management of post-prostatectomy incontinence (ppi) primary care conference 2/25/04 mary jo willis,...
TRANSCRIPT

Management of Post-Prostatectomy Management of Post-Prostatectomy Incontinence (PPI)Incontinence (PPI)
Primary Care ConferencePrimary Care Conference2/25/042/25/04
MARY JO WILLIS, MS, APRN-BCMARY JO WILLIS, MS, APRN-BC
CLINICAL ASSOCIATE PROFESSORCLINICAL ASSOCIATE PROFESSOR
NURSE PRACTITIONER, USIMNURSE PRACTITIONER, USIM

OBJECTIVESOBJECTIVES
Discuss the incidence of incontinence in males post radical prostatectomy for Prostate cancer
Address the common causes of the incontinence post prostatectomy
Describe which conservative treatments offer benefit
Describe the surgical options for treatment

CONFLICTS OF INTERESTCONFLICTS OF INTEREST
I have not received compensation for this presentation
I have a personal interest in understanding what options for treatment exist and what works.
I wish to thank Dr Wade Bushman for his assistance with this presentation

CASE STUDYCASE STUDY
Patient is a 69 y/o w/m who underwent retropubic radical prostatectomy for prostate cancer 4/02.– Prostate cancer was a moderately
aggressive Gleason 7 found on biopsy after patient had increased problem with nocturia, frequency and inability to completely empty bladder. No incontinence
– PSA history 4.4 in 10/2000, 4.5 in 10/2001, and 5.0 at the time of diagnosis 4/02

RISKS OF RADICAL RISKS OF RADICAL PROSTATECTOMY PROSTATECTOMY COMPLICATIONSCOMPLICATIONS
Multi-center study of over 1069 men provided self reported incidence of incontinence, impotence, and bladder neck contracture /stricture revealed the following results:– Incontinence=65%– Impotence=88.4%– Bladder neck contracture/stricture=20.5%– Even though complications of post radical
prostatectomy are common and affects overall quality of life, most patients would elect the same treatment again.
Journal of Urology 163,858-864, March 2000

GENERAL MALE POPULATION GENERAL MALE POPULATION URINARY INCONTINENCEURINARY INCONTINENCE
Community population rate on incontinence in persons over 60 is 15-30%; 10-15% in women; 50% in institutionalized elderly
Prevalence rate on incontinence in men >60 in Michigan study in 1998 was 19% with
– 34.9% had urge incontinence
– 7.9% had stress incontinence
– 28.9 had mixed
– 28.3% had other– Ostomy/Wound Management 44(6), 54-59, (1998)

GENERAL MALE POPULATION GENERAL MALE POPULATION URINARY INCONTINENCEURINARY INCONTINENCE
Study conducted by questionnaire in one county in Minnesota assessing UI in men >50 in previous 12 months found a prevalence rate of 23% with:– 24.9% with stress and urge incontinence– 40.8% had only urge incontinence– 30.88% had neither stress or urge
incontinence– 77.8% rated it as mild and 22.2% moderate
to severe
RISKS FOR PPIRISKS FOR PPI
Age Size and configuration of the prostate Size and location of tumor Presence and degree of bladder outlet
obstruction and detrusor muscle dysfunction preoperatively
Surgical technique and skill of surgeon: resection of neurovascular bundles, bladder neck preservation/reconstruction
Other studies found no association based upon the above variables nor cancer stage, tumor grade

CAUSES OF PPI CAUSES OF PPI
Injury to bladder
– Bladder instability
– Trigonal denervation (reduced sensitivity in the trigone with altered voiding sensation)
– Bladder wall damage from longstanding outlet obstruction or decreased bladder wall compliance
– Bladder outlet obstruction (BOO) causing overflow incontinence is rare

CAUSES OF PPICAUSES OF PPI
Injury to the sphincter with – Difficulty emptying the urethra leading
to post void dribble– Intrinsic sphincter deficiency/weakness
is most common cause
Sphinter injury, pudendal nerve injury
Ischemia and immobilization by scar, atrophy
Shortening of the urethra below critical functional length of 2.8 cm

ANATOMYANATOMY
There are 2 separate continence zones: Proximal urethral sphincter (PUS) includes
– The bladder neck, prostate and prostatic urethra to veru montanum
Distal urethral sphincter –DUS extending from the veru montanum to the bulbar urethra– Includes slow twitch intrinsic rhabdosphincter fibers
that sustain urethral lumen tone– Fast twitch fibers of the periurethral extrinsic skeletal
muscle layer that supplement the activity of slow twitch fibers
– Intrinsic smooth muscle layer that is a continuation of the superficial layer of the detrusor muscle lining the posterior prostatic urethra

POINTS OF DAMAGE POST OPPOINTS OF DAMAGE POST OP
Either the PUS or DUS must be intact to maintain continence After prostatectomy the PUS is destroyed and continence
relies totally upon an intact DUS During a radical prostatectomy, the proximal portion of the
DUS is also removed Continence therefore is dependent on an intact distal
sphincter as well as normal bladder function (capacity and compliance without detrusor instability)
Any bladder dysfunction resulting in an intravesical pressure that exceeds that of the distal urethral spincter resistence leads to PPI
Urodynamically based studies point out that sphincter weakness with secondary detrusor weakness based upon reduced maximum urethral closure pressure, low leak point pressure and shortened urethral length lead to incontinence

ANATOMYANATOMY

PROBLEMS DEFINING PROBLEMS DEFINING INCONTINENCE RATESINCONTINENCE RATES
Krane(2000) and Parekh(2003) found incidence post op to range from2.5-87 % depending on definition, method and time of data collection
Centers of excellence research indicate overall rates from 6-20%;70-90% were dry at 1 year
Reported incontinence rates were influenced by the– Lack of consensus of definition– Optimal time to assess continence– Methodology– Inclusion of pts incontinent prior to surgery– Variations of operative technique

PPIPPI
Multicenter study: 1990-97
– Immediately after surgery: 81.5%
– 6 months post op status=65.6%)
–53.9% <15ml
–23.2% notice leakage once or less daily
–44% used protection with 27% using pads
–Most commonly used Rx was pelvic exercise (34%)

PPIPPI
Study by Gomha and Boone(2003) found– 100% of patients with stress incontinence– 48% with urgency and urge incontinence– 42% had delayed first sensation
Study by Chao and Mayo (1995) found– 57% reported sphincter weakness– 39% had detrusor dysfunction– 50% had combined causes

PPIPPI
Findings of Eastham et. al. from Baylor College of Medicine and The Methodist Hospital– Continence returned at a median of 1.5 months
in pts treated since 1990 and 95% eventually regained control
– Patient’s age (less than 70) and technical features of the surgery significantly improved recovery of continence (e.g wide resection of 1 bundle substantially decreased recovery), and increase in functional length of the urethra improved continence
– Incontinence was largely refractory to conservative measures
CONSERVATIVE TREATMENTCONSERVATIVE TREATMENT
Urodynamic Testing Role of Pelvic Floor Exercises
– Commonly recommended
– May be effective when employed in an intensive, supervised program
– Improved continence at 3 mo (88% vs 56%). Difference diminished at 1 year (14%).
[Van Kampen et al., Lancet 2000 355(9198):98-102]
– Benefit of office based instruction is questionable
– Sueppel et.al (2001) found that starting PFM exercises prior to surgery improved outcomes
CONSERVATIVE TREATMENTCONSERVATIVE TREATMENT
INSTRUCTIONS: DIETARY IRRITANTS TO THE URINARY TRACTIf your bladder symptoms are related to dietary factors, strict adherence to a diet which eliminates certain food products should bring significant relief in 10 days.The proof is resuming your old dietary habits followed by the return of your symptom complex. Once you are feeling better, you can begin to add these things back into your diet, one item at the time. This way, if something really does cause you symptoms, you will be able to identify what it is. When you do begin to add foods back into your diet, it is crucial that you maintain a significant water intake. Water should be the majority of what you drink everyday (approximately 1-2 quarts a day). Mayo Clinic Urology Clinic 11/02

CONSERVATIVE TREATMENTCONSERVATIVE TREATMENT
FOODS TO BE AVOIDED:
**All alcoholic beverages *Chocolate
*Apples, apple juice Grapes
*NutraSweet Guava
Cantaloupe Vitamin E if powered
*Carbonated beverages Peaches, pineapple, plums
*Chiles/spicy foods *Citrus foods incl lemons
**Coffee, tea, (incl decaf) Tomatoes
Strawberries, cranberries Onions
Vinegar Vitamin B complex(B6 okay)

CONSERVATIVE TREATMENTCONSERVATIVE TREATMENT
DAILY DIET SUBSTITUTIONS:1. Coffee-acid removed: Kava, cold brewed coffee
2. Weak or Herbal teas-if free of large amounts of citrus. dunk a tea bag in water 4 times quickly to color the water. Sun-brewed tea
3. Carob for chocolate; Ovaltine instead of chocolate drinks 4. Fruit juices: apricot, nectar, pear nectar, papaya,
watermelon 5. Late harvest dessert wines 6. Fructose, as in Superose instead of NutraSweet or saccharin 7. Orange or lime peel without white part of rind 8. Pine nuts in place of other types of nuts 9. Consider wheat allergy: breads made of potato, soya, rice
flour 10. Vitamins: Vit. C in calcium ascorbate co-buffered with
calcium carbon

CONSERVATIVE TREATMENTCONSERVATIVE TREATMENT
Electomyography (EMG) can be used as an adjunct when teaching the PFM exercises to provide visual and audible assessment of the pelvic floor.
– Low EMG profile is an identifiable risk factor for incontinence. Can be done preoperatively to establish risk

CONSERVATIVE TREATMENTCONSERVATIVE TREATMENT
Bladder retraining
– Helpful if detrusor dysfunction is present, especially with adjunctive anticholinergics
– Useful for urinary urge and frequency
– Patient needs to keep a bladder diary with information on voiding pattern, frequency and voided volumes

MEDICAL AND SURGICAL MEDICAL AND SURGICAL TREATMENT OPTIONSTREATMENT OPTIONS
Medical: In addition to conservative measures:
– Anticholinergics for detrusor instability
Surgical:– Bulbourethral Sling– Artificial Urinary Sphincter
BULBOURETHRAL SLlNGBULBOURETHRAL SLlNG
Northwestern technique – bulbourethral Northwestern technique – bulbourethral slingsling
Recent interest in male sling procedures Recent interest in male sling procedures for post-radical prostatectomy for post-radical prostatectomy incontinenceincontinence preserve volitional voidingpreserve volitional voiding quick, simple to performquick, simple to perform

PRE-OPERATIVE URODYNAMIC PRE-OPERATIVE URODYNAMIC EVALUATIONEVALUATION
Confirm Sphincter deficiency R/O detrusor instability as cause of
leakage R/O diminished bladder compliance

BACKGROUNDBACKGROUND
Northwestern technique (bulbourethral sling)
– Gore-tex bolsters placed beneath bulbar urethra, suspended from rectus fascia
– Intraoperative urodynamics
– Goal = analogous procedure to pubovaginal sling

BACKGROUNDBACKGROUND
Previous analysis with 12-month follow-up: 91% cured or improved 85% 0-2 pads per day 6% removal rate for infection, erosion
The purpose of this study was to review the long-term outcomes of the first 95 patients ( 95 patients (10/94 to 6/00) who underwent the bulbourethral sling procedure at Northwestern.



STUDY MATERIALS AND METHODSSTUDY MATERIALS AND METHODS
95 patients from 10/94 to 6/00
8 patients deceased at time of questionnaire
71/87 patients completed survey (82% contact rate)
Mean follow-up interval 4.0 years (0.27-6.55)
Mean age at time of surgery: 69 years (55-81)
Preoperative adjuvant radiation therapy: 9 (13%)

PREOPERATIVE INCONTINENCEPREOPERATIVE INCONTINENCE
(%)
Complete 20
> 5 pads 40
> 2 pads 98
*Median duration of incontinence: 68 month (range 14-198)

RESULTS AT 4 YEARSRESULTS AT 4 YEARS
Overall Sling Intact
Total patients 71 64
Cured (n=25) 35% 39%
Cured/ Improved
(n=52)
73% 81%
0 pads (n=23) 32% 36%
<2 pads per day
(n=44)
62% 69%

POSTOPERATIVE CONTINENCE POSTOPERATIVE CONTINENCE STATUS: Non-radiated PatientsSTATUS: Non-radiated Patients
12%
38%
50%
Cured (n=22)
Improved (n=28)
Unchanged (n=7)
42%
30%
28% 0 Pads(n=24)
1-2 Pads(n=17)
>2 Pads(n=16)
CCII
UU
1-21-2
>>22 00

POSTOPERATIVE CONTINENCE POSTOPERATIVE CONTINENCE STATUS: Radiated PatientsSTATUS: Radiated Patients
72%
14%
14% Cured (n=1))
Improved (n=1)
Unchanged (n=5)
14%
29%57%
0 Pads (n=1)
1-2 Pads(n=2)
>2 Pads(n=4)
CCII
UU
001-1-22>2>2

PATIENT SATISFACTION: PATIENT SATISFACTION: Non-radiated PatientsNon-radiated Patients
Would you undergo the procedure all over again?
19%
81%
No (n=11)
Yes (n=46)YY
NN

PATIENT SATISFACTION: PATIENT SATISFACTION: Radiated PatientsRadiated Patients
Would you undergo the procedure all over again?
57%
43% No (n=4)
Yes (n=3)
YY NN

POST-OPERATIVE PAINPOST-OPERATIVE PAIN
Do you have persistent perineal pain or numbeness?
6%
82%
3% 9%
severe (n=2)
moderate (n=6)
minimal (n=4)
none (n=52)

INCONTINENCE QUALITY OF LIFE INCONTINENCE QUALITY OF LIFE QuestionnaireQuestionnaire
20%
80%
moderate/severeimpact (n=12)
minimal/mildimpact (n=48)

SLING COMPLICATIONSSLING COMPLICATIONS
no. (%)
Retightening 15 (21)
Sling removal 7 (10)
- infection 6 (8)
-urethral erosion 1 (1)
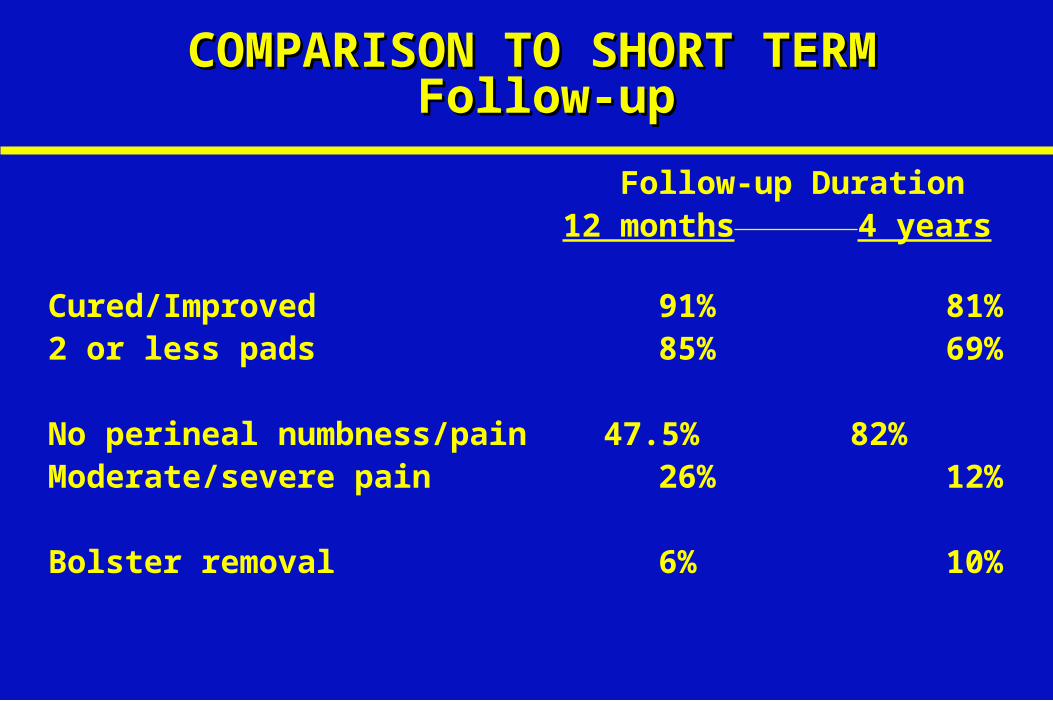
COMPARISON TO SHORT TERMCOMPARISON TO SHORT TERM Follow-up Follow-up
Follow-up Duration 12 months 4 years
Cured/Improved 91%81%
2 or less pads 85%69%
No perineal numbness/pain 47.5% 82%Moderate/severe pain 26% 12%
Bolster removal 6%10%

COMPLICATIONS SUMMARYCOMPLICATIONS SUMMARY
Infection/erosion rate=10%
– AUS 6.8%
– Barrett 2000
Revision rate = 21%
– XRT 66%; no XRT 15 %
– AUS 20-40%
– Light 1989; Barrett 1989; Montague 1992; Webster 1992; Singh 1996; Herschorn 1996; Castro Diaz 1997

CONCLUSIONSCONCLUSIONS
Bulbourethral Sling is effective for post-radical prostatectomy incontinence
Radiation significantly reduced efficacy
Post-operative discomfort resolved in most patients


ARTIFICIAL URINARY ARTIFICIAL URINARY SPHINCTERSPHINCTER
Gold standard for surgical treatment of PPI
First developed in 1947 by Foley; refined in the 1970s. AMS 800 developed in 1983
AUS implantation usually delayed for 12 months after RP
Men usually seeking this option have significant incontinence

ARTIFICIAL URINARY SPHINCTER ARTIFICIAL URINARY SPHINCTER DATADATA
Gousse et al1 : mean follow-up 7.7 years
0 pads: 27% very satisfied: 58%
>3 pads: 25% satisfied: 19%
16% revision rate unsatisfied: 23%
Montague et al2: mean follow-up 73 months
0-1 pads: 64% very satisfied: 28%
2+ pads: 35% satisfied: 45%
12% revision rate dissatisfied/
very dissatisfied: 10%
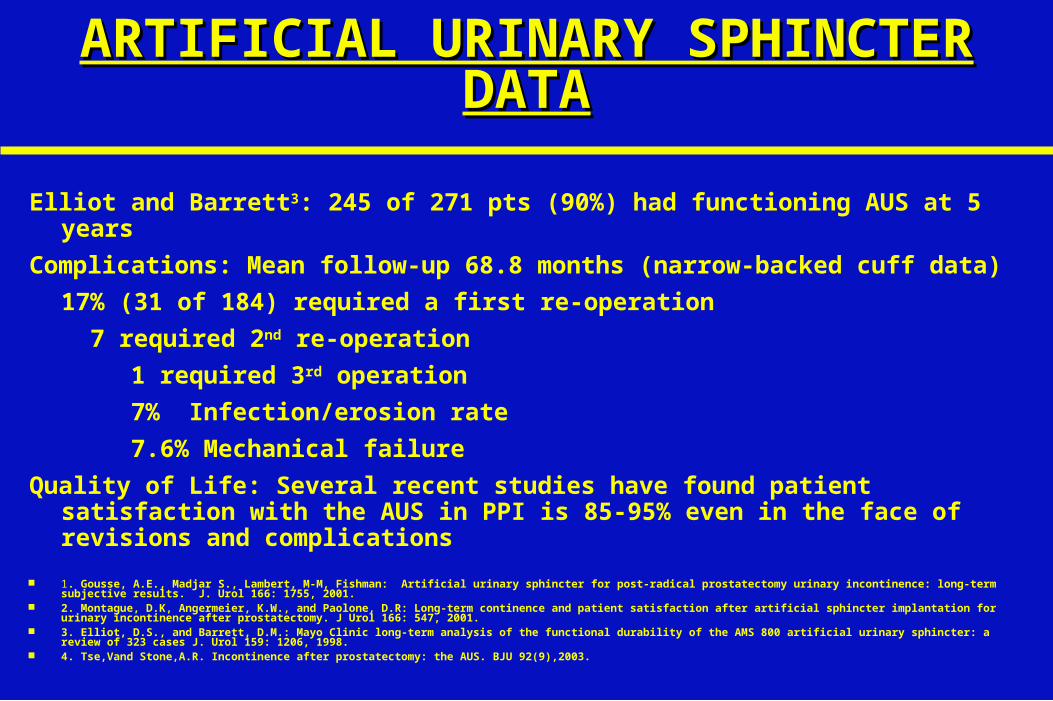
ARTIFICIAL URINARY SPHINCTER ARTIFICIAL URINARY SPHINCTER DATADATA
Elliot and Barrett3: 245 of 271 pts (90%) had functioning AUS at 5 years
Complications: Mean follow-up 68.8 months (narrow-backed cuff data)
17% (31 of 184) required a first re-operation
7 required 2nd re-operation
1 required 3rd operation
7% Infection/erosion rate
7.6% Mechanical failure
Quality of Life: Several recent studies have found patient satisfaction with the AUS in PPI is 85-95% even in the face of revisions and complications
1. Gousse, A.E., Madjar S., Lambert, M-M, Fishman: Artificial urinary sphincter for post-radical prostatectomy urinary incontinence: long-term subjective results. J. Urol 166: 1755, 2001.
2. Montague, D.K, Angermeier, K.W., and Paolone, D.R: Long-term continence and patient satisfaction after artificial sphincter implantation for urinary incontinence after prostatectomy. J Urol 166: 547, 2001.
3. Elliot, D.S., and Barrett, D.M.: Mayo Clinic long-term analysis of the functional durability of the AMS 800 artificial urinary sphincter: a review of 323 cases J. Urol 159: 1206, 1998.
4. Tse,Vand Stone,A.R. Incontinence after prostatectomy: the AUS. BJU 92(9),2003.

CONCLUSIONS:CONCLUSIONS:
Pelvic floor exercises are not helpful for patients with established SUI
Medical therapy is of limited value Urodynamic testing is useful to R/O detrusor
instability or diminished compliance Artificial Sphincter and BUS show similar
efficacy. Artificial sphincter is preferred in patients
with history of radiation and in post-TUPR incontinence.

CASE STUDY OUTCOMECASE STUDY OUTCOME
Initial reaction to incontinence Patient uses <2 pads per day
– Stress incontinence continues to limited patient’s hobbies such as golf, tennis and landscaping
– Has limited social events to avoid embarrassment
– PFM exercises were never really beneficial in fact it worsened the problem after 6 months
– Will not consider further surgery unless the PPI gets worse.