management of anterior wall mi with shock in a non pci center
TRANSCRIPT

Management of Anterior Myocardial Infarction with Shock
in a Non PCI center

What is shock?
• Shock is the clinical syndrome that results from inadequate
tissue perfusion ,leading to impaired oxygen delivery –
cellular dysfunction.
• Clinically accompanied by hypotension (i.e MAP <60mm
Hg in previously normotensive individual).
Harrison’s Principles of Internal Medicine ,18th ed ,2215.

Non cardiac cause of shock
Hypovolemia Excess use of diuretics
Blood loss Post fibrinolysis
Dehydration Diabetics,elderly,acute pancreatitis
Vasodilation excess use of nitrates
Septicemia Infection secondary to indwelling urinary catheter
Anaphylaxis During thrombolysis
Renal failure Diabetics,elderly,previous CKD
They should ruled out in a MI patient with shock,as the management is different and some are reversible. though they add to the mortality risk.

Cardiogenic Shock• One of the most common causes of death after an MI.
• Mostly occurs < 48 hrs after hospitalization, rather at presentation
(90% vs 4.5%).
• About 6% of STEMI, 3% of NSTEACS patients.
• Mortality is 6 times more(within index hospitalization).
• 90% mortality (pre thrombolytic era), 40-50% presently.
• Survival at 3yrs and 6 yrs – 40% and 30% respectively.
• Early recognition, prompt revascularization helps in improved
survival. 1.SHOCK registry, Circulation 1995;91:873-881.2.MILIS Study group, JACC;1989;14:40-6..3.Goldberg RJ et al,NEJM 1991;325:1117-1122.4.Goldberg et al ,Circulation 2009 ; 119(9):1211-9.

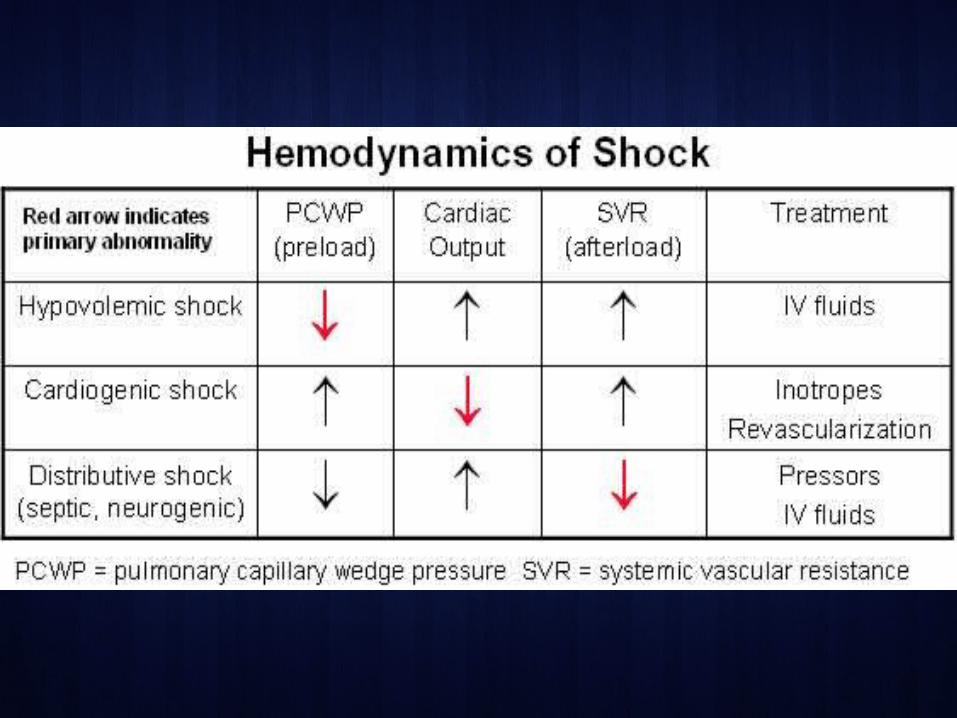
Definition Characterized by
• Marked and persistent (>30 min) hypotension
• SBP < 90 mmHg, or
• Drop in SBP by 30 mm Hg below basal levels, or
• Supportive pharmacotherapy required to maintain SBP > 90 mm Hg.
• Reduced cardiac index (<2.2 liters/min/m2)
• signs of impaired organ perfusion (altered mental status,cold
extremeties,oliguria)
• elevated left ventricular filling pressure (PCWP >18 mmHg).
About 40% of left ventricular mass to be affected. Braunwald’s HEART DISEASE,10th ed. Pg:1123.


Causes of Cardiogenic Shock
Predominant LV Failure
74.5%
Acute Severe MR
8.3%
VSD
4.6%
Isolated RV Shock
3.4%
Tamponade/rupture
1.7%Other
7.5%
Shock Registry
JACC 2000 35:1063

Killip – Kimball Classification
Am J Cardiol. 1967 Oct;20(4):457-64

APPROACH
Approach to patient in shock

Predictive indicators of Cardiogenic shockHistorical Features
Age > 65 yrs Lab FindingsFemale gender Hyperglycemia (>180mg/dl)
Previous infarction Increased blood lactate
Diabetes mellitus CK-MB >160 IU/L
History of angina,stroke or PVD Peak LDH > 4normal
Physical examinationSinus tachycardia Cardiac
Clinical hemodynamic class III - IV ECG – new ST elevation,LBBB
Agitation,abnormal mental status CXR – pulmonary edema
Clinical events ECHO LVEF < 0.35
Reinfarction Remote Asynergy
Hypotension Wall motion index

CAD patients at risk…
• Extensive Anterior wall STEMI
• LMCA stenosis + previous LVDysfunction.
• Osteoproximal LAD total occlusion.
• LAD + Previous h/o CAD.
• TVD + Diabetes.


Cardiac biomarkers• Established markers - CPK-MB, Quantitative troponins.
• NT Pro BNP – reflect LV dysfunction, effects of therapy (Normal
<400pg/ml).
• ST -2 - new biomarker( IL2 family) - marker of cardiac stress and
myocardial fibrosis.
• High levels post AMI - higher incidence of HF, readmission at 30
days ,higher mortality at 30 days.
Circulation ,2004;109(18):2186-90.

Preliminary • Back rest
• Oxygen supplementation (O2 Sat < 90%)
• Early mechanical ventilation if O2 supplementation not effective.
• ABG analysis for acid-base status.
• CVP monitoring after insertion of a jugular venous line.
• Hourly monitoring of urine.
• Anxiolytics
• Loading dose of Soluble aspirin,clopidogrel (if not given).
• Subcutaneous heparin – 60U/kg bolus – 10-12 U/hr

Rule out reversible causes.
• Correct acidosis (MC neglected).
• Hyperglycemia with insulin.(strict control of blood sugars not
advised) . NICE study.
• Bradyarrhythmias – transvenous pacing.
• Recurrent VT,AF - DC shock,overdrive pacing .

Medical management
• Vasopressors/Inotropic support (double edged swords)
– Dopamine
– Noradrenaline
– Dobutamine
– Levosimendan
– Milrinone
• Vasodilators
• Diuretics
Aim:Maintaining adequate systemic and coronary perfusion by ↑ SBP with pressors, optimal LV filling pressure - adjusting volume status.
Recommended is SBP 90mm Hg or Mean BP >60mmHgPCWP >20 mmHg

Dopamine• Initial drug of choice in hypotension.• and receptor and DA receptor stimulator.• ↑ HR,BP,CO,SVR,PCWP• Higher mortality when compared to NE in maintaining an effective
MAP. SOAP NEJM2010;362:779-789
Dosage Effect
0.5 -4 µg/kg/min Renal arteriolar vasodilation(DA receptor)Increase in urinary output.
4 -6 µg/kg/min Renal beneficial effects lost.Vasoconstriction (1 and NE)
Increased HR,CO,BP.
> 15 µg/kg/min Marked vasconstriction occurs.Seldom advised in Cardiogenic Shock.
Management of Cardiogenic Shock,Chirstopher.P.Cannon

Combination with dobutamine
• Dopamine (6-10µg/kg/min) and dobutamine
(2-10µg/kg/min) has several merits.
• If SBP&DBP low, PCWP >24 mmHg - Norepinephrine to
be tried in combination with dobutamine.
Circulation,1983;67:620-626.
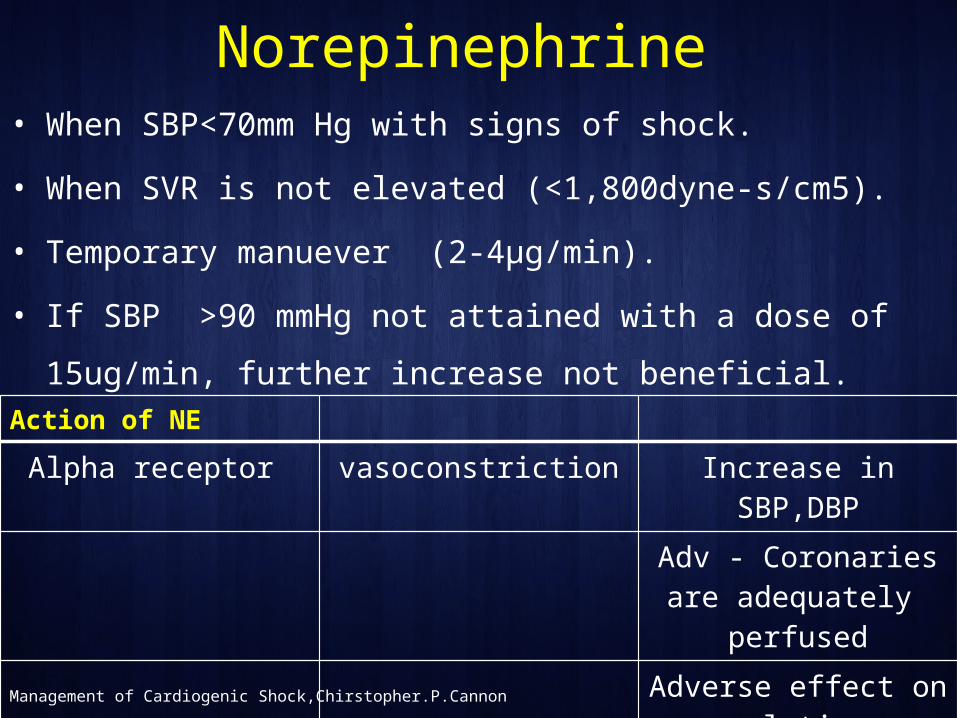
Norepinephrine • When SBP<70mm Hg with signs of shock.
• When SVR is not elevated (<1,800dyne-s/cm5).
• Temporary manuever (2-4µg/min).
• If SBP >90 mmHg not attained with a dose of 15ug/min, further
increase not beneficial.Action of NE
Alpha receptor vasoconstriction Increase in SBP,DBP
Adv - Coronaries are adequately perfused
Adverse effect on renal tissue
Causes necrosis.
Management of Cardiogenic Shock,Chirstopher.P.Cannon

Milrinone
• Positive inotropic and significant vasodilator actions.
• ↑CO, LV filling pressures.
• Effective in RV dysfunction.
• Minimal effect on myocardial oxygen demand.
• Long half life.
• 50µg/kg bolus over 10 min – 0.0375 to 0.75 µg/kg/min.
Goodman & Gilman’s The Pharmacological basis of Therapeutics

Nitroprusside
• Very low dose (0.4 ug/kg/min).
• Reduces afterload .
• Useful in patients with severe MR or ventricular septal rupture.
• Causes coronary steal.
• Deleterious effect (If given <8 hrs of onset of pain).
• Combined with dopamine/dobutamine when afterload is to be
reduced without fall in BP.
Goodman & Gilman’s The Pharmacological basis of Therapeutics

Levosimendan
• Inotropic action by binding cardiac troponin C.
• Sensitizes myofilaments to calcium.
• 6 to 12 µg/kg loading dose over 10 minutes ----- 0.05 to 0.2
µg/kg/min as a continuous infusion.
• Effective in acute HF post MI - RUSSLAN trial.
• Risk of hypokalemia, frequent VPCs.
Murphy ,Mayo Clinic Cardiology Concise Textbook,4th Ed
Eur Heart J. 2002 Sep;23(18):1422-32.

Tilarginine
• Excess NO contributes to hypotension.,plays a role in
pathophysiology of cardiogenic shock.
Dzavik et al. 2007.
Alexander et al.2007.
• Isoform – nonselective NOS inhibitor.
• Despite establishment of an open infarct artery ,it revealed no
effect on mortality.
• An increase in blood pressure noted. Khan,Encylopedia of Cardiac Diseases,2nd ED

Unproven benefit
• Oxygen radical scavangers
• Adenosine
• Neutrophil inhibitors
• Substrate infusions of glutamate/aspartate
• Glucose – insulin – potassium infusion
• Coenzyme Q10
• Intravenous L- Carnitine.
Semin Thoracic Cardiovascul Surg 1993;5:151-161.

SHOCK trial
• Median time to onset of shock was 5.6 hrs.
• Most infarcts were Anterior in location.
• At 30 days - no significant overall benefit of early revascularization
for patients with STEMI or new LBBB who had cardiogenic shock
due to LV dysfunction. (46.7 % and 56.0 %; P= 0.11).
• lower mortality from all causes at 6 months. (50.3 % vs. 63.1 %,
P=0.027).
• Early revascularization be strongly considered for patients with
Acute Myocardial Infarction complicated by cardiogenic shock.N Engl J Med 1999; 341:625-634
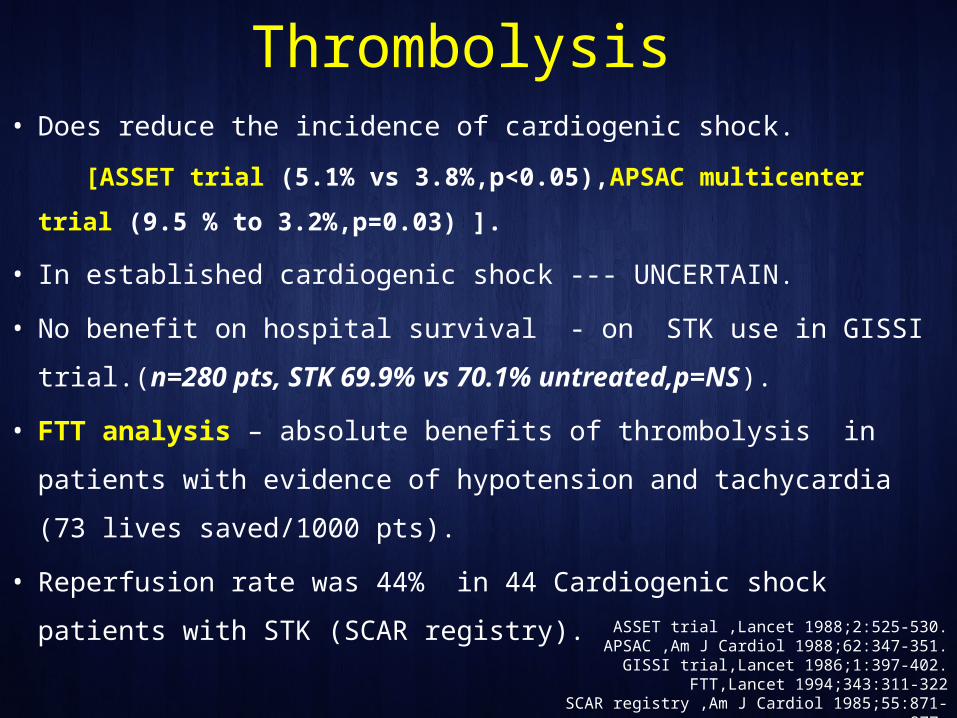
Thrombolysis • Does reduce the incidence of cardiogenic shock.
[ASSET trial (5.1% vs 3.8%,p<0.05),APSAC multicenter trial (9.5 % to
3.2%,p=0.03) ].
• In established cardiogenic shock --- UNCERTAIN.
• No benefit on hospital survival - on STK use in GISSI trial.(n=280 pts,
STK 69.9% vs 70.1% untreated,p=NS).
• FTT analysis – absolute benefits of thrombolysis in patients with
evidence of hypotension and tachycardia (73 lives saved/1000 pts).
• Reperfusion rate was 44% in 44 Cardiogenic shock patients with STK
(SCAR registry).ASSET trial ,Lancet 1988;2:525-530.
APSAC ,Am J Cardiol 1988;62:347-351.GISSI trial,Lancet 1986;1:397-402.
FTT,Lancet 1994;343:311-322SCAR registry ,Am J Cardiol 1985;55:871-877.

Why thrombolysis not effective?
• Limited evidence.
• Complex mechanical, hemodynamic ,metabolic factors.
• Acidosis - impaired transformation of plasminogen to plasmin
- decreased efficacy
Becker et al.A Heart J 1993;125:919-929.
• coronary perfusion pressure – delivery of plasminogen
activators to thrombus impaired. Zidansek et al,Thromb Hemostat,1991.
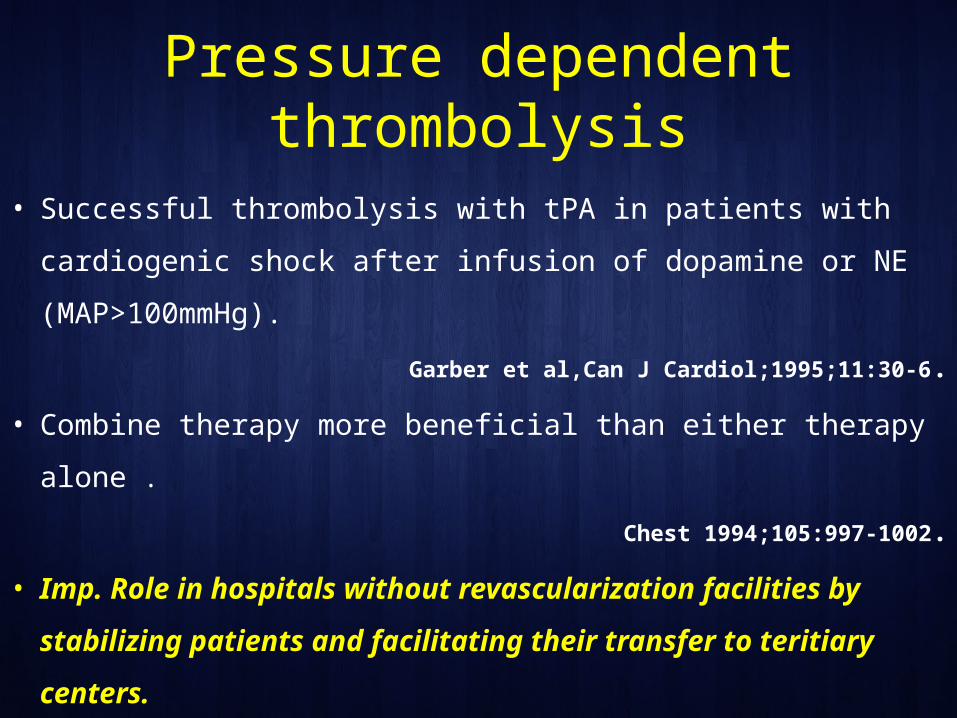
Pressure dependent thrombolysis
• Successful thrombolysis with tPA in patients with cardiogenic
shock after infusion of dopamine or NE (MAP>100mmHg).
Garber et al,Can J Cardiol;1995;11:30-6.
• Combine therapy more beneficial than either therapy alone .
Chest 1994;105:997-1002.
• Imp. Role in hospitals without revascularization facilities by
stabilizing patients and facilitating their transfer to teritiary
centers.

IABP assisted Thrombolysis
• Patients in cardiogenic shock
– TT had lower in-hospital mortality rates (54% vs 64%),
– IABP counterpulsation had lower in-hospital mortality rates
(50% vs 72%).
• Revascularization influenced in-hospital mortality rates
significantly (39% vs 78%).
SHOCK registry

Which thrombolytic agent is effective?
• Use of accelerated tPA better than STK in reducing cardiogenic
shock (5.5% vs 6.9%)(GUSTO1).
• Cardiogenic shock after treatment - STK,Heparin better than tPA
(51% vs 57%,p=0.061).
• Advantage of STK – prolonged systemic fibrinolytic state with
decreased viscosity produced by streptokinase.

Mechanical and other causes
• MR – Nitroprusside ,NTG.
• VSR – Surgical referral.
• Percardial tamponade – Pericardiocentesis.
• AF – Cardioversion.
• VT – Cardioversion.
• VT storm – Magnesium infusion, Esmolol, Overdrive pacing.
• Pneumothorax secondary to CPR – ICD.



Treatment of Cardiogenic Shock
Emergency revascularization with either PCI or CABG is
recommended in suitable patients with cardiogenic shock
due to pump failure after STEMI irrespective of the time
delay from MI onset.
In the absence of contraindications, fibrinolytic therapy
should be administered to patients with STEMI and
cardiogenic shock who are unsuitable candidates for
either PCI or CABG.
I IIaIIbIII
I IIaIIbIII
ACC/AHA STEMI GUIDELINES 2013;Circulation.2013; 127: 529-555

Treatment of Cardiogenic Shock
The use of intra-aortic balloon pump counterpulsation
can be useful for patients with cardiogenic shock after
STEMI who do not quickly stabilize with
pharmacological.
Alternative LV assist devices for circulatory support
may be considered in patients with refractory
cardiogenic shock.
I IIaIIbIII
I IIaIIbIII
ACC/AHA STEMI GUIDELINES 2013;Circulation.2013; 127: 529-555

Conclusion • Cardiogenic shock main cause of death in AMI patients.
• Immediate diagnosis & management required.
• Rule out Noncardiac causes of shock .
• Gold standard - Invasive approach.
• In Non PCI center, fibrinolytic therapy and IABP should be used
while provisions are made for invasive treatment.
• Newer therapies may help in decreasing the significant mortality
of cardiogenic shock in the future.

An ounce of prevention is
worth a pound of care Benjamin Franklin