location and outcome of anticoagulant-associated intracerebral hemorrhage
TRANSCRIPT
197
Neurocritical CareCopyright © 2006 Humana Press Inc.All rights of any nature whatsoever are reserved.ISSN 1541-6933/06/5:197–201 ISSN 1556-0961 (Online)DOI: 10.1385/Neurocrit. Care 2006;05:197–201
*Correspondence and reprint requests to:
Matthew L. Flaherty, MD, 231 Albert Sabin Way, MSB Room 5161B, University of Cincinnati Medical Center, Cincinnati, OH, 45267-0525. Telephone (513) 558-6609. Fax (513) 558-4305.
E-mail: [email protected]
Warfarin use for stroke prevention in patients with atrial fibrillation became more common in the 1990s (1). During this time, there was a concomitant increase in the frequency of anticoagulant-associated intracerebral hemorrhages (AAICH) (2).
AbstractBackground: The characteristics of patients with anticoagulant-associated intracerebral hemorrhage (AAICH) have not been well characterized in a population-based setting.
Methods: We attempted to ascertain all patients with ICH in Greater Cincinnati from May 1998 to July 2001 and August 2002 to April 2003 via retrospective review of ICD-9 codes 430–438.9 at all area hospitals and prospective surveillance at tertiary centers. Cases of ICH without coagulopathy and AAICH were compared with multivariate logistic modeling and survival analysis.
Results: AAICH occurred in 190 of 1041 ICH cases (18%). In multivariate analysis, predictors of AAICH were cerebellar location of hemorrhage (p = 0.01) and a history of coronary artery disease (p < 0.001), ischemic stroke (p < 0.001), atrial fibrillation (p < 0.001) and DVT or PE (p < 0.001). Relative to other ICH locations, only cerebellar ICH showed an excess risk of anticoagulant-associated hemorrhage (OR 2.2, 95% CI 1.2 to 4.0). In multivariate modeling the only predictor of cerebellar location of ICH was anticoagulation (p < 0.001). Patients with AAICH were more likely to die than other ICH patients. The difference in morality occurred by day one (mortality 33.2% vs 16.3%, p < 0.001) and remained stable through one year (mortality 66.3% vs 50.3%, p < 0.001).
Conclusions: AAICH preferentially affects the cerebellum. Despite its association with amyloid angiopathy, lobar ICH was no more likely to be anticoagulant-associated than deep cerebral ICH. The excess mortality among AAICH patients accrues within one day of hemorrhage. Patients with AAICH have a high burden of vascular risk factors. New treatments for AAICH with prothrombotic potential should be evaluated in randomized controlled trials before routine use.
Key Words: Intracerebral hemorrhage; anticoagulants; warfarin; epidemiology.
(Neurocrit. Care 2006;05:197–201)
Location and Outcome of Anticoagulant-Associated Intracerebral HemorrhageMatthew L. Flaherty,1,* Mary Haverbusch,1 Padmini Sekar,2 Brett M. Kissela,1 Dawn Kleindorfer,1 Charles J. Moomaw,1 Joseph P. Broderick,1 and Daniel Woo1
1Departments of Neurology and 2Environmental Health, University of Cincinnati Medical Center, Cincinnati, OH
Better understanding of AAICH patterns will aid in refining risk-benefit analyses for anticoagulation as well as planning for studies of AAICH treatment. We there-fore investigated the profile of AAICH patients in a large, population-based stroke study.
Original Article
198 Flaherty et al.
Neurocritical Care ♦ Volume 5, 2006
MethodsThis report analyzes a population-based ICH cohort
ascertained from May 1998 to July 2001 and August 2002 to April 2003 as part of the Genetic and Environmental Risk Factors for Hemorrhagic Stroke (GERFHS) study. The methodology of the GERFHS study has been described (3).
We attempted to ascertain all hospitalized cases of first-ever ICH in persons aged ³ 18 years occurring within the five-county Greater Cincinnati/Northern Kentucky (GCNK) area. Cases were identified by retrospective review of primary and secondary ICD-9 codes 430–432 through October 1999 and codes 430–438.9 thereafter. Study nurses also maintained ac-tive surveillance (“hot pursuit”) at several hospitals that treat most ICH in the area by reviewing neurosurgery logs and pa-tient rosters several times each week (3). All potential cases were abstracted by study nurses and reviewed in detail by study physicians. Patients living outside of the five counties of interest were excluded based upon zip code of residence. Other exclusion criteria were previous ICH, traumatic ICH, hemorrhagic cerebral infarction, and hemorrhage associated with brain tumor, encephalitis, recent endarterectomy, and thrombolytic treatment of ischemic stroke. AAICH was de-fined as ICH while patients were receiving warfarin or hepa-rin. Among warfarin users no lower limits of prothrombin time (PT) or international normalized ratio (INR) values were set because a previous study has suggested that among these patients INR values < 2 confer similar ICH risk to values of 2–3.(4) Warfarin or heparin use was determined from chart re-view. The first available INR value upon medical presentation was recorded. For any case in which ICH location was not un-equivocally identified by radiographic reports, radiographic films were reviewed by investigators. Hemorrhage volumes
and the presence of intraventricular hemorrhage were not rou-tinely documented.
Patient demographics and putative risk factors for ICH were recorded by chart review and compared with the chi-square test, Fisher’s exact test, Student’s t-test, or Wilcoxon two-sample test, as appropriate. Among all patients with ICH, multivariate logistic regression modeling was used to identify factors independently associated with AAICH using variables from Table 1. Variables with a p value of > 0.10 were backward eliminated from the model. Based on the findings of this anal-ysis, multivariate logistic regression modeling was also per-formed to determine predictors of cerebellar location of ICH using variables from Table 2. Variables with a p value of > 0.10 were again backward eliminated from the model. Survival fol-lowing ICH was calculated using actuarial methods after que-rying GERFHS study records, the Social Security Death Index, and Ohio and Kentucky death registers. The institutional re-view board for each participating hospital system approved the GERFHS study.
ResultsWe identified 1041 persons with first-ever ICH after exclu-
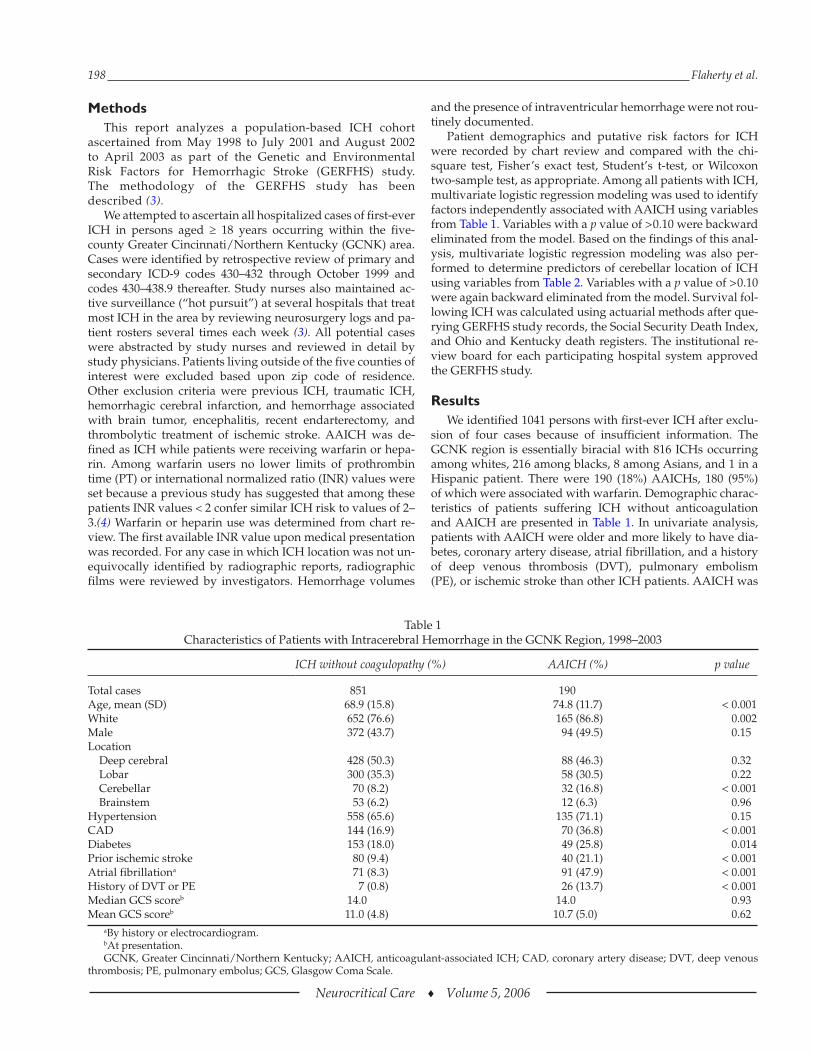
sion of four cases because of insufficient information. The GCNK region is essentially biracial with 816 ICHs occurring among whites, 216 among blacks, 8 among Asians, and 1 in a Hispanic patient. There were 190 (18%) AAICHs, 180 (95%) of which were associated with warfarin. Demographic charac-teristics of patients suffering ICH without anticoagulation and AAICH are presented in Table 1. In univariate analysis, patients with AAICH were older and more likely to have dia-betes, coronary artery disease, atrial fibrillation, and a history of deep venous thrombosis (DVT), pulmonary embolism (PE), or ischemic stroke than other ICH patients. AAICH was
Table 1Characteristics of Patients with Intracerebral Hemorrhage in the GCNK Region, 1998–2003
ICH without coagulopathy (%) AAICH (%) p value
Total cases 851 190Age, mean (SD) 68.9 (15.8) 74.8 (11.7) < 0.001White 652 (76.6) 165 (86.8) 0.002Male 372 (43.7) 94 (49.5) 0.15Location Deep cerebral 428 (50.3) 88 (46.3) 0.32 Lobar 300 (35.3) 58 (30.5) 0.22 Cerebellar 70 (8.2) 32 (16.8) < 0.001 Brainstem 53 (6.2) 12 (6.3) 0.96Hypertension 558 (65.6) 135 (71.1) 0.15CAD 144 (16.9) 70 (36.8) < 0.001Diabetes 153 (18.0) 49 (25.8) 0.014Prior ischemic stroke 80 (9.4) 40 (21.1) < 0.001Atrial fibrillationa 71 (8.3) 91 (47.9) < 0.001History of DVT or PE 7 (0.8) 26 (13.7) < 0.001Median GCS scoreb 14.0 14.0 0.93Mean GCS scoreb 11.0 (4.8) 10.7 (5.0) 0.62
aBy history or electrocardiogram.bAt presentation.GCNK, Greater Cincinnati/Northern Kentucky; AAICH, anticoagulant-associated ICH; CAD, coronary artery disease; DVT, deep venous
thrombosis; PE, pulmonary embolus; GCS, Glasgow Coma Scale.
Anticoagulant-Associated Intracerebral Hemorrhage 199
Neurocritical Care ♦ Volume 5, 2006
responsible for a higher percentage of ICH cases in whites than other races (20% vs 11%, p = 0.002). Results of the multivariate logistic regression analysis of AAICHs are found in Table 3. Histories of coronary artery disease, isch-emic stroke, atrial fibrillation, or deep venous thrombo-embolism were all strongly associated with AAICH. Relative to other ICH locations, only cerebellar ICH showed an ex-cess risk of anticoagulant-associated hemorrhage (OR 2.2, 95% CI 1.2 to 4.0). For patients on warfarin, the relationship of AAICH and hemorrhage location remained relatively constant through the range of INR intensities (data not shown).
A separate analysis was undertaken to identify predictors of cerebellar location of ICH. Univariate results are shown in Table 2. In multivariate modeling, the only predictor of cere-bellar location of ICH was anticoagulation (OR 2.2, 95% CI 1.4–3.4), with a trend toward fewer cerebellar ICHs in non-whites (OR 0.6, 95% CI 0.3–1.1).
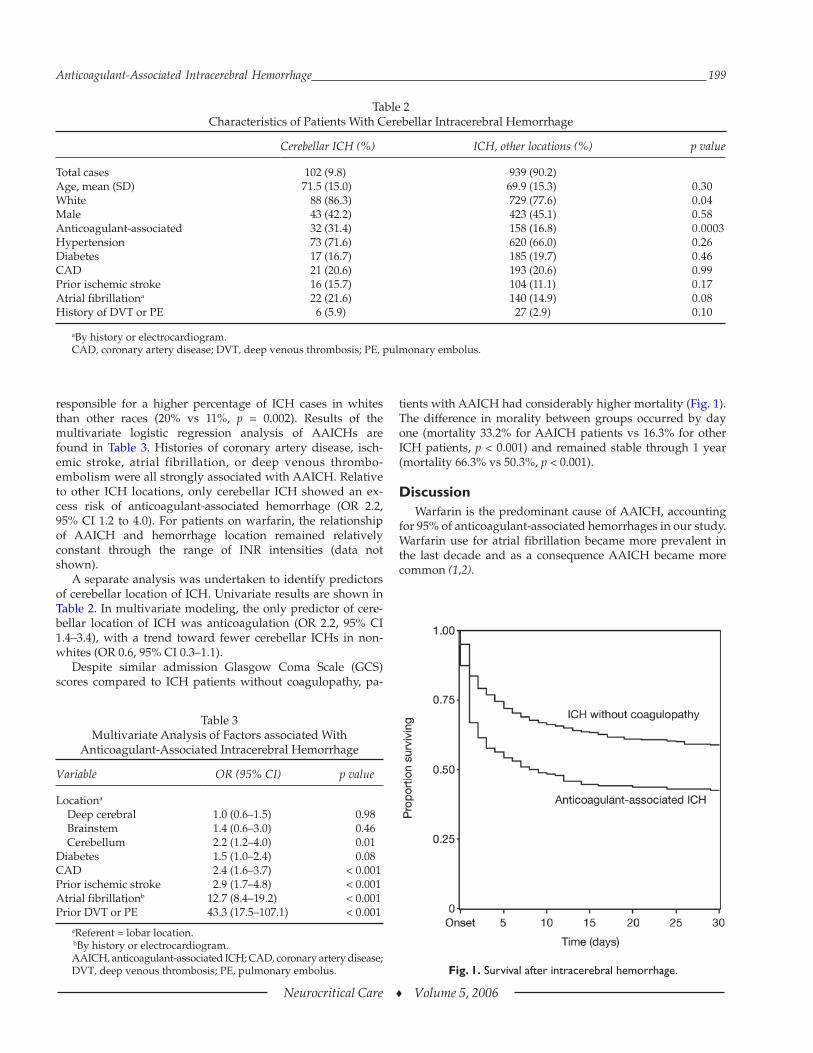
Despite similar admission Glasgow Coma Scale (GCS) scores compared to ICH patients without coagulopathy, pa-
tients with AAICH had considerably higher mortality (Fig. 1). The difference in morality between groups occurred by day one (mortality 33.2% for AAICH patients vs 16.3% for other ICH patients, p < 0.001) and remained stable through 1 year (mortality 66.3% vs 50.3%, p < 0.001).
DiscussionWarfarin is the predominant cause of AAICH, accounting
for 95% of anticoagulant-associated hemorrhages in our study. Warfarin use for atrial fibrillation became more prevalent in the last decade and as a consequence AAICH became more common (1,2).
Table 2Characteristics of Patients With Cerebellar Intracerebral Hemorrhage
Cerebellar ICH (%) ICH, other locations (%) p value
Total cases 102 (9.8) 939 (90.2)Age, mean (SD) 71.5 (15.0) 69.9 (15.3) 0.30White 88 (86.3) 729 (77.6) 0.04Male 43 (42.2) 423 (45.1) 0.58Anticoagulant-associated 32 (31.4) 158 (16.8) 0.0003Hypertension 73 (71.6) 620 (66.0) 0.26Diabetes 17 (16.7) 185 (19.7) 0.46CAD 21 (20.6) 193 (20.6) 0.99Prior ischemic stroke 16 (15.7) 104 (11.1) 0.17Atrial fibrillationa 22 (21.6) 140 (14.9) 0.08History of DVT or PE 6 (5.9) 27 (2.9) 0.10
aBy history or electrocardiogram.CAD, coronary artery disease; DVT, deep venous thrombosis; PE, pulmonary embolus.
Table 3Multivariate Analysis of Factors associated With
Anticoagulant-Associated Intracerebral Hemorrhage
Variable OR (95% CI) p value
Locationa
Deep cerebral 1.0 (0.6–1.5) 0.98 Brainstem 1.4 (0.6–3.0) 0.46 Cerebellum 2.2 (1.2–4.0) 0.01Diabetes 1.5 (1.0–2.4) 0.08CAD 2.4 (1.6–3.7) < 0.001Prior ischemic stroke 2.9 (1.7–4.8) < 0.001Atrial fibrillationb 12.7 (8.4–19.2) < 0.001Prior DVT or PE 43.3 (17.5–107.1) < 0.001
aReferent = lobar location. bBy history or electrocardiogram.AAICH, anticoagulant-associated ICH; CAD, coronary artery disease;DVT, deep venous thrombosis; PE, pulmonary embolus. Fig. 1. Survival after intracerebral hemorrhage.

200 Flaherty et al.
Neurocritical Care ♦ Volume 5, 2006
Risk factors for AAICH in trials and case-control studies have included increasing age, increasing intensity of antico-agulation, hypertension, prior ischemic stroke, and leukoara-iosis (5). In our cohort, patients with AAICH were more likely than ICH patients without coagulopathy to have medi-cal comorbidities and vascular risk factors. This is not sur-prising, as these comorbidities often prompt warfarin use. Whereas blacks in the United States have significantly higher rates of ICH than whites, AAICH accounted for a higher per-centage of all ICH in whites than blacks (3). This association became nonsignificant in multivariate analysis, suggesting the explanation lies in the epidemiology of atrial fibrillation and hypertension. Atrial fibrillation becomes more prevalent with increasing age and is more common in whites than blacks (6). Higher community rates of atrial fibrillation (and presumably warfarin use) among whites are likely counter-balanced by a higher prevalence of hypertension among blacks (7).
Whether AAICH has a predilection for particular brain regions has been debated with conflicting data from small studies. Kase and colleagues reported a preponderance of cerebellar hemorrhages in their experience (24 total AAICHs), but other reports have produced conflicting results (8,9). Our study shows a clear excess of AAICH in the cerebellum. Despite the association of amyloid angiopathy and lobar ICH, we did not find a special propensity for AAICH in this loca-tion. Amyloid angiopathy might increase the risk of AAICH because of its association with cerebral microbleeds and its tendency to induce vessel fragility, but it appears that other risk factors such as hypertension predispose patients to AAICH in other locations and have an equal or greater impact (10). The cerebellum can be affected by amyloid angiopathy and chronic hypertension and these factors may act synergisti-cally in this location (11).
It should be noted that for this report, we compared predic-tors of AAICH and cerebellar location of hemorrhage only among patients with ICH (and not a control population of stroke-free patients). Therefore, risk factors that are ubiquitous in ICH, such as age and hypertension, did not emerge in our modeling.
Despite similar admission GCS scores, our AAICH patients had significantly higher mortality rates than ICH patients without coagulopathy. The excess mortality (an absolute increase of approximately 17%) accrued the first day after hemorrhage and subsequently remained stable (Fig. 1). In agreement with data from Rosand and colleagues, a previous analysis of our population showed anticoagulation to be an independent predictor of mortality after ICH (2,12). We have not previously analyzed the timing of mortality following AAICH. Our results show that interventions to improve out-come of AAICH relative to ICH without coagulopathy needs to occur within 24 hours. We do not have more detailed mortality data to define how many hours after ictus mortality curves become parallel.
Prior studies have not agreed about whether ICH without coagulopathy and AAICH are of similar size upon presenta-tion (13–16). Hematoma expansion is a determinant of deterio-ration following ICH and at least one study has shown more delayed hematoma expansion among anticoagulated patients than those without coagulopathy (15). Because we did not re-
cord hemorrhage size, we cannot determine whether larger hematoma size upon presentation, more frequent hematoma expansion after presentation, or both factors contribute to the excess mortality associated with AAICH. It is also likely that the greater average age and the medical comorbidities of AAICH patients contribute to their poor outcomes. Finally, we cannot determine how preconceived notions of outcome and the withdrawal of care by clinicians (the “self-fulfilling proph-ecy”) affected mortality (17).
We included only patients with first-ever ICH and so can-not determine the relationship between warfarin and recur-rent ICH. Patients with recurrent ICH in a lobar location are likely to have amyloid angiopathy and may be at greater risk of anticoagulant-associated hemorrhage than patients in our cohort.
Current treatment of AAICH is empiric and little evidence-based data exists to guide management. Recently, several case series have described the off-label use of recombinant acti-vated factor VII (rFVIIa) for AAICH (18,19). Given the pro-thrombotic potential of rFVIIa as well as the advanced age and high prevalence of medical comorbidities and vascular risk factors among AAICH patients, we believe that a randomized trial comparing rFVIIa to standard care for AAICH is neces-sary before its routine use can be justified.
AcknowledgmentSupported in part by NINDS (R-01-NS 36695).
References 1. Smith NL, Psaty BM, Furberg CD, et al. Temporal trends in the
use of anticoagulants among older adults with atrial fibrillation. Arch Intern Med 1999;159:1574–1578.
2. Flaherty ML, Haverbusch M, Sekar P, et al. Long-term mortality after intracerebral hemorrhage. Neurology 2006;66:1182–1186.
3. Flaherty ML, Woo D, Haverbusch M, et al. Racial variations in location and risk of intracerebral hemorrhage. Stroke 2005;36:934–937.
4. Fang MC, Chang Y, Hylek EM, et al. Advanced age, anticoagula-tion intensity, and risk for intracranial hemorrhage among pa-tients taking warfarin for atrial fibrillation. Ann Intern Med 2004;141:745–752.
5. Hart RG, Tonarelli SB, Pearce LA. Avoiding central nervous sys-tem bleeding during antithrombotic therapy. Stroke 2005;36:1588–1593.
6. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults. National implications for rhythm management and stroke prevention: The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) study. JAMA 2001;285:2370–2375.
7. Burt VL, Whelton P, Roccella EJ, et al. Prevalence of hypertension in the US adult population. Results from the third National Health and Nutrition Examination Survey, 1988–1991. Hyperten-sion 1995;25:305–313.
8. Hart RG, Boop BS, Anderson DC. Oral anticoagulants and intra-cranial hemorrhage. Facts and hypotheses. Stroke 1995;26:1471–1477.
9. Kase CS, Robinson K, Stein RW, et al. Anticoagulant- related intracerebral hemorrhage. Neurology 1985;35:943–948.
10. Hart RG. What causes intracerebral hemorrhage during warfarin therapy? Neurology 2000;55:907–908.
11. Mann DM, Jones D, Prinja D, Purkiss MS. The prevalence of amyloid (a4) protein deposits within the cerebral and cerebellar cortex in Down’s syndrome and Alzheimer’s disease. Acta Neuropathol (Berl) 1990;80:318–327.

Anticoagulant-Associated Intracerebral Hemorrhage 201
Neurocritical Care ♦ Volume 5, 2006
12. Rosand J, Eckman MH, Knudsen KA, Singer DE, Greenberg SM. The effect of warfarin and intensity of anticoagulation on outcome of intracerebral hemorrhage. Arch Intern Med 2004;164:880–884.
13. Radberg JA, Olsson JE, Radberg CT. Prognostic parameters in spontaneous intracerebral hematomas with special reference to anticoagulant treatment. Stroke 1991;22:571–576.
14. Neau JP, Couderq C, Ingrand P, Blanchon P, Gil R, and the VGP Study Group. Intracranial hemorrhage and oral anticoagulant treatment. Cerebrovasc Dis 2001;11:195–200.
15. Flibotte JJ, Hagan N, O’Donnell J, Greenberg SM, Rosand J. Warfarin, hematoma expansion, and outcome of intracerebral hemorrhage. Neurology 2004;63:1059–1064.
16. Franke CL, de Jonge J, van Swieten JC, Op de Coul AA, van Gijn J. Intracerebral hematomas during anticoagulant treatment. Stroke 1990;21:726–730.
17. Becker KJ, Baxter AB, Cohen WA, et al. Withdrawal of support in intracerebral hemorrhage may lead to self-fulfilling prophecies. Neurology 2001;56:766–772.
18. Freeman WD, Brott TG, Barrett KM, et al. Recombinant factor VIIa for rapid reversal of warfarin anticoagulation in acute intracranial hemorrhage. Mayo Clin Proc 2004;79:1495–1500.
19. Brody DL, Aiyagari V, Shackleford AM, Diringer MN. Use of recombinant factor VIIa in patients with warfarin-associated intracranial hemorrhage. Neurocrit Care 2005;2:263–267.