medical management of nash - university of pittsburgh
TRANSCRIPT

Medical Management of NASH
Jaideep Behari, MD, PhDUPMC Fatty Liver, Obesity and Wellness (UPMC FLOW®) ClinicUPMC Center for Liver DiseasesDivision of Gastroenterology, Hepatology, & NutritionUniversity of Pittsburgh School of Medicine

Overview of the presentation
Part 1: Background and new terminology for 2020
Part 2: Clinical challenges in management
Part 3: A practical framework for clinical management

Part 1
Background and new terminology for 2020

Clinical case
70 year old female had abdominal US for mild self-limited RUQ pain
BMI 31, no DM, dyslipidemia on statin
No alcohol
ALT 35, AST 22
US reports “echogenic liver suggestive of fatty infiltration of the liver”

= Liver
= Kidney
US at initial diagnosis 1 year later after 13% weight loss
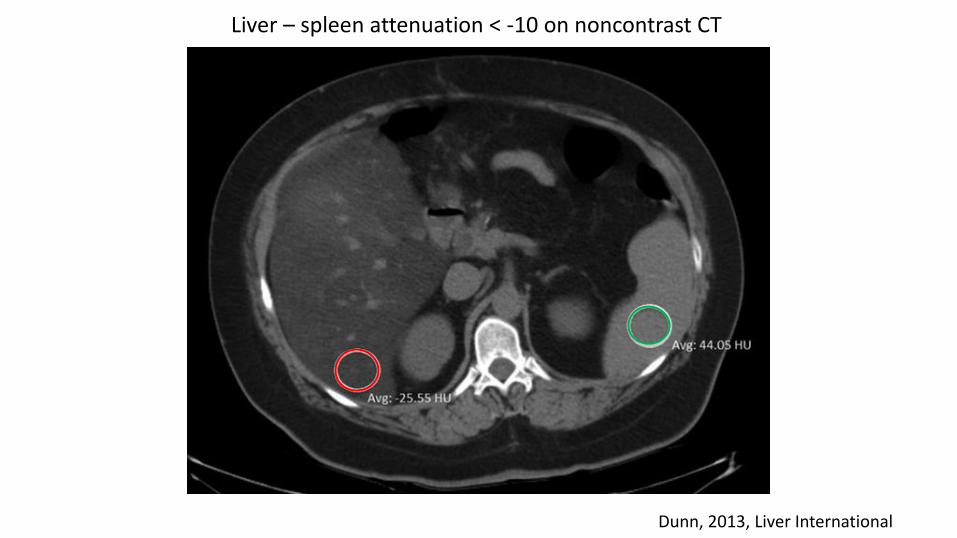
Dunn, 2013, Liver International
Liver – spleen attenuation < -10 on noncontrast CT

Histology of nonalcoholic steatohepatitis (NASH)

NASH is characterized by chicken-wire pattern of liverfibrosis

Natural history of NASHHealthy Nonalcoholic fatty liver Nonalcoholic steatohepatitis (NASH)
NASH with fibrosis NASH Cirrhosis NASH Cirrhosis with HCC

NAFLD is closely associated with inulin resistance and the metabolic syndrome
Siegel 2009

NAFLD has a complex “multihit” pathogenesis involving genetics and multiple organ systems
Mann et al 2016

New terminology for 2020 : “Positive” diagnostic criteria for MAFLD
Eslam et al, J Hepatol, 2020
Liver biopsy not requiredfor diagnosis of “NASH”

MAFLD-associated cirrhosis
Patient with cirrhosis in the absence of typical histology who meet at least oneof the following criteria:
Past or present evidence of metabolic risk factors that meet the criteria to diagnose MAFLD
With at least one of the following:- Documentation of MAFLD on a previous liver biopsy- Historical documentation of steatosis by hepatic imaging
Eslam et al, J Hepatol, 2020

Dual etiology fatty liver disease
Meeting criteria for MAFLD
+
Any other cause of liver disease (alcoholic liver disease*, HCV, HBV etc.)
* > 3 drinks per day in males; >2 drinks per day in females;or binge drinking (>5 drinks in males or >4 drinks in females in 2 hours)
Eslam et al, J Hepatol, 2020

Clinical examples- 54 year old male with BMI 40 and US with hepatic steatosis (MAFLD)
- 34 year old female BMI 24 with dyslipidemia and prediabetes (“Lean” MAFLD) and fatty liver on CT
- 60 year old male with steatohepatitis on biopsy with BMI 33 and 4 alcoholic drinks per day (Dual etiology fatty liver MAFLD + ALD)
- 71 year old female with MRI showing steatotic, nodular liver, BMI 39, T2DM (MAFLD associated cirrhosis)

Part 2
Clinical challenges in the management of NASH (MAFLD)

Prevalence of NAFLD (MAFLD) is increasing worldwide
Younossi et al, 2017, Nat. Rev. Gastroenterol. Hepatol.

First-degree relatives of individuals with NASH-cirrhosis have increased risk of advanced fibrosis
Caussy et al, JCI, 2017

NASH is very common in certain high risk populations
Sanchez, 2015, J Clin Endocrinol Metabol
Obesity T2DM

Most patients in our population have BMI > 25 kg/m2
Dudekula, 2014, PLoS One
924 non-cirrhotic NAFLD patients in CLD

NAFLD can occur in individuals with or without obesityProportion of individuals with NAFLD stratified by country and obesity status
Younossi, Z et al, 2017, Nat. Rev. Gastroenterol. Hepatol.

Due to the high prevalence of NAFLD, the public health burden is huge
Buzzetti et al 2016

Likely low risk of progression
Likely some risk of progression High risk of progression
Liver fibrosis stage is the most important prognostic factor for liver-related outcomes
Fibrosis stage: F0 no fibrosis, F1 mild, F2 moderate, F3 severe, F4 cirrhosis

Liver fibrosis stage is the only histological feature of NASH associated with survival
UPMC Center for Liver Diseases(2007-2017)
Biopsy-proven NASHN = 899 patients
**Clinical challenge:Staging fibrosiswithout a liver biopsy**

There is no FDA approved treatment for NASH (MAFLD)
Source: Clinicaltrials.gov; Accessed August 2019
>200 ongoing clinical studies around the world

Part 3
A practical framework for clinical management

Step 1: Suspect MAFLD in the appropriate clinical setting
Obesity, DM, metabolic syndrome with or without elevated liver enzymes

NASH NASH + Fibrosis
NASH + Cirrhosis
Total NASH No NASH
N 3,820 233 3,139 7,192 11,072,655FIB-4 category
Low (%)Intermediate (%)High (%)
54.434.411.2
53.836.210.0
9.722.867.5
32.928.938.2
63.328.87.9
Is NASH underdiagnosed in the community?
Behari, et al, 2020 Liver Meeting
11 million patients across 7 sites in the Northeast and Midwest US

Step 2: Define the etiology
MAFLD alone
Dual etiology fatty liver (MAFLD + ALD?)
Dual etiology liver disease (MAFLD + AIH?)
Triple etiology fatty liver (MAFLD + ALD + HCV?)

Concurrent etiologies to consider
1. Alcoholic liver disease (very common)
2. Viral hepatitis (common)
3. Autoimmune hepatitis (uncommon)
4. Other causes (hemochromatosis etc.)

Presence of autoantibodies (ANA/ASMA) is not associated with increased risk of NASH/fibrosis
P = ns
Vuppalanchi, Liver Int, 2011

Step 3: Perform non-invasive tests of liver fibrosis to stage disease
1. Point of care (FIB-4, NAFLD Fibrosis Score)
2. Commercial panels (NASH Fibrosure panel)
3. Imaging based (Fibroscan, US elastography, MR elastography)

Serum markers of liver fibrosis in NAFLD have high NPV but low PPV
Test Components AUROC Sensitivity(%)
Specificity(%)
Cutoff Fibrosisstage
NAFLD Fibrosis Score (NFS)
Age, IFG/DM, BMI, Plt, AST/ALT
.81 51 96 -1.45 (low)0.67 (high)
F3/4
FIB-4 Age, AST, plt, ALT .88 26-74 71-98 -1.92 (low)3.25 (high)
F3/4
APRI AST/Plt .67-.94 30 93 .45 (low)1.5 (high)
F2-4
Fibrosure Alpha2 macrogloblulin,haptoglobin, GGT, Total bili, apoliprotein
.81-.92 15-77 77-90 .3 (low)
.7 (high)
F2-4
BARD BMI, AST/ALT ratio, DM
.8 86.8 32.5 2 F3/4
Kawala et al 2016 Dig Sci

FIB-4 score can be used as a simple noninvasive fibrosis assessment tool
<1.45 = High NPV forabsence of advanced fibrosis
>3.25 = 97% specificity foradvanced fibrosis (65%PPV)

Vibration Controlled Transient Elastography (Fibroscan®) is very useful for point-of-care risk stratification
•CAP: Assessment of liver fat (dB/m)
35
Image source: Echosens
Eddowes, Gastroenterol, 2019
LSM: Assessment of liver fibrosis (kPa)
Steatosis cutoff: 274 dB/m for grade ≥1 steatosis [sensitivity
of .90 (95% CI
.87-.93)]
Fibrosis: liver stiffness
measurement cutoff values of 8.2 kPa for ≥F2, 9.7 kPa for
≥F3 and 13.6 kPa for F4.

Ultrasound Shear Wave Elastography is available for noninvasive fibrosis assessment
Image source: GE Healthcare
36

MR Elastography and proton density fat fraction (PDFF) can accurately measure liver fibrosis and steatosis
Venkatesh et al 2013 J Magn Reson Imaging
MRI-PDFF Proton density fat fraction for steatosis determination

Noninvasive approaches to fibrosis assessment can avoid liver biopsy in a large percentage of patients
Furlan, 2020, Am J Roent.
35 year old maleFIB-4: <1.45
5.7 kPa 2.35 kPa

Proposed simplified diagnostic workflow for MAFLDM: ALT>30; F > 19
Repeat labs; Risk factors
Alcohol history, HBsAg, HCV Ab, ferritin/iron sat, ANA, ASMA, ASMA, AIAT level, ceruloplasmin
Treat as appropriateAbd US echobright
Liver screen negative
Abd US normalLiver screen negative
NAFLD
NAFLD Fibrosis scoreVCTE/FibroscanLow risk:
NFS<-1.455 (NPV 93%)VCTE < 5 kPa*
IndeterminateNFS -1.455-0.676
VCTE 7-12.5*OR Discordant NFS/VCTE
High riskNFS > 0.676 (PPV 90%)VCTE > 12.5 (+/-1) kPa*
<-2.5<5 kPa
-1.45 to -2.55-7 kPa
Alternate diagnosis?Mild steatosis?
PCP follow up/3 years
Reassess in 1 yearLifestyle mod.
Manage as cirrhosis
Liver biopsyTreat if F2-3 fibrosis

Simplified algorithm for risk stratification in NASH
NAFLD
FIB-4 VCTE or SWE+
BOTH CONCORDANT FOR LOW RISK<1.45 / < 7 kPa
BOTH CONCORDANT FOR HIGH RISK>3.25 / >15 kPa
MRE + PDFF
DISCORDANT RESULTS OR BOTH CONCORDANT FOR MODERATE RISK
1.5-3 / 7-15 kPa
Liver biopsy

Step 4: Manage based on risk stratified MAFLD disease stage
Adapted from Rinella and Sanyal, Nat Rev Gastroenterol Hep, 2016

Step 5: Focus on lifestyle modification for all MAFLD disease stages
• Diet quality
• Smoking cessation
• Alcohol cessation
• Physical activity
• Weight management

There is limited data on optimal dietary advice for patients with MAFLD
Zivkovic, 2007, Am J Clin Nutr; Musso, 2009, Am J Clin Nutr; Ryan, 2013, J Hepatol;Harrison, 2009, Hepatology; Molloy, 2012, Hepatology
• The best diet to treat NAFLD is unknown (high protein diet?)• >5% weight loss improves steatosis• >7-9% weight loss improves histology in NASH• Avoid saturated fats, sugary drinks, simple carbohydrates
(fructose)• A Mediterranean diet (monounsaturated fatty acids-rich) improves
hepatic steatosis and insulin sensitivity• Coffee consumption is associated with reduced risk of fibrosis in
NASH patients

Coffee consumption is associated with reduction in risk of fibrosis in MAFLD patients
Molloy et al, Hepatology, 2011

Weight loss is an effective treatment for MAFLD but difficult to achieve for most patients
Romero-Gomez, J Hepatol, 2017

Weight loss is associated with improved liver histology in MAFLD
Promrat, 2010, Hepatology

Bariatric surgery can improve fat, inflammation and fibrosis in patients with severe obesity
Lassailly, 2015, Gastroenterology
NASH grade Fibrosis stage
82 patients at 1 year after surgery
Premature to consider weight loss surgery solely for NASH but can be considered if otherwise indicated (caution if cirrhosis/portal hypertension)

250 min/week of moderate exercise with weight loss may be optimal for improvement of MAFLD
Oh, 2015, Hepatology

Lifestyle modification is effective for MAFLD at any disease stage
10/2017 8/2019

Step 6: Consider liver-directed pharmacotherapy for moderate to severe fibrosis
Cusi, 2018, Ann Int MedSanyal, 2010, NEJM
Vitamin E800 I.U. daily
Pioglitazone45 mg daily
Non-diabeticNon-cirrhotic
Non-diabetic or diabeticNon-cirrhotic
GLP-1 RA?SGLT2 inhibitors?

There are over 200 ongoing clinical trials for MAFLD around the world
Source: Clinicaltrials.gov; Accessed August 2019

Clinical trials are taking three main approaches to treating MAFLD
Fat accumulation → Liver cell injury → Cell death → Fibrosis
UPMC FLOW clinic =9 MAFLD clinical trialsF1 to F4 fibrosis

Step 7: Manage MAFLD associated comorbid metabolic problems
• T2DM
• Hypertension
• Dyslipidemia
• OSA
• Cardiovascular risk reduction

Statins are safe and should not be withheld if indicated in MAFLD
- MAFLD patients are at high risk for CVS morbidity and mortality
- Aggressive CVD risk modification should be considered for all MAFLD patients
- MAFLD patient are not at high risk from statins and they can be used for dyslipidemia
- Avoid in decompensated cirrhosis
AASLD NAFLD Guidance

Patients with NASH-cirrhosis and diabetes should continue metformin after cirrhosis diagnosis
Zhang, 2014, Hepatology

Step 8: Screen for HCC and varices in MAFLD-associated cirrhosis / advanced fibrosis
Mittal et al, Clin Gastroenterol Hepatol, 2019
Proportion of HCC patients with or without evidence of cirrhosis by risk factor

Summary and conclusions• NAFLD/NASH is very commonly encountered in
clinical practice• The new definition of MAFLD enables a “positive”
diagnosis of fatty liver• Diagnosis, staging and management of MAFLD
remains challenging• A step-wise approach to risk stratification and
management can enable effective management