making a lasting impression on mental health.€¦ · · 2015-03-19making a lasting impression on...
TRANSCRIPT

making a lasting impression on mental health.

ContentsIntroduction� 03
Operational and Financial Review 10 incorporating Environmental Issues, Complaints, Finance Director’s Report, Quality Accounts�
Trust Board Members incorporating 45Register of InterestsSenior Managers’ Remuneration ReportAnnual Governance Statement 53
Statement of the Chief Executive’s 55Responsibilities as the Accountable Officer to the Trust
Performance and Activity 56
Independent Auditor’s Report to the 64Directors of Mersey Care NHS Trust
Annual Accounts incorporating Foreword 72 to the Accounts, Statement of Comprehensive Income for the Year, Statement of Financial Position, Statement of Changes in Tax Payers’ Equity, Statement of Cash Flows
This Annual Report Mersey Care welcomes ideas and feedback regarding the Annual Report. In the June 2012 issue of Mersey Cares (*), the Trust magazine, readers were asked for their views on non-statutory content of this report and were asked about improvements that could be made on previous editions. If you have any ideas or comments that you would like to share with us, please contact us at:Mersey Care NHS Trust, 8 Princes Parade, Princes Dock, St Nicholas Place, Liverpool, L3 1DL.www.merseycare.nhs.uk (*) Note: Mersey Cares has a distribution of approximately 6,000 copies to all stakeholders (and 3,000 sent electronically) including: service users, carers, staff, Trust members, public libraries, health centres and clinics.
This report is available in other formats and languages on request.
Mersey Care has people at its heart.
Simply put, it’s about who we are,
not what we are.

IntroductionMersey Care has people at its heart. That is why this annual report focuses on the personalities who are connected to us in our mutual endeavour. Mersey Care is less an organisation and more an enterprise where people join together contributing skills, knowledge and progress to meet needs. Simply put, it’s about who we are, not what we are.
Mersey Care has done well against its many targets during 2011-12, including those around quality of service and patient experience, staff satisfaction, and finances.
Several inspections of our services, including those carried out by the Care Quality Commission and the Royal College of Psychiatrists, were public statements of the high levels of service quality and patient experience and satisfaction achieved.
As for staff, who are our most valuable asset and constitute 79% of our operating costs, our annual NHS Staff Survey showed an overall improvement in staff satisfaction.
Targets help in benchmarking the performance of the Trust. In budgetary terms we operated within our statutory limits, achieved planned savings and made capital expenditure of more than £7m. We also reduced our overall reference costs to be more in line with that of other health providers. The measurement of achievement against targets is of course very important, but it is the impact of that achievement on individual people - service users, carers and staff that really matters.
We surpassed our target numbers for membership. By the year end, more than 10,000 had joined us – further evidence of the importance of different people with different viewpoints forming part of our Trust. We have held elections to our Members Council, who now meet regularly to represent their members’ views and advise the Trust Board on the strategic direction and service development plans for the Trust.
Membership is very important and provides an accountable link to our many and varied stakeholders. They further assist us in our efforts to become a foundation trust. These efforts are continuing and we are hopeful of authorisation by April 2014.
We hope you enjoy our report of 2011-12, and reading about some of the people who are Mersey Care.
2 3
Beatrice Fraenkel, Chairman Alan Yates, Chief Executive in post until 12th September 2012 Joe Rafferty, Chief Executive from 1st September 2012

I’m Brian. I’m Mersey Care.

I was brought up in Crosby but my school was a rugby school, so I went elsewhere to watch football.
I love the fact it’s a members’ club – no one individual owns it; it’s a hub for the community, with lots of separate components and ‘owned’ by lots of people.
I feel relaxed and comfortable, where I have a common interest and where I know I can turn for help when anything is needed. That’s why... I’m Brian and I’m Mersey Care.
Me and my friends started what was to become a lifelong interest – I’m proud to say I’ve been a Marine Football Club supporter for nearly 50 years.
From watching football at the age of 10 I went onto play until my late 20s and then took up lower league refereeing for 20 years, refereeing all over the country as well as being a linesman at Goodison and Anfield. But it’s hard to fit work in when you travel hundreds of miles for an evening game and are back at work the next morning.
Watching football isn’t everyone’s cup of tea and I often find myself looking after the changing rooms and the officials on a typical Saturday at my own club.
It’s made up of things like junior coaching, ladies’ football, social events, fund-raising, not to mention the first and reserve sides. In that respect it’s like Mersey Care – the sum of its parts are greater than the individual bits, and like Mersey Care all of its members have a stake in it and a say in how it achieves success.
My first proper encounter of mental health was when I was refereeing and was asked to ref’ some matches at Ashworth Hospital many years ago. Football can be a great way of sharing and communicating for everyone.
I’ve learned a lot from football. Things like only through both individual and team effort can you get through both the bad times, as well as the good times.
Since the 1980s I’ve been a member of my club’s committee. As a volunteer I’m no different to everyone else who helps out in any club. You read a lot these days about football clubs and their big money, but I don’t consider any of that really important as a supporter. Because of my interest and career as a solicitor I’m now Company Secretary to the league as well as its legal advisor.
Most supporters become lifelong supporters; it gets into your blood. I feel it’s all about commitment. It’s also somewhere
4 5

I’m Justine. I’m Mersey Care.

6 7
At the age of 41 my proudest moment was to carry the Olympic Torch into Liverpool. All of my family was there to see me and my friends and workmates turned out. It was like being a celebrity.
As I got better I started to learn more about skin cancer and other cancers and realised that spotting skin cancer early can save lives.
I’ve always been conscious of my personal appearance, I wanted to look good and have a nice tan, so it was only natural to top up my tan before and after holidays. As a teenager and into my 20s I often used sunbeds to give my skin that bronzed look.
Six years ago I was due to go on holiday again and noticed a spot on my chest. I didn’t think anything of it – in fact I thought the sun would help clear it up. But it didn’t. In fact it got worse and my Auntie suggested I get it checked out by my doctor.
I was referred to a Consultant Dermatologist who said it wasn’t a spot on my skin but a melanoma. It was so bad the Consultant said it was the type of melanoma he normally saw on a patient in their 80s. It was hard for me to take in that one lesion on my body could kill me.
I was initially diagnosed with malignant melanoma five years ago; from then on my life was put on hold for three years. Since then I’ve had to undergo lots of hospital visits and constant checks and monitoring as other melanomas appeared and were treated. And all because I wanted a tan!
I got involved with Cancer Research UK in 2008 and since then have been helping them raise awareness, appearing on local and national television and radio, newspapers, magazines, lobbied MPs in Westminster and I am an ambassador for Cancer Research UK.
Volunteering for Cancer Research UK has given me my self-esteem back and made me the confident person I am today. It’s helped me bring something of that back to work too. When you have had cancer you have good days and bad days, but going out and talking to people about the experience has made me a better and stronger person.
One of the most rewarding things I’ve recently been doing is going into schools to talk to children and young people about skin cancer by just telling them what happened to me. If just one person can be saved the same heartache by knowing the facts it will be worth it. Like mental health, cancer is something we all must talk about, and by raising awareness it will help people. That’s why… I’m Justine and I’m Mersey Care.

I’m Dave. I’m Mersey Care.

My latest stint of four months’ active service was at Camp Bastion in Helmand Province,
We are so lucky having the health service and mental health services we have. In some ways it makes you stronger having to deal with those challenging situations.
8 9
which meant I was away from home for six months on my second tour of duty in Afghanistan. I’m a Warrant Officer First Class, which is equivalent to a Regimental Sergeant Major, and am qualified as a combatant medical technician Class 1.
My role has moved away from clinical to management and my title is ‘ward master’ which basically means I deal with all sorts of things for the smooth running of a ward in a field hospital. That can involve taking the signals about incoming casualties,
As a bandsman you are trained as a regimental medic as a secondary role. The Army took me on, trained me and gave me opportunities I didn’t have before. It was a total contrast from working on a factory production line to being mainly outside, doing different things and responsible for myself as well as others.
When I left the Army one of my first jobs was on a hospital unit in Liverpool and I found I had an aptitude for working in
liaising with the trauma teams so the right kind of specialists are on hand when the injured arrive, to dealing with staffing issues and helping the patients through their onward journey, whether that’s back home or elsewhere. OK, yes, you could say a sort of Radar O’Reilly from MASH!
I’ve been in the Territorial Army Medical Corps for 28 years. Without doubt it’s taught me to stay calm under pressure, being able to rationalise things, being self aware of situations, and aware of cultural differences. For instance, if we get an injured Muslim woman brought in it would only be right to bring a female medic in to treat her, and to respect her by addressing her through an interpreter.
The hardest part of the job is after we’ve treated the Afghan patients, especially children, knowing they are going back to a non-existent health service in Afghanistan.
I joined the Regular Army as a bandsman with the Royal Regiment of Fusiliers, 3rd Battalion, before my 18th birthday and did four years service stationed in Germany.
the area of mental health. I went from a day hospital, then onto the wards and then in the resettlement of people into the community in supported housing. I ended up working specifically with men and women who had agoraphobia, working alongside psychologists and other practitioners and found it very rewarding.
In the Army it was all about being around people and being able to communicate with people from all walks of life, as well as supporting each other, especially when you are away from home and away from familiar surroundings. It helped me be me and people might say I’m fairly relaxed and like a bit of fun, and I’ve found it’s possible to be professional as well as being a bit less formal. I’ve also found that no two people are the same, their needs may be different and aspirations may be different and that sometimes you have to have the confidence to take calculated risks to help them achieve their potential. That’s why... I’m Dave and I’m Mersey Care.

Incorporating Environmental Issues, Complaints, Finance Director’s Report, Quality Accounts
Operational and Financial Review
Mersey Care provides specialist mental health, substance misuse and learning disability services for adults in Liverpool, Sefton and Kirkby, a population of more than one million people.
We also have a wider role offering medium secure services for Cheshire and Merseyside and we are one of only three trusts in the country providing high secure services covering the North West of England, West Midlands and Wales at Ashworth Hospital.
The Trust has a number of specialist community and inpatient services covering a wider catchment area such as outreach alcohol clinics extending to St Helens; and residential drug detoxification for clients from Liverpool, Knowsley, Sefton, St Helens, Blackpool and Central Lancs, as well as a community alcohol service commissioned and based in Knowsley and the Liverpool Community Alcohol Service.
The Trust, first established in 2001, has 4165 members of staff (as at 31st March 2012) and an income of £196m in 2011-2012.
Mersey Care is committed to campaigning for better services, improving the outcomes for its service users and their carers, and combating the stigma around mental illness and learning disability.
Services offered for the treatment and support of patients and service users are provided within Mersey Care by a number of Clinical Business Units (CBUs), based on service speciality and/or geographical location. These CBUs are: Addiction Services, High Secure Services, Liverpool, Positive Care Partnership, Rebuild, and SaFE Partnerships. The CBUs are each supported by Specialist Management Services.
Mersey Care NHS Trust

Service development
Throughout 2011-2012, Mersey Care continued to be a high performing organisation. The Trust achieved both its key service and financial performance targets by continuing to improve quality and increase the value of services that we provide. We made excellent progress in the delivery of our objectives, ensuring that equality and human rights underpin all that we do.
The Trust has continued to build on significant developments, reflected in our achievements throughout the year. Examples of progress made in line with the Trust’s strategy are highlighted below:
In 2011-2012 Liverpool CBU researched the possibilities of developing light therapy which is a relatively simple method of assisting in the treatment of seasonal affective disorder, depression and bi-polar schizoaffective disorder. From the research carried out it was recommended by the CBU that the scheme should be run as a pilot.
Scott Clinic, the medium secure unit within SaFE Partnerships CBU, was subject to a peer review by the Quality Network for Forensic Mental Health Services which concluded that Scott Clinic provides high quality services that meet the standards of quality and safety set by the network.
Positive Care Partnerships CBU, in conjunction with The Kings Fund and key stakeholders, developed a sensory garden at Stoddart House for their older adult inpatients with dementia.
A procurement product standardisation group was established in 2011 - 2012 by the finance department, in conjunction with the Trust’s medical devices group. Standardisation of products should improve quality and provide value for money from supplier contracts.
Fact FileDuring 2011- 2012, Mersey Care: • Provided care, treatment and support to 31,488 service users• Had 503,519 outpatient attendances and contacts• Had 9,012 day hospital attendances• Had 678 inpatient beds as at 31st March 2012 • Was dispersed across over 33 sites both of its own and premises
rented from others.
Our strategy for service developmentTo improve quality and increase the value of services
10 11

Throughout 2011- 2012 Addiction Services CBU completed the training programme for its first cohort of recovery mentors from service user volunteers. These volunteers have experienced addiction first hand or have been involved in a personal recovery journey. This will give service users, already in treatment or new to the service, a recovery orientated approach to treatment.
Positive Care Partnerships launched the Our Hospital booklet for children whose family members are receiving care from the Trust. The booklet encourages children to talk about how they feel, especially about a family member’s admission to hospital. The booklet has been recognised by the Equality and Human Rights Commission as one of the many ways in which the Trust is promoting Article 8 of the Human Rights Act, the right to family life.
The initial findings from the most recent annual Staff Survey, completed by 63% of Trust staff, show an overall improvement in staff satisfaction. Areas where staff have reported significant improvements are:
• Effectiveness of communications between staff and senior management• Number of staff who think senior managers are committed to patient care• Number of staff reporting they had an appraisal• Number of staff who said their personal development review helped them agree
clear objectives• Number of staff with a personal development plan• Number of staff agreeing that their team had shared objectives• Number of staff satisfied or very satisfied with the recognition they received for good
work and the extent to which the Trust values their work.
Following an assessment by two auditors from British Standards Institute (BSI), the Maghull site has achieved verification of its ongoing accreditation to the international standard ISO14001. The standard recognises the Trust’s quality approach to minimising damage to the environment and follows progress since the publication of its environmental strategy two years ago. As well as continuing to look for further improvements at Maghull (both high secure and non-secure sites), the Trust’s environmental management team will consider rolling out its programme to other large sites.
The Trust set up Project 21 to relocate 350 specialist management services (SMS) members of staff from the Trust offices at Maghull to modern purpose-built accommodation. The new accommodation will embrace agile working and innovative technology to maximise efficiencies.
The facilities department was involved in two major change initiatives during the year. The first project was to change the Southport housekeeper/assistant housekeeper service from the traditional cook and catering assistants and the ‘cook serve’ system, to a fully integrated facilities management assistant (FMA) facilities and ‘cook freeze’ catering.

The second project involved the same change at Rathbone, resulting in reduced storage, production and management costs and meals with a consistent nutritional content to meet the clinical needs of patients, service users and carers.
In Liverpool CBU there were developments in health and wellbeing and expansion of the existing memory service, replacing the out-dated day hospital. Positive Care Partnerships CBU developed a neighbourhood centre at Waterloo to replace the day hospital services in South Sefton. Both developments meet service user needs on an individual basis rather than fitting into a traditional model.
Mersey Care’s assistant practitioners were runners-up at the workforce modernisation and innovation award event, recognising the impact of new roles and new ways of working and their contribution to service improvement. The Star Unit at Mossley Hill Hospital had an unannounced visit by the Care Quality Commission (CQC) whose inspectors were joined by two ‘experts by experience’ service users or family members. This review was part of a targeted inspection programme in hospitals and care homes for people with learning disabilities. The inspection assessed how well service users experience effective, safe and appropriate care, treatment and support that meet their needs and protect their rights; and whether they are protected from abuse. The CQC found that: “The Star Unit, Mossley Hill Hospital, was meeting all the essential standards of quality and safety that they reviewed.”
In collaboration with the head of catering, service users and staff from Scott Clinic medium secure unit have formed a ‘food for thought group’ to improve catering at the clinic to meet both the needs of service users and the healthy options agenda.
Both the Low Secure Unit and the Scott Clinic held service users, carer and family events, and SaFE Partnerships CBU plans to hold more events in the future.
The finance performance procurement and information department received the highest accreditation (Level 3) for staff development. The prestigious award was received from the North West Staff Development Network which recognised Mersey Care as one of only six out of 72 organisations across the North West to have achieved Level 3, reflecting our commitment to staff development.
12 13

Rebuild CBU used the Green Light Toolkit to increase awareness throughout the Trust and the wider health and social care economy of the needs of people with a learning disability accessing health care. Training events have helped staff to become better equipped when dealing with service users who have a dual diagnosis. Cross working has also taken place between consultant psychiatrists, police and probation.
Hope House Drug Dependency Unit in Liverpool closed in 2011 and the Trust opened the Drug and Alcohol Recovery Team (DART) at 3 to 5 Rodney Street in Liverpool in 2012. A recovery based approach for service users with addictions is the basis of the new service. The year saw the development of an acute care model for older people’s services within Positive Care Partnerships CBU, complementing the current adult mental health service model and delivering efficient and effective care to older people. The older adult inpatient wards now have dedicated older adult acute care consultants and are working toward a needs-led service.
SaFE Partnerships CBU has secured funding to develop an enhanced care team to work with Scott Clinic patients with more complex needs by providing psychological input to service users and to support existing staff and develop their skills.
Regular chaplaincy provision within inpatient services was increased throughout 2011- 2012 and strengthened by the introduction of a pilot programme of volunteer pastoral assistants. Work to raise the profile of spiritual and pastoral care resulted in increased referrals from community services particularly on managing the impact of bereavement on mental health. Mindfulness pilot groups were extended to a third of community mental health teams.
A national conference on spirituality and mental health was held in October providing training for a large number of Mersey Care staff. The team continues to roll out a structured training programme for staff.
SaFE Partnerships CBU’s prison in-reach team relocated from Oak House on the Aintree site into HMP Liverpool.
Liverpool CBU reviewed its day hospital services in partnership with other key stakeholders and agreed to provide some of the functions undertaken at Park Lodge at the Health and Wellbeing service at Broadoak.
To consolidate, develop and expand the range of services we provide
To enhance partnership arrangements to deliver a better range of quality services

Since the launch of Liverpool Community Alcohol Service in 2011 the original five community clinic sites have grown to ten with more planned for 2012.
The acting director of estates and facilities reviewed current facilities across Merseyside to gain economies of scale. The improvement of services will ultimately benefit service users, carers and staff by ensuring financial and physical resources are used appropriately and effectively.
During the last 12 months, the Trust chose two pilot sites to develop improvements to community mental health services. These will provide integrated services in partnership with service users, carers, commissioners and partner organisations. This will ensure choice, be socially inclusive, promote recovery and independence and deliver effective outcomes.
Rebuild CBU has embedded human rights based approaches to its person-centred services. These have had a significant impact on the lives of service users, demonstrated through service user and carer events where feedback was very positive. Rebuild staff have built powerful alliances which have helped to produce positive service change along with the benefit of former service users working as volunteers.
The service development and delivery team worked internationally and supported two projects. The development and submission of a European funding bid for a human rights project (Making Rights Real Project) is being undertaken with partners in Spain, Cyprus and Brussels and the Department of Health and the Human Rights and Social Justice Research Unit in London. The second project involved the development, submission and winning of a European trans-national project (Place and Train Project) looking at life-long learning and employment. This is a two year project working with partners in Spain, Lithuania, Greece and Holland and started in October 2011.
The team supported the Addiction Services CBU to secure a contract to provide the Liverpool Community Alcohol Service as a sub contractor to Aintree University Hospital NHS Foundation Trust. This added to what is already a successful relationship, as the two trusts secure and develop new business opportunities. The Addictions Service was also supported by the team to secure a place on the North Lancashire Framework for Substance Misuse which gives service users more choice in where they are treated.
Within high secure services this year, there has been a positive acknowledgement for staff who attended work for a year with no sickness absence. Health and wellbeing activities are available to all staff and specific activities have been arranged to take place in the high secure site at times that allow staff who work shifts to attend.
14 15

In 2011 the Department of Health signed our Tripartite Formal Agreement. This is an agreement between the Strategic Health Authority, the Department of Health and the Trust, supported by our lead commissioner, Liverpool PCT, confirming when the Trust can apply to become an NHS foundation trust. The agreement also outlines what issues need to be addressed before we can submit our application and the timeframe within which we must apply.
A consultation document, TIME to TALK, was launched inviting all Trust staff, service users and carers to take part in a conversation about how services can increase access to psychological thinking and working (including talking therapies) for the benefit of service users. The impact of this work will enable staff, service users and carers to be better informed about how psychological approaches can support recovery.
Addiction Services CBU continues to strengthen collaborative working with partners Intuitive Recovery, improving successful completions with an intense programme for service users to achieve abstinence within six months. The CBU was also part of the Pan-Lancashire Framework providing the opportunity to enhance tier 4 drug and alcohol detoxification and detoxification intervention services to adult patients through a framework (call-off) agreement with preferred providers.
The communications team advised on and supported the promotion of Asylum Link Merseyside and an article was published in the April/May edition of Mersey Cares. Similar work took place for the social care seminar which focused on asylum seekers and refugees with an article appearing in the June/July edition of Mersey Cares. A member of the team attended the first meeting of the service user and carer forum run by Irish Community Care Merseyside. Providing professional advice and support in the promotion and organisation of these events helped organising staff gain knowledge and experience and improve the quality of these events.
The director of communications and engagement gave a presentation on stakeholder engagement at the 13th national Chinese mental health, housing and social care conference. A stand staffed by the communications team promoted the work of the Trust including membership recruitment.
By continuing to invest in person centred planning, Rebuild CBU had a positive effect on staff morale which in turn has led to an overall improvement in the standards of care delivered by our staff. It has also led to a greater involvement and ownership of staff in patient care and greater involvement of service users and their carers in the care journey.
To become a better organisation by building on our involvement with stakeholders and strengthening our governance

This objective has been key to Rebuild’s ‘move on’ project which has already seen the successful transition of service users into their own homes in the community after many years of inpatient services.
As part of our application to achieve foundation trust status, the Trust had an overall target of 10,124 members to recruit by 31st March 2012. This was exceeded and means that the Trust is actively engaged and in touch with this large group of people who reflect our staff and our community. Information about membership is available from the membership office on 0151 473 2885 or join online at www.merseycare.nhs.uk
Liverpool City Council formally approved planning consent for Mersey Care to build a new mental health inpatient facility on the former Ian Skelly site off Edge Lane, Liverpool. This was a major step forward for our proposals to modernise our services within the TIME Project. Plans for a similar facility on the old Walton General Hospital site were approved in January 2011 and together the two new inpatient units will help modernise Liverpool and Sefton inpatient services, replacing old and unfit buildings at other Mersey Care sites, as outlined in our five-year Integrated Business Plan.
Demolition work began on the Walton Hospital site on 1st August 2011 in preparation for a new inpatient unit as part of phase one of the TIME Project. Most of the material will be reused on site to create the foundation of the new facility. In addition we worked with local artists, residents and schools to decorate parts of the hoardings promoting health and wellbeing and reducing stigma and telling children not to try to enter the site.
These new units will provide modern, fit-for-purpose healthcare in accommodation which respects patients’ needs for privacy and dignity. They will be two 85-bedded units offering single sex accommodation in single bedrooms with their own bathroom, as well as activity and garden areas. Liverpool CBU was represented in all of the major TIME Project work streams and has given valuable input into future plans.
Rebuild CBU continues to work closely with colleagues in estates to ensure that existing buildings are maintained to a high standard and that work on the acquisition of buildings for future service delivery will remain a priority. The CBU has maintained close liaison with the estates department to ensure effective progression of the estates strategy to ensure appropriate provision is made for Wavertree Bungalow and the Brain Injury Rehabilitation Centre.
Our four major key developmentsThe TIME (To Improve Mental health Environments) Project
16 17

Liverpool and Positive Care Partnerships CBUs reviewed their service provision across community services, in line with the improving community mental health services programme. Two pilot sites will start in June at Newhall and Arundel House.
We will continue to position ourselves to take advantage of any new business development opportunities as they arise.
We intend to use our estate more effectively and more efficiently in the future and following rationalisation will raise funds from sale proceeds. We will use this resource to finance a replacement and modernisation programme.
To improve community mental health services
New business development
Effective estates strategy

The Department of Health introduced the Equality Delivery System (EDS) to all NHS trusts in 2011 bringing significant changes to the equality agenda for the NHS. EDS enabled Mersey Care to assess itself, in partnership with representatives from the communities we serve, staff groups and key stakeholders in four key areas:
• Better health outcomes for all• Improved patient access and experience• Empowered, engaged and included staff• Inclusive leadership.
Our aim for the next year is to improve on our rating and continue to develop the system of working with partners to look at progress made and improve where we identify gaps.
A second change for equality came with the general and specific duties required as a part of the Equality Act 2010. The general duty directs all public bodies to:
• Eliminate unlawful discrimination, harassment and victimisation and other conduct that is prohibited by the Act
• Advance equality of opportunity between people who share a characteristic and those who don’t
• Foster good relations between people who share a characteristic and those who don’t.
Mersey Care published equality information to demonstrate some of the activities and progress it has made to meet the duty. We also defined six equality objectives to direct the Trust’s commitment to equality and human rights with the aim of ensuring it is central to what the Trust does and how it is done. We use internal and external governance checks, such as the quality account, to analyse the quality of the services we provide to people with protected characteristics. The objectives were developed in partnership as a part of the EDS process. They are:
• To have comprehensive service user equality data• To have comprehensive staff equality• Analysis of service user experience by protected characteristics• Data reported to the Trust Board and all committees of the Board to be regularly
analysed by protected characteristics• Service change being developed to meet the Trust’s strategic objectives will
explicitly take account of the needs of those with protected characteristics and human rights based approach
• Mersey Care will introduce equality and human rights analysis to replace equality and human rights impact assessments.
Equality, diversity and human rights
18 19

The Trust has a single equality and human rights scheme in place for 2010 - 2013. The equality and human rights action plans for the scheme are monitored internally by equality co-ordinators within each of the CBUs and specialist management services. The Trust’s equality and human rights steering group provides the external governance reporting annually to the Board. The steering group is chaired by a non-executive Board member and attended by members of the communities we serve. It acts as a critical friend to the work we do, enabling positive challenge to the equality and human rights team for the Trust and this in turn enables developments to be discussed and introduced.
A major achievement by the Trust in May 2011 was the accreditation of the prestigious international environmental management standard, ISO 14001, for implementing effective environmental management practices at its Maghull site. This was a key objective of the Trust’s Environmental Strategy.
The ISO 14001 Standard indicates the Trust has adopted a quality approach to environmental management and minimises any adverse impacts on the environment. Following a four- day assessment the appointed auditors highlighted particular areas of commendation on the Trust’s waste management facilities on site, the high level of staff awareness of environmental communications activities, its comprehensive approach to carbon management and the Trust’s on-going commitment to continual improvement in environmental performance.
The Trust was re-accredited to the Carbon Trust Standard during the year, following initial accreditation in 2009. Award of the standard requires three criteria to be met:
• Submission of an accurate carbon footprint measurement including all required emission sources
• Demonstration of an absolute reduction in the organisation’s carbon footprint• Demonstration of good carbon management including carbon governance,
accounting, reduction methods and targets in accordance with the Standard.
The Trust is continuing to meet the commitments set out in its five-year carbon management plan which sets out a 30% reduction in CO2 by 2015, and underpins potential financial savings of over £1m annually by that date. The drivers for this commitment are achieving reductions in environmental impact, improving the health of the people of Merseyside and reinvesting the savings made into therapeutic improvements for our service users.
Environment and SustainabilityEnvironmental management
Carbon management

The carbon emissions and energy consumption figures for the current year are as follows. These are currently based on projections using data from 10 months and so are subject to further revision.
Projects successfully implemented to date have included the installation of building management systems (computer-based systems that control and monitor energy using equipment to optimise efficiency) in Trust local services properties. Voltage optimisation equipment has also been installed in Heys Court and the Hesketh Centre. These two projects have anticipated annual savings of £33,700.
Carbon emissions 2009 -10 2010 -11 2011-12 Target by(electricity and gas) (base year) 2014 -15
CO2e tonnes 11,222 11,175 10,306 7,855
Carbon emissions savings 2010-11 2011-12(electricity and gas)
Actual CO2e tonnes 47 869
Annual Target CO2e tonnes 327 796*
Percentage achievement 14% 109% of annual target
*Target for 11-12 increased on original carbon management plan target in line with under-achievement of the 10-11 target
Greenhouse gas emissions indicator Consumption Emissions (MWh) (CO
2e tonnes)
Scope 1 (Direct) Emissions 28,961 5,365* - gas consumption
Scope 2 (Indirect) Emissions 9,062 4,941* - electricity consumption
Scope 3 – official business travel N/A 51,657** emissions (air, road, rail)
* best estimates based on average 10 month data ** estimate based on previous years.
Financial indicator for energy Cost £
Cost of Scope 1 and Scope 2 consumption 1,752,581
Cost of Scope 3 – official business travel 2,372,499
20 21

The cost of the Trust’s carbon reduction commitment (CRC) obligations for 2010 - 2011 was £127,524, based on ‘core regulated’ carbon emissions of 10,627 tonnes equivalent of CO2 (carbon allowances cost the Trust £12 / tonne). The exact cost for the current year is subject to the finalisation of emissions data.
As part of meeting the Trust’s CRC obligations, the energy management function has been outsourced to MITIE through a maintenance contract. This provides the Trust with bill validation, energy usage monitoring, collation of consumption patterns and compilation of the Trust’s annual carbon footprint report as required under statutory CRC obligations. The latest carbon footprint report saw the Trust achieving a rank of 597 out of 2103 in the national CRC performance league table and being positioned 42 out of 151 for all NHS organisations.
The Trust has engaged consultants Carbon Credentials to conduct a stage 1 internal audit of the Trust’s performance under the CRC Energy Efficiency Scheme to meet the Environment Agency’s audit requirements. Out of 10 areas of audit, six have gained ‘approval’ status with the other four awarded ‘approval with observations’ status. Twenty-seven recommendations have been put forward to the Trust for implementation. A stage 2 audit will be performed in May 2012.
Mersey Care was one of only a few NHS trusts invited on to a national committee involved in selecting and approving contractors to provide infrastructure upgrades as part of a £100m national ‘Carbon and Energy Fund’.
To maintain the momentum needed to achieve the increasingly tough targets under the carbon management plan, a further five capital projects (costing £658,000) have been identified, including a building management system for high secure services and photo-voltaic solar cell installations to generate electricity from sunlight on various Trust properties. Once implemented these would provide annual savings of at least £216,000.
As a major user of domestic water, the Trust aims to manage its consumption responsibly through its environmental management system. Water consumption in previous years has been on an upward trend, and during 2011- 2012 major water leaks occurred within the high secure site as a result of an outdated mains supply system failing to cope with land subsidence. The Trust has now set an environmental improvement objective within its ISO 14001 environmental management system, for a wholesale replacement of the water mains system during 2012 -2013.
Water consumption and management
Finite resource consumption indicator 2011-12
Water consumption (m3) 169,259
Total expenditure - water £ 472,661

The production of clinical and hazardous waste by the Trust involves the commitment of significant financial resources to ensure statutory responsibilities are met. As a result we are working towards a concept of total waste management to reduce pollution and the Trust’s carbon footprint and make efficient cost savings that can be diverted to direct patient care.
The Trust has rolled out an integrated waste and recycling contract across all sites during the year, in conjunction with waste contractors Bagnall & Morris. Recyclable wastes are collected within the general waste containers and separated out into recyclable fractions at a transfer station off site. On average between 70 - 80% of collected general waste (not including clinical waste) is now sent for either recycling or energy recovery (utilising refuse derived fuel).
Challenges remain in minimising the overall production of waste at source as well as reducing the amount of non-clinical waste being disposed of through clinical waste receptacles. A recent clinical waste audit indicated that between 40 - 50% of clinical waste bins contained waste that should have been disposed of as domestic waste.
We continued to develop our arrangements for dealing with major incidents and other emergency situations throughout this year. A full review of the Trust major incident plan has been undertaken and the plan amended to reflect internal changes and the changes to the wider NHS.
Waste management
Waste minimisation and management 2011-12 % indicators (tonnes)Waste recycled / reused 407 52
Waste incinerated (clinical waste) 114 14 energy from waste
Waste to landfill 268 34
Total waste arising (tonnes) 789 100
Financial indicators on waste
Cost of waste incineration / energy from waste £ 45,445
Total expenditure on waste arising £ 174,635
Emergency planning
22 23

The plan has been tested on several occasions with exercises and real-time situations. It is supplemented by other contingency plans and guidance documents that relate to events such as fuel shortage, pandemic influenza, heat wave and floods. These are supported at CBU level with robust business continuity plans, designed to ensure the continued provision of services in the event of a major incident, whether that is internal or external to the Trust.
Development of the Trust’s major incident and contingency plans lies with the emergency planning forum which has met throughout the year.
Emergency planning can only be successful if our plans are linked with those of the wider health economy and to this end the Trust is an active member of the NHS Merseyside Health and Social Care Group. With representatives from all local trusts, this group, represented by the head of quality and risk, ensures that plans are not written in isolation but are done so with the co-operation and involvement of key partners and stakeholders, essential in any emergency situation where assistance may be required.
Risk management enables individuals and the Trust to deal competently with all key risks, clinical and non-clinical, providing confidence that the Trust will achieve its objectives.
The integrated governance committee is the Trust’s overarching committee responsible for managing risk and providing advice and expertise to the Board on risk management issues.
This is supported by the Board and the following sub-committees:• Audit committee• Remuneration committee• Mental Health Act managers committee• Health and safety committee• Infection control committee• Drugs and therapeutics committee• Information governance and Caldicott committee• Research governance committee.
Risk management

The head of quality and risk is responsible for implementing the effective systems and processes of risk management across the organisation; the identification, management and monitoring of risks; and providing reports, information and training as appropriate. Other senior staff, managers and individual staff members, as well as executive and non-executive directors, and clinical directors, are responsible for ensuring they engage with risk management objectives to ensure their clinical and managerial responsibilities for risk management are met.
Each CBU has governance arrangements in place and the local governance lead is responsible for implementing the corporate risk management processes locally, in addition to facilitating the sharing of best practice.
The development of effective risk management across the organisation is underpinned by clear processes and procedures.
Embedding risk management as a core activity within the organisation is achieved through many systems and processes and 2011-2012 has seen:
• A fully revised assurance framework linked to the Integrated Business Plan• Implementation, development and scrutiny of CBU risk registers• Work to improve the systems and processes that support the assurance framework• Changes to organisational committee structures to improve effectiveness and
ensure all committees actively support the risk agenda• Development of action plans to ensure continued compliance with NHS Litigation
Authority (NHSLA) risk management standards• Plans implemented to achieve full compliance with the Care Quality Commission’s
essential standards of quality and safety• Continued development of the emergency planning forum including revisiting and
ratifying a revised major incident plan• Reviews of, and improvements to, the complaints, claims and adverse incident functions• Significant development of organisational policies, particularly relating to the
NHSLA standards• Development of environmental risk assessments to reduce the risk of suicide in
inpatient units• Unconditional registration from the Care Quality Commission.
Commenting on the assurance framework, Mersey Internal Audit Agency stated: “An assurance framework has been established which is designed and operating to meet the requirements of the annual governance statement and provide reasonable assurance that there is an effective system of internal control to manage the principle risks identified by the organisation.”
24 25
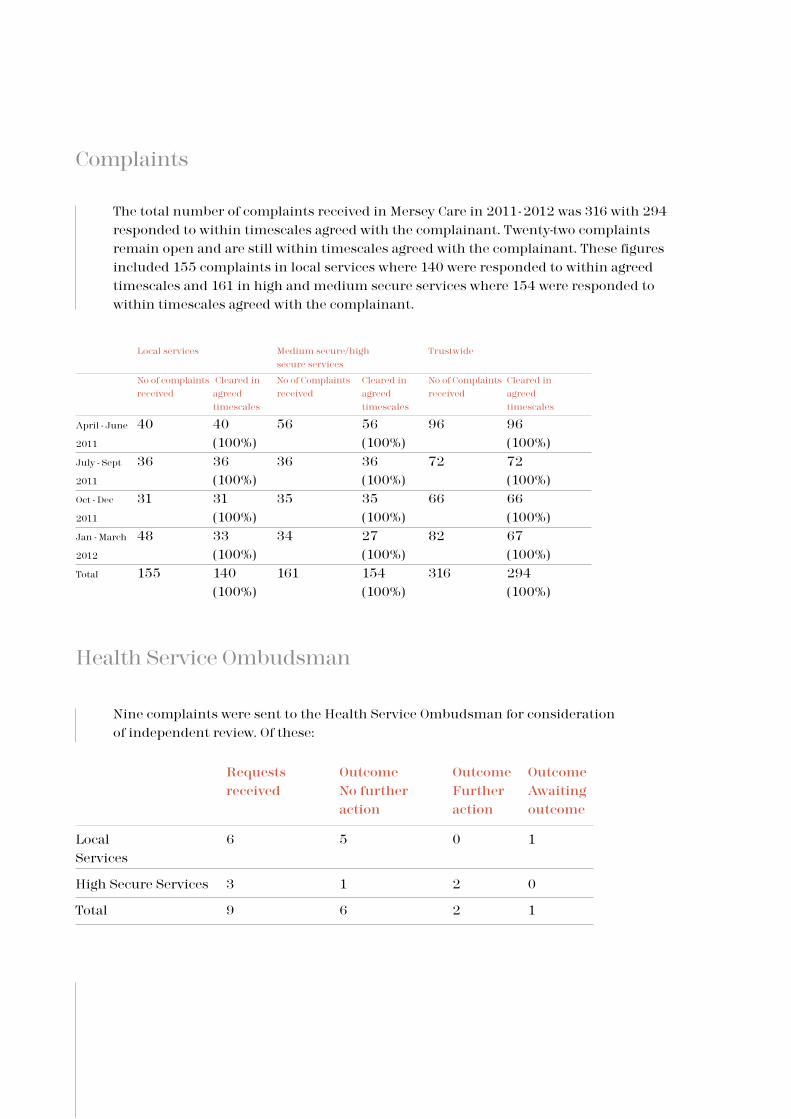
The total number of complaints received in Mersey Care in 2011- 2012 was 316 with 294 responded to within timescales agreed with the complainant. Twenty-two complaints remain open and are still within timescales agreed with the complainant. These figures included 155 complaints in local services where 140 were responded to within agreed timescales and 161 in high and medium secure services where 154 were responded to within timescales agreed with the complainant.
Nine complaints were sent to the Health Service Ombudsman for consideration of independent review. Of these:
Complaints
Local services Medium secure/high Trustwide secure services
No of complaints Cleared in No of Complaints Cleared in No of Complaints Cleared in received agreed received agreed received agreed timescales timescales timescales
April - June 40 40 56 56 96 96
2011 (100%) (100%) (100%)July - Sept 36 36 36 36 72 72
2011 (100%) (100%) (100%)Oct - Dec 31 31 35 35 66 66
2011 (100%) (100%) (100%)Jan - March 48 33 34 27 82 67
2012 (100%) (100%) (100%)Total 155 140 161 154 316 294 (100%) (100%) (100%)
Requests Outcome Outcome Outcome received No further Further Awaiting action action outcome
Local 6 5 0 1 Services
High Secure Services 3 1 2 0
Total 9 6 2 1
Health Service Ombudsman

• The number of complaints received by the Trust has reduced significantly from 372 during the period 1st April 2010 to 31st March 2011, to 316 during the last 12 month period. This can be largely attributed to the reduction of complaints concerning patients’ property in high secure services after measures were taken by the Trust to address this issue.
• The number of complaints referred to the Parliamentary and Health Service Ombudsman has also reduced significantly from 18 to 9 during the last 12 month period.
As a result of complaints, changes to service provision have been made:
• The process used for booking outpatient appointments at the memory clinic has been improved:
- paper clinic books were removed - a clinic has been more clearly identified to reflect that it is ‘nurse led’ to avoid
any possible confusion/error - an additional dedicated administrator has been provided to support the clinic.
• Facilities for service users with a disability were improved following a workplace inspection at the Park Unit in the Hesketh Centre focusing on disabled access undertaken by the health and safety lead and the service governance co-ordinator.
• Patients in high secure services raised concerns about the size of food portions:
- Several wards were visited and it was agreed that some of the portion sizes would be increased.
• Following a complaint that a patient’s confidentiality was breached in high secure services, the following recommendations have now been actioned:
- All documents deemed clinical waste are shredded immediately after use and clinical waste awaiting disposal is stored within a designated non-patient area of the ward
- All wards have a large industrial sized shredder and have been issued with instructions to ensure any clinical waste awaiting disposal is secured in a designated area that does not contain any patient property
- Patients’ property must not be stored anywhere on the ward other than within designated secure areas of the ward identified for this purpose.
Comparison with 2011
Service improvement
26 27

Summary of other personal data related incidents in 2011 -2012
Summary of personal data related incidents
Date of Nature of Nature of data Number of Notification incident incident involved people steps potentially affected14th December Diary stolen Initials and 65 Decision made 2011 from postcodes not to disclose employee’s car on clinical grounds
Further action Recommendations on information risk 1. Staff should ensure both in the workplace and at home that
physical security measures are adequate to prevent unauthorised access to, or loss of diaries or any other personal data required to be kept by any staff member working in the Trust and in particular personal data should not be left unattended in vehicles.
2. Hard copy documentation should contain the minimum amount of personal data required for its purpose and will be anonymised where possible.
3. Managers must ensure that their staff have access to and awareness of the content of Trust policies around retention, storage and use of personal data and have attended all training relevant to these policies.
4. Other measures to ensure the security of personal data against accidental loss will be explored such as the use of electronic diaries and digital technology which would minimise the amount of hard copy documentation used by staff.
Category Nature of Incident Total
Level 1 Unauthorised disclosure of paper documents 2
Level 1 Loss of paper documents from secured NHS premises 1
Level 2 Unauthorised disclosure of paper documents 1
Level 3 Loss of paper documents from outside secured 1 NHS premises

The Trust achieved all financial duties in 2011 - 2012. The performance against the targets is summarised below.
1. To achieve a balanced position on the income expenditure account
The Trust had an income budget of £196m in 2011 - 2012. The Trust made a surplus after impairment of £5m at the year end.
2. To operate within the capital resource limit (CRL)
The Trust operated within its CRL. The Trust had capital funding of £10.3m available in 2011 - 2012 and spent £7.2m during the financial year. All of the underspend will be added to the Trust’s 2012- 2013 capital funding.
3. To operate within the external financing limit (EFL)
The Trust had a duty to hold a minimum cash balance of £9.4m at the end of the year. The Trust achieved a balance of £13.5m.
4. To achieve a 3.5% return on the assets owned by the Trust
This target was achieved with a 3.5% return on net assets.The Trust received additional funding from Commissioners in 2011 - 2012 for service developments, including:
• £2.6m for quality and innovation (CQUIN)• £0.3m for dementia services• £0.4m for addiction services• £0.1m for other services developments.
The Trust also received funding of £4.6m as a contribution to inflationary cost pressures and was required to generate efficiency savings of £7.8m. Staff throughout the Trust worked hard to identify and deliver the savings whilst maintaining high standards of patient care. The Trust Board recognises this contribution and is grateful for the efforts of all staff.
Finance director’s reportSummary
28 29

The income received in 2011 -12 of £196m was generated from a number of sources. This is summarised in Chart 1.
The Trust has used the income it receives to fund the cost of services provided. The major areas of cost are summarised in Chart 2.
Income and expenditureIncome
Operating expenditure
AnaIysis of Income
Education and Training
Staff Costs 79%Establishment and Premises Costs 9%Clinical Supplies and Services 7%Depreciation and Authorisation 3%Other Costs 2%

The Trust spent £7.2m on capital schemes during the year. An analysis of how capital resources have been used is summarised in Table 1.
The Better Payments Practice Code (BPPC) requires the Trust to pay all valid invoices within 30 days of receipt of goods. In 2011-2012, the Trust achieved an average of 98%.
The Trust is committed to assisting local businesses and is focused on paying invoices for small businesses and individuals within 10 days where possible.
The prompt payment code is a payment initiative developed by Government with the Institute of Credit Management (ICM) to improve liquidity for small businesses.
Mersey Care has signed up to the code and is committed to pay all invoices relating to small and medium businesses and individuals within 10 days, wherever practical.
A guide for suppliers and contractors regarding the code is available on the Trust website, within the financial policies and procedures section.
In March 2012, the Trust Board approved a financial strategy and a five year financial plan that will support the delivery of the Integrated Business Plan.
The Trust is planning to achieve an annual surplus of between £4m to £5m over the next five years. The Trust will continue to achieve all financial duties and will ensure the continued achievement of the Better Payment Practice Code (BPPC).The NHS Operating Framework for 2012 -2013 stated the requirement for savings
Capital
Table 1 – Analysis of capital expenditure
Capital Scheme £000
High Secure Services CBU schemes 3,262
TIME Project 1,584
SaFE Partnerships CBU schemes 831
I.T. infrastructure 464
Positive Care Partnerships CBU schemes 384
Estate improvements 658
Total Expenditure 7,183
Better payment practice code
Long term outlook
Prompt payment code
30 31

targets of 4% to be found each year. Savings plans of £36.9m for the period 2012 - 2013 to 2017 -2018 have been produced to ensure the Trust will achieve recurrent financial balance each year. The savings target for 2012 - 2013 is £7.9m. Differential savings targets have been applied within the Trust to target areas of inefficiency.
The Trust’s services are benchmarked nationally and a reference cost index is awarded that shows each Trust its relative efficiency. A score of 100 represents the average. A score above 100 indicates a Trust is above average cost and a score below 100 indicates a Trust is below average cost. The Trust’s productivity has improved and the reference cost score has reduced from 106 to 103. A target has been set within the financial plan to reduce the reference cost score for local services to under 100 by 2013 -2014.
The Trust has an agreement with Liverpool and Sefton Health Partnerships to deliver two new inpatient facilities in Walton and Wavertree. The Walton scheme is expected to reach financial close in September 2012 with build completion expected September 2014. The Wavertree scheme is dependent on the land acquisition for which negotiations are ongoing and financial close is expected later in 2012 -2013.
The Trust will become host of the Health Informatics Service (HIS) from April 2012. The HIS provides IT services for 11 NHS bodies in the Mersey region. This will increase the Trust’s income and expenditure by £12.5m in 2012 -2013.
The external auditor for the Trust was the Audit Commission, who provides audit services in relation to the statutory audit duties as required by the Department of Health in providing an independent audit opinion. The total fee for work carried out during 2011 - 2012 was £139,493 (2010 - 2011, £158,288) detailed as follows:
In preparation for our quality account for 2011 - 2012 the Trust has undertaken a process of involvement and engagement with key stakeholders to establish their views on what our key priorities should be. Representatives from the following groups have been involved and invited to provide views on our priorities and the draft quality account:• Local Involvement Networks (LINKs) for Liverpool, Sefton and Knowsley• Local overview and scrutiny committees• NHS Merseyside
Trust auditors
Audit services £
Financial statements and VFM 151,618
Rebate 2011-12 (12,125)
139,493
Quality account

• Mersey Care NHS Trust Members Council• Local service user groups• The executive team• The quality steering group• Trust Board.
In addition to receiving these views, the quality steering group has considered suggestions for quality improvement priorities and has decided that it would be beneficial to have new priorities linked to the three main elements of quality:• Patient safety• Clinical effectiveness• Patient experience.
After consultation and discussion with the Trust Board the areas of quality improvement for 2012 - 2013 will be to:• Improve access to services, especially at times of crisis and for psychological
therapy, by clinical audits of current access and the availability of evidence based interventions
• Promote harm-free care through the use of the national ‘safety thermometer’ and continued analysis of incidents and complaints
• Develop a quality dashboard for use at individual, team, CBU and Board level; this will include the measures for harm-free care, patient experience, effectiveness, and gather key quality metrics for wide dissemination and learning
• Review progress of care clustering as part of payment by results for mental health, focusing on transition between clusters, and care pathways for recovery and co-existing physical health needs
• Set up ‘Mersey Care AQuA’ as a successor to the quality steering group, to help stimulate a quality improvement culture
• Quality reviews of cost improvement plans to be held with CBU directors and specialist management services managers at the extended executive team meetings in 2012 - 2013
• Embedded equality and human rights throughout all aspects of the quality account process.
These priorities are all linked to the Trust’s quality strategy and ensure the areas of safety, clinical effectiveness and patient experience remain at the top of our agenda.
In June 2011, the Trust published its second year of quality accounts reporting on the quality of services in 2010- 2011 against three areas of priority: improving the care pathway, improving the patient environment and improving stakeholder involvement. Following extensive engagement with key stakeholders, it was decided that within these three areas there were the following seven specific areas on which to focus quality improvement action: • Health of the Nation Outcome Scores• Cost improvement plans• Recovery, health and wellbeing approach• Incidents and complaints
32 33

• Safeguarding• Membership• Quality development.
With the commitment and dedication of its staff the Trust has made excellent progress in all of these areas.
Health of the Nation Outcome Scores (HoNOS)
Aim: HoNOS will be recorded for all relevant service users, analysed and used to ensure continual improvement in defined outcomes. This process will be linked to the Trust’s clinical audit programme to ensure evidence-based care pathways are implemented.
Improvements achieved:Action plans to achieve targets were developed by each CBU.• Reports are now created on the electronic portal (data warehouse)• Weekly communications were issued Trust wide• Over 13,500 service users assigned to a mental health cluster between April to December 2011 – 98% of eligible service users.CBUs are analysing movement between clusters and outcomes.
Cost improvement plans
Aim: Regular review and interrogation of cost improvement plans using a quality focused impact assessment tool will be undertaken to identify potential risks to quality, and support CBUs to improve quality and ensure efficient care planning.
Improvements achieved:• Review completed. Minor changes to documentation agreed and implemented• Initial list of indicators shared with CBUs• All CIPs have been individually risk assessed for financial deliverability and the
impact on quality; the key themes and risks have been shared and discussed with all CBUs/SMSs to assess the interdependency of plans
• Summary plans and confirmation of the risk assessment and agreement of the medical director and executive director of nursing presented to the Trust Board on 29th March
• There is agreement to repeat the sharing and supportive challenge within the wider executive meetings during 2012 - 2013.
Key area of improvement 1
Key area of improvement 2

Recovery, health and wellbeing approach
Aim: Development of a recovery, health and wellbeing approach as part of the innovative ‘Implementing Recovery through Organisational Change’ (ImROC) project which will identify and share outcome measures based upon 10 areas of organisational change that are thought to improve recovery (including appropriate and timely access to physical health care resulting in reduced levels of morbidity for Trust’s service users).
Improvements achieved:• The ImROC project has continued to develop strategy, co-production
and personalised care• The ‘Launch Pad’, which is an emerging recovery college, was recently started• Service user co-workers are in place with each of the project leads to develop peer
support initiatives.
Incidents and complaints
Aim: A rolling ‘Top 5 programme’ will aim to reduce the frequency of the three most common types of incident, and two most common types of complaint each year. Evidence-based guidance and clinical audit outcomes will be used to produce monthly reductions in incidents of: violence and aggression, falls and self- harm. Complaints about care and treatment and staff attitude will be analysed and action plans developed in response.
Improvements achieved:• Assaults reduced by 19%, slips, trips and falls by 13%; self harm incidents rose
slightly by 6% but the severity of harm fell - this work has helped stimulate better reporting and analysis of incidents
• The top two types of complaints have also reduced. Training has taken place for staff with the focus on these key areas of risk
• Psychiatric Intensive Care Unit assault figures have reduced noticeably and working methods have been amended.
Key area of improvement 3
Key area of improvement 4
34 35

Safeguarding
Aim: Development of more effective safeguarding services for children and adults,
Improvements achieved:• Quality reporting processes for safeguarding children and vulnerable adults• Mersey Internal Audit - significant assurance achieved in 2011- 2012• Service user and carer leaflet developed and Rebuild service users have agreed to
assist in development of easy read safeguarding policies• An unannounced inspection by the CQC in October 2011 found that the STAR Unit
at Mossley Hill Hospital was compliant with the essential standards of safety and quality in relation to safeguarding.
Membership
Aim: Development of the membership and governorship in preparation for foundation trust authorisation.
Improvements achieved:• The Members Council was established in January 2012 and met for the first time in March• The Trust achieved its target for recruiting members - over 10,000.
Quality development
Aim: Continuation of service user and carer engagement in quality improvement, including the quality account and quality strategy (which will be produced in 2011-2012), and development of better measures of the experience of care.
Improvements achieved:• Service user representative member of the quality steering group• Regular meetings with LINks• Patient surveys have taken place using the ‘Patient Experience Tracker’ and there
are now 24 devices in the Trust.
Key area of improvement 6
Key area of improvement 7
Key area of improvement 5

• Care Quality Commission unannounced visit of the STAR Unit at Mossley Hill Hospital found the unit to be fully compliant with the standards assessed
• SaFE Partnerships CBU has opened Reed Lodge, a purpose built 10-bed step-down facility, to expand the care pathway based on our service user needs and in line with commissioner intentions
• Successful implementation of the healthy lifestyles programme on two wards in High Secure Services CBU, which resulted in significant weight reduction and increased uptake of physical activities; as a consequence, the pilot will be further extended over the coming year
• The High Secure Services CBU achieved a 50% reduction in seclusion and segregation through shared multidisciplinary efforts, underpinned by recovery principles, focusing on enhanced training initiatives for all clinicians and support for ward based nurses
• In Positive Care Partnerships, the team from Newhall CMHT devised a unique colouring book, called Our Hospital, which helps young children (three to seven year olds) whose parents have mental health problems. Won “winner of winners” in the 2011 Positive Achievement Awards
• All wards in Positive Care Partnerships accredited with Aims (Acute Inpatient Mental Health services programme), with Clarence Ward and The Park Unit being accredited as excellent
• The memory service in Liverpool was the first service nationally to be accredited by the Royal College of Psychiatrists as ‘excellent’ in 2010. The service has been re-accredited and retains its ‘excellent’ status
• In Liverpool CBU a new service started in January 2012 aiming to improve the management of physical health and wellbeing for people with mental illness; the service will incorporate existing health promotion, screening, self management and recovery initiatives.
Key achievements 2011-2012
36 37

I’m Mike. I’m Mersey Care.
When I was six months old I would play on the family piano.
But to me I have been given a talent and by playing on a Sunday for church services I’m applying that talent back for God and assisting others on their spiritual journey.
I’m proud of being responsible for the Finance Cadets. It’s a scheme run by the Skills Academy for Health to give young people who have just left school the opportunity to gain experience in the NHS while learning before they move on to permanent employment. There are two cadets at the moment and it has been good to see them make the transition from school to the work environment. They sometimes encounter problems throughout their placement and I try to encourage and nurture them throughout this time. Cadets both past and present know that they only have to pick up the phone if they have a query, or need somebody to talk to. This year, I was honoured to receive the first Skills Academy for Health Michael McNally Mentor of the Year Award, which was established in memory of one of our Cadets who sadly passed away during 2011.
The way I look at it is, people have invested time and energy in me over my lifetime so why shouldn’t I give something back? That’s why… I’m Mike and I’m Mersey Care.
As I got older I took up the piano properly, did my exams and as my dad was a vicar they asked me to play in church one Sunday. I’ve been playing either the piano or organ in church since the age of 12 and I’m 44 now.
My Sundays might seem a bit hectic to some people as I play in three parishes, starting first thing in Roby, doing a mid-morning service in Bootle and then an evening service in South Liverpool, and that’s every Sunday.
I’m very lucky to have played at Blenheim Palace, Liverpool Cathedral, not to mention cathedrals in Chester, Ripon and St Asaph. I’ve also been involved with the Royal School of Church Music and performances at the Royal Liverpool Philharmonic at various times.
There are a lot of people who are always looking for a quick fix and they pass over something and move onto something else. But for me having the tenacity to stick at something is what really brings the long-term gains.
In 1991 I got involved with the NHS Carols Service held each Christmas at Liverpool Cathedral and I am now its main organiser, with the support of Ann Bainbridge. The NHS choir has 250 people who rehearse from September onwards under five area co-ordinators and an orchestra of 40 musicians. It’s one of those events that people know about and ideas and support roll in each year and it somehow just happens. The one that sticks in my memory is the NHS 60th anniversary year in 2008 when we had nurses’ uniforms going back to Florence Nightingale’s time on display.
I started working in the NHS at 22 after studying accountancy at what was then Liverpool Polytechnic. My job at Mersey Care means I’m often a point of contact for anyone who has queries or problems they can’t solve and often get into unchartered financial territory and I do quite a bit of work on behalf of patients in high secure services because of the complexity of the issues involved. I think you have to be prepared to build up relationships with people, be willing to help and have a sense of humour too!
38 39

I’m Melissa. I’m Mersey Care.

I came to the UK in 1993 from Sierra Leone in West Africa, two years after the start of its civil war.
Then my ward manager said to me she could see I was a caring person and encouraged me to do more; she motivated me to do nursing. I said to myself this is a turning point in my life to get professionally qualified.
(an inspirational and achievement course to help develop leadership potential) which has made me more self-confident.
I live with my family in Everton and have made Liverpool our home. Sometimes it can feel strange being the only black person working on a ward but I’ve made lots of friends and I love to wear traditional dress at special occasions or get-togethers. It’s important to remember your culture and respect that everyone is different. That’s why… I’m Melissa and I’m Mersey Care.
I was born in Freetown, the capital, and I’m proud that I have two sons who were born there too, but I wanted a better life for my family.
Although English is the second language in Sierra Leone I found that language was my biggest barrier when I got here; I’ve worked hard to improve my English, which I think has helped my career. I lived in London at that time and had various cleaning jobs before becoming a healthcare assistant.
I started off studying general nursing but I dropped off. I had another try and applied to several universities looking at different courses before taking up mental health nursing at Liverpool John Moores University. It wasn’t easy; I had to move to Liverpool, leaving my family behind and I held down night shifts to send money back home.
I settled in and was getting through it, seeing my family whenever I could. Then in my third year while I was away someone set fire to the house where I was living, destroying all my coursework, text books, everything I needed to complete the course. My tutor suggested I take six months out to work,
earn some money and then come back to study again, but I insisted I did not want to give up. So with the help of friends I copied up all the coursework and got the books I needed to finish. It was a setback but I was so proud to finally graduate.
I come from a big family and I have been looking after my dad, so I know caring for people can be hard work, but I just love working with older people. I’ve been able to continue to do other things too and I’ve completed a programme
40 41

I’m Barry. I’m Mersey Care.

I started doing motivational talks to service users at the Kevin White Unit about what helped me through alcohol and drug abuse. Then one of my friends told me they were starting a volunteer programme at Mersey Care and asked if I’d be interested.
42 43
I was brought up in a big family in Huyton and Kirkbyso there was always cookinggoing on.I’ve always been able to cook but it was quite late in life that I learned to cook properly and studied to get some certificates to prove it.
I couldn’t complete the first professional cookery course I was doing at Liverpool Community College because of a health condition called fibromyalgia. It started about 10 years ago and is a bit like arthritis. It affects almost every muscle in my body, even my eye; it’s like having toothache all over your body, real Chinese water torture.
The medical profession don’t really understand it; a bit like they didn’t really know what M.E. (chronic fatigue syndrome) was a few years ago. One theory is it’s affected by atmospheric pressure and when the weather is bad I do feel it through pain. Sometimes the pain gets so bad I can’t get out of bed. It also causes me fatigue and that just adds to my anxiety. I know I have to avoid stress as that’s no good for it either.
Due to the condition and the fact I couldn’t finish the cookery course I developed depression and had treatment. But I knew I had to do something with my life and the following year managed to get on a course at Knowsley Community College. I thought that if I had some professional qualifications then one day I could move to a better climate where my condition might ease and I could work as a chef.
I’ve always been a drinker but when the fibromyalgia started I turned to drink in a big way. I was in a bad, dark place then. I was
also on cocaine but found the drug was making the pain worse, as well as affecting my mental health as I was hallucinating. When I came off the drugs I hit the alcohol even more, a bottle of vodka a day.
Everything seemed to go wrong including my relationship with family members. It took really good friends to tell me, with insults you wouldn’t believe, what they really thought of me. I couldn’t see it myself but when they said some of those things I thought they wouldn’t say them unless they were true. Something clicked.
I got booked into the Windsor Clinic. I met other people who had similar lifestyles to me. I realise now I was a horrible person because of the alcohol and drugs. Five years on I’m 53 but I still carry a picture of the Windsor Clinic on my phone – and every time I even think about alcohol I just look at that photo of the Windsor to remind me. I got the help I needed and thanks to friends, people at the clinic and lots of other places, I knew I had to do something to help other people like the person I used to be.
I’m all for service users and know that boredom can be a terrible thing when you are trying to stop drinking or taking drugs. I was asked if I could put my professional cookery skills to good use by teaching service users at the Windsor Clinic and Kevin White Unit. I love showing people how to cook simple things on a budget, encouraging them to do things, and keeping well by eating healthy things. That’s why...I’m Barry and I’m Mersey Care.

See the person, meet the need,
challenge the stigma.

Trust Board Members
Position New in year Date of leaving or change
Included in executive directors and senior staff at 31st March 2012
Alan Yates Chief Executive
Kim Crowe Executive Director of Service Development and Delivery
David Fearnley Medical Director
Neil Smith Executive Director of Finance and Performance
Helena McCourt Acting Executive Director 19.06.11 of Nursing and Care
Martin Brown Executive Director of High Secure 24.06.11 Services and Estates
Ray Walker Executive Director of High 20.06.11 Secure Services and Executive Director of Nursing
Non-executive directors and chairman
Beatrice Fraenkel – Chairman +
Brian Lawlor + *
Elizabeth Powell + *
Neil Willcox + *
Les Byrom 30.11.11
Michael Shields + *
Christopher Dowrick + *
Other senior staff
Christine Hughes Director of Communications and Engagement
Paul Weare Director of Security
Kath Davies Director of Workforce
Lindsey Dyer Director, Service Users and Carers
John Doyle TIME Project Director
+ Member of the Remuneration and Terms of Service Committee* Member of the Audit Committee (Chairman, Neil Willcox)
Year ended 31st March 2012
44 45
Incorporating register of interests

Name Job Title Declaration 2011-12
Beatrice Fraenkel Chairman • Liverpool City Councillor • Director, Normal Properties Ltd • Chair – Architects Registration Board • School Governor, King David High School • Fellow of the Royal Society of Arts • Trustee of St Georges Hall • Board Member of the Business Improvement District
(BID Board) • Member of Public Chairs Forum • Member of the Labour Party • Member of the Council of the University of the
South Bank, London • Council Member of Edge Hill University
Brian Lawlor Non-executive director • Partner, Morecrofts LLP Solicitors • Governor, Melling Community School • Trustee, Royal School for the Blind (Liverpool) Ltd • Vice Chairman, Marine Football Club • Director, Rossett Park Land Company Ltd • Company Secretary, Northern Premier Football
League Limited
Elizabeth Powell Non-executive director • Director, Age Concern Liverpool (Services) Ltd
• Trustee / Chair, Age Concern Liverpool & Sefton (Charity)
Neil Willcox Non-executive director • Director, Resman Ltd
Robert Michael Shields Non-executive director • Deputy Chairman, The Manufacturing Institute
Christopher Dowrick Non-executive director • Part-time general practitioner, Aintree Park Group Practice
Alan Yates Chief Executive • Partner, Head of Speech and Language Therapy Service – Royal Liverpool and Broadgreen University Hospital
Kim Crowe Executive Director of Service • Nil Return Development and Delivery
David Fearnley Medical Director • Nil Return
Christine Hughes Director of Communications • Trustee, Netherton Feelgood Factory and Engagement
Neil Smith Executive Director of Finance • Nil Return and Performance
Ray Walker* Executive Director of High • Nil Return Secure Services and Executive Director of Nursing
Helena McCourt* Acting Director of Nursing • Nil Return
Kath Davies Director of Workforce • Director, Tyre and Battery Specialists Ltd
Lindsey Dyer Director, Service Users and Carers • Vice Chair, The Reader Organisation
John Doyle TIME Project Director • Nil Return
Anne Cleminson Trust Secretary • Nil Return
Paul Weare Director of Security • Nil Return
Name *Note
Ray Walker Commenced in post 20.06.11Helena McCourt Acting ceased 19.06.11
Register of interests

1. What this report covers
This report to stakeholders:
• Sets out the Trust’s remuneration policy
• Explains the policy under which the Chairman, executive directors, and non-executive directors were remunerated for the year ended 31st March 2012
• Sets out tables of information showing details of the salary and pension interests of all directors for the year ended 31st March 2012.
2. Role of the Remuneration Committee
The Remuneration Committee is a committee of the Trust Board. An effective committee is key to ensuring that executive directors’ remuneration is aligned with stakeholders’ interests and that directors are motivated to enhance the performance of the Trust.
3. Membership of the Remuneration Committee
The members of the committee are the Chairman and all non-executive directors. Committee meetings are considered to be quorate when the Chairman and two non- executive directors are present. The Chief Executive may also attend in an advisory role except when his or her own remuneration or other terms of service are under discussion.
4. Service contracts
All executive directors have service contracts. Contracts are usually awarded on a permanent basis, unless the post is for a fixed period of time. Directors have a three month notice period within their contracts of employment, with the exception of the Chief Executive and the Director of Service Development and Delivery who each have a twelve month notice period. Termination payments are made in accordance with contractual agreements.
5. Remuneration policy for executive directors
Directors’ posts are currently evaluated using the North West Strategic Health Authority Job Evaluation Panel and are subject to approval by the Remuneration Committee. Any pay awards are agreed by the committee.
Directors participate in an annual appraisal process which identifies and agrees objectives to be met. This is supported by a personal development plan where appropriate.
The Trust does not operate a performance related pay scheme.
6. Remuneration policy for the Chairman and non-executive directors
Increases in the remuneration of the Chairman and non-executive directors are agreed nationally by the Department of Health and implemented locally by the Trust.
Senior managers’ remuneration report
46 47

7. Directors’ remuneration for the year ended 31st March 2012
2011-12 2010 -11
Salary Other Bonus Benefits Salary Other Bonus Benefits Remuneration Payments in Kind Remuneration Payments in Kind
Notes (bands of (bands of (bands of Rounded (bands of (bands of (bands of Rounded £5000) £5000) £5000) to nearest £5000) £5000) £5000) to nearest £’000 £’000 £’000 £’00 £’000 £’000 £’000 £’00
Executive Directors
Alan Yates – 160-165 77 160-165 79 Chief Executive
Kim Crowe – 115-120 54 115-120 50 Executive Director of Service Development and Delivery
David Fearnley – 1 85-90 105-110 35-40 37 85-90 90-95 10-15 34 Medical Director
Neil Smith – 120-125 22 120 -125 31 Executive Director of Finance and Performance
Ray Walker – 2 90-95 34 Executive Director of High Secure Services and Executive Director of Nursing
Martin Brown – 3 30-35 140-145 Executive Director of High Secure Services and Estates
Karen Wilson – 4 110-115 72 Executive Director of Nursing and Care
Helena McCourt – 5 20-25 5-10 Acting Executive Director of Nursing and Care

2011-12 2010-11
Salary Other Bonus Benefits Salary Other Bonus Benefits Remuneration Payments in Kind Remuneration Payments in Kind
Notes (bands of (bands of (bands of Rounded (bands of (bands of (bands of Rounded £5000) £5000) £5000) to nearest £5000) £5000) £5000) to nearest £’000 £’000 £’000 £’00 £’000 £’000 £’000 £’00
Other Senior Staff
Kath Davies – 90-95 18 85-90 19 Director of Workforce
John Doyle – 95-100 35 95-100 36 TIME Project Director
Lindsey Dyer – 75-80 12 75-80 Director, Service Users and Carers
Band of Highest 230-235 200-205 Paid Director Total Remuneration (£’000)
Median Total 28,373 27,976 Remuneration of all staff
Pay Multiple Ratio 8.2 7.2
Non-executive Directors
Beatrice Fraenkel – 20-25 2 20-25 - Chairman
Leslie Byrom 6 0-5 1 5-10 -
Brian Lawlor 5-10 1 5-10 -
Elizabeth Powell 5-10 1 5-10 -
Michael Shields 5-10 2 5-10 1
Philip Thomas 7 0-5 -
Christ Dowrick 8 5-10 0-5 -
Neil Willcox 5-10 1 5-10 -
Benefits in kind are the taxable gains on lease cars.
7. Directors’ remuneration for the year ended 31st March 2012 (continued)
48 49

Emoluments
Notes:1 The bonus payments relate to Clinical Excellence awards.2 Ray Walker was appointed as Executive Director of High Secure Services and
Executive Director of Nursing on 20th June 2011.3 Martin Brown was Executive Director of High Secure Services until 24th June 2011.4 Karen Wilson left the Trust on 28th February 2011.5 Helena McCourt was acting Executive Director of Nursing and Care from 1st March
2011 to 19th June 2011.6 Leslie Byrom retired as a Non-executive Director on 30th November 2011.7 Dr Philip Thomas retired as a Non-executive Director on 13th October 2010.8 Christopher Dowrick was appointed as a Non-executive Director (designate) on 1st
December 2010.
Benefits in kind are the taxable gains on home to work expenses.
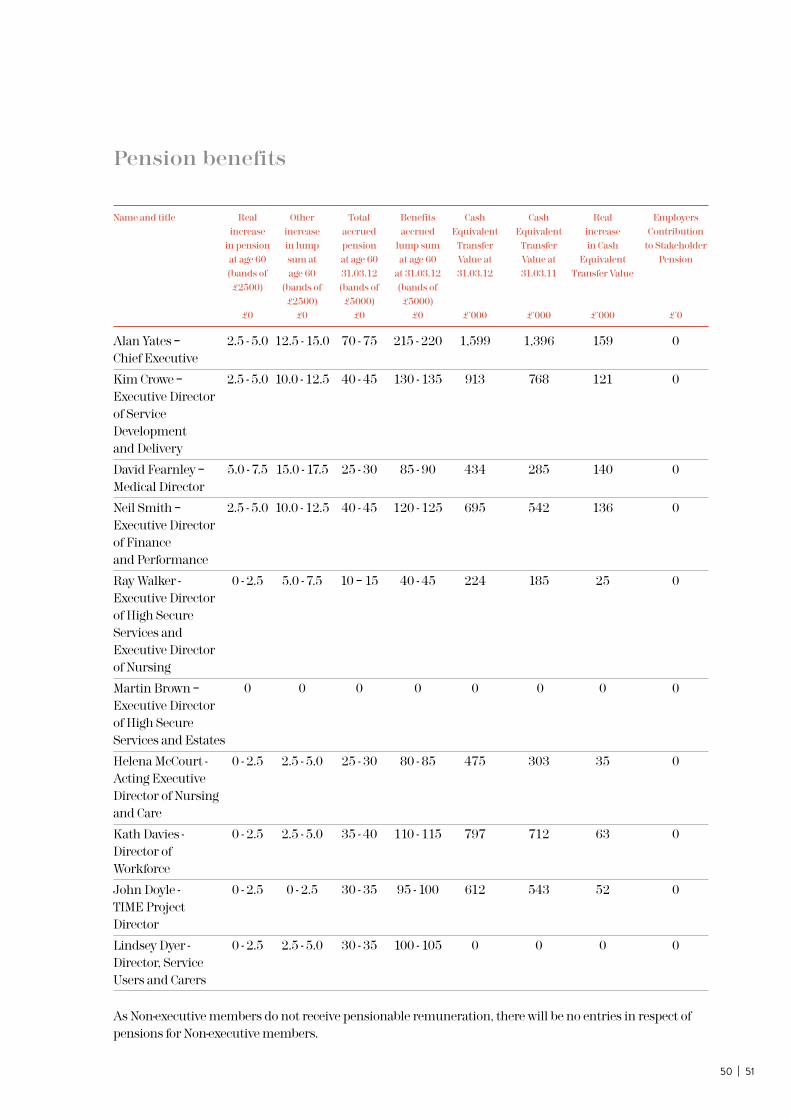
Pension benefits
Name and title Real Other Total Benefits Cash Cash Real Employers increase increase accrued accrued Equivalent Equivalent increase Contribution in pension in lump pension lump sum Transfer Transfer in Cash to Stakeholder at age 60 sum at at age 60 at age 60 Value at Value at Equivalent Pension (bands of age 60 31.03.12 at 31.03.12 31.03.12 31.03.11 Transfer Value £2500) (bands of (bands of (bands of £2500) £5000) £5000) £0 £0 £0 £0 £’000 £’000 £’000 £’0
Alan Yates – 2.5 - 5.0 12.5 - 15.0 70 - 75 215 - 220 1,599 1,396 159 0 Chief Executive
Kim Crowe – 2.5 - 5.0 10.0 - 12.5 40 - 45 130 - 135 913 768 121 0 Executive Director of Service Development and Delivery
David Fearnley – 5.0 - 7.5 15.0 - 17.5 25 - 30 85 - 90 434 285 140 0 Medical Director
Neil Smith – 2.5 - 5.0 10.0 - 12.5 40 - 45 120 - 125 695 542 136 0 Executive Director of Finance and Performance
Ray Walker - 0 - 2.5 5.0 - 7.5 10 – 15 40 - 45 224 185 25 0 Executive Director of High Secure Services and Executive Director of Nursing
Martin Brown – 0 0 0 0 0 0 0 0 Executive Director of High Secure Services and Estates
Helena McCourt - 0 - 2.5 2.5 - 5.0 25 - 30 80 - 85 475 303 35 0 Acting Executive Director of Nursing and Care
Kath Davies - 0 - 2.5 2.5 - 5.0 35 - 40 110 - 115 797 712 63 0 Director of Workforce
John Doyle - 0 - 2.5 0 - 2.5 30 - 35 95 - 100 612 543 52 0 TIME Project Director
Lindsey Dyer - 0 - 2.5 2.5 - 5.0 30 - 35 100 - 105 0 0 0 0 Director, Service Users and Carers
As Non-executive members do not receive pensionable remuneration, there will be no entries in respect of pensions for Non-executive members.
50 51

A Cash Equivalent Transfer Value (CETV) is the actuarially assessed capital value of the pension scheme benefits accrued by a member at a particular point in time. The benefits valued are the member’s accrued benefits and any contingent spouse’s pension payable from the scheme. A CETV is a payment made by a pension scheme or arrangement to secure pension benefits in another pension scheme or arrangement when the member leaves a scheme and chooses to transfer the benefits accrued in their former scheme. The pension figures shown relate to the benefits that the individual has accrued as a consequence of their total membership of the pension scheme, not just their service in a senior capacity to which disclosure applies. The CETV figures and the other pension details include the value of any pension benefits in another scheme or arrangement which the individual has transferred to the NHS pension scheme. They also include any additional pension benefit accrued to the member as a result of their purchasing additional years of pension service in the scheme at their own cost. CETVs are calculated within the guidelines and framework prescribed by the Institute and Faculty of Actuaries.
This reflects the increase in CETV effectively funded by the employer. It takes account of the increase in accrued pension due to inflation; contributions paid by the employee (including the value of any benefits transferred from another scheme or arrangement) and uses the most recent set of actuarial valuation factors produced by the Government Actuary’s Department (GAD).
Cash equivalent transfer values
Real increase in CETV
Approved by:
Chief Executive Date

50 | 5152 53
The Board is accountable for internal control. As Accountable Officer, and Chief Executive of this Board, I have responsibility for maintaining a sound system of internal control that supports the achievement of the organisation’s policies, aims and objectives. I also have responsibility for safeguarding the public funds and the organisation’s assets for which I am personally responsible as set out in the Accountable Officer Memorandum.
The Trust Board is ultimately accountable for the management of all risks in the organisation. The Chief Executive, supported by Board members, has responsibility for the implementation of the Risk Management Strategy. These responsibilities are met in a variety of ways.
The Chief Executive, with overall responsibility for risk within Mersey Care NHS Trust, ensures the work of the Integrated Governance Committee and other specialist sub-committees is reviewed by the Trust Board. The Chief Executive has overall responsibility for having effective risk management systems in place within the Trust, and for meeting all statutory requirements and adhering to guidance issued by the Department of Health in respect of risk and governance.
The Trust Board has overall responsibility for consideration of the Assurance Framework and resource allocation relating to the ‘significant risks’ of the Trust. The recommendations of the Integrated Governance Committee and relevant sub-committees are made to the Trust Board where competing priorities are debated and agreed or accepted.
The accountability arrangements for risk management in 2011-12 involved the following:
• The Medical Director had overall responsibility across the organisation for medicines management and as the Accountable Officer (Controlled Drugs) for the Trust, research and development, information governance and was the identified Caldicott Guardian. In addition to these key functions the Medical Director was accountable for Safeguarding Children and Adults and the regulation requirements relating to registration with the Care Quality Commission as the Nominated Individual. The Medical Director is also the Responsible Officer for medical revalidation.
AnnualGovernanceStatementScope of responsibility

• The Executive Director of Service Development and Delivery had delegated specific responsibilities for the day to day operational management of key risk areas and for ensuring that the Trust had sound and effective systems for the management of patient safety, complaints, claims and adverse incidents.
• The Executive Director of Nursing and High Secure Services as Director for the Prevention and Control of Infection (DIPC) was accountable for the management and prevention of health care associated infection.
• The Executive Director of Finance and Performance was responsible for ensuring that the Trust had sound financial governance arrangements that were controlled and monitored through robust audit and accounting mechanisms and in addition, the Senior Information Risk Officer (SIRO).
The development of effective and appropriate risk management processes within Mersey Care has been monitored by the Trust Board and through the various performance review processes of the NHS. The Assurance Framework, Corporate Risk Register, Clinical Business Unit (CBU) risk registers and Risk Management Strategy have collectively been presented and approved by various review processes, which include health economy partner organisations. The Trust’s strategic direction, policies, procedures and supporting documentation are openly accessible via the Mersey Care website to internal and external stakeholders for comment, scrutiny and reference.
The Trust contracts for local mental health, learning disability and addiction services with its main commissioners NHS Merseyside which covers Liverpool, Sefton, Knowsley and Halton and St Helens. NHS Wirral and NHS Central Lancashire are Associates to this contract. The Trust contracts with North West Secure Commissioners in respect of high, medium and low secure services. Formal contract monitoring meetings and strategic commissioning meetings are established between the Commissioners and the Trust, where risks relating to the contract and/or performance/delivery of services are addressed.
The SHA and PCTs are notified of and monitor all serious incidents related to circumstances involving service users of Trust services. The Trust is an active member of the Merseyside NHS Health and Social Care Group responsible for directing emergency planning/business continuity arrangements across Merseyside on behalf of the Local Resilience Forum.
The Trust has a fully functioning Infection Control Committee chaired by a Consultant Microbiologist from Aintree Hospitals NHS Foundation Trust who is employed on a sessional basis to undertake the role of Infection Control Doctor.
The Trust attends the Overview and Scrutiny Committees (OSC) operating in Liverpool, Sefton and Knowsley where issues relating to service change, service development and matters of interest/concern to the OSCs are discussed and/or information provided.

54 55
The Chief Executive of the NHS has designated that the Chief Executive should be the Accountable Officer to the Trust. The relevant responsibilities of accountable officers are set out in the Accountable Officers Memorandum issued by the Department of Health. These include ensuring that: • there are effective management systems in place to safeguard public funds and assets and
assist in the implementation of corporate governance • value for money is achieved from the resources available to the Trust • the expenditure and income of the Trust has been applied to the purposes intended by
Parliament and conform to the authorities who govern them • effective and sound financial management systems are in place; and annual
statutory accounts are prepared in a format directed by the Secretary of State with the approval of the Treasury to give a true and fair view of the state of affairs as at the end of the financial year and the income and expenditure, recognised gains and losses and cash flows for the year.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in my letter of appointment as an Accountable Officer.
Review of the effectiveness of risk management and internal control
As Accountable Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review is informed in a number of ways. The Head of Internal Audit provides me with an opinion on the overall arrangements for gaining assurance through the Assurance Framework and on the controls reviewed as part of Internal Audit’s work. The overall opinion for 2011-12 is that there is significant assurance. Executive managers within the organisation who have responsibility for the development and maintenance of the system of internal control provide me with assurance. The Assurance Framework itself provides me with evidence that the effectiveness of controls that manage the risks to the organisation achieving its principal objectives have been reviewed.
I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Board, Integrated Governance Committee and Audit Committee.
Significant Issues
There are no significant issues to report.
Accountable Officer: Alan Yates
Signature
Date
Statement of the chief executive’s responsibilities as the accountable officer of the Trust

Performance and activity
Ethnicity Number of % of total service users service users
African 54 0.3%
Arab 39 0.2%
Asian other 53 0.3%
Bangladeshi 11 0.1%
Black British 201 1.3%
Black other 41 0.3%
Caribbean 29 0.2%
Chinese 63 0.4%
Indian 25 0.2%
Mixed other 71 0.4%
Other ethnicity 71 0.4%
Pakistani 17 0.1%
Somali 26 0.2%
Turkish/Cypriot 6 0.0%
White British 14,746 92.7%
White European 120 0.8%
White Irish 143 0.9%
White other 71 0.4%
White Welsh 3 0.0%
White/Asian 18 0.1%
White/Black/African 45 0.3%
White/Black/Caribbean 46 0.3%
Total service users with known ethnicity 15,899
As at 31st March 2012, 16,847 service users were being provided with a service by Mersey Care, of which ethnicity was known for 15,899. 92.7% of service users with known ethnicity were White British (92.4% as at 31st March 2011). 93.1% of the population served by the Trust are White British. Source: ePEX and PACIS.
Number of service users
Patient chose 107 not to answer
Not known 841
Total service users with unknown ethnicity 948
Ethnic breakdown of service users as at 31st March 2012

There has been a small increase in admissions in 2011-12 with an average of 291 admissions across the Trust per month compared with 289 admissions per month in 2010-11. Source: ePEX and PACIS.
Mental health trusts are required to demonstrate that service users are assessed (gatekept) prior to admission by Crisis Resolution Home Treatment teams to avoid unnecessary admissions to inpatient units. During 2011-12, 99.8% of service users admitted to acute inpatient wards were gatekept by CRHT, compared to 98.9% in 2010-11. The chart shows the percentage of admitted service users gatekept against the national target each month. Source: ePEX.
Admissions to Mersey Careinpatient units in month April 2011 to March 2012
Ap
r 1
1
Nu
mb
er o
f ad
mis
sion
s
May
11
Jun
11
Jul
11
Au
g 1
1
Sep
11
Oct
11
Nov
11
Dec
11
Jan
12
Feb
12
Mar
12
Total admissions
220_
240_
260_
280_
300_
320_
Percentage of admissions gatekept by Crisis Resolution Home Treatment April 2011 to March 2012 (in month)
Ap
r 1
1
% G
atek
ept
May
11
Jun
11
Jul
11
Au
g 1
1
Sep
11
Oct
11
Nov
11
Dec
11
Jan
12
Feb
12
Mar
12
% admissions gatekept by CHRT (in month)
National Target (95%)
90%_
91%_
92%_
93%_
94%_
95%_
96%_
97%_
98%_
99%_
100%_
56 57

Mental health trusts are required to demonstrate that service users discharged on a Care Programme Approach are followed up within 7 days of discharge. 98.9% of service users discharged on a CPA in 2011-12 were followed up within 7 days, compared to 98.2% in 2010-11. The chart shows the percentage of service users followed up within 7 days of discharge against the national target each month. Source: ePEX.
Over the last few years, the Trust has successfully reduced the number of patients whose discharge from an inpatient bed has been delayed. In 2011-12 an average of 17 delayed discharges were reported at the end of each month, compared with 17 during 2010-11. The average proportion of beds occupied by delayed discharges (excluding those attributable to social care only) was 2.04% in 2011-12 compared with 4.4% in 2010-11. Source: ePEX.
CPA 7 day follow up April 2011 to March 2012 (in month)
Ap
r 1
1
% 7
Day
Fol
low
Up
May
11
Jun
11
Jul
11
Au
g 1
1
Sep
11
Oct
11
Nov
11
Dec
11
Jan
12
Feb
12
Mar
12
% followed up within 7 days (in months)
National Target (95%)
90%_
91%_
92%_
93%_
94%_
95%_
96%_
97%_
98%_
99%_
100%_
Delayed discharges 2008-09 to 2011-12
20
08
-09
20
09
-10
201
0-1
1
201
1-1
2
Average number of patients delayed
0_
10_
20_
30_
40_
50_
60_

The Trust has made significant gains in terms of improving productivity over the last few years. The graph demonstrates the year on year reductions in the proportion of outpatient appointments cancelled by the Trust and not attended by service users. Source: ePEX.
2011-12 Specialist team activity
New Cases Early Intervention in Psychosis
CRHTEpisodes
Assertive Outreach Caseload
2011-12 Performance Target 100%
0%_
20%_
40%_
60%_
80%_
100%_
120%_
140%_
The Early Intervention in Psychosis service works with people aged 16-35 who are experiencing their first episode of psychosis or who are showing signs or symptoms of developing an episode of psychosis. The service has successfully worked to increase the number of people it reaches, and was able to exceed the Department of Health’s target for the number of new service users seen during 2011-12, providing a service to 179 new patients.
The Crisis Resolution Home Treatment service works with people experiencing a crisis in order to avoid admission to hospital as appropriate. The service co-ordinates admissions to inpatient beds and facilitates early discharge from hospital. The service has successfully worked to increase the number of people it reaches, and was able to exceed the Department of Health’s target for the number of episodes of care managed by the Trust during 2011-12 to deliver 2,636 episodes.
The Assertive Outreach service works with people who find it difficult to engage with traditional mental health services. The service has successfully worked to increase the number of people it reaches, and was able to exceed the Department of Health’s target for the number of service users seen during 2011-12. As at the end of March 2012, the Trust was providing an Assertive Outreach service to 442 patients. Source: ePEX.
Cancellations and DNAs
2008 -9 2009 -10 2010 -11 2011-12
0%_
2%_
4%_
6%_
8%_
10%_
12%_
14%_
16%_
18%_
Outpatients cancellations by provider
Outpatients DNAs
58 59

The Trust has made significant gains in terms of improving waiting times for outpatients over the last few years. The graph demonstrates the year on year reductions in the number of patients waiting 6 weeks or more for their first outpatient appointment. Source: ePEX.
The cumulative sickness rate in 2011-12 was 6.23% compared with 6.17% in 2010 -11. Source: ESR.
2009-10 20010-11 20011-12
0%_
10%_
20%_
30%_
40%_
50%_
60%_
70%_
80%_
Staff sickness rates
5.8%_
5.9%_
6.0%_
6.1%_
6.2%_
6.3%_
6.4%_
6.5%_
6.6%_
6.7%_
6.8%_
2007-08 2008-09 2009-10 2010-11 2011-12
Staff Sickness Rates
Cumulative numbers of patients waiting 6 weeks or more for first outpatient appointment

Local Services and SaFE Partnerships Data 2011-12
Number of Consultant Outpatient and Face to Face Consultant Community Contacts
Positive Addiction Care SaFESpecialty Services Liverpool Partnerships Rebuild Partnerships Total
Alcohol 322 0 0 0 0 322
Drugs 1,542 0 0 0 0 1,542
Forensic 0 0 0 0 713 713
Learning Disability 0 0 142 1,778 0 1,920
Mental Illness Acute 0 9,103 13,270 0 0 22,373
Older Persons 0 4,926 8,241 0 0 13,167
Psychological 0 0 0 0 0 0
Psychotherapy 0 880 0 0 0 880
Specialist Services 0 0 0 773 0 773
Total 1,864 14,909 21,653 2,551 713 41,690
There were 41,690 consultant outpatient attendances and face to face consultant community contacts in 2011-12, compared with 42,623 in 2010-11. Source: ePEX.
Total number of patients provided with a service by local services and SaFE Partnerships in 2011-12 31,246
Number of Face to Face Community Contacts not carried out by a Consultant
Positive Addiction Care SaFESpecialty Services Liverpool Partnerships Rebuild Partnerships Total
Alcohol 5,083 0 0 0 0 5,083
Drugs 129,191 0 0 0 0 129,191
Forensic 0 0 0 0 20,570 20,570
Learning Disability 0 0 20 22,450 0 22,470
Mental Illness Acute 0 92,672 100,066 0 0 192,738
Older Persons 0 34,434 47,687 0 0 82,121
Psychological 0 0 0 0 0 0
Psychotherapy 0 4,210 0 0 0 4,210
Specialist Services 0 0 5,446 0 5,446
Total 134,274 131,316 147,773 27,896 20,570 461,829
There were 461,829 face to face community contacts not carried out by a Consultant in 2011-12, compared with 345,746 in 2010-11. Source: ePEX.
60 61

High Secure Data 2011-12
Patient Population by Service as at 31st March 2012
Service Category No. Patients % of Population
Admission and Mental Health 41 20.1% High Dependency Personality Disorder 37 18.1%
Specialist Services Mental Health 93 45.6% Personality Disorder 33 16.2%
Total 204 100.00%
The High Secure service operates with wards of a maximum of 20 patients. The wards are split into two service types: admission and high dependency and specialist services to cater for specific patient needs. The table indicates the patient population as at 31st March 2012 was 204, compared to 212 as at 31st March 2011. In addition to the 204 inpatient population, there were 15 patients on leave as at 31st March 2012 (compared to 18 patients on leave as at 31st March 2011). Source: PACIS.
Source of Patient Admission
Admission Source No. Patients % of Admissions
Prison 21 70.0%
High Secure Hospital 1 3.3%
Medium Secure Unit 7 23.3%
Hospital 0 0.0%
Low Secure Unit 1 3.3%
Total 30 100.00%
This table shows the number of patients admitted to High Secure services in 2011-12, and where they were admitted from. 30 patients were admitted in 2011-2012, compared with 38 in 2010-11. Source: PACIS.
Outcome of Referrals
Outcome No. Patients % of Referrals
Rejected 21 42.9%
Accepted 25 51.0%
Open 3 6.1%
Referred 49 100.00%
Of the 49 patients referred for admission to the service in 2011-12, 25 were accepted (51.02%). This is a decrease in the proportion accepted from 55.2% in 2010 -11. Source: PACIS.

Patients Transferred/Discharged by Place
Destination No. Patients % of Discharges
Medium Secure Unit 29 70.7%
Prison 8 19.5%
Court 0 0.0%
Hospital 0 0.0%
Deceased 4 9.8%
Total 41 100.00%
During 2011-12, 41 patients were discharged from High Secure services, which is an increase from 32 in 2010 -11. The table shows where these patients were discharged/transferred to. The majority of High Secure patients discharged during 2011-12 went to a Medium Secure Unit (70.7%). Source: PACIS.
Regional Split of Patients
Region No. Patients % of Population
London 4 1.7%
Northern 2 0.8%
North Cumbria 3 1.2%
North West 119 49.2%
Trent 0 0.0%
Wales 47 19.4%
West Midlands 66 27.3%
Yorkshire 1 0.4%
Total 242 100.00%
The table shows the number of patients accessing High Secure services in 2011-12. From the information it can be seen that the majority of patients came from the North West, West Midlands and Wales. (95.9% of patients in total). Source: PACIS.
Total number of patients provided with a service by High Secure services in 2011-12 242
62 63

Independent Auditor’s Report to the Directors of Mersey Care NHS TrustI have audited the financial statements of Mersey Care NHS Trust for the year ended 31st March 2012 under the Audit Commission Act 1998. The financial statements comprise the Statement of Comprehensive Income, the Statement of Financial Position, the Statement of Changes in Taxpayers’ Equity, the Statement of Cash Flows and the related notes. The financial reporting framework that has been applied in their preparation is applicable law and the accounting policies directed by the Secretary of State with the consent of the Treasury as relevant to the National Health Service in England.
I have also audited the information in the Remuneration Report that is subject to audit, being:
• the table of salaries and allowances of senior managers and related narrative notes
• the table of pension benefits of senior managers and related narrative notes
• the table of pay multiples and related narrative notes.
This report is made solely to the Board of Directors of Mersey Care NHS Trust in accordance with Part II of the Audit Commission Act 1998 and for no other purpose, as set out in paragraph 45 of the Statement of Responsibilities of Auditors and Audited Bodies published by the Audit Commission in March 2010.

As explained more fully in the Statement of Directors’ Responsibilities, the Directors are responsible for the preparation of the financial statements and for being satisfied that they give a true and fair view. My responsibility is to audit and express an opinion on the financial statements in accordance with applicable law and International Standards on Auditing (UK and Ireland). Those standards require me to comply with the Auditing Practices Board’s Ethical Standards for Auditors.
An audit involves obtaining evidence about the amounts and disclosures in the financial statements sufficient to give reasonable assurance that the financial statements are free from material misstatement, whether caused by fraud or error. This includes an assessment of: whether the accounting policies are appropriate to the Trust’s circumstances and have been consistently applied and adequately disclosed; the reasonableness of significant accounting estimates made by the Trust; and the overall presentation of the financial statements. In addition, I read all the financial and non-financial information in the annual report to identify material inconsistencies with the audited financial statements. If I become aware of any apparent material misstatements or inconsistencies I consider the implications for my report.
In my opinion the financial statements:
• give a true and fair view of the financial position of Mersey Care NHS Trust as at 31st March 2012 and of its expenditure and income for the year then ended; and
• have been prepared properly in accordance with the accounting policies directed by the Secretary of State with the consent of the Treasury as relevant to the National Health Service in England.
Julian Farmer, Officer of the Audit Commission
Audit Commission,2nd Floor Aspinall House,Aspinall Close,Middlebrook, Horwich, Bolton,BL6 6QQ
31st May 2012
Scope of the audit of the financial statements
Opinion on financial statements
64 65
Respective responsibilities of directors and auditor

I’m Sandy. I’m Mersey Care.

I suppose I’m a bit of a paradox in that I’m a serious mathematician
I worked as a teacher for a while but I’ve done all sorts of things since including bar work, I’ve been a semi-professional singer, I’ve coached people to do public speaking as a former speakers’ club president and master of ceremonies, and most recently I was a paid carer.
66 67
and can spend hours working on complicated formulas and problems just for the fun of it, but I’m also a very social animal who loves pub quizzes, parties and singing karaoke in clubs and pubs.
I did a computer science degree and then worked in London as a computer systems designer before returning to Liverpool in 1991.
It took a long time to decide if it was right for me – and knowing you are ready to do it is different than wanting to do it. I was referred to Mersey Care’s Hesketh Centre in Southport and then onto the gender identity service in Leeds.
Before you start you fill in their massive questionnaire and they assess you to see if you are of sound mind. Living as a man was driving me mad and I knew that changing my
I would love to work with people with autism, including Asperger’s syndrome. I’ve done some work with autistic children in Manchester and autistic adults in Southport. I’ve found that no matter what situation I’m in I’ve got the patience to listen, try to understand and then respond to them, no matter how long it takes.
I love singing and can sing in the style of lots of artists. I used to do a Dido tribute act, but I do all sorts of material really, acts like Joan Armatrading, Boz Scaggs, Mott the Hoople, you name it! I’ve appeared in clubs and the Manchester Fringe Festival but it’s mainly for fun at pub karaoke nights now.
In 2008 I moved to Southport. It was around this time that I decided to take the remaining steps towards my sex change. To give it its proper description I’m a male to female pre-operative transsexual. Oh and the irony of my surname (Manley) doesn’t escape me!
lifestyle was not a choice, I just had to do it; there was no other way to be.
Making the final changes to your body is about feeling and showing all aspects of being female; it is at least as much about a mental mindset as it is about the (still very important) physical aspects. To be honest 90 out of 100 people you see in public don’t notice, the other nine don’t care, and one will meet you half-way with a polite question.
I like to think I am living my life the same as everybody else, and I’m reassured that Mersey Care will listen to the things that I and others have to say. I’ve joined one of its equality groups, which meets once a month.
I’m now 52 and this is what makes me, me. That’s why… I’m Sandy and I’m Mersey Care.

I’m Mark. I’m Mersey Care.
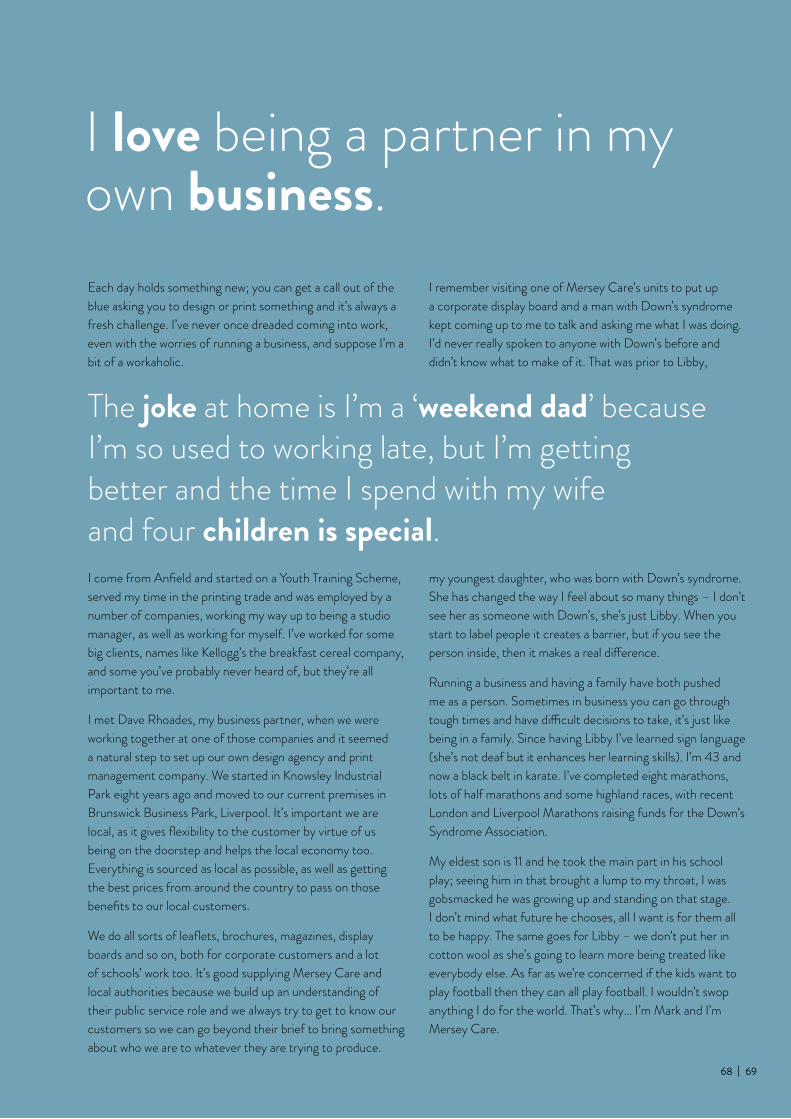
I love being a partner in my own business.
The joke at home is I’m a ‘weekend dad’ because I’m so used to working late, but I’m getting better and the time I spend with my wife and four children is special.
my youngest daughter, who was born with Down’s syndrome. She has changed the way I feel about so many things – I don’t see her as someone with Down’s, she’s just Libby. When you start to label people it creates a barrier, but if you see the person inside, then it makes a real difference.
Running a business and having a family have both pushed me as a person. Sometimes in business you can go through tough times and have difficult decisions to take, it’s just like being in a family. Since having Libby I’ve learned sign language (she’s not deaf but it enhances her learning skills). I’m 43 and now a black belt in karate. I’ve completed eight marathons, lots of half marathons and some highland races, with recent London and Liverpool Marathons raising funds for the Down’s Syndrome Association.
My eldest son is 11 and he took the main part in his school play; seeing him in that brought a lump to my throat, I was gobsmacked he was growing up and standing on that stage. I don’t mind what future he chooses, all I want is for them all to be happy. The same goes for Libby – we don’t put her in cotton wool as she’s going to learn more being treated like everybody else. As far as we’re concerned if the kids want to play football then they can all play football. I wouldn’t swop anything I do for the world. That’s why… I’m Mark and I’m Mersey Care.
Each day holds something new; you can get a call out of the blue asking you to design or print something and it’s always a fresh challenge. I’ve never once dreaded coming into work, even with the worries of running a business, and suppose I’m a bit of a workaholic.
I come from Anfield and started on a Youth Training Scheme, served my time in the printing trade and was employed by a number of companies, working my way up to being a studio manager, as well as working for myself. I’ve worked for some big clients, names like Kellogg’s the breakfast cereal company, and some you’ve probably never heard of, but they’re all important to me.
I met Dave Rhoades, my business partner, when we were working together at one of those companies and it seemed a natural step to set up our own design agency and print management company. We started in Knowsley Industrial Park eight years ago and moved to our current premises in Brunswick Business Park, Liverpool. It’s important we are local, as it gives flexibility to the customer by virtue of us being on the doorstep and helps the local economy too. Everything is sourced as local as possible, as well as getting the best prices from around the country to pass on those benefits to our local customers.
We do all sorts of leaflets, brochures, magazines, display boards and so on, both for corporate customers and a lot of schools’ work too. It’s good supplying Mersey Care and local authorities because we build up an understanding of their public service role and we always try to get to know our customers so we can go beyond their brief to bring something about who we are to whatever they are trying to produce.
I remember visiting one of Mersey Care’s units to put up a corporate display board and a man with Down’s syndrome kept coming up to me to talk and asking me what I was doing. I’d never really spoken to anyone with Down’s before and didn’t know what to make of it. That was prior to Libby,
68 69

I’m Anna. I’m Mersey Care.
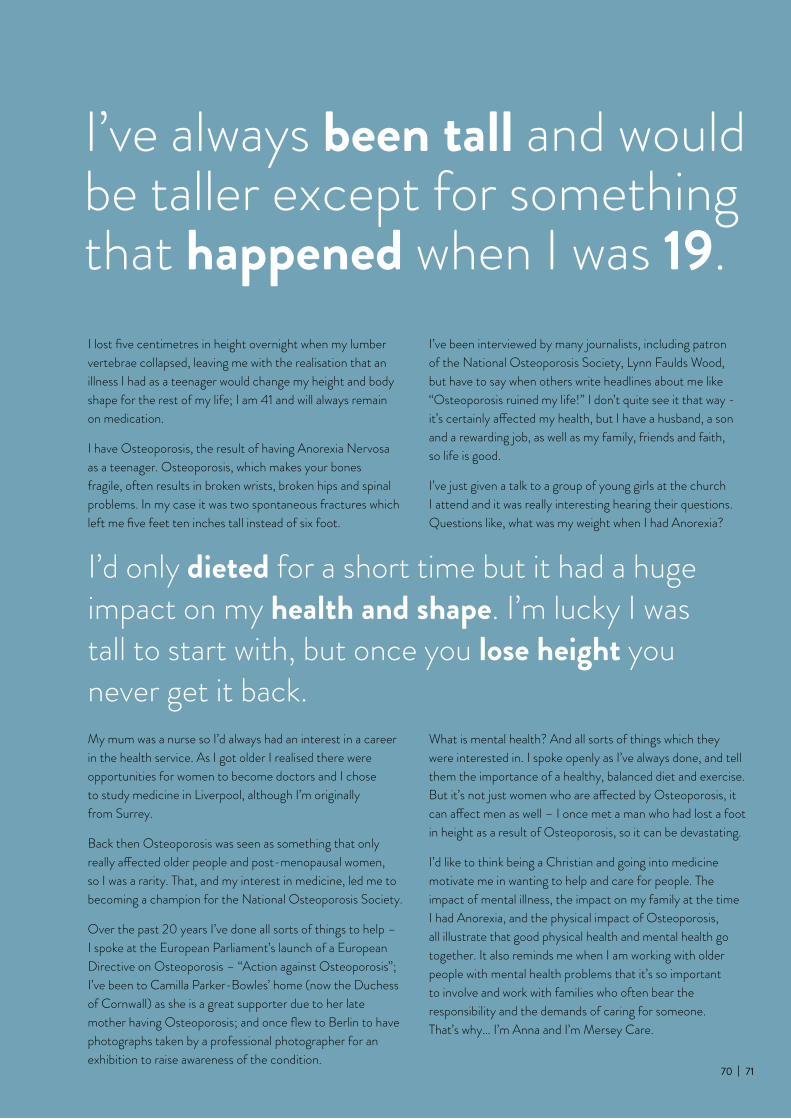
I’ve always been tall and would be taller except for something that happened when I was 19.
I’d only dieted for a short time but it had a huge impact on my health and shape. I’m lucky I was tall to start with, but once you lose height you never get it back.
What is mental health? And all sorts of things which they were interested in. I spoke openly as I’ve always done, and tell them the importance of a healthy, balanced diet and exercise. But it’s not just women who are affected by Osteoporosis, it can affect men as well – I once met a man who had lost a foot in height as a result of Osteoporosis, so it can be devastating.
I’d like to think being a Christian and going into medicine motivate me in wanting to help and care for people. The impact of mental illness, the impact on my family at the time I had Anorexia, and the physical impact of Osteoporosis, all illustrate that good physical health and mental health go together. It also reminds me when I am working with older people with mental health problems that it’s so important to involve and work with families who often bear the responsibility and the demands of caring for someone. That’s why… I’m Anna and I’m Mersey Care.
I lost five centimetres in height overnight when my lumber vertebrae collapsed, leaving me with the realisation that an illness I had as a teenager would change my height and body shape for the rest of my life; I am 41 and will always remain on medication.
I have Osteoporosis, the result of having Anorexia Nervosa as a teenager. Osteoporosis, which makes your bones fragile, often results in broken wrists, broken hips and spinal problems. In my case it was two spontaneous fractures which left me five feet ten inches tall instead of six foot.
My mum was a nurse so I’d always had an interest in a career in the health service. As I got older I realised there were opportunities for women to become doctors and I chose to study medicine in Liverpool, although I’m originally from Surrey.
Back then Osteoporosis was seen as something that only really affected older people and post-menopausal women, so I was a rarity. That, and my interest in medicine, led me to becoming a champion for the National Osteoporosis Society.
Over the past 20 years I’ve done all sorts of things to help – I spoke at the European Parliament’s launch of a European Directive on Osteoporosis – “Action against Osteoporosis”; I’ve been to Camilla Parker-Bowles’ home (now the Duchess of Cornwall) as she is a great supporter due to her late mother having Osteoporosis; and once flew to Berlin to have photographs taken by a professional photographer for an exhibition to raise awareness of the condition.
I’ve been interviewed by many journalists, including patron of the National Osteoporosis Society, Lynn Faulds Wood, but have to say when others write headlines about me like “Osteoporosis ruined my life!” I don’t quite see it that way - it’s certainly affected my health, but I have a husband, a son and a rewarding job, as well as my family, friends and faith, so life is good.
I’ve just given a talk to a group of young girls at the church I attend and it was really interesting hearing their questions. Questions like, what was my weight when I had Anorexia?
70 71
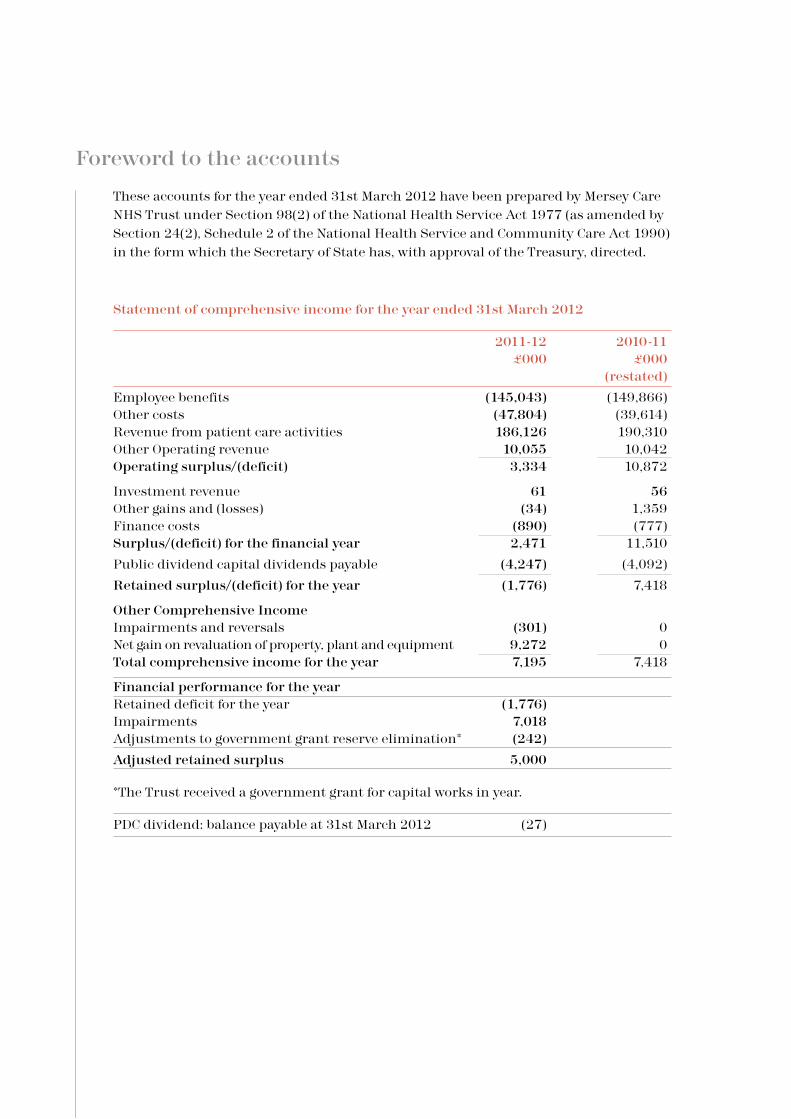
These accounts for the year ended 31st March 2012 have been prepared by Mersey Care NHS Trust under Section 98(2) of the National Health Service Act 1977 (as amended by Section 24(2), Schedule 2 of the National Health Service and Community Care Act 1990) in the form which the Secretary of State has, with approval of the Treasury, directed.
Statement of comprehensive income for the year ended 31st March 2012
2011-12 2010-11 £000 £000 (restated)
Employee benefits (145,043) (149,866)Other costs (47,804) (39,614)Revenue from patient care activities 186,126 190,310Other Operating revenue 10,055 10,042Operating surplus/(deficit) 3,334 10,872
Investment revenue 61 56Other gains and (losses) (34) 1,359Finance costs (890) (777)Surplus/(deficit) for the financial year 2,471 11,510
Public dividend capital dividends payable (4,247) (4,092)
Retained surplus/(deficit) for the year (1,776) 7,418
Other Comprehensive IncomeImpairments and reversals (301) 0Net gain on revaluation of property, plant and equipment 9,272 0Total comprehensive income for the year 7,195 7,418
Financial performance for the year Retained deficit for the year (1,776) Impairments 7,018 Adjustments to government grant reserve elimination* (242)
Adjusted retained surplus 5,000
*The Trust received a government grant for capital works in year.
PDC dividend: balance payable at 31st March 2012 (27)
Foreword to the accounts

Statement of financial position as at 31st March 2012
31st March 2012 31st March 2011 31st March 2010 (restated) (restated) £000 £000 £000Non-current assets Property, plant and equipment 149,589 146,141 141,457Intangible assets 188 400 604
Total non-current assets 149,777 146,541 142,061Current assetsInventories 467 518 434Trade and other receivables 5,202 3,521 3,600Cash and cash equivalents 13,510 9,218 6,797
Total current assets 19,179 13,257 10,831Non-current assets held for sale 0 0 0
Total current assets 19,179 13,257 10,831
Total assets 168,956 159,798 152,892
Current liabilities Trade and other payables (8,458) (7,361) (9,392)Other liabilities 0 0 0Provisions (1,715) (1,394) (1,328)Borrowings (84) (67) (426)Total current liabilities (10,257) (8,822) (11,146)
Non-current assets plus/less net 158,699 150,976 141,746 current assets/liabilities
Non-current liabilities Provisions (17,389) (16,782) (16,220)Borrowings (5,056) (5,141) (4,829)Total non-current liabilities (22,445) (21,923) (21,049)
Total Assets Employed 136,254 129,053 120,697
Financed by: taxpayers’ equity Public Dividend Capital 58,099 58,099 57,161Retained earnings (31,019) (33,172) (41,738)Revaluation reserve 49,267 44,219 45,367Other reserves 59,907 59,907 59,907
Total Taxpayers’ Equity 136,254 129,053 120,697
72 73
Approved by:
Chief Executive Date

Statement of change in taxpayers’ equity for the year ended in 31st March 2012
Public Retained Revaluation Other Total Dividend earnings reserve reserves reserves capital
£000 £000 £000 £000 £000
Balance at 1st April 2011 58,099 (33,172) 44,219 59,907 129,053
Restated balance at 1st April 2011 58,099 (33,172) 44,219 59,907 129,053
Changes in taxpayers’ equity for 2011-12 Retained surplus/(deficit) for the year (1,776) (1,776)Net gain on revaluation of property, plant, equipment 9,272 9,272Impairments and reversals (301) (301)Transfers between reserves 3,923 (3,923) 0 0Transfers to/(from) other bodies within the Resource Account boundary 0 6 0 0 6Net recognised revenue/(expense) for the year 0 2,153 5,048 0 7,201
Balance at 31st March 2012 58,099 (31,019) 49,267 59,907 136,254
Included above: Transfer from revaluation reserve to retained earnings in respect 2,744 (2,744) 0of impairments

Statement of cash flows for the year ended 31st March 2012
2011-12 2010-11 £000 £000
Cash Flows from Operating Activities
Operating Surplus/Deficit 3,334 10,872
Depreciation and Amortisation 6,142 5,882
Impairments and Reversals 7,018 0
Interest paid (442) (438)
Dividend paid (4,244) (4,075)
(Increase)/Decrease in inventories 51 (84)
(Increase)/Decrease in trade and other receivables (1,681) 79
Increase/(Decrease) in trade and other payables 1,468 (1,803)
Provisions utilised (1,563) (1,540)
Increase in provisions 2,043 3,188
Net cash inflow from operating activities 12,126 12,081
Cash flows from investing activities
Interest received 61 56
(Payments) for property, plant and equipment (8,067) (11,338)
(Payments) for Intangible assets (3) (10)
Proceeds of disposal of assets held for sale (PPE) 0 742
Net cash outflow from investing activities (8,009) (10,550)
Net cash inflow before financing 4,117 1,531
Cash flow from financing activities
Public Dividend Capital received 0 1,680
Public Dividend Capital repaid 0 (742)
Capital element of payments in respect of finance
leases and On-SoFP, PFI and LIFT (67) (48)
Capital grants and other capital receipts 242 0
Net cash inflow from financing activities 175 890
Net increase in cash and cash equivalents 4,292 2,421
Cash and cash equivalents at beginning of the period 9,218 6,797
Restated cash and cash equivalents at beginning of
the period 9,218 6,797
Cash equivalents at year end 13,510 9,218
74 75

Better Payment Practice Code
Measure of compliance 2011-12 2011-12 2010 -11 2010-11 Number £000 Number £000
Non-NHS payables Total non-NHS trade invoices paid in the year 37,324 114,578 40,455 129,649Total non-NHS trade invoices paid within target 36,653 114,156 39,911 128,973
percentage of NHS trade invoices paid within target 98.20% 99.63% 98.66% 99.48%
NHS payables Total NHS trade invoices paid in the year 791 20,921 832 12,598Total NHS trade invoices paid within target 766 20,895 815 12,578
percentage of NHS trade invoices paid within target 96.84% 99.88% 97.96% 99.84%
The Better Payment Practice Code requires the Trust to aim to pay all valid invoices by the due date or within 30 days of receipt of a valid invoice, whichever is later.

76 77
We are Mersey Care.
I’m Brian Lawlor, non-executive director of the Board which oversees the strategic direction and statutory obligations of the Trust
I’m Justine Sheils, an administrator from Ashworth Hospital
I’m Mike Jones, financial accountant within specialist management services at Mersey Care NHS Trust
I’m Melissa Jackson, registered mental nurse on an inpatient ward at Mersey Care
I’m Sandy Manley, a public member of the Trust from the Sefton constituency
I’m Barry Vaz, service user and volunteer supporting the work of the Trust
I’m Dave Leigh, mental health advocate working for Together an independent sector organisation supporting patients in low, medium and high secure care.
I’m Mark Edwardson, of Mustang Creative, one of many local businesses supplying the Trust
I’m Anna Richman, consultant psychiatrist working with older people at Mossley Hill Hospital

www.merseycare.nhs.uk