locked versus standard unlocked plating of the symphysis pubis in a type-c pelvic injury: a cadaver...
TRANSCRIPT

Injury, Int. J. Care Injured 45 (2014) 748–751
Locked versus standard unlocked plating of the symphysis pubis in aType-C pelvic injury: A cadaver biomechanical study
Berton R. Moed a,b,*, Christopher P. O’Boynick a, J. Gary Bledsoe a,b
a Department of Orthopaedic Surgery, Saint Louis University School of Medicine, 3635 Vista Avenue, 7th Floor Desloge Towers, St. Louis 63110,
Missouri, United Statesb Department of Biomedical Engineering, Parks College of Engineering, Aviation and Technology, Saint Louis University, 3450 Lindell Boulevard, St. Louis
63103, Missouri, United States
A R T I C L E I N F O
Article history:
Received 14 February 2013
Received in revised form 7 June 2013
Accepted 11 November 2013
Keywords:
Symphyseal locked plating
Locked plating
Fixation failure
A B S T R A C T
Introduction: The benefits of locked plating for pubic symphyseal disruption have not been established.
The purpose of this biomechanical study was to determine whether locked plating offers any advantage
over conventional unlocked plating of the pubic symphysis in the vertically unstable, Type-C pelvic
injury.
Methods: In each of eight embalmed cadaver pelvis specimens, sectioning of the pubic symphysis in
conjunction with a unilateral release of the sacroiliac, sacrospinous, and sacrotuberous ligaments and
pelvic floor was performed to simulate a vertically unstable Type-C (Orthopaedic Trauma Association
61-C1.2) pelvic injury. The disrupted SI joint was then reduced and fixed using two 6.5 mm cannulated
screws inserted into the S1 body. Using a six-hole 3.5 mm plate specifically designed for the symphysis
pubis having both locked and unlocked capability, four pelvises were fixed with locked screws and four
pelvises were fixed with standard unlocked bicortical screws. Both groups were similar based on a dual-
emission X-ray absorptiometry evaluation (P = 0.69). Each pelvis was then mounted on a servohydraulic
materials-testing apparatus using a bilateral stance model to mainly stress the symphyseal fixation
and was cycled up to 1 million cycles or failure, whichever occurred first.
Results: Five specimens experienced failure at the jig mounting/S1 vertebral body interface, occurring
between 360,000 and 715,000 cycles. Frank failure of the anterior or posterior instrumentation did not
occur. However, end-trialing diastasis of the initial pubic symphysis reduction was found in all pelvises.
There were no differences between the groups with respect to this loss of symphyseal reduction
(P = 0.69) or average cycles to failure (P = 1.0).
Conclusion: Pubic symphyseal locked plating does not appear to offer any advantage over standard
unlocked plating for a Type-C (OTA 61-C1.2) pelvic ring injury.
� 2013 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
Introduction
Plate fixation for disruption of the pubic symphysis as anaddition to posterior fixation for completely unstable, Type-C (AO/Orthopaedic Trauma Association [OTA] 61-C [1]) pelvic ringinjuries has been shown to improve pelvic stiffness and stability[2–5]. Over the last decade new surgical plating systems have beendeveloped with the capability of locking the screw heads to theplate and this locked plating technology has been shown to haveadvantages for diaphyseal and metaphyseal fracture fixation,especially involving osteoporotic bone [6–8]. Symphyseal plateswith this locking capability are currently available. However, any
* Corresponding author. Tel.: +13145778850; fax: +13142685121.
E-mail address: [email protected] (B.R. Moed).
0020–1383/$ – see front matter � 2013 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.injury.2013.11.017
benefit from the use of this technique for stabilization of an acutepubic symphyseal disruption has not been demonstrated. In fact,recent study indicates that locked plating of the pubic symphysisdoes not appear to offer any advantage over the standard unlockedtechnique for partially stable, open-book (OTA 61-B3.1 [1]) pelvicring injuries [9].
The purpose of this biomechanical study was to determinewhether locked plating offers any advantage over conventionalunlocked plating of the pubic symphysis in the vertically unstable,Type-C pelvic injury.
Materials and methods
Eight embalmed pelvic specimens were obtained with thesacroiliac (SI), sacrospinous, sacrotuberous, symphyseal ligaments,and the pelvic floor intact. The mean age was 77 years (range,
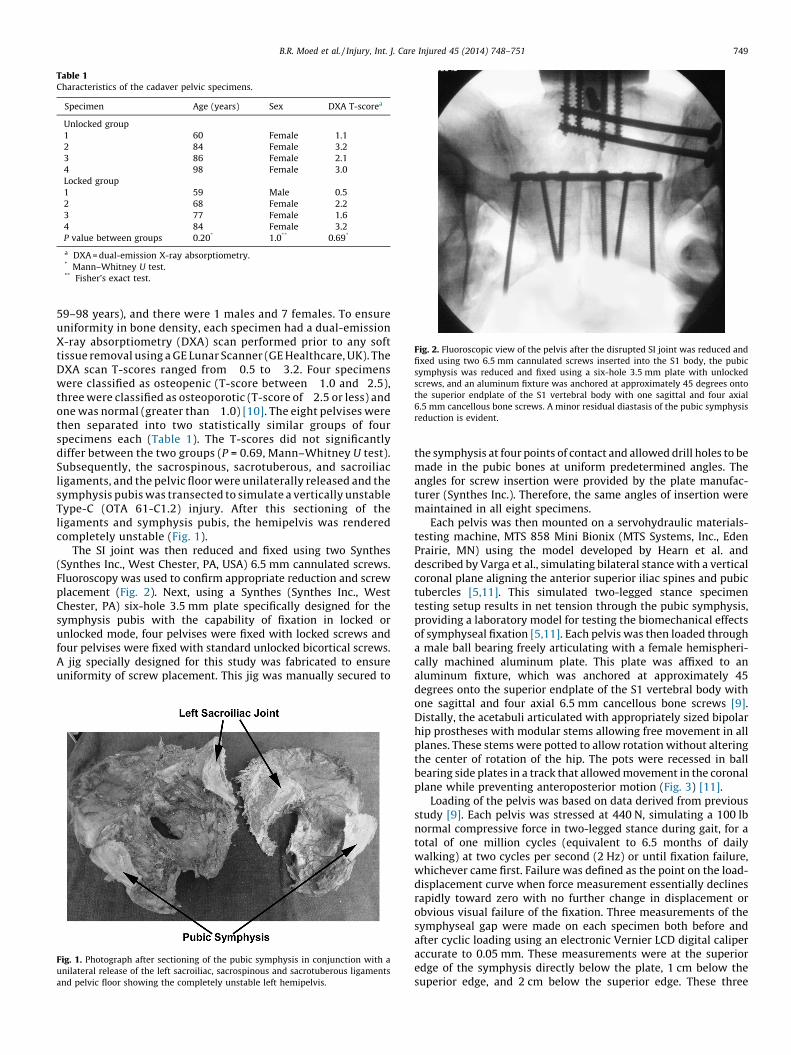
Table 1Characteristics of the cadaver pelvic specimens.
Specimen Age (years) Sex DXA T-scorea
Unlocked group
1 60 Female �1.1
2 84 Female �3.2
3 86 Female �2.1
4 98 Female �3.0
Locked group
1 59 Male �0.5
2 68 Female �2.2
3 77 Female �1.6
4 84 Female �3.2
P value between groups 0.20* 1.0** 0.69*
a DXA = dual-emission X-ray absorptiometry.* Mann–Whitney U test.** Fisher’s exact test.
Fig. 2. Fluoroscopic view of the pelvis after the disrupted SI joint was reduced and
fixed using two 6.5 mm cannulated screws inserted into the S1 body, the pubic
symphysis was reduced and fixed using a six-hole 3.5 mm plate with unlocked
screws, and an aluminum fixture was anchored at approximately 45 degrees onto
the superior endplate of the S1 vertebral body with one sagittal and four axial
6.5 mm cancellous bone screws. A minor residual diastasis of the pubic symphysis
reduction is evident.
B.R. Moed et al. / Injury, Int. J. Care Injured 45 (2014) 748–751 749
59–98 years), and there were 1 males and 7 females. To ensureuniformity in bone density, each specimen had a dual-emissionX-ray absorptiometry (DXA) scan performed prior to any softtissue removal using a GE Lunar Scanner (GE Healthcare, UK). TheDXA scan T-scores ranged from �0.5 to �3.2. Four specimenswere classified as osteopenic (T-score between �1.0 and�2.5),three were classified as osteoporotic (T-score of �2.5 or less) andone was normal (greater than �1.0) [10]. The eight pelvises werethen separated into two statistically similar groups of fourspecimens each (Table 1). The T-scores did not significantlydiffer between the two groups (P = 0.69, Mann–Whitney U test).Subsequently, the sacrospinous, sacrotuberous, and sacroiliacligaments, and the pelvic floor were unilaterally released and thesymphysis pubis was transected to simulate a vertically unstableType-C (OTA 61-C1.2) injury. After this sectioning of theligaments and symphysis pubis, the hemipelvis was renderedcompletely unstable (Fig. 1).
The SI joint was then reduced and fixed using two Synthes(Synthes Inc., West Chester, PA, USA) 6.5 mm cannulated screws.Fluoroscopy was used to confirm appropriate reduction and screwplacement (Fig. 2). Next, using a Synthes (Synthes Inc., WestChester, PA) six-hole 3.5 mm plate specifically designed for thesymphysis pubis with the capability of fixation in locked orunlocked mode, four pelvises were fixed with locked screws andfour pelvises were fixed with standard unlocked bicortical screws.A jig specially designed for this study was fabricated to ensureuniformity of screw placement. This jig was manually secured to
Fig. 1. Photograph after sectioning of the pubic symphysis in conjunction with a
unilateral release of the left sacroiliac, sacrospinous and sacrotuberous ligaments
and pelvic floor showing the completely unstable left hemipelvis.
the symphysis at four points of contact and allowed drill holes to bemade in the pubic bones at uniform predetermined angles. Theangles for screw insertion were provided by the plate manufac-turer (Synthes Inc.). Therefore, the same angles of insertion weremaintained in all eight specimens.
Each pelvis was then mounted on a servohydraulic materials-testing machine, MTS 858 Mini Bionix (MTS Systems, Inc., EdenPrairie, MN) using the model developed by Hearn et al. anddescribed by Varga et al., simulating bilateral stance with a verticalcoronal plane aligning the anterior superior iliac spines and pubictubercles [5,11]. This simulated two-legged stance specimentesting setup results in net tension through the pubic symphysis,providing a laboratory model for testing the biomechanical effectsof symphyseal fixation [5,11]. Each pelvis was then loaded througha male ball bearing freely articulating with a female hemispheri-cally machined aluminum plate. This plate was affixed to analuminum fixture, which was anchored at approximately 45degrees onto the superior endplate of the S1 vertebral body withone sagittal and four axial 6.5 mm cancellous bone screws [9].Distally, the acetabuli articulated with appropriately sized bipolarhip prostheses with modular stems allowing free movement in allplanes. These stems were potted to allow rotation without alteringthe center of rotation of the hip. The pots were recessed in ballbearing side plates in a track that allowed movement in the coronalplane while preventing anteroposterior motion (Fig. 3) [11].
Loading of the pelvis was based on data derived from previousstudy [9]. Each pelvis was stressed at 440 N, simulating a 100 lbnormal compressive force in two-legged stance during gait, for atotal of one million cycles (equivalent to 6.5 months of dailywalking) at two cycles per second (2 Hz) or until fixation failure,whichever came first. Failure was defined as the point on the load-displacement curve when force measurement essentially declinesrapidly toward zero with no further change in displacement orobvious visual failure of the fixation. Three measurements of thesymphyseal gap were made on each specimen both before andafter cyclic loading using an electronic Vernier LCD digital caliperaccurate to 0.05 mm. These measurements were at the superioredge of the symphysis directly below the plate, 1 cm below thesuperior edge, and 2 cm below the superior edge. These three

Fig. 3. Photograph of a pelvis specimen mounted on the materials-testing machine.
Fig. 4. Photograph of a pelvis specimen from an 86 year old woman shown in Fig. 2
after undergoing one million cycles on the materials-testing machine. A slight
increase in the original diastasis was evident (white arrows).
B.R. Moed et al. / Injury, Int. J. Care Injured 45 (2014) 748–751750
measurements were made to allow for the detection of anyasymmetric symphyseal gapping.
Appropriate for the number of specimens, the nonparametricMann–Whitney U test was used to compare the two groups ofcadaver pelvic specimens for all statistical evaluations with theexception gender, for which the Fisher’s exact test was used(Table 1). Level of statistical significance was defined as P < 0.05.
Results
No frank failure of the symphyseal or the posterior fixationoccurred during testing. However, five specimens experiencedfailure at the interface between the mounting jig and the S1vertebral body. These five failures occurred through the S1vertebral body, anterior to the 6.5 mm cannulated SI screws,between 360,000 cycles and 715,000 cycles. Of the threespecimens completing the full one million cycles, one was inthe locked group and two were in the unlocked group.Unlocked specimens averaged approximately 692,000 cyclesbefore failure compared with 701,000 for the specimens withlocked plates. This difference was not statistically significant(P = 1.0).
A slight diastasis of the initial pubic symphysis reduction wasfound in all pelvises regardless of fixation method (Fig. 4) with anoverall mean of 1.0 mm (range 0.2–1.7 mm). The symphysealseparation for the unlocked group before loading averaged 2.0, 2.7,and 3.3 mm, respectively for the three levels of measurement (i.e.,superior edge of the symphysis directly below the plate, 1 cmbelow the superior edge, and 2 cm below the superior edge) andafter loading this measurement averaged 3.0, 3.5, and 4.3 mm,respectively. The symphyseal separation for the locked groupbefore loading averaged 1.4, 2.0, and 2.3 mm, respectively for thethree levels of measurement and after loading this measurementaveraged 2.5, 3.0, and 3.4 mm, respectively. At each of the threelevels, no significant difference was found between the two groupswhen comparing symphyseal widening after cyclic loading(P = 0.69).
Discussion
Open reduction and internal fixation (ORIF) of the pubicsymphysis has progressively evolved over the last half centuryfrom treatment with cerclage wiring to external fixation to moderntechniques using plate and screw constructs [12]. Currently, theplate and screw construct is the preferred fixation method for thetreatment of pubic symphyseal disruption in conjunction with anOTA 61-C pelvic injury [12,13]. With the arrival of locked platetechnology, surgical implants designed specifically for internalfixation of the pubic symphysis have been made commerciallyavailable. Despite touted potential advantages of locked plating forfracture fixation, especially in osteoporotic bone, recent bio-mechanical study indicates that locked plating of the pubicsymphysis does not appear to offer any advantage over thestandard unlocked technique for partially stable, open-book (OTA61-B3.12) pelvic ring injuries [9]. Furthermore, a recent case seriesof six patients further supports this contention [14]. In thisadmittedly small series, failure mechanisms of locked design-specific plate fixation of the pubic symphysis included those seenwith conventional uniplanar fixation as well as those common tolocked plate technology [14]. The authors concluded that theindications for the use of these implants remain to be determined.
The pubic symphysis has inherent physiologic motion [2,11,15–17]. Fixation with a locked screw construct provides angularstability, neutralizing bending forces through the screw/plateinterface, creating a stiffer construct [6,18]. Therefore, its use totreat a pubic symphyseal disruption is counterintuitive. Consistentwith this expectation, there was minor loss of symphysealreduction in all of the unlocked pelvis specimens, which has beenshown to be common with standard unlocked plating techniques[11,12,16,19,20]. Somewhat unexpected was this occurrence ofthis loosening at the screw–bone interface and gapping of thepubic symphyseal reduction with all the pelvises treated withlocked fixation. However, this finding is consistent with thefindings of previous studies [9,14]. This type of fixation failure hasbeen shown to be clinically unimportant [21].
The testing apparatus used in this study is a proven model forbiomechanical evaluation of pubic symphyseal fixation. It wasinitially developed by Hearn et al. at the biomechanics laboratoryat Sunnybrook Health Sciences Centre in Toronto [22]. It has beenused in numerous studies to evaluate the effectiveness andbiomechanics of pelvic fixation [2,11,17,23]. Specifically, the two-legged stance apparatus is thought to be more appropriate than asingle-leg stance model for the testing of symphyseal fixationbecause it produces distraction at the pubic symphysis [5,11].

B.R. Moed et al. / Injury, Int. J. Care Injured 45 (2014) 748–751 751
This study does have limitations. The cadaver specimens usedfor this study were embalmed and not fresh-frozen. However,Comstock et al. used embalmed cadaver specimens in abiomechanical evaluation of fixation of the posterior pelvic ringand found comparative results to studies performed with freshfrozen specimens [24]. More recently, van Zwienen et al. foundembalmed pelvic specimens to be satisfactory for the biomechani-cal evaluation of unstable pelvic ring injuries [25]. Because of theirrelatively low bone density, as demonstrated by the DXAmeasurements, the specimens in this study should be consideredappropriate to determine any advantage of locked plating overstandard unlocked plating. Although the two groups were notstatistically different by DXA measurement, if anything, the minorraw number differences in bone density would favor the lockedover the unlocked group. We had hoped that the testing protocolwould produce a few complete fixation failures. Another limitationis that five of the eight specimens failed at interface between themounting jig and the S1 vertebral body without completing theplanned one million cycles, occurring between 360,000 cycles and715,000 cycles. We selected a load magnitude and a number ofcycles that were thought to be adequate to produce fixationfailures [26–28]. The fact that we did not produce any examples ofprogressive complete fixation failure is likely the result of thenumber of cycles rather than the magnitude of the load. Theseearly failures, which occurred through the S1 body, most likelyindicate that the S1 vertebral body was not of sufficient size and/ordensity to accommodate the two 6.5 mm SI fixation screws incombination with the mounting jig screws. While this issue didcreate minor differences in total cycles between the two groups itwas not statistically significant (P = 1.0). In addition, usingapproximately 5000 steps per day for the average United Statesadult, each specimen experienced a minimum 2 to 3 months ofsimulated walking conditions before mounting failure [30]. Afurther limitation of this study is the small number of specimenstested, which is a universal issue with biomechanical cadaverstudies. However, the appropriate use of nonparametric statisticsshould minimize this shortcoming, obviating the need for a poweranalysis.
There are many described fixation methods for disruption of thepubic symphysis. These different techniques include variations inthe types of plates used, the number of screws used and the typesof screws used, including combinations of locked and standardunlocked screws [3,5,11–13,15,16,20,29]. It is possible techniquesother than those examined in this study, such as longer plates withmore screws or plating using locked and standard unlocked screws,could show improved dynamic biomechanical properties ascompared to standard unlocked plating. However, these othertechniques were not the subject of this report, and their evaluationmust await further study.
In conclusion, this study indicates that in the setting of an acuteType-C (OTA 61-C1.2) pelvic ring injury pubic symphyseal lockedplating does not appear to offer any advantage over standardunlocked plating. Therefore, we recommend continued use ofstandard plating techniques for disruption of the pubic symphysis.
References
[1] Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, et al. Fractureand dislocation classification compendium. J Orthop Trauma 2007;21(10suppl.):S1–63.
[2] Tile M, Hearn T, Vrahas M. Biomechanics of the pelvic ring. In: Tile M, HelfetDL, Kellam JF, editors. Fractures of the pelvis and acetabulum. 3rd ed.,Philadelphia: Lippincott Williams & Wilkins; 2003. p. 32–45.
[3] Sagi HC, Ordway NR, Dipasquale T. Biomechanical analysis of fixation forvertically unstable sacroiliac dislocations with iliosacral screws and symphy-seal plating. J Orthop Trauma 2004;18:138–43.
[4] Matta JM. Indications for anterior fixation of pelvic fractures. Clin Orthop RelatRes 1996;329:88–96.
[5] Gorczyca J, Hearn T, Tile M. Biomechanics and methods of pelvic fixation. In:Tile M, Helfet DL, Kellam JF, editors. Fractures of the pelvis and acetabulum. 3rded., Philadelphia: Lippincott Williams & Wilkins; 2003. p. 116–29.
[6] Kretteck C, Gosling T. Principles of internal fixation. In: Bucholz RW, Heck-man JD, Court-Brown C, Tornetta P, Koval KJ, editors. Rockwood and Green’sfractures in adults. 6th ed., Philadelphia: Lippincott Williams & Wilkins;2006 . p. 209–56.
[7] Strauss EJ, Schwarzkopf R, Kummer F, Egol KA. The current status of lockedplating: the good, the bad, and the ugly. J Orthop Trauma 2008;22:479–86.
[8] Schutz M, Ruedi TP. Principles of internal fixation. In: Bucholz RW, Court-Brown C, Heckman JD, Tornetta PII, editors. Rockwood and Green’s fractures inadults. 7th ed., Philadelphia: Lippincott Williams & Wilkins; 2010. p. 162–90.
[9] Grimshaw CS, Bledsoe JG, Moed BR. Locked versus standard unlocked platingof the symphysis pubis: a cadaver pelvic biomechanical study. J OrthopTrauma 2012;26:402–6.
[10] Kanis JA. Assessment of fracture risk and its application to screening forpostmenopausal osteoporosis: synopsis of a WHO report. Osteoporos Int1994;4:368–81. WHO Study Group.
[11] Varga E, Hearn T, Powell J, Tile M. Effects of method of internal fixation ofsymphyseal disruptions on stability of pelvic ring. Injury 1995;26:75–80.
[12] Sagi HC, Papp S. Comparative radiographic and clinical outcome of two-holeand multi-hole symphyseal plating. J Orthop Trauma 2008;22:373–8.
[13] Moed BR, Kellam JF, McLaren A, Tile M. Disruption of the pelvic ring: internalfixation for the injured pelvic ring. In: Tile M, Helfet DL, Kellam JF, editors.Fractures of the pelvis and acetabulum. 3rd ed., Philadelphia: LippincottWilliams & Wilkins; 2003. p. 217–93.
[14] Moed BR, Grimshaw CS, Segina DN. Failure of locked design-specific platefixation of the pubic symphysis: a report of six cases. J Orthop Trauma2012;26:e71–5.
[15] Webb L, Gristina A, Wilson J, et al. Two-hole plate fixation for traumaticsymphysis pubis diastasis. J Trauma 1988;28:813–7.
[16] Simonian PT, Schwappach JR, Routt Jr ML. Evaluation of new plate designs forsymphysis pubis internal fixation. J Trauma 1996;41:498–502.
[17] Vrahas M, Hearn TC, Diangelo D, Kellam J, Tile M. Ligamentous contributions topelvic stability. Orthopedics 1995;18:271–4.
[18] Lujan TJ, Henderson CE, Madey SM, Fitzpatrick DC, Marsh JL, Bottlang M.Locked plating of distal femur fractures leads to inconsistent and asymmetriccallus formation. J Orthop Trauma 2010;24:156–62.
[19] Collinge C, Archdeacon MT, Dulaney-Cripe E, Moed BR. Radiographic changesof implant failure after plating for pubic symphysis diastasis: an underappre-ciated reality? Clin Orthop Relat Res 2012;470:2148–53.
[20] Simonian PT, Routt Jr ML, Harington RM, Tencer AF. Box plate fixation of thesymphysis pubis: biomechanical evaluation of a new technique. J OrthopTrauma 1994;8:483–9.
[21] Morris SAC, Loveridge J, Smart DKA, Ward AJ, Chesser TJS. Is fixation failureafter plate fixation of the symphysis pubis clinically important? Clin OrthopRelat Res 2012;470:2154–60.
[22] Tile M, Hearn T. Biomechanics. In: Tile M, editor. Fractures of the pelvis andacetabulum. 2nd ed., Baltimore, MD: Williams & Wilkins; 1995. p. 22–36.
[23] Kim WY, Hearn TC, Seleem O, Mahalingam E, Stephen D, Tile M. Effect of pinlocation on stability of pelvic external fixation. Clin Orthop Relat Res1999;361:237–44.
[24] Comstock CP, van der Meulen MCH, Goodman SB. Biomechanical comparisonof posterior internal fixation techniques for unstable pelvic fractures. J OrthopTrauma 1996;10:517–22.
[25] van Zwienen CMA, van den Bosch EW, Snijders CJ, Kleinrensink GJ, van VugtAB. Biomechanical comparison of sacroiliac screw techniques for unstablepelvic ring fractures. J Orthop Trauma 2004;18:589–95.
[26] Walheim G, Olerud S, Ribbe T. Mobility of the pubic symphysis. Measurementsby an electromechanical method. Acta Orthop Scand 1984;55:203–8.
[27] Meissner A, Fell M, Wilk R, Boenick U, Rahmanzadeh R. Biomechanics of thepubic symphysis. Which forces lead to mobility of the symphysis in physio-logical conditions? Unfallchirurg 1996;99:415–21.
[28] Cowin SC. Bone mechanics handbook. 2nd ed. Boca Raton, FL: CRC Press; 2001.[29] Pizanis A, Garcia P, Santelmann M, Culemann U, Pohlemann T. Reduction and
fixation capabilities of different plate designs for pubic symphysis disruption:a biomechanical comparison. Injury 2013;44:183–8.
[30] Bassett Jr DR, Wyatt HR, Thompson H, Peters JC, Hill JO. Pedometer-measuredphysical activity and health behaviors in United States adults. Med Sci SportsExerc 2010;42:1819–25.