lip cancer and reconstruction - university of texas … cancer and reconstruction naren n....
TRANSCRIPT

Lip Cancer and Reconstruction
Naren N Venkatesan MD
Faculty Advisor Raghu Athre MD
University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
December 2011
Overview
bull Anatomy
bull Function
bull Lip Cancer
ndash Brief Facts
ndash PathologyStaging
ndash Treatment
bull Key Flaps for Reconstruction
Anatomy
Melolabial crease
Labiomandibular crease
Red Lip
White Lip Vermillion Border
Mental Crease
Anatomy
Philtral Ridge
Anatomy
Anatomy
Arterial Details
bull Course of Facial Artery
ndash Branches off External Carotid Artery
ndash Courses across the mandible to the oral commissure
ndash Deep to Risorius and Superficial to Buccinator
ndash Can be found approximately 1 ndash 2 cm from oral commissure2
Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Overview
bull Anatomy
bull Function
bull Lip Cancer
ndash Brief Facts
ndash PathologyStaging
ndash Treatment
bull Key Flaps for Reconstruction
Anatomy
Melolabial crease
Labiomandibular crease
Red Lip
White Lip Vermillion Border
Mental Crease
Anatomy
Philtral Ridge
Anatomy
Anatomy
Arterial Details
bull Course of Facial Artery
ndash Branches off External Carotid Artery
ndash Courses across the mandible to the oral commissure
ndash Deep to Risorius and Superficial to Buccinator
ndash Can be found approximately 1 ndash 2 cm from oral commissure2
Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7
Anatomy
Melolabial crease
Labiomandibular crease
Red Lip
White Lip Vermillion Border
Mental Crease
Anatomy
Philtral Ridge
Anatomy
Anatomy
Arterial Details
bull Course of Facial Artery
ndash Branches off External Carotid Artery
ndash Courses across the mandible to the oral commissure
ndash Deep to Risorius and Superficial to Buccinator
ndash Can be found approximately 1 ndash 2 cm from oral commissure2
Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Melolabial crease
Labiomandibular crease
Red Lip
White Lip Vermillion Border
Mental Crease
Anatomy
Philtral Ridge
Anatomy
Anatomy
Arterial Details
bull Course of Facial Artery
ndash Branches off External Carotid Artery
ndash Courses across the mandible to the oral commissure
ndash Deep to Risorius and Superficial to Buccinator
ndash Can be found approximately 1 ndash 2 cm from oral commissure2
Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Anatomy
Anatomy
Arterial Details
bull Course of Facial Artery
ndash Branches off External Carotid Artery
ndash Courses across the mandible to the oral commissure
ndash Deep to Risorius and Superficial to Buccinator
ndash Can be found approximately 1 ndash 2 cm from oral commissure2
Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Anatomy
Arterial Details
bull Course of Facial Artery
ndash Branches off External Carotid Artery
ndash Courses across the mandible to the oral commissure
ndash Deep to Risorius and Superficial to Buccinator
ndash Can be found approximately 1 ndash 2 cm from oral commissure2
Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Arterial Details
bull Course of Facial Artery
ndash Branches off External Carotid Artery
ndash Courses across the mandible to the oral commissure
ndash Deep to Risorius and Superficial to Buccinator
ndash Can be found approximately 1 ndash 2 cm from oral commissure2
Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Further Arterial Details
bull Superior Labial Artery ndash Deep to Zygomaticus Major ndash Gives of Angular artery then
enters orbicularis oris ndash Runs along upper lip and
anastamoses with opposite side
bull Inferior Labial Artery ndash Branches from Facial Artery
near the commissure ndash Deep to Depressor Angularis
Oris ndash Enters Orbicularis Oris and runs
along lower lip to anastamose with opposite side
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7
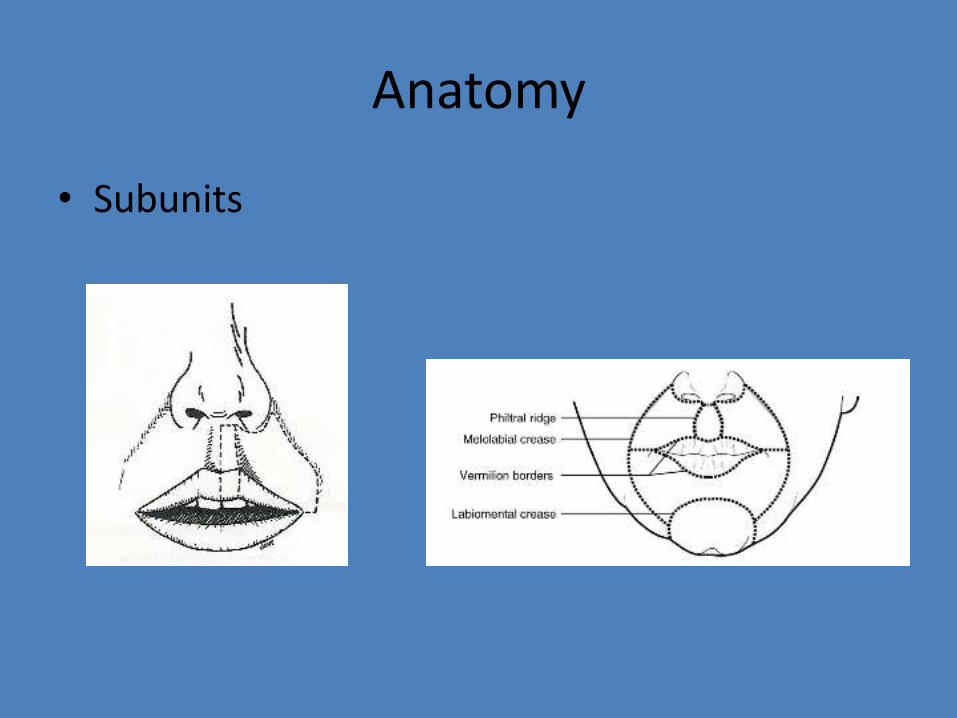
Anatomy
bull Subunits
Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Functional Importance
bull Roles
ndash Oral Competence
ndash Deglutition
ndash Expression of Emotions
ndash Speech ndash required for 6 consonants
bull Purely Labial ndash ldquobrdquo ldquomrdquo ldquowrdquo ldquoprdquo
bull Labial-Dental ndash ldquofrdquo ldquovrdquo
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7
Functional Importance
bull Another key factor to consider prior to reconstruction is the patientrsquos dentition
bull Edentulous patients pose an important challenge to reconstruction as only a mild degree of microstomia may be acceptable if dentures are worn
Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Lip Cancer Staging and Treatment
Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Lip Cancer Facts
bull Lip Cancer Incidence ndash 1-2 1
bull Most Common Oral Cavity Cancer
bull Risk Factors
ndash Prolonged Sun Exposure
ndash Male
ndash Pipe-smokingTobacco Chewing
ndash Alcohol consumption
Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Lip Cancer
bull gt 90 is on red lip
bull 90 is on Lower Lip
bull 90 is Squamous Cell Carcinoma
bull Basal Cell Carcinoma occurs more commonly on Upper Lip
bull Excellent 5-year prognosis if lt 2 cm
Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Lip Cancer
bull Squamous Cell Carcinoma ndash Mainly on Red Lip
bull Basal Cell Carcinoma ndash Mainly on Cutaneous White Lip
bull Rarer Types ndash Adenocarcinoma ndash secondary to minor salivary gland
presence
ndash Melanoma
ndash Lymphoma
ndash Sarcoma
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7
Lip Cancer
bull Upper Lip spreads to ipsilateral lymph nodes ndash Levels I ndash III
ndash Embryologic fusion in the midline prevents contralateral spread
bull Lower Lip spreads to ipsilateral and contralateral lymph nodes ndash Levels I - III
Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Staging of Lip Cancer
bull T1 primary tumor lt2 cm
bull T2 primary tumor 2ndash4 cm
bull T3 primary tumor gt4 cm
bull T4 primary tumor invades adjacent structures (eg through cortical bone skin through floor of mouth)
Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Treatment of Lip Cancer
bull Surgical Treatment is Mainstay
ndash Need 05 cm margins around tumor
bull Neck Dissection is often performed in conjunction especially if lower lip cancer
ndash Elective Supraomohyoid neck dissection for N0 necks
ndash Levels I-IV neck dissection for N1-N3 disease
Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Radiation Therapy for Lip Cancer
bull Radiation Therapy
ndash May be used as primary treatment if T1 or non-operable patient
ndash Also used for
bull post-operative XRT for advanced stages
bull close margins
bull extracapsular extension
bull perineuralintravascular invasion
Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Reconstruction
Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Upper Lip Algorithm
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7
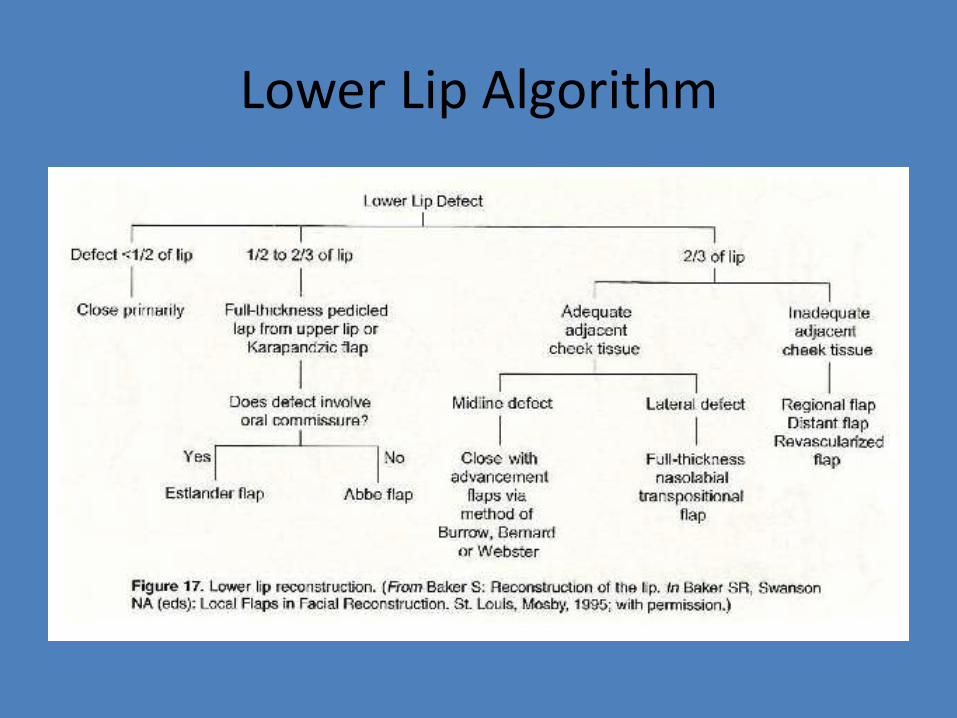
Lower Lip Algorithm
Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Reconstruction Options
bull Small Defect
ndash Wedge Excision ndash Primary closure
ndash Local V-Y flaps can also be used for very small defects
Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Full Thickness Excision Wedge Resection
bull Best suited for Lesions smaller than frac12 the lip
bull Can be closed as a V or W
bull Good functional and aesthetic outcome
bull Key is to re-approximate the vermillion border appropriately
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Full Thickness Excision Wedge Resection
Pictures courtesy of Dr Etai Funk
Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Reconstruction Options
bull Large Defect
ndash Mucosal Advancement Flap
ndash Abbeacute Flap
ndash Estlander-Abbeacute Flap
ndash Karapandzic Flap
ndash Gilles Fan Flap (Nasolabial)
ndash Radial Forearm Free Flap
Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Mucosal Advancement Flap
bull For use only in lesions of the red lip
bull Favored method for restoration of the vermillion
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7
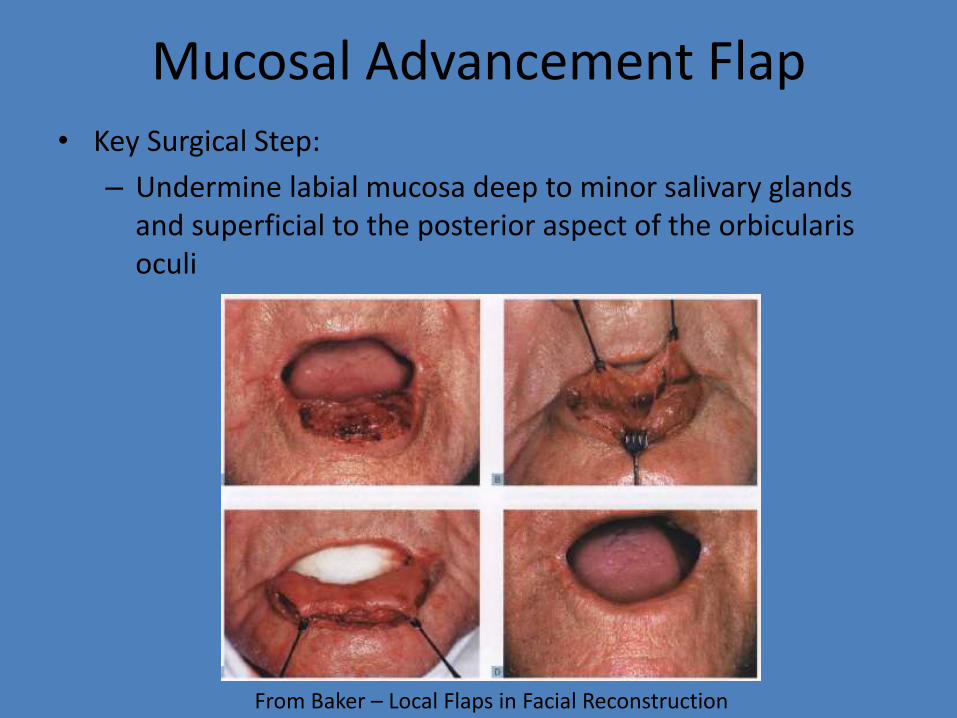
Mucosal Advancement Flap bull Key Surgical Step
ndash Undermine labial mucosa deep to minor salivary glands and superficial to the posterior aspect of the orbicularis oculi
From Baker ndash Local Flaps in Facial Reconstruction
Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Mucosal Advancement Flap
bull Concerns
ndash Advanced mucosa may display a deeper red color than natural vermillion
ndash Difficult to approximate vermillion line if lip skin is involved
ndash Contracture of flap can lead to inversion of lip
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Mucosal Advancement Flap
Pictures Courtesy of Dr Athre
Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Abbeacute Flap
bull Flap is based on the principle of creating a pedicle from the lip without the lesion to the area of the defect
bull Based of the arterial supply of the labial artery ndash either superior or inferior
bull Ideal for lesions involving 13 ndash 23 of the lip
bull Lesions must not involve the commissure
Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Abbeacute Steps (Cross Lip Flap)
bull Surgical Steps ndash 1 Draw defect on affected lip
ndash 2 Draw the flap on the opposite lip to be half the width of the defect
ndash 3 Make the full-thickness incision
ndash 4 Rotate the flap 180 degrees
ndash 5 Suture flap with each individual layer
ndash 6 Dress wound to minimize tension
ndash 7 Divide pedicle at 14-21 days
Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Abbeacute Flap
Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Abbeacute Flap
Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Abbeacute Flap
Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Estlander Flap
bull Similar to Abbeacute Flap
bull Key is that the Estlander Flap involves the commissure
Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Estlander Flap
Pictures courtesy of Dr Patt
Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Estalander Flap
Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Estlander Flap
Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Estlander Flap
Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Karapandzic Flap
Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Karapandzic
bull Indications
ndash Defects less than frac12 of upper lip
ndash Defects less than 23 of lower lip
ndash Full thickness defects
ndash Best suited for rectangular defects of the central lower lip
Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Karapandzic
bull Key Surgical Steps
ndash Superiorly continue the incisions into the nasolabial fold
ndash Raise only skin and mucosa
ndash May selectively cut portions of the orbicularis oris near the original commissure
bull Advantage
ndash Preserves perioral sensation and function of the orbicularis oris by saving CN V3 and VII
bull Disadvantage
ndash Risk of Microstomia (directly proportional to size of defect)
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Karapandzic Flap
Pictures Courtesy of Dr Moody and Dr Lies
Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Nasolabial Transpositional Flap
bull Aka Gilles Fan Flap
bull Rotation-Advancement Flap
bull Rotate the flap around the commissure to create a neo-commissure
bull Useful with upper lip lesions
Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Gillies Flap
bull Surgical Steps ndash 1 For lower lip start with full thickness incision
medial to defect
ndash 2 Then continue the full thickness incision laterally and around the commissure
ndash 3 Then follow the melolabial fold
ndash 4 Then carry the incision down to the superior vermillion border
ndash 5 Advance flap and suture individual layers together
Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Nasolabial Flap
Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Nasolabial Flap
Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Radial Forearm Free Flap bull Selected for Large Full-
Thickness Defects
bull Can be performed with the Palmaris Longus Tendon
bull Skin Paddle is used to cover both the lip skin and oral mucosal defect
bull Palmaris Longus Tendon is transected within 5 cm of either end of the flap
bull Secure the Palmaris Longus Tendon into the Orbicularis Oris Muscle
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Radial Forearm Free Flap
Pictures courtesy of Dr Athre
Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Upper Lip Algorithm
Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Lower Lip Algorithm
Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Pictures
Thanks to
- Dr Athre
- Dr Lies and Dr Moody
- Dr Funk
- Dr Patt
Other pictures and drawings were taken from Baker
Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7

Bibliography
bull Papel I et al Facial Plastic and Reconstructive Surgery Chapter 51 Lip Reconstruction Thieme Publishing New York NY 2002 634-645
bull Baker SR et al Local Flaps in Facial Reconstruction Chapter 19 Reconstruction of the Lip Mosby Elsevier Philadelphia PA 2007 475-524
bull Dolan RW et al Facial Plastic Reconstructive and Trauma Surgery Chapter 7 Specialized Local Facial Flaps for the Eyelids and Lips Marcel Dekker Inc New York NY 2003 201-232
bull Pasha R et al Otolaryngology Head and Neck Surgery Clinical Reference Guide Chapter 5 Head and Neck Cancer Singular San Diego CA 2001 239-243
bull 1Moretti A et al Surgical Management of Lip Cancer Acta Otorhinolaryngol Ital 2011 February 31(1) 5ndash10 bull 2Schulte DL Sherris DA Kasperbauer JL The anatomical basis of the Abbeacute flap Laryngoscope 2001
Mar111(3)382-6 bull McCarn KE Park SS Lip reconstruction Otolaryngol Clin North Am 2007 Apr40(2)361-80 bull Jeng SF Kuo YR Wei FC Su CY Chien CY Total lower lip reconstruction with a composite radial forearm-palmaris
longus tendon flap a clinical series Plast Reconstr Surg 2004 Jan113(1)19-23 bull Abbeacute RA A new plastic operation for the relief of deformity due to double hairlip Med Rec 188953447 bull Estlander JA Eine Methods ans der einen Lippe substanzverluste der anderen zu ersetzen Arch Klin Chir 187214
622 bull Karapandzic M Reconstruction of lip defects by local arterial flaps Br J Plast Surg 19742793-7 bull Freedman A M and Hidalgo D A Full-thickness cheek and lip reconstruction with the radial forearm free flap
Ann Plast Surg 25 287 1990 bull Daya M Nair V Free radial forearm flap lip reconstruction a clinical series and case reports of technical
refinements Ann Plast Surg 2009 Apr62(4)361-7