26
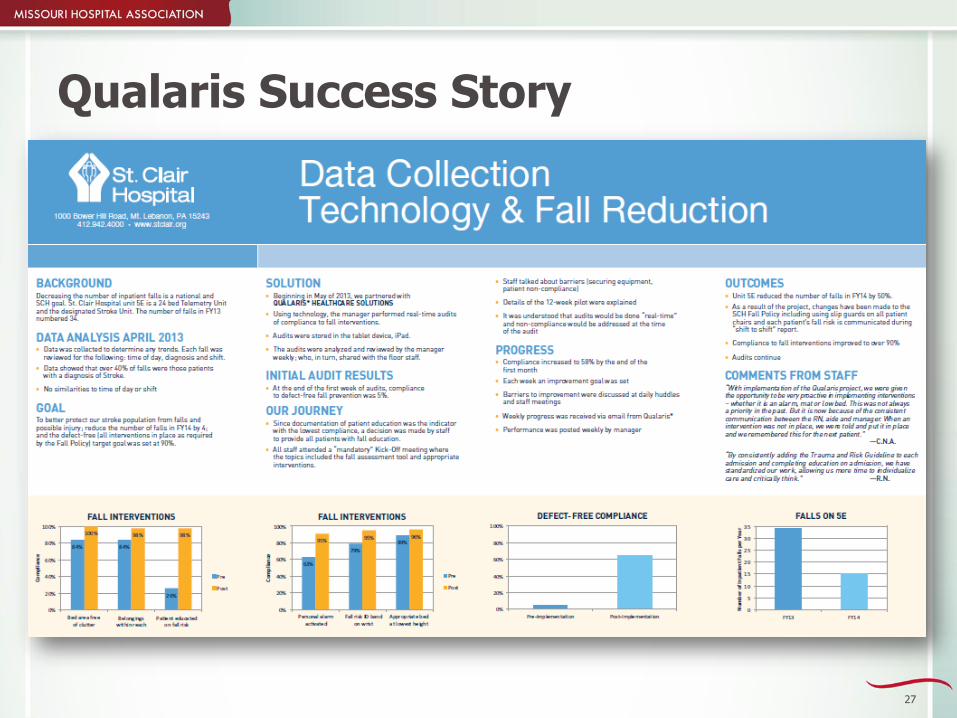
Qualaris Success Story
27

NHSN
28

Confer your NHSN Data to HIDI
60 hospitals have completed this step
Why?
To provide you the most robust data portfolio
To better assist you with more improvement opportunities
See the Instructional Guide
29
Transparency
30

MHA PRICE AND QUALITY TRANSPARENCY INITIATIVE
After months of planning and preparation, the Focus on Hospitals website has now been updated. The public launch of the website went live this morning. Please accept our appreciation for your participation and assistance in refining the data and website.
More than 80 percent of hospitals across the state are participating.
A short video on the website provides a quick explanation of how MHA intends to communicate the site to the public.
If you have questions about the quality data, contact Dana Downing at 573/893-3700, ext. 1314. If you have questions on the price data, contact Mary Becker at 573/893-3700, ext. 1303.
31


Immersion Pilot Project Update
33

Immersion Project Topics
Readmission
CAUTI
Falls
Sepsis
OB Harm
34

Immersion Projects
Kicked off in October
Recruitment phase is closed
In the midst of quarter two tasks
Plan to share your findings, barriers during the webinars
MHA leads per project
Sepsis & Falls – Jessica Rowden
OB, CAUTI, Readmissions – Alison Williams
35

Immersion Project Webinars
36
Quarter Two Wrap Up• March 22, 11-12 – Sepsis Immersion Project webinar• March 22, 1-2 – Falls Immersion Project webinar• March 23, 11-12 – Readmission Immersion Project webinar• March 24, 11-12 – CAUTI Immersion Project webinar• March 24, 1-2 – OB Immersion Project webinar
Quarter Three Wrap Up• June 14, 11-12 – Sepsis Immersion Project webinar• June 14, 1-2 – Falls Immersion Project webinar• June 15, 11-12 – Readmission Immersion Project webinar• June 16, 11-12 – CAUTI Immersion Project webinar• June 16, 1-2 – OB Immersion Project webinar

Methodology
Webinars/shared learning
90-day work cycles
MHA convention
2016
37

HEN 2.0
38
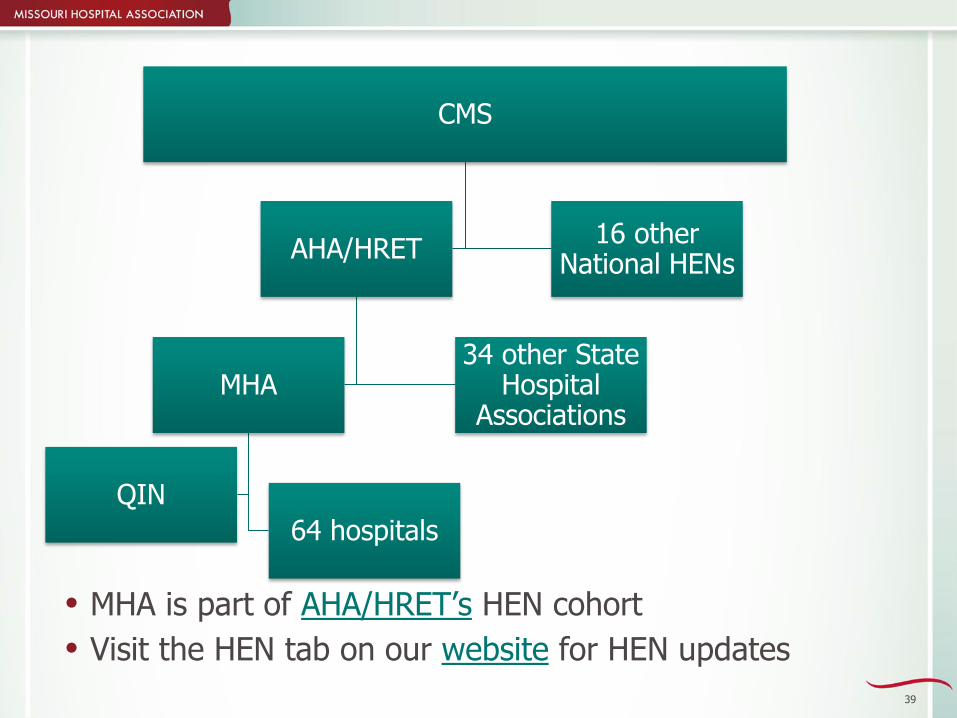
CMS
AHA/HRET
MHA
QIN
64 hospitals
34 other State Hospital
Associations
16 other National HENs
MHA is part of AHA/HRET’s HEN cohort
Visit the HEN tab on our website for HEN updates
39

40
Barton County Memorial Hospital
Bates County Memorial Hospital
Black River Medical Center
Bothwell Regional Health Center
Capital Region Medical Center
Carroll County Memorial Hospital
Cass Regional Medical Center
Cedar County Memorial Hospital
Citizens Memorial Hospital
Community Hospital - Fairfax
Cooper County Memorial Hospital
Des Peres Hospital
Ellett Memorial Hospital
Excelsior Springs Hospital
Fitzgibbon Hospital
Freeman Health System
Freeman Neosho Hospital
Golden Valley Memorial Healthcare
Hannibal Regional Hospital
Harrison County Community Hospital
Hermann Area District Hospital
I-70 Community Hospital
Iron County Medical Center
Lafayette Regional Health Center
Lake Regional Health System
Lee's Summit Medical Center
Liberty Hospital
Madison Medical Center
Mercy Hospital Carthage
Mercy Hospital Joplin
Mercy Hospital Washington
Missouri Delta Medical Center
Mosaic Life Care at St. Joseph
Nevada Regional Medical Center
North Kansas City Hospital
Northeast Regional Medical Center
Northwest Medical Center
Ozarks Medical Center
Perry County Memorial Hospital
Pershing Memorial Hospital
Phelps County Regional Medical Center
Pike County Memorial Hospital
Poplar Bluff Regional Medical Center
Putnam County Memorial Hospital
Ray County Memorial Hospital
Saint Francis Medical Center
Salem Memorial District Hospital
Samaritan Hospital
Scotland County Hospital
Southeast Health Center of Reynolds County
Southeast Health Center of Ripley County
Southeast Health Center of Stoddard County
Southeast Hospital
SSM Health Saint Louis University Hospital
St. Alexius Hospital, Broadway Campus
St. Anthony's Medical Center
St. Mary's Medical Center
Ste. Genevieve County
Sullivan County Memorial Hospital
Texas County Memorial Hospital
University Hospital and Clinics
Twin Rivers Regional Medical Center
Washington County Memorial Hospital
Western Missouri Medical Center

HEN 2.0 Update and Milestones
Baseline data was due January 27
Complete baseline submission earns $2,000
Checks will be mailed out mid-February
Preliminary results = 54 meeting the submission deadline
– THANK YOU!!
NHSN data being validated
Please ensure your hospital submits data on all HEN 2.0 infection rates and utilization ratios of central lines and urinary catheters
Readmission and NHSN baseline data will be sent to HRET before the end of the week
56 site visits completed = 88 percent (exceeding our goal of 70 percent)
41
Data
Monthly monitoring data due to HIDI Quality Collections on the Wednesday before the last Friday of the month for the performance period of the previous month
Example: January data is due February 24th
Next data due date for the evaluation of the Pay-for-Performance stipend will be MARCH 23. Please ensure your data from October 1, 2015 through February 29, 2016 is uploaded
42

Pay for Performance ModelMHA Pay For Performance Model Of Stipend Distribution Based On Improvement And Data Submission
Six Month Milestone
Data submission – to be eligible for performance stipends, Hospital must report data at ≥ 85% of required data submission totals at six months on all preferred, applicable measures
Performance Stipend sliding scale
Hospital achieves 17.6-39% harm reduction for at least 50-74% of the harm topicsand/or achieves 10-19% readmission reduction
$1,500
Hospital achieves ≥40% harm reduction for at least 75-100% of the harm topicsor maintains zero baseline and/or achieves ≥20% readmission reduction
$3,000
Twelve Month Milestone
Data submission – to be eligible for performance stipends, Hospital must report data at ≥ 85% of required data submission totals at twelve months on all preferred, applicable measures
Performance Stipend sliding scale
Hospital achieves 17.6-39% harm reduction for at least 50-74% of the harm topicsand/or achieves 10-19% readmission reduction
$1,500
Hospital achieves ≥40% harm reduction for at least 75-100% of the harm topicsor maintains zero baseline and/or achieves ≥20% readmission reduction
$3,000
$6,000 is maximum pay for performance amount + $2,000 for complete baseline submission = $8,000 per hospital

HRET List-serv
http://www.hret-hen.org/inc/dhtml/listserv.dhtml
Get signed up and start asking your national colleagues questions!

Member Resources and Support
45

Monthly Newsletter
46

Resources
Links
MHA
HIDI Quality Collections and Analytic Advantage
HRET-HEN
Cynosure Health

National Tools and Resources
C Diff change package 2016 update
Hospital Acquired Pressure Ulcer change package 2016 update
Preventable Readmissions change package 2015 update
Severe Sepsis and Septic Shock change package 2016 update
Patient and Family Engagement Compendium
Huddle for Care
HELP! I need to keep my team motivated…
HELP! We have limited resources…
HELP! Our patients aren’t going to follow-up appointments…
HELP! Our patients aren’t motivated to take care of themselves…
48

Upcoming Events
49

MHA Collaboration with Children’s Mercy Hospital
Thursday, Feb. 18, Noon - 1 p.m.Medication SafetyRegister
Thursday, May 19, Noon - 1 p.m.Recruiting Patient AdvocatesRegister
Thursday, Aug. 18, Noon - 1 p.m.Patient Advocate-Policy Design StrategiesRegister
Thursday, Nov. 17, Noon - 1 p.m.Family-Centered RoundsRegister
50

Put us on your calendars!
HEN
Monthly HEN webinars
– Third Wednesday of the month. Noon to 1 p.m. Register for all webinars using this link. Dial 866/450-8659 and use ID# 61279316.
HEN Mid-Project Convening – March 9, Columbia, MO –Hilton Garden Inn Convention Center, Register
MHA
Monthly What’s Up Wednesday
– First Wednesday of the month at noon
– Register for 2016 WUW
51
TeamSTEPPS® in Small and Rural Hospitals AHRQ is hosting a webinar on February 10, 12 to 1 on the strategies and lessons
learned about how to introduce and train small and rural hospitals in TeamSTEPPS® concepts. The webinar, "How to Introduce TeamSTEPPS in Small and Rural Hospitals: The Yellow Brick Road of Teamwork," will feature Kenneth Alexander, vice president at the Louisiana Hospital Association. His presentation will provide insights on engaging hospitals to become interested in TeamSTEPPS, and he will share strategies for working to improve teamwork and communication skills within hospital settings with limited resources. Specifically, the presentation will seek to:
Provide an overview of the work of hospitals within the Louisiana Hospital Association (LHA) to implement with TeamSTEPPS;
Present the need for adapting an approach to introducing a teamwork intervention in small or rural hospitals;
Discuss specific strategies that LHA uses to implement TeamSTEPPS skills and concepts; and
Discuss how these strategies have worked in gaining buy-in and sustainment of teamwork skills in small and rural hospitals.
There is no cost to participate. Click here to register.
52

TeamSTEPPS® to Improve Patient Transfers from the OR to the ICU
AHRQ is hosting a webinar on March 9 from 12 to 1 p.m. CT, on the implementation of TeamSTEPPS® as part of a collaborative effort to improve the triaging of patients from the operating room (OR) to the intensive care unit (ICU). The webinar, "Five hours in the PACU? MetroHealth Uses TeamSTEPPS to Improve Patient Transfer from the OR to ICU," will feature two TeamSTEPPS champions from the MetroHealth System in Cleveland, OH: Joseph F. Golob Jr., M.D., medical director of patient safety and the surgical ICU, and Robert L. Smith, Ph.D., director of medical staff assistance and TeamSTEPPS programs. Their presentation will discuss how the need for the TeamSTEPPS intervention was identified, the role of the electronic health record (EHR) in the implementation effort, and the results of this cross-unit effort. Specifically, the presentation will seek to:1. Describe how MetroHealth used its TeamSTEPPS Action Councils to identify a need for a TeamSTEPPS intervention to improve the triaging of patients from the OR to the ICU;2. Present the collaborative TeamSTEPPS implementation between the OR and ICU;3. Discuss how the implementation efforts were integrated into the EHR; and4. Present the results of the implementation thus far, as well as discuss plans for long-term sustainment.
Register link: https://www.onlineregistrationcenter.com/register.asp?m=347&c=220&usc=march
53

HRET SPONSORED WEBINARSSurgical Site Infection Risk Reduction
February 4, 2016 11 – 12:30 p.m.
Register here https://hret.adobeconnect.com/ssifebruary/event/registration.html
CLABSI Webinar - Nailing CLABSI Prevention!
February 11, 2016 11 – 12:30 p.m.
Register here https://hret.adobeconnect.com/clabsi/event/registration.html
OB Harm Webinar
February 25, 2016 11 – 12:30 p.m.
Register here https://hret.adobeconnect.com/obharm/event/registration.html
Ventilator-associated Events Webinar
March 3, 2016 11 – 12:30 p.m.
Register here https://hret.adobeconnect.com/ventilatorassociatedeventswebinar/event/registration.html
Adverse Drug Events Webinar
March 15, 2016 11 – 12:30 p.m.Register; https://hret.adobeconnect.com/adversedrugeventswebinar/event/registration.html
Readmissions Webinar
March 17, 2016 11 – 12:30 p.m.Register here https://hret.adobeconnect.com/hen20readmissionswebinar/event/registration.html
54

Patient Safety and Quality
Barnes Jewish sponsored: Sixth annual Patient Safety and Quality Symposium: Hardwiring for High Reliability
March 4, 2016, 8 a.m. to 4 p.m., Eric P Newman Education Center, Register
55

Collaboration with the QIO
Join the group for free and get access to more resources!!
56
https://www.tmfqin.org/

New Website!
57

Thank You for Joining Us
Please fill out the evaluation
Be a featured hospital speaker during WUW 2016
See you next month!
March 2 at noon
–Mercy Washington: Partnering with Clinics: Readmission Reduction Strategies
58

Contact Information
Jessica Rowden, MHA, BSN, R.N., CPHQ
Director of Clinical Quality
Missouri Hospital Association
573/893-3700, ext. 1391
59