medical imaging of neglected tropical diseases of the … · eases are especially prominent with...
TRANSCRIPT

393
CEDirected Reading
This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference.
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Neglected tropical diseases (NTDs) are a group of protozo-an, parasitic, bacterial, and viral diseases that are endemic in 149
countries and cause substantial illness for more than 1.4 billion people globally.1 They are called neglected diseases because they have been largely eradicated in more developed parts of the world and persist only in the poorest, most margin-alized communities and conflict areas. These diseases are contrasted with HIV/AIDS, tuberculosis, and malaria, which generally receive greater treatment and research funding. One hundred per-cent of low-income countries are affected by at least 5 NTDs simultaneously.1
In endemic countries, NTDs cause impaired physical and cognitive devel-opment as well as illness and death, killing an estimated 534 000 people worldwide every year.1 Furthermore, individuals often are aff licted with more than one parasite or infection at a time. Subsequently, related morbidity and mortality, as well as contamina-tion of potential farmland, results in
difficulty earning a living and limited productivity in the workplace. These conditions trap the poor in a cycle of poverty and disease and cost develop-ing economies billions of dollars annu-ally. It is especially difficult to rational-ize neglecting these conditions consid-ering that the treatment cost for most NTDs mass drug administration pro-grams is estimated at less than $0.50 per person per year. The World Health Organization (WHO) has prioritized 17 NTDs, and in May 2013, the 66th World Health Assembly adopted reso-lution WHA66.12 that calls for intensi-fied, integrated measures and planned investments to improve the health and social well-being of populations affected by NTDs. WHO also has been working with member states to ensure implementation of the resolution.2
Impact in the AmericasThe Americas comprise North
America, Central America, and South America. The phrase “Latin American and Caribbean region” can be used to
After completing this article, the reader should be able to:Define the term neglected tropical disease and discuss international interest in these
conditions. Discuss neglected tropical diseases affecting the Americas including their pathophysiol-
ogy, clinical manifestations, radiologic signs, diagnosis, and treatment.Describe the need for the medical community to actively prevent continued spread of
neglected tropical diseases within resource-limited communities.
Neglected tropical diseases are a group of protozoan, parasitic, bacterial, and viral diseases endemic in 149 countries causing substantial illness globally. Extreme poverty and warm tropical climates are the 2 most potent forces promoting the spread of neglected tropical diseases. These forces are prevalent in Central and South America, as well as the U.S. Gulf Coast. Advanced cases often require specialized medical imaging for diagnosis, disease staging, and follow-up. This article offers a review of epidemiology, pathophysiology, clinical manifestations, diagnosis (with special attention to medical imaging), and treatment of neglected tropical diseases specific to the Americas.
Patrick Jones, BS, R.T.(R)Jonathan Mazal, MS, R.R.A., R.T.(R)(MR)
Medical Imaging of Neglected Tropical Diseases of the Americas
394
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
(Tamaulipas, Veracruz, Tabasco, Campeche, Yucatan, and Quintana Roo) and in Chiapas and Oaxaca on the southern Pacific coast. Mosquito-borne dis-eases are especially prominent with dengue incidence rates increasing approximately 8-fold from 2000 to 2011, with peaks occurring in 2002, 2007, and 2009 (see Table 1).11
Extreme poverty and warm tropical climates are the 2 most potent forces promoting the endemicity of NTDs, and these same forces are widely prevalent in the 5 states bordering the U.S. Gulf Coast: Texas, Louisiana, Mississippi, Alabama, and Florida, with 10 million Gulf Coast residents living below the U.S. poverty line.13 Thus, today the Gulf Coast is considered North America’s most vulnerable and impoverished region14,15 with high rates of NTDs emerging there (see Table 2).15 In fact, the term emerging should be used with caution because many of these NTDs are not new to the region.16 Outbreaks of dengue were reported in Texas from 2003-2005, with a return of the disease in late 2013 affecting the poorest communi-ties.17-19 In addition, dengue was reported in Florida in 2009 and 2010.20 The U.S. Gulf Coast also is consid-ered vulnerable to the introduction of chikungunya, a virus transmitted by Aedes mosquitoes that clinically resembles dengue, with the possibility of year-round transmission in the warm Gulf climate.21 Chagas dis-ease transmission also has been confirmed in Texas and Louisiana,6,15,22 and a recent economic analysis revealed that Chagas disease already incurs nearly $900 million in costs in the United States.23
Some urgent needs in addressing NTDs include spe-cific recommendations for greatly expanded disease sur-veillance and understanding of disease transmission.15,24,25 For many NTDs, diagnostic tests are cumbersome or not widely available. One example is the lack of access to radi-ology services. Many advanced cases require specialized medical imaging, and affected individuals must travel to specialty clinics situated in more affluent communities, a journey that often is not feasible.26 As of 1997, when data was last collected, more than half of rural hospitals in Latin America did not offer radiology services.27 For this reason, a lack of awareness exists among health profes-sionals regarding tropical disease management including identification of radiologic manifestations.
identify all countries within the Western Hemisphere and south of the United States (see Figure 1).
The Latin American and Caribbean region has a population of almost 600 million people,3 of whom an estimated 99 million live on less than $2 per day.4 Approximately 10% of the region’s extremely poor live in Bolivia, Ecuador, Nicaragua, and Venezuela.5 NTDs are common wherever poverty is pervasive, and these 4 countries carry approximately 14% to 15% of regional cases of Chagas disease, cutaneous leishmaniasis, den-gue, and intestinal helminth infections.6-10 Bolivia leads in the number of Chagas disease cases (620 000) and the number of children who require deworming for intestinal helminth infections (3.4 million), whereas Nicaragua leads in cutaneous leishmaniasis cases (9000-14 800), and Venezuela has the largest number of dengue cases (3.5 million).6-8 Although Cuba is bet-ter off economically, it also has many cases of dengue and intestinal helminth infections.8-10 NTDs also are widespread along the Gulf Coast states of Mexico
Figure 1. Map of the Western Hemisphere with Latin American and Caribbean regions in blue. Image courtesy of Heraldry via Wikimedia Commons. Licensed under the Creative Commons Attribution-Share Alike 3.0 Unported license.
395
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
in Chagas disease becoming a health care concern in Europe and the United States as well. Furthermore, 2015 estimates from WHO indicate that 6 million to 7 million people are infected worldwide.28
PathophysiologyThe pathophysiology of Chagas disease is not entire-
ly known. Sometimes referred to as the kissing bug, tri-atomine bugs transmit the T cruzi parasite when insect feces enter an individual through an insect bite or skin
Chagas DiseaseEpidemiology
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by triatomine bugs.28 Chagas disease is recognized as one of the major health problems in almost every Central and South American country. Once a rural disease, Chagas disease has become an urban phenomenon as a result of socio-economic changes, rural exodus, deforestation, and urbanization. Increases in immigration have resulted
Table 1
Ranking of Neglected Tropical Diseases in Latin American Countries by Prevalence and Distribution12
DiseasePopulation Currently Infected in LAC
Population at Risk in LAC
Main Vulnerable Populations or Geographic Areas
No. of LAC Countries Infected
Percentage of LAC Population Infected (% Poor People Infected)
Percent Global Disease Burden in LAC
Trichuriasis 100 million 523 million Poor rural & urban slums
27 17.8 (46.9) 16.6
Ascariasis 84 million 514 million Poor rural & urban slums
27 15.0 (39.4) 10.4
Hookworm 50 million 346 million Poor rural 26 8.9 (23.5) 8.7
Chagas disease 8 million-9 million 25 million- 90 million
Poor rural & urban slums
13 1.6 (4.1) 99.8
Schistosomiasis 1.8 million 36 million Poor rural 4 with 1000 cases
0.3 (0.8) 0.9
Blinding trachoma
1.1 million ND Poor rural 3 0.2 (0.5) 1.3
Lymphatic filariasis
720 000 8.9 million Poor rural & urban slums
7 0.1 (0.3) 0.6
Dengue 552 141 reported in 2006
ND Urban slums 23 0.1 (0.2) ND
Cysticercosis 400 000 75 million Poor rural 15 0.1 (0.2) ND
Cutaneous (CL) and visceral (VL) leishmaniasis
62 000 CL5000 VL
ND Poor rural & urban slums
18 ND ND
Leprosy 47 612 new cases ND Poor rural & urban slums
22 0.1 ( 0.1) 11.4
Onchocerciasis 64 new cases in 2004 515 675 Poor rural 6 0.1 ( 0.1) 0.3
Jungle yellow fever
86 new cases in 2004 ND Jungle & urban slums
4 0.1 ( 0.1) 0.1
Abbreviation: LAC, Latin American Countries; ND, not determined.

396
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
partial or absent relaxation of the lower esophageal sphincter occuring simultaneously.29 In the late stages of the disease, patients begin to experience megaesopha-gus and megacolon involving damage to submucosal layers and the mesenteric nerve plexus. As a result, megacolon patients can present with severe constipa-tion for periods of 60 days or longer.30 Chagas disease often affects the heart, resulting in epicardial ventricu-lar tachycardia,31 which can lead to sudden death.
DiagnosisGastrointestinal and cardiac symptoms accompa-
nied with recent travel to Latin America would be sug-gestive of Chagas disease. Physical examination should identify one of the following disease phases32: ■ Acute, nonspecific symptoms.■ Asymptomatic and a significant chronic cardiac
disease.■ Formation of digestive megaesophagus or mega-
colon. To confirm diagnosis, laboratory tests might include
enzyme-linked immunosorbent assay (ELISA) serology testing, a technique that uses the absorption of antibod-ies by insoluble preparations of antigens. Another option for infectious disease diagnosis is polymerase chain reac-tion assays that amplify a few copies of a piece of DNA across several orders of magnitude.33 In addition, histo-logic studies show that when host cells within parasitized
defect. Body parts particularly vulnerable to parasitic transmission are the mucous membranes of the eyes or mouth. Other routes of infection include consumption of contaminated water or food, blood transfusions, and organ transplantation.
Clinical ManifestationsPatients with acute Chagas disease usually have
characteristic inflammatory lesions at the site of T cruzi entry called chagomas. Other early signs of the disease include fever, headache, enlarged lymph glands, pallor, muscle pain, difficulty breathing, abdominal or chest pain, and purplish swelling of one eyelid called Romaña sign (see Figure 2).28 As the disease progresses, the 3 organs predominantly affected are the esophagus, colon, and heart. Dysphagia is the most common diges-tive symptom and results from abnormalities of esopha-geal motility with esophageal muscle contractions and
Table 2
Main NTDs Affecting the Gulf of Mexico16
Disease
Current Status in United Statesa
Current Status in Mexicoa
Vector-borne NTDs
Vivax malaria Nonendemic Endemic
Dengue Emerging Endemic
West Nile virus infection Endemic Emerging
Chagas disease Endemic Endemic
Cutaneous leishmaniasis Emerging Endemic
Rickettsial infections Endemic Endemic
Helminthic NTDs
Soil-transmitted helminth infections
Not determined Endemic
Cysticercosis Endemic Endemic
Toxocariasis Endemic Endemic
Fascioliasis Nonendemic Endemic
Other NTDs
Intestinal protozoan infections
Endemic Endemic
Leptospirosis Sporadic or emerging EmergingaEndemic is defined as being regularly found among a particular people or in a certain area.
Figure 2. Romaña sign. Reprinted from Parasites – American Trypanosomiasis (also known as Chagas disease). Centers for Disease Control and Prevention Web site. http://www.cdc.gov /parasites/chagas/. Updated July 19, 2013. Accessed April 9, 2015. Image courtesy of WHO/TDR.
397
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
tissue rupture, trypomastigotes (a developmental stage of T cruzi) are released and often can be detected by micro-scopic examination of anticoagulated blood.34
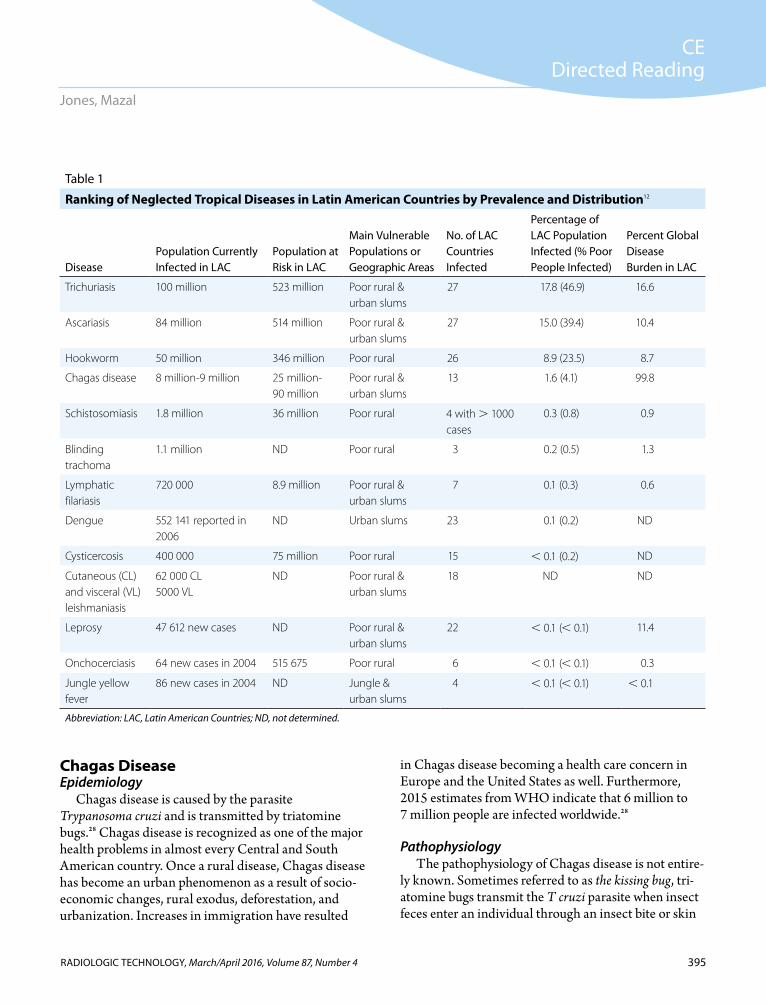
Dysphagia studies using f luoroscopy can exhibit a measurable delay in digestive and swallowing move-ments as compared to normal esophageal motility. These delays can affect the upper esophageal sphincter and various stages of the swallowing process including oropharyngeal transit, pharyngeal transit, and pharyn-geal clearance.34 Approximately 7% of Chagas disease patients with megaesophagus develop esophageal cancer (see Figure 3). Computed tomography (CT) can demonstrate the extent of such tumors, detecting mediastinal and nodal involvement, and it can be used to confirm cases of mediastinitis and esophageal perfo-ration.35
Chest radiography is an important and inexpensive tool used to identify patients with dilated cardiomyopa-thy secondary to Chagas disease. Calcifications in the apical vasculature often are a radiologic manifestation of this condition.33 CT, as well as ultrasonography, mag-netic resonance (MR) imaging, scintigraphy, and angi-ography, enable evaluation of infarcts resulting from chronic Chagas heart disease.35 When advanced imag-ing capabilities are available, noncontrast multidetector electrocardiography-gated CT scanning for calcium scoring is the protocol of choice, followed by contrast-enhanced CT coronary angiography for examining Chagas disease–associated infectious myocarditis.36
Cardiac MR imaging studies have shown that both myocardial fibrosis and segmental cardiac wall motion abnormalities were associated with ventricular arrhyth-mia in patients with chronic Chagas heart disease. Even in patients with this condition who have preserved or minimally impaired ventricular function, the arrhyth-mogenic substrate can be present. Myocardial fibrosis detected on cardiac MR is the most important variable associated with ventricular arrhythmia.37
TreatmentChagas disease is curable if treated in the acute
phase.32 Surgery is a treatment option for megacolon secondary to the disease and can consist of either the Duhamel-Haddad or the Habr-Gama procedures, which result in similar final configurations involving
Figure 3. Anterolateral (A) and lateral (B) chest projections showing megaesophagus as a result of Chagas disease in a man with development of cancer in the distal third of the esophagus with perforation forming a large abscess that extends into the right lower lobe and pleural space. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases/tmcr/chapter4/esopha gus6.htm. Accessed December 17, 2015.
A
B

398
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
bloodstream, providing access to the liver, eyes, cen-tral nervous system, and striated muscle, where they develop into cysticerci, larval tapeworms enclosed within a sac. Pigs with cysticercosis become inter-mediate hosts, and the disease lifecycle is completed when undercooked pork infected with cysts is con-sumed by humans.43,44 After cysts are ingested by humans, the scolex, or tapeworm head, turns inside out, attaches to the intestinal wall, and in 2 months matures into a 2-m to 4-m ribbon-like tapeworm.
Cysticercosis infections usually cluster around tape-worm carriers, meaning person-to-person spreading of the disease is likely to be the predominant means of human contamination vs contamination through envi-ronmental sources.45-47 Individuals infected with tape-worms spread T solium eggs indirectly through poor hygiene practices such as lack of hand washing and con-taminated food, water, or surfaces. Affected individuals can be reinfected with larvae produced by tapeworms already in the body.
Clinical ManifestationsAcute cysticercosis outside of the central nervous
system usually is not associated with clinical manifesta-tions, with the exceptions of ocular involvement and rare cases of massive muscular involvement. It can be months or years after initial infection before symptoms of chronic infection manifest, and these symptoms are dependent on the location and number of cysts in the body. When the cysts die, the surrounding tissue swells, increasing pressure and inducing symptoms. Cysts in muscle tissue might develop into palpable, sometimes tender, subcutaneous masses. Cysts in the eyes can f loat in the vitreous humor, disturbing vision and potentially swelling, causing detachment of the retina. Recurrent seizures occur in approximately 80% of symptomatic cases of neurocysticercosis, making epilepsy the most common neurologic manifestation48 and neurocysti-cercosis one of the most important causes of seizures in the world.49 Other neurologic symptoms include focal deficits (16%), increased intracranial pressure (12%), and cognitive decline (5%).48 In fact, neurocysticercosis is regarded as “the great imitator” because it can mimic almost any neurological disorder including isolated headaches, stroke, or involuntary movement.43,50-52
rectalsigmoidectomies of all, or almost all, of the dyski-netic rectum.38 Most patients with Chagas disease have some form of heart disease, and this must be considered when determining the level of risk in surgical interven-tion.32
To cure patients of parasitemia from Chagas disease, the prescribed medication is either benznidazole or nifurtimox. These 2 medications destroy the T cruzi par-asite.39 In the United States, these antiprotozoal agents are not U.S. Food and Drug Administration approved and are available only from the Centers for Disease Control and Prevention (CDC) under investigational protocols.40 The main contraindications to these treat-ment options are pregnancy, neurologic and psychiatric conditions, and existing kidney or liver failure.
Preventive measures involve spraying insecticides and improving housing to increase hygienic living con-ditions because no vaccination solutions are available for Chagas disease.41
Cysticercosis Epidemiology
Cysticercosis is an infection caused by a helminth (par-asitic worm), specifically the tapeworm, Taenia solium. It is found worldwide and is endemic in most Latin American countries, most often in rural areas where hygiene prac-tices are poor. As a result of increasing immigration, num-bers of patients with cysticercosis are rising in countries where local transmission typically is low. The prevalence of neurocysticercosis, which occurs when larvae reach the brain, is 0.2 to 0.6 per 100 000 inhabitants in some western states of the United States, and it is diagnosed in more than 2% of patients visiting emergency departments for seizures.42
PathophysiologyTaenia solium has a 2-host life cycle between
humans and pigs. Only humans can serve as a host for adult tapeworms, whereas both pigs and humans can serve as intermediate hosts for the larval form. Oncospheres, or tapeworm embryos, are passed to the environment in human feces, which in settings of poor sanitation and free-roaming animals can be ingested by pigs. After ingestion, the embryos hatch and actively cross the intestinal mucosa to the

399
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
pathognomonic millet seed-shaped elliptical calcifica-tions in soft tissue described on radiography.55
In regions where CT and MR are available, these scans can provide information on the morphology and localization of cysticercosis cysts, burden of infection, stage of the cysts, and surrounding inflammation. The appearance of parenchymal brain lesions on neuroimag-ing indicates their stage of shrinkage and can be used to monitor the effectiveness of treatment regimens. Live vesicular cysts are small, rounded lesions with little or no pericystic edema; they do not enhance with con-trast. The cysts frequently show the tapeworm scolex as an internal asymmetric nodule (ie, a hole-with-dot), and several viable cysts showing scolices confirm the diagnosis. Calcified cysticerci are clearly visible on CT as nonenhancing hyperdense nodules, also without peripheral edema. The degenerative process becomes apparent when colloid cysts with poorly defined borders are surrounded by edema and show a marked ring or nodular contrast enhancement. MR diffusion-weighted
DiagnosisHistological confirmation of the parasite is not
possible in most neurocysticercosis cases because of complications from inflammatory response or effects of prior medications. Diagnosis usually is based on neuroimaging and confirmed by serological testing via enzyme-linked immunoelectrotransfer blot assays, which use lentil-lectin purified glycoprotein antigens to detect T solium antibodies. Enzyme-linked immu-noelectrotransfer blot sensitivity is approximately 98%, meaning patients with more than one viable cyst will have a positive serology, and a negative serology result should lead to investigation of alternative diagnoses.53 Detection of anticysticercal antibodies in the cerebral spinal f luid by ELISA is 89% sensitive and 93% specific in patients with viable neurocysticercosis infections and is used when enzyme-linked immunoelectrotransfer blot is not available.54 Antibodies to T solium frequently are reported in the asymptomatic general population in endemic regions, suggesting prior or current exposure to the parasite.
Radiologic confirmation of cysticercosis can be com-pleted with radiography or ultrasonography, although it typically is limited to late disease identification when cysticerci are more distinguishable. Soft tissue radiog-raphy commonly demonstrates multiple (often several hundred) calcifications. These calcifications appear either linear or oval and measure 4 mm to 10 mm or more in length and 2 mm to 5 mm in width. Moreover, calcified cysts have their long axes in the plane of the surrounding muscle bundle (see Figure 4).
On chest radiography, cysticerci might be seen in the lungs with measurements of about 3 mm to 6 mm in diameter. The outer shells of the lesions are calcified, with somewhat lighter and softer centers, and remain more rounded when compared with the oval calcified cysts found in muscle.35
Ultrasonography is particularly useful in examin-ing cysticercosis of the eye and extraocular muscles. In examinations of the orbit, as well as other soft tissue and musculoskeletal structures, the primary diagnostic features are oval or round well-defined cystic lesions with an eccentric echogenic scolex within them. In cases of calcified cysticercosis, ultrasonography demon-strates multiple calcifications in soft tissue similar to the
Figure 4. Cysticercosis of the lower extremity. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www .isradiology.org/tropical_deseases/tmcr/chapter7/clinical2a.htm. Accessed December 17, 2015.

400
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
f latworm infection in the world,63 affecting more than 1 million people and costing $3 billion annually in clinical treatments and livestock compensation.64 The disease has 2 predominant forms: alveolar and cystic. Alveolar echinococcosis is not commonly found in the Americas, whereas cystic echinococcosis can be found in Central America, South America, and in rare cases, North America.
PathophysiologyCystic echinococcosis is zoonotic (ie, transmissible
from vertebrate animals to humans),65 and the trans-mission cycle begins when dogs eat meat infected with cysts that grow into adult tapeworms (Echinococcus granulosus). The dogs eventually shed tapeworm eggs in their feces, contaminating the soil. Sheep subse-quently consume the eggs and develop parasitic larva in their viscera. The cycle affects humans when they consume water or food that has been contaminated by dog fecal matter,64 thus sheep farmers are more likely to develop hydatidosis because their f lock often acts as
imaging and apparent diffusion coefficient maps might allow visualization of the scolex in colloidal cysticerci, which are seldom visible on CT or conventional MR sequences.56,57 In rare cases in which a solitary degener-ating cyst is present, misleading differential diagnoses can lead to unnecessary biopsies. For example, neuro-cysticercosis and tuberculosis often are encountered in low-income regions of the world and have some similar clinical and radiological features. Thus, diagnostic cri-teria have been validated to differentiate these entities in patients with one brain nodule on the basis of size, edema, and clinical presentation (see Figure 5).58
TreatmentTherapy can include symptomatic therapy, antipara-
sitic treatment, or surgery (eg, lesion resection or shunt placement) and often requires a combination of these options. Advantages of medical therapy include treat-ing surgically unreachable and multifocal cysticercosis. Therapy planning depends on proper characterization of the neurocysticercosis type, location, and level of brain involvement. Surgery is considered only when a diagnosis is in doubt or the infection is clinically pro-gressive.43
The International Task Force for Disease Eradication has targeted T solium infection for focal elimination and eventual eradication.59 Furthermore, field control efforts have been attempted since 1987 in Latin American countries including Ecuador, Mexico, Peru, Guatemala, and Honduras.60,61 Preventive mea-sures recommended by the CDC include good hand washing hygiene using soap and warm water after bath-room use and changing diapers and before handling food. Proper food and water consumption practices involve washing and peeling all raw vegetables and fruits before eating, drinking only bottled or boiled water and bottled drinks, and filtering and dissolving iodine tablets into water when traveling within devel-oping countries.44
Echinococcosis Epidemiology
One of the oldest known diseases is hydatid disease, also called human cystic echinococcosis.62 Today, this par-asitic disease is the most serious and widespread human
Figure 5. Computed tomography imaging of human neurocysti-cercosis. A. Viable cysts. B. Enhancing nodule. C. Brain calcifica-tions. D. Parenchymal neurocysticercosis. E. Basal subarachnoid neurocysticercosis. F. Intraventricular cysticercosis. Reprinted from The Lancet Neurology, Vol. 13. Garcia HH, Nash, TE, Del Brutto OH. Clinical symptoms, diagnosis, and treatment of neurocysticercosis. 1212-1215. Copyright 2014, with permission from Elsevier.
A
D
B
E
C
F
401
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
Ultrasonography can provide multiple imaging planes for optimized diagnosis of hydatid cysts. Used exclusively or in combination with laboratory tests, radiography and ultrasonography can allow for an almost 100% positive diagnosis of hydatid disease in the majority of cases.35 Using ultrasonography, cysts initially were categorized via the Gharbi classification in 1981, a system widely used but in modified forms. The Gharbi classification is as follows35,65,69: Type I – pure f luid collection. Type II – f luid collection with a split wall. Type III – f luid collection with septa. Type IV – heterogeneous echo patterns. Type V – reflecting thick walls.
The cyst classification process also was dependent on information related to the size, number, and localization of the cysts and any associated complications.65 In 2003, WHO proposed a standardized classification based on the active-transitional-inactive cyst status as indicated by ultrasonography (see Table 3).70
Contrast-enhanced CT (CECT) also is an effec-tive modality for diagnosing cystic echinococcosis. The “air bubble” sign, caused by air trapped within a cyst, can provide significant statistical results (85.7%
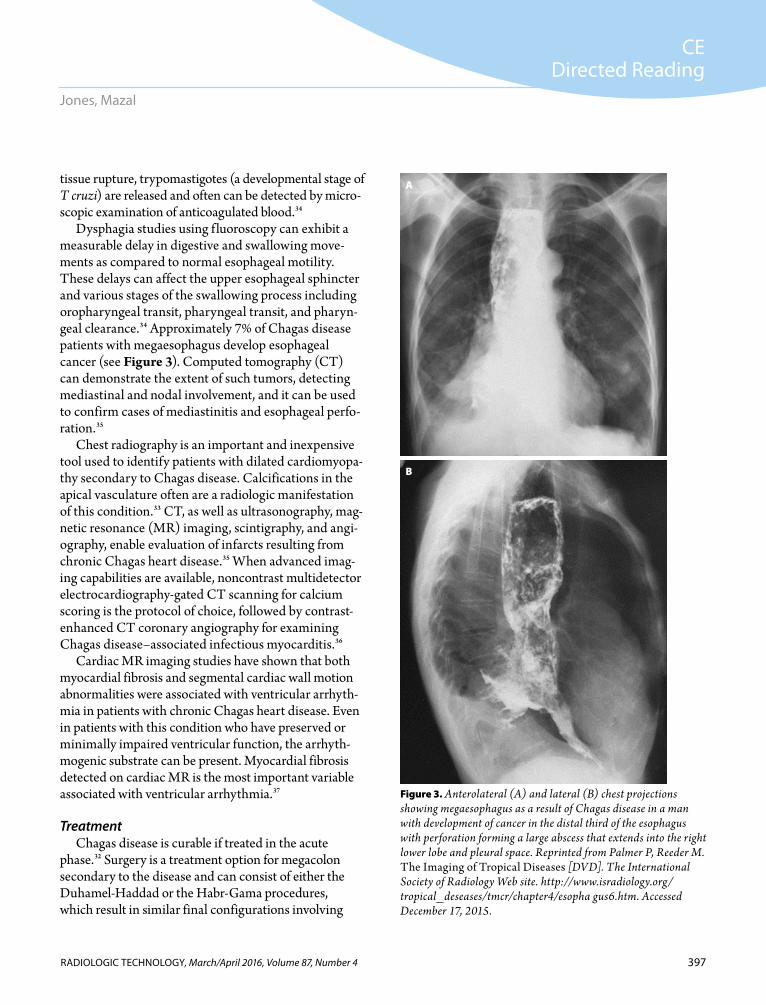
an intermediate host. The risk of farm ani-mal infection is high in these environments because E granulosus eggs can remain viable for up to a year.66 Once ingested by humans, the eggs enter a larval stage resulting in hyda-tid, or larval, cyst formation (see Figure 6).
Clinical Manifestations
Infected individuals often are asymp-tomatic until the hydatid cysts grow large enough to cause discomfort, pain, nausea, and vomiting. The cysts will grow for several years before reaching maturity, and symptom development depends on the cysts’ location. A majority (50%-70%) develop in the liver,65 but they also can occur in the lungs, spleen, kidneys, heart, eyes, and skeletal and central nervous systems. Trauma to an infected person can result in cyst rupture causing cystic f luid and daughter cysts to be released into sur-rounding tissues, potentially exerting pressure on adjacent organs. When this happens, patients might have a high fever and become severely ill. They might also experience anaphylaxis, demonstrat-ed by a range of complications from urticaria (hives) to life-threatening circulatory shock.67
Diagnosis A patient presenting with a cyst-like mass and a his-
tory of recent exposure to sheepdogs while in an area in which E granulosus is endemic is suggestive of cystic echi-nococcosis. Laboratory tests such as indirect fluorescent antibody, immunoelectrophoresis, ELISA serology, and radioallergosorbent tests can confirm diagnosis.35,68
In most instances, radiography is used for initial screening. In positive cases, an unruptured hydatid cyst in the lung presents as a homogenous round or oval-shaped mass with smooth borders surrounded by healthy lung tissue. Many times this will be an incidental finding, with the radiography ordered for an unrelated condition. Ruptured cysts are more common in lung tissue than liver tissue because of a higher incidence of bronchial rather than biliary patency through the cyst.35 If a cyst ruptures in the lungs, radiologic signs include the “double arch” or “cumbo” sign, and the “air bubble.” 68
Figure 6. Life cycle of Echinococcus granulosus. Public domain image courtesy of the Centers for Disease Control and Prevention.
2
2
1
3 3
4
4
4444
4
6
5

402
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
■ Surgery.■ Anti-infective drug regimen.■ Expectant management, or watching and waiting
with medical imaging surveillance. Surgery remains the preferred treatment for liver
cystic echinococcosis65 and often can lead to a cured status, whereas treatment with a drug therapy of alben-dazole or mebendazole decreases the risk of disease recurrence and intraperitoneal seeding of infection that might develop with cyst rupture.72 Some cysts can be asymptomatic and remain inactive. These often disap-pear without treatment; therefore, watching and wait-ing can be beneficial.65
Foodborne TrematodiasesEpidemiology
Foodborne trematodes (flatworms or “flukes”) in the larval stage enter a host when they are ingested as part of a contaminated meal. These infections are particularly prevalent in East and Southeast Asia, and in Central and South America. The WHO estimates that 40 million people have these types of infections.73 Most of these infections are mildly pathogenic, but several are severe including clonorchiasis, opisthorchiasis, paragonimiasis, and fascioliasis. Of these, only paragonimiasis and fascio-liasis are known to affect people in the Americas.74
Paragonimiasis infections are transmitted by fresh-water shellfish within the Western Hemisphere.74
sensitivity and 96.6% specificity). A hydatid cyst is viewed optimally in the mediastinal window as a single or multiple small, rounded radiolucent area with specific margins in the outer portion of a solid mass lesion. An infected cyst also will produce higher attenuation values ( 20 HU), appearing brighter when compared with unruptured cysts. The density of an infected cyst can be problematic when differ-entiating it from an abscess or neoplasm. However, follow-up CECT scans can be useful in determining the presence of an “empty cyst” sign, an indication that contents were completely expectorated.68 Unless infection produces gas, premature death of the cyst and infection have the same appearances on CT and ultrasonography. In both cases, the f luid component becomes echogenic on ultrasonography and denser on CT, and there is an overall loss of clarity of the lesion’s internal detail.35
TreatmentCystic echinococcosis can be expensive and compli-
cated to treat, sometimes requiring extensive surgery, prolonged drug therapy, or both.64 Today, the accepted form of treatment is an image-based and stage-specific approach.71 Options for management are64: ■ Percutaneous treatment of the cysts with punc-
ture, aspiration, injection, and re-aspiration (PAIR technique).
Table 3
World Health Organization Classification of Cystic Echinococcosis Cysts and Imaging Features71
Classification Clinical Group Ultrasonography Imaging Features
Cystic lesion Group 1: Active group: cysts developing and are usually fertile
Unilocular, with uniform content, cyst wall not visible
CE1 Unilocular, simple cyst with visible cyst wall
CE2 Multivesicular, multiseptated cysts; cyst septations produce “wheel-like” structures, and the prescence of daughter cysts is indicated by “rosette-like” or “honeycomb-like” structures
CE3 Group 2: Transition group: cysts starting to degen-erate, but usually contain viable protoscoleces
Unilocular cyst that might contain daughter cysts; detach-ment of laminated membrane; “water-lily” sign
CE4 Group 3: Inactive group: degenerated or partially or totally calcified cysts; very unlikely to be fertile
Heterogeneous content, “ball of wool” sign, which is indicative of degenerating membranes
CE5 Thick calcified wall
Abbreviation: CE, cystic echinococcosis.

403
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
intestines, peritoneal cavity, and liver to reach the biliary ducts where they become adult flukes.1
Clinical ManifestationsClinical signs of paragonimiasis are from mechani-
cal damage caused by the migration of the worm from the gut to the lungs. In some instances, the f lukes can migrate in the host ectopically to the brain or subcu-taneous sites of the extremities.5 When the parasite reaches the lung, the most common site of infection, it causes hemorrhaging, inflammatory response, necrosis of lung parenchyma, and fibrotic encapsulation. Acute paragonimiasis is demonstrated by a cough, abdominal pain, discomfort, and low-grade fever that can occur 2 to 15 days after infection.1 A person with chronic pul-monary paragonimiasis has a cough producing brown and blood-streaked pneumonia-like sputum. The hemoptysis typically is induced by strenuous work, and the coughing often can be confused with chronic bron-chitis or bronchial asthma.75
In contrast, symptoms in the acute phase of fascio-liasis can correspond with the parasite’s migration from
Various species, including Paragonimus mexica-nus, Paragonimus ecuadoriensis, and Paragonimus kellicotti, have affected humans in Canada and Central and South America, especially Colombia, Ecuador, Peru, Venezuela, and parts of Brazil, as well as Costa Rica, Honduras, and Mexico.35 In contrast, fascioliasis, which is caused by the parasite Fasciola hepatica, is prev-alent in sheep- and cattle-raising areas of South America,74 with worldwide infection estimated to exceed 2 million.1
PathophysiologyThe life cycle of Paragonimus strains begins
when the unembryonated eggs are released into fresh water by infected humans via unsanitary practices regarding their mucus or stool.1 While in the fresh water, the eggs become embryo-nated and hatch into miracidia (larvae) that infect snails, their primary host. Within the snail, the miracadia undergo several changes and leave the snail as cercariae that then infect a secondary host of crustacean crabs and cray-fish, enclosing themselves within metacercariae (soft tissue cysts). Humans become infected following consumption of raw, undercooked, or pickled freshwa-ter shellfish containing the metacercariae. The parasite then exits its cystic stage to penetrate the human host’s peritoneum and lungs. Once settled, the trematodes develop into adult f lukes in 2 months (see Figure 7).74
In contrast, fascioliasis involves development of F hepatica following consumption by sheep and cattle where they grow into adult flukes, specifically in the bile ducts of the infected mammals. These animals then introduce immature F hepatica eggs in their feces to a freshwater environment. Similar to Paragonimus strains, the eggs embryonate and hatch in the water after several weeks as the miracidium that infects a snail host. After several more weeks, the parasites emerge from the snail as cercariae; however, they select water plants to encyst as metacercariae. Humans become infected following con-sumption of contaminated plants, especially watercress. The maturation of the parasite in the human host can take approximately 3 to 4 months. During this time, the meta-cercariae exist in the duodenum and travel through the
Figure 7. Life cycle of Paragonimus strains. Public domain image courtesy of the Centers for Disease Control and Prevention.
7
8
21
3
4
4a 4b 4c
6
5

404
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
thin-walled borders of cystic cavities, with a crescent-shaped opacity along one side of the border appearing like the corona of a solar eclipse. This feature represents worms attached to the wall of a cyst (see Figure 8).35
Similarly, in fascioliasis-endemic areas, examining stool samples for evidence of parasitic eggs can be per-formed; however, serologic diagnosis using F hepatica excretion-secretion antigens and ELISA testing has been more effective. The indirect hemaglutination test, a suspension that binds red blood cells, has a 100% diagnostic sensitivity and 97% specificity, if the meta-bolic antigen is used.35 In addition, testing the blood for high eosinophil levels has been effective in up to 68% of individuals with severe fascioliasis infections. Although laboratory tests help with diagnosis, serologic assays are limited because they cannot distinguish between past and current infection.74
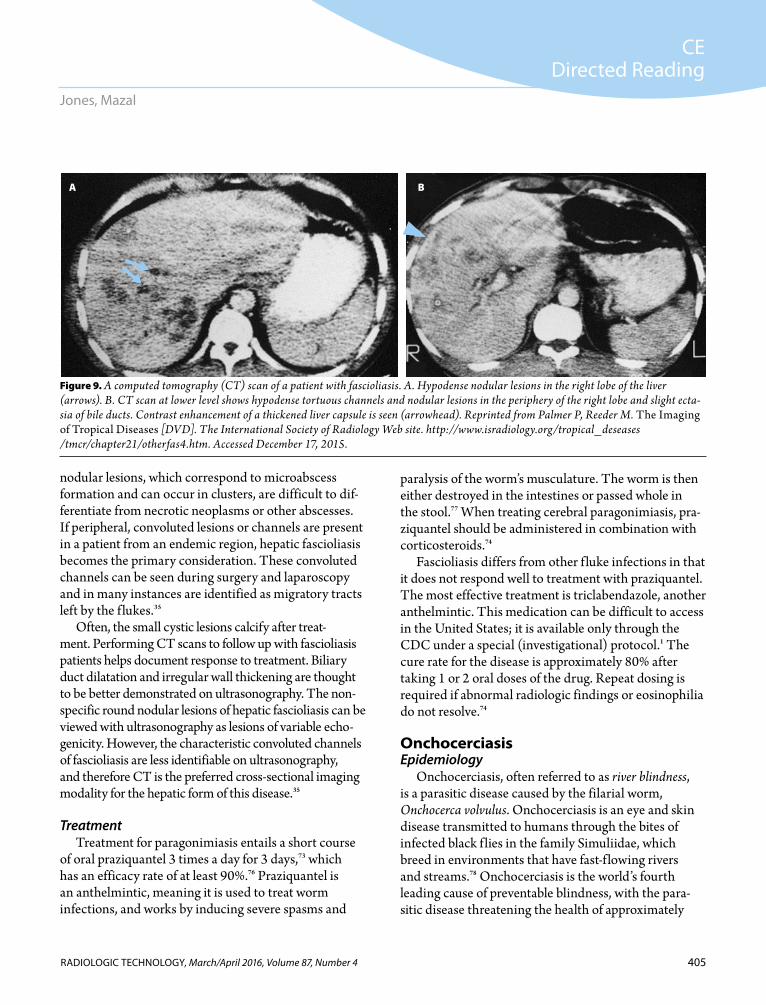
CT and ultrasonography have become widely avail-able in endemic areas to assist with diagnosing fascio-liasism.35 When using CT to assess an infected liver, imaging shows hypodense migratory lesions.74 These nodular intrahepatic lesions present with diminished attenuation, ranging in size from 4 mm to 10 mm but sometimes as large as 2 cm. Intravenous contrast medium might allow definition of these lesions on dynamic and delayed scans (see Figure 9). These
the intestine to and through the liver. Symptoms can include nausea, vomiting, and abdominal pain or ten-derness. In addition, fever, rash, and difficulty breath-ing can occur in acute cases.1 When the f luke reaches the liver, hepatomegaly occurs as the migratory f lukes destroy liver parenchyma. Chronic fascioliasis is associ-ated with the presence of adult worms in the bile ducts of the host. At this stage, symptoms can be difficult to distinguish from other hepatic diseases such as cholan-gitis, cholecystitis, and cholelithiasis.75
Diagnosis Diagnosing paragonimiasis involves analysis of patient
sputum, stool, and biopsies, as well as medical imaging.74 To overcome the low sensitivity of egg detection tests and low specificity of intradermal tests, serological test-ing, such as ELISA, is used to measure the serum levels of antibodies and has been found by the CDC to have a sensitivity and specificity greater than 95%.74
In people suspected of having a paragonimiasis infection, chest radiographs show abnormalities of the lungs or pleura similar to tuberculosis including infil-trates, nodules, cavities, and fibrosis. Evaluation of the radiographs is based on the migration of the f lukes. Once the f lukes penetrate the lung, hemorrhagic and exudative pneumonia occurs around them, and 2-mm to 4-mm thick and 2-cm to 7-cm long band-like opaci-ties adjacent to the pleura representing worm migra-tion tracts or peripheral atelectasis are commonly seen.35
Better-defined nodules or thin-walled cysts appear on medical imaging if f lukes remain in the same posi-tion because surrounding airspace consolidation can occur. In patients with airspace consolidation without visible cysts on radiographs, a CT scan with intravenous contrast can highlight cysts within the consolidated lung because of the difference of the darker (lower attenuation) f luid-filled cysts compared with brighter adjacent consolidated lung. Once lytic cysts extrude intracystic f luid, a CT scan might show them as air-filled cysts within the consolidated lung.35 The most characteristic radiographic feature of the mature stage of paragonimiasis is the “solar eclipse” sign, which has been seen in up to 82% of patients in chest radiography and chest CT scans. These ring shadows represent the
Figure 8. Pulmonary paragonimiasis. High resolution CT image showing the “solar eclipse” effect indicating worm cysts (arrow). A right-sided pneumothorax and worm cyst appear in the posterior right lung. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases/tmcr /chapter22/radiological4b.htm. Accessed December 17, 2015.
405
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
paralysis of the worm’s musculature. The worm is then either destroyed in the intestines or passed whole in the stool.77 When treating cerebral paragonimiasis, pra-ziquantel should be administered in combination with corticosteroids.74
Fascioliasis differs from other f luke infections in that it does not respond well to treatment with praziquantel. The most effective treatment is triclabendazole, another anthelmintic. This medication can be difficult to access in the United States; it is available only through the CDC under a special (investigational) protocol.1 The cure rate for the disease is approximately 80% after taking 1 or 2 oral doses of the drug. Repeat dosing is required if abnormal radiologic findings or eosinophilia do not resolve.74
OnchocerciasisEpidemiology
Onchocerciasis, often referred to as river blindness, is a parasitic disease caused by the filarial worm, Onchocerca volvulus. Onchocerciasis is an eye and skin disease transmitted to humans through the bites of infected black f lies in the family Simuliidae, which breed in environments that have fast-f lowing rivers and streams.78 Onchocerciasis is the world’s fourth leading cause of preventable blindness, with the para-sitic disease threatening the health of approximately
nodular lesions, which correspond to microabscess formation and can occur in clusters, are difficult to dif-ferentiate from necrotic neoplasms or other abscesses. If peripheral, convoluted lesions or channels are present in a patient from an endemic region, hepatic fascioliasis becomes the primary consideration. These convoluted channels can be seen during surgery and laparoscopy and in many instances are identified as migratory tracts left by the f lukes.35
Often, the small cystic lesions calcify after treat-ment. Performing CT scans to follow up with fascioliasis patients helps document response to treatment. Biliary duct dilatation and irregular wall thickening are thought to be better demonstrated on ultrasonography. The non-specific round nodular lesions of hepatic fascioliasis can be viewed with ultrasonography as lesions of variable echo-genicity. However, the characteristic convoluted channels of fascioliasis are less identifiable on ultrasonography, and therefore CT is the preferred cross-sectional imaging modality for the hepatic form of this disease.35
TreatmentTreatment for paragonimiasis entails a short course
of oral praziquantel 3 times a day for 3 days,73 which has an efficacy rate of at least 90%.76 Praziquantel is an anthelmintic, meaning it is used to treat worm infections, and works by inducing severe spasms and
Figure 9. A computed tomography (CT) scan of a patient with fascioliasis. A. Hypodense nodular lesions in the right lobe of the liver (arrows). B. CT scan at lower level shows hypodense tortuous channels and nodular lesions in the periphery of the right lobe and slight ecta-sia of bile ducts. Contrast enhancement of a thickened liver capsule is seen (arrowhead). Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases /tmcr/chapter21/otherfas4.htm. Accessed December 17, 2015.
A B

406
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
Dermal elastic fibers are lost gradually, resulting in abnormally wrinkled skin.35
Evaluation of visually impaired patients involves assessing the amount of microfilaria in the cornea and the anterior chamber of each eye. Assessment also is performed for other conditions that might result from onchocerciasis such as limbitis, iridocyclitis, sclerosing keratitis, chorioretinitis, and papillitis.81
DiagnosisPhysical examination and diagnosis begins with skin
biopsies. Biopsy sites in people from South America suspected of having the onchocerciasis infection are more commonly collected from the upper body because the black f ly endemic to the Americas is the Simulium ochraceum, a high-biting species. This differs from Simulium damnosum, which is endemic to Africa and a low-biting species.82
Radiography demonstrates filamentous calcification within nodules, particularly on soft tissue extremity images or mammograms, although the pattern in many cases is nonspecific. Even with the anatomic regions of interest biopsied, the diagnosis still might be difficult to confirm because of microcalcification occurring late in the inflammatory process, long after the worms are dead and fragmented.35
Ultrasonography increasingly is used in the developing world to diagnose onchocerciasis and identify associated skin nodules. With improvements in 2-D grayscale imag-ing and use of higher frequency transducers, onchocer-comas can be categorized and differentiated from other nodules and lymph nodes. A typical pattern demonstrates a lateral acoustic (refractive) shadow, a hypoechoic rim or layer, and a central zone of intermediate echogenicity in which numerous tiny, highly echogenic foci are seen. These foci are referred to as a worm center. Single and conglomerate nodules also can be distinguished (see Figure 10). The conglomerate can be evaluated based on the presence of multiple worm centers.35 After images are obtained, nodules can be removed surgically. Comparisons then can be made between sonograms and pathological sections (see Figure 11).
Advances are being made with the use of MR imaging in regard to associations between onchocer-ciasis and epilepsy.83 T1-weighted and T2-weighted,
25 million to 125 million people worldwide. Although 99% of those affected by onchocerciasis live in Africa, approximately 500 000 people in the Americas also are at risk.78-80 It is believed that onchocerciasis was brought to the Western Hemisphere through slave trade in the Americas and spread through migration.80 The great-est risks within the Americas region have been isolated to 13 foci of infection throughout Brazil, Colombia, Ecuador, Guatemala, Mexico, and Venezuela.80
PathophysiologyPeople who live in remote villages near rivers have the
greatest susceptibility for black fly bites. Once the O volvu-lus parasite is transmitted to the human host, the infective-stage larvae molt twice and mature into adult worms within nodules under the skin. These nodules are referred to as onchocercomas. At this point, the adult worms begin to reproduce, creating millions of larvae (microfilariae).80
Clinical ManifestationsThe infective activity of onchoceriasis can be dif-
ferentiated by that of microfilariae and of adult worms. The most significant activity pertains to the wander-ing microfilariae, which can result in groups as high as 2000 larvae/mg of skin. In the infected host, microfilar-iae are found in all layers of skin, but are most concen-trated within the dermal papillae.35 Histopathology of onchocercomas demonstrate that the nodules are firm and have 3 separate layers4: ■ An outer fibrous layer of granulation and scar tissue.■ A middle layer of inflammatory cells.■ A central soft core that contains adult nematodes
surrounded by an amorphous, eosinophilic, hya-line material named Splendore-Hoeppli material.
Symptoms of an onchoceriasis infection are caused by the migration of the microfilariae and include intense itching, rashes, disfiguring skin lesions (referred to as leopard or lizard skin), and eye disease that can result in blindness.79 Although the most severe infections occur in the skin and eyes, lymph nodes also are commonly affected.79 Onchocercal dermatitis is inf lammatory and progressive, leading to fibrosis and replacement of healthy skin. Changes in skin thickness, pigmentation, edema, and scarring of the epidermis are key indicators of this disease.

407
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
f luid-attenuated inversion recovery imaging and 3-D spoiled gradient recall imaging sequences to examine hippocampus anatomy have shown an association of intraparenchymal brain pathologies and O volvulus infection that might indicate a cause of nodding syn-drome in young people in areas endemic for onchocer-ciasis. Symptoms of nodding syndrome are repetitive dropping forward of the head and other seizure-like activity.83
A diagnostic test reserved for cases in which all other tests prove negative is the Mazzotti test. This test involves 5 mg diethylcarbamazine administered orally to the patient to inhibit neuromuscular transmis-sion in nematodes. The test is considered positive for onchocerciasis if an intense skin rash and itching results within 2 hours; these symptoms are caused by dying microfilariae. Corticosteroids can be administered postexamination to relieve pruritus for a few days, but severe systemic reactions and ocular complications are risks with this diagnostic method.74
TreatmentThe treatment of choice for onchocerciasis is iver-
mectin, which has been shown to reduce the occurrence of blindness and to reduce the occurrence and severity
Figure 10. Characteristic sonographic appearance of a solitary onchocercal nodule. Worm center (small arrows). Lateral acous-tic shadows (large arrows) and echo-poor capsule (arrowhead). Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases/tmcr/chapter 26/clinical8.htm. Accessed December 17, 2015.
Figure 11. A. Excision of an oncheroma under local anesthesia. B. Open nodule showing coiled adult worms in a central soft core with fibrotic outer layer. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases /tmcr/chapter26/clinical6.htm. Accessed December 17, 2015.
A
B

408
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
and the Caribbean is S mansoni. The various strains of schistosomes have different egg-laying capacities, which have been estimated to be as high as 3500 eggs per day in the case of S japonicum and 300 eggs per day in the case of S mansoni.35 Schistosomes can survive in the water without a host for 48 hours. People become infected when their skin comes in contact with the contaminated water and the cercariae penetrate the human host’s skin. While the egg matures into an adult worm, it can travel to and invade the intestines, liver, or bladder. Schistosoma mansoni causes intestinal schistosomiasis, dwelling within the blood vessels surrounding the intestines, in contrast to other strains that can cause urogenital schis-tosomiasis.85 The next generation of schistosome eggs undergoes asexual multiplication and is deposited within the rectum or large intestine. From there, the eggs are reintroduced to the environment via poor sanitation prac-tices and contamination of fresh water with infected feces (see Figure 12).35
Clinical ManifestationsIn the first days of infection, a rash or uticaria might
develop. Fever, chills, cough, and muscle aches can
of skin symptoms. Another preventive measure involves using environmentally safe insecticides to spray areas where black f lies lay their eggs.79
Pan American Health Organization resolution CD48.R12 was established in 2008 to interrupt trans-mission of onchocerciasis in Latin America.80 This public health program has been effective in eliminating the disease in Colombia and Ecuador. Such program-matic success is attributed to robust public-private partnerships involving national governments, local communities, donor organizations, intergovernmental bodies, academic institutions, nonprofit organizations, and the pharmaceutical industry. The accomplishment of disease control in these Latin American countries is informing the program about ways to control and elimi-nate onchocerciasis in Africa.80
SchistosomiasisEpidemiology
Schistosomiasis, also known as bilharzia,84 ranks second only to malaria in prevalence, affecting approxi-mately 240 million people worldwide.85 It is considered the most lethal of all NTDs, leaving many chronically ill and causing 100 000 deaths annually.74,84,86 More than 76 countries are affected, with Brazil, Suriname, Venezuela, the Dominican Republic, Guadeloupe, Martinique, and Saint Lucia experiencing the greatest impact within South America and the Caribbean.84 These regions have a tropical and sub-tropical climate and consist of limited-resource communities without potable water and adequate sanitation.
PathophysiologyDisease transmission occurs when infectious
forms of the parasite (cercariae) living in certain types of freshwater snails emerge and contami-nate the surrounding environment. Human hosts become infected when they come into contact with fresh water infested with blood trematodes, known as schistosomes. Most human infections are caused by the larval forms of parasitic blood f luke strains including Schistosoma mansoni, Schistosoma hae-matobium, or Schistosoma japonicum84; however, the most common variety within South America
Figure 12. Life cycle of Schistosoma haematobium, Schistosoma japoni-cum, and Schistosoma mansoni. Public domain image courtesy of the Centers for Disease Control and Prevention.
7
8
9
10
2
1
3
4
6
5
409
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
plaques beneath the normal mucosa of the rectum. In some cases, the bowel wall might be limited to glisten-ing granulation tissue, whereas in others, evidence of immune reaction might be related to polyp formation, with polyps potentially large enough to be mistaken for neoplasms. A biopsy of the lesions will determine whether they contain parasitic eggs, but some patients could have a normal examination, despite presence of an active infection.35
Sonographic examinations can show liver enlarge-ment, more prevalent in the left lobe than in the right. Multiple small nodules throughout the liver paren-chyma also might be identified as having a hypoechoic character. These nodules can be 4 mm to 5 mm in
manifest within 1 to 2 months postinfection. The majority of human hosts remain asymptomatic during this early phase. Eggs dwelling within the intestine, liver, or bladder can induce inflammation and scarring, which are caused by the body’s reaction to the eggs pro-duced and not by the worms themselves.84 In endemic areas, children with schistosomiasis can manifest ane-mia, stunted growth, decreased physical activity, and decreased general level of intelligence, although typi-cally not until the condition has progressed to signifi-cant cirrhosis.35,74,85 In children who avoid early death, infections can become chronic.
DiagnosisIdentifying the parasite in stool and urine samples
often is the first step when schistosomiasis is among the differential diagnoses. Evidence of infection also can be established through blood samples. However, the accu-racy of blood tests requires deferring sample collection until 6 to 8 weeks following the most recent exposure to contaminated water.1 The most reliable serological tests are indirect immunofluorescence, using 2 antibodies to label a specific target antigen with a f luorescent dye, and ELISA.35
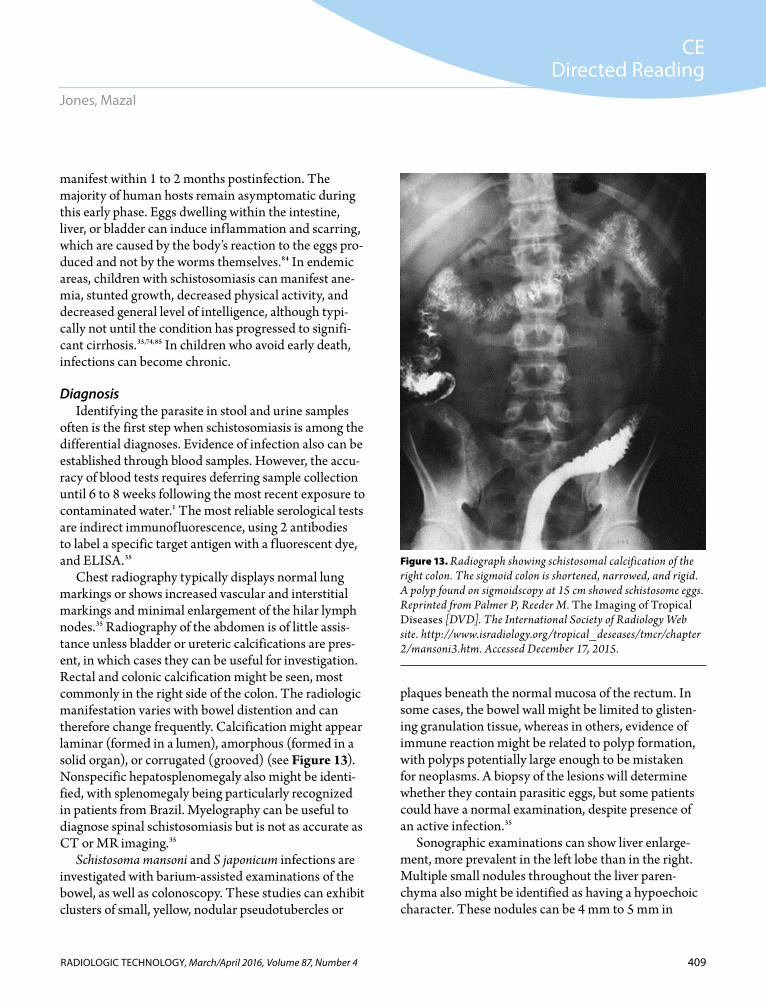
Chest radiography typically displays normal lung markings or shows increased vascular and interstitial markings and minimal enlargement of the hilar lymph nodes.35 Radiography of the abdomen is of little assis-tance unless bladder or ureteric calcifications are pres-ent, in which cases they can be useful for investigation. Rectal and colonic calcification might be seen, most commonly in the right side of the colon. The radiologic manifestation varies with bowel distention and can therefore change frequently. Calcification might appear laminar (formed in a lumen), amorphous (formed in a solid organ), or corrugated (grooved) (see Figure 13). Nonspecific hepatosplenomegaly also might be identi-fied, with splenomegaly being particularly recognized in patients from Brazil. Myelography can be useful to diagnose spinal schistosomiasis but is not as accurate as CT or MR imaging.35
Schistosoma mansoni and S japonicum infections are investigated with barium-assisted examinations of the bowel, as well as colonoscopy. These studies can exhibit clusters of small, yellow, nodular pseudotubercles or
Figure 13. Radiograph showing schistosomal calcification of the right colon. The sigmoid colon is shortened, narrowed, and rigid. A polyp found on sigmoidscopy at 15 cm showed schistosome eggs. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases/tmcr/chapter 2/mansoni3.htm. Accessed December 17, 2015.

410
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
these communities, children are most often infected. Furthermore, because these infections are linked to populations with poor hygiene and a lack of sanitation, they occur wherever poverty exists. More than 4 billion people are at high risk throughout the world, with more than 1 billion already infected.89
Transmitted by contact with contaminated soil, the most infectious of these parasitic worms are the roundworm ascaris (Ascaris lumbricoides), affecting approximately 807 million to 1.12 billion people; the whipworm causing trichuriasis (Trichuris trichiura), which affects approximately 604 million to 795 million people; and hookworms (Anclostoma duodenale and Necator americanus), affecting approximately 576 mil-lion to 740 million people.90 These diseases are distrib-uted widely in tropical and subtropical areas where they proliferate but also can be found in temperate zones during warmer months.
PathophysiologySoil-transmitted helminths live in the human intestine,
and their eggs are passed to the environment through the host’s feces when defecation occurs near bushes, in a garden or field, or when used as fertilizer. After the eggs mature in the soil, they become infectious and infect new human hosts when the eggs are ingested, often when veg-etables and fruits have not been carefully cooked, washed, or peeled before consumption.
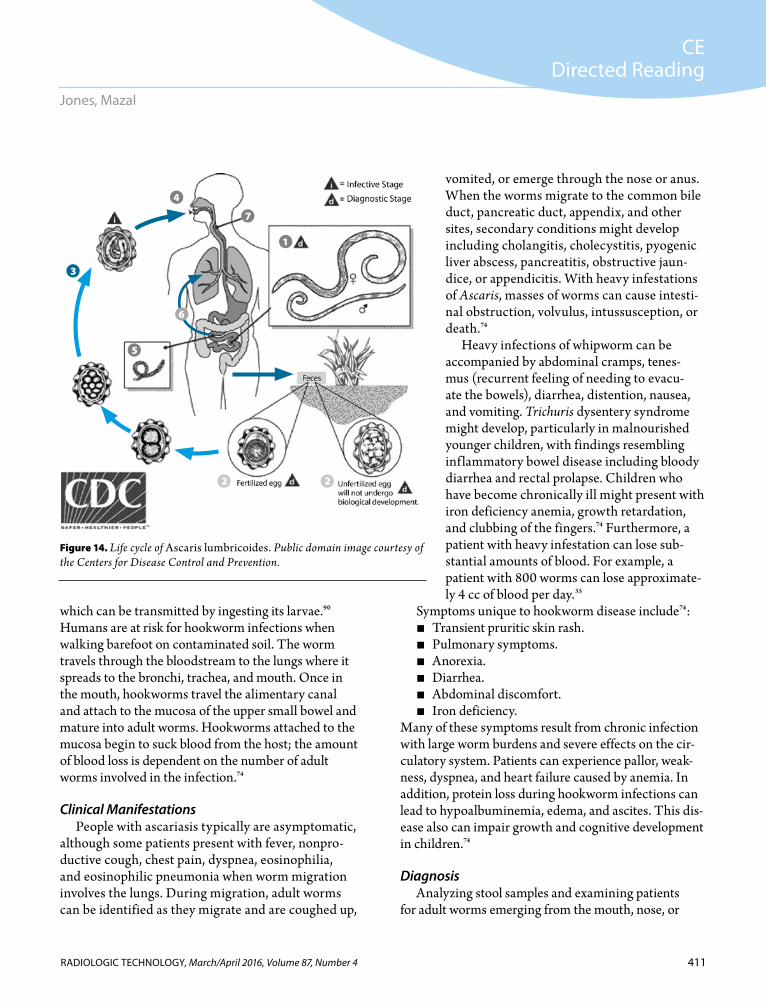
Ascariasis develops when larvae hatch in the small intestine, penetrate the bloodstream, travel to the lungs, and return to the intestines via the airway. Once Ascaris is transmitted to a host, the adult form can live in the body for 1 to 2 years, and grow as long as 40 cm with the thickness of a pencil (see Figure 14).74
As with ascariasis, humans are infected with whip-worm when eggs are ingested. Whipworm larvae hatch in the small intestine, but rather than penetrat-ing tissue and traveling throughout the host, they mature and remain in the large intestine. The adult whipworm grows to 4 cm and can live in a person’s bowel for 1 to 3 years.74
Hookworm eggs are not infectious in the egg form. They hatch while still in the soil and larvae mature into a form that can penetrate the skin of humans. One exception is the Anclostoma duodenale hookworm,
diameter and are typically well demonstrated on CT imaging as hypodense lesions with delayed contrast enhancement. Diagnosis is reliable only when imaging findings are correlated with the clinical findings, with marked eosinophilia, and with eggs found in feces or on biopsy.35
MR imaging previously was limited to evaluation of the central nervous system, particularly for imaging the brain or spinal cord when infected with S mansoni. In addition, it was thought that MR imaging of intra-abdominal schistosomiasis had little advantage over ultrasonography or CT.35 However, abdominal MR imaging reveals related focal or diffuse liver disease and vascular territories. MR can show heterogene-ity of hepatic parenchyma, the presence of peripheral perihepatic vessels, periportal fibrosis, splenomegaly, siderotic nodules (pigmented by iron), and the presence of venous collateral pathways. Furthermore, when com-pared with ultrasonography and CT, MR imaging also might be more sensitive, showing disease progression, stage, and response to therapy.87
TreatmentThe WHO strategy on using anthelmintic drugs
makes it possible to control schistosomiasis in poor and marginalized communities.85 Efforts to control the disease have involved education on the appropriate disposal of feces and urine and treatment with praziqu-antel.86 Although treatment with praziquantel is fairly effective in reducing or eliminating active infection, it is not a cure for everyone. Reinfection continues to be a problem in high-risk communities. A repeat dose of praziquantel, given 2 to 8 weeks after the first dose, can improve cure rates and reduce the intensity of remain-ing infections in population-based programs. Repeated dosing has demonstrated particular advantages in the treatment of S mansoni, but less consistent improvement was seen after double-dosing for S haematobium, the cause of urogenital schistosomiasis.88
Soil-transmitted HelminthsEpidemiology
Soil-transmitted helminth infections are some of the most common infections worldwide and affect the poorest and most deprived communities. Among
411
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
vomited, or emerge through the nose or anus. When the worms migrate to the common bile duct, pancreatic duct, appendix, and other sites, secondary conditions might develop including cholangitis, cholecystitis, pyogenic liver abscess, pancreatitis, obstructive jaun-dice, or appendicitis. With heavy infestations of Ascaris, masses of worms can cause intesti-nal obstruction, volvulus, intussusception, or death.74
Heavy infections of whipworm can be accompanied by abdominal cramps, tenes-mus (recurrent feeling of needing to evacu-ate the bowels), diarrhea, distention, nausea, and vomiting. Trichuris dysentery syndrome might develop, particularly in malnourished younger children, with findings resembling inf lammatory bowel disease including bloody diarrhea and rectal prolapse. Children who have become chronically ill might present with iron deficiency anemia, growth retardation, and clubbing of the fingers.74 Furthermore, a patient with heavy infestation can lose sub-stantial amounts of blood. For example, a patient with 800 worms can lose approximate-ly 4 cc of blood per day.35
Symptoms unique to hookworm disease include74: ■ Transient pruritic skin rash.■ Pulmonary symptoms.■ Anorexia.■ Diarrhea.■ Abdominal discomfort.■ Iron deficiency.
Many of these symptoms result from chronic infection with large worm burdens and severe effects on the cir-culatory system. Patients can experience pallor, weak-ness, dyspnea, and heart failure caused by anemia. In addition, protein loss during hookworm infections can lead to hypoalbuminemia, edema, and ascites. This dis-ease also can impair growth and cognitive development in children.74
Diagnosis Analyzing stool samples and examining patients
for adult worms emerging from the mouth, nose, or
which can be transmitted by ingesting its larvae.90 Humans are at risk for hookworm infections when walking barefoot on contaminated soil. The worm travels through the bloodstream to the lungs where it spreads to the bronchi, trachea, and mouth. Once in the mouth, hookworms travel the alimentary canal and attach to the mucosa of the upper small bowel and mature into adult worms. Hookworms attached to the mucosa begin to suck blood from the host; the amount of blood loss is dependent on the number of adult worms involved in the infection.74
Clinical ManifestationsPeople with ascariasis typically are asymptomatic,
although some patients present with fever, nonpro-ductive cough, chest pain, dyspnea, eosinophilia, and eosinophilic pneumonia when worm migration involves the lungs. During migration, adult worms can be identified as they migrate and are coughed up,
Figure 14. Life cycle of Ascaris lumbricoides. Public domain image courtesy of the Centers for Disease Control and Prevention.
7
22
1
3
4
5
6

412
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
Identifying whipworm in the colon using an air-contrast barium enema examination enables visualiza-tion of wavy radiolucent outlines of numerous small worms against the air-barium background of the colon and rectum. Furthermore, characteristic uncurled curvilinear patterns or S-shaped configurations of the female worms and the tightly coiled “pinwheel” or “tar-get” pattern of the male worm might be recognizable. The posterior portions of the worms become outlined and are approximately 1 cm long, with the longer, slen-der anterior two-thirds of the worms lying uncoated by barium within the colonic mucosa (see Figure 16).35
In patients with chronic and severe cases of hookworm disease, chest radiographs show a mild to moderate gen-eralized cardiac enlargement caused by profound anemia and hypoproteinemia. General radiography also can be used to identify initial migration patterns of hookworms, with radiographs of the feet and ankles demonstrating evidence of hookworm infection (see Figure 17).35 Most patients with hookworm infection do not demonstrate radiographic abnormality on barium examination of the upper gastrointestinal tract; however, small bowel abnor-malities can be found in 60% of hosts, with changes being proportional to the disease burden. For example, irregu-larities have been observed in the mucosal folds of the jejunum resulting in 2 to 3 times the thickness of healthy tissue. More advanced infections show increased tone in several loops, narrowing of the lumen, and vigorous peri-stalsis appearing to be in constant motion.35
TreatmentSoil-transmitted helminths can be controlled and elim-
inated by drugs called benzimidazoles, which interfere with the worm’s cellular energy metabolism. The 2 main drugs used to treat ascariasis, whipworm, and hookworm infections are mebendazole and albendazole. Using these drugs is known as deworming and is not limited to treating symptomatic infections; it also is part of large-scale pre-vention effort in children in endemic areas, often paired with immunization campaigns for added effectiveness.
DengueEpidemiology
Dengue is the second most common vector-borne disease in humans after malaria. A member of the genus
anus are the primary tests for ascariasis, whipworm, or hookworm infections. Other useful tests in acute stages include skin tests, fecal smear techniques, and medical imaging. Serological tests, including ELISA, have been used experimentally to measure antibodies but are not used for routine diagnosis of ascariasis, whipworm, or hookworm.35
Radiologic findings of intestinal worms often are secondary to investigation of rectal bleeding or other colonic disease. In contrast-enhanced studies, worms are identified as filling defects and as intestinal or bili-ary obstructions.74 This is true especially when imag-ing children with severe ascariasis. The collection of worms contrasted against gas in the bowel (usually a distended portion) looks like a tangled group of thick cords and sometimes produces a “whirlpool” effect (see Figure 15).35
Figure 15. An upper gastrointestinal series reveals multiple ascarids in the stomach and proximal small bowel. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases/tmcr/chapter10 /imaging4.htm. Accessed December 17, 2015.

413
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
dengue hemorrhagic fever occur each year. The disease prevalence is attributed to climatic factors, travel, and urbanization.74 In the past 20 years, severe epidemics of dengue hemorrhagic fever have occurred in East Africa, Sri Lanka, and Latin America. Despite having this knowledge, it has been difficult to pinpoint specific locations at greatest risk considering that the virus has been detected in 128 countries in endemic regions.28
Chikungunya is another virus recognized as an NTD, but it is primarily endemic to Asia and Africa. Although it has spread to much of the Americas region as recently as 2013, relatively speaking, it has a low impact in Latin America.92
PathophysiologyDuring the rainy season in endemic regions, the breed-
ing of Aedes mosquitoes is abundant. Poor water manage-ment in these areas often is coupled with a population uneducated about mosquitoes’ breeding and mosquito bite protection.93 Aedes mosquitoes spend their lifetime near a single location, traveling an average of 400 meters. This means that infected humans, rather than the mos-quitoes, are the primary reason the virus spreads between communities.94
The virus has 4 distinct serotypes (DEN-1, DEN-2, DEN-3, and DEN-4), and the severity of the dengue
Flavivirus, it is transmitted by the bite of the Aedes aegypti mosquito, which also transmits yellow fever and chikungunya viruses. An estimated 400 million cases of dengue 91 and several hundred thousand cases of
Figure 16. Trichuriasis in a 7-year-old boy with profuse rectal bleed-ing and innumerable whipworms attached to the rectal mucosa. A. Postevacuation image from barium enema shows flocculation of barium and poor mucosal coat-ing. B. Air contrast study reveals the radiolucent outlines of many small trichurids. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology .org/tropical_deseases/tmcr/chapter17/imaging.htm. Accessed December 17, 2015.
Figure 17. Radiograph showing a lytic lesion of the left ankle. Subsequent histological examination confirmed that the lesion contained calcified larvae of Necator americanus. Reprinted from Palmer P, Reeder M. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases/tmcr/chapter12/radio logical2.htm. Accessed December 17, 2015.
A B

414
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
show pleural effusions within the first week of infec-tion.96 When advanced imaging is available to provid-ers, CT scans without contrast can detect intracranial bleeding or cerebral edema from dengue hemorrhagic fever.
Ultrasonography can show thickening of the gall-bladder wall and, in some patients, ascites. A correlation exists between the severity of the illness and increasing thickness of the gallbladder wall, with 93% of patients with severe cases of dengue displaying gallbladder wall thickness exceeding 3 mm. When there is ascites, the gallbladder wall is significantly thicker than in patients without intraperitoneal f luid (see Figure 18).35 Sonographic findings of f luid collection typically can occur in the perirenal and pararenal, hepatic and splenic subcapsular, and pericardial regions. In addition, ultra-sonography can demonstrate evidence of pancreatic enlargement and hepatosplenomegaly, with an altera-tion in the normal liver echo texture caused by intrapa-renchymal and subcapsular hemorrhages.
Although serology is used to confirm dengue fever, ultrasonography can be used to assess the infection’s
burden is dependent on the number of serotypes with which an individual becomes infected.94 The virus cir-culates in the blood of an infected host for 2 to 7 days over which time the host might begin to develop symp-toms. For the disease to spread among people, the mos-quito must feed on a person during this period. Then it must bite another person after an 8-day to 12-day incubation period.
Clinical ManifestationsDengue infection can range from being asymptom-
atic to causing severe hemorrhagic fever or fatal shock (dengue shock syndrome). More than half of infected children are asymptomatic, whereas in adults the illness is more severe and begins more suddenly. After an incu-bation period of 4 to 5 days, infected individuals expe-rience a sudden onset of “breakbone” fever including chills, aching of the head, back, and extremities accom-panied by sore throat, prostration, and malaise.94 After 3 to 4 days of infection, a maculopapular rash sparing the palms and soles appears in more than 50% of cases.74
Dengue hemorrhagic fever typically occurs in sec-ondary infections and in infections with DEN-2. Signs of hemorrhage appear in the first few days of infec-tion and include ecchymoses (nontraumatic bruises), gastrointestinal bleeding, and epistaxis. Dengue shock syndrome is indicated when acute fever, hemorrhagic manifestations, pleural effusions, and ascites occur. Other indicators of dengue shock syndrome include continuous abdominal pain with vomiting, mucosal bleeding, a decrease in consciousness, rash, conjuncti-val congestion, and hypothermia.74
Diagnosis Serological findings can be useful in dengue
diagnosis including the nonstructural protein-1 antigen test, measurement of glycoprotein levels, and immunoglobulin G and M tests. During the fifth and sixth day of febrile illness from this disease, hemagglutination inhibition antibodies begin to appear at detectable levels.95
Medical imaging of mild dengue syndromes does not reveal specific abnormalities. In severe cases, how-ever, abdominal imaging might display the presence of associated hepatomegaly, and chest radiographs can
Figure 18. A 32-year-old patient with a history of fever and thrombocy-topenia was diagnosed with dengue. This abdominal sonogram shows a thickened, edematous gallbladder wall. Reprinted with permission from Santhosh VR, Patil PG, Srinath MG, Kumar A, Jain A, Archana M. Sonography in the diagnosis and assessment of dengue fever. J Clin Imaging Sci. 2014;4:14. doi:10.4103/2156-7514.129260.

415
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
imaging plays in initial disease diagnosis and confirma-tion, as well as recognize the radiologic manifestations of the NTDs specific to the Americas region.
Reviewing a patient’s history for recent travel to an endemic country can provide insight into symptoms that initially might seem to be benign. Performing a basic physical examination for signs of disease can trig-ger a need for laboratory analyses and imaging assess-ment. Immunosorbent assays, such as ELISA, as well as stool sample testing often can lead directly to diagnosis when an NTD is being considered. When such technol-ogy is unavailable, an understanding of the basic modes of transmission for each NTD, related pathophysiology, and common clinical manifestations can aid in select-ing the appropriate imaging modality and technical parameters necessary to make an accurate diagnosis.
In Latin America and the Caribbean, ultraso-nography has been the most widely used imaging modality given its low cost, noninvasiveness, and portability; however, this modality can be limited by user-dependency and considerable interobserver vari-ability. Ultrasonography generally is used for screening purposes to identify nonspecific evidence of parasitic presence and invasion. In urban settings, CT and MR technology are more likely to be available. These high-resolution imaging techniques, often with the aid of contrast enhancement, can help characterize parasitic lesions and offer advanced assessment of organ involve-ment and damage.
It also is important to recognize the need for greater investment into radiology outreach initiatives98-103 within endemic regions of the Americas to control and reverse the spread of diseases at their points of origin. Although an “imaging gap” continues to exist between developed and developing countries with regard to access to reliable imaging services and radiology-specific training, the presence of NTDs in endemic regions of the Americas remains a persistent risk to the resource-rich countries that border them.
severity and often serves as a catalyst to disease man-agement when serology testing is unavailable. The severity of dengue infection is linked directly to platelet count, with patients demonstrating all sonographic features associated with dengue likely having platelet counts less than 40 000/L and potentially requiring blood transfusion. In addition, sonographic features also have a direct relationship with the degree of throm-bocytopenia affecting dengue patients.95
TreatmentNo pharmaceutical treatment for dengue infections
is available. A person experiencing associated symp-toms should use analgesics with acetaminophen and avoid use of aspirin-based medications because they can compound bleeding issues. Rest and hydration are recommended until a physician can be consulted, but worsening symptoms, such as vomiting and severe abdominal pain within 24 hours of fever decline, require emergent evaluation. In-hospital treatment involves f luid volume support, blood products, vaso-pressor agents, acetaminophen, and endoscopic therapy to assist in managing gastrointestinal hemorrhage.91
Recovery from infection by a dengue virus results in lifelong immunity against that particular virus sero-type; however this immunity provides only partial and transient protection against subsequent infection by the 3 other serotypes. In addition, studies show that sequential infection increases the risk of developing a severe dengue infection.97
ConclusionWith WHO’s official recognition of the 17 global
NTDs and the 66th World Health Assembly’s 2013 adoption of resolution WHA66.12 calling for intensi-fied, integrated measures and planned investments to improve the health and social well-being of popula-tions affected by NTDs, member states are focusing increased attention on these diseases. Although the majority of countries endemic for NTDs within the Americas are in Central and South America, these conditions exist in the Caribbean and the southern por-tions of North America including the states bordering the U.S. Gulf Coast. For this reason, it is important for radiologic technologists to understand the role medical
The ASRT Foundation in partnership with RAD-AID International provides medical relief efforts to communities around the world. Learn how you can get involved at asrtfoundation.org/outreach.

416
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
PLoS Negl Trop Dis. 2014;8(9):e2922. doi:10.1371/journal .pntd.0002922.
11. Dantés HG, Farfán-Ale JA, Sarti E. Epidemiological trends of dengue disease in Mexico (2000-2011): a sys-tematic literature search and analysis. PLoS Negl Trop Dis. 2014;8(11):e3158. doi:10.1371/journal.pntd.0003158.
12. Hotez PJ, Bottazzi ME, Franco-Paredes C, Ault SK, Periago MR. The neglected tropical diseases of Latin America and the Caribbean: a review of disease burden and distribution and a roadmap for control and elimination. PLoS Negl Trop Dis. 2008;2(9):e300. doi:10.1371/journal.pntd.0000300.
13. Hotez PJ, Murray KO, Buekens P. The Gulf Coast: a new American underbelly of tropical diseases and poverty. PLoS Negl Trop Dis. 2014;8(5):e2760. doi:10.1371/journal .pntd.0002760.
14. EPA’s work in the Gulf of Mexico. United States Environmental Protection Agency Web site. http://www .epa.gov/gmpo/about/facts.html. Updated December 18, 2015. Accessed April 16, 2014.
15. Hotez PJ. America’s most distressed areas and their neglected infections: the United States Gulf Coast and the District of Columbia. PLoS Negl Trop Dis. 2011;5(3):e843. doi:10.1371 /journal.pntd.0000843.
16. Hotez PJ, Bottazzi ME, Dumonteil E, Buekens P. The Gulf of Mexico: a “hot zone” for neglected tropical diseases? PLoS Negl Trop Dis. 2015;9(2):e0003481. doi:10.1371/journal .pntd.0003481.
17. Murray KO, Rodriguez LF, Herrington E, et al. Identification of dengue fever cases in Houston, Texas, with evidence of autochthonous transmission between 2003 and 2005. Vector Borne Zoonotic Dis. 2013;13(12):835-845. doi:10.1089 /vbz.2013.1413.
18. Brunkard JM, Robles Lopez JL, Ramirez J, et al. Dengue fever seroprevalence and risk factors, Texas-Mexico border, 2004. Emerg Infect Dis. 2007;13(10):1477-1483.
19. Ramos MM, Mohammed H, Zielinski-Gutierrez E, et al. Epidemic dengue and dengue hemorrhagic fever at the Texas-Mexico border: results of a household-based seroepi-demiologic survey, December 2005. Am J Trop Med Hyg. 2008;78(3):364-369.
20. Centers for Disease Control and Prevention. Locally acquired dengue—Key West, Florida, 2009-2010. Morbidity and Mortality Weekly Report. 2010;59(19):577-581.
21. Ruiz-Moreno D, Vargas IS, Olson KE, Harrington LC. Modeling dynamic introduction of chikungunya virus in the United States. PLoS Negl Trop Dis. 2012;6(11):e1918. doi:10.1371/journal.pntd.0001918.
22. Dorn PL, Perniciaro L, Yabsley MJ, et al. Autochthonous transmission of Trypanosoma cruzi, Louisiana. Emerg Infect Dis. 2007;13(4):605-607. doi:10.3201/eid1304.061002.
Patrick Jones, BS, R.T.(R), is a radiologic technologist in Tulsa, Oklahoma.
Jonathan Mazal, MS, R.R.A., R.T.(R)(MR), is a radio-logic technologist in Bethesda, Maryland. He is a board member for the International Society of Radiographers & Radiologic Technologists and also serves as the organiza-tion’s regional director for the Americas.
Reprint requests may be mailed to the American Society of Radiologic Technologists, Communications Department, at 15000 Central Ave SE, Albuquerque, NM 87123-3909, or emailed to [email protected].
© 2016 American Society of Radiologic Technologists
References1. Neglected tropical diseases. Centers for Disease Control and
Prevention Web site. http://www.cdc.gov/globalhealth/ntd/. Accessed April 9, 2015.
2. Sixty-sixth World Health Assembly. Neglected tropical dis-eases. WHA66.12. http://www.who.int/neglected_diseases /mediacentre/WHA_66.12_Eng.pdf?ua=1. Published May 27, 2013. Accessed January 18, 2016.
3. Latin America & Caribbean (developing only). The World Bank Web site. http://data.worldbank.org/region/LAC. Accessed January 5, 2014.
4. Hotez PJ, Dumonteil E, Heffernan MJ, Bottazzi ME. Innovation for the ‘bottom 100 million’: eliminating neglect-ed tropical diseases in the Americas. Adv Exp Med Biol. 2013;764:1-12.
5. Wikipedia (2014) List of Countries by percentage of popula-tion living in poverty. https://en.wikipedia.org/wiki/List _of_countries_by_percentage_of_population_living_in _poverty. Accessed January 5, 2014.
6. Bern C, Kjos S, Yabsley MJ, Montgomery SP. Trypanosoma cruzi and Chagas’ disease in the United States. Clin Microbiol Rev. 2011;24(4):655-681. doi:10.1128/CMR.00005-11.
7. Alvar J, Vélez ID, Bern C, et al. Leishmaniasis world-wide and global estimates of its incidence. PLoS One. 2012;7(5):e35671. doi:10.1371/journal.pone.0035671.
8. Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature. 2013;496(7446):504-507. doi:10.1038/nature12060.
9. World Health Organization (2014) Neglected tropical diseases, PCT Databank. Soil-transmitted helminthiases.http://www.who.int/neglected_diseases/diseases/en/. Accessed January 14, 2014.
10. Hotez PJ. The NTDs and vaccine diplomacy in Latin America: opportunities for United States foreign policy.
417
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
36. Sparrow PJ, Merchant N, Provost YL, Doyle DJ, Nguyen ET, Paul NS. CT and MR imaging findings in patients with acquired heart disease at risk for sudden cardiac death. Radiographics. 2009;29(3):805-823. doi:10.1148 /rg.293085715.
37. Barral MM, Nunes Mdo C, Barbosa MM, Ferreira CS, Tavares Jr WC, Rocha MO. Echocardiographic parameters associated with pulmonary congestion in outpatients with Chagas’ cardiomyopathy and non-chagasic cardiomyopathy. Rev Soc Bras Med Trop. 2012;45(2):215-219.
38. Garcia RL, Matos BM, Féres O, Rocha JJ. Surgical treatment of Chagas megacolon. Critical analysis of outcome in opera-tive methods. Acta Cir Bras. 2008;23 (suppl 1)83-92.
39. Rodriques Coura J, de Castro SL. A critical review on Chagas disease chemotherapy. Mem Inst Oswaldo Cruz. 2002;97(1):3-24.
40. Parasites – American Trypanosomiasis (also known as Chagas disease). Centers for Disease Control and Prevention Web site. http://www.cdc.gov/parasites/chagas/. Updated July 19, 2013. Accessed April 9, 2015.
41. Chagas disease: potentially a life-threatening neglected tropical disease. World Health Organization Web site. http://www.who.int/chagas/en/. Accessed April 10, 2015.
42. Coyle CM, Mahanty S, Zunt JR, et al. Neurocysticercosis: neglected but not forgotten. PLoS Negl Trop Dis. 2012;6(5):e1500. doi:10.1371/journal.pntd.0001500.
43. Garcia HH, Nash TE, Del Brutto OH. Clinical symptoms, diagnosis, and treatment of neurocysticercosis. Lancet Neurol. 2014;13(12):1202-1215. doi:10.1016/S1474 -4422(14)70094-8.
44. Parasites – cystericercosis. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/parasites/cysticer cosis/gen_info/faqs.html. Updated April 17, 2014. Accessed June 7, 2015.
45. Sarti-Gutierrez EJ, Schantz PM, Lara-Aguilera R, Gomez Dandoy H, Flisser A. Taenia solium taeniasis and cysticercosis in a Mexican village. Trop Med Parasitol. 1988;39(3):194-198.
46. Lescano AG, Garcia HH, Gilman RH, et al. Taenia solium cysticercosis hotspots surrounding tapeworm carriers: clus-tering on human seroprevalence but not on seizures. PLoS Negl Trop Dis. 2009;3(1):e371. doi:10.1371/journal.pntd .0000371.
47. O’Neal SE, Moyano LM, Ayvar V, et al. Geographic correla-tion between tapeworm carriers and heavily infected cysti-cercotic pigs. PLoS Negl Trop Dis. 2012;6(12):e1953. doi:10.1371/journal.pntd.0001953.
48. Carabin H, Ndimubanzi PC, Budke CM, et al. Clinical man-ifestations associated with neurocysticercosis: a systematic review. PLoS Negl Trop Dis. 2011;5(5):e1152. doi:10.1371 /journal.pntd.0001152.
23. Lee BY, Bacon KM, Bottazzi ME, Hotez PJ. Global eco-nomic burden of Chagas disease: a computational simulation model. Lancet Infect Dis. 2013;13(4):342-348. doi:10.1016 /S1473-3099(13)70002-1.
24. Hotez PJ. Neglected infections of poverty in the United States of America. PLoS Negl Trop Dis. 2008;2(6):e256. doi:10.1371/journal.pntd.0000256.
25. Andrus J, Bottazzi ME, Chow J, et al. Ears of the armadillo: global health research and neglected diseases in Texas. PLoS Negl Trop Dis. 2013;7(6):e2021. doi:10.1371/journal .pntd.0002021.
26. Teague J. Radiology practice in Latin America: a literature review. Radiol Technol. 2013;84(3):228-240.
27. Pan American Health Organization. Borras C, ed. Organization, development, quality assurance and radiation protection in radiology services: imaging and radiation thera-py. http://apps.who.int/medicinedocs/documents/s16602e /s16602e.pdf. Published December 1997. Accessed December 18, 2015.
28. Chagas disease (American trypanosomiasis). World Health Organization Web site. http://www.who.int/mediacentre /factsheets/fs340/en/. Accessed April 10, 2015.
29. Bern C, Martin DL, Gilman RH. Acute and congenital Chagas disease. Adv Parasitol. 2011;75:19-47. doi:10.1016 /B978-0-12-385863-4.00002-2.
30. Marchiori E, Zanetti G, Nobre LF, Takayassu TC, Irion KL. Lipoid pneumonia complicating megaesophagus secondary to Chagas disease: high-resolution computed tomography findings. J Thorac Imaging. 2010;25(2):179-182. doi:10.1097 /RTI.0b013e3181ad883b.
31. Valdigem BP, da Silva NJ, Dietrich CO, et al. Accuracy of epi-cardial electroanatomic mapping and ablation of sustained ventricular tachycardia merged with heart CT scan in chron-ic Chagasic cardiomyopathy. J Interv Card Electrophysiol. 2010;29(2):119-125. doi:10.1007/s10840-010-9513-5.
32. Pallisera A, Ortiz-de-Zarate L, Moral A, et al. Chagas disease in the differential diagnosis of megacolon. Rev Esp Enferm Dig. 2011;103(10):554-555.
33. Buysschaert I, De Keyser J, Dujardin K. Stone heart or apical retraction and calcification in Chagas’ cardiomyopathy. Eur Heart J Cardiovasc Imaging. 2012;13(7):625. doi:10.1093 /ehjci/jes020.
34. dos Santos CM, Cassiani RA, Dantas RO. Videofluoroscopic evaluation of swallowing in Chagas’ disease. Dysphagia. 2011;26(4):361-365. doi:10.1007/s00455-010-9321-1.
35. Palmer P, Reeder MM. The Imaging of Tropical Diseases [DVD]. The International Society of Radiology Web site. http://www.isradiology.org/tropical_deseases/tmcr/main .htm. Accessed December 17, 2015.
418
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Medical Imaging of Neglected Tropical Diseases of the Americas
64. Echinococcus. World Health Organization Web site. http://www.who.int/echinococcosis/en/. Accessed April 14, 2015.
65. Akkucuk S, Aydogan A, Ugur M, et al. Comparison of surgi-cal procedures and percutaneous drainage in the treatment of liver hydatide cysts: a retrospective study in an endemic area. Int J Clin Exp Med. 2014;7(8):2280-2285.
66. Parasites – echinococcosis. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/parasites/echino coccosis/epi.html. Updated December 12, 2012. Accessed April 14, 2015.
67. Bensghir M, Fjouji S, Bouhabba N, et al. Anaphylactic shock during hydatid cyst surgery. Saudi J Anaesth. 2012;6(2):161-164. doi:10.4103/1658-354X.97031.
68. Singh U, Kumar S, Gour H, et al. Complicated hydatid cyst and “air bubble” sign: a stepping-stone to correct diagnosis. Am J Case Rep. 2015;16:20-24. doi:10.12659/AJCR.892621.
69. Gharbi HA, Hassine W, Brauner MW, Dupuch K. Ultrasound examination of the hydatic liver. Radiology. 1981;139(2):459-463.
70. Sirigu D, Puddu S. Hepatic Echinococcus cyst. SonoWorld Web site. http://sonoworld.com/CaseDetails/Hepatic_Echinococcus_Cyst.aspx?CaseId=430. Accessed April 14, 2015.
71. Teke M, Göçmez C, Hamidi C, et al. Imaging features of cerebral and spinal cystic echinococcosis. Radiol Med. 2015;120(5):458-465. doi:10.1007/s11547-014-0475-z.
72. Smego RA Jr, Sebanego P. Treatment options for hepatic cystic echinococcosis. Int J Infect Dis. 2005;9(2):69-76.
73. Foodborne treamatode infections. World Health Organization Web site. http://www.who.int/foodborne _trematode_infections/en/. Accessed May 31, 2015.
74. Papadakis M, McPhee SJ, Rabow MW. Current Medical Diagnosis and Treatment 2015. 54th ed. Columbus, OH: McGraw-Hill Education; 2015:1374-1376.
75. Toledo R, Esteban JG, Fried B. Current status of food-borne trematode infections. Eur J Clin Microbiol Infect Dis. 2012;31(8):1705-1718. doi:10.1007/s10096-011-1515-4.
76. Chai JY. Praziquantel treatment in trematode and cestode infections: an update. Infect Chemother. 2013;45(1):32-43. doi:10.3947/ic.2013.45.1.32.
77. Praziquantel (oral route). Mayo Clinic Web site. http://www .mayoclinic.org/drugs-supplements/praziquantel-oral-route /description/drg-20065610. Accessed June 1, 2015.
78. Onchocerciasis – or “river blindness” – is a parasitic disease. World Health Organization Web site. http://www.who.int /onchocerciasis/en/. Accessed May 1, 2015.
79. Parasites – onchocerciasis (also known as river blindness). Centers for Disease Control and Prevention Web site. http://www.cdc.gov/parasites/onchocerciasis/index.html. Updated August 10, 2015. Accessed May 1, 2015.
49. Fogang YF, Savadogo AA, Camara M, et al. Managing neurocysticercosis: challenges and solutions. Int J Gen Med. 2015;8:333-344. doi:10.2147/IJGM.S73249.
50. Rajshekhar V. Severe episodic headache as the sole present-ing ictal event in patients with a solitary cysticercus granu-loma. Acta Neurol Scand. 2000;102(1):44-46.
51. Cantú C, Barinagarrementeria F. Cerebrovascular complica-tions of neurocysticercosis. Clinical and neuroimaging spec-trum. Arch Neurol. 1996;53(3):233-239.
52. Sá DS, Teive HA, Troiano AR, Werneck LC. Parkinsonism associated with neurocysticercosis. Parkinsonism Relat Disord. 2005;11(1):69-72. doi:10.1016/j.parkrel dis.2004.07.009.
53. Tsang VC, Brand JA, Boyer AE. An enzyme-linked immu-noelectrotransfer blot assay and glycoprotein antigens for diagnosing human cysticercosis (Taenia solium). J Infect Dis. 1989;159(1):50-59.
54. Odashima NS, Takayanagui OM, Figueiredo JF. Enzyme linked immunosorbent assay (ELISA) for the detection of IgG, IgM, IgE and IgA against cysticercus cellulosae in cerebrospinal f luid of patients with neurocysticercosis. Arq Neuropsiquiatr. 2002;60(2-B):400-405.
55. Vijayaraghavan SB. Sonographic appearances in cysticerco-sis. J Ultrasound Med. 2004;23(3):423-427.
56. Jayakumar PN, Chandrashekar HS, Ellika S. Imaging of parasitic infections of the central nervous system. Handb Clin Neurol. 2013;114:37-64. doi:10.1016/B978-0-444-53490 -3.00004-2.
57. Lerner A, Shiroishi MS, Zee CS, Law M, Go JL. Imaging of neurocysticercosis. Neuroimaging Clin N Am. 2012;22(4):659-676. doi:10.1016/j.nic.2012.05.004.
58. Rajshekhar V, Chandy MJ. Validation of diagnostic criteria for solitary cerebral cysticercus granuloma in patients pre-senting with seizures. Acta Neurol Scand. 1997;96(2):76-81.
59. Schantz PM, Cruz M, Sarti E, Pawlowski Z. Potential eradi-cability of taeniasis and cysticercosis. Bull Pan Am Health Organ. 1993;27(4):397-403.
60. Garcia HH, Gonzalez AE, Del Brutto OH, et al. Strategies for the elimination of taeniasis/cysticercosis. J Neurol Sci. 2007;262(1-2):153-157.
61. Assana E, Kyngdon CT, Gauci CG, et al. Elimination of Taenia solium transmission to pigs in a field trial of the TSOL18 vaccine in Cameroon. Int J Parasitol. 2010;40(5):515-519. doi:10.1016/j.ijpara.2010.01.006.
62. Bagga PK, Bhargava SK, Aggarwal N, Chander Y. Primary subcutaneous inguinal hydatid cyst: diagnosis by fine needle aspiration cytology. J Clin Diagn Res. 2014;8(8):FD11-13. doi:10.7860/JCDR/2014/8692.4744.
63. Awasthy N, Chand K. Primary hydatid disease of the spine: an unusual case. Br J Neurosurg. 2005;19(5):425-427.

419
CEDirected Reading
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Jones, Mazal
94. Thongcharoen P. Monograph on Dengue/Dengue Haemorrhagic Fever. Geneva, Switzerland: World Health Organization; 1983:22.
95. Santhosh VR, Patil PG, Srinath MG, Kumar A, Jain A, Archana M. Sonography in the diagnosis and assess-ment of dengue fever. J Clin Imaging Sci. 2014;4:14. doi:10.4103/2156-7514.129260.
96. Wang CC, Wu CC, Liu JW, et al. Chest radiographic presen-tation in patients with dengue hemorrhagic fever. Am J Trop Med Hyg. 2007;77(2):291-296.
97. Dengue control. The World Health Organization Web site. http://www.who.int/denguecontrol/human/en/. Accessed June 15, 2015.
98. Culp M, Mollura DJ, Mazal J; RAD-AID Conference Writing Group. 2014 RAD-AID Conference on International Radiology for Developing Countries: the road ahead for global health radiology. J Am Coll Radiol. 2015;12(5):475-480.
99. Welling RD, Azene EM, Kalia V, et al. White Paper Report of the 2010 RAD-AID Conference on International Radiology for Developing Countries: identifying sustainable strate-gies for imaging services in the developing world. J Am Coll Radiol. 2011;8(8):556-562. doi:10.1016/j.jacr.2011.01.011.
100. Everton KL, Mazal J, Mollura DJ; RAD-AID Conference Writing Group. White Paper Report of the 2011 RAD-AID Conference on International Radiology for Developing Countries: integrating multidisciplinary strategies for imaging services in the developing world. J Am Coll Radiol. 2012;9(7):488-494.
101. Mollura DJ, Mazal J, Everton KL, et al. White Paper Report of the 2012 RAD-AID Conference on International Radiology for Developing Countries: planning the implementation of global radiology. J Am Coll Radiol. 2013;10(8):618-624. doi:10.1016/j.jacr.2013.01.019.
102. Mollura DJ, Shah N, Mazal J; RAD-AID Conference Writing Group. White Paper Report of the 2013 RAD-AID Conference: improving radiology in resource-limited regions and developing countries. J Am Coll Radiol. 2014;11(9):913-919. doi:10.1016/j.jacr.2014.03.026.
103. Mollura DJ, Azene EM, Starikovsky A, et al. White Paper Report of the RAD-AID Conference on International Radiology for Developing Countries: identifying chal-lenges, opportunities, and strategies for imaging services in the developing world. J Am Coll Radiol. 2010;7(7):495-500. doi:10.1016/j.jacr.2010.01.018.
80. Gustavsen K, Hopkins A, Sauerbrey M. Onchocerciasis in the Americas: from arrival to (near) elimination. Parasites & Vectors. 2011;4:205. doi:10.1186/1756-3305-4-205.
81. Banla M, Tchalim S, Karabou PK, et al. Sustainable con-trol of onchocerciasis: ocular pathology in onchocerciasis patients treated annually with ivermectin for 23 years: a cohort study. PLoS One. 2014;9(6):e98411. doi:10.1371/jour nal.pone.0098411.
82. Young RM, Burkett-Cadena ND, McGaha TW Jr, et al. Identification of human semiochemicals attractive to the major vectors of onchocerciasis. PLoS Negl Trop Dis. 2015;9(1):e3450. doi:10.1371/journal.pntd.0003450.
83. Winkler AS, Friedrich K, Velicheti S, et al. MRI findings in people with epilepsy and nodding syndrome in an area endemic for onchocerciasis: an observational study. Afr Health Sci. 2013;13(2):529-540. doi:10.4314/ahs.v13i2.51.
84. Parasites – schistosomiasis. Centers for Disease Control and Prevention Web site. http://www.cdc.gov/parasites/schisto somiasis/index.html. Accessed May 18, 2015.
85. Schistosomiasis: a major health problem. The World Health Organization Web site. http://www.who.int/schistosomiasis /en/. Accessed April 9, 2015.
86. The burden of schistosomiasis (schisto, bilharzia, snail fever). Centers for Disease Control and Prevention Web site. http://www.cdc.gov/globalhealth/ntd/diseases/schisto_bur den.html. Updatead June 6, 2011. Accessed May 18, 2015.
87. Bezerra AS, D’Ippolito G, Caldana RP, Cecin AO, Ahmed M, Szejnfeld J. Chronic hepatosplenic schistosomiasis man-soni: magnetic resonance imaging and magnetic resonance angiography findings. Acta Radiol. 2007;48(2):125-134.
88. King CH, Olbrych SK, Soon M, Singer ME, Carter J, Colley DG. Utility of repeated praziquantel dosing in the treat-ment of schistosomiasis in high-risk communities in Africa: a systematic review. PLoS Negl Trop Dis. 2011;5(9):e1321. doi:10.1371/journal.pntd.0001321.
89. Intestinal worms. The World Health Organization Web site. http://www.who.int/intestinal_worms/en/. Accessed June 15, 2015.
90. Parasites – soil-transmitted helminths. http://www.cdc.gov /parasites/sth/. Updated January 20, 2013. Accessed June 15, 2015.
91. Dengue. Frequently asked questions. Centers for Disease Control and Prevention Web site. http://www.cdc.gov /dengue/fAQFacts/index.html. Updated June, 15 2015. Accessed Janaury 8, 2016.
92. Weaver SC, Forrester NL. Chikungunya: evolutionary his-tory and recent epidemic spread. Antiviral Res. 2015;120:32-39. doi:10.1016/j.antiviral.2015.04.016.
93. Singh B. Dengue outbreak in 2006: failure of public health system? Indian J Community Med. 2007;32(2):99.
420 RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Directed Reading Quiz
continued on next page
Read the preceding Directed Reading and choose the answer that is most correct based on the article.
To earn continuing education credit: Take this Directed Reading quiz online at www.asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 410M and mail to ASRT, PO Box 51870, Albuquerque, NM 87181-1870.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to www.asrt.org/store.
*Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date.
To earn continuing education credit: Take this Directed Reading quiz online at www.asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 424 and mail to ASRT, PO Box 51870, Albuquerque, NM 87181-1870.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to www.asrt.org/store.
*Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date.
16802-01 2.75 Category A+ creditsExpires April 30, 2019*
1. Chagas disease is caused by the parasite ______ and is transmitted by triatomine bugs.a. Giardia lambliab. Trypanosoma cruzi c. Entamoeba histolyticad. Plasmodium knowlesi
2. Medical imaging of Chagas disease can reveal:1. cardiomyopathy.2. calcifications in the apical vasculature.3. delayed esophageal motility.
a. 1 and 2 b. 1 and 3c. 2 and 3 d. 1, 2, and 3
3. Cysticercosis infections are caused by:a. helminths.b. filarial worms.c. flatworms.d. mosquitoes.
4. The predominant means of spreading cysticercosis infections is: a. person to person.b. via environmental sources.c. animal to person. d. insect to person.
5. In regions where computed tomography (CT) and magnetic resonance (MR) imaging are available, these scans can provide information on:
1. morphology and localization of cysticercosis cysts.
2. stage of cysts.3. inflammation.
a. 1 and 2 b. 1 and 3c. 2 and 3 d. 1, 2, and 3
Medical Imaging of Neglected Tropical Diseases of the Americas

RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Directed Reading Quiz
421
11. Which is the most characteristic radiologic sign of the mature stage of paragonimiasis and represents worms attached to the wall of a cyst?a. air bubbleb. Cumboc. solar eclipsed. double-arch
12. The characteristic convoluted channels of fascioliasis are less identifiable on ultrasonography, and therefore, ______ is the preferred imaging modality for the hepatic form of this disease. a. CTb. MRc. positron emission tomographyd. radiography
13. Changes in skin thickness, pigmentation, edema, and scarring of the epidermis are key indicators of:a. dengue.b. fascioliasis. c. onchoceriasis. d. schistosomiasis.
14. Which modality is being used increasingly in the developing world to diagnose onchocerciasis? a. ultrasonography b. radiographyc. CTd. MR
15. This disease is considered the most lethal of all neglected tropical diseases leaving many chronically ill and causing 100 000 deaths annually.a. onchocerciasis b. schistosomiasis c. dengued. chorioretinitis
6. The majority (50%-70%) of echinococcosis cysts develop in the liver.a. true b. false
7. A patient presenting with a cyst-like mass and a history of recent exposure to sheepdogs while in an area in which Echinococcus granulosus is endemic is suggestive of: a. Chagas disease.b. cystic echinococcosis. c. neurocysticercosis.d. paragonimiasis.
8. All of the following are descriptions of Gharbi classification type for echinococcosis cysts, except:a. pure fluid collection in the cyst. b. fluid collection with septa. c. reflecting thick walls.d. multiple cysts with calcified walls .
9. The most common site of a paragonimiasis infection is the:a. heart.b. lung.c. brain.d. extremities.
10. Chest radiographs of people suspected of having a paragonimiasis infection show abnormalities of the lungs or pleura similar to tuberculosis including all of the following except: a. cavities.b. fibrosis.c. infiltrates.d. “air bubble” sign.
continued on next page
RADIOLOGIC TECHNOLOGY, March/April 2016, Volume 87, Number 4
Directed Reading Quiz
422
20. Aedes aegypti mosquitoes transmit all of the following viruses except:a. malaria.b. dengue.c. chikungunya.d. yellow fever.
21. Ultrasonography can show which signs of dengue fever?
1. thickening of the wall of the gallbladder 2. ascites3. kidney stones
a. 1 and 2 b. 1 and 3c. 2 and 3 d. 1, 2, and 3
22. Recommendations to treat dengue symptoms include:
1. aspirin-based medications.2. rest.3. hydration.
a. 1 and 2 b. 1 and 3c. 2 and 3 d. 1, 2, and 3
16. Which imaging modality might be more sensitive to show disease progression, stage, and response to therapy for Schistosoma mansoni infections? a. CTb. MRc. radiographyd. ultrasonography
17. Once ______ is transmitted to a host, the adult form can live in the body for 1 to 2 years, and grow as long as 40 cm with the thickness of a pencil. a. Ascaris b. Schistosoma mansoni c. Simulium damnosum d. Trypanosoma cruzi
18. Heavy infestations of ______ can involve masses of worms that can cause intestinal obstruction, volvulus, intussusception, or death.a. Ascarisb. Fasciola hepaticusc. Onchocera volvulusd. Schistosoma japonicum
19. Identifying whipworm in the colon using an air-contrast barium enema enables visualization of which of the following?
1. radiolucent outlines of small worms2. S-shaped configurations of female worms3. tightly coiled male worms
a. 1 and 2 b. 1 and 3c. 2 and 3 d. 1, 2, and 3
Your post-test is now complete. The ARRT now requires only 8 questions per CE credit. For additional information, read the recent ASRT Scanner story at asrt.org/as.rt?BvrzKx.
!