major incident plan (mip) - basics south west · major incident plan (mip) version: 7.8 status:...
TRANSCRIPT

Major Incident Plan (MIP)
Version: 7.8
Status: UPDATE FOR APPROVAL
Title of originator/author: Wayne Darch, Emergency Preparedness Manager
Name of responsible director: Neil Le Chevalier, Director of Operations
Protective Marking OFFICIAL
Approved by group/committee and Date:
Trust Board
Effective date of issue: (1 month after approval date)
1st March 2017
Next annual review date: 1st March 2018
Date Equality Impact Assessment Completed
November 2013
Regulatory Requirement: Health and Social Care Act 2012 / Civil Contingences Act 2004
NHS England EPRR Core Standards Requirement

IF A MAJOR INCIDENT HAS BEEN
DECLARED
TURN IMMEDIATELY TO YOUR ACTION CARDS
DOCUMENT NAVIGATION
This document utilises colour coded pages for ease of navigation
The sections relating to response arrangements have been aligned to the ‘9 Key tasks’ in order to provide a sequential framework which is familiar to commanders.
Electronic links are provided throughout the document and can be utilised with a ‘left mouse click’.
1
SECTION CONTENT PAGE
1 CONTENTS 1
2 GOVERNANCE 3
3 ROLE AND PURPOSE OF THE MAJOR
INCIDENT PLAN 4
4 DEFINITIONS 7
5 ROLES AND RESPONSIBILITIES 9
6 ACTIVATION, ESCALATION &
MOBILISATION, 10
7 ARRIVAL AT SCENE 19
8 SCENE ASSESSMENT 20
9 COMMAND, CONTROL & CO-ORDINATION
22
10 SCENE MANAGEMENT 37
11 TRIAGE AND TREATMENT 41
12 TRANSPORT AND PATIENT MOVEMENT 54
13 SURVIVOR MANAGEMENT 56
14 COMMUNICATIONS AND MEDIA 57
15 POST INCIDENT PROCEDURES 59
ANNEX A ACTION CARDS
ANNEX B LINKED PLANS AND SOPS
ANNEX C HOSPITAL BED STATE FORM
ANNEX D C.R.I.P. TEMPLATE
ANNEX E TRUST GOLD STRATEGY
ANNEX F REFERENCES
ANNEX G VEHICLES AND EQUIPMENT
CC COO O
NN NTT T
EE ENN N
TT TSS S

2
FOREWARD BY THE CHIEF EXECUTIVE
Under the NHS constitution, the NHS is there to help the public when they need it most; this is especially true during a significant or major incident. The Major Incident Plan (MIP) describes the response of South Western Ambulance Service NHS Foundation Trust at the time of a major emergency. It has been prepared as part of meeting our reasonability’s under the Civil Contingencies Act, 2004 (CCA) and the Health and Social Care Act 2012. As Chief Executive, I accept executive responsibility for Emergency Preparedness, Resilience and Response (EPRR) arrangements and this MIP has been adopted and approved by the Trust Board. The arrangements in this plan form the basis of the Trust’s generic response to a major incident. However, the Trust’s operational area contains a wide range of hazards each having potential to become ‘major incidents’. The information contained in this MIP offers guidance and direction, but every incident will also require ambulance staff to display flexibility, professionalism and initiative. All staff should familiarise themselves with the contents of this plan, not only as preparation for their response to an incident, but to feed back useful information and suggested improvements. The MIP is supported by individual Action Cards and specific, linked contingency plans. Ambulance staff will be trained and exercised in the IRP to ensure an effective response. Debriefing of, and feedback from ambulance staff will ensure that this MIP remains up-to-date and relevant. It presents the Trust with the very best opportunity of continually improving the care which we provide to the patients of major incidents. This Trust develops its strategic, tactical and operational responses in cooperation with partner agencies in the Local Health Resilience Partnerships and Local Resilience Forums. Extensive consultation has also been undertaken with the other emergency services, local authorities, the military, and the voluntary sector. By its very nature, this plan will be subject to frequent review and, if necessary, revised to reflect the changing requirements of the NHS.
Ken Wenman Chief Executive Officer South Western Ambulance Service NHS Foundation Trust
FF FOO O
RR RWW W
AA ARR R
DD D

3
2. GOVERNANCE 2.1 Statutory and Contractual Compliance
2.1.1 The South Western Ambulance Service NHS Foundation Trust is committed
to meeting the obligations placed upon the Trust by
The Civil Contingences Act (2004)
NHS Act 2006 (as amended)
The Health and Social Care Act (2012)
NHS Standard Ambulance Contract
NHS England EPRR Core Standards
2.1.2 This document forms part of our planning process and thus assists with meeting these obligations. The Trust undertakes to work with partner agencies within the five Local Resilience Forums and Local health Resilience Partnerships areas that the Trust covers.
2.2 Consultation With Stakeholders
2.2.1 In order to ensure that the Trust‘s arrangements dovetail with responding
agencies, all internal and external stakeholders are consulted and collaborated with concerning their roles and responsibilities as far as is reasonably practicable.
2.3 Training and Exercising
2.3.1 The Trust is committed to a regular and continuous process of training and
exercising the Major Incident Plan using a combination of communication, tabletop and live exercises commensurate with the requirements of the NHS England Core Standards for Emergency Preparedness, Resilience and Response (2015).
2.4 Joint Emergency Services Interoperability Principles (JESIP) &
Lexicon of Terms
2.4.1 Common terms and abbreviations are explained throughout the document however a comprehensive list of terminology and abbreviations can be found at:
Lexicon of Terms
2.4.2 This document has been written to be compliant with the JESIP Joint
Doctrine.
2.5 Risks, Threats and Planning Assumptions
2.5.1 This plan has been produced to reflect the planning assumptions detailed within the National Resilience Planning Assumptions (Cabinet Office, 2015) and the Community Risk Registers which cover the Trusts area.
GG GOO O
VV VEE E
RR RNN N
AA ANN N
CC CEE E
GG G
OO OVV V
EE ERR R
NN NAA A
NN NCC C
EE E

4
3. ROLE AND PURPORSE OF THE MAJOR INCIDENT PLAN
3.1 Aim and Objectives of the Major Incident Plan
3.1.1 Experience in emergency management has repeatedly demonstrated the value of detailed planning and preparation for dealing with emergency situations.
3.1.2 The aim of this Major Incident Plan is to ensure the South Western
Ambulance Service NHS Foundation Trust (the Trust) response to a major incident is patient focused, clinically led and effectively managed.
3.1.3 The objectives of this plan are to :
Offer guidance, direction and information to ambulance staff and other NHS personnel
Assist in identifying roles, responsibilities and resources
Assist in forming action plans in order that normal provision of service may be maintained during a major incident as far as is reasonably practicable
Provide a source of reference that will assist in the integration of plans with hospitals, other NHS provider organisations, other emergency services and external agencies
Provide guidance for effective cross-boundary inter-service collaboration
Identify related plans and capabilities.
3.1.4 This plan provides a generic framework for operational response, however no plan can ever be complete against all possible contingencies and it is therefore essential that all staff and commanders exercise their judgment and initiative when confronted with such an incident utilising the principles outlined in this and associated plans and the Joint Decision Model
FF FOO O
RR RWW W
AA ARR R
DD D
RR ROO O
LL LEE E
AA ANN N
DD D PP P
UU URR R
PP POO O
SS SEE E
OO OFF F
TT THH H
EE E PP P
LL LAA A
NN N

5
4. DECISION MAKING AND USING THE PLAN 4.0.1 A Commander’s ability to perform their role effectively depends on them
being in a location where they have:
Knowledge of the circumstances and the available intelligence
The ability to communicate effectively with others
Advice available from National Inter-agency Liaison officers (NILO)
A suitable environment from which to exercise their command function.
4.0.2 Effective command and control can only be achieved by commanders who are capable of making reasoned, lawful and justifiable decisions.
4.0.3 The Joint Decision Model (JDM) should be used throughout any complex
or major incident in order to provide a consistent methodology within the Trust and across emergency services for making informed, reasoned, rationale and auditable decisions.
DD DEE E
CC CII I SS S
II I OO ONN N
MM MAA A
KK KII I NN N
GG G AA A
NN NDD D
UU USS S
II I NN NGG G
TT THH H
EE E PP P
LL LAA A
NN N

6
4.1 Using the Joint Decision Model
Info
rma
tio
n / In
fo
Re
ce
ive
d
During this stage the decision maker defines the situation (i.e. what is happening or has happened) and clarifies matters relating to any initial information and intelligence.
What is happening?
What do I know so far?
What further information (or intelligence) do I want or need?
As
se
ss
Ris
ks
& T
hre
ats
. D
eve
lop
a
Wo
rkin
g S
tra
teg
y.
This stage involves assessing the situation, including any specific threat, the risk of harm and the potential for benefits.
Do I need to take action immediately?
Do I need to seek more information?
What could go wrong? What could go well?
How probable is the risk of harm?
How serious would it be?
Is that level of risk acceptable?
Is this a situation for the ambulance service alone to deal with?
Am I the appropriate person to deal with this? Develop a working strategy to guide subsequent stages by asking yourself what you are trying to achieve. Remember that circumstances are constantly changing and so it might be necessary to conduct a Dynamic Risk Assessment at any given stage, according to the principles of the Hierarchy of Control.
Co
ns
ide
r P
oli
cie
s &
Pro
ced
ure
s
This stage involves considering what policies and procedures might be applicable in this particular situation.
What Ambulance resources might be required?
Is there any national guidance covering this type of incident?
Do any local organisational policies or guidelines apply?
What legislation might apply?
DD DEE E
CC CII I SS S
II I OO ONN N
MM MAA A
KK KII I NN N
GG G AA A
NN NDD D
UU USS S
II I NN NGG G
TT THH H
EE E PP P
LL LAA A
NN N
RR ROO O
LL LEE E
AA ANN N
DD D PP P
UU URR R
PP POO O
SS SEE E
OO OFF F
TT THH H
EE E PP P
LL LAA A
NN N

7
Wh
at
are
th
e O
pti
on
s?
This stage involves considering the different ways to make a particular decision (or resolve a situation) with the minimum risk of harm. Options
What options are open to me? Consider the immediacy of any threat, the limits of information to hand, the amount of time available, available resources and support, your own knowledge, experience and skills and the impact of potential actions on the situation and the public.
If you have to account for your decision, will you be able to say it was:
Proportionate, legitimate, necessary and ethical?
Reasonable in the circumstances facing you at the time?
Contingencies
What will I do if things do not happen as I anticipate?
What is my ‘plan b’?
4.2 Links to Associated Plans and Documents
4.2.1 This document is supported by the NARU Major Incident and CBRNE action cards which have been issued to all members of Operations Staff and Commanders and can be accessed on the intranet and internet sites.
4.2.2 It is vital that this plan is read in conjunction with Trust procedures and
arrangements and does not represent a complete ‘stand alone‘ resource. Sign posts are provided throughout this document to relevant supporting plans and materials.
4.2.3 This document does not seek to duplicate the comprehensive coverage of the subject within the suite of statutory and non-statutory guidance in this subject area.
4.2.4 A full list of linked / relevant plans, policies and procedures can be found in
Annex B.
9
DD DEE E
CC CII I SS S
II I OO ONN N
MM MAA A
KK KII I NN N
GG G AA A
NN NDD D
UU USS S
II I NN NGG G
TT THH H
EE E PP P
LL LAA A
NN N
DD DEE E
FF FII I NN N
II I TT TII I OO O
NN NSS S

8
5. DEFINITIONS
5.1 This section describes the definition of significant incidents and
emergencies as they may apply to NHS funded organisations and the varying scale of these incidents.
5.2 The JESIP Doctrine defines a Major Incident as: An event or situation requiring a response under one or more of the emergency services’ major incident plans.
5.3 A significant incident or emergency can be described as any event that
cannot be managed within routine service arrangements. Each require the implementation of special procedures and may involve one or more of the emergency services, the wider NHS or a local authority, a significant or emergency may include;
a) Times of severe pressure, such as winter periods, a sustained
increase in demand for services such as surge or an infectious disease outbreak that would necessitate the declaration of a significant incident however not a major incident..
b) Any occurrence where NHS funded organisations are required to
implement special arrangements to ensure the effectiveness of the organisations internal response. This is too ensure that incidents above routine work but not meeting the definition of a major incident are managed effectively.
c) An event or situation that threatens serious damage to human welfare
in a place in the UK or to the environment of a place in the UK, or war or terrorism which threatens serious damage to the security of the UK. The term ‘major incident’ is commonly used to describe such emergencies. These include multiple casualty incidents, terrorism or national emergencies such as pandemic influenza.
d) An emergency is sometimes referred to by an organisation as a major
incident. Within NHS funded organisations an emergency is defined as the above for which robust management arrangements must be in place.
5.4 The term significant incident or emergency is deliberately broad to ensure
that potential incidents are not missed. It recognises the fundamental importance of community confidence and trust in the NHS organisational response to any incident.
5.5 A significant incident or emergency to the NHS may not be any of these for
other agencies, and equally the reverse is also true. An incident may present as a variety of different scenarios, they may start as a response to a routine emergency call or 999 response situation and as this evolves it may then become a significant incident or be declared as a major incident, examples of these scenarios are overleaf.
DD DEE E
FF FII I NN N
II I TT TII I OO O
NN NSS S
DD D
EE EFF F
II I NN NII I TT T
II I OO ONN N
SS S
DD DEE E
FF FII I NN N
II I TT TII I OO O
NN NSS S

9
A disastrous single or simultaneous event(s) or other circumstances where the normal major incident response of several NHS organisations must be augmented by extraordinary measures in order to maintain an effective, suitable and sustainable response
DD DEE E
FF FII I NN N
II I TT TII I OO O
NN NSS S
DD D
EE EFF F
II I NN NII I TT T
II I OO ONN N
SS S

10
5. ROLES AND RESPONSIBILITIES
5.1 South Western Ambulance Service NHS Foundation Trust
5.1.1 South Western Ambulance Service NHS Foundation Trust has the responsibility for coordinating the on-site National Health Service response at the scene unless it is an internal NHS incident.
5.1.2 In the event of an incident, SWASFT may call on the support of adjacent
Ambulance Services and voluntary aid societies to ensure sufficient ambulances and trained medical personnel are rapidly deployed to the incident scene.
5.1.3 Key Strategic Responsibilities.
Save life, in conjunction with the other emergency services.
Instigate a command and control structure for NHS assets deployed to an incident.
Protect the health, safety and welfare of all health service personnel on site.
Co-ordinate the NHS communications on site and to alert the 'receiving' hospitals for the receipt of the injured.
Carry out a health service assessment for the incident.
Instigate a triage process.
Treat casualties.
Transport casualties to hospital.
Provide clinical decontamination of casualties, if required, and to support mass decontamination.
Mobilise the UK national reserve stock, as appropriate.
Maintain adequate emergency cover throughout other parts of the Ambulance Service area.
Reduce to a minimum the disruption of the normal work of the Service.
Alert and co-ordinate the work of the relevant Voluntary Aid Societies and private ambulances, enabling them to provide support services as appropriate.
Alert and make provision for the transport of the Burns Assessment Teams (BAT) and Mobile Surgical Teams if required.
Deploy a Hazardous Area Response Team (HART) or Ambulance Intervention Team (AIT) if required.
5.2 Other Responders
5.2.1 The roles and responsibilities of all other responders are detailed in full within
Emergency Response and Recovery (HM Gov, 2013) which can be located at this link
RR ROO O
LL LEE E
AA ANN N
DD D PP P
UU URR R
PP POO O
SS SEE E
OO OFF F
TT THH H
EE E PP P
LL LAA A
NN N

11
6. ACTIVATION, ESCALATION & MOBILISATION
6.1 Plan Activation
6.1.1 Any member of Trust staff may declare a major incident or major incident standby.
6.1.2 It is however the responsibility of the Divisional Tactical Commander to ratify
the decision and thus implement the Major Incident Plan, this process must be supported by the duty NILO.
6.1.3 It must be remembered that it is often easier to escalate unnecessarily and
subsequently stand down a response than it is to escalate further into an incident.
6.1.4 Once a major incident or major incident standby is initiated it can only be
stood down with authority from the Strategic Commander. This decision should be undertaken together with the Clinical Hub Duty Manager, Tactical Commander & N-ILO.
6.2 Major Incidents Declared By Other Agencies
6.2.1 Other agencies should always notify the Trust of a declared major incident by informing either the Operational / Tactical Commander (where one is present) or via the Clinical Hub
6.2.2 An appropriate response should be made to the incident based on the
information and intelligence available, however it must be noted that what is a major incident for another organisation need not necessarily be one for SWASFT.
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N
12
6.3 Role of the Ambulance Clinical Hub
6.3.1 The task undertaken by the Ambulance Clinical Hub (ACH) in any major or large-scale incident is an extension of their normal role, i.e. to act as a center for the communication of information, direction, dispatching and authorisation.
6.3.2 The Trust has three ACH’s, however when a Major Incident is declared a
‘lead’ ACH will assume responsibility for the management of the incident with support from the others. The ACH’s within the Trust are:
North Division Lead ACH: North Hub Support ACH: West Hub East and West Division Lead ACH: West Hub Support ACH: North Hub
6.3.3 In the initial stages of a major incident, information can be confusing,
conflicting and misleading. Therefore, it is vital that all Clinical Hub staff think ‘worst case scenario ‘until such time as information can be substantiated and confirmed. It is vital that Clinical Hub staff rapidly identify a potential or actual major incident and resource it appropriately in order to fulfill the Trust’s responsibilities as an emergency service and ‘gateway to the NHS‘.
6.3.4 Whilst the detailed functions and tasks for Clinical Hubs are detailed within
action cards within Clinical Hubs the key functions of the Clinical Hubs can be summarised as:
Deployment of the Pre-determined Attendance (PDA)
Initiating a cascade to the NHS and other stakeholders
Mobilising specialist assets e.g. HART
Mobilising Commanders and NILO’s
Establishing a communications network
Establishing the ACH Major Incident Room.
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N
CLINICAL HUB MAJOR INCIDENT ACTIONS
EACH CLINICAL HUB HAS SPECIFIC MAJOR INCIDENT ACTION CARDS WHICH SHOULD BE FOLLOWED IF A MAJOR INCIDENT OR MAJOR
INCIDENT STANDBY HAS BEEN DECLARED

13
6.3.5 Each of the Trust ACH’s has provision to coordinate a Major Incident in a Major Incident Room. The Major Incident room has provision for radio, telephony and CAD systems along with admin PC’s and SMART boards. The minimum requirement to staff the Major Incident Room should be two dispatchers with one call handler and a trained loggist. Ideally a ACH Senior Manager and the appointed Critical Information Manager should also be present.
6.4 Role of the Special Operations Desk (North Division Only)
6.4.1 The Special Operations Desk (SOD) has responsibility for the mobilisation
and co-ordination of:
Hazardous Area Response Team (HART)
National Inter-agency Liaison Officers (NILO)
Special Operations Response Team (SORT)
6.4.2 During a major incident the SOD dispatcher will continue to execute its normal functions within the context of the incident.
6.4.3 It should be noted that the SOD dispatcher is unlikely to have capacity to
undertake any additional functions.
6.4.4 Where possible consideration should be given to providing the SOD dispatcher with additional assistance to support their function.
6.5 Role of the HEMS Desk (East & West Division)
6.5.1 The Helicopter Emergency Medical Service (HEMS) has responsibility for the
mobilisation and co-ordination of all Air Assets including Critical Care. 6.5.2 During a major incident the HEMS dispatcher will continue to execute its
normal functions within the context of the incident.
6.5.3 It should be noted that the HEMS dispatcher is unlikely to have capacity to undertake any additional functions unless a number of Air Assets are grounded due to weather or operational limitations.
6.6 Critical Information Manager
6.6.1 During any major incident, significant amounts of information and intelligence will pass through the ACH, some of which will be critical to achieving a robust response, e.g. requests for further resources.
6.6.2 In order to avoid critical information being missed or suitable action not being
taken a member of staff should be appointed to constantly review all incoming information to ensure that where necessary action is taken.
6.6.3 An Action Card for this role is in Appendix A
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N

14
6.7 Pre-determined Attendance
6.7.1 The Trust has a standard pre-determined attendance for any major incident which must be sent as soon as the resource is available from any locality within the Trust.
6.7.2 It is however the responsibility of the Incident commander to stand the
resources down if they are not required.
6.7.3 In order to balance the needs of the incident against delivering an effective service across the whole Trust area the Incident Commander MUST make and communicate the decision to keep
6.7.4 The pre-determined attendance for a Major Incident Standby consists of:
3 Double Crewed Ambulances (DCAs)
3 Officers (Including Tactical & Operational Commanders)
1 N-ILO
Nearest Hazardous Area Response Team (HART)
1 Command Unit
1 Incident / Equipment Support Units
6.7.5 In addition to the pre-determined attendance for a Major Incident Standby the following resources must be dispatched as part of the pre-determined attendance for a Major Incident Declared:
3 Further Double Crewed Ambulances (DCAs)
3 Additional Officers
2 additional NILO’s
1 Additional Hazardous Area Response Team (HART)
1 National Mass Casualty Vehicle
6.7.6 The need for further specialist vehicles should be considered by the Incident Commander in conjunction with the N-ILO/Tactical Advisor at an early stage.
6.8 Multi-sited Incidents
From the outset of any potential or confirmed terrorist incident it should be assumed that there has been or will be further incidents and the Trust should ensure that the predetermined response is sent to each and every scene unless an appropriate Incident Commander positively indicates that it is not required.
6.9 Commitment
6.9.1 It will be important for the Tactical, Strategic and Clinical Hub Command team to consider the balance between committing resources to the scene and withholding them for further incidents and normal business until such time as additional resource is available through escalation and mutual aid to staff both.
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N
15
6.9.2 If a terrorist incident is suspected the command team should consider creating ‘pools’ made up of resources in line with the Major Incident PDA (See 6.7.4) in order to provide a response to further incidents.
6.9.3 The development of such resource cells should not be at the expense of
adequately resourcing incidents so the resources may necessarily therefore be derived from mutual aid.
6.10 System-Wide Escalation
6.10.1 During any major incident it is essential that the Trust uses the actions outlined within escalating REAP levels in line with the Trust’s Capacity Management Plan.
6.10.2 Measures should be authorised by the Strategic Commander but should
include measures to reduce demand, maximise availability of resources, utilise alternative care pathways, use of third party providers, etc.
6.10.3 The actions outlined in the Trust Capacity Management Plan represent a
significant part of major incident response and should be considered at an early stage.
6.11 Coordination of Hospital Capacity 6.11.1 In order for commanders to be able to meet the objective of sending the
correct patient, in the right order, to the right destination, using the right transport it is vital that good intelligence is available about what capacity exists at each point during the incident.
6.11.2 Upon the declaration of a major incident or major incident standby Acute
Trusts will provide bed states and capacity to receive casualties via the online reporting system accessible by the ACH and Command app no less than every 60 minutes.
6.11.3 This information should be collated and passed to the Incident Commander
to inform casualty distribution.
6.11.4 During a Major Incident it is imperative that Acute Trusts update CMS at least every 30 minutes.
6.12 Mutual Aid 6.12.1 A major incident has the potential to place significant pressure on the Trust
across all spheres of resources including:
Human
Vehicles
Equipment (Medical and Communications)
Consumable medical and surgical supplies.
6.12.2 In order to augment the Trust response it would be appropriate for the Strategic Commander to consider requesting mutual aid at a very early stage
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N

16
of a Major Incident.
6.12.3 In substantial Major Incidents, it is likely that large numbers of Ambulance resource type will be required (Emergency Ambulances for transportation). In these circumstances, resources should be mobilised in cells, each cell should be made up of 10 ambulances and 1 operationally command qualified manager. Mutual Aid in this type of incident would therefore be requested, by stating the number of cells required.
6.12.4 Mutual Aid is defined as:
“An agreement between responders, within the same sector or across sectors and across boundaries to provide assistance with the additional resources during an emergency which may go beyond the resources of an individual respondent.” (DoH 2015, EPRR Framework).
6.12.5 In order for mutual aid to be implementable every Trust is required by the
National MoU to ensure it is capable of providing support to other Trusts in a structured and progressive fashion.
6.12.6 The MOU provides a framework for:
• The request of mutual aid by any NHS Ambulance Service in response to a major emergency.
• Arrangements to supply assets/resources to a requesting NHS
Ambulance Service. • Arrangements for the receipt of assets/resources within an NHS
Ambulance Service that have been supplied by another NHS Ambulance Service.
6.12.7 The three primary criteria for implementing mutual aid arrangements are:
• SWASFT must have declared a major incident. • SWASFT can no longer manage the incident within its resource levels.
The Trust is potentially or actually unable to maintain safe level of critical services either through lack of material or human resources and be at REAP level Black (level 4).
6.12.8 Each Trust receiving such a request will have a duty to supply mutual aid on
request, subject to the maintenance of a safe level of service delivery within its own area.
6.12.9 The Service supplying mutual aid will nominate Form Up Points FUP(s) to
which all Mutual Aid resources will be deployed in the first instance to be held there prior to deployment on the instructions of the Trust. SWASFT should nominate an officer to manage the arrangements at the FUP.
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N

17
6.12.10 SWASFT Incident Commander should designate a RVP(s)/Marshalling
Areas for resources to be called forward to, from the FUP(s).
6.12.11 Supporting Services should be notified of “Casualty Evacuation Complete” by the ACH.
6.12.12 It is the responsibility of SWASFT Strategic Commander to initiate the
decision to return Mutual Aid assets to Services.
6.12.13 Should the Trust wish to cancel a Mutual Aid request the supporting Service should be notified without delay.
6.12.14 The principle of ‘shared risk’ in the context of the national MoU, recognises the fact that the risk of a major incident occurring, which results in the need for mutual aid, is equal amongst all NHS organisations.
6.12.15 Any mutual aid provided by assisting Ambulance Services will be on the
basis of ‘shared risk’ and costs lie where they fall. Consequently, there will be no cross charging for mutual aid between Ambulance Services.
6.12.16 It is recognised that the level of resources, which NHS Ambulance Services
are able to provide, will be governed by the resources that are available to it. To this extent the mutual aid provided will inevitably be time-limited and will be for discussion when an incident occurs.
6.12.17 If any NHS Ambulance Service wishes to discuss associated costs of
supplying extended mutual aid with the NHS then discussions may take place between the relevant finance directors once the major incident has been stood down.
6.12.18 As part of the national MoU each NHS Ambulance Service has agreed to
provide assistance in the form of:
The mobilisation, attendance, deployment and use of such of its available resources as are requested to deal with the major incident (these will be substantive NHS resources, not private or voluntary sector resources);
The mobilisation, attendance and deployment and use of such of its available resources as are requested to deal with other emergency incidents within the affected Ambulance Services area;
The deployment of such of its available resources as are requested to such locations in the affected Ambulance Services area as may be agreed in order to provide cover for other emergency incidents.
The attendance of such of its available senior officer resources as are requested to assist the command, control or deployment of ambulance resources for the purpose of any incident within the affected Ambulance Services area.
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N

18
6.11.21 In order to assist with the process of mutual aid SWASFT Strategic Commander should give consideration to holding a national teleconference with Strategic Commanders from each Trust.
6.12.19 SWASFT will have primacy at the scene of all NHS resources and all
resources deployed in pursuance of ambulance mutual aid will at all times act under the command and control of the Trust.
6.12.20 There are many specialist resources available within Services which may be
requested. SWASFT should indicate what specialist resources are required, i.e. CBRN, control, HART, SORT, USAR, air support etc.
6.12.21 Support from Voluntary Aid Services will be retained locally by Trusts to
augment core response.
6.13 National Co-ordination 6.13.1 In order to provide robust and coherent management of mutual aid and
national resources across the United Kingdom the National Ambulance Co-ordination Centre (NACC) may be established.
6.13.2 The Centre will be activated where immediate mutual aid across borders is
required. Its purpose is primarily three fold, firstly to maintain a database of information detailing the levels of pressure in the system for each Trust, secondly to coordinate requests for mutual aid between Ambulance Trusts and thirdly to provide a conduit between Ambulance Trusts and DH to highlight problems and disseminate agreed solutions.
6.13.3 It should be noted that the Centre will have no role in intervening in how
situations are being managed locally by SWASFT and will not be reporting information back to local Commissioners.
6.13.4 The NACC will be established and run by West Midlands Ambulance
Service with London Ambulance Service as a fallback if West Midlands is the affected Trust.
6.13.5 All mutual aid will be managed utilising the Proclus software through the
lead Clinical Hub.
6.14 Role of the 111 Service
6.14.1 NHS 111 is a free to call non-emergency medical helpline operating across England.
6.14.2 The service has replaced the triage and advice service previously provided
by NHS Direct
6.14.3 The service is available 24 hours a day, every day of the year and is intended for ‘urgent but not life threatening’ health complaints.
AA ACC C
TT TII I VV V
AA ATT T
II I OO ONN N
,, , EE ESS S
CC CAA A
LL LAA A
TT TII I OO O
NN N AA A
NN NDD D
MM MOO O
BB BII I LL L
II I SS SAA A
TT TII I OO O
NN N
18

19
6.14.4 NHS 111 Operators are able to dispatch ambulances when appropriate using the NHS pathways triage system.
6.14.5 SWASFT are the service providers some areas across the South West.
6.14.6 On declaration of a Major Incident the Clinical Hub will contact the relevant
111 service provider.
6.14.7 The 111 Service has escalation plans which will ensure its ability to surge and escalate capacity as part of the wider NHS community effort.
6.14.8 The 111 service provider will not be able to set and run ‘help lines’ or
provide incident specific information. Should these facilities be required liaison with NHS England should take place in the first instance.

20
7. ARRIVAL AT SCENE
7.1 Strategic Holding Areas
7.1.1 It will be necessary to organise Strategic Holding Area(s) (SHA) to be used as a marshalling site for the considerable resource and mutual aid coming into the area. Resources not immediately required should be held here on standby until called forward. At this location staff are made aware of their commanders, allocated call signs and radio talk groups. Full details are contained within the relevant LRF Strategic Holding Area Plan, however a summary of locations include:
Leigh Delamere Services (M4)
Strensham Services (M5)
Bath and West Showground
Cheltenham Racecourse
Devon County Show Ground (West Point)
Cornwall County Showground
Ringwood St Leonards
Taunton Dean Services
7.2 Rendezvous Point and Forward Control Point
7.2.1 A Rendezvous Point (RVP) will be needed closer to the scene, to coordinate resource deployment to the Forward Control Point (FCP).
7.2.2 The Rendezvous Point is the location where local resources and resources
from the Strategic Holding Area can come together and receive a tactical briefing prior to being operationally deployed forward to their working areas .
7.2.3 Depending on the size and complexity of the incident the FCP and RVP may be co-located.
7.2.4 The RVP and/or FCP location may also be dependant on wind direction
and ground drainage.
7.2.5 Suggested locations for FCPs and RVPs when responding to model response sites are available to commanders on a SECRET basis.
7.2.6 RVPs should always be searched for secondary devices and commanders
aware of the prospect of deliberate targeting.
7.2.7 Multi-agency Common RVPs will be agreed dynamically at the outset of the Incident with the relevant Police and Fire & Rescue Service
AA ARR R
RR RII I VV V
AA ALL L
AA ATT T
SS SCC C
EE ENN N
EE E

21
8. SCENE ASSESSMENT 8.0.1 Scene assessment will occur continuously throughout the incident. It will
commence at the Clinical Hub, continue with first responders and will not cease until the incident is resolved. What will change however is the increasing amount of scene assessment information available.
8.0.2 Initial responders should ensure they conduct a rapid scene assessment which should be communicated to the Clinical Hub using the METHANE mnemonic as detailed below and in individual action cards. This will ensure the provision of shared situational awareness.
SS SCC C
EE ENN N
EE E AA A
SS SSS S
EE ESS S
SS SMM M
EE ENN N
TT T
M
E
T
N
A
H
E
MAJOR INCIDENT DECLARED / STANDBY? (If not a major incident use ‘My Call Sign’)
EXACT LOCATION (Grid Reference / Road Name
ACCESS & EGRESS (Best routes in & out)
TYPE OF INCIDENT (E.g. Explosion, RTC, HAZMAT etc)
HAZARDS (Present & Potential)
NUMBER OF PATIENTS (Include type & severity)
EMERGENCY SERVICES / RESOURCES (Present & Required)

22
8.0.3 METHANE should be used as the format for briefings, situation boards and passing informative messages throughout an incident as apposed to simply being a tool for first arriving resources. The picture below demonstrates how it may be used in a command environment to secure shared situational awareness.
8.0.4 Once on scene the Hazardous Area Response Team (HART) have been trained to conduct a more detailed scene assessment which should be shared rapidly internally, with other emergency services and the rest of the NHS, again utilizing the METHANE format
8.1 Common Operating Picture (COP)
8.1.1 It is essential that commanders at all levels develop and share a common operating picture (COP) so as to ensure all responders have the same information.
8.1.2 JESIP defines a common operating picture as: Single display of information collected from and shared by more than one agency or organisation that contributes to a common understanding of a situation and its associated hazards and risks along with the position of resources and other overlays of information that support individual and collective decision making.
8.1.3 Responding Commanders and Clinical Hubs will wish to begin to develop
a COP in a standard format in order to facilitate easy sharing of information. A suggested format for a COP can be found in Annex D.
8.1.4 The use of the COP in Annex D will also provide a structured approach to
assessing how impactive a Major Incident may be.
SS SCC C
EE ENN N
EE E AA A
SS SSS S
EE ESS S
SS SMM M
EE ENN N
TT T
SS SCC C
EE ENN N
EE E AA A
SS SSS S
EE ESS S
SS SMM M
EE ENN N
TT T
23
8.2 Scene Assessment – HAZMAT / CBRNe
8.2.1 Should there be any concern that a CBRNe release may have occurred the scene assessment section of the Trust CBRNe Response Plan should be consulted for guidance.
8.3 Scene Assessment – Explosive Hazard
8.3.1 Should there be any concern that there may be explosive hazards
then the SWASFT SOP Responding to Incidents Involving Explosives & Suspect Packages must be consulted for guidance.
8.4 Scene Assessment – Marauding Terrorist Firearms Attacks (MTFA)
8.4.1 If firearms are involved then the actions and arrangements detailed
within the MTFA Joint Operating Principles (JOPS).
8.5 Intelligence
8.5.1 The Ambulance Incident Commander will establish a method of gathering intelligence from the following sources in order to determine a suitable measurement of threat and to inform decision making:
Feed from the National Inter-Agency Liaison Officer (N-ILO) and/or Tactical Advisor
Clinical Hub Duty Manager feeding intelligence as new calls are taken
Feed from Operational Commanders
News agency reports
CCTV systems and police helicopter downlink feed
AA ARR R
RR RII I VV V
AA ALL L
AA ATT T
SS SCC C
EE ENN N
EE E
SS SCC C
EE ENN N
EE E AA A
SS SSS S
EE ESS S
SS SMM M
EE ENN N
TT T

24
9. COMMAND, CONTROL AND CO-ORDINATION
9.0.1 This section of the Major Incident Plan is designed to compliment the detail contained within the SWASFT Command Policy, Command SOPs and the Association of Ambulance Chief Executives (AACE) Command Guidance (NARU, 2015)
9.0.2 Command and Control is defined by the Association of Ambulance Chief
Executives as:
The principles adopted by an organisation acting with full authority for the deployment and utilization of its resources. (AACE.2015)
COMMANDER ACTION CARDS
EACH COMMAND AND SUPPORT ROLE HAS SPECIFIC MAJOR INCIDENT ACTION CARDS WHICH SHOULD BE
FOLLOWED IF A MAJOR INCIDENT OR MAJOR INCIDENT STANDBY HAS BEEN DECLARED
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N
25
9.1 Framework of Command
9.1.1 In order to achieve a combined and co-ordinated response to a major incident the response structure of the Trust must be closely linked and dovetailed with those of all other responding organisations.
9.1.2 The system of command and control has been designed to provide all
responding agencies with a clear operating framework which promotes safe and efficient systems of work.
9.1.3 Ambulance trusts, akin to many emergency responders employs a three tier
command system comprising of a Strategic (Gold) Commander, Tactical (Silver) Commander and an Operational (Bronze) Commander.
9.1.4 This is a hierarchical system whereby individuals are empowered through
their role within the structure, providing them with specific authority over others for the duration of the event.
9.1.5 This is regardless of an individuals rank in the organisations day to day
structure. During an incident where the command structure is activated, the day to day rank of the individual changes into that persons role within the incident.
9.1.6 Command of an agency’s staff remains with the parent or designated
agency and, while working within the overall multi-agency structure, each agency has a vertical chain of command at the scene. However, in order to achieve an effective response to a Major Incident, the capabilities of the Ambulance service, and the NHS overall, must be closely co-ordinated with those of the other emergency services and participating agencies. Therefore, multi-agency strategic, tactical and operational activities in the response phase are routinely co-ordinated by the Police.
9.1.7 The command structure should be regularly reviewed to ensure that those
performing the required roles are sufficiently trained and competent. This assessment must always be documented formally.
9.1.8 It is important that the Trust command structure remains flexible enough to
meet changes in the nature of the threat, incident or operation without jeopardising clear lines of communication or accountability.
9.1.9 Every Commander must be aware that they are at all time legally
accountable for the actions and commands they provide.
9.1.10 A pictorial diagram of the SWASFT Command Structure can be found overleaf.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N
26
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

26
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N
Strategic Medical
Advisor
Medical
Advisor
Tactical Commander
Operational Commander
27
9.2 Command Resilience 9.2.1 Protracted incidents put pressure on the ability of the command team to
resolve an incident. Replacing commanders with fully briefed and appropriately trained and competent equivalents will prevent fatigue and, consequently poor judgment.
9.2.2 To ensure command resilience throughout the duration of the incident
consideration should be given to commanders fitness for duty, the identification of emerging stress factors and the capability and capacity of others involved in the response.
9.2.3 Where a commander is replaced, the command group have a responsibility
to ensure that:
The incoming commander has a full grasp of the situation, is fully briefed and able to undertake the role.
The integrity of the audit trail is maintained.
The integrity of the individual logs is protected.
Others in the command structure are informed when the handover is complete.
Everyone involved in the response is aware at all times who is in command.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

28
9.3 Command Inter-operability 9.3.1 Co-ordinated decision making between agencies and departments is
necessary to establish proper and coherent governance and is critical to achieving interoperability.
9.3.2 Commanders must be particularly aware of the need to ensure an
interoperable response through the application of the JESIP Principles, the use of the Joint Decision Model, METHANE for shared situational awareness and the key principles for joint working which are below.
CO-LOCATE Co-location of Operational Commanders as soon as
possible
Wearing tabards for easy identification
Identification of a multi-agency forward command point
COMMUNICATE
Face-to-face
Airwave (as secondary option)
Plain speech – no jargon!
CO-ORDINATE Identify lead service
Identify key priorities, resources and actions
Regular scheduled command meetings
JOINT UNDERSTANDING OF RISK All services understand relative likelihood & impacts of
threats and risks including clincial risks to patients.
Jointly agreed risk tolerances and control measures.
SHARED SITUATIONAL AWARENESS All services using METHANE
Use of joint decision model to frame all decisions.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

29
9.4 Strategic Command 9.4.1 The Strategic Commander operates at the strategic level and has overall
responsibility for the command, response and recovery from any Major Incident.
9.4.2 The Strategic Commander is responsible for setting the Trust’s strategic
aims (the strategy) for the incident, providing a framework for the Incident Commander to work within.
9.4.3 The default SWASFT strategy for any Major Incident is:
It is our intention to deal with any incident in an appropriate manner which promotes and saves life, reduces humanitarian suffering and is compatible with the vision and values of South Western Ambulance Service NHS Foundation Trust. Further Strategic Objectives can be located in Annex E
9.4.4 It should be noted that these may be changed by the SWASFT Strategic
Commander however consideration should be given to the interface with multi-agency strategic objectives.
9.4.5 Agreement of the multi-agency strategic objectives should be a priority for
the first Strategic Co-ordinating Group (SCG). 9.4.6 The purpose of implementing a strategic level of management is to establish
a framework within which Tactical Commanders will work. During Major Incidents the Strategic Commander will:
Establish a framework for the overall management of the incident.
Assess and assure the effectivness of the response.
Determine strategic objectives and priorities.
Rapidly formulate and implement an integrated media and communications plan.
Ensure clear lines of communication with the Tactical (Silver) Commander and external agencies.
Instigate further contingency and recovery planning as required.
Ensure the long term resourcing and expertise for command resilience.
Decide on what resources or expertise can be made available (mutual aid).
Undertake liaison with strategic commanders in other agencies.
Plan beyond the immediate response phase from recovering from the emergency to returning to or towards a new state of normality.
9.4.7 The Trust Strategic Commander function will be undertaken by the On Call
Strategic Commander in line with the rota and they have responsibility for the organisation.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

30
9.4.8 The Duty Strategic Commander will normally represent the Trust at the
multi-agency Strategic Co-ordinating Group (SCG).
9.4.9 Should the Strategic Commander deem it necessary they can elect to stand
up a Trust Incident Co-ordination Centre (ICC) located in the most appropriate Trust building in order to support the response.
9.4.10 The ICC locations for the Trust are Bristol (Acuma House), Exeter (HQ) and
St Leonard’s (East Hub)
9.4.11 The Trust Business Continuity SOP for establishing a ICC provides greater detail on locations, membership and operating arrangements.
9.5 Multi-Agency Strategic (Gold) Command 9.5.1 The scale or complexity of an incident may require the initiation of a Strategic
Coordination Groups (SCGs) which will require attendance and input from the Trust and are responsible for the overall strategic multi-agency management and coordination of the incident response.
9.5.2 Each organisation retains its own responsibilities but coordinated senior level
discussions ensure that links between strategic decisions are identified and corporate policies are agreed and applied.
9.5.3 Some of the issues which may need to be considered by the group are:
Welfare support for those dealing with events
Media warning and informing
Long term implications for the community or the environment
Visits by VIPs
Inquiries and investigations
The recovery phase
9.5.4 Where multiple SCGs are established, as a regional service, the Trust Strategic Commander may nominate a senior officer to liaise and attend local Strategic Co-ordinating Group, however in the representative case; they will not have delegated decision making powers.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

31
9.5.5 The pre-agreed Strategic Co-ordinating Centre / Group locations for the
SWASFT area are as follows:
Avon and Somerset: Police Headquarters, Valley Road, Portishead, Bristol. BS208QJ.
Dorset Police Headquarters, Winfrith. DT28DZ. Devon and Cornwall Police Headquarters, Middlemoor, Exeter. EX27HQ.
Gloucestershire Police Headquarters, Quedgley, Gloucestershire. GL22AN Wiltshire and Swindon Police Headquarters, London Road, Devizes. SN102DN
9.6 Tactical Command
9.6.1 The Tactical Commander works at the tactical level and is also known as the
Ambulance Incident Commander (AIC). The Tactical Commander has the responsibility for developing the Tactical Plan for the use of resources at the incident.
9.6.2 The Tactical Plan will be developed within the framework of the Strategy
and any available intelligence and associated risks.
9.6.3 Due to the dynamics of a Major Incident, the Tactical Commander may put a Tactical Plan into place before the strategy has been set. Where this is the case, the Tactical Plan should be reviewed against the strategy once it becomes available and ratified by SWASFT Strategic Commander.
9.6.4 The Tactical Commander will provide a framework and parameters for the
Operational Commander to operate (within the Tactical Plan).
9.6.5 The Tactical Commander must support the Operational Commander to achieve their objectives and manage the incident effectively; however they must not get involved in the direct operational management of the incident.
9.6.6 It is critical that the Tactical Commander can effectively manage the
incident and co-ordinate the ambulance response. With this in mind the Tactical Commander should locate themselves alongside the Tactical Commanders of the other emergency services and responding agencies in order to ensure a multi agency approach to the resolution of the incident.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N
32
9.6.7 The actual location of the Tactical Commander will be determined by the location of the Tactical Co-ordinating Group (TCG), which will usually be held at a local Police Station or near the incident scene.
9.6.8 In the event of multiple major incidents within the SWASFT area there
should only be one Ambulance Incident Commander, each scene should be commanded by a Operational Commander which may have functional roles reporting to him/her, this will be reviewed by the Strategic Commander as required.
9.7 Operational Command 9.7.1 The Ambulance Operational Commander works at the operational level and
has responsibility for the activities undertaken at the scene.
9.7.2 As such they will be located at the incident scene and ideally alongside the Operational Commanders of the other responding agencies at the Forward Command Post.
9.7.3 Where this is not possible, the Operational Commander must ensure regular
multi-agency face to face briefings take place. 9.7.4 As the Operational Commander they will provide leadership and
management to the Functional Role Officers and other direct reports.
9.8 Functional Roles 9.8.1 Once the AIC has nominated a Operational Commander, they may be
delegated the responsibility to then assign functional roles. 9.8.2 Functional roles may include:
Ambulance Communications Officer
Ambulance Decontamination Officer
Ambulance Equipment Officer
Ambulance Loading Officer
Ambulance Casualty Clearing Officer
Ambulance Parking Officer
Ambulance Safety Officer
HART Team Leader
Primary Triage Officer
Secondary Triage Officer
Sector Commander
9.8.3 The list above is neither exhaustive nor prescriptive and best use of available resources should be made to reflect the nature of the incident and the requirements of the Tactical Plan. All available roles are detailed within the Trusts Major Incident Action Cards.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

33
9.10 Receiving Hospital Based Functional Roles 9.10.1 The Tactical Commander should consider dispatch of Hospital Ambulance
Liaison Officers (HALO) to receiving Trusts where resources permit.
9.10.2 Hospital Ambulance Liaison Officer (HALO)
Based at receiving hospitals and working closely with the hospital management team (medical and operations), the HALO will ensure capacity issues are addressed early on (As described in Co-ordination of Hospital Capacity) advising the Ambulance Incident Commander of the requirement to find alternative hospitals. They will also facilitate swift handover and turnaround of ambulance resources.
9.11 Specialist Support Functions 9.11.1 Medical Advisor
The purpose of this role is to support the On Scene Ambulance Commander, providing medical advice with overall responsibility for medical resources deployed to the scene and the provision of appropriate clinical interventions. They ensure rapid throughput at the casualty clearing station, liaising with the ambulance loading officer, and advise on the need to escort Enhanced Care Teams forward to the incident. The Medical Advisor would request the invocation of P4 category in conjunction with the AIC and Strategic Medical Advisor.
9.11.2 Strategic Medical Advisor
The purpose of this role is to have medical input in the ambulance Incident Co-ordination Centre (ICC) where issues around appropriate hospitals, bed capacity and surge capacity can be identified and resolved, extra medical resources can be arranged and the outstanding normal patient workload can be monitored and prioritised when resources are diverted to a mass casualty incident. In addition, having the strategic overview they should advise on any necessary inter-hospital transfers that may be required e.g. stable critical care patients to hospitals outside of the receiving area to free up capacity.
9.11.2 National Inter-Agency Liaison Officer (N-ILO)
NILOs are specifically trained, qualified and vetted officers. The ILO will provide an interface to partnership agencies in order to facilitate a secure and robust exchange of information with a focus on risk reduction to staff and patients. Live intelligence can be fed by the ILO to the AIC and Strat via secure airwave communications.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N
34
9.11.3 Tactical Advisor
The Tactical Advisor has expertise to provide specialist advice on matters relating to the organisational major incident response.
N.B. It is important to recognise that whilst the role of the N-ILO and the Tactical Advisor will be undertaken by different individuals it may be necessary for one person to undertake both.
9.11.4 Loggist
The Trust has a number of trained Loggists who are able to maintain accurate log books and records in accordance with legal standards and best practice.
9.12 NHS Command and Control - Overview
9.12.1 Incidents can take many forms, therefore the responses need to match
individual situations. Most incidents will be dealt with by individual NHS organisations at operational/tactical level without the need for others to be involved. However, some incidents may require a wider NHS or multi-agency response.
9.12.2 NHS England Area teams (Hereon in referred to as ‘area teams’) provide
leadership across the following geographical areas:
Devon and Cornwall, Bristol, North Somerset, Somerset and South Gloucestershire
Hampshire, Dorset and the Isle of Wight (Wessex)
Wiltshire, Swindon, BaNES, Gloucestershire & Thames Valley.
9.12.3 Most incidents and emergencies can be managed at local or organisational level, so there is no need for the Area Team to take any action. However, SWASFT Strategic Commander must inform the Trusts commissioners and Area Team director on-call about any internal incidents, responses to local emergencies or cases of extreme pressure so that the area team has a detailed understanding of local NHS demand and capacity.
9.12.4 In some cases, several NHS and partner organisations may be involved
and the need for a coordinating role may arise. In these cases, the area team on-call director may take strategic command and control of the NHS.
9.12.5 If there is a Strategic Coordination Group, ‘health’ will be represented by
the on-call area team director (NHS Gold). If necessary, Public Health England, local authority directors
9.12.6 The Ambulance Service will also attend in its own capacity.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

35
9.13 Role of the Health Incident Co-ordination Centre (ICC)
9.13.1 The ICC will serve as a focal point for all liaisons between NHS and partner organisations regarding the incident. It is likely to be located away from the SCC and will be equipped with robust and resilient IT and telecommunications.
9.13.2 The ICC will have direct contact with all responding NHS providers. Its role
is to remain informed of their current status and provide relevant information to the SCG Health Gold representative.
9.13.3 The room will normally be staffed by a support team incorporating a range
of disciplines such as communications and EPRR specialists.
9.13.4 The main role of the area team ICC will be to:
Draw together information regarding the operational/tactical response across the NHS;
Gather information from wider sources relating to the incident; and
Make sure information flows efficiently between the chain of command and partner organisations.
9.14 NHS Command and Control – Wide Area Emergencies
9.14.1 If an incident affects two or more areas, the NHS response will normally
be led by the area team first affected and responding to it.
9.14.2 If the NHS England regional office has to take command of all NHS resources across the South of England, this will be actioned through the area team.
9.14.3 If an incident escalates to a national level (for example, a fuel shortage or
influenza pandemic), NHS England national office may take command of all NHS resources across England. In this situation, direction from the national office will be actioned through regional offices and onto the area teams.
9.14.4 In both cases, the NHS will be represented at the SCG by the Area Team
on-call director. 9.14.5 If there is a large or prolonged incident in one area, the Area Team may
need to request support from a neighboring area team. 9.14.6 The national emergency response structure can be found in a diagram
overleaf.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

36
9.15 Command and Control of SWASFT Service Lines (Non A&E)
9.15.1 The A&E Service Line will be directly commanded and managed by the command structure put in place by SWASFT albeit it will be in liaison with partners including Clinical Commissioning Groups and NHS England.
9.15.2 Where the Trust delivers commissioned services outside of A&E service
line e.g. 111 and Unscheduled Care these service lines will be commanded at the strategic level through the Clinical Commissioning group into NHS England.
9.15.3 In this instance it is vital that a high level of communication and co-
ordination is maintained with the SWASFT command structure through the trusts ICC.
9.15.4 The diagram overleaf is designed in a simplified way to show these
relationships.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

37
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N
ICC Manager

38
9.15 Airwave 9.15.1 En route to an incident assets will remain on their normal ‘domestic’
dispatch talkgroup until instructed to change talkgroups. 9.15.2 The Tactical Commander in conjunction with the Clinical Hub is
responsible for putting in place a communications plan. This should make use of the Major Incident talkgroups available on ICCS terminals and hand portables.
9.15.3 Any Major Incident talkgroups utilised should where possible be monitored
and recorded by the Clinical Hub. 9.16 Airwave Interoperability 9.16.1 Interoperability voice communications (IVC) is the ability to operate and
communicate with other agencies in a Command and Control scenario. 9.16.2 Interoperability can improve communications between emergency
services and appropriate partners helping to inform decision making through greater understanding of the incident and improved situational awareness.
9.16.3 The use of IVC through the airwave system should not replace face to
face meetings between Commanders, but compliment them. 9.16.4 Instigation of IVC should be made utilising the Communications
Interoperability Flowchart overleaf. 9.17 Department of Health Resilience Airwave Handsets 9.17.1 The Department of Health have provided SWASFT with additional Airwave
Handsets which are located within the Primary Clinical Hubs for use during an incident, communications failure or national emergency.
9.18 Interim Bronze Inter-Operability Solution Handsets (IBIS) 9.18.1 Each Police Force in the region has been provided with 10 additional
airwave handsets to facilitate the use of inter-operability talk groups amongst regular and non registered users of airwave.
9.19 Mobile Telephone Preferential Access Scheme (MTPAS) 9.19.1 The Trust has many Commanders with MTPAS enabled SIMs which will
ensure they will be prioritised for access to the mobile network once MTPAS is enabled by the Police and Network providers.
CC COO O
MM MMM M
AA ANN N
DD D,, , CC C
OO ONN N
TT TRR R
OO OLL L
&& & CC C
OO O-- - OO O
RR RDD D
II I NN NAA A
TT TII I OO O
NN N

39
INTEROPERABILITY FLOWCHART

40
10. SCENE MANAGEMENT
10.1 The Systematic Approach 10.1.1 The mnemonic CSCATTT provides a useful context for the tactical
priorities in the management of any scene which is summarised below
COMMAND AND CONTROL
Commanders must ensure that they have command and control of the incident. This is achieved through the implementation of the command structure.
SAFETY
Commanders must ensure the safety of all responders, patients and members of the public. This is achieved through risk assessment and the use of control measures.
COMMUNICATIONS
Commanders must ensure effective communications at incidents, internally and externally. The use of Airwave interoperability is a key part of this. Commanders must also provide information to inform the development of a Common Recognised Information Picture (CRIP).
ASSESSMENT
Using information, intelligence, risk assessments and available policies, plans and procedures, Commanders should make an assessment of the incident. From this the Commanders will develop the strategy and tactics for dealing with the incident. During the assessment phase Commanders will identify the level and types of resources required to manage an incident. This will include specialist resources such as HART and also the requirement for mutual aid.
TRIAGE
In order that casualties can be treated in the most appropriate manner a triage process is required. This will consist of an initial triage sieve, with a further triage SORT. During CBRN or active shooter incidents the triage process may need to be modified due to the environment and the levels of PPE required for responders.
TREATMENT Once casualty triage has taken place treatment (beyond life saving interventions) can commence.
TRANSPORT The availability of transport may vary so careful consideration must be given to the capability and suitability of transport types.
SS SCC C
EE ENN N
EE E MM M
AA ANN N
AA AGG G
EE EMM M
EE ENN N
TT T
SS SCC C
EE ENN N
EE E MM M
AA ANN N
AA AGG G
EE EMM M
EE ENN N
TT T

41
10.2 Scene Overview 10.2.1 The schematic below provides a pictorial reference for the key functions
within a major incident scene.
10.3 The Inner Cordon
10.3.1 The inner cordon will surround the area considered hazardous and will be subject to strict entry control requirements.
10.3.2 The boundary of the inner cordon will usually be marked by red and white
barrier tape laid out by Fire and Rescue Service (FRS). However, a degree of flexibility will exist in marking the perimeter of the inner cordon (e.g. for an incident in a building with restricted entry, the walls of that building may be designated as the inner cordon perimeter).
10.3.3 The FRS is responsible for monitoring the inner cordon for the safety of all
personnel. However, the Ambulance Safety Officer will support this role by specifically monitoring the health, safety and welfare of all ambulance and medical personnel at the scene.
10.3.4 The FRS will log all personnel in and out of the inner cordon although HART
personnel will be responsible for their own entry control.
SS SCC C
EE ENN N
EE E AA A
SS SSS S
EE ESS S
SS SMM M
EE ENN N
TT T

42
10.3.5 Access to the inner cordon will be strictly limited to personnel with a specifically designated task. On the completion of the task, personnel should withdraw from the inner cordon unless designated a further specific task.
10.4 The Outer Cordon
10.4.1 The outer cordon will surround the entire incident and will usually
encompass an area with a radius of several hundred meters. 10.4.2 Entry and exit through the outer cordon will be strictly controlled by Police
Officers / Police Staff.
10.4.3 The outer cordon may consist of police vehicles or officers blocking streets, traffic cones, tape, portable metal fencing, etc
10.4.4 Whilst situations do vary, the following key functions will usually be situated
within the outer cordon but outside the inner cordon:
The Command Unit
TCG and a working base for the Ambulance Incident Commander / Medical Advisor
The Casualty Clearing Station
The Ambulance Loading Point
The Ambulance Parking Point
Any Equipment Collection Points
11.4.5 The Ambulance Loading Point may need to be located on the periphery of the outer cordon, with resources called forward to the Ambulance Loading Point as required.
10.5 Specialist Major Incident Resources
10.5.1 A range of resources are available both within the trust and externally to support and augment a Major Incident response.
10.5.2 Whilst many resources already form part of a pre-determined attendance it
will be necessary to consider what additional resources may be required at the earliest possible opportunity.
10.5.3 Full details of the available resources can be found in Appendix G.
SS SCC C
EE ENN N
EE E MM M
AA ANN N
AA AGG G
EE EMM M
EE ENN N
TT T
43
10.6 Hazardous Area Response Team (HART)
10.6.1 SWASFT has two HART teams which are based in Bristol and Exeter.
10.6.2 The HART provision forms the capability to provide paramedic level care within inner cordons previously not accessible by the Trust.
10.6.3 These capabilities are delivered through the use of dedicated fleet and
specialist PPE such as Extended Duration Breathing Apparatus, Safe Working at Heights (SWAH) Equipment, and ballistic protection.
10.6.4 Both HART units are fully interoperable and should be utilised in a Major
Incident.
10.6.5 Full details on HART can be found within the HART Standard Operating Procedures
SS SCC C
EE ENN N
EE E MM M
AA ANN N
AA AGG G
EE EMM M
EE ENN N
TT T
SS SCC C
EE ENN N
EE E MM M
AA ANN N
AA AGG G
EE EMM M
EE ENN N
TT T

41
11. TRIAGE, TREATMENT AND TRANSPORT
11.1 Patient Triage
11.1.1 In situations where demand exceeds resources available it is important that
treatment priorities are established so that resources can be appropriately focused on those patients most in need.
11.1.2 Complete anatomical examination is too time consuming to be used in these
circumstances however, physiological methods are simple, quick and reproducible ways of reliably identifying patients who have serious injury.
11.1.3 Triage must be a dynamic and continuous process. The principles of triage
should therefore be used whenever the number of casualties exceeds the number of skilled rescuers available.
11.1.4 Triage of casualties merely establishes order of treatment, not which or
whether treatment is provided. Obviously all casualties require treatment.
11.1.5 However, triage is a tool that aids the medic’s ability to predict which casualties have the greatest probability of survival or the need for a casualty to undergo a Life Saving Intervention (LSI), thus determining the priority and urgency of treatment and evacuation.
11.1.6 Each Ambulance and Rapid Response vehicle within the Trust carries
supplies of triage equipment. Additional supplies are contained within the Incident Support Units, National Mass Casualty Equipment Vehicles and HART vehicles.
11.1.7 Patients should be reassessed and re-triaged where appropriate at regular
intervals and where practical no less than every 15 minutes.
11.1.8 The Trust recognises the importance placed on Triage by the Corporate Manslaughter and Corporate Homicide Act 2007.
11.1.9 Where, possible appropriately trained and equipped doctors should be
utilised to support the triage undertaken by ambulance staff.
11.1.10 During the triage process, clinicians MUST provide life saving interventions to maintain an airway or stem catastrophic haemorrhage.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
AA ANN N
DD D CC C
AA ASS S
UU UAA A
LL LTT T
YY Y
CC CLL L
EE EAA A
RR RII I NN N
GG G
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G
CORE PRINCIPLE OF MAJOR INCIDENT RESPONSE
The over riding principles of the response at all times, and particularly when considering treatment regimes, are that:
The needs of patients must always be kept at the centre of
the response and ongoing care

42
11.1.11 The range of Triage Categories are as follows:
RReedd
PP11 Immediate First Priority
YYeellllooww
PP22
Urgent Second Priority
GGrreeeenn
PP33 Delayed Third Priority
BBlluuee PP44 Expectant (special circumstances only)
11.2 Casualty Labeling & Patient Records
11.2.1 There are three stages of casualty labelling and documentation, namely;
SMART Triage Cards
Patient Care Record Forms
Electronic Patient Care Records
11.2.1 SMART Triage Cards
To be used for the Triage Sort process. These uniquely numbered cards allow for patient details e.g. brief identifying information (i.e. Male, 40s) to be recorded along with details of any drugs administered or interventions taken. This allows for the casualty to be better tracked and provides more information for further care.
11.3 Patient Care Record Form
11.3.1 All patients must have a Patient Care Record (PCR) completed during a major incident, even if details have been captured within the SMART triage card.
11.3.2 The PCR should be completed at the Casualty Clearing Station and during onward transport.
11.3.3 A record of those leaving the scene will be kept by the Ambulance Loading Officer.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G
TT T
RR RII I AA A
GG GEE E
,, , TT TRR R
EE EAA A
TT TMM M
EE ENN N
TT T && &
CC CAA A
SS SUU U
AA ALL L
TT TYY Y
CC CLL L
EE EAA A
RR RII I NN N
GG G

43
11.3.4 Lists of those transported may be viewed and / or copied by the Police
documentation teams, but the original should be held by the Ambulance Loading Officer.
11.3 Casualty Labeling & Patient Records 11.4 Triage Sieve
11.4.1 This is a very rapid assessment of casualties. This should be undertaken at the scene of the incident using the triage cards.
11.3.1 Whilst the triage Sieve includes Capillary Refill Time as an indicator, this
should only be used in the absence of pulse or AVPU as it can be less accurate.
11.3.2 Clinicians are required to verify the absence of signs of life where they
encounter victims who have already been covered by other agencies / individuals and triage accordingly.`
11.3.3 The NASMeD approved triage sieve algorithm can be found overleaf

44
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G
TT T
RR RII I AA A
GG GEE E
,, , TT TRR R
EE EAA A
TT TMM M
EE ENN N
TT T && &
CC CAA A
SS SUU U
AA ALL L
TT TYY Y
CC CLL L
EE EAA A
RR RII I NN N
GG G

45
11.4 Triage Sort
11.4.1 This is a more anatomically based system which makes use of the Glasgow Coma Scale, Systolic Blood Pressure and Respiratory Rate. Triage Sort should be undertaken at the Casualty Clearing Station utilising the Triage Cards. There is the opportunity to also record basic patient details and treatments or drugs administered.
11.4.2 The algorithm and assessment criteria utilised during triage Sort can be seen
below.
11.5 Paediatric Triage Sort 11.5.1 Separate Triage algorithms exist for Paediatric casualties based on height –
copies of these algorithms are included with all triage packs on ambulances. Should the Triage Tape not be available, then the child should be triaged as an adult as this will lead to the child being over not under triaged.
11.6 Expectant Category
11.6.1 The expectant category has never been formally implemented within a
civilian setting though it is foreseeable that there may come a time when there is not sufficient resource to treat all Priority One patients. However, should at any point the expectant category be suggested it must be passed to SWASFT Strategic Commander for consideration in conjunction with the Strategic Medical Advisor.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G

46
11.6 Injured Children
11.7.1 Specific arrangements apply for the management of children in major incidents which take account of the following situations:
Those involving only children.
Those which result in adult and child casualties. Those in which only adults are injured, but attendant children must be
cared for.
11.7.2 Where children are present, the Clinical Hub and receiving hospitals must be notified to allow the receiving hospitals to prepare for their reception. Where many children are injured, the Ambulance Incident Commander (AIC) will advise the Clinical Hub and must request access to paediatric life support equipment, which may need to be supplemented from local paediatric units. Whenever possible, the parents’ wish to remain with their children should be accommodated.
11.7.3 In order to balance the needs for the treatment of seriously injured adults and/or children against the availability of hospital resources; the following model should be adopted within operational capabilities:
If adults and children are seriously injured.
They may need to be taken to separate facilities, but a balance needs to be struck between the benefits to children of being kept close to their parents and their distress at seeing severely injured parents
If the adults are seriously injured but the children have only minor injuries
The family should be taken to the hospital for adults where arrangements for the care of children should be made .
If the children are seriously injured and the adults are uninjured or have only minor injuries
The family should be taken to the appropriate hospital, where the adults can be treated and help with care of the children. The Ambulance Incident Commander should liaise with the Medical Incident Advisor to decide which hospital should be used.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G

47
11.8 Uninjured Children 11.8.3 SWASFT discharge their duties with regard to the need to safeguard the
well being of children. Children should not be entrusted to adults with no connection with the child, however well meaning, and Ambulance personnel are to ensure their safety until relieved by an appropriate authority. In the event of an incident where children are left unaccompanied, but uninjured, the responsible authority is the Local Authority for the area of the incident.
11.8.4 The AIC is to advise the Clinical Hub of the numbers and details of
uninjured and unaccompanied children and make arrangements for their temporary well-being. The Clinical Hub will make contact with the Social Services/Children’s Services directorates in the Local Authorities to arrange for their on-care.
11.9 Incidents Involving Burns
11.9.1 Major Incidents involving high numbers of patients with burns require
special considerations.
11.9.2 The Trust’s arrangements for the management of burns incidents is outlined in the South West Regional NHS Burns Plan however overview arrangements are provided within this section for immediate reference.
11.9.3 Burn care in the SWUK area is organised using a tiered model of care
(centre, units and facilities). The most severely injured are cared for in burn Centre’s with those requiring less intensive support being cared for in burn units. Patients with smaller burn injuries are cared for in facility-level burn care services. Each service provides care at and below the level of the service designation.
Burn Facilities This level of in-patient care equates to a standard plastic surgical ward for the care of smaller and less severe burn injuries.
Burn Units This level of in-patient care is for the moderate level of injury complexity and offers a separately staffed, discrete ward.
Burn Centres This level of in-patient burn care is for the highest level of injury complexity and offers a separately staffed, geographically discrete ward. The service is skilled to the highest level of critical care and has immediate operating theatre access.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G

48
Hospital Location for Burn Care Services Service Level
Morriston Hospital Swansea SA6 6NL
Adults Centre/Unit/Facility level
care Children Unit /Facility level care
Southmead Hospital , Bristol (Note: Paediatric Intensive Care (provided by Bristol Children’s Hospital)
Adults Unit /Facility level care Children Centre/ Unit /Facility Level
care
Salisbury District General Hospital
Unit /Facility level care for Adults and Children
Derriford Hospital, Plymouth Facility level care for Adults and Children
11.9.4 A burn major incident is an event which results in a significant increase in the demands placed on a specialised burn service and as a consequence the service cannot deliver optimal level of burn care using the routine resources available to the local burn service.
11.9.5 In a major Incident the decision regarding the receiving hospital for burns
patients rests with the Ambulance Incident Commander who should seek clinical advice and support from the Medical Incident Advisor. The bale below provides a quick reference guide.
Injury type Transported to/Transferred to or
Outreach obtained from:
Multiple injuries with burns as secondary injuries
Trauma Centre
Life threatening burns Burn Centre
Non life threatening Burns Burns Service (Centre/Unit/facility)
Life threatening inhalation injury Critical Care
11.9.6 In the event of there being a major incident involving significant numbers of
adult and child casualties, the Burn Care Centre at Swansea would take the overall lead in Network co-ordination, but would work in close liaison with the Paediatric Burn Care Centre at Southmead Hospital.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G

49
11.10 Incidents Involving Major Trauma
11.10.1 It is highly likely that in any ‘big bang’ Major Incident will result in casualties suffering from major trauma. It is therefore imperative that the existing mechanisms for management of trauma are utilised during a Major Incident.
11.10.2 NHS Choice defines ‘Major Trauma’ as multiple, serious injuries that could
result in disability or death. These might include serious head injuries, severe gunshot wounds or road traffic accidents.
11.10.3 Major Trauma is defined in the scientific literature using the Injury Severity
Score (ISS), which assigns a value to injuries in different parts of the body and totals them to give a figure representing the severity of injury. An ISS greater than 15 is defined as Major Trauma. This would include serious injuries such as bleeding in the brain or a fracture of the pelvis and cases of multiple injuries.
11.10.4 Trauma services are currently provided by a number of the Acute trusts
within the SWASFT area (Trauma Units). High end specialist trauma care is provided by Southmead Hospital (Bristol) and Derriford Hospital (Plymouth). These are known as Trauma Centres. The diagram below shows the existing Trauma Centres, Trauma Units and their links through the Trauma Networks.
11.10.5 The existing SWASFT trauma triage tool should be utilised when managing casualty dispersal and transport.
11.10.6 The diagram overleaf should be used as a quick reference guide to assist
in assessing likely journey times to a Major Trauma Centre.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G

50
11.11 Patient Confidentiality
11.11.1 The police will establish Documentation Teams, where casualties are being received, in order to provide the Police Casualty Bureau with information. While Ambulance personnel need to co-operate with Police, they must also bear in mind their duty of confidentiality to individual patients. Staff should not normally disclose personal information outside the NHS without the consent of a patient. In a major incident, the duty of confidentiality is not automatically lifted.
11.11.2 Generally, patient consent is needed unless:
There is overriding public interest in disclosing information, or
It is in the patient’s best interests.
11.11.3 If a patient specifically refuses consent to information being disclosed, that wish must be respected unless there is an overriding duty to the public. The Ambulance Incident Commander will provide guidance in consultation with the Police.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G
51
11.12 Dealing With Fatalities
11.12.1 The overall responsibility for all matters concerning deceased casualties lies with HM Coroner. The Police, acting for HM Coroner, will make arrangements for the temporary storage of bodies. Where there are significant numbers of deceased casualties an emergency mortuary facility (as opposed to a hospital mortuary) will generally be established by a Local Authority at the request of HM Coroner.
11.12.2 The dead should not be moved from scene unless that is the only way of reaching a live casualty, or if the deceased is likely to deteriorate due to environmental hazards such as fire. Where this is the case, every effort must be made to record the original location prior to movement. Dead bodies must otherwise be left in place until the evidence gathering stage begins.
11.12.3 In addition to the black triage label attached to those confirmed dead, the police will attach numbered sections of a blue National Body Label to the body.
11.12.4 All Emergency Services on-scene have a legal obligation to provide evidential continuity of the handling of a deceased from its location at the incident, through its recovery to the post mortem examination. Deceased persons if removed from scene, will be taken to a Body Holding Area, usually adjacent to the Casualty Clearing Station, where a Medical Body Holding Officer, if appointed, will confirm death if necessary.
11.12.5 Casualties Who Die En Route to Hospital. For casualties who die en route to hospital, normal arrangements apply with the casualty being certified ‘dead on arrival’ in the Emergency Department and then transferred to the hospital mortuary.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G
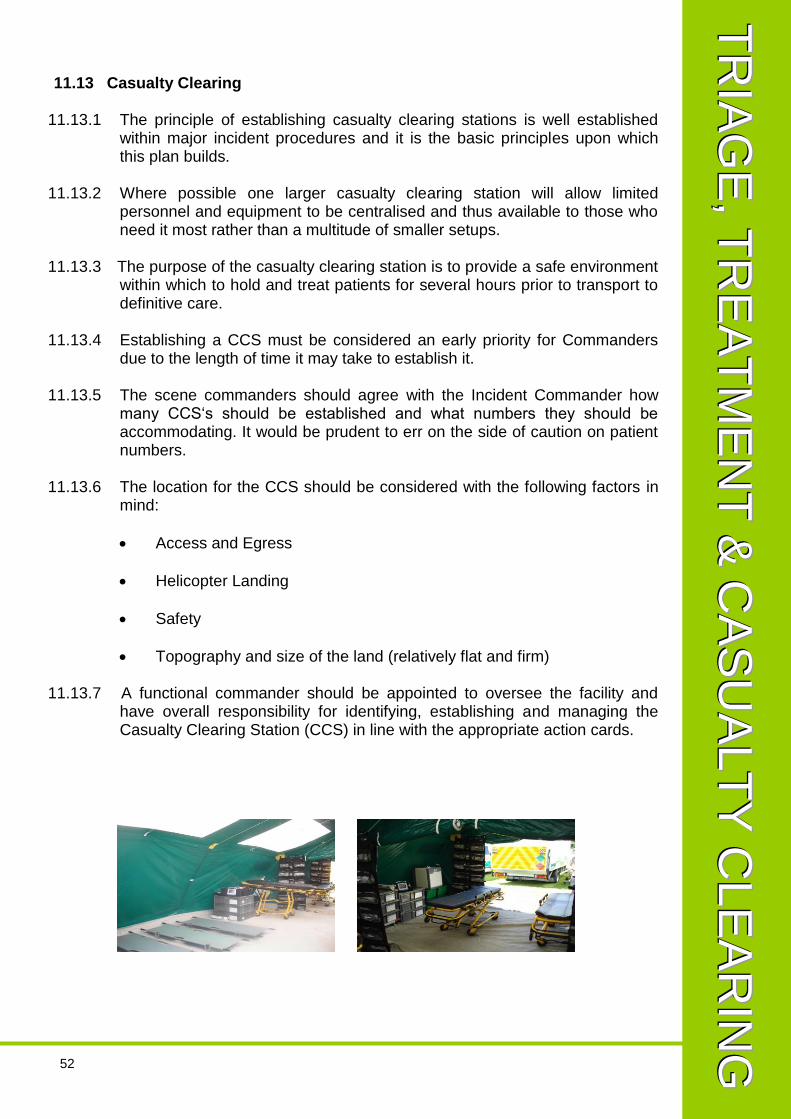
52
11.13 Casualty Clearing 11.13.1 The principle of establishing casualty clearing stations is well established
within major incident procedures and it is the basic principles upon which this plan builds.
11.13.2 Where possible one larger casualty clearing station will allow limited
personnel and equipment to be centralised and thus available to those who need it most rather than a multitude of smaller setups.
11.13.3 The purpose of the casualty clearing station is to provide a safe environment
within which to hold and treat patients for several hours prior to transport to definitive care.
11.13.4 Establishing a CCS must be considered an early priority for Commanders
due to the length of time it may take to establish it. 11.13.5 The scene commanders should agree with the Incident Commander how
many CCS‘s should be established and what numbers they should be accommodating. It would be prudent to err on the side of caution on patient numbers.
11.13.6 The location for the CCS should be considered with the following factors in
mind:
Access and Egress
Helicopter Landing
Safety
Topography and size of the land (relatively flat and firm)
11.13.7 A functional commander should be appointed to oversee the facility and have overall responsibility for identifying, establishing and managing the Casualty Clearing Station (CCS) in line with the appropriate action cards.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G

53
11.14 Options for Shelters
11.14.1 A variety of options are available to Commanders, a mixture should be utilised as the capacity / location demands. Options include:
TM36/TM18 Tents
Aireshelters / Inflatable Shelters
Buildings
Mass Decontamination Units
11.15 Staffing a Casualty Clearing Station 11.15.1 The staffing for the CCS should be on extended skills practitioners including:
Critical Care Team
Emergency Care Practitioners
Paramedics
11.15.2 The staff should be sought from within the existing Trust capacity, mutual aid and that which is provided by the regional mass casualty plan.
TT TRR R
II I AA AGG G
EE E,, , TT T
RR REE E
AA ATT T
MM MEE E
NN NTT T
&& & CC C
AA ASS S
UU UAA A
LL LTT T
YY Y CC C
LL LEE E
AA ARR R
II I NN NGG G

54
12. TRANSPORT AND PATIENT MOVEMENT
12.1 Use of Double Crewed Ambulances 12.1.1 Additional DCAs may be sourced. However access to DCAs should be
prioritised for those patients requiring active management en route to definitive care.
12.1.2 Consideration should be given to carrying more than one patient in each
DCA where possible, especially where journey times allow for a reduced level of care en route. In order to maximise transportation space families and relatives should not be carried except in instances where not doing so would place a patient at risk and thus reduce the opportunity for crew staff to undertake a quick turn around.
12.1.3 Authority to carry next of kin, families or carers rests with the Ambulance
Loading Officer.
12.1.4 Consideration must be given to splitting crews to maximise skill mixes and using double unqualified crews where this is permitted by the patients injuries.
12.1.5 Commanders should consider using DCAs on mutual aid from the service
covering the Trust if the destination Acute Trust is outside of the SWASFT operational area. e.g. Use a West Midlands Ambulance DCA for conveying patients to Birmingham.
12.2 Patient Transport Service (PTS) 12.2.1 PTS provision across the southwest region is principally supplied by other
provider organisations.
12.2.2 PTS providers may be able to assist with resources however this should be negotiated through the Trust ICC in conjunction with NHS England & CCGs.
12.3 Public Transport 12.3.1 The use of double decker buses or similar as a form of transport may
represent a viable option for walking wounded/P3 patients, however their use must be pre-agreed by the Strategic Commander and the destinations notified. Ambulance /NHS personnel must travel with the patients.
12.4 Motorcycle Responders 12.4.1 Motorcycle responders can be used for their clinical skills as they are not in
a position to carry patients and convey only a limited amount of equipment 12.4.2 They can also be used as “runners” should lines of communication break
down.
TT TRR R
AA ANN N
SS SPP P
OO ORR R
TT T AA A
NN NDD D
PP PAA A
TT TII I EE E
NN NTT T
MM MOO O
VV VEE E
MM MEE E
NN NTT T

55
12.5 British Red Cross & St John Ambulance 12.5.1 The British Red Cross (BRC) and St John Ambulance (SJA) will be able to
provide a range of Ambulances, First Aiders and Treatment Centers to support a response either at scene or at another centre e.g. Emergency Treatment Centre.
12.5.2 Memorandums Of Understanding are in place with both SJA and BRC
which provide full details on the arrangements for deploying their assets.
12.5.3 If deployed both the BRCS and SJA will provide a liaison officer too provide expert advice on what assets are available and how they can be best deployed.
12.6 Air Assets 12.6.1 Across the UK there is a wide variety of Air Ambulances, Helicopter
Emergency Medical Services(s) (HEMS) and Search and Rescue aircraft available. These assets may be invaluable in taking patients to receiving hospitals some distance away or bringing staff /supplies to the scene.
12.6.2 The HM Coastguard National Maritime Operations Centre (NMOC) has the
overarching responsibility for co-ordinating the activities of and mobilising UK Search and Rescue assets. The SWASFT Special Operations Desk will coordinate the mobilisation of any regional air ambulance assets, it must be noted that air ambulances are day time only but it maybe possible to arrange night capability for transfers.
12.6.3 NMOC contact details are held within the Clinical Hubs
TT TRR R
AA ANN N
SS SPP P
OO ORR R
TT T AA A
NN NDD D
PP PAA A
TT TII I EE E
NN NTT T
MM MOO O
VV VEE E
MM MEE E
NN NTT T

56
13. SURVIVOR MANAGEMENT
13.0.1 In responding to a major incident and to achieve the goal of doing the most
for the most‘ it is vital to ensure that P3 patients are managed effectively without absorbing resource which may be better utilised elsewhere.
13.0.3 P3s by virtue of the fact that they are ambulant will usually self evacuate the
area in search of familiar surroundings e.g. home or healthcare, which may be the nearest NHS establishment, not necessarily one designed for accident and emergencies.
13.0.4 On arrival SWASFT Commanders would assist the Police to identify a
suitable survivor reception point to which all P3s can be directed. It must however be remembered that this remains a Police function.
13.0.5 Once a survivor reception point has been established the Commander
should consider, where feasible, allocating resource to that area. It must be remembered that P3 patients can rapidly deteriorate, especially once out of immediate danger and ‘fight or flight‘ syndrome subsides.
13.0.6 The additional benefit of allocating some resource to an area containing P3s
is that they will be able to provide intelligence both for SWASFT and the wider NHS about how many P3s there are and how many of them require what treatment.
13.0.7 In the early stage of an incident self help should be encouraged and those
with some medical training, e.g. first aiders identified to assist.
13.0.8 Depending on the size of incident and the number of resulting P3s clinical equipment may be provided by Emergency Dressings Packs, Mass Casualty Equipment Vehicles or other sources.
13.0.9 Emergency Dressings packs are located at transport hubs and others areas
such as shopping centers where large crowds gather. A full list of locations is contained within Appendix G
13.0.9 Commanders will need to give due consideration about how best to prevent
key NHS premises and resources being overwhelmed through self presenters, this should be done in conjunction with the Police.
SS SUU U
RR RVV V
II I VV VOO O
RR R MM M
AA ANN N
AA AGG G
EE EMM M
EE ENN N
TT T

57
14 COMMUNICATIONS AND MEDIA
14.1 External Communications 14.1.1 During an emergency, the media are an important stakeholder group with
whom all agencies will need to communicate. This is important on two levels:
The media have a vital role to play in warning and informing the public, a requirement on all category 1 agencies under the Civil Contingencies Act 2005.
The media also have a job to do. They will report on anything that is deemed newsworthy and within an emergency there is an immediate need for information to fill those news spots.
14.1.2 In today‘s global economy, during an emergency, agencies could find
themselves contacted by a full range of print and broadcast media working to the 24 hour news agenda on a regional, national and international basis. Social media sites also have a well established role in breaking news and reporting details and eye witness accounts of major incidents.
14.1.3 As a category 1 responder, SWASFT, along with its partner agencies, must
be prepared to communicate 24 hours a day during a large scale emergency.
14.1.4 Depending upon the incident, certain agencies would be subjected to
intense pressure by worldwide media, journalists and film crews, all requiring up-to-date information at regular intervals. Social media sites will also require constant monitoring and updating. Confident, uniformed spokespeople able to give broadcast and print media interviews 24/7 will be essential and the Strategic Commander will be expected to identify the spokesperson available at any one time.
14.1.5 In order to prepare for this SWASFT maintains a toolkit which acts as an
ambulance service guide for the protocols to be followed and includes practical tools to support this should a crisis occur.
14.1.6 The purpose of this toolkit is to make available a framework to supply a
speedy, but accurate and regular flow of co-ordinated information to all media agencies and key stakeholders. It is vital that the information that is provided to the media is factually accurate, consistent and timely. This can only be achieved through a co-ordinated partnership approach by SWASFT and its partner agencies to ensure that fast, accurate information is available and updated on a timely basis and key messages are joined up.
CC COO O
MM MMM M
UU UNN N
II I CC CAA A
TT TII I OO O
NN NSS S
&& & MM M
EE EDD D
II I AA A

58
14.2 Internal Communications
14.2.1 The Trust Communications Department will co-ordinate corporate communications in relation to any incident, both externally and internally.
14.2.2 The need to inform internal staff of any developments, intentions and
accurate information has become an expectation and full consideration needs to be taken in the depth of information released.
14.2.3 Internally it is important to inform staff of an incident, otherwise staff run the
risk of making assumptions from the local media with no substantial truth. This may run the risk of staff self-deploying to the location, inappropriately contacting the ACH for information and/or to offer overtime duties. To map these offers of availability can not effectively be captured in the ACH during an incident, and consideration needs to made at a Gold level of when and where to draft in extra staff.
14.2.4 To mitigate the desire for staff to contact ACH, and also as an emergency
‘call-out‘ process all operational and support staff have been invited to express permission to be contacted and supply the Trust with their contact details. These details will be held on a database owned by the Resilience Unit.
14.2.5 Using the relevant electronic / web based system these staff can be
contacted via SMS, Pager and Email to advise of an incident, and to reiterate the importance of not self-deploying and to not make contact into the ACH.
14.2.6 The staff, if available, can return a message by either leaving an answer-
phone message on a dedicated phone line or text availability details which will then be sent to an email inbox that can be picked up at a later stage.
14.2.7 The answer-phone message bank and text message inbox will need to be
periodically monitored and a comprehensive database kept. Administration staff can manage this at the request of Gold or Silver commanders when reviewing available resources.
14.2.8 The communications team will update the staff intranet with appropriate
details about an incident, with any other information the trust requires to bring to the attention of staff. The team will also use the full range of internal communication tools including special bulletins as appropriate.
14.2.9 Any further messages / briefings will be authorised by commanders and
issue by the communications team.
CC COO O
MM MMM M
UU UNN N
II I CC CAA A
TT TII I OO O
NN NSS S
&& & MM M
EE EDD D
II I AA A

59
15. POST INCIDENT PROCEDURES 15.1 Debriefing
15.1.1 Commanders need to give early consideration for how debriefs at every
level will be conducted, from hot debriefs amongst teams to more formal structured debriefs in line with the Trusts debriefing protocol.
15.1.2 Immediately following a Major Incident a Hot Debrief should be conducted.
The aim of this is to identify any major gaps in response and also allows those involved to offload any issues or concerns. This hot debrief will be lead by the Silver Commander.
15.1.3 Formal debriefs are essential following any Major Incident. They identify
areas which went well, and areas for improvement. As such, anyone who is assigned an Action Card MUST submit a report and attend debriefs as required. Because operational pressures are unavoidable and on must take priority, SWASFT will make debriefs as accessible as possible using electronic means where possible. All debrief reports will be circulated to the Board for information and action where required, and will detail attendance.
15.1.4 It can be expected that the events preceding and the response to a Major
Incident may be subject to a later public enquiry. In anticipation of this it is vital that all communications are timed/dated and retained with justification for action included. If the response to an incident is protracted, timed and dated position summaries are helpful.
15.1.5 Any Trust declared major incidents will be reviewed in line with the Trusts
Incident reporting arrangements and a datix should be submitted. 15.2 Re-Supply
15.2.1 All SWASFT resources that have utilised equipment, consumables and
drugs will need to be brought back to normal operational standard as soon as possible. Any lost or faulty equipment must also be reported and logged as per normal operating procedures.
15.3 Staff Welfare
15.3.1 Any major incident will invariably expose members of Trust staff to sights,
sounds and environments which may be traumatic and difficult. The organisation has a responsibility to ensure the welfare of staff during and following the incident.
15.3.2 At the conclusion of the incident critical incident defusing and ‘buddying‘
would be appropriate, a clear strategy developed for TRIM and support to individuals. This should be drawn up in conjunction with Occupational Health and if appropriate other NHS providers.
PP POO O
SS STT T
II I NN NCC C
II I DD DEE E
NN NTT T

60
NB: Action Cards are personally issued to Commanders and are available on all A&E vehicles, so are not held within the plan. Action cards are also available within each Clinical Hub and Incident Coordination Centre.
AA ANN N
NN NEE E
XX X AA A
–– – AA A
CC CTT T
II I OO ONN N
CC CAA A
RR RDD D
SS S

61
PROCEDURES
Relevant plans and top-level documents linked to this Major Incident Plan include, but are not necessarily restricted to those detailed below, and are available either in hard copy or in e-format via the SWASFT Resilience Department or N-ILO.They may be available in e-format via the Local Resilience Fora. Al the plans listed below can be found on the SWASFT Commander iPad ‘App’. If you would like to download this please contact the Resilience Unit.
Cabinet Office EPRR Guidance
DH Published Guidance
HPA Guidance
NHS Commissioning
Board Guidance Key
:
NARU / National Ambulance Document
SWASFT Plan LRF Plan Multi-agency Site Specific Plan
CBRNe Plan
Capacity Management Plan
Active Shooter & MTFA Plan
Severe Weather Plan
Incidents Involving Aircraft
Incidents Involving Aircraft
Mass Casualty Incident Plan
HART SOPs
CBRN & SORT SOPs
Trust Mutual Aid Plan
HART Mutual Aid Plan
ACH Fall Back Plan
Small Pox Plan
Service Disruption Plan
Pandemic Influenza Plan
Bath Rugby Plan
Bristol Rovers Plan
Bristol City FC Plan
Swindon Town Plan
AACE Mutual Aid MoU
Threat Status and Escalation Plan
Command Policy
AACE Command and Control Guidance
NARU CBRNe Guidance
HART Service Specification
Bristol (Model Response) Site Specific Plan
Severn Tunnel Site Specific Plan
Hinckley Point (A&B) Site Specific Plan
Oldbury Power Station Site Specific Plan
Severnside Site Specific Plan
AA ANN N
NN NEE E
XX X BB B
–– – PP P
LL LAA A
NN NSS S
AA ANN N
DD D PP P
RR ROO O
CC CEE E
DD DUU U
RR REE E
SS S
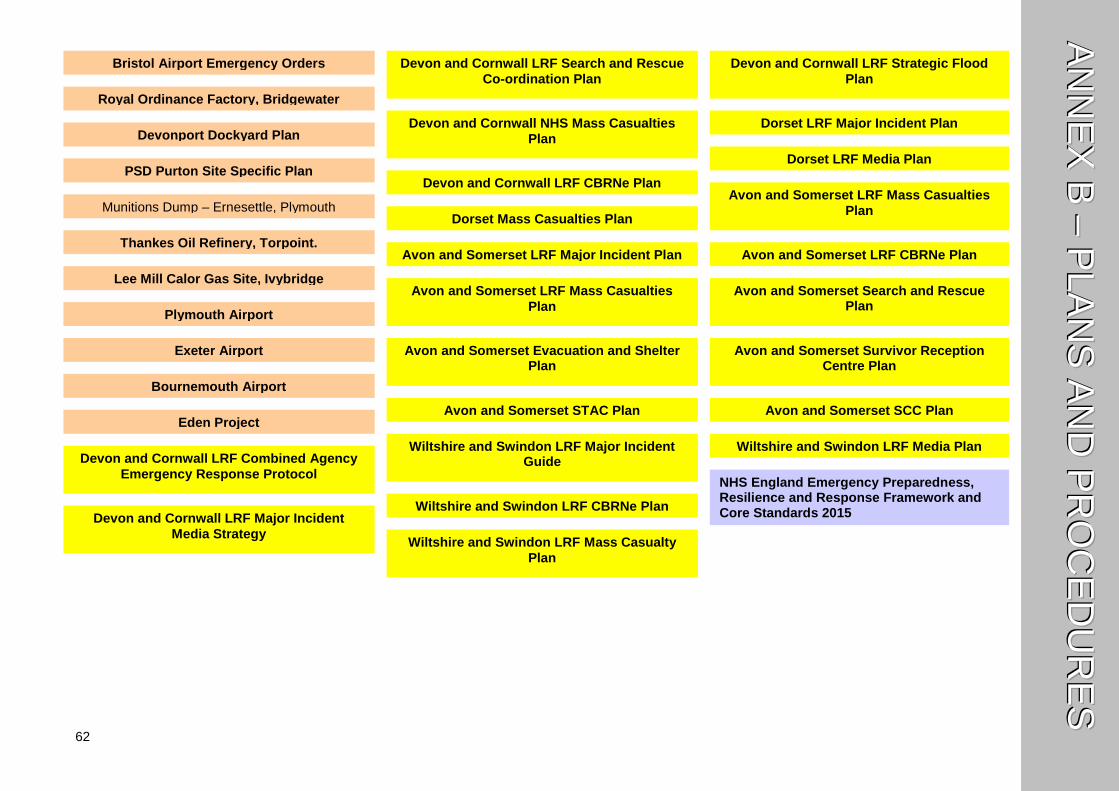
62
Bristol Airport Emergency Orders
AA ANN N
NN NEE E
XX X BB B
–– – PP P
LL LAA A
NN NSS S
AA ANN N
DD D PP P
RR ROO O
CC CEE E
DD DUU U
RR REE E
SS S
Royal Ordinance Factory, Bridgewater
Devonport Dockyard Plan
PSD Purton Site Specific Plan
Munitions Dump – Ernesettle, Plymouth
Thankes Oil Refinery, Torpoint.
Lee Mill Calor Gas Site, Ivybridge
Plymouth Airport
Bournemouth Airport
Exeter Airport
Eden Project
Devon and Cornwall LRF Combined Agency
Emergency Response Protocol
Devon and Cornwall LRF Major Incident
Media Strategy
Devon and Cornwall LRF Search and Rescue
Co-ordination Plan
Devon and Cornwall LRF Strategic Flood
Plan
Devon and Cornwall NHS Mass Casualties
Plan
Devon and Cornwall LRF CBRNe Plan
Dorset LRF Major Incident Plan
Dorset LRF Media Plan
Dorset Mass Casualties Plan
Avon and Somerset LRF Mass Casualties
Plan
Avon and Somerset LRF Major Incident Plan
Avon and Somerset LRF Mass Casualties
Plan
Avon and Somerset LRF CBRNe Plan
Avon and Somerset Search and Rescue Plan
Avon and Somerset Evacuation and Shelter Plan
Avon and Somerset Survivor Reception Centre Plan
Avon and Somerset STAC Plan
Avon and Somerset SCC Plan
Wiltshire and Swindon LRF Major Incident Guide
Wiltshire and Swindon LRF CBRNe Plan
Wiltshire and Swindon LRF Mass Casualty
Plan
Wiltshire and Swindon LRF Media Plan
NHS England Emergency Preparedness, Resilience and Response Framework and Core Standards 2015
63
NHS England Command and Control Framework Note: supersedes the Strategic command arrangements for the NHS during a major incident (Dec ‘07) from 1 April 2013
AA ANN N
NN NEE E
XX X BB B
–– – PP P
LL LAA A
NN NSS S
AA ANN N
DD D PP P
RR ROO O
CC CEE E
DD DUU U
RR REE E
SS S
NHS England Business Continuity Management Framework (service resilience) (2013)
BSI, PAS 2015:2010 Framework for health services resilience (NHS version of BSI/ISO) ISO 22301 business continuity
management system (BCMS)
Cabinet Office: Emergency Preparedness, Guidance on Part 1 of the Civil Contingencies Act 2004, its associated Regulations and non-statutory arrangement (March 2012)
Cabinet Office Emergency Response and Recovery (July 2012)
Cabinet Office: Lexicon of UK Civil Protection Terminology
Cabinet Office: Provision of Scientific and Technical Advice in the Strategic Co-Ordination Centre (STAC) - Guidance to Local Responders (April ’07)
Cabinet Office: A strategic framework for the Scientific Advisory Group for Emergencies (SAGE) (Oct’12)
Cabinet Office Formal Information Sharing Under the Civil Contingencies Act 2004 (Chapter 3,
DH: NHS Guidance - Incidents Involving Radioactivity (’98)
HPA: CBRN Incidents: A Guide to Clinical Management and Health Protection (Sep ‘08)
DH: Ambulance service guidance on dealing with radiological incidents and emergencies (Mar ‘10)
DH: Emergency planning - UK reserve national stock for major incidents - how to access stock (Feb’10)
DH: Trauma Network: Regional Network for Major Trauma (September 2010)
DH: Trauma Network: Management of Children with Major Trauma (February 2011)
DH: Mass casualties incidents: a framework for planning (Mar ‘07)
DH: Planning for the management of burn-injured patients in the event of a major incident: interim strategic national guidance (Apr ‘11)
DH: Planning for the management of blast injured patients (Dec’07)
DH: Development & Deployment of Medical Emergency Response Incident Teams (MERIT) in the provision of advanced medical care at the scene of an incident (Mar ‘10)
DH: Immediate Medical Care at the scene of a major incident (Oct ‘05)

64
AA ANN N
NN NEE E
XX X CC C
–– – HH H
OO OSS S
PP PII I TT T
AA ALL L
BB BEE E
DD D SS S
TT TAA A
TT TEE E
FF FOO O
RR RMM M

65
SOUTH WESTERN AMBULANCE SERVICE NHS TRUST MAJOR INCIDENT – ACUTE HOSPITAL BEDSTATE
One per hospital and to be faxed to the Ambulance Control Room (Compiled by ACH/Hospital Ambulance Liaison Officer)
HOSPITAL: DATE:
BEDS CURRENTLY AVAILABLE AT _________ : __________ hrs (time is 24-hour clock)
CAPACITY Emergency Dept
(space for casualties & beds)
Critical Care ICU & HDU
Neuro surgery
Coronary Care
Surgical Specialities
Medical Specialities
Paediatric P3s
Now
Majors Minors Obs beds
ICU/HDU Ward Beds
In 1 hour (anticipated)
In 4 hours (anticipated)
Please do not leave any column blank – insert ‘N/A’ if not applicable SUBMITTED BY:
NAME (please print) SIGNATURE
CONTROL ROOM TEL NUMBER
CONTROL ROOM FAX NUMBER

66
AA ANN N
NN NEE E
XX X DD D
–– – CC C
.. . OO OPP P
.. . TT TEE E
MM MPP P
LL LAA A
TT TEE E

67
ANNEX D – TEMPLATE COMMON OPERATING PICTURE (COP)
INCIDENT LOCATION
CRIP Number CAD LOG
DATE TIME (24hr)
COMPLETED BY ROLE
TRUST COMMAND TIER
STRATEGIC COMMANDER NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
ON CALL DIRECTOR NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
STRATEGIC ADVISOR NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
STRATEGIC CO-ORDINATING GROUP LIAISON OFFICER (AVON AND SOMERSET) NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
STRATEGIC CO-ORDINATING GROUP LIAISON OFFICER (DEVON AND CORNWALL) NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
TRUST COMMAND TIER STRATEGIC CO-ORDINATING GROUP LIAISON OFFICER (DORSET)
NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
OFFICIAL / OFFICIAL SENSITIVE (DELETE AS APPRORIATE)

68
ANNEX D – TEMPLATE COMMON OPERATING PICTURE (COP)
STRATEGIC CO-ORDINATING GROUP LIAISON OFFICER (WILTSHIRE AND SWINDON)
NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
STRATEGIC CO-ORDINATING GROUP LIAISON OFFICER (GLOUCESTERSHIRE) NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
STRATEGIC MEDICAL ADVISOR NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
TACTICAL / COMMANDER NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
TACTICAL ADVISOR NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
NATIONAL INTER-AGENCY LIAISON OFFICER (N-ILO) NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
RADIATION PROTECTION SUPERVISOR NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
MEDICAL INCIDENT ADVISOR NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
OPERATIONAL COMMANDER NAME LANDLINE MOBILE EMAIL ISSI SECURE CONTACT
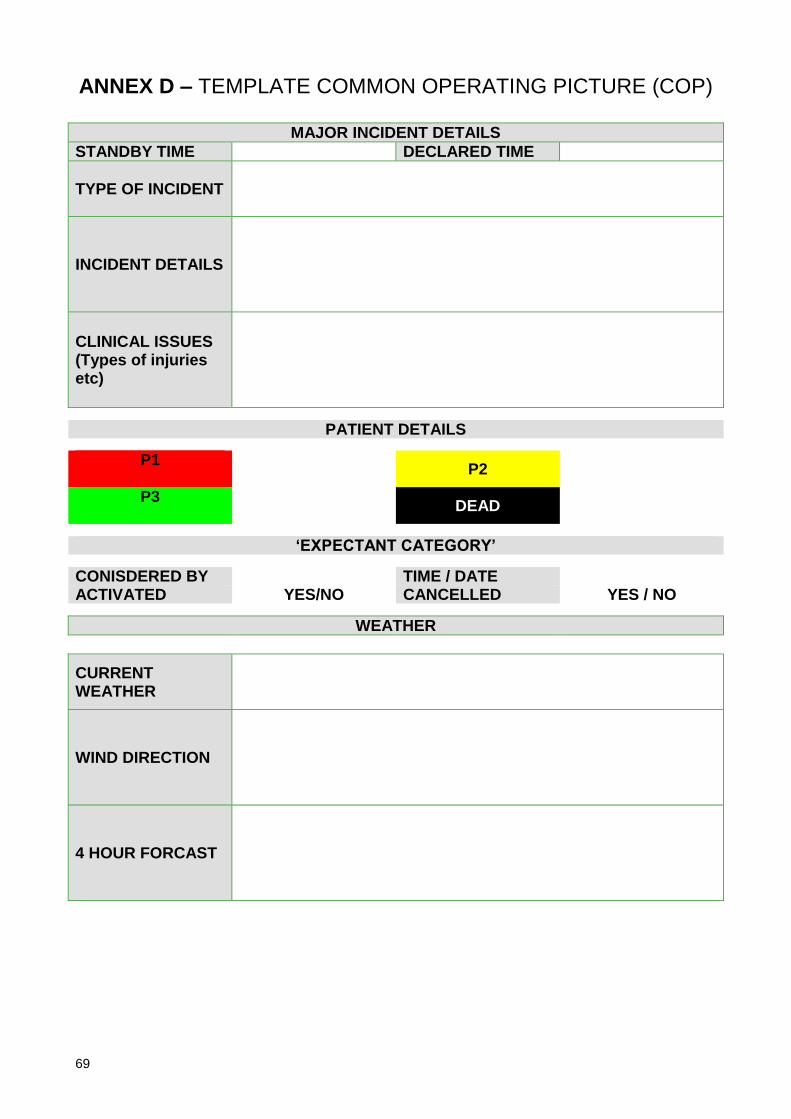
69
ANNEX D – TEMPLATE COMMON OPERATING PICTURE (COP)
MAJOR INCIDENT DETAILS
STANDBY TIME DECLARED TIME
TYPE OF INCIDENT
INCIDENT DETAILS
CLINICAL ISSUES (Types of injuries etc)
PATIENT DETAILS
P1
P2
P3
DEAD
‘EXPECTANT CATEGORY’
CONISDERED BY TIME / DATE ACTIVATED YES/NO CANCELLED YES / NO
WEATHER
CURRENT WEATHER
WIND DIRECTION
4 HOUR FORCAST
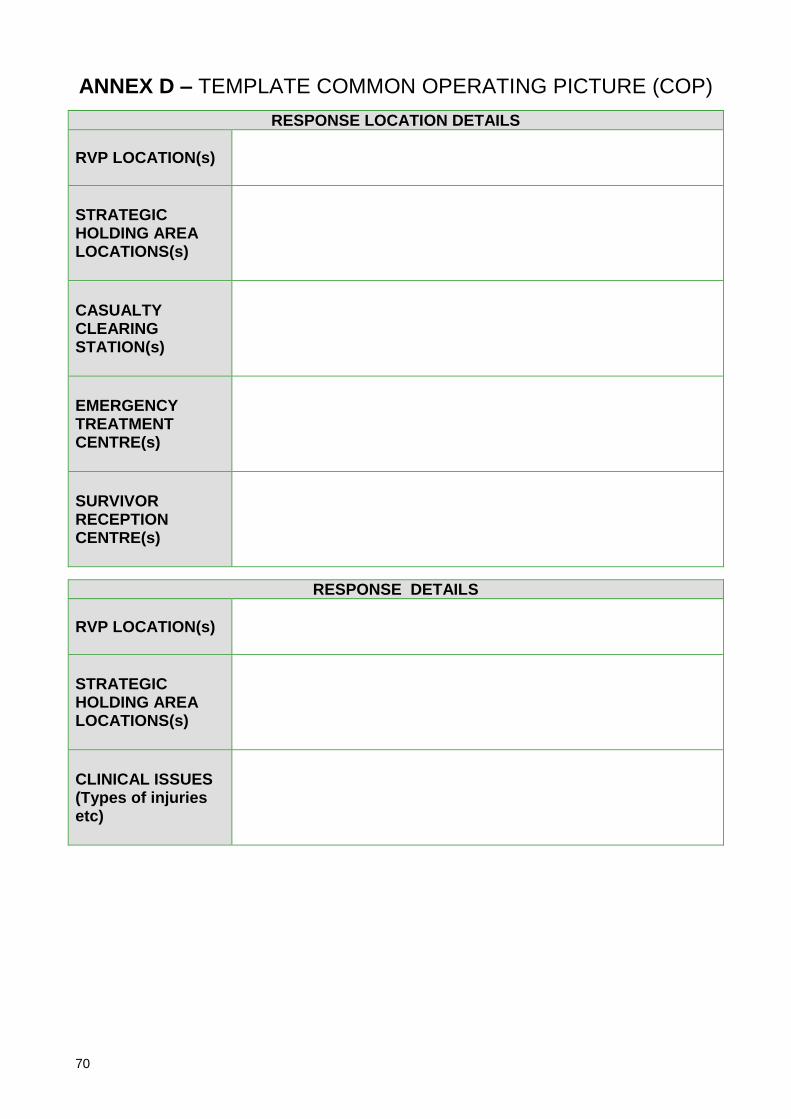
70
ANNEX D – TEMPLATE COMMON OPERATING PICTURE (COP)
RESPONSE LOCATION DETAILS
RVP LOCATION(s)
STRATEGIC HOLDING AREA LOCATIONS(s)
CASUALTY CLEARING STATION(s)
EMERGENCY TREATMENT CENTRE(s)
SURVIVOR RECEPTION CENTRE(s)
RESPONSE DETAILS
RVP LOCATION(s)
STRATEGIC HOLDING AREA LOCATIONS(s)
CLINICAL ISSUES (Types of injuries etc)

71
RECIEVING HOSPITAL CAPACITY NOW
EM
ER
GE
NC
Y
DE
PT
CR
ITIC
AL
CA
RE
/HD
U
NE
UR
O
PA
ED
IAT
RIC
BU
RN
S
P3
OT
HE
R
EM
ER
GE
NC
Y
DE
PT
CR
ITIC
AL
CA
RE
/HD
U
NE
UR
O
PE
AD
IAT
RIC
BU
RN
S
P3
OT
HE
R
Gloucester Royal
Cheltenham General
North Bristol
University Hospitals Bristol
Weston General
Musgrove Park
Yeovil District
RUH Bath
Great Western Hospital
Salisbury District
Dorset County
Poole General
Royal Devon and Exeter
North Devon District
Torbay
Royal Cornwall
Derriford
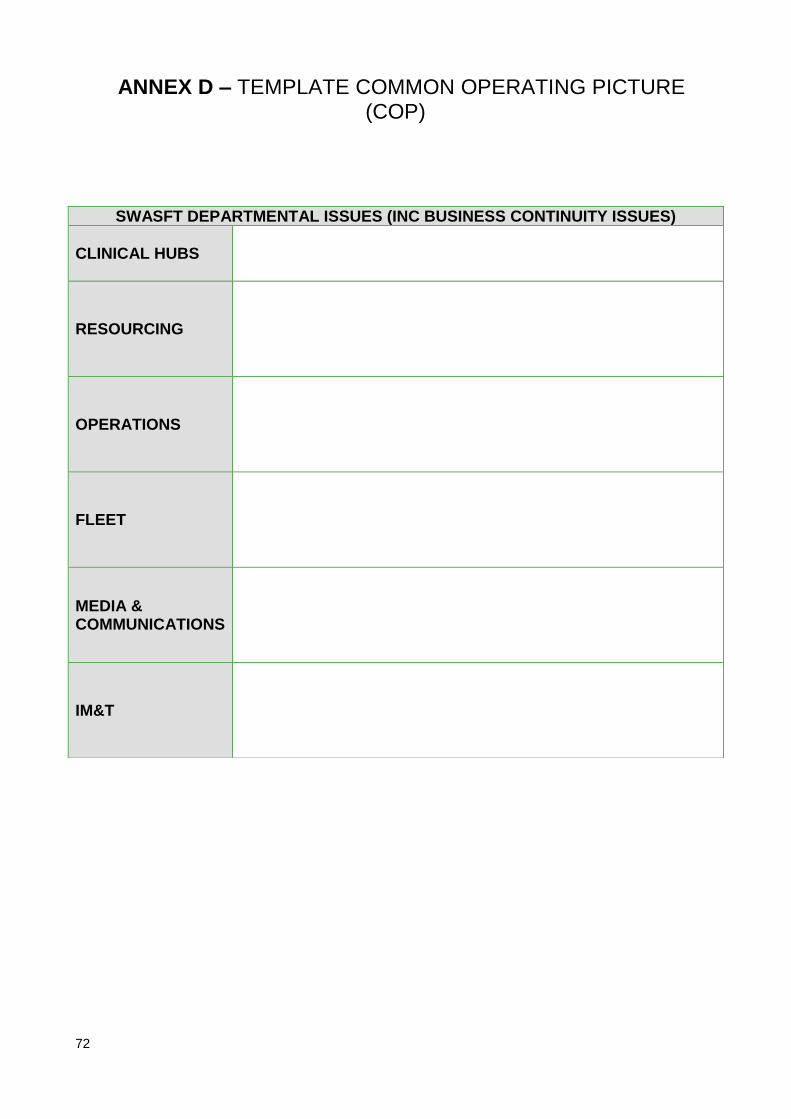
72
ANNEX D – TEMPLATE COMMON OPERATING PICTURE (COP)
SWASFT DEPARTMENTAL ISSUES (INC BUSINESS CONTINUITY ISSUES)
CLINICAL HUBS
RESOURCING
OPERATIONS
FLEET
MEDIA & COMMUNICATIONS
IM&T

73
ANNEX E. TRUST STRATEGIC INTENT
It is our intention to deal with any incident in an appropriate manner which promotes and saves life, reduces humanitarian suffering and is compatible with the vision and values of South Western Ambulance Service NHS Foundation Trust. Through effective co-ordination, sound planning and good leadership the Gold Commander will:
Maintain public confidence and minimise the impact of any occurrence by ensuring that SWASFT are responding rapidly and effectively to the event and / or incident;
Ensure that the SWASFT response is co-ordinated and integrated with the wider health and other responding agencies where applicable;
Ensure that the SWASFT response is co-ordinated and integrated with the other responding agencies where applicable;
Maintain effective capacity management within the Accident and Emergency Service, Emergency Operations Centres and Planned Care Services;
Assess and identify any gaps in the response capability of the organisation for dealing any incident;
Through the identification and use of mutual aid, minimise the impact on the Emergency Operations Centre, and normal operational functions;
So far as is reasonably practicable, take all measures to safeguard the following people under the terms of health and safety legislation;
o SWASFT staff and other responders; o Local communities;
Ensure public messages are co-coordinated with other agencies and partners and maintain a positive reputation for the trust;
Provide support and representation at the strategic coordination centre (SCG) where appropriate;
Create and maintain a well documented, auditable plan and decision log for the event and / or incident at all levels of command.
.
AA ANN N
NN NEE E
XX X EE E
–– – GG G
OO OLL L
DD D SS S
TT TRR R
AA ATT T
EE EGG G
YY Y

74
ANNEX F. REFERENCES
1. ACPO. (2009) Emergency Procedures. [Online]
http://www.npia.police.uk/en/6533.htm
2. Cabinet Office. (2011) Emergency Response and Recovery. [Online]
http://ukresilience.info/preparedness/ccact/eppdfs.aspx
3. Cabinet Office. (2011) Emergency Preparedness. [Online]
http://ukresilience.info/preparedness/ccact/eppdfs.aspx
4. Coles, E et al.. (2006) Health Emergency Planning: A handbook for
practitioners. [2nd Ed] London: Stationary Office.
5. Department of Health. (2005) NHS Emergency Planning Guidance. [Online]
http://www.dh.gov.uk/en/Publicationsandstatistics
/Publications/PublicationsPolicyAndGuidance/DH_4121072
6. NHS England EPRR Framework and Core Standards 2015
https://www.england.nhs.uk/ourwork/eprr/
AA ANN N
NN NEE E
XX X FF F
–– – RR R
EE EFF F
EE ERR R
EE ENN N
CC CEE E
SS S
AA ANN N
NN NEE E
XX X FF F
–– – RR R
EE EFF F
EE ERR R
EE ENN N
CC CEE E
SS S

75
EQUIPMENT SUPPORT UNITS
VEHICLE PURPOSE
To be deployed as a ‘first strike’ for all major and mass casualty incidents. These vehicle’s are scaled for 100 patients (25 P1, 25P2 and 50 P3)
EQUIPMENT CARRIED (INDICATIVE)
Paramedic Bags (4) Dressing Bags (10)
Casualty Clearing Bag (1) ‘Self Help Packs’
Stretchers Medium Sized Inflatable Tents
Tripod Lighting Units Mass Oxygen Unit
AA ANN N
NN NEE E
XX X GG G
–– – VV V
EE EHH H
II I CC CLL L
EE ESS S
AA ANN N
DD D EE E
QQ QUU U
II I PP PMM M
EE ENN N
TT T

76
MASS CASUALTY VEHICLES
VEHICLE PURPOSE
There are 24 Mass Casualty Vehicles strategically located across the UK. Four of which are located within SWASFT. These may be deployed to any incident across the UK at the request of the NACC. These should also be sent to any major or mass casualty incident within the South West and principally contains Paramedical and Casualty Clearing supplies for 100 patients (80 adults and 20 Peadiatrics)
EQUIPMENT CARRIED (INDICATIVE)
80 x Adult Paramedic Treatment Packs
20 x Paediatric Paramedic Treatment
Packs
Pain Relief and Anesthetic Drugs Mass Oxygen
Emergency Dressings Pack Amputation Equipment
Casualty Clearing Clinical Equipment
AA ANN N
NN NEE E
XX X GG G
–– – VV V
EE EHH H
II I CC CLL L
EE ESS S
AA ANN N
DD D EE E
QQ QUU U
II I PP PMM M
EE ENN N
TT T

77
INCIDENT SUPPORT UNITS (LOGISTICS & CBRNE)
VEHICLE PURPOSE
These vehicles are designed to provide all necessary equipment to support an incident scene. Specifically it provides all necessary equipment to establish a Clinical Decontamination Unit or a Casualty Clearing Station (CCS).
EQUIPMENT CARRIED (INDICATIVE)
TM 36 and TM 18 Tent Scene Signage
Lighting Decontamination
Accessories
PRPS Mass Oxygen
Heating Limited Clinical Equipment
AA ANN N
NN NEE E
XX X GG G
–– – VV V
EE EHH H
II I CC CLL L
EE ESS S
AA ANN N
DD D EE E
QQ QUU U
II I PP PMM M
EE ENN N
TT T

78
EXTENDED CASUALTY CLEARING (LOGISTICS)
VEHICLE PURPOSE
This vehicle is designed to provide the necessary logistics and limited clinical equipment to manage a large casualty clearing station. This vehicle should be deployed alongside the Extended Casualty Clearing Vehicle (Clinical).
EQUIPMENT CARRIED (INDICATIVE)
Stretchers Wheel / Carry Chairs
Drip Stands Blankets and Pillows
Tables, chairs and screens Limited Treatment Equipment
Casualty Clearing Clinical Equipment
Generators
Heaters
AA ANN N
NN NEE E
XX X GG G
–– – VV V
EE EHH H
II I CC CLL L
EE ESS S
AA ANN N
DD D EE E
QQ QUU U
II I PP PMM M
EE ENN N
TT T

79
EMERGENCY DRESSINGS PACKS (EDP)
PURPOSE
Emergency Dressing Packs, each equipped with sufficient haemorrhage control and burns supplies for mass casualties are located at major transport hubs and crowded places. The equipment is designed for ‘self help’ and ‘lay responders’.
EQUIPMENT CARRIED 400 Mixed Size Dressings Kling Film Paramedic Shears
LOCATIONS
Bristol Temple Meads Station Bristol Parkway Station
Weston-Super-Mare Station Bath Spa Station
Swindon Rail Station Cabot Circus (Bristol)
Westbury Rail Station Cheltenham Rail Station
Paulton Walk In Centre Gloucester Rail Station
Bristol Airport (x3) The Mall at Cribbs Causeway
Sedgemoor Services (North) Sedgemoor Services (South)
Bridgewater Services Taunton Deane Services
Cullompton Services Exeter Services
Eden Project Weymouth Rail Station
Bournemouth Rail Station Dolphin Shopping Centre
Castlepoint Shopping Centre Weymouth Debenhams
Poole Ferry Terminal Princesshay Shopping Centre
Weymouth Ferry Terminal Drakes Circus Shopping Centre
Plymouth Ferry Terminal Tiverton Services
Bournemouth Airport Exeter St Davids Rail Station
Newquay Airport Newton Abbot Rail Station
Penzance Rail Station Plymouth Rail Station
Totnes Rail Station Taunton Rail Station
AA ANN N
NN NEE E
XX X GG G
–– – VV V
EE EHH H
II I CC CLL L
EE ESS S
AA ANN N
DD D EE E
QQ QUU U
II I PP PMM M
EE ENN N
TT T

80
AMBULANCE MOBILE COMMAND UNITS
VEHICLE PURPOSE
The MCU should be sent to scene. The purpose of the MCU is to manage communications on scene and provide all the necessary infrastructure commanders require e.g. IT, interactive whiteboards, cameras, briefing areas etc.
On arrival at the scene, the MCU will position itself inside the outer cordon, adjacent to the other emergency services Command Units and positioned to ensure good radio communications on and off-site. Normally a separation of 10 metres between control vehicles is ideal.
VEHICLE LOCATIONS
Filton (North Bristol)
EQUIPMENT CARRIED (INDICATIVE)
CAD Access Lighting
Cameras Command Meeting Facility
Tetra Sets
AA ANN N
NN NEE E
XX X GG G
–– – VV V
EE EHH H
II I CC CLL L
EE ESS S
AA ANN N
DD D EE E
QQ QUU U
II I PP PMM M
EE ENN N
TT T