managing attendance line manager’s toolkit · policies are available on the trust intranet or...
TRANSCRIPT

Managing Attendance
Line Manager’s Toolkit
- 1 -
Managing Attendance Toolkit Version 2

Contents
Section Page 1 Introduction 3 Appendices 1 Leaflet for Managers to hand out to employees 5
2 Staff Counselling (Medra) 7 3 Guidance on Non-Essential Clinical Procedures 9
4 ESR 10 Self Certification form 10
5 Request for Management Referral / Sickness Absence Assessment from Occupational Health
12
6 Additional Information to Support Sickness Absence Review Assessment by Occupational Health
19
7 Return to Work Interview form 22 8 Tailored adjustment agreement Individually tailored reasonabl – e
adjustments 27
9 Return to Work - Assessment Resulting From GP Fit Note 33 10 HSE Return to work Questionnaire 35
11 ESR 11 Weekly Sickness Absence Return 38 12 Short-Term Sickness Absence Flowchart 39 13 Stage 1 Informal Counselling Flowchart 40 14 Stage 2 (Formal) Flowchart 41
15 Stage 3 (Formal) Flowchart 42 16 Stage 4 (Formal) Flowchart 43 17 Scheme of Delegation 44 18 Procedures to be used at Appeal Hearings 45 19 Equal Opportunities Monitoring form 47
- 2 -
Managing Attendance Toolkit Version 2

INTRODUCTION The toolkit includes a number of forms and documents to support you as a Line Manager to manage attendance in line with the Managing Attendance Policy HRP5. It is recommended that before you read this document you familiarise yourself with the Policy which is available on the internet. Please click on the link below to access the policy: www.wirralct.nhs.uk/document_uploads/Policies-HR/HRP5ManagingAttendancePolicynov11.pdf The forms and documents are as follows: Form/Document Description Leaflet for Managers to handout to staff titled ‘What to do if staff are too ill to come to work’
A template that can be used to send out to staff providing information on what to do if they are too ill to come to work
Staff Counselling (Medra) Counselling service that can be used for work, relationship or personal problems that may be affecting the individual’s ability to manage work
Guidance on Non Essential Clinical Procedures
This relates to Section 20 relating to Cosmetic Surgery and provides guidance on how to assess non-essential procedures in relation to staff taking time off for procedures
ESR 10 Self Certification form To be completed if the individual is absent due to sickness/accident for between 4-7 days
Request for Management Referral / Sickness Absence Assessment from Occupational Health
To be completed if a referral to occupational health is required
Additional Information to Support Sickness Absence Review Assessment by Occupational Health
To be completed when there has been a change in the individual’s circumstances / work duties/responsibilities that might impact on their ability to return to/continue with their normal work duties
Return to Work Interview form Must be completed following every occasion of sickness absence
Tailored adjustment agreement An agreement of tailored adjustments in the workplace for individuals with disabilities
- 3 -
Managing Attendance Toolkit Version 2

- 4 -
Managing Attendance Toolkit Version 2
Return to Work - Assessment Resulting From GP Fit NOTE
To be completed when Occupational Health advice is required following a member of staff being issued with a GP Fit Note
HSE Return to work Questionnaire Return to work questionnaire focuses on the HSE Stress Indicator factors. This can be used where an employee has been absent from work as a result of stress
ESR 11 Weekly Sickness Absence Return
To be completed by managers on a weekly basis reporting sickness absence in their department
Short - Term Sickness Absence Flowchart
A guide for managers on dealing with short-term absence
Stage 1 Informal Counselling Flowchart A guide for managers when dealing with the informal procedure
Stage 2 (Formal) Flowchart A guide for managers when dealing with the first formal stage of the procedure
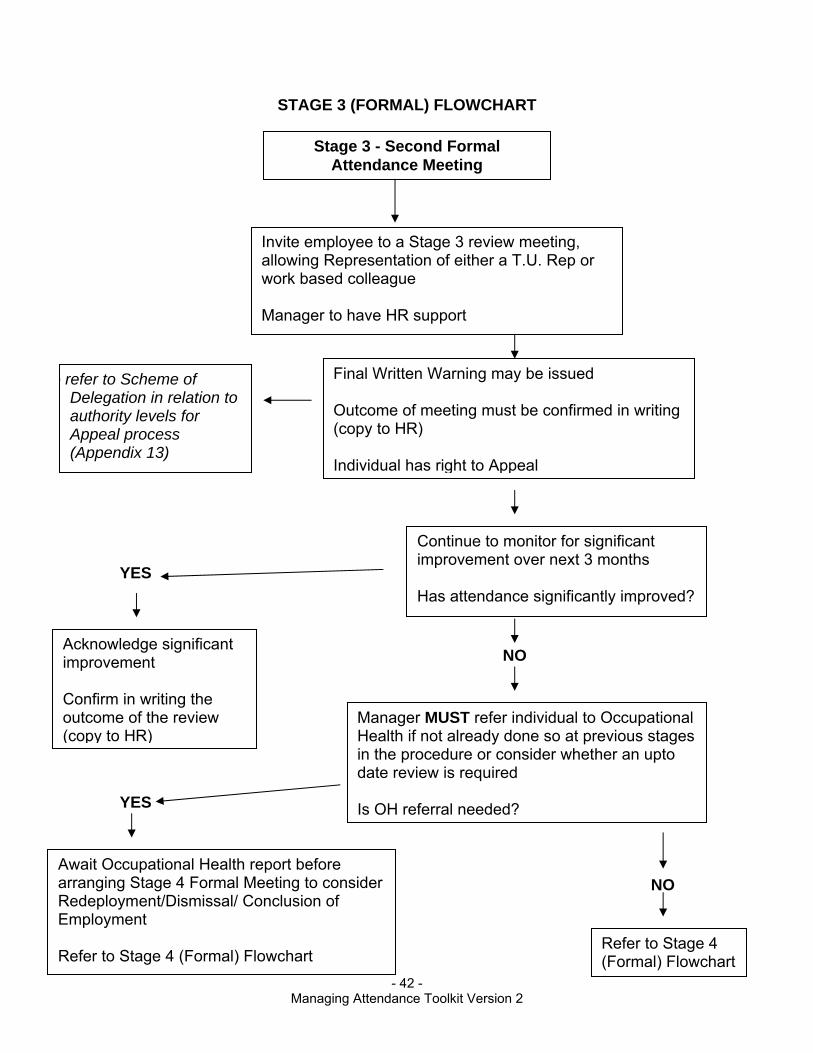
Stage 3 (Formal) Flowchart A guide for managers when dealing with the second formal stage of the procedure
Stage 4 (Formal) Flowchart A guide for managers when dealing with the final formal stage of the procedure
Scheme of Delegation Details the appropriate levels of authority to make a decision when issuing a sanction and/or considering dismissal within the policy
Procedures to be used at Appeal Hearings
Information on the procedure for appeal hearings
Equal Opportunities Monitoring form A form on ethnicity and disability to be completed by the Line Manager

- 5 -
Managing Attendance Toolkit Version 2
WHAT DO I DO IF I AM TOO ILL TO COME TO WORK
COMPLETE AS APPROPRIATE DEPARTMENT WE NEED TO KNOW! PLEASE DO THE FOLLOWING…….
COMPLETE AS APPROPRIATE DEPARTMENT CONTACT NUMBERS Name of contact Telephone number (s) If you have any queries regarding the managing attendance policy please do not hesitate to contact your Line Manager. The points highlighted in this leaflet are the main aspects of the Managing Attendance Policy. It is up to all individuals to familiarise themselves with all relevant Trust policies. Trust policies are available on the Trust intranet or hard copies are kept for staff to access in the department. Staff are able to access hard copies in their department.

- 6 -
Managing Attendance Toolkit Version 2
‘PLEASE WOULD YOU’ Ring work as soon as you know you will not be able to come
in, but definitely before the start of your shift. Normal working day contact number(s) are on the back page
of this leaflet. You must ask to speak to your Line Manager or the person
on duty in charge. Please state the broad nature of your medical condition. If
you wish this information to remain confidential from the contact person, please contact your department manager as soon as possible to discuss this.
Always inform us if your absence is related to a road traffic accident or an accident at work.
If you have a workplace accident or are absent following an incident at work you must complete an incident form at the time and discuss it with your Line Manager.
Please agree with your line manager how frequently you need to contact them throughout your absence (daily/weekly/monthly).
If you do not contact your manager regularly then they will contact you to gain an update on your progress.
It helps us if you can estimate when you are likely to return to work to enable cover to be arranged if necessary.
If you are unable to take your holiday due to sickness and wish to have your leave reimbursed you must inform your manager at the time. You must have provided a doctors fit note for this to be considered. Annual leave will not be reimbursed retrospectively (except in exceptional circumstances).
‘MEDICAL CERTIFICATES’ We will need a self certification note for absences of 4—7 days. A doctors ‘fit note’ is required from the 8th day of absence. Failure to provide medical certificates may result in unauthorised
unpaid absence.
All certificates are required to be addressed for the attention of …….Name/Department (complete as appropriate).
All staff have a return to work interview undertaken by their supervisor/team leader/manager (complete as appropriate) upon return to work.
This leaflet should be read in conjunction with the Managing Attendance Policy and Toolkit.
‘OCCUPATIONAL HEALTH’ OH offer confidential support to all staff. Your manager may
refer you if he/she feel it is appropriate. If you are off with a stress related issue, please talk to your
manager about being referred immediately to Occupational Health.
You will also be able to access the Staff Counselling service by accessing the following link www.medracounselling.com
Username WCNHST Password: support01

STAFF COUNSELLING SERVICE Medra provide a confidential staff counselling service. This service is open to all staff in Wirral Community NHS Trust. The service can be used for work, relationship or personal problems that may be affecting the individual’s ability to cope with their work. All counsellors are independent of the organisation and follow strict professional rules that safeguard their identity and the content of the sessions. To use the service staff should go to the ‘Staff Page’ on the Medra website; www.medracounselling.com and log in using the following username and password: Wirral NHS Community Trust Staff: Username: WCNHST Password: SUPPORT01
- 7 -
Managing Attendance Toolkit Version 2

- 8 -
Managing Attendance Toolkit Version 2

GUIDANCE ON NON ESSENTIAL CLINICAL PROCEDURES In relation to Section 20 of the Managing Attendance Policy relating to cosmetic surgery it states ‘Staff wishing to undertake medical treatment such as cosmetic surgery must take annual leave to do so. This would not ordinarily include reconstructive surgery or gastric band surgery. In order to assist Managers assess whether it is appropriate for staff to take annual to undertake medical treatments please see links below which provide a list of Procedures of Lower Clinical Priority. As guidance for Managers it is recommended that any treatment not funded or commissioned by the NHS would be classed as non-essential and therefore, staff would be expected to take annual leave for the time that they were absent from work. http://www.wirral.nhs.uk/document_uploads/Policies_Commissioning/CMWPLCPA-ZListJune2011fin_ca683.doc#AZlist http://www.wirral.nhs.uk/document_uploads/Policies_Commissioning/WirralPLCPPolicy.pdf Further advice or guidance should be sought from your HR Business Partner.
- 9 -
Managing Attendance Toolkit Version 2

- 10 -
Managing Attendance Toolkit Version 2
SELF CERTIFICATION ESR 10
If you are absent from work due to sickness/accident for between 4 – 7 days you should complete the details below and give to your line manager immediately. *please delete as necessary.
Strictly Confidential Employee to Complete Surname: ------------------------------- Forename(s) -------------------------- Title (Mr/Mrs/Miss/Ms) ---------------------- Date of birth: ----------------------- National Insurance --------------------- Payroll no. ---------------------- Number Address: ---------------------------------------------------------------------------------------- Doctor’s Name: Address: ------------------------------ --------------------------------------I confirm that I have been absent from my place of work due to illness/accident/incident at work/elsewhere* My first day of illness (DD/MON/YY) was My last day of illness (DD/MON/YY) was (Please note you may not know when your sickness will end) I returned to work on (DD/MON/YY) What date did you last work before your sickness began? (DD/MON/YY) The reason for absence was (please give brief description of illness/accident)* ------------------------------------------------------------------------------------------------------------- ------------------------------------------------------------------------------------------------------------ I consulted my Doctor on (DD/MON/YY)
(
D/MM/YY)

- 11 -
Managing Attendance Toolkit Version 2
I understand that Wirral Community NHS Trust may wish to contact my Doctor in respect of this absence. (This will be done via Occupational Health) I understand that to give false information on this form will be regarded as serious misconduct, which will result in disciplinary action being taken against me. Signed: ---------------------------------------------------------------------------------------- Date: ----------------------------------------------------------------------------------------
I am/am not* satisfied that the absence was justified and authorise/do not authorise* payment Reason for absence discussed Yes No Return to work interview completed Yes No (if applicable) Action Required Support required from Yes No n/a Occupational Health Support with flexible working Yes n/a Support with Risk Assessment/Health and Safety Yes No n/a Other (please state) --------------------------------------------------------------------- Signed: Date: --------------------------------------------------- ----------------------------- Line Manager: ------------------------------------------------------------------------------------- Once completed this form should be forwarded to the Payroll Department immediately
No
– Manager to Retain Copy
Manager use only

OCCUPATIONAL HEALTH DEPARTMENT
Request for Management Referral / Sickness Absence Assessment from Occupational Health
Please carefully complete the relevant information and then forward to your designated Occupational Health Department. Failure to do this will result in the form being returned and may lead to appointment allocation delays. (Manager guidance for completing Section E is available on the Trust intranet site and should be consulted where necessary prior to completion).
Employer:………………………………………………………………. (please clearly state Trust, PCT or Employing Organisation)
SECTION A – PERSONAL DETAILS OF EMPLOYEE Surname:.………………………………………… First name:……………….……………..… DOB: ………./………./………. Job Title:……………….………………… Home Tel No:…………………………………. Alternative contact: ……………………….. Employee Home Address:………………………………………………………………………………………...… …………………………………………..….… Postcode:…………………….…………………
SECTION B – EMPLOYMENT DETAILS Division: …………………………………… Employing Department:…….………………… Work Location:..……………………………… Contact No:……………………………............ Date of commencement in this Post: ………/………/………
Name of Manager:………………………………… Mgr Contact no: ……………………….
Managers Job Title:………...………….…………….. E-mail address: …………………….
- 12 -
Managing Attendance Toolkit Version 2
© Cheshire and Wirral Partnership NHS Foundation Trust

Managers Address details: ………...……………………………………………………… .……………………………………………………………….. SECTION C – CURRENT SICKNESS ABSENCE DETAILS 1. Is the employee currently on sick leave? Yes No
2. What is the expiry date of the current sick note? (if appropriate) ……………………………....... 3. Has this employee been referred previously in relation to this sickness/absence?
Yes No If yes, approximate date:…...……....….................................................. 4. Nature of absence: Short and frequent Long Both SECTION D PREVIOUS SICKNESS ABSENCE Please provide details of the employee’s absences for the past twelve months. (Please continue on a separate sheet if necessary) From To Total No. of Cause of Absence Days lost ……….. …. ……… …………….. ……………………………………………... ……….. …. ……… …………….. ……………………………………………... ……….. …. ……… …………….. ……………………………………………... ……….. …. ……… …………….. ……………………………………………...
–
SECTION E – DETAILS OF REASONS FOR REFERRAL 1. Give details of medical condition/reason for referral leading to referral: …………………………………………………………………………………………………
………………………………………………………………………………………………….
2. Has the individual seen their GP/healthcare professional in relation to this? Yes No Unsure 3. Please give details if you know what treatment or medication has been prescribed
- 13 -
Managing Attendance Toolkit Version 2
© Cheshire and Wirral Partnership NHS Foundation Trust

…………………………………………………………………………………………………….… ………….…………………………………………………………………………………………… 4. Is the employee awaiting results of treatments/tests or investigations? Yes No Don’t know 5. Is the problem related to an alleged Occupational Injury, accident or suspected Occupational disease? � Yes � No If Yes give details ……………………………………………………………………………………………… ……………………………………………………………………………………………… 6. If the illness or injury may be caused by, or made worse by work, please provide details, including a copy of the accident report form (IR1), COSHH data hazard sheet and appropriate risk assessment. ………………………………………………………………………………………………………. ……………………………………………………………………………………………………….
SECTION F – JOB ANALYSIS (refer to Manager Guidance for Completion) 1. What pattern of work does the employee undertake? (Please state number of hours worked
and tick all the appropriate shift(s)
Number of office hours ………………………… Number of on call hours ………………. Has any other pattern been discussed / agreed / refused: Yes No Please specify ………………………………………………………………………………………………...
2. Have any alterations or adaptations been made to the job to assist the employee? � Yes � No If yes tick box(s) to indicate which � Reduced hours � Redeployment � Redefined Duties � Use of special equipment � Phased return � Other Please give details:…………………………………………………………… ………………………………………………………………………………………………….. …………………………………………………………………………………………………..
.…
- 14 -
Managing Attendance Toolkit Version 2
© Cheshire and Wirral Partnership NHS Foundation Trust

…………………………………………………………………………………………………..
3. What are the specific requirements of the job? Tick the appropriate boxes and provide further details where necessary.
Requirements Yes Further Details
1.Manual Handling Patient Indicate S L M H V:*
Non Patient Indicate S L M H V:*
2. Care & responsibility 3. Direct Patient Contact 4. Display Screen Equipment
User under Regulations. Average daily length of time at PC:
- 15 -
Managing Attendance Toolkit Version 2
5. Exposure Prone Procedures 6. Biological Agents
State what agents:
7. Lone Worker 8. Night Work 9. Shift work 10. Colour differentiation 11. Food Handling 12. Hot / Cold environment
Details of temperature:
13. Hazardous Substances
State what substances:
14. Noise exposure
State what action level:
15. Vibration exposure
State what exposure value:
16. Fumes / Dust State :
17. Asbestos 18. Radiation
Ionising / Non-ionising / Lasers*
19. Driving car as integral part of job (not to & from work)
Other Driving LGV / FLT / PCV / * Other :
© Cheshire and Wirral Partnership NHS Foundation Trust

20. Work in confined spaces
21. Work at heights
22. Work with machinery
State:
23. Electrical work 24. Latex 25. Skin Irritants/Sensitisers
State what agents and exposure:
26. Respiratory sensitisers
State what agents and exposure:
4. Are there any outstanding employment matters that need to be identified
and / or discussed in relation to health? Yes No If yes, give details:…………………………………………………………………………………………
……………………………….……………………………………………………………………… Any other relevant information: .……………………………………………………………………………………………….…… …………………………………………………………………………………………………..… ………………………………………………………………………………………………………. SECTION G – REPORT CRITERIA Please tick ONLY those boxes relevant to the individual referral. This will allow the OH professional to provide you with a considered opinion to assist you in the management of the referred employee. 1. � What impact does the condition / illness have on the employee’s functional ability? 2. � In your opinion is the employee’s medical condition caused by or exacerbated by their job (including shift patterns/hours of work), working conditions and/or location? 3. � What is the likelihood of recovery / recurrence in the future? 4. � Is there any additional support the Trust could provide? 5. � Is the employee likely to be covered by the Disability Discrimination Act?
- 16 -
Managing Attendance Toolkit Version 2
© Cheshire and Wirral Partnership NHS Foundation Trust

6. � What is the employee’s current state of fitness to work? 7. � What is likely timescale for the employee to recover/return to work? Is the employee likely to return by (state date) …………..……...……………………… 8. � Would a phased return to work (covering hours worked) be appropriate? If so, what
measures should be put in place? 9. � Are there any short term (up to 1 month) reasonable adjustments/modifications to
duties/responsibilities which would alleviate the condition and facilitate the individual to return to/remain in work?
Please list any proposed or suggested restricted / modified duties available ……………………………………………………………………………………………………… ……………………………………………………………………………………….…………….. 10. � Are there any longer term reasonable adjustments that might be necessary? 11. � Are there any permanent longer term reasonable adjustments that might be necessary? 12. � Would redeployment be appropriate and if so, should it be on a temporary or permanent basis? 13. � a) As a contributor to the NHS pension scheme, Is the individual suitable for ill – health retirement? � b) As a non-contributor to the NHS pension scheme should the individual be considered for retirement on medical grounds? SECTION H – ADDITIONAL INFORMATION Please use this space to provide further relevant information e.g. relating to the individuals domestic / work situation or to request specific information from the Occupational Doctor/Health Adviser. ………………………………………………………………………………………………………. ………………………………………………………………………………………………………. ………………………………………………………………………………………………………. ……………………………………………………………………………………………………….
SECTION I – MANAGER INFORMATION AND SIGNATORY (MUST be same as details in Section B.) By signing below I confirm that:
- 17 -
Managing Attendance Toolkit Version 2 © Cheshire and Wirral
Partnership NHS Foundation Trust

• I have discussed the contents of the referral with the individual along with why it is being sought. • I have advised the individual that an appointment will be made for them to attend the Occupational Health Department for appropriate support and an independent opinion regarding their health. • I have advised the individual of their contractual obligation to attend. • I have advised the individual that following their consultation a report will be issued to myself and copied to them and Human Resources, regarding their fitness to work along with any appropriate recommendations for their work activity. • I have forwarded a copy of this form to the individual. In certain circumstances it may be necessary for the occupational health specialist to obtain further information from the individual’s General Practitioner or Specialist in order fully respond to the questions you have raised. Such requests can be subject to a fee in accordance with BMA guidelines. Please indicate below if you are happy to meet any such costs.
I am happy to meet any reasonable costs incurred (max £100) should a GP/Specialist report be necessary. (Further approval required for reports in excess of £100. Yes / No
Signed (manager):…………………………………………………………………… (Manager) Print name:………………………………………………………………………………………... Date: ……………../………………../………………
Please forward this form by post to your relevant Occupational Health Department. Please note: Incorrectly completed / incomplete forms will be returned. INSERT ‘ RETURN TO WORK ASSESSMENT RESULTING FROM GP FIT NOTE’
- 18 -
Managing Attendance Toolkit Version 2
© Cheshire and Wirral Partnership NHS Foundation Trust

VERSION 1
OCCUPATIONAL HEALTH DEPARTMENT
Additional Information to Support Sickness Absence Review Assessment by Occupational Health
This form should be completed when there has been a change in the individual’s circumstances / work duties/responsibilities that might impact on their ability to return to/continue with their normal work duties.
Please carefully complete the relevant information and send to your designated Occupational Health Department.
SECTION A – PERSONAL DETAILS OF EMPLOYEE Surname:.………………………………………… First name: …….…………………………..… DOB: ………./………./………. Contact No: ……………………………..…… Address: …………………………………………………………………………………………… Date of Occupational Health Review Appointment: ………………………………………………
SECTION B – EMPLOYMENT DETAILS Please provide details of any change in employment details since last appointment (i.e. department, work location, manager details, role/duties, hours/shifts etc). ………………………………………………………………………………………………………. ………………………………………………………………………………………………………. ………………………………………………………………………………………………………. Please tick if current restrictions are in place and you would like to know if these should continue.?
- 19 -
Managing Attendance Toolkit Version 2 © Cheshire and Wirral
Partnership NHS Foundation Trust

SECTION C – SICKNESS / ABSENCE DETAILS Please provide details of further sickness absence (nature, dates, duration etc) if relevant ………………………………………………………………………………………………………. ………………………………………………………………………………………………………. ……………………………………………………………………………………………………….
SECTION D – DETAILS OF MEDICAL CONDITION Please provide further details of medical condition resulting in the sickness/absence (only complete if this has changed since last occupational health assessment). ………………………………………………………………………………………………………. ………………………………………………………………………………………………………. ………………………………………………………………………………………………………. What is the expiry date of the current sick note? (if appropriate) ………………………...............
SECTION E – FURTHER INFORMATION Please use this space to provide further relevant information e.g. relating to the individuals domestic / work situation or to request specific information from the Occupational Physician/Adviser.
…………………………………………………………………….…………………………………
……………………………………………………………………………………………………….
……………………………………………………………………………………………………….
SECTION F – MANAGER INFORMATION AND SIGNATORY (tick boxes to confirm/accept)
By signing below I confirm that:
I have discussed the contents of this document with the individual and the reasons for its’ provision.
I have advised the individual that a review appointment will be made for them to attend the Occupational Health Department for appropriate support and an independent opinion regarding their health.
- 20 -
Managing Attendance Toolkit Version 2 © Cheshire and Wirral Partnership NHS Foundation Trust

I have advised the individual of their contractual obligation to attend and that following
their consultation a report will be issued to myself and copied to them and Human Resources, regarding their fitness to work along with any appropriate recommendations for their work activity.
I have forwarded a copy of this form to the HR department and the individual.
In certain circumstances it may be necessary for the occupational health specialist to obtain further information from the individual’s General Practitioner or Specialist in order fully respond to the questions you have raised. Such requests can be subject to a fee in accordance with BMA guidelines. Please indicate below if you are happy to meet any such costs.
I am happy to meet any reasonable costs incurred (max £100) should a GP / Specialist report be necessary. (Further approval required for reports in excess of £100. Yes / No Signed (manager):……………………………………………………………..……… (Manager) Print name: ……………………………………………………….. Date: …..…./………/….... Please forward this form by post to your relevant Occupational Health Department
- 21 - Managing Attendance Toolkit Version 2
© Cheshire and Wirral Partnership NHS Foundation Trust

- 22 -
Managing Attendance Toolkit Version 2
RETURN TO WORK INTERVIEW FORM
Interview MUST be undertaken following every occasion of sickness absence
Name: Department:
Job Title: Date:
Sickness Period from: Interview Conducted by:
Last day of Sickness: No. of occasions absent within last 12 months:
Total number of work Total No. of work days absent days absent: within last 12 months:
Sickness Reason: Sickness Absence History over last twelve months * Please complete this section in advance of your discussions with the employee Date From Date to Number of days Reason
Please attach an additional sheet if required.
Questions How are you feeling now? Have you suffered from this condition before?
Yes No □ □
If so, when?
Have you seen your GConsultant/Dentist or other?
Yes No □ □
If yes, with whom and was treatment given?

Brief details of advice given by GP / Consultant / Dentist etc? Please indicate/circle if sickness was: Uncertified / Self Certified / Medical Certificate / Fit Note Has your GP/Dentist/ Consultant etc… confirmed you are fit to return to work? Are you fit for full duties? (list any restrictions to be considered)
Yes No □ □ Yes No □ □
Was your absence due to an accident, injury or incident that occurred at work? If yes, have you completed an incident form? If yes, has a RIDDOR been completed?
Yes No □ □ Yes No □ □ Yes No □ □
If yes, give details
Are you receiving any ongoing treatment or medication (i.e. tablets, medicine) resulting from your condition?
Yes No □ □
If yes, give details
Will the medication affect your performance at work, or be a safhazard?
Yes No □ □
If yes, please specify.
Is there anything the Trust could do to support you? i.e. the need for support fany other source e.g. OCounselling/ Return to Work Risk Assessment
Yes No □ □
If yes, please specify.
Has the employee followed the correct procedure for notifying their absence? YES NO If No then explain the correct procedure and why it has to be followed.
- 23 -
Managing Attendance Toolkit Version 2

Returning to Work from a period of Long Term Sickness (over 4 weeks) Has a phased return to work been considered/implemented? * Normally up to 2 weeks, if extension to 4 weeks is required authorisation must be sought from Director of HR & Corporate Affairs or Head of HR
Yes No □ □
If phased return to work has been agreed, give/attach details of hours / days /pattern of hours agreand period after that this will be reviewed. If reasonable adjustments e.g. to the workplace/duties are to be made, please give/attach details: Has the member of staff missed any important information whilst he/she has been absent? Yes/No (give details overleaf if necessary) Additional Comments or Details of Further Action attach overleaf e.g. appointment with OH, follup/review meeting, formal interview to discuss sickness absence levels, review of working arrangements…
Managers Prompt Try to uncover any underlying health issues and ask what the employee is doing to ensure they are fit for work in the future. Examples include wellbeing, relationships at work, motivation, issues outswork and workload. Discussions/Agreed Actions:
Managers Comments Comments by Manager: Name: Department: Signature: Date:
- 24 -
Managing Attendance Toolkit Version 2

Employee’s Comments Comments by Employee: Name: Department: Signature Date:
ORIGINAL TO STAY ON FILE & COPY TO BE PROVIDED TO INDIVIDUAL
- 25 -
Managing Attendance Toolkit Version 2

- 26 -
Managing Attendance Toolkit Version 2
RETURN TO WORK INTERVIEW
Continuation Sheet No.
Name:
ORIGINAL TO STAY ON FILE & COPY TO BE PROVIDED TO INDIVIDUAL
Employee’s Signature: Date: Manager’s Signature: Date:

Tailored adjustment agreement – Individually tailored reasonable adjustments This ‘Tailored adjustment agreement’ is a living record of reasonable adjustments agreed between a disabled employee and their line manager. The purpose of this agreement is to
Ensure that both parties, the individual and the employer, have an accurate record of what has been agreed.
Minimise the need to re-negotiate reasonable adjustments every time the employee changes jobs, is re-located or assigned a new manager within the organisation.
Provide employees and their line managers with the basis for discussions about reasonable adjustments at future meetings.
This is a live document and should be reviewed regularly by both the employee and manager and amended as appropriate. Remember, however, that expert advice from third parties, such as occupational health advisers, Access to Work or IT specialists may be needed before changes can be agreed and implemented. Managers who need help in deciding whether or not an adjustment is reasonable will find it helpful to use the Reasonable Adjustment Request Form available at: www.efd.org.uk/publications/line-manager-guide or from the Disability Directions team at Employers’ Forum on Disability. New managers of employees with such ‘Tailored adjustment agreements’ should accept the adjustments outlined in the agreement as reasonable and ensure that they continue to be implemented. The agreement may need to be reviewed and amended at a later date but this should not happen until both parties have worked together for a reasonable period of time. The agreement allows the employee to:
Explain the impact of their disability on them at work. Suggest adjustments that will make it easier for them to do their job. Offer further information from their doctor, specialist or other expert. Request an assessment by occupational health, Access to Work or another expert. Review the effectiveness of the adjustments agreed. Explain any change in their circumstances. Be reassured that their manager knows what to do if they become unwell at work and who to contact if necessary. Know how and when their manager will keep in touch with them if they are absent from work because of illness or a disability related reason.
• • • •
• • •
•
- 27 -
Managing Attendance Toolkit Version 2

The agreement allows the line manager to:
Understand how a particular employee’s disability affects them at work. Explain the needs of the business or organisation. Explain the organisation’s attendance and reasonable adjustment policy. Recognise signs that an employee might be unwell and know what the employee wants you to do in these circumstances including who to contact for help. Know how and when to stay in touch if the employee is off sick. Consider whether or not the employee needs to be referred for an assessment by an occupational health or another adviser to help both parties understand what adjustments are needed. Review the effectiveness of the adjustments already agreed. Explain any change in the employer’s circumstances.
Tailored adjustment agreement This is a record of the reasonable adjustments agreed between [employee’s name] and [line manager name] This agreement may be reviewed and amended as necessary with the agreement of both parties:
At any regular one-to-one meeting. At a return to work meeting following a period of sickness absence. At six monthly and/or annual appraisals. Before a change of job or duties or introduction of new technology or ways of working. Before or after any change in circumstances for either party.
• • • •
• •
• •
• • • •
•
Employee - My disability in the workplace My disability has the following impact on me at work
I need the following agreed reasonable adjustments (refer to
Date budget holder contacted if relevant
Date implemented:
- 28 -
Managing Attendance Toolkit Version 2

Access to Work agreement if relevant)
Wellness at work – employees who have fluctuating mental or physical disabilities On a ‘good day’ my disability has the following impact on me at work When things are breaking down. The following symptoms are indications that I am not well enough to be at work Emergency contacts
- 29 -
Managing Attendance Toolkit Version 2

If I am not well enough to be at work I am happy for my line manager to contact any of the following emergency contacts in the order of preference indicated below Please add, amend or delete types of contacts as appropriate GP (preference X)
Care co-ordinator (preference X)
Name: Surgery: Telephone: Address:
Name: Telephone: Mobile: Address:
Relative (preference X) Specialist (preference X) Name: Relation to me: Telephone: Mobile: Address:
Name: Telephone: Mobile: Address:
Friend (preference X) Other (preference X)
Name: Telephone: Mobile: Address:
Name: Telephone: Mobile: Address:
- 30 -
Managing Attendance Toolkit Version 2

I will let you know if there are changes to my condition, which have an effect on my work and/or if the agreed adjustments are not working. We will then meet privately to discuss any further reasonable adjustments or changes that should be made. If you notice a change in my performance at work or feel these reasonable adjustments are not working I would be happy to meet you privately to discuss what needs to be done. Line manager - Keeping in touch If you are absent from work on sick leave or for a reason relating to your disability for more than [x] days and have followed the usual procedures for notifying the organisation of your absence I will keep in contact with you in the following way:
Who will contact whom?
How will contact be made? (email, telephone, text, letter, minicom)
How often? (daily, weekly, monthly)
When? (preferred day, preferred time)
- 31 -
Managing Attendance Toolkit Version 2

- 32 -
Managing Attendance Toolkit Version 2
Conversations while you are on sick leave Return to work When you are ready to return to work after a period of sickness or disability related absence of more than [x] days we will meet to review this agreement and make any necessary amendments. At this return to work meeting we will also discuss:
Unauthorised absences from work If you are absent from work and have not followed usual procedures for notifying us that you are sick or absent for a reason relating to your disability we have agreed that I will do the following: An up to date copy of this form will be retained by employee/line manager/HR. A copy of this form may also be given to a new or prospective line manager with the prior consent of the employee. Employee signature: Date: Employer signature: Date:
These are topics we have agreed we will discuss while you are absent, for example:
How are you feeling. What I can do to help. Current work. Planned phased return to work Return to work date etc…
For example: Current work issues. A phased return/back to work plan. What to tell the team. Assessments to review existing reasonable adjustments
(Access to Work, GP, occupational health) and identify new adjustments that might be needed etc
For example;
Try to contact you on your mobile and/or notify your emergency contact whose up to date details are as follows:

OCCUPATIONAL HEALTH DEPARTMENT
Return to Work Assessment Resulting From GP Fit NOTE
This form should be completed when Occupational Health advice is required following a member of staff being issued with a GP Fit Note whereby adjustments recommended by the GP cannot be accommodated:
Please carefully complete the relevant information and forward to your designated Occupational Health Department along with a copy of the GP Fit Note.
SECTION A – PERSONAL DETAILS OF EMPLOYEE Surname:.………………………………………… First Name:…….………….………………… DOB: ………./………./………. Contact No: ……………….……………….. Address: ………………………………………………………………………………………… Job Role: ……………………………………….. Contracted Hours: …………………………… Service Line: ……………………………………. Work Base: ……………………………….
SECTION B – REASONS FOR OH ADVICE BEING SOUGHT Please provide details of any recommendation suggested by the GP that cannot be accommodated and reasons why and/or suggested alternatives: (i.e. role/duties, hours/shifts etc). ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………
SECTION C – SICKNESS / ABSENCE DETAILS Please provide details of reason for current absence (nature, dates, duration etc) and any previous relevant absence where indicated: …………………………………………………………………………………………………… ………………………………………………………………………………………………………
- 33 -
Managing Attendance Toolkit Version 2 © Cheshire and Wirral Partnership NHS Foundation Trust

……………………………………………………………………………………………………… ……………………………………………………………………………………………………… SECTION D – FURTHER INFORMATION Please use this space to provide further relevant information.
……………………………………………………………………………………………………… ……………………………………………………………………………………………………… ……………………………………………………………………………………………………… ………………………………………………………………………………………………………
SECTION E – MANAGER INFORMATION AND SIGNATORY (tick boxes to confirm/accept By signing below I confirm that:
I have discussed the contents of and reason for this referral document with the individual. I have advised the individual that an appointment will be made for them to attend the
Occupational Health Department for additional advice/support and an independent opinion regarding their ability to return to work and any potential adjustments that might be required.
I have advised the individual of their contractual obligation to attend and that following their consultation a report will be issued to myself and copied to them, their GP and the Trust’s Human Resources department, regarding their fitness to work along with any appropriate recommendations for their work activity.
In certain circumstances it may be necessary for the occupational health specialist to liaise further with the individual’s Specialist. Such requests can be subject to a fee in accordance with BMA guidelines. Please indicate below if you are happy to meet any such costs.
I am happy to meet any reasonable costs incurred (max £100) should a Specialist report be necessary. (Further approval required for reports in excess of £100. Yes / No
Signed (manager):………………………………………………………………………………… (Manager) Print name: ………………………………………………………. Date: ………./………/…….. Please forward this form by post to your relevant Occupational Health Department.
- 34 -
Managing Attendance Toolkit Version 2 © Cheshire and Wirral Partnership NHS Foundation Trust

- 35 -
Managing Attendance Toolkit Version 2
work questionnaire Cause of stress
you? Use this space to detail what the problem was. If it was not a problem leave it blank
done about it? Can we make any adjustments?
Return to Question Was it a problem for What can be
Did different people at work demand things from you that were hard to combine?
Did you have unachievable deadlines?
Did you have to work very intensively?
Did you have to neglect some tasks because you had too much to do?
Were you unable to take sufficient breaks?
Did you feel pressured to work long hours?
Did you feel you had to work very fast?
Demands
Did you have unrealistic time pressures?
Could you decide when to take a break?
Did you feel you had a say in your work speed?
Did you feel you had a choice in deciding how you did your work?
Did you feel you had a choice in deciding what you did at work?
Did you feel you had some say over the way you did your work?
Control
Did you feel your time could be flexible?

Did your manager give you enough supportive feedback on the work you did?
Did you feel you could rely on your manager to help you with a work problem?
Did you feel you could talk to your manager about something that upset or annoyed you at work?
Did you feel your manager supported you through any emotionally demanding work?
Support* (Manager)
Did you feel your manager encouraged you enough at work?
Did you feel your colleagues would help you if work became difficult?
Did you get the help and support you needed from your colleagues?
Did you get the respect at work you deserved from your colleagues?
(Peers)
Were your colleagues willing to listen to your work-related problems?
Were you clear about what was expected of you at work?
Did you know how to go about getting your job done?
Were you clear about what your duties and responsibilities were?
Were you clear about the goals and objectives for this department?
Relationships*
Did you understand how your work fits into the overall aim of the organisation?
Did you have enough opportunities to question managers about change at work?
Change
Did you feel consulted about change at work?
- 36 -
Managing Attendance Toolkit Version 2

- 37 -
Managing Attendance Toolkit Version 2
When changes were made at work, were you clear about how they would work out in practice?
Other issues
Is there anything else that was a source of stress for you, at work or at home, that may have contributed to you going off work with work-related stress?

** Week Ending
Division
Sub Division/Area
Service
Department/Team
Department/Team Headcount - WTE * Please refer to Payroll Paypoint box below** Please refer to Week Ending (WE) box above
*Payroll Paypoint:(found oneg 660 z 8720
M T W T F S S
Certified Correct:
Please indicate 'YES/NO' if this
absence is confirmed/suspe
cted swine flu
Work Related?
(Y/N)
WEEKLY SICKNESS ABSENCE RETURN
This return should be emailed to the Payroll department ([email protected]) on Monday of every week showing details of all sickness absence from the previous week. The subject line of the email must read ' 660 z xxxx* WE xx/xx/xx** '. Nil Returns are required. Self
certificates and/or medical certificates should accompany the SAR return to Payroll. For convenience, an electronic version of th Inland Revenue self certificate is embedded within this document. There is also an absence
categorisation help sheet to ensure you categorise the absence correctly.
660 z Sickness absence is monitored on a 7 day calendar week, therefore if an employee has not returned to work after an absence by the end of a working week/shift, the last day should be left blank and completed the following week.
Employee Name Employee No.First Day of
sicknessLast Day of
sickness
Please tick (or selct the symbol from the list) for each day of
absence
Hours off
Please select ESR code/description from the
absence categorisation help list.
Certificates received
Designation:
- 38 -
Managing Attendance Toolkit Version 2

- 39 -
Managing Attendance Toolkit Version 2
SHORT-TERM SICKNESS ABSENCE FLOWCHART
YES NO
Employee is absent from work
Carry out Return to work interview (Appendix 7)
Carry out a Return to work interview (Appendix 7)
On receipt of the OH report and return to work, carry out a Return to Work Interview on return (Appendix 7) Consider whether to complete HSE Return to Work Questionnaire (Appendix 10), if appropriate
Manager recognises from monitoring that employee has reached the trigger point
(12 working days or 3 occasions or more within a 12 month period)
If a psychological problem is identified, an immediate Occupational Health referral should be discussed with individual Provide a MEDRA staff counselling leaflet Refer to HRP29 Stress Management Policy
Consider whether employee needs any support May need to refer to other HR policies which are available on the intranet e.g. HRP6 Flexible Working Policy etc…
Consider whether employee needs any support May need to refer to other HR policies which are available on the intranet e.g. HRP6 Flexible Working Policy etc…
please refer to Stage 1 Informal Counselling Flowchart and consider any recommendations
Refer to Stage 1 Informal Counselling Flowchart

- 40 -
Managing Attendance Toolkit Version 2
STAGE 1 INFORMAL COUNSELLING FLOWCHART YES NO
NO YES
NO YES
Manager to fact find to establish the cause of sickness Review the employees’ whole sickness record within the last 12 months Consider whether to provide MEDRA staff counselling leaflet
Manager to consider whether it’s appopriate to refer the employee to Occupational Health?
Await Occupational Health report & arrange Informal Counselling Meeting between Manager/individual to discuss report and sickness absence Counselling session and details of the review period should be recorded (copy to employee & HR)
Discussion over significant improvement expected over next 3 months Counselling session and details of the review period should be recorded on the Return to Work Interview Form (copy to employee & HR)
Monitor improvement over next 3 months. Has attendance significantly improved?
Is an Occupational Health referral necessary?
Acknowledge significant improvement Confirm in writing the outcome of the review (copy to HR)
Await Occupational Health report before arranging Stage 2 Second Formal Meeting. Refer to Stage 2 (Formal) Flowchart
Refer to Stage 2 (Formal) Flowchart

- 41 -
Managing Attendance Toolkit Version 2
STAGE 2 (FORMAL) FLOWCHART
NO YES
YES NO
Stage 2 - First Formal Attendance Meeting
Invite employee to a Stage 2 review meeting, in writing, allowing representation of either a T.U. Rep or work based colleague Manager to have HR support
First Written Warning may be issued Outcome of meeting must be confirmed in writing (copy to HR) Individual has ri
o refer to Scheme of Delegation in relation to authority levels for Appeal process (Appendix 13)
ght to Appeal
N Continue to monitor for significant improvement over next 3 months Has attendance significantly improved?
Is an Occupational Health referral
Acknowledge significant improvement Await Occupational Health report before
arranging Stage 3 Second Formal Meeting. Refer to Stage 3 (Formal) Flowchart
Confirm in writing the outcome of the review (copy to HR)
Refer to Stage 3 (Formal) Flowchart
- 42 -
Managing Attendance Toolkit Version 2
STAGE 3 (FORMAL) FLOWCHART YES
NO
YES
NO
Stage 3 - Second Formal Attendance Meeting
Invite employee to a Stage 3 review meeting, allowing Representation of either a T.U. Rep or work based colleague Manager to have HR support
Final Written Warning may be issued Outcome of meeting must be confirmed in writing (copy to HR) Individual has right to Appeal
o refer to Scheme of Delegation in relation to authority levels for Appeal process (Appendix 13)
Continue to monitor for significant improvement over next 3 months Has attendance significantly improved?
Acknowledge significant improvement Confirm in writing the outcome of the review Manager MUST refer individual to Occupational
Health if not already done so at previous stages in the procedure or consider whether an upto date review is required Is OH referral needed?
(copy to HR)
Await Occupational Health report before arranging Stage 4 Formal Meeting to consider Redeployment/Dismissal/ Conclusion of Employment Refer to Stage 4 (Formal) Flowchart
Refer to Stage 4 (Formal) Flowchart

- 43 -
Managing Attendance Toolkit Version 2
STAGE 4 (FORMAL) FLOWCHART
Stage 4 Formal Meeting
Redeployment/Dismissal/ Conclusion of Employment
Invite employee to a Final review meeting, allowing representation of either a T.U. Rep or work based colleague Manager to have HR support
A decision on Redeployment/ Dismissal/Conclusion of employment may be taken Outcome of meeting must be confirmed in writing (copy to HR) Individual has right to appeal
o refer to Scheme of Delegation in relation to authority to dismiss and Appeal process
Dismissal/Conclusion of Employment
Redeployment
Individuals will be given a maximum of 3 months on the redeployment register, where they will have access to jobs on a restricted basis. If at the end of the 3 months they have not secured an alternative post, then their employment will end
Employee should be given notice as per their contract of employment ESR forms to be completed and sent to HR

- 44 -
Managing Attendance Toolkit Version 2
SCHEME OF DELEGATION
Category of Staff
Issue of First
Written Warning By:
Appeal to: Issue of Final
Written Warning By:
Appeal to: Issue of Dismissal/Conclusion
of Employment By:
Appeal to:
Chief Executive (CEO)
Chairman Designated Non-Executive Wirral Community NHS Trust member
Chairman Designated Non-Executive Wirral Community NHS Trust member
Chairman Designated Non-Executive Wirral Community NHS Trust Member
Executive
Directors
Chief Executive Chairman Chief Executive Chairman Chief Executive Chairman or Designated Non- Executive
Other staff directly responsible to the CEO
Chief Executive Chairman Chief Executive Chairman Chief Executive Chairman or Designated Non- Executive
Medical & Dental staff (i.e. Doctors & Dentists)
Head of Service Medical Director Head of Service Medical Director
Head of Service CEO
All other staff
Immediate Manager
Head of Service or Designated representative
Next level Manager above Immediate Manager
Head of Service or Designated representative
Head of Service or Designated representative
Director
Notes 1. In the event that Chairman is not available, the role of the Chairman may be undertaken by a designated representative. 2. In all instances involving the Chairman, Chief Executive or Executive Directors, discussion will first take place with Wirral
Community NHS Trust’s Director of HR & Corporate Affairs. 3. In relation to appeals against any dismissal/conclusion of employment, the appeal panel will be heard by 1 Non-Executive
Director and 2 other Directors, not previously involved will in the case.

PROCEDURES TO BE USED AT MANAGING ATTENDANCE APPEAL HEARINGS An Appeal Panel will consist of at least 3 panel members: The Chairperson of the Panel shall: Introduce all present Explain that the purpose of the Appeal Hearing and decide if the original decision should
be supported, revoked or amended Explain the format of the Appeal Hearing 1. Management Presentation of Case
(a) The manager or management representative shall state the case in the presence of the employee and/or his or her representative
(b) The employee or representative shall have the opportunity to question
management (c) The panel members shall have the opportunity to question management 2. Employee Presentation of Case (a) The employee or his or her representative shall state the case in the presence
of Management (b) Management shall have the opportunity to question the employee or
representative (c) The panel members shall have the opportunity to question the employee or
representative
3. Summing-Up
(a) Management shall have the opportunity to sum up the case (b) The employee or representative shall have the opportunity to sum up the case.
The employee or representative shall have the right to speak last.
- 45 -
Managing Attendance Toolkit Version 2

NB: In their summing-up neither party may introduce any new matter 4. The manager or management representative, employee, or representative shall
withdraw from the proceedings. 5. The panel shall deliberate in private, only recalling both parties to clear points of
uncertainty on evidence already given. If recall is necessary both parties shall return, notwithstanding only one is concerned
with the point giving rise to doubt. 6. The panel shall recall both parties so that the decision can be announced.
In the case of an Appeal Hearing the panel will advise the employee that no further internal processes are possible and the decision of the Appeal Panel is final. The decision of the panel will be confirmed formally in writing within 5 working days of the date of the hearing. Exceptionally, depending on the complexity of the case, the panel may not be able to give their decision on the day. In such cases contact will subsequently be made with the employee or representative as soon as possible after the hearing and certainly within 5 working days of it, or a suitable explanation will instead be given.
NB: At any point in the proceedings the panel may, at its discretion, adjourns the proceedings where they feel this is appropriate
- 46 -
Managing Attendance Toolkit Version 2

- 47 -
Managing Attendance Toolkit Version 2
EQUAL OPPORTUNITIES MONITORING We require this information for monitoring under the Equality Act 2010 as well as other legislation and directives covering equal opportunities and diversity. The Trust is committed to equal opportunities and fully supports this monitoring. As a Public Authority it is our duty under the Equality Act.
Ethnicity Codes
White Mixed Asian or Asian British
Black or Black British
White British A White & black Caribbean
D Indian H Caribbean M
White Irish B White & Black African
E
Pakistani J African N
Any other White
C White & Asian
F Bangladeshi K Any other Black background
P
Any other mixed background
G Any other Asian background
L
Other ethnic groups
Not stated
Chinese R Not stated Z Any other ethnic group
S
Disability codes
Age Category
Gender code
No disabilities
N
Under 20 years
1 Male M
Dyslexic D
20-24 years
2 Female F
Blind/sight impaired
S
25-44 years
3
Deaf/hearing impaired
H 45+ years 4
Mobility difficulties
M
Other
MANAGER TO FORWARD A COPY OF FORM TO HR