manas kanungo - lunch & learn august 4th, 2017
TRANSCRIPT
UC Irvine Applied Innovation Center
Lunch-n-Learn Presentation @ The COVE Friday August 4, 2017
“Defining a Commercially Viable Product”
A Case Study: Phase – 0 to Phase 2
Manas Kanungo Int’l Medical Marketing (IMM) USA, LLC
I love a challenging role – where I can learn and create innovative, sustainable global solutions that enhance health outcomes.
Manas Kanungo Confidential 1

Career Summary Define, Plan, Execute Innovative Solutions - Enter & Grow Int’l Markets
Manas Kanungo Confidential 2
15+ Yrs in Hospital, Lab, POL, POC Medical Device, Diagnostic industry
Small - Large companies: Start-ups, BioTek, Quidel, Roche, Bayer, Abbott
Built, coached, supervised, led direct, in-direct, matrixed teams
Define, Develop, Execute market entries, growth, product & brand launches, exits
Multi-country, multi-segment VOC qual/quant market, ethnography research
Unique ability to cross boundaries between diseases, therapies, technologies, providers, payers, patients for impactful, competitively sustainable solutions
Lived, worked out of 3, traveled in 50+ countries US citizen with work visas for Brazil and India Native English w/business fluency in Portuguese, Hindi, Oriya; basic Spanish
Int’l Sales, Distribution, Product, Marketing, JV, Commercial Leadership Roles
Strong Strategic Upstream Planning, Downstream Execution – Products, Markets
Academic Achievements Degrees
HealthCare Executive MBA: UC Irvine
MS Bioengineering & MS Electrical Engineering: West Virginia University
BS Electrical Engineering: National Institute of Technology, India
Continuing Education
Omics, Bioscience, BioPharma, Life Science Trends & Strategies: UC Berkeley
Cloud Computing: Stanford University
Mobile Medical: UC Santa Clara
High Impact Leadership: UC Berkeley
Global Leadership: Thunderbird
Recognitions, Publications, Patent
Honorary Diploma, Association of Hospital Engineers, Spain
SBIR Grants, MS Thesis, VT State Award, ISO/ASTM for Ventilator Tester
Published in Electrophysiology area; White Papers; Patent applied for.
Manas Kanungo Confidential 3
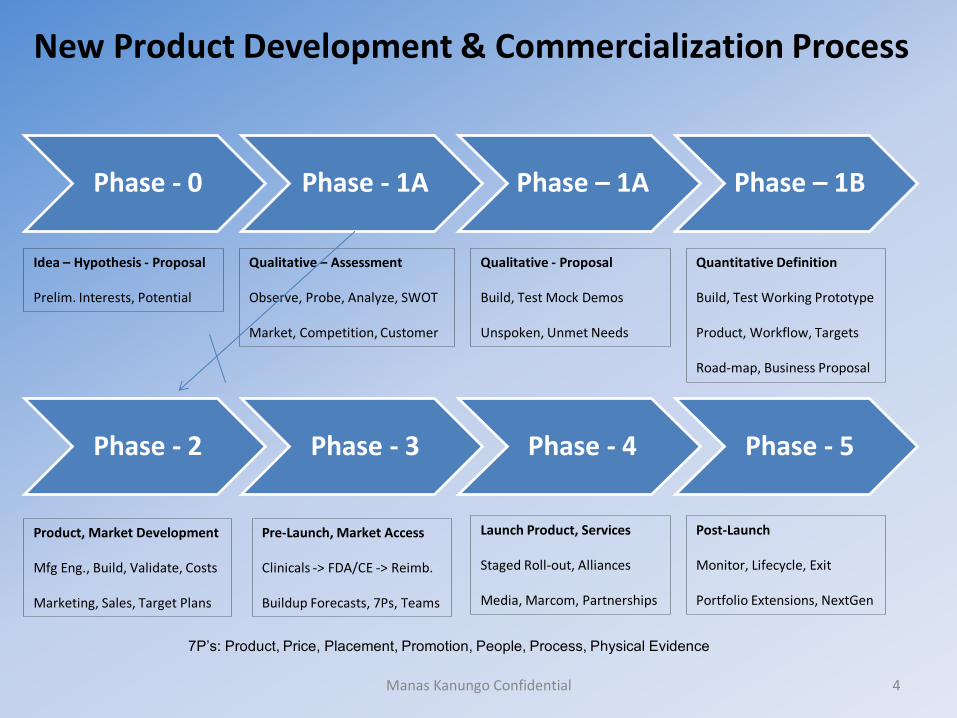
New Product Development & Commercialization Process
Phase - 0 Phase - 1A Phase – 1A Phase – 1B
Manas Kanungo Confidential 4
Phase - 2 Phase - 3 Phase - 4 Phase - 5
Idea – Hypothesis - Proposal Prelim. Interests, Potential
Qualitative – Assessment Observe, Probe, Analyze, SWOT Market, Competition, Customer
Qualitative - Proposal Build, Test Mock Demos Unspoken, Unmet Needs
Quantitative Definition Build, Test Working Prototype Product, Workflow, Targets Road-map, Business Proposal
Product, Market Development Mfg Eng., Build, Validate, Costs Marketing, Sales, Target Plans
Pre-Launch, Market Access Clinicals -> FDA/CE -> Reimb. Buildup Forecasts, 7Ps, Teams
Launch Product, Services Staged Roll-out, Alliances Media, Marcom, Partnerships
Post-Launch Monitor, Lifecycle, Exit Portfolio Extensions, NextGen
7P’s: Product, Price, Placement, Promotion, People, Process, Physical Evidence
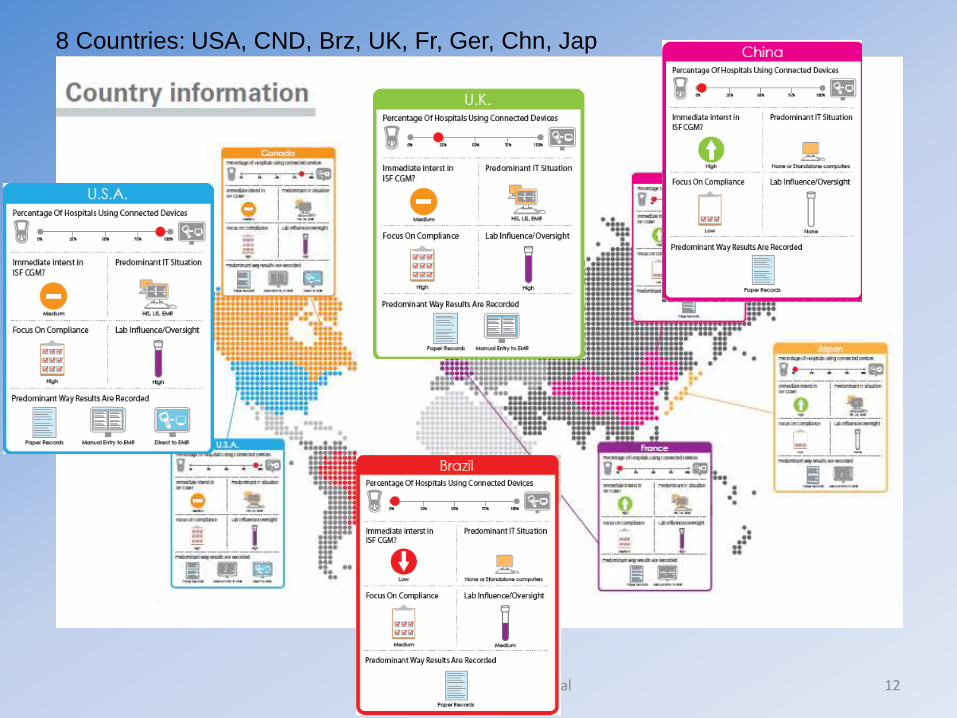
Phase – 0: Idea, Hypothesis, Proposal
Manas Kanungo Confidential 5
Page 6
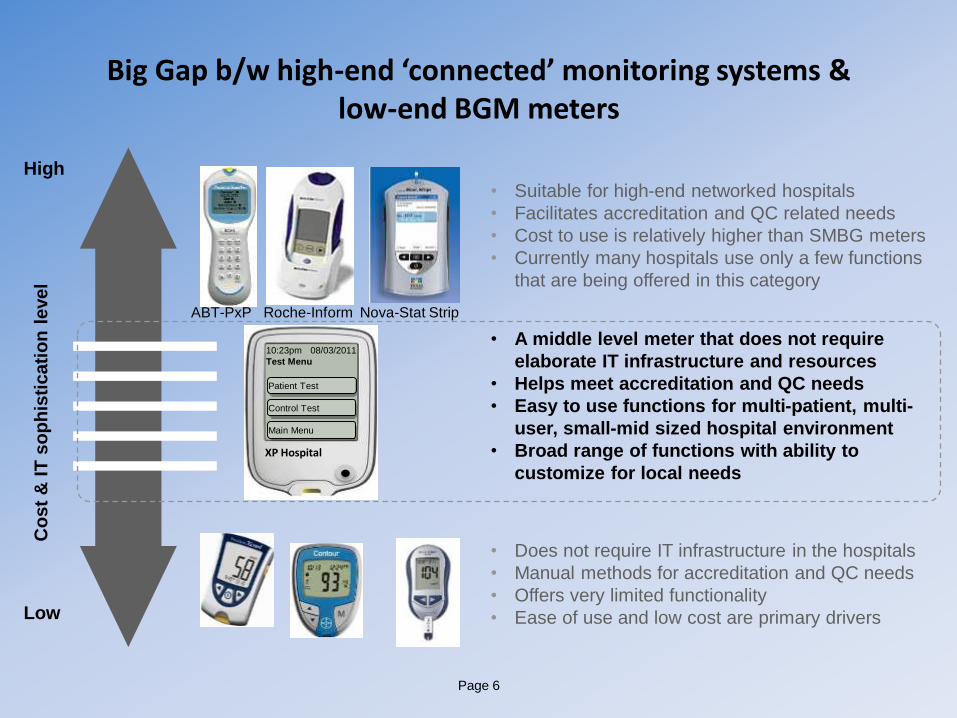
Big Gap b/w high-end ‘connected’ monitoring systems & low-end BGM meters
• Suitable for high-end networked hospitals
• Facilitates accreditation and QC related needs
• Cost to use is relatively higher than SMBG meters
• Currently many hospitals use only a few functions
that are being offered in this category
• Does not require IT infrastructure in the hospitals
• Manual methods for accreditation and QC needs
• Offers very limited functionality
• Ease of use and low cost are primary drivers
10:23pm 08/03/2011
Test Menu
Control Test
Patient Test
Main Menu
XP Hospital
• A middle level meter that does not require
elaborate IT infrastructure and resources
• Helps meet accreditation and QC needs
• Easy to use functions for multi-patient, multi-
user, small-mid sized hospital environment
• Broad range of functions with ability to
customize for local needs
Co
st
& I
T s
op
his
ticati
on
level
High
Low
ABT-PxP Roche-Inform Nova-Stat Strip

Industry Trends, External Forces
• Push to Implement New Point-of-Care Standards
– With better performance: + 10-15% accuracy with no interference from drugs or other health conditions
– Prevent cross-contamination: multi-patient / user
• More hospitals world-wide wanting to adopt ISO, POC Standards for Accreditation
– To be equal to their peers, be a global player
– Command higher reimbursement, fees
• New Entrants Challenging BGM Market Leaders MK 2014 Manas Kanungo Confidential 7
Page 8
• To develop a cost-effective, multi-patient, multi-user,
“middle meter” w/new technology platform in development.
• To fill an important gap in the portfolio, by meeting the
needs of hospitals motivated for QA or Accreditation, but
w/o budget or infrastructure for IT or high-end systems.
Opportunity
• A meter positioned towards ‘aspiring’ hospitals in emerging
economies with a broad range of relevant features and
offered at a price point close to existing SMBGs commonly
used in hospitals by leveraging the new platform.
• Additional potential for US, CND, EU
Strategic
Intent
• Hospitals that need compliance with QA, QC, audit,
Accreditation and Regulatory requirements for multi-
patient, multi-user POC blood glucose testing without
additional investment in IT infrastructure and resources
Target
Market
PROJECT OVERVIEW – Initial Proposal
Phase – 1A: Qualitative Assessment
Observe, Probe, Analyze, SWOT
Market, Competition, Customer
Manas Kanungo Confidential 9

Page 10
Amongst Top BGM Manufacturers, LifeScan [ J&J ] was the only known competitor developing a “middle meter” for emerging hospital markets.
OneTouch Verio PRO; 1st Generation meter (H1:12 Asia Pac)
• Uses OneTouch Verio test strip (0.4 µL, 5 sec), no-coding, POC hospital accuracy
• Verio test strip is NOT approved for neonatal use at this time; venous, capillary, and arterial testing only
• Expected 1st gen meter features:
•Test Strip ejector
• Color Screen, use in low light
• New industrial design, created specifically for the hospital segment (can withstand rigorous cleaning/ disinfection, durable, etc.)
• NO Connectivity, NO Ketones
2nd Generation Verio PRO (currently in
early development stage, est 2013 - 2014 )
• Same meter chassis and test strip
• Enhanced software functionality:
• Connectivity, data transfer
• Multi-patient capability with ability to
validate results recorded
• QA/QC
While Roche and Bayer did not appear to have internal
“middle-meter” hospital products in development,
select Asia Pacific based secondary players (Sanwa,
Arkray, Terumo) have shown hospital focused meters
for Japan with strip ejectors.
Page 11
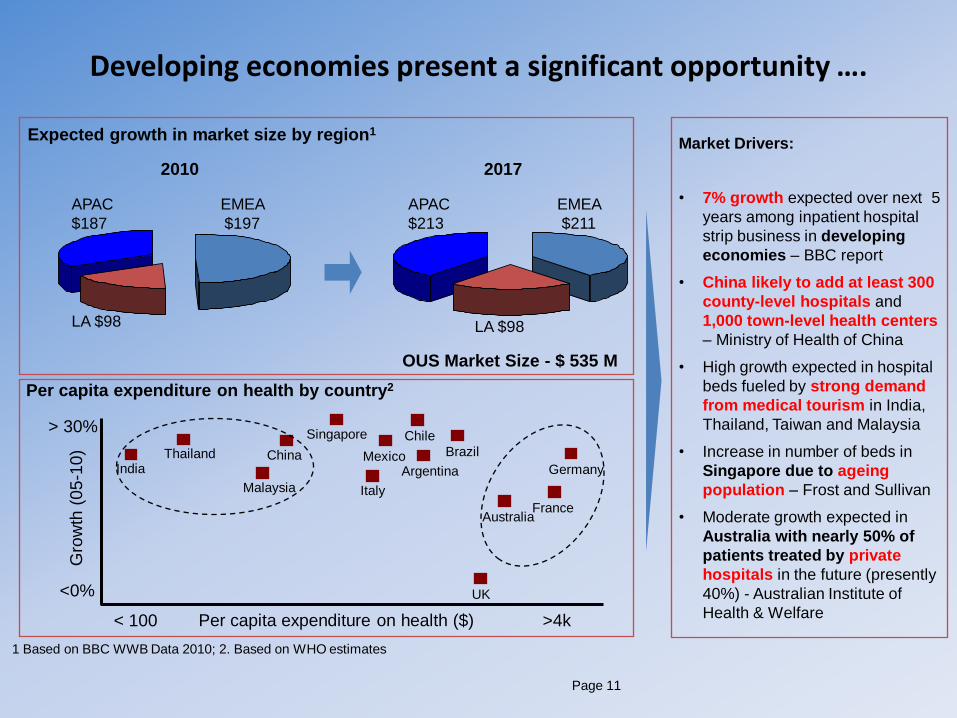
Developing economies present a significant opportunity ….
LA $98
EMEA
$197
APAC
$187
2010 2017
LA $98
EMEA
$211
APAC
$213
< 100
OUS Market Size - $ 535 M
Expected growth in market size by region1
Per capita expenditure on health by country2
1 Based on BBC WWB Data 2010; 2. Based on WHO estimates
Market Drivers:
• 7% growth expected over next 5
years among inpatient hospital
strip business in developing
economies – BBC report
• China likely to add at least 300
county-level hospitals and
1,000 town-level health centers
– Ministry of Health of China
• High growth expected in hospital
beds fueled by strong demand
from medical tourism in India,
Thailand, Taiwan and Malaysia
• Increase in number of beds in
Singapore due to ageing
population – Frost and Sullivan
• Moderate growth expected in
Australia with nearly 50% of
patients treated by private
hospitals in the future (presently
40%) - Australian Institute of
Health & Welfare >4k Per capita expenditure on health ($)
<0%
> 30%
Gro
wth
(05
-10)
India
Thailand
UK
Argentina
Australia
Brazil Chile
China
France
Germany
Italy Malaysia
Mexico
Singapore
Manas Kanungo Confidential 12
8 Countries: USA, CND, Brz, UK, Fr, Ger, Chn, Jap
Manas Kanungo Confidential 13
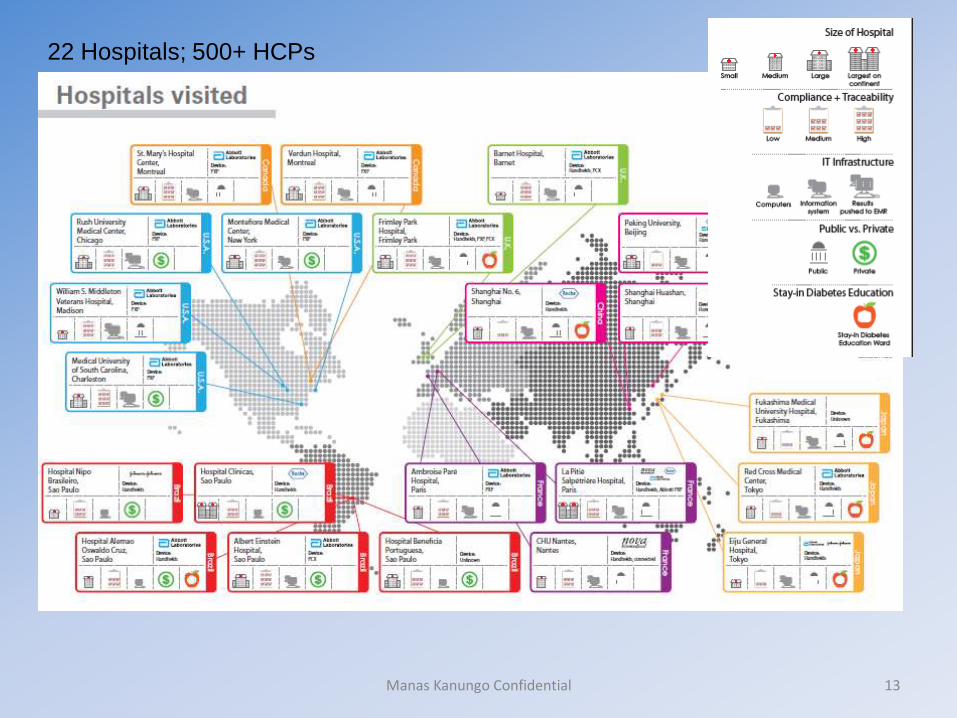
22 Hospitals; 500+ HCPs

Manas Kanungo Confidential 14

Manas Kanungo Confidential 15
Manas Kanungo Confidential 16

Manas Kanungo Confidential 17

Manas Kanungo Confidential 18

Phase – 1A: Qualitative Proposal
Build, Test Mock Demos – Alpha Units
Validate Unspoken, Unmet Needs
Manas Kanungo Confidential 19

Manas Kanungo Confidential 20
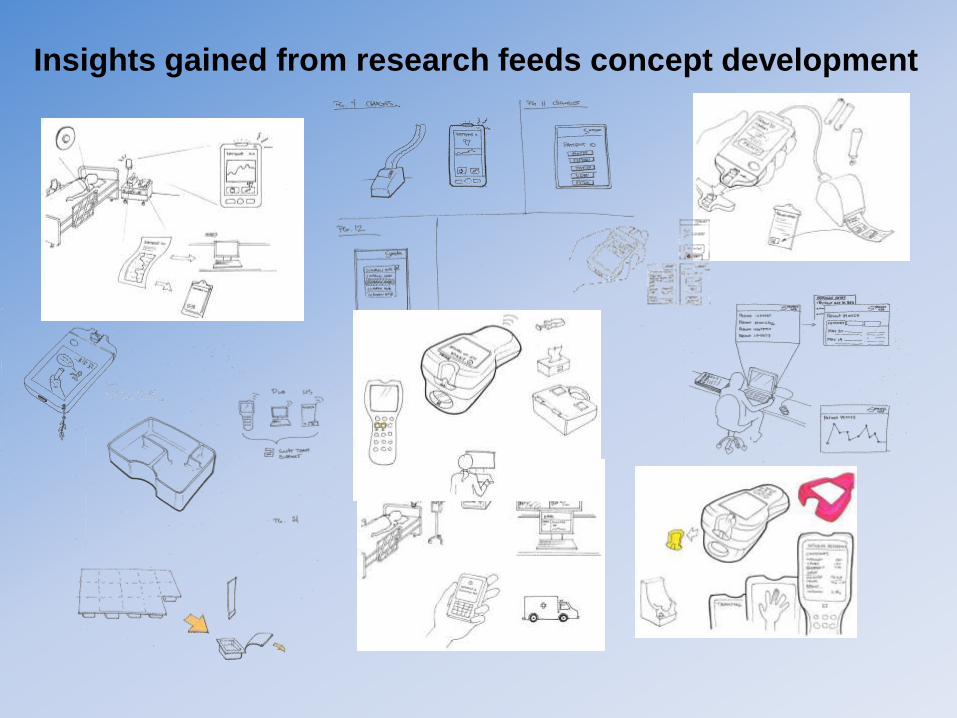
Insights gained from research feeds concept development

MK 2014 Manas Kanungo Confidential 22
Phase – 1B: Quantitative Definition
Fine-tune Product – Beta Units
Define Workflow, Target Market/s
Strategic Road-map, Business Proposal
Manas Kanungo Confidential 23

Page 24
Market Research: Phase 0 - 1B: 8 Countries, 44 Hospitals, 500+ HCPs
COUNTRIES Phase-0 Qualitative 7 Countries, 24 Hospitals, 126 HCPs
Phase-1A Qualitative 4 Countries, 20 Hospitals, 64 HCPs
Phase-1A Quantitative 227 Online Participants:
Decision Makers & Influencers
Phase-1B: 82 HCPs Sept GUI: 3 Countries
Sept Feedbacks: 5 Countries UK: Nov GUI, Dec Formative
In Field: 13 mths May – July ‘2010 Nov ’10 – Jan ‘11 May – June ‘11 Sept– Dec ‘11
UK • Frimley Hospital • Barnet Hospital • Kings Cross College
• Royal Free Hosp * Chlesea/ Westmr • North Middlesex * Kings College • Royal London Hosp * Homerton NHS
126 Admins, Purchasers; Nurses, POCCs, Lab,
Endos, Diabetologists
• Feedbacks: Sept 19 – 20 (3 POCCs) • GUI & Formative: 12 + 12 HCPs Nov 1-3; Dec 13-15
Germany • Charite Berlin * Martin-Luther • Vivantes * Diab Clinic Berlin
France • CHU Nantes • La Pitie Salpetriere • Ambroise Pare
• Le Havre Hospital • Reims Hospital • Bichat Hospital
• Feedbacks: Sept 22 – 23 (7HCPs)
China • Peking University Hospital • Shanghai Huashan • Shanghai No. 6 Hospital
• Feedbacks & GUI: Sept 26 – 30 (17 HCPs)
Japan • Japanese Red Cross Medical Center • Eiju General Hospital • Fukushima Medical University Hosp
• Feedbacks: Oct 4-6 (12 HCPs)
Brazil
• Santa Casa de Misericordia • Hospital Nipo Brasileiro • Hospital Clinicas • Hospital Alemao Oswaldo Cruz • Albert Einstein Hospital • Hospital Beneficia Portuguesa
• Darcy Vargas * Hospital Pasteur • Lefort • Sabara • Santa Paula • Pro-Cardiaco • HCN - Niteroi
101 Admins, Purchasers; Nurses, POCCs, Lab,
Endos, Diabetologists
• Feedbacks & GUI: Sept 26 – 30 (16 HCPs)
Canada • St. Mary’s Hospital Centre Montreal • Verdun Hospital Centre Montreal
• San Francisco: Dry Run Sept 1 (3 HCPs)
USA • RUSH Hospital Chicago • Montefiore, Bronx NY • MUSC, Charleston, SC • VA Hospital, Madison
Page 25
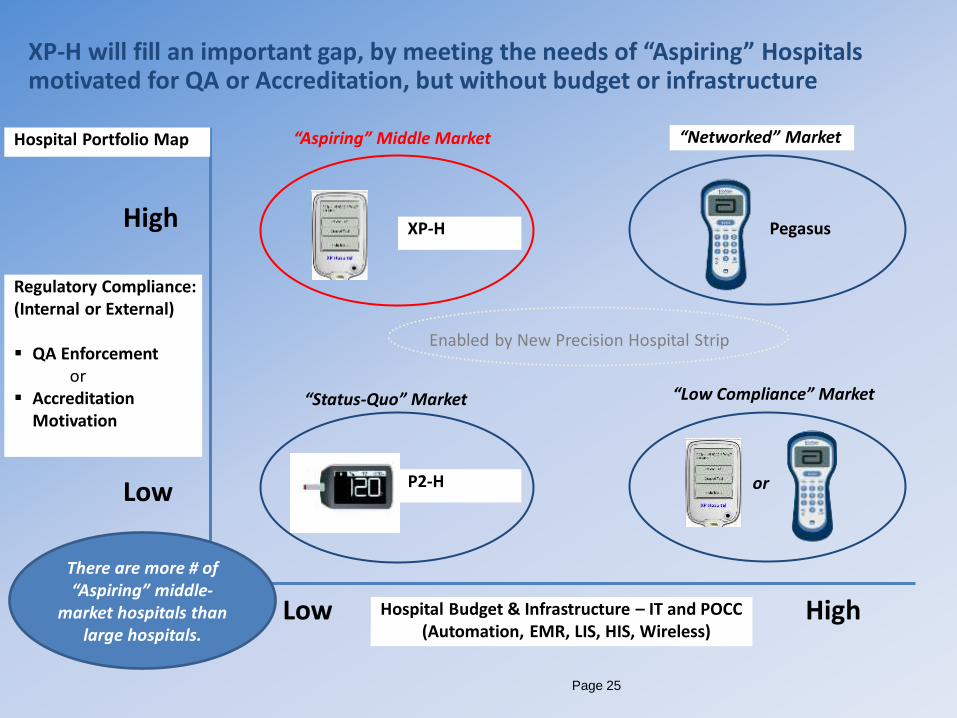
Regulatory Compliance: (Internal or External) QA Enforcement or Accreditation
Motivation
Hospital Budget & Infrastructure – IT and POCC (Automation, EMR, LIS, HIS, Wireless)
Low
XP-H Pegasus
P2-H
Enabled by New Precision Hospital Strip
“Aspiring” Middle Market “Networked” Market
“Status-Quo” Market
High
Low High
“Low Compliance” Market
or
XP-H will fill an important gap, by meeting the needs of “Aspiring” Hospitals motivated for QA or Accreditation, but without budget or infrastructure
Hospital Portfolio Map
There are more # of “Aspiring” middle-
market hospitals than large hospitals.
Page 26
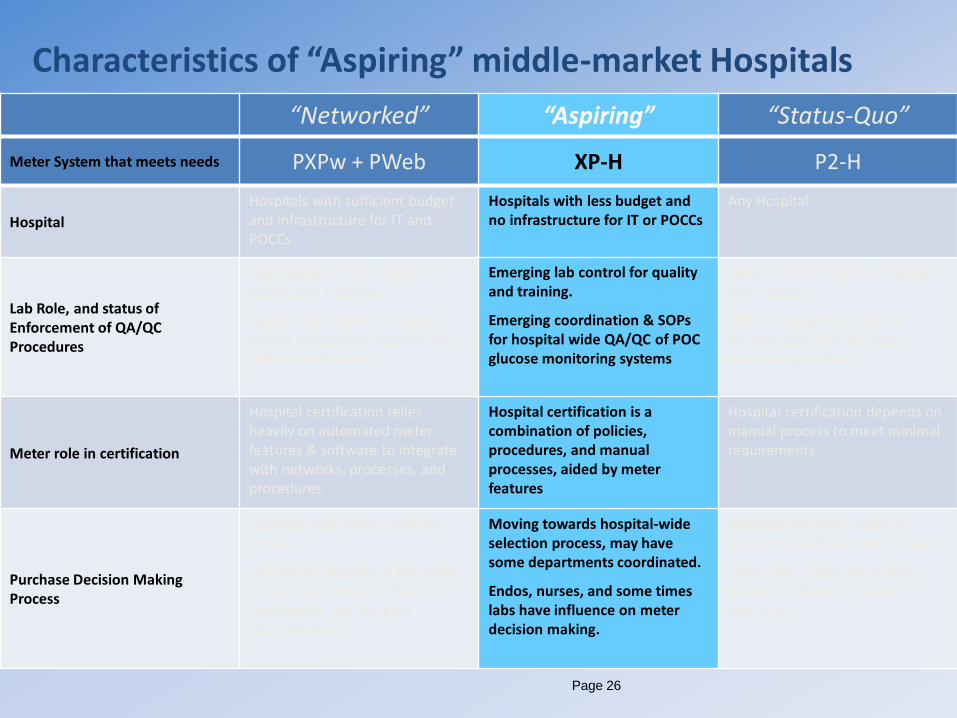
“Networked” “Aspiring” “Status-Quo”
Meter System that meets needs PXPw + PWeb XP-H P2-H
Hospital
Hospitals with sufficient budget and infrastructure for IT and POCCs
Hospitals with less budget and no infrastructure for IT or POCCs
Any Hospital
Lab Role, and status of Enforcement of QA/QC Procedures
High degree of lab control of quality and training.
QA/QC SOPs for POC glucose testing throughout hospital are highly coordinated.
Emerging lab control for quality and training.
Emerging coordination & SOPs for hospital wide QA/QC of POC glucose monitoring systems
Little or no lab control of quality and training.
Little or no QA/QC SOPs for hospital wide POC glucose monitoring systems
Meter role in certification
Hospital certification relies heavily on automated meter features & software to integrate with networks, processes, and procedures
Hospital certification is a combination of policies, procedures, and manual processes, aided by meter features
Hospital certification depends on manual process to meet minimal requirements
Purchase Decision Making Process
Hospital-wide meter selection process.
Individuals external to the point of use have primary influence (purchasing, lab, hospital administrator)
Moving towards hospital-wide selection process, may have some departments coordinated.
Endos, nurses, and some times labs have influence on meter decision making.
Purchase Decisions made by point-of-use department or ward.
Endos and nurses are primary decision makers for meter selection.
Characteristics of “Aspiring” middle-market Hospitals

Page 27
Users, Influencers, Decision Makers – “Personas”
Specialties Features Used
Hospital Administration
• Administrators • Department Managers • Audit Managers • Risk Managers
• All consolidated hospital-wide and location reports • Exception reports • Results Traceability – Patients, Hypo/Hyper, QC, • Benchmark performance • Operator Training Compliance • Strip inventory / usage summary stats, trend graph
Physicians • Endos • Diabetologists
• Patient results on meter, reports, with IDs • Hypo/Hyper alerts, readings, guidance for next steps
Laboratory • Lab Managers & Technicians • POCCs
• Meter set up • QC: readings, reminders, lockout, exception reports • Operator Training Compliance • Data export, consolidation, reports
Nurses
• Head Nurse • Floor / Ward Nurse • Diabetes Specialist Nurses (DSN) • Nurse / Health Care Assistants
• Perform patient tests, use results for therapy • Perform QC tests • Patient results w/traceability to record, act on • Operator Training Compliance • Guidance messages for next steps
Page 28
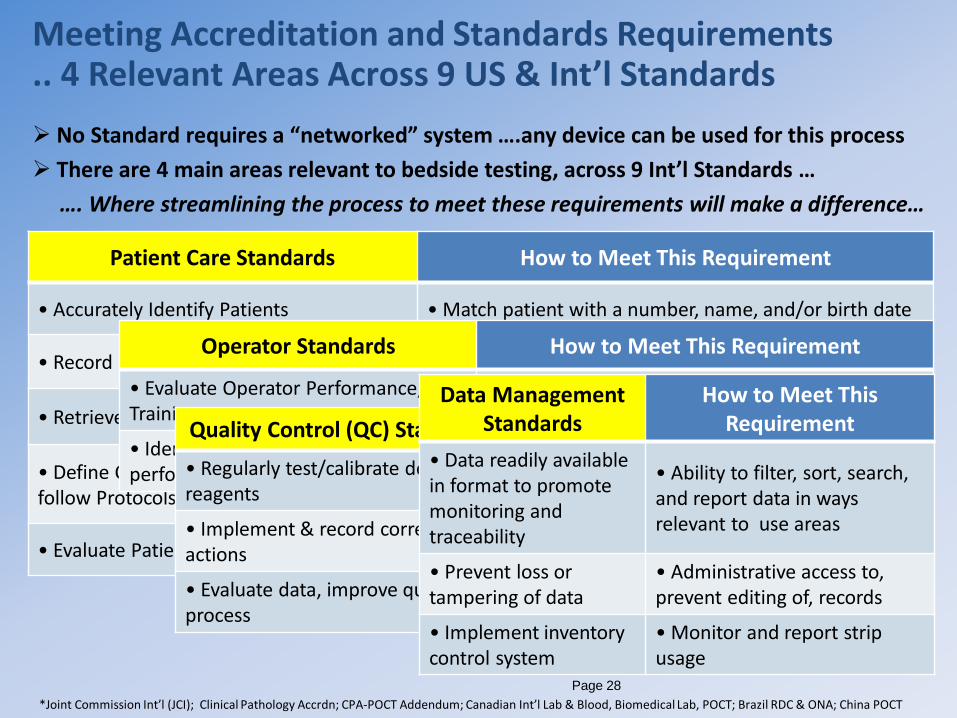
Meeting Accreditation and Standards Requirements .. 4 Relevant Areas Across 9 US & Int’l Standards
Patient Care Standards How to Meet This Requirement
• Accurately Identify Patients • Match patient with a number, name, and/or birth date
• Record Results for the right Patient • Enter and confirm Patient ID before testing
• Retrieve Patients’ Results • Search and retrieve patient results using IDs
• Define Critical Results & Guidelines, follow Protocols for Clinical Care
• Method to identify and alert out-of-range patient results, and provide guidelines for next steps
• Evaluate Patient data to Improve Care • Consolidate data, generate statistical & trend reports
*Joint Commission Int’l (JCI); Clinical Pathology Accrdn; CPA-POCT Addendum; Canadian Int’l Lab & Blood, Biomedical Lab, POCT; Brazil RDC & ONA; China POCT
No Standard requires a “networked” system ….any device can be used for this process
There are 4 main areas relevant to bedside testing, across 9 Int’l Standards …
…. Where streamlining the process to meet these requirements will make a difference…
Operator Standards How to Meet This Requirement
• Evaluate Operator Performance, Training
• Consolidate data, generate statistical & trend reports
• Identify Operator when test is performed
• Enter Operator ID before a patient or QC test
Quality Control (QC) Standards How to Meet This Requirement
• Regularly test/calibrate devices, reagents
• Perform, record regular QC tests on devices, reagents
• Implement & record corrective actions
• Prevent patient testing if QC fails; record & report data
• Evaluate data, improve quality of process
• Consolidate data, generate statistical & trend reports
Data Management Standards
How to Meet This Requirement
• Data readily available in format to promote monitoring and traceability
• Ability to filter, sort, search, and report data in ways relevant to use areas
• Prevent loss or tampering of data
• Administrative access to, prevent editing of, records
• Implement inventory control system
• Monitor and report strip usage

POC Lab Accuracy
Shazam H
Positioning & Differentiation
XXXXXXXXX
Page 30
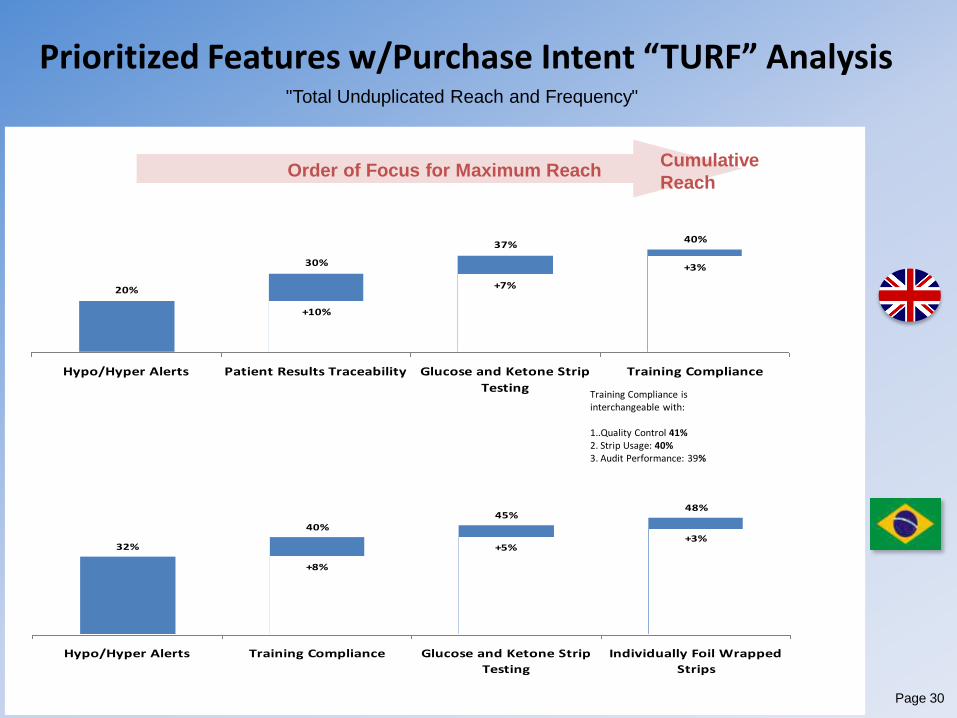
40%37%
30%
20%
+3%
+7%
+10%
Hypo/Hyper Alerts Patient Results Traceability Glucose and Ketone Strip
Testing
Training Compliance
Prioritized Features w/Purchase Intent “TURF” Analysis
Order of Focus for Maximum Reach Cumulative
Reach
48%45%
40%
32%+3%
+5%
+8%
Hypo/Hyper Alerts Training Compliance Glucose and Ketone Strip
Testing
Individually Foil Wrapped
Strips
Training Compliance is interchangeable with:
1..Quality Control 41% 2. Strip Usage: 40% 3. Audit Performance: 39%
"Total Unduplicated Reach and Frequency"
Page 31
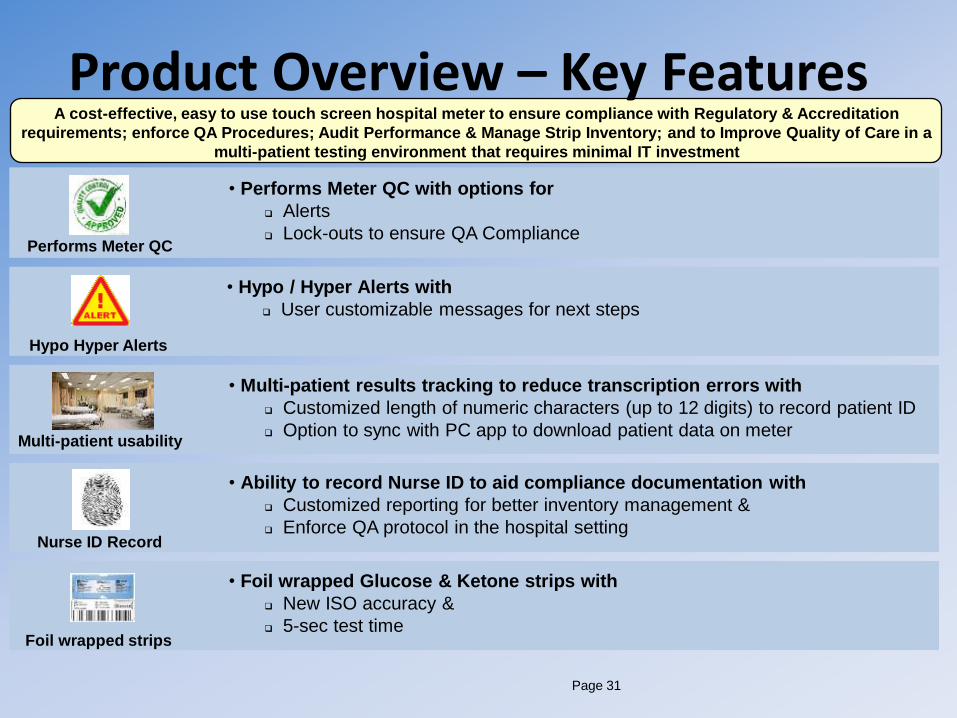
Product Overview – Key Features A cost-effective, easy to use touch screen hospital meter to ensure compliance with Regulatory & Accreditation
requirements; enforce QA Procedures; Audit Performance & Manage Strip Inventory; and to Improve Quality of Care in a
multi-patient testing environment that requires minimal IT investment
Performs Meter QC
Hypo Hyper Alerts
Multi-patient usability
Nurse ID Record
Foil wrapped strips
• Performs Meter QC with options for
Alerts
Lock-outs to ensure QA Compliance
• Hypo / Hyper Alerts with
User customizable messages for next steps
• Multi-patient results tracking to reduce transcription errors with
Customized length of numeric characters (up to 12 digits) to record patient ID
Option to sync with PC app to download patient data on meter
• Ability to record Nurse ID to aid compliance documentation with
Customized reporting for better inventory management &
Enforce QA protocol in the hospital setting
• Foil wrapped Glucose & Ketone strips with
New ISO accuracy &
5-sec test time

Page 32
Data Review Settings Test Menu
Main Menu
BETA UNITS, MENU OPERATION CLIA Waived, FDA Class-II, POC System for Hospitals, Clinics, POLs

Page 33
Work-flow: Patient Testing GUI

Page 34
Work-flow: QC Testing - GUI

Page 35
Patient & QC Reports via PC App
Page 36
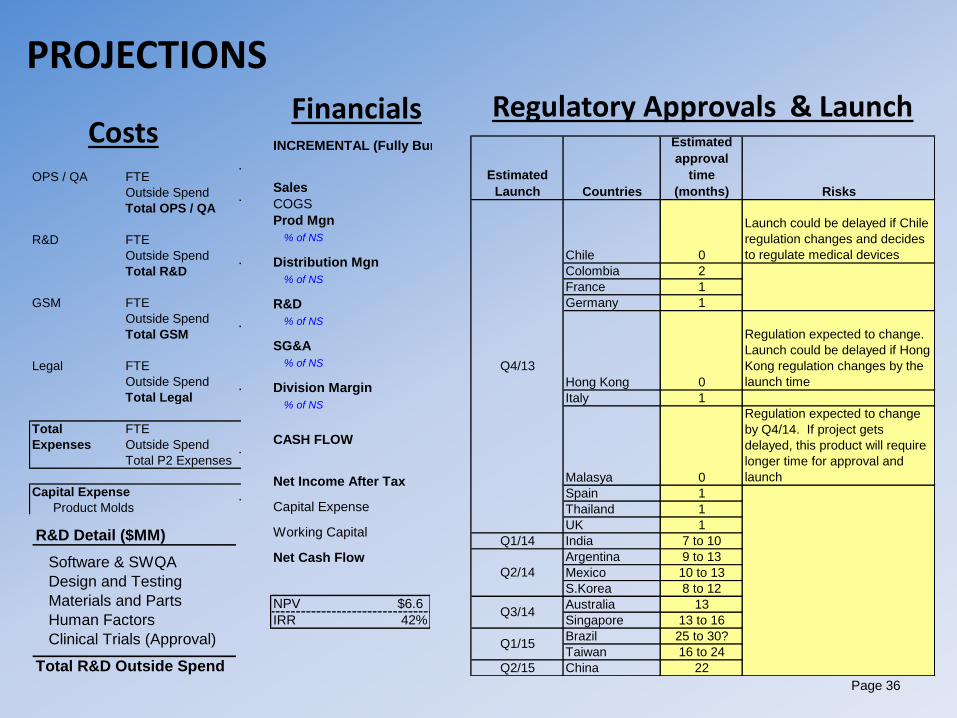
PROJECTIONS
Estimated
Launch Countries
Estimated
approval
time
(months) Risks
Chile 0
Launch could be delayed if Chile
regulation changes and decides
to regulate medical devices
Colombia 2
France 1
Germany 1
Hong Kong 0
Regulation expected to change.
Launch could be delayed if Hong
Kong regulation changes by the
launch time
Italy 1
Malasya 0
Regulation expected to change
by Q4/14. If project gets
delayed, this product will require
longer time for approval and
launch
Spain 1
Thailand 1
UK 1
Q1/14 India 7 to 10
Argentina 9 to 13
Mexico 10 to 13
S.Korea 8 to 12
Australia 13
Singapore 13 to 16
Brazil 25 to 30?
Taiwan 16 to 24
Q2/15 China 22
Q4/13
Q2/14
Q3/14
Q1/15
Total
2010 2011 2012 2013 Program
OPS / QA FTE - - - - -
Outside Spend - - 0.1 - 0.1 Capital Equipment Setup
Total OPS / QA - - 0.1 - 0.1
R&D FTE - 0.5 2.6 2.6 5.7 R&D, Ops/QA and NPI Proj Leadership HC
Outside Spend - 0.5 3.2 2.0 5.6 See Detail Below
Total R&D - 1.0 5.8 4.6 11.3
GSM FTE - 0.5 0.5 0.5 1.5
Outside Spend 0.6 0.2 0.3 1.2 2.3 Market Research, Toolkit Development
Total GSM 0.6 0.7 0.8 1.7 3.8
Legal FTE - - 0.1 0.1 0.2
Outside Spend - - 0.3 - 0.3 FTO / Patent Landscape
Total Legal - - 0.4 0.1 0.5
Total FTE - 1.0 3.2 3.2 7.4
Expenses Outside Spend 0.6 0.7 3.9 3.2 8.3
Total P2 Expenses 0.6 1.7 7.1 6.4 15.7
Capital Expense 2010 2011 2012 2013 Total
Product Molds - - 0.5 - 0.5
R&D Detail ($MM) 2012
Software & SWQA $1.5
Design and Testing 1.2
Materials and Parts 0.1
Human Factors 0.1
Clinical Trials (Approval) 0.4
Total R&D Outside Spend $3.2
Costs INCREMENTAL (Fully Burdened) P&L
2012 2013 2014 2015 2016 2017
Sales - 15.6 21.4 39.3 41.4 43.6
COGS - 4.5 5.1 10.1 11.5 11.7
Prod Mgn - 11.1 16.3 29.2 29.8 31.9
% of NS n/a 71% 76% 74% 72% 73%
Distribution Mgn (0.1) 9.5 14.2 25.2 25.7 27.5
% of NS n/a 61% 66% 64% 62% 63%
R&D 5.8 4.6 1.3 2.4 2.5 2.6
% of NS n/a 30% 6% 6% 6% 6%
SG&A 1.2 1.8 7.3 13.5 14.2 15.0
% of NS n/a 12% 34% 34% 34% 34%
Division Margin (7.1) 3.1 5.5 9.3 9.0 9.9
% of NS n/a 20% 26% 24% 22% 23%
CASH FLOW
2012 2013 2014 2015 2016 2017
Net Income After Tax (4.4) 1.9 3.4 5.8 5.6 6.1
Capital Expense (0.5) - - - - -
Working Capital 0.9 (3.1) (0.6) (2.6) (0.5) (0.2)
Net Cash Flow (4.0) (1.2) 2.9 3.2 5.1 5.9
NPV $6.6
IRR 42%
Financials Regulatory Approvals & Launch
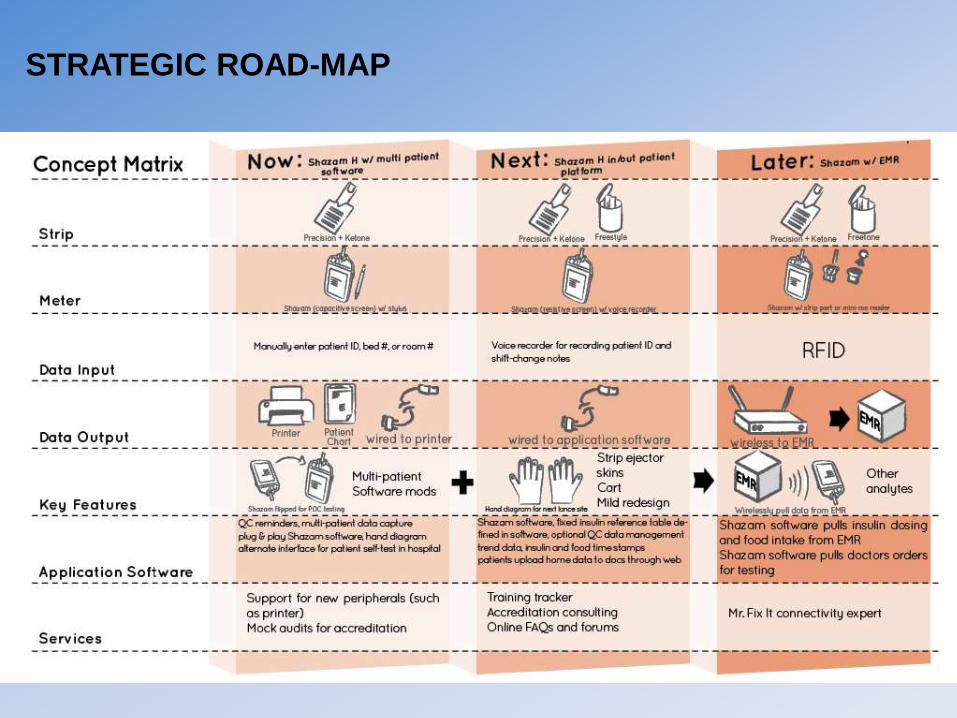
STRATEGIC ROAD-MAP