long-term efficacy and safety of catheter ablation for af: what is the evidence? aha qcor washington...
TRANSCRIPT
Long-term Efficacy and Safety of Catheter
Ablation for AF: What is the Evidence?
AHA QCOR Washington DC
D. George Wyse MD PhD
May 20, 2010
Disclosures*
* All < $10,000
DSMB, SC or Grant Reviewer (Research)
Advisory Board
Speaker
• Boerhinger Ingelheim (PHRI); RE-LY; RE-LYABLE
• Medtronic (Mayo) – TRENDS; PACIFIC
• Sanofi Aventis/Bristol Myers Squibb (PHRI)
- ACTIVE-A; ACTIVE –W; ACTIVE-I
• Bristol Myers Squibb/Pfizer (DCRI) – ARISTOTLE
• Sanofi Aventis – BOREALIS, DETECT-AF
• Biotronik (Axio) - IMPACT
• Boston Scientific/Guident (PHRI) - SIMPLE
• NHLBI (DCRI; U Penn) – TACT; COAG
• European Commission – FP-7 Grant Applications
• Sanofi Aventis (PHRI) – POSEIDON
• Merck
• Bayer
• Sanofi Aventis
• BMS
PHRI – Population Health Research Institute – McMaster UniversityDCRI – Duke Clinical Research Institute; Mayo – Mayo ClinicAxio – Axio Research CorporationU. Penn – University of Pennsylvania

Outline
• Key Patient Characteristics of RCT of LA/PV RFA and AAD
• Quantitative “Gradient” between Groups of SR vs. AF in AAD vs. RFA RCT
• Goals for Therapy of AF• Reduce Mortality• Prevent Stroke/SE• Preserve/Improve Ventricular Function and Prevent CHF• Relief of Symptoms
• RFA of AV Junction and Pacemaker

Age and Duration of Follow-up in RTCof LA/PV Catheter Ablation for RFA
Study N Mean/median Age Mean FU
Haissaguerre (2000) 90 51 0.7
Natale (2000) 15 59 0.8
Oral (2003) 40 51 0.5
RAAFT Pilot (2005) 70 53 1.0
APAF (2006) 198 56 1.0
CACAF (2006) 137 62 1.0
A4 (2008) 112 51 1.0
CABANA Pilot (2009) 60 64 1.0
AAD RCT: AFFIRM, AF-CHF & ATHENAN = ~ 10,000Mean Age = 70yMean FU = 4.5y
Table unpublished, courtesy of Win Shen – Mayo University
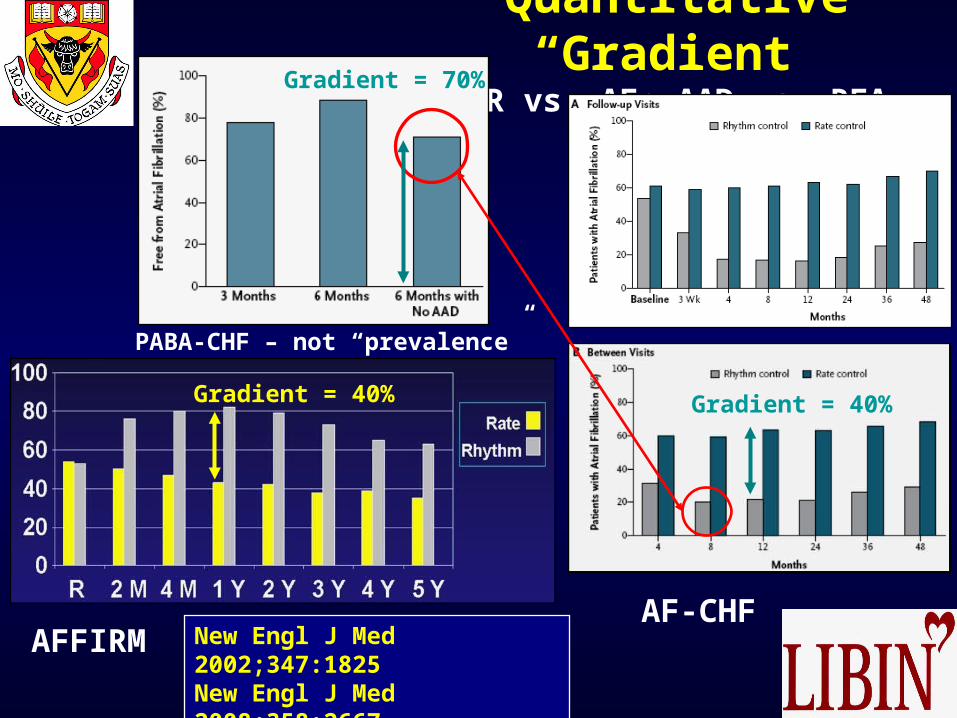
Quantitative “Gradient”SR vs. AF; AAD vs. RFA
New Engl J Med 2002;347:1825New Engl J Med 2008;358:2667New Engl J Med 2008;359:1778
AF-CHFAFFIRM
PABA-CHF – not “prevalence”
Gradient = 40%
Gradient = 70%
Gradient = 40%
Goals of Therapy for AF
Reduce Mortality

Death After RFA for AFShort-term
Circulation 2005;111:1100
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Death
Tamponade
Sepsis
PneumoX
HemoX
Phrenic N
Vessel Inj
Stroke
TIAPV Senosis
Per
cen
t
Based on 45, 115procedures in 35, 569patients between1995-2006 = 0.98 per1,000
JACC 2009;53:1798
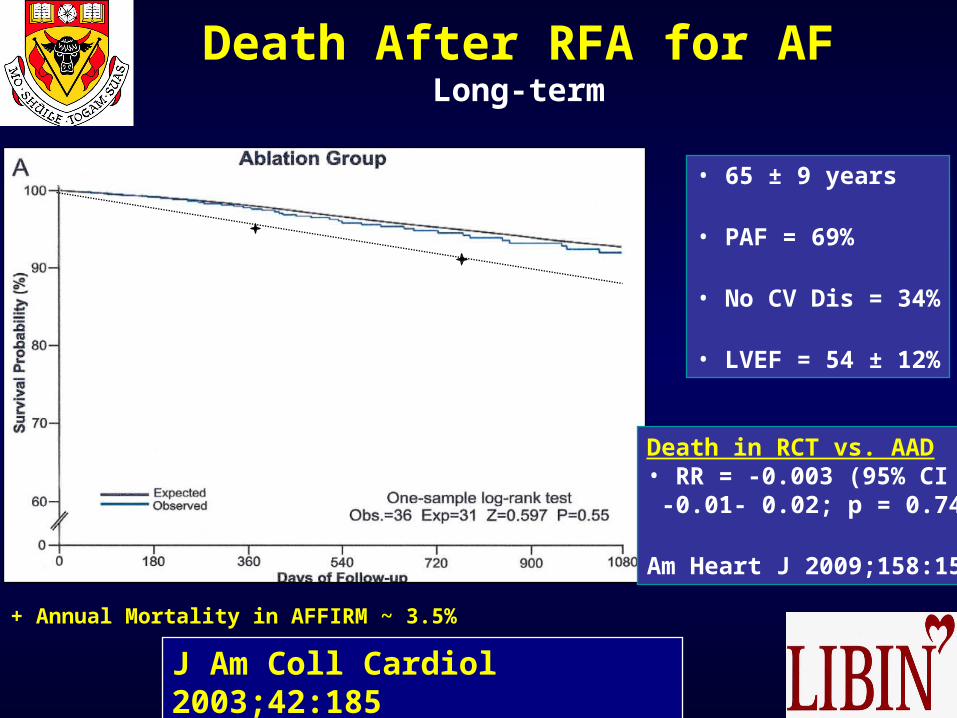
Death After RFA for AFLong-term
J Am Coll Cardiol 2003;42:185
• 65 ± 9 years
• PAF = 69%
• No CV Dis = 34%
• LVEF = 54 ± 12%
Death in RCT vs. AAD• RR = -0.003 (95% CI -0.01- 0.02; p = 0.74)
Am Heart J 2009;158:15
+ Annual Mortality in AFFIRM ~ 3.5%

Prevent Stroke/SE
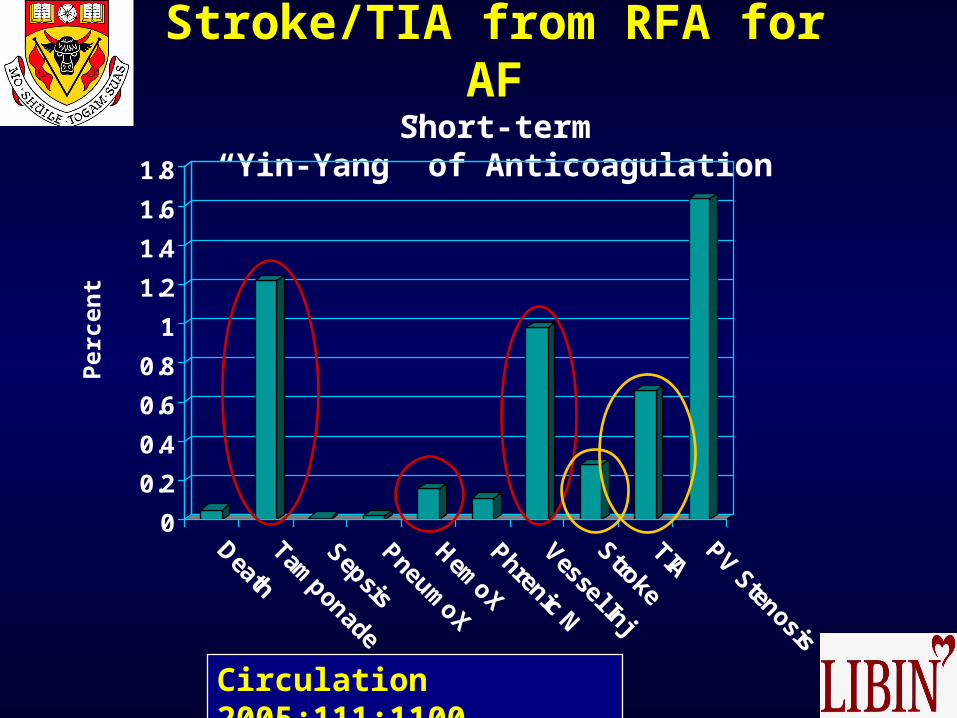
Stroke/TIA from RFA for AFShort-term
“Yin-Yang” of Anticoagulation
Circulation 2005;111:1100
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Death
Tamponade
Sepsis
PneumoX
HemoX
Phrenic N
Vessel Inj
Stroke
TIAPV Stenosis
Per
cen
t
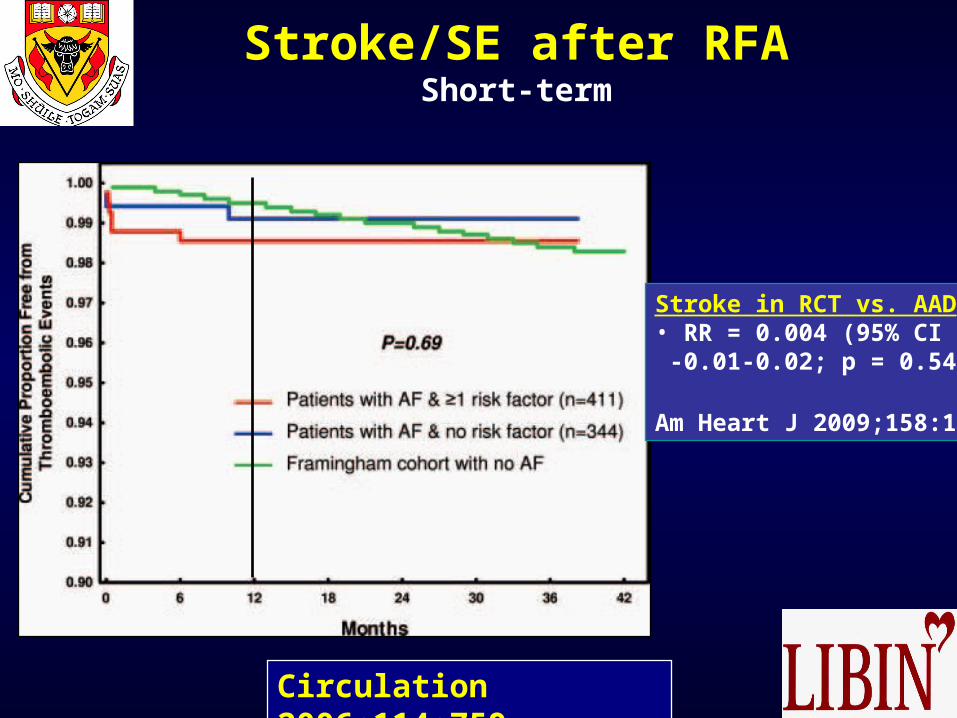
Stroke/SE after RFAShort-term
Circulation 2006;114:759
Stroke in RCT vs. AAD• RR = 0.004 (95% CI -0.01-0.02; p = 0.54)
Am Heart J 2009;158:15

Impact of Absence of AF on Stroke
Stroke In AF Patients
Cardioembolic~60 - 65%*
Other~35 - 40%*
AtheroembolicArterial Thrombosis
HemorrhageOther
•LAA•LA•LV
•Valves
* Neurology 1993;43:32 & Arch Intern Med 2005:165:1185

Perception of AF after RFA
Circulation 2005;112:307
Episodes of AF % Episodes withNo Symptoms

AF Patterns Before/After AF Ablation with 24/7 Monitoring
J Cardiovasc Electrophysiol 2007;18:818
• “Permanent Cure” after 3 mo blanking = 3/14

Preserve/Improve Ventricular Function & Prevent CHF
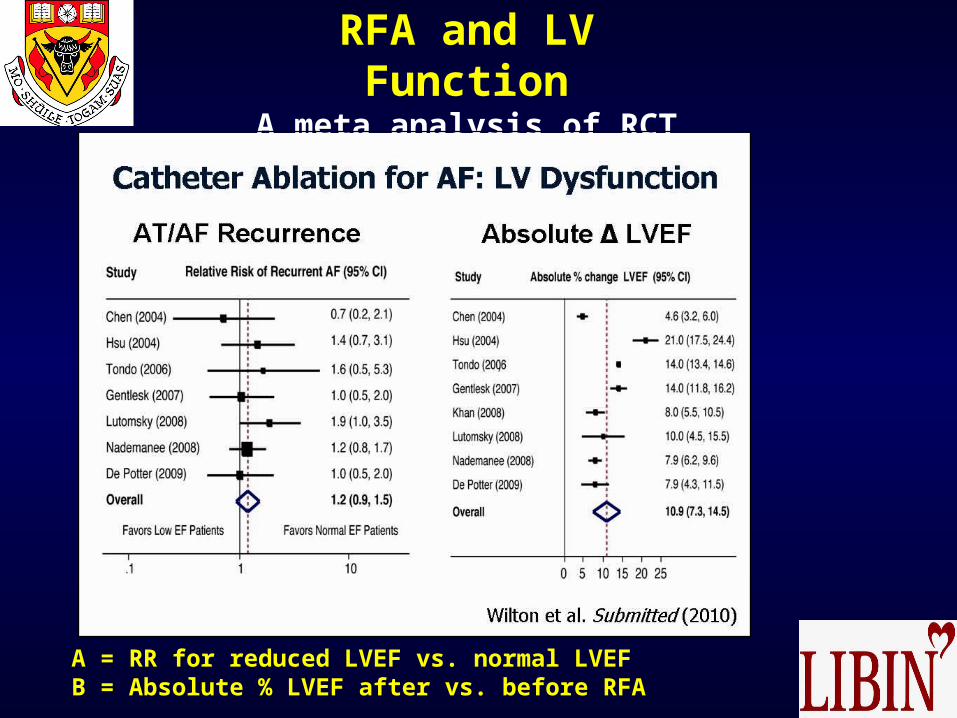
RFA and LV FunctionA meta analysis of RCT
A = RR for reduced LVEF vs. normal LVEFB = Absolute % LVEF after vs. before RFA

Relief of Symptoms

SymptomsAblation vs. AAD
J Am Med Assoc 2010;303:333
• Symptomatic AF• Failed at least 1 AAD• No amiodarone in 6 months• LA diameter <5cm• Mean age = 56y• Mean follow-up = 13 months

Symptoms of AFCCS- SAF Class N = 484
Circ Arrhythmia EP 2009:2;218
0
5
10
15
20
25
30
0 1 2 3 4
Percent
Symptom Class
Per
cen
t
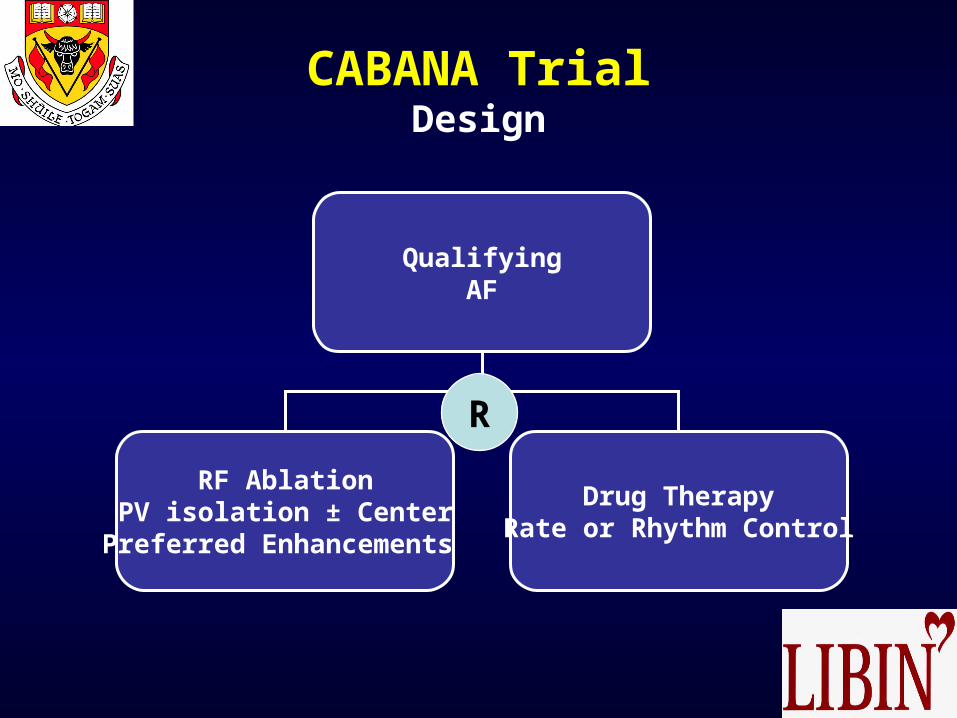
CABANA TrialDesign
QualifyingAF
RF AblationPV isolation ± Center
Preferred Enhancements
Drug TherapyRate or Rhythm Control
R

Ablate [and Pace]
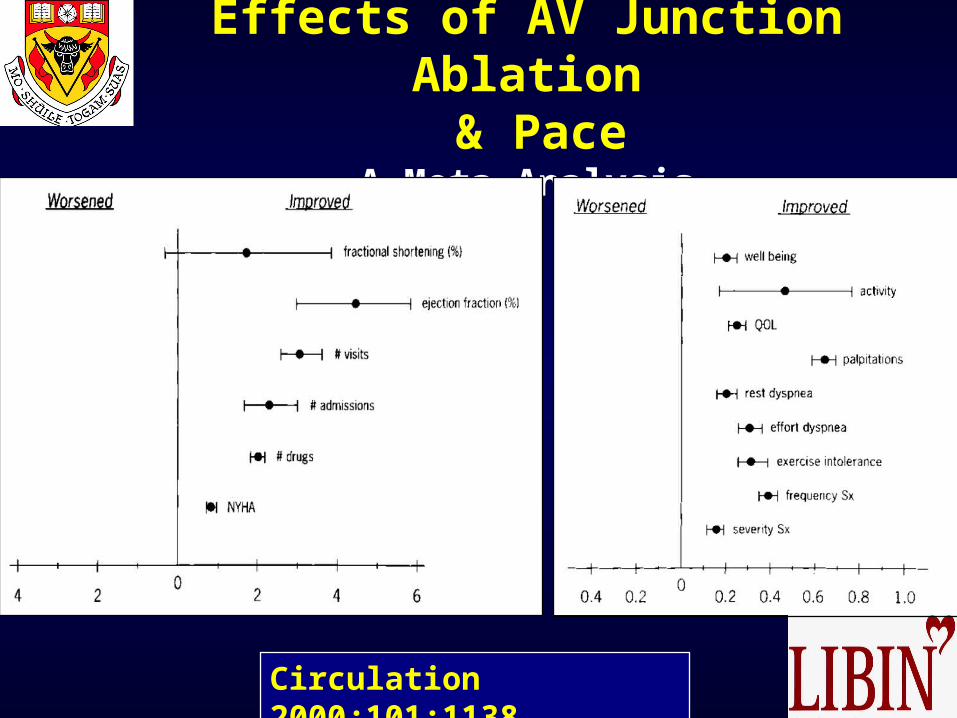
Effects of AV Junction Ablation & Pace
A Meta Analysis
Circulation 2000;101:1138
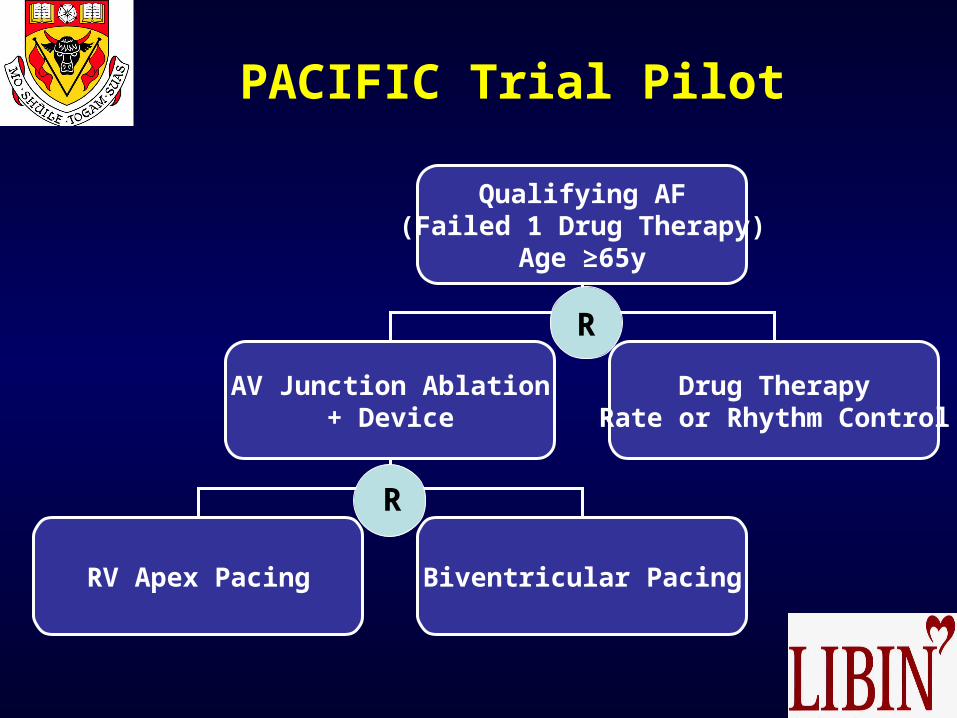
PACIFIC Trial Pilot
Qualifying AF(Failed 1 Drug Therapy)
Age ≥65y
AV Junction Ablation+ Device
Drug TherapyRate or Rhythm Control
RV Apex Pacing Biventricular Pacing
R
R