long-term neurological implications of somnolence syndrome in children with acute lymphocytic...
TRANSCRIPT
Long-Term Neurologcal Implications of Somnolence Syndrome in Chddren
with Acute Lymphocytic Leukemia Lawrence T. Ch’ien, MD, Rhomes J. A. Aur, MD, Shirley Stagner, RN, PNP, Katie Cavallo, Adynel Wood, RN, PNP, John Goff, PhD, Samuel Pitner, MD,
H. Omar Hustu, MD, M. J. Seifert, MS, and Joseph V. Simone, MD
A longitudinal study of 49 children with acute lymphocytic leukemia (ALL) assessed the long-term effects of central nervous system (CNS) prophylaxis on brain function. From 10 to 12 electroencephalograms (EEGs) were done before and at intervals during and after 30 months of treatment that included 2,400 rads of CNS irradiation plus intrathecal methotrexate therapy. None of the children had CNS leukemia, and all remained in first complete remissions. All 4 9 had abnormally slow EEG background frequencies during the four-year study, and 29 (60%) developed somnolence syndrome six to eight weeks after CNS prophylaxis. During this syndrome, EEG background frequencies decreased more than 3 standard deviations below the expected mean values for normal children. There- after, 7 of the 29 began to show signs of learning disabilities and 7 developed recurrent seizures. Of the 20 children who did not have the syndrome, none showed later evidence of CNS dysfunction. Somnolence may be an early indicator of long-term neurological sequelae after cranial irradiation.
Ch’ien LT, Aur RJA, Stagner S, et al: Long-term neurological implications of somnolence syndrome in children with acute lymphocytic leukemia. Ann Neurol 8:273-277, 1980
The current therapy for childhood acute lymphocytic leukemia (ALL) provides cure in over one-third of the patients [ 111. A large measure of this success can be attributed to prevention of leukemia relapse in the central nervous system (CNS) by prophylactic cranial irradiation and the simultaneous administration of intrathecal methotrexate L141. In 1972 we initiated a prospective study [21 to monitor brain function in all children who would be receiving CNS prophylaxis.
When that study began, little was known about the effects of combined chemotherapy and cranial irradi- ation on CNS functions in children with ALL. Al- though subtle neurological dysfunction and structural changes have recently been described in children re- ceiving cranial prophylaxis, the long-term implica- tions of postirradiation somnolence syndrome were unclear.
With increasing numbers of children surviving dis- ease free for extended periods, we were able to eval- uate long-term possibly therapy related neurological sequelae. This paper reports the results of serial noninvasive assessments of CNS function in children surviving more than four years after the initial diag- nosis of ALL. and describes several risk factors that may be related to CNS dysfunction.
Patients and Methods From August, 1972, to December, l 9 7 4 , 2 11 children with ALL who were consecutively admitted to St. Jude Chil- dren’s Research Hospital entered this study if they met certain criteria: ( 1 ) received antileukemia treatment ac- cording to the protocol for Total Therapy Study VIII r2]; ( 2 ) attained bone marrow remission within the first eight weeks of therapy; and (3) did not have CNS leukemia at diagnosis or early CNS relapse (either condition would have required additional CNS irradiation, with or without intrathecal methotrexate therapy). Of the 2 11 patients en- tering the study, only 49 met the criteria for long-term sur- vival without evidence of leukemia. The remaining 162 pa- tients were excluded for multiple reasons, e.g., young age, early relapses, and deaths in remission during therapy [2].
Each child in the study underwent serial neurological examinations and cranial computed tomography (CT). Neuropsychological evaluations were performed for selected patients with evidence of neurological dysfunc- tion. Children remained in the study as long as: (1) they had no clinical evidence of CNS leukemia and no lymphoblasts in the cerebrospinal fluid (CSF); and (2) they kept ap- pointments for at least 10 of the 12 electroencephalograms (EEGs) scheduled over a four-year period.
Therapy Details of the three phases of therapy in protocol Study VIII for children with ALL have been reported [ 2 ] . Ther-
From the Sections of Neurology, Hematology-Oncology, Neu- ropsychology, and Radiotherapy, St. Jude Children’s Research Hospital, Memphis, TN. Received Dec 3, 1979. Accepted for publication Jan 7, 1980.
Address reprint requests to Lawrence T. Chien, MD, Section of Neurology, St. Jude Children’s Research Hospital, 332 N Lauder- dale, PO Box 318, Memphis, TN 38101.
0364-5134/80/090273-05$01.25 @ 1979 by Lawrence T. Ch’ien 273
apy to induce remission was started shortly after diagnosis and included daily prednisone, weekly intravenous vincris- tine, and two doses of asparaginase at one-week intervals. Patients who failed to attain bone marrow remission after four weeks of therapy were given daunorubicin and predni- sone for two to four weeks.
The second (18-day) phase of therapy, directed to the CNS, consisted of 2,400 rads of cranial irradiation plus five doses of intrathecal methotrexate (12 mglm2). Children less than 2 years old received a reduced total dose of cranial irradiation (2,000 rads for those 1 to 2 years old, 1,500 rad for those less than 1 year old).
The third phase (continuation chemotherapy) was started one week after completion of CNS therapy. All patients were randomized by the card-envelope technique to re- ceive one-, two-, three-, or four-drug therapy. Group 1 received methotrexate only; Group 2 received 6-mer- captopurine with methouexate; Group 3 received cyclo- phosphamide as well; and Group 4 received all three drugs plus arabinosyl cytosine. All therapy was discon- tinued after 30 months of continuous complete remission.
WEEKS
I I I I I I I I I I I I I I I I I I
Neurological Egalzration Complete neurological examinations were done before therapy for leukemia was started, and they were repeated when clinical evidence of neurological dysfunction was found. CT scanning was later added to the test battery for selected patients with neurological or psychological ab- normalities or a history of seizures.
Children with behavior disorders, school problems, o r neurological dysfunction were evaluated by the Halstead- Reitan method. This technique of neuropsychological evaluation has been fully described previously (Goff J, An- derson JR, Powazek M, Marten GW: Distractibility and memory deficits in long term survivors of acute lympho- blastic leukemia. Submitted for publication).
EEGs were recorded with a Grass Model 6 ten-channel electroencephalograph. We used a variety of referential and bipolar montages with electrode placement according to the international 10-20 system. At least 20 minutes of recording were obtained while the child was asleep and awake; the child's alertness during the awake recordings was maintained by periodically asking questions. To avoid hypoglycemia, a common cause of slow cerebral electrical activity, we gave the children food and drinks within 2 hours before the recording was made.
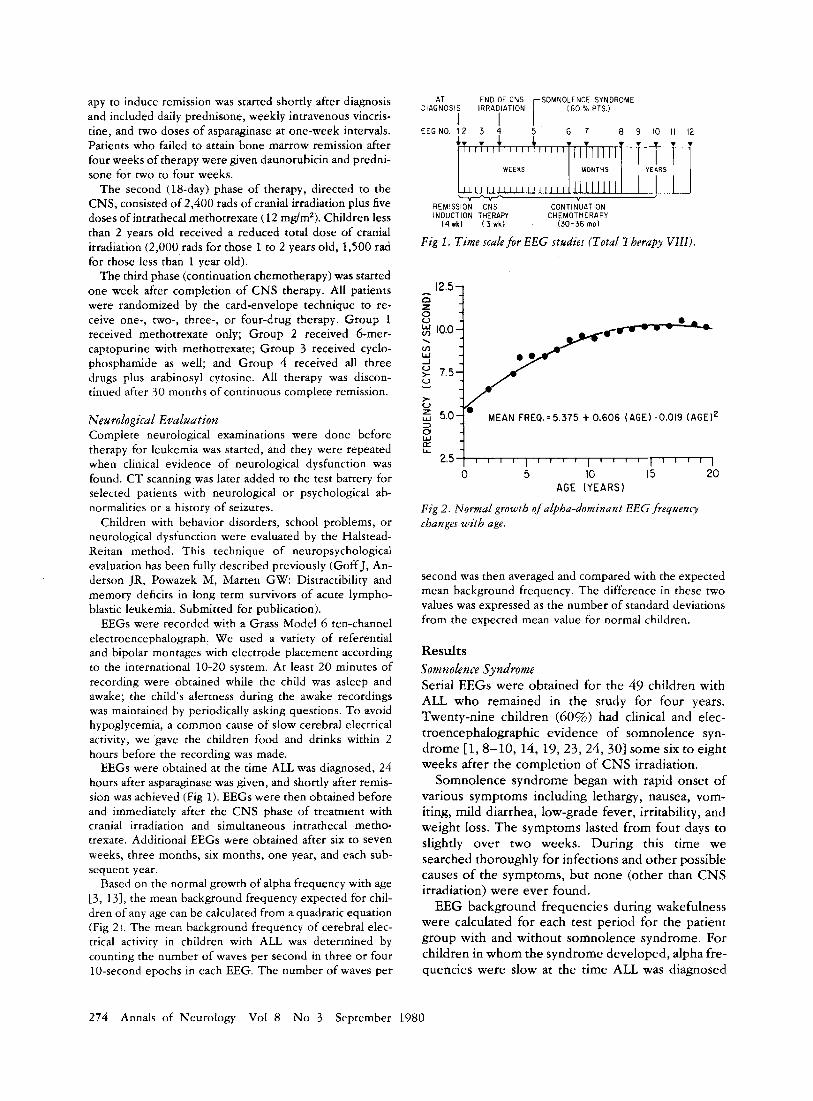
EEGs were obtained at the time ALL was diagnosed, 24 hours after asparaginase was given, and shortly after remis- sion was achieved (Fig 1). EEGs were then obtained before and immediately after the CNS phase of treatment with cranial irradiation and simultaneous intrathecal metho- trexate. Additional EEGs were obtained after six to seven weeks, three months, six months, one year, and each sub- sequent year.
Based on the normal growth of alpha frequency with age [3 , 131, the mean background frequency expected for chil- dren of any age can be calculated from a quadratic equation (Fig 2). The mean background frequency of cerebral elec- trical activity in children with ALL was determined by counting the number of waves per second in three or four 10-second epochs in each EEG. The number of waves per
. . MONTHS YEARS
I I t
E N 0 OF CNS SOMNOLENCE SYNDROME I60 PTS.) r AT
DIAGNOSIS IRRADIATION
EEGNO. 12 3 4 5 6 7 8 9 10 II 12 I I
- w L a
2.5 1 r i I i r r r 1 r r r r I i I 1 1 I
E '7 g 10.0 " i .
k 5Or M E A N FREGk.5.375 t 0.606 ( A G E ) - 0 . 0 1 9 (AGE] ' 3 0
second was then averaged and compared with the expected mean background frequency. The difference in these two values was expressed as the number of standard deviations from the expected mean value for normal children.
Results Somnolence Syndrome Serial EEGs were obtained for the 49 children with ALL. who remained in the study for four years. Twenty-nine children (60%) had clinical and elec- troencephalographic evidence of somnolence syn- drome [l, 8-10, 14, 19, 23,24,301 some six to eight weeks after the completion of CNS irradiation.
Somnolence syndrome began with rapid onset of various symptoms including lethargy, nausea, vom- iting, mild diarrhea, low-grade fever, irritability, and weight loss. The symptoms lasted from four days to slightly over two weeks. During this time we searched thoroughly for infections and other possible causes of the symptoms, but none (other than CNS irradiation) were ever found.
EEG background frequencies during wakefulness were calculated for each test period for the patient group with and without somnolence syndrome. For children in whom the syndrome developed, alpha fre- quencies were slow at the time A U was diagnosed
274 Annals of Neurology Vol 8 No 3 September 1980
Signs of CNS Damage dfter Craniul Irradiation
-4 4 ; : ; Li ; 9 11, 1'1 :2 SERIAL EEG NUMBER
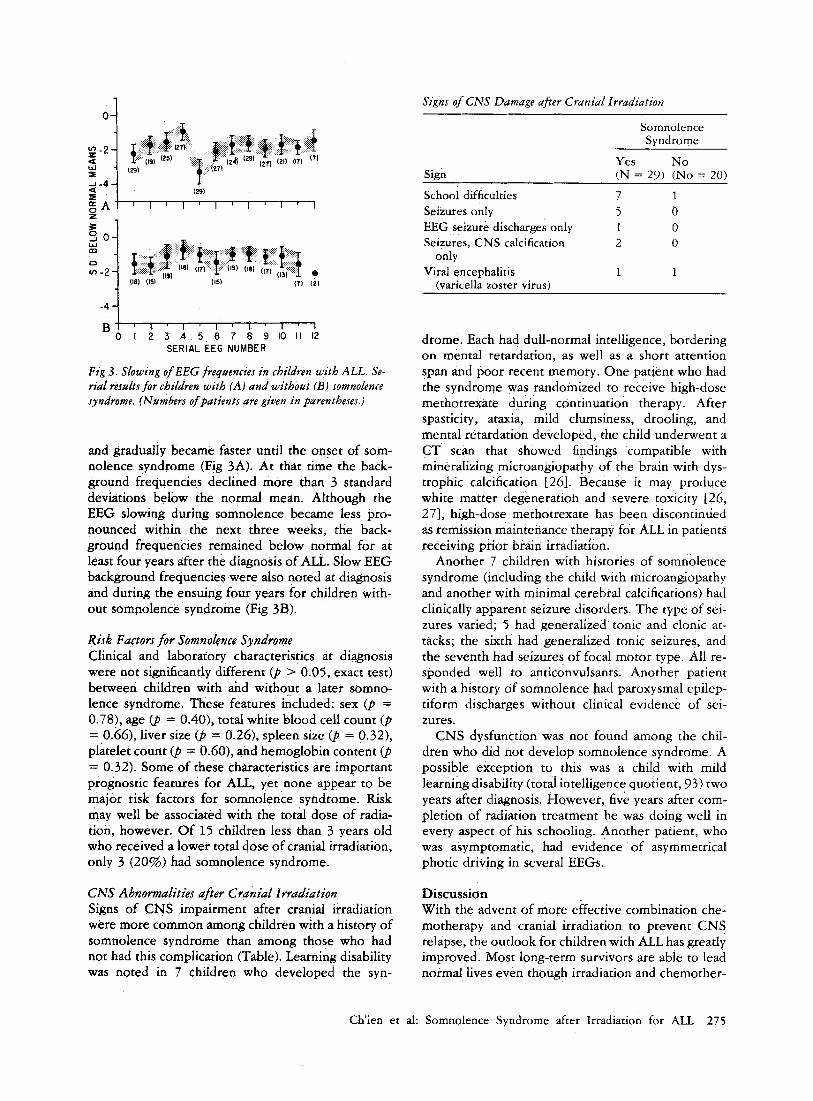
F i g 3 . Slowing of EEG frequencies in children with ALL. Se- rial resultsfor children with (A) and without (3) somnolence syndrome. (Nambers of patients are given in parentheses.)
and gradually became faster until the onset of som- nolence syndrome (Fig 3A). At that time the back- ground frequencies declined more than 3 standard deviations below the normal mean. Although the EEG slowing during somnolence became less pro- nounced within the next three weeks, the back- ground frequencies remained below normal for at least four years after the diagnosis of ALL. Slow EEG background frequencies were also noted at diagnosis and during the ensuing four years for children with- out sompolence syndrome (Fig 3B).
Risk Factors for Somnolence Syndrome Clinical and laboratory characteristics at diagnosis were not significantly different (p > 0.05, exact test) between children with and without a later somno- lence syndrome. These features included: sex (p = 0.78), age (p = 0.40), total white blood cell count (p = 0.66), liver size (p = 0.26), spleen size (p = 0.32), platelet count (p = 0.60), and hemoglobin content (p = 0.32). Some of these characteristics are important prognostic features for ALL, yet none appear to be major risk factors for somnolence syndrome. Risk may well be associated with the total dose of radia- tion, however. Of 15 children less than 3 years old who received a lower total dose of cranial irradiation, only 3 (20%) had somnolence syndrome.
CNS Abnormalities a f e r Cranial Irradiation Signs of CNS impairment after cranial irradiation were more common among children with a histoty of somnolence syndrome than among those who had not had this complication (Table). Learning disability was noted in 7 children who developed the syn-
Somnolence Syndrome
Yes No Sign (N = 29) (No = 20)
School difficulties 7 1 Seizures only 5 0 EEG seizure discharges only 1 0 Seizures, CNS calcification 2 0
Viral encephalitis 1 1 only
(varicella zoster virus)
drome. Each had dull-normal intelligence, bordering o n mental retardation, as well as a short attention span and poor recent memory. One patient who had the syndrome was randomized to receive high-dose methotrexate during continuation therapy. After spasticity, ataxia, mild clumsiness, drooling, and mental retardation developed, the child underwent a CT scan that showed findings compatible with mineralizing microangiopathy of the brairi with dys- trophic calcification [261. Because it may produce white matter degeneration and severe toxicity [26, 2 71, high-dose methotrexate has been discontinued as remission maintenance therapy for ALL in patients receiving prior braio irradiation.
Another 7 children with histories of somnolence syndrome (including the child with microangiopathy and another with minimal cerebral calcifications) had clinically apparent seizure disorders. The type of sei- zures varied; 5 had generalized tonic and clonic at- tacks; the sixth had generalized tonic seizures, and the seventh had seizures of focal motor type. All re- sponded well to anticonvulsants. Another patient with a history of somnolence had paroxysmal epilep- tiform discharges without clinical evidence of sei- zures.
CNS dysfunction was not found among the chil- dren who did not develop somnolence syndrome. A possible exception to this was a child with mild learning disability (totai intelligence quotient, 93) two years after diagnosis. However, five years after com- pletion of radiation treatment he was doing well in every aspect of his schooling. Another patient, who was asymptomatic, had evidence of asymmetrical photic driving in several EEGs.
Discussian With the advent of more effective combination che- motherapy and cranial irradiation to prevent CNS relapse, the outlook for children with ALL has greatly improved. Most long-term survivors are able to lead normal lives even though irradiation and chemother-
Ch'ien et al: Somnolence Syndrome after Irradiation for ALL 275
apy may have had some undesirable effects on vari- ous organ systems. While some of these effects emerge and abate early in the clinical course, others may represent delayed, permanent complications. In this regard, the possibility of CNS damage after cra- nial irradiation is of particular concern not only be- cause nerve cells are unable to regenerate, but also because the full extent of radiation-induced damage may not be known for many months or years.
Neuropathological features have been described for some patients with ALL who died after prolonged remissions [12, 15, 281, but therapy-related neuro- logical and neuropsychoiogical dysfunction has not yet been delineated in prospective studies. Even though longitudinal EEG studies were done in the present series, it is difficult to identify the causes of specific EEG changes because our treatment protocol was complex and the types of disease-related CNS complications are so numerous.
EEG background slowing was present in many children at the time ALL was diagnosed. Possible causes of this diffuse EEG abnormality include elec- trolyte imbalance secondary to nausea and vomiting as well as anemia and CNS leukemic infiltrations. Electrolyte imbalance was uncommon in our patients, and anemia would not have substantially affected the EEG unless its onset were rapid. Patients with chronically low hemoglobin values have little or no changes in their EEGs because the blood supply to the nervous system is usually increased, which pro- tects the brain from hypoxia. It is unlikely that EEG slowing resulted from any leukemic infiltration of the brain. First, none of our patients had pleocytosis or immature cells in the CSF at diagnosis. Second, leukemic infiltration tends to cause focal rather than diffuse EEG slowing [ lo , 231.
Persistent EEG slowing during induction chemo- therapy may have been due to asparaginase, a drug that can induce dose-related CNS symptoms includ- ing lethargy, somnolence, personality changes, con- fusion, and coma [17, 20, 21, 311. Transient diffuse EEG slowing has accompanied these symptoms in re- ported patients who received high doses of the drug [20, 25, 311. None of our patients received high doses of asparaginase, however, and none had any appreciable EEG changes after the drug was given.
Further decreases in electrocortical activity six to eight weeks after CNS treatment in our patients cor- responded to symptoms of radiation-induced som- nolence syndrome. Reports since 1973 indicate that 10 to 7595 of leukemic children who receive cranial irradiation have symptoms of somnolence syndrome six to eight weeks after completing the treatment. The symptoms may be associated with pronounced slowing of background EEG activity even when the child appears to be awake. Although longitudinal
evaluations were not done in past studies, it was con- cluded that somnolence syndrome is a transient cere- bral disturbance with impairment of new myelin synthesis that probably does not produce long-lived sequelae 19, 10, 24, 301.
Contrary to this conclusion, our present data sug- gest that somnolence syndrome may be an early indi- cator of permanent neurological damage related to the dosage of cranial irradiation. Radiation alone, given in sufficient dosage, is known to cause perma- nent changes in the CNS [4, 12, 161. In one report [12], 24 children who died of ALL had parenchyma- tous changes that included fibrillary gliosis, myelin loss, and axonal dystrophy. The severity of CNS de- terioration was related to the intensity of CNS treat- ment but not to the patients’ age at death, the dura- tion of illness, the amount of intracranial pressure, or the type of systemic treatment. With higher dosages, radiation induced acute necrosis of all cellular ele- ments, demyelination of white matter, loss of oligodendrocytes, and reactive astrocytosis. Inter- estingly, the cortex and neurons were often spared 161.
Among the variety of CNS changes in 85 of 91 children who died of acute leukemia [ 5 ] , cerebral at- rophy was the most common, prominent change. The severity of atrophy was not related directly to the in- tensity of cranial irradiation, but rather to younger patient age at the time methotrexate was given and to brevity of the clinical course. Cerebral atrophy in many instances may parallel the development of sub- acute leukoencephalopathy, one of the two well- described encephalopathies in children with ALL [7, 26, 271. Although high-dose methotrexate rather than cranial irradiation is the proposed direct cause of leukoencephalopathy, increased permeability of the blood-brain barrier due to immaturity of the CNS or to radiogenic vascular lesions may be a deciding fac- tor.
The susceptibility of the microvasculature to ra- diation may be an even more important factor in the development of mineralizing microangiopathy and dystrophic cerebral calcification [26]. Both radiation dose and schedule of administration appear to be related to cerebrovascular deterioration [4, 161, starting with alterations of the blood-brain barrier [29] and mineralization of the small vessels, and pro- gressing to encephalopathic changes 16, 181 and perhaps to various strokelike syndromes [22].
It is conceivable that such radiogenic changes could detrimentally affect intellectual functioning. Although reports of poor short-term memory and learning disabilities in long-term survivors of ALL provide little direct evidence to implicate CNS ir- radiation (or any other specific part of therapy) as the cause of this type of intellectual impairment, it is likely to be at least a contributing factor. In this re-
276 Annals of Neurology Vol 8 No 3 September 1980

spect, the current study has furnished new evidence of clinical importance. Just as cranial irradiation with 2,400 rads o r more is a high-risk feature of somno- lence syndrome, the syndrome itself is a high-risk feature of later learning disabilities.
We concur with Crosley and others [51 that treat- ment of children with acute leukemia must be care- fully gauged to minimize the risks of therapeutic complications as well as disease recurrence. De- creasing the dosage of CNS irradiation should reduce the incidence and severity of neurological sequelae, but it may also increase the risk of CNS leukemia. Thus, more conservative treatment should be tried cautiously, with close monitoring of the patient’s CNS status.
Supported in part by the Leukemia Program Project Grant CA- 20180, by Grants CA-24079 and CA-21765 from the National Cancer Institute, and by ALSAC.
Presented in part at the Eighth Annual Meeting of the Child Neu- rology Society, Hanover, NH, Sept 13, 1979.
The authors thank Ms Kit Yatsula and co-workers from the Medi- cal Records Department and Ms Lee-Sea Chen and Dr Stephen George for the statistical analysis.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Aur RJ, Hustu HO, Verzosa MS, et al: Comparison of two methods of preventing central nervous system leukemia.
Aur RJ, Simone JV, Verzosa MS, et al: Childhood acute lym- phocytic leukemia, Study VIII. Cancer 42:2123-2134, 1978 Bernhard CG, Skogland CR: On the alpha frequency of human brain potentials as a function of age. Scand Arch Physiol 26:195-201, 1939 Caveness WF: Pathology of radiation damage to the normal brain of the monkey. Natl Cancer Inst Monogr 46:57-76, 1977 Crosley CJ, Rorke LB, Evans A, Nigro M: Central nervous system lesions in childhood leukemia. Neurology 28:678- 685, 1978 DeReuck J, Vander Eecken H: The anatomy of the late radia- tion encephalopathy. Eur Neurol 13:481-494, 1975 DeVivo DC, Malas D, Nelson JS, et al: Leukoencephalopathy in childhood leukemia. Neurology 27:609-613, 1.977 Fassetta G, Cadi M, Conte G: EEG changes in leukemic chil- dren following cranial irradiation with cobalt-60 associated with intrathecal chemotherapy. Electroencephalogr Clin Neurophysiol 41:326-327, 1976 Freeman JE, Johnston PG, Voke JM: Somnolence after prophylactic cranial irradiation in children with acute lym- phoblastic leukemia. Br Med J 4523-525, 1973 Garwicz S, Aronson S, Elmqvist D, et al: Postirradiation syn- drome and EEG findings in children with acute lymphoblastic leukemia. Acta Paediatr Scand 64:399-403, 1975 George SL, Aur RJ, Mauer AM, Simone JV: A reappraisal of
Blood 42~349-357, 1973
the results of stopping therapy in childhood leukemia. N Engl J Med 300:269-273, 1979
12. Hendin B, DeVivo DC, Torack R, et al: Parenchymatous de- generation of the central nervous system in childhood leu- kemia. Cancer 33:468-482, 1974
13. Henry CE: Electroencephalograms of normal children. So- ciety for Research in Child Development Monographs. Washington, DC, National Research Council, 1944, vol9, pp 1-71
14. Hustu HO, Aur RJ, Verzosa MS, et al: Prevention of central nervous system leukemia by irradiation. Cancer 32:585-597, 1973
15. Kay HE, Knapton PJ, O’Sullivan JP, et al: Encephalopathy in acute leukaemia associated with methotrexate therapy. Arch Dis Child 47:344-354, 1972
16. Kramer S, Lee KF: Complications of radiation therapy: the central nervous system. Semin Roentgen01 9:75-83, I974
17. Land VJ, Sutow WW, Fernbach DJ, et al: Toxicity of L- asparaginase in children with advanced leukemia. Cancer 30: 3 39-347, 1972
18. Llena JF, Cespedes G, Hirario A, et al: Vascular alterations in delayed radiation necrosis of the brain. An electron mi- croscopical study. Arch Path01 Lab Med 100:531-534, 1976
19. McIntosh S, Aspnes GT: Encephalopathy following CNS prophylaxis in childhood lymphoblastic leukemia. Pediatrics
20. Moure JM, Whitecar JP Jr, Bodey GP: Electroencephalogram changes secondary to asparaginase. Arch Neurol23:365-368, 1970
21. Oettgen HF, Stephenson PA, Schwartz MK, et al: Toxiciry of E . colz L-asparaginase in man. Cancer 25:253-278, 1970
22. Painter MJ, Chutorian AM, Hilal SK: Cerebrovasculopathy following irradiation in childhood. Neurology (Minneap) 25:189-194, 1975
23. Pampiglione G: Somnolence in children with acute leukemia (letter). Br Med J 1:158, 1974
24. Parker D, Malpas JS, Sandland R, et al: Outlook following “somnolence syndrome” after prophylactic cranial irradiation. Br Med J 1:554-559, 1978
25. Pratt CB, Choi SI, Holton CP: Low-dosage asparaginase treatment of childhood acute lymphocytic leukemia. Am J Dis Child 121:406-409, 1971
26. Price RA, Birdwell DA: The central nervous system in child- hood leukemia. 111. Mineralizing microangiopathy and dys- trophic calcification. Cancer 42:717-728, 1078
27. Price RA, Jamieson PA: The central nervous system in child- hood leukemia. 11. Subacute leukoencephalopathy. Cancer
28. Rubinstein LJ, Herman MM, Long TF, Wilbur JR: Dissemi- nated necrotizing leukoencephalopathy: a complication of treated central nervous system leukemia and lymphoma. Cancer 35:291-305, 1975
29. Schettler T, Shealy CN: Experimental selective alteration of blood-brain barrier by x-irradiation. J Neurosurg 32:89-94, 1970
30. Verzosa MS, AUK RJ, Simone JV, et al: Five years after central nervous system irradiation of children with leukemia. Int J Radiar Oncol Biol Phys 1:209-215, 1976
31. Zubrod CG: The clinical toxicities of L-asparaginase in treat- ment of leukemia and lymphoma. Pediatrics 45:555-559, 1970
52:612-615, 1973
35:306-318, 1975
Ch’ien et al: Somnolence Syndrome after Irradiation for ALL 277