linfomi - ematologialasapienza.it settembre/pdf/2… · linfomi umberto vitolo hematology...
TRANSCRIPT

Linfomi
Umberto VitoloHematology
University Hospital Città della Salute e della Scienza
Torino, Italy

Disclosures – Umberto Vitolo
Research Support/P.I. Roche, Celgene, Mundipharma
Employee N/A
Consultant N/A
Major Stockholder N/A
Conferences/Educational Activities
Janssen, Roche, Celgene, Pfizer,
Takeda
Scientific Advisory Board
Janssen, Roche, Celgene

Outline of discussion
• First line treatment in young MCL
• Relapsed MCL
• Rituximab subcute in DLCL
• Relapsed Hodgkin’s lymphoma: standard
agents
• Relapsed Hodgkin’s lymphoma: treatment wih
T-cell check point blockade
• Relapsed DLBCL: inhibitor nuclear export

1st line Induction Treatment
CR/Cru
or PR
ObservationB
LenalidomideA
Consolidation
QuickTime™ and aGIF decompressor
are needed to see this picture.
Arm A: Lenalidomide, once daily on days 1-21, every 28-days
Arm B: Observation with no any active drugs for MCL
R
Randomization within 120 days after the end of consolidation
Advanced MCL
5.
A phase III multicenter, randomized study
with Lenalidomide (Revlimid®) maintenance versus observation
after intensified induction regimen containing rituximab
followed by high dose chemotherapy and Autologous Stem Cell Transplantation as first line
treatment in adult patients with advanced Mantle Cell Lymphoma
Sergio Cortelazzo, MD on behalf of FIL
Unit of Oncology-Hematology, Humanitas
Bergamo, Italy

Restaging
Restaging
R-HD-Ara-C 2g/m2 q12h x 3
Ritux 375mg/m2 d 4, 10
3. Maintenance:
Phase 3, 1:1 Randomized, comparative, observation-controlled study after completion of intensive immunochemotherapy followed by ASCT
Staging
Restaging
2. Consolidation:
1. Induction:
PR <50%, SD, NROff-study
CR/PR
MRD
MRD
MRD
MRD
MRD
Harvest CD34+
2° Harvest CD34+
R-HD-Ara-C 2g/m2 q12h x 3
Ritux 375mg/m2 d 4, 10
BEAM-PBSCT
R-CHOP-21 x 3
CTX 4g/m2
?DECISION MAKING
RANDOM observation vs. lenalidomide
15 mg (plts >100x109/ L) or 10 mg (plts 60-100x109/L ) once daily on days 1-21 every 28 day cycle) for 24 months.
QuickTime™ and aGIF decompressor
are needed to see this picture.
6.
High-Dose Sequential
Chemotherapy+R (R-HDS)

Response
Final Response (includingIntermediate+Final Response)
R-HDC+ASCT
n = 228
CR/CRu 178(78%)
PR 18 (8%)
SD 3 (1%)
NR/PG 15 (7%)
Deaths during treatment* 7 (3%)
Interruption not due to PD or death
7(3%)
* One not related to treatment: road accident
67%
24%
1%
3%
2%
3%
CR PR SD PD Death Other
Restaging 1 – after Induction+hd-CTX
67%20%
2%
4%
2% 5%
CR PR SD PD Death Other
Restaging 2 – after hd-Ara-C
6%
77%
3%
8%
6%
0%
CR PR SD PD Death Other
Restaging 3 – afer ASCT
10.
QuickTime™ and aGIF decompressor
are needed to see this picture.

BONE MARROW
0
20
40
60
80
100
R-CHOP LK1 LK2 preASCT postASCT
MRD+
MRD-
43%
73%
27%
56%
44%
78%82%
57%
18%
PERIPHERAL BLOOD
22%
0
20
40
60
80
100
R-CHOP preASCT postASCT
MRD+
MRD-
36%
64%
31%
69%
68%
32%
MRD by ASO RQ-PCR on 100 patients
Patients with molecular marker: 249/283 (88%) IGH + 192/283 (69%) BCL-1 + 101/283 (36%)
1st LK: 152/192 MRD- (79%)
2nd LK: 14/35 MRD- (40%)
MRD assessed by ASO nested-PCR
12.

2-year PFS: 77.7% (95% CI:71.1-83.0)2-year OS: 89.2% (95% CI: 83.7-92.9)
median follow-up 22 months
QuickTime™ and aGIF decompressor
are needed to see this picture.
14.
0.00
0.25
0.50
0.75
1.00
270 226 180 138 106 67 44 26 4 3 0 At risk:
0 6 12 18 24 30 36 42 48 54 60Months from Enrollment
2y PFS 78%
0.00
0.25
0.50
0.75
1.00
270 234 189 150 118 79 49 31 8 4 0 At risk:
0 6 12 18 24 30 36 42 48 54 60Months from Enrollment
2 y OS 89.2%

2-year PFS for MIPI low, intermediate and high
CG Gaisler, Haematologica, 2010
M Magni et al., Bone Marrow Transplant, 2009
15.
QuickTime™ and aGIF decompressor
are needed to see this picture.
0.00
0.25
0.50
0.75
1.00
128 116 99 74 56 38 26 17 2 1 0Low74 61 46 39 29 18 10 6 1 1 0Intermed.52 39 29 20 17 9 6 2 1 1 0High
At risk:
0 6 12 18 24 30 36 42 48 54 60Months from Enrollment
High
Intermed.
Low
P=0.0076

Outline of discussion
• First line treatment in young MCL
• Relapsed MCL
• Rituximab subcute in DLCL
• Relapsed Hodgkin’s lymphoma: standard
agents
• Relapsed Hodgkin’s lymphoma: treatment wih
T-cell check point blockade
• Relapsed DLBCL: inhibitor nuclear export

Lenalidomide†
25 mg/day PO, days 1-21, q28d (until PD or toxicity)
CT scans every
56 days for
6 months, then
every 90 days
thereafter
Primary endpoint: PFS (per independent central review)Secondary endpoints: ORR, DOR, OS, safety, and QOL
Control: Investigator’s choice
If PD
Crossover tolenalidomide
Chlorambucil or rituximab until PD or toxicityCytarabine, fludarabine, or gemcitabine for ≤6 cycles
NCT00875667; data cut-off March 7, 2014.*≥1 prior combination chemotherapy with an alkylating agent and either an anthracycline and/or cytarabine and/or fludarabine (± rituximab); ≤3 relapses or failure of prior therapy and ineligible for intensified treatment or SCT.†Prophylaxis for all lenalidomide patients included aspirin or low molecular weight heparin, warfarin, or equivalent prophylaxis for thromboembolic events and allopurinol or equivalent with oral hydration during the first 7 days for tumor lysis syndrome.
R/R MCL (N = 254)• Pretreatment*• ECOG PS 0-2• Cyclin D1 or t(11;14)• Measurable disease ≥2
cm
Ran
do
miz
atio
n
Stratification • <3 or ≥3 years from
diagnosis• <6 vs. ≥6 months from
last systemic anti-lymphoma therapy
• Prior SCT
2:1
Impact of Prior Treatment on PFS for R/R MCL Patients Randomized to Lenalidomide vs. Investigator’s Choice: A Subgroup Analysis of the
MCL-002 (SPRINT) Study: Marek Trněný, MD, PhD1

MCL-002: Overall Efficacy (ITT, central review)
Efficacy Lenalidomide (n = 170) IC (n = 84) P value
Median PFS, months (95% CI)*
8.7 (5.5-12.1) 5.2 (3.6-6.9) 0.004
HR = 0.61 (95% CI, 0.44-0.84); P = 0.004
ORR, n (%) 68 (40) 9 (11) <0.001
CR/CRu, n (%) 8 (5) 0 0.043
PR, n (%) 60 (35) 9 (11) —
PD, n (%) 34 (20) 26 (31) —
Median DOR, months (95% CI)
16.0 (9.5-20.0) 10.4 (8.4-18.6) —
Median OS, months (95% CI)
27.8 (20.0-36.9) 21.2 (16.0-28.9) —
• Lenalidomide treatment significantly improved PFS, ORR, and CR/CRu vs. IC
ITT, included all randomized patients irrespective of whether they received study treatment. Data cut-off March 7, 2014.*No response evaluations for several patients in each arm; however, they still contributed to PFS.

13
MCL-002: Progression-Free Survival (Central Review)
• At a median follow-up of 15.9 months, lenalidomide-treated patients
showed a 39% reduction in the risk of progression or death vs. IC,
reflected as an estimated improvement in median PFS of 3.5 months
Lenalidomide
(n = 170)
IC
(n = 84)
Median PFS, mo (95% CI) 8.7 (5.5-12.1) 5.2 (3.6-6.9)
HR (95% CI) 0.61 (0.44-0.84); P = 0.004
Number of patients at risk
Lenalidomide
IC
170
84
86
31
63
15
36
7
27
5
20
4
16
4
12
2
7
0
1 1 0
1.0
0.8
0.6
0.4
0.2
0.0
Su
rviv
al P
rob
ab
ility
Progression-Free Survival, months
0.1
0.3
0.5
0.7
0.9
0 5 10 15 20 25 30 35 40 45 50 55
LenalidomideIC
ITT patients; data cut-off March 7, 2014.

14
MCL-002: Prior Treatment Subgroup Analysis for PFS
Patients, n/N Median PFS, wk
Log-rank P HR (95% CI)Subgroup Len IC Len IC
Time from MCL
diagnosis to
first treatment
<3 years
≥3 years61/91
45/76
30/44
29/39
37.6
39.3
15.1
26.3
0.022
0.052
No. of prior
systemic
therapies
1
2
≥3
30/55
44/70
32/45
20/37
18/23
21/24
52.9
26.6
24.0
40.7
19.4
10.0
0.321
<0.001
0.006
No. of prior
relapses
<2
≥269/112
37/58
28/47
31/37
48.7
24.1
25.9
19.3
0.280
0.003
Time from last
prior therapy
<6 months
≥6 months50/71
56/95
26/36
33/47
25.1
50.6
21.6
24.7
0.061
0.030
Time from last
rituximab to
1st dose
<230 days
≥230 days49/64
50/89
24/33
29/42
26.6
50.6
19.3
24.7
0.223
0.025
Central review of ITT patients; data cut-off March 7, 2014.
• Significant improvements in PFS favored lenalidomide over IC for <3 years
from MCL diagnosis, ≥2 prior systemic therapies or relapses,
≥6 months from last therapy, and ≥230 days from last rituximab dose
0 1
2

15
MCL-002: Prior Treatment Subgroup Analysis for PFS
cont.
Patients, n/N Median PFS, wk
Log-rank P Subgroup Len IC Len IC HR (95% CI)
Response
status to last
therapy
Refractory
Relapsed45/70
61/100
19/25
40/59
32.7
48.7
7.4
26.3
<0.001
0.143
Prior SCTYes
No17/30
89/140
12/18
47/66
52.9
37.6
19.4
24.7
0.534
0.003
Prior HDT*Yes
No18/31
88/139
12/18
47/66
52.9
37.6
19.4
24.7
0.594
0.002
Type of prior
therapy†
Rituximab
Ara-C
Fludarabine
99/156
39/62
37/53
54/77
24/32
11/16
39.3
22.3
22.3
24.7
19.4
18.6
0.008
0.303
0.075
• Significant improvements in PFS favored lenalidomide over IC for patients with
prior refractory disease, no prior SCT/HDT, and prior rituximab
*HDT includes SCT, hyperCVAD, and R-hyperCVAD. †Most frequent (≥20%) prior therapy in addition to alkylator/anthracycline.
Central review of ITT patients; data cut-off March 7, 2014.
0 1 2

Outline of discussion
• First line treatment in young MCL
• Relapsed MCL
• Rituximab subcute in DLCL
• Relapsed Hodgkin’s lymphoma: standard
agents
• Relapsed Hodgkin’s lymphoma: treatment wih
T-cell check point blockade
• Relapsed DLBCL: inhibitor nuclear export

Stratification by age (<60/≥60 years)
IPI category (low/low-intermediate/high-intermediate/high)
Chemotherapy regimen (CHOP-14/CHOP-21)
*Selected by investigators
**Cheson 1999 criteria
IPI, International Prognostic Index; PD, progressive disease; SD, stable disease
Untreated
CD20+ DLBCL (N=572)
Age 18–80 years
IPI score 1–5 or
IPI 0 with bulky
disease
INTERIM
STAGING
RESPONSE
ASSESSMENT**
SD, PD:
off study
R
A
N
D
O
M
I
S
E
2:1
Rituximab IV
(375 mg/m2)
Rituximab SC
(1400 mg)
n=378
n=194
1 x rituximab IV followed by 7 x rituximab SC
+
6 or 8 CHOP-14 / 6 or 8 CHOP-21*
8 x rituximab IV
+
6 or 8 CHOP-14 / 6 or 8 CHOP-21*
Subcutaneous versus intravenous rituximab in combination with CHOP for previously untreated diffuse large B-cell lymphoma: efficacy and safety results from the phase IIIb MabEase study

At risk
SC, n 342 342 342 322 316 303 264 217 296 183 168 160 135 113 101 88 83 72 44 32 21 11 4 2 1 0
IV, n 177 177 176 169 163 159 141 115 107 97 94 84 72 62 57 48 41 33 20 15 9 6 4 2 0 0
Progression-free survival (ITT)
KM, Kaplan-Meier; NR, not reached; PFS, progression-free survival
PFS was comparable between treatment arms
• The KM PFS curves were almost identical for rituximab SC (1400 mg) and IV (375 mg/m2)
1.0
0.0
Pro
babili
ty o
f P
FS
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Months
Median follow-up: 64 weeks
Censored n Censored Events Median
Rituximab SC 342 288 54 NR
Rituximab IV 177 149 28 NR

Administration time
Administration time was substantially shorter for rituximab SC
R-CHOP administration
at cycle 7Rituximab administration
by cycle

Adverse events grade ≥3 in cycle 2 or later (safety population)
AE of grade ≥3 in cycle 2 or later Rituximab SC Rituximab IV
Total number of patients with ≥1 AE of grade ≥3 195 (52.8%) 93 (49.5%)
Total number of events of grade ≥3 476 229
21,7
12,2
3,5 3,5 3,3
19,7
6,43,7 3,7
1.6
0,0
5,0
10,0
15,0
20,0
25,0
30,0
Neutropenia Febrile neutropenia Anaemia Leukopenia Pneumonia
Pa
tie
nts
(%
)
Rituximab SC (n=369)
Rituximab IV (n=188)
Similar safety profile in both arms, with no unexpected safety signals

Outline of discussion
• First line treatment in young MCL
• Relapsed MCL
• Rituximab subcute in DLCL
• Relapsed Hodgkin’s lymphoma: standard
agents
• Relapsed Hodgkin’s lymphoma: treatment wih
T-cell check point blockade
• Relapsed DLBCL: inhibitor nuclear export

Phase II Study of BEGEV [Bendamustine, Gemcitabine, Vinorelbine] as Induction Regimen Prior to ASCT in R/R HL
R. Mazza, A. Pulsoni, G. Rossi, C. Carlo-Stella, A. Anastasia, M. Bonfichi, C. Rusconi, F. Salvi, S. Luminari, A. Re, M. Gotti, A.M. Liberati, N. Di Renzo, L. Giordano, A. Santoro
on behalf of Fondazione Italiana Linfomi (FIL)
ClinicalTrials.gov Identifier: NCT01884441
Day Medication Dose Route
1 Gemcitabine 800 mg/sqm IV
Vinorelbine 20 mg/sqm IV
2 Bendamustine 90 mg/sqm IV
3 Bendamustine 90 mg/sqm IV
4 Gemcitabine 800 mg/sqm IV
Four cycles every 21 days
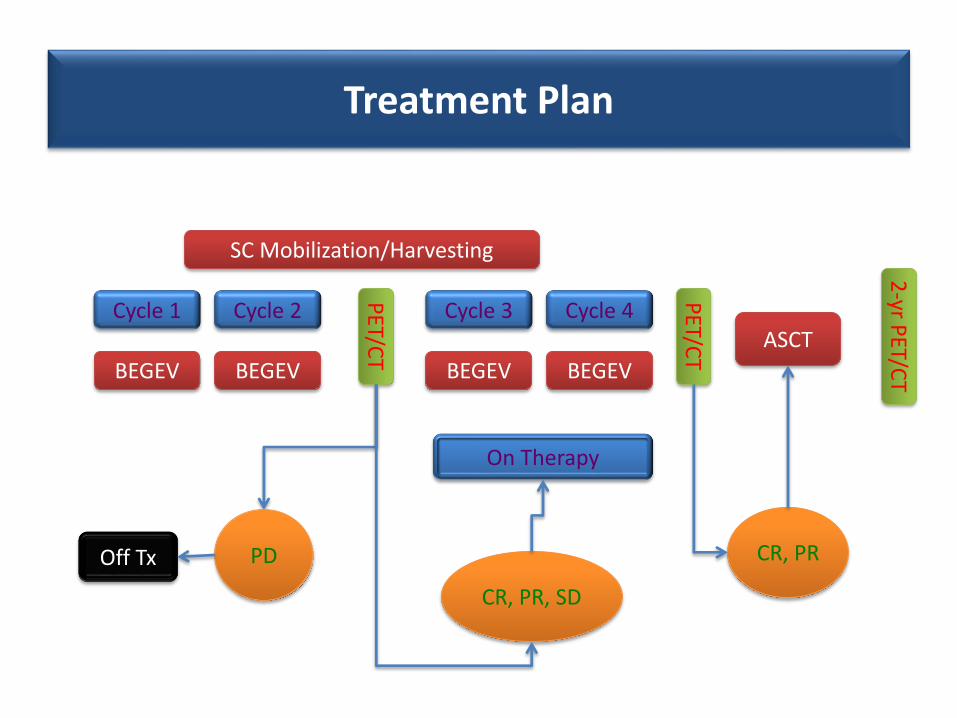
Treatment Plan
Cycle 1 Cycle 2 Cycle 4Cycle 3
BEGEV BEGEV BEGEV BEGEV
PET/C
T
PET/C
T ASCT
PDOff Tx
CR, PR, SD
On Therapy
2-yr P
ET/CT
SC Mobilization/Harvesting
CR, PR

Patient Characteristics Prior to BEGEV
Characteristics # %
Patients 59 100
M/F 31/28 52/48
Age, median (range) 33 (18 - 68) -
Response to primary therapyPrimary refractoryRelapsed disease
2732
4654
B symptomsYesNo
2732
46 54
Extranodal sites of diseaseYesNo
2435
4159
Relapsed diseaseCR < 1 yrCR > 1 yr
2210
6931

Overall Response and by Disease Status
Disease Status at
Study Entry CR + PR SD PD P
Relapse30
(94%)1
(3%)1
(3%)0.033*
Refractory19
(70%)- 8
(30%)
* CR-PR vs SD-PD
n %
Patients 59 100
CR 43 73
PR 6 10
SD 1 2
PD 8 13
Drop out 1 2

OS and PFS
0 10 20 30 40
0
20
40
60
80
100
Months
Overa
ll S
urv
ival (%
)
n = 59, 48 censoredMedian OS: not reached
0 10 20 30 40
0
20
40
60
80
100
Months
Overa
ll S
urv
ival (%
)n = 59, 38 censoredMedian PFS: 26 mos

G1 G2 G3 G4 TotalN % N % N %
Asthenia 5 8.5 0 0.0 5 8.5Skin 6 10.2 0 0.0 6 10.2
Hepatic 7 11.9 2 3.4 9 15.3Fever 5 8.5 7 11.9 12 20.3
Gastrointestinal 10 16.9 4 6.8 14 23.7Infection 9 15.3 4 6.8 13 22.0
G1 G2 G3 G4 totalN % N % N %
Anemia 3 5.1 2 3.4 5 8.5
Neutropenia 1 1.7 8 13.6 9 15.3
Thrombocytopenia 0 0.0 4 6.8 4 6.8
Piastinopenia 0 0.0 4 6.8 4 6.8
Adverse Events by Patients

Outline of discussion
• First line treatment in young MCL
• Relapsed MCL
• Rituximab subcute in DLCL
• Relapsed Hodgkin’s lymphoma: standard
agents
• Relapsed Hodgkin’s lymphoma: treatment wih
T-cell check point blockade
• Relapsed DLBCL: inhibitor nuclear export

• PD-1 is expressed on the surface of activated T cells
• Its ligands, PD-L1 and PD-L2, are overexpressed in certain tumor cells
• Binding of PD-1 to its ligands inhibits T-cell activation, allowing tumors to evade the immune response
PD-1 Pathway and Immune Surveillance
Nivolumab

Philippe Armand1, John Timmerman2, Alexander M. Lesokhin3, Ahmad Halwani4, Michael M. Millenson5, Stephen J. Schuster6, Martin Gutierrez7, Emma C. Scott8,
Deepika Cattry3, Gordon J. Freeman1, Bjoern Chapuy1, Azra H. Ligon9, Scott J. Rodig9, Lili Zhu10, Joseph F. Grosso10, Jason Simon10, Margaret A. Shipp1,
Adam D. Cohen6, Daniel Lebovic11, Madhav Dhodapkar12, David Avigan13, Stephen M. Ansell14, Ivan Borrello15
Nivolumab in Relapsed or Refractory Lymphoid Malignancies and
Classical Hodgkin Lymphoma: Updated Results of a Phase 1 Study
1Dana-Farber Cancer Institute, Boston, MA; 2Jonsson Comprehensive Cancer Center, University of California, Los Angeles, CA; 3Memorial Sloan Kettering Cancer Center, New York, NY; 4University of Utah Huntsman Cancer Institute, Salt Lake City, UT; 5Fox Chase Cancer
Center, Philadelphia, PA; 6Abramson Cancer Center, University of Pennsylvania, Philadelphia, PA; 7John Theurer Cancer Center, Hackensack University Medical Center, Hackensack, NJ; 8Oregon Health and Science University, Portland, Oregon; 9Brigham and
Women’s Hospital, Boston, MA; 10Bristol-Myers Squibb, Princeton, NJ; 11University of Michigan Hematology, Ann Arbor, MI; 12Yale Cancer Center, New Haven, CT; 13Beth Israel Deaconess Medical Center, Boston, MA; 14Mayo Clinic, Rochester, MN; 15Johns Hopkins University
School of Medicine and the Sidney Kimmel Comprehensive Cancer Center, Baltimore, MD
E H A 2 0 T H C O N G R E S S
J U N E 2 0 1 5
V I E N N A , A U S T R I A

Relapsed or Refractory Lymphoid Malignancies
(n=105)
•No autoimmune disease•No organ/stem cell allograft•No prior checkpoint blockade
Endpoints
Primary•Safety and Tolerability
Secondary•Best Overall Response•Objective Response•Duration of Response•Progression-free survival•Biomarker studies
Study Design
August 2012Start
June 2014(ASH 2014)
April 2015(EHA 2015)
Dose Escalation(n=13)
1 mg/kg 3 mg/kg
Dose Expansion(n=92)
3 mg/kg
Wk 1,4 then q2wk until PD, toxicity, CR or 2y
Classical Hodgkin (n=23)B-cell NHL (n=31)T-cell NHL (n=23)Myeloma (n=27)
CML (n=1)
• CA 209-039: Phase 1 study of nivolumab in lymphoid malignancies

Baseline Characteristics
CharacteristicMultipleMyeloma
(n=27)
B-cell NHL
(n=31)
T-cellNHL
(n=23)
HodgkinLymphoma
(n=23)
Histology, n
Follicular: 11DLBCL: 10PMBL: 2 Other: 8
CTCL/MF:13PTCL: 5Other: 5
NS HL: 22MC HL: 1
Age, median (range)63
(32–81)65
(23–74)61
(29–81)35
(20–54)
Prior auto transplant, n (%)Prior brentuximab vedotin, n (%)
15 (56)0 (0)
4 (14)3 (10)
2 (9)6 (26)
18 (78)18 (78)
Prior therapies, median (range) 4 (1–12) 3 (1–16) 4 (1–9) 5 (2–15)

0
5
10
15
20
25
30
35
Nu
mb
er
of
Pa
tie
nts
Grade 1Grade 2Grade 3Grade 4Grade 5
Drug-Related AEs
General Blood Skin GI Pulmonary Lab Infections Eye

Tumor Type # pts ORR CR PR SD
Multiple Myeloma 27 1 (4) 1 (4) 0 17 (63)
B-Cell Non-Hodgkin Lymphoma 31 8 (26) 3 (10) 5 (16) 16 (52)
Diffuse Large B-Cell 11 4 (36) 2 (18) 2 (18) 3 (27)
Follicular NHL 10 4 (40) 1 (10) 3 (30) 6 (60)
Mantle Cell Lymphoma 4 0 0 0 3 (75)
Primary Mediastinal B-Cell 2 0 0 0 2 (100)
Other B-NHL 4 0 0 0 2 (50)
T-Cell Non-Hodgkin Lymphoma 23 4 (17) 0 4 (17) 10 (43)
CTCL/MF 13 2 (15) 0 2 (15) 9 (69)
Peripheral T-Cell 5 2 (40) 0 2 (40) 0
Other T-NHL 5 0 0 0 1 (20)
Hodgkin Lymphoma 23 20 (87) 6 (26) 14 (61) 3 (13)
Best Response

Tumor type n ORR Median
Follow-upin weeks
Median Response Durationin weeks
OngoingResponses
Multiple Myeloma 27 1 (4%) 46 12+ 1 (100%)
DLBCL 11 4 (36%) 23 22 (6 , 77+) 1 (25%)
Follicular NHL 10 4 (40%) 91 NR (27+ , 82+) 3 (75%)
CTCL/MF 13 2 (15%) 43 NR (24+ , 50+) 2 (100%)
PTCL 5 2 (40%) 31 NR (11 , 79+) 1 (50%)
Hodgkin Lymphoma 23 20 (87%) 86 NR (2 , 91+) 10 (50%)
Durability of Response
74 weeks median follow-up

DLBCL and Follicular NHL
First response X First occurrence of new lesion
8 16 24 32 40 48 56 64 72 80 88 96
-100
-50
0
50
100200
400
600
X
X
X
X
X
Pe
rce
nt
Ch
an
ge
Fro
m B
ase
lin
e
Time Since First Dose, Weeks0
X
Pe
rce
nt
Ch
an
ge
Fro
m B
ase
lin
e
8 16 24 32 40 48 56 64 72 80 88 96
-100
-50
0
50
100200
400
600
Time Since First Dose, Weeks
0
DLBCL Follicular NHL

Hodgkin Lymphoma Durability of Response

Outline of discussion
• First line treatment in young MCL
• Relapsed MCL
• Rituximab subcute in DLCL
• Relapsed Hodgkin’s lymphoma: standard
agents
• Relapsed Hodgkin’s lymphoma: treatment wih
T-cell check point blockade
• Relapsed DLBCL: inhibitor nuclear export

Presented at the 20th Congress of the European Hematology Association, Vienna, Austria 201539
Patients with Heavily Pretreated Diffuse Large B-Cell Lymphoma (DLBCL) Who Respond
to Oral Selinexor Therapy Show Prolonged Survival: Updated Phase I Results
J. Kuruvilla1, M. Mau-Sorensen2, R. Stone3, N. Wagner-Johnston4, R. Garzon5, L. Savoie6, I. Flinn7, R. Baz8, M. Wang9, P. Martin10, N. Gabrial11, P. Brown2, A. Goy13, T. Rashal12, R. Carlson12, Y. Landesman12, JR. Saint-Martin12, T. Marshal12, M. Savona15, S. Norori14, S. Shacham12, Michael Kauffman12 and M. Guttierez13
(1) Princess Margaret Cancer Center, Toronto, Canada; (2) Dept. of Oncology, Rigshospitalet, Copenhagen, Denmark; (3) Dana-Farber Cancer Institute, Boston, MA, USA; (4) Washington University St. Louis, MO, USA; (5) The Ohio State University, OH, USA; (6) University of Calgary Calgary, Canada; (7) Sarah Cannon Research Institute, Tennessee Oncology, Nashville, TN, USA; (8) H. Lee Moffitt Cancer Center & Research Institute Inc., Tampa, FL, USA; (9) MD Anderson Cancer Center, Houston, TX USA; (10) Weil Cornell Medical College, New York, NY, USA; (11) GabrailCancer Center, Canton, OH; (12) Karyopharm Therapeutics Inc, Newton, MA, USA; (13) Hackensack University Medical Center, Hackensack, NJ, USA; (14) Ozmosis Research Inc, Toronto, ON, Canada; (15) Vanderbilt University School of Medicine, Nashville, TN, USA

Presented at the 20th Congress of the European Hematology Association, Vienna, Austria 2015 40
• The nuclear export protein Exportin 1 (XPO1) is overexpressed in all types of malignant lymphoma, including DLBCL
• Selinexor is a Selective Inhibitor of Nuclear Export (SINE) compound that inhibits XPO1 to force nuclear retention of tumor suppressors and other proteins integral to tumorigenesis
• Selinexor interferes with proteins known to play critical roles in DLBCL
– Reduces Myc, Bcl2 and Bcl6 protein through forced nuclear retention of eIF4E
• Overexpression and translocations of Myc, Bcl2 and Bcl6 lead to more aggressive DLBCL
– Blocks NF- B activation through nuclear retention of IkB
• NF- B activation is important for DLBCL ABC subtype survival
Selinexor – Mechanism of Action

Presented at the 20th Congress of the European Hematology Association, Vienna, Austria 2015 41
Exportin 1 (XPO1) Expression in DLBCL
XPO1 Expression in DLBCL Tissues (by IHC)
XPO1 Expression in Chemo-sensitive and Chemo-refractory DLBCL Patient Cells
• XPO1 is highly expressed in DLBCL, specially in chemo relapsed/refractory cases with 60% of patients having >70% XPO1 positive cells
Marullo et al AACR 2015
!!
Background
Materials and Methods
Results
Conclusions
XPO1 is highly expressed in DLBCL preferentially
in chemorefractory cases
Inhibition of XPO1 by KPT-330 impairs proliferation and survival in double/triple
hit DLBCLs
Inhibition of XPO1 by KPT-330 reduces the expression of multiple oncogenic
proteins by affecting the nuclear export of their mRNA
XPO1 inhibition impairs DNA damage response and repair in DLBCL
KPT-330 is active as single agent and improves the response to CHOP in a
patient-derived xenograft model of triple-hit DLBCL
46.5%
41.3%
12.3%
>5% <30% >5% <30%
XPO1 expression in DLBCL tissues by IHC
% of XPO1-positive cells
XPO1 expression in chemosensitive and chemorefractory DLBCL patients
60%
40%
18.1%
45.4%
36.3
>5% <30%
>30% <70%
>70%
Sustained Response Relapsed/refractory
n=23 n=20 n=58
Double/triple hit cell lines in our study
KPT-330 induces cell cycle arrest in Toledo cells
Ly1
KPT-330 IC50
- + - + - + - + DoHH2 K422 Toledo
p53
β-actin
KPT-330-induced cell cycle arrest is independent of p53
Cell$line Myc$ BCL2$ BCL6$
Toledo Dup/t3,8 Rea Del/t3,8
DoHH2 Rea Amp Amp
LY1 Amp/Del t14,8 3q27
SUDHL6 Amp T14,18 WT
XPO1
MYC
BCL2
BCL6
RAD51
CHEK1
KPT330
(0.5 µM)
KPT V
eh KPT
CHOP
KPT+
CHOP
0
10000
20000
30000
p<0.0001
p<0.0001
p=0.0355
p=0.0015
p<0.0001
Treatment
AU
C
CTRL KPT330 CHOP CHOP + KPT330
p=0.0355
p<0.0001
p=0.0015
Cells were exposed to a dose range of KPT330 for 48h
and viability measured by Cell Titer Blue
Double-Triple hit cells were identified by performing
FISH analysis for MYC, BCL6 and BCL2 genes
Cells were exposed to KPT330 at IC50 dose (0.2 µM) and cell
cycle profile was determined at 24h and 48h by Propidium Iodide
staining and subsequent flow cytometry analysis
KPT-330 is active at nanomolar dose in
DLBCL cell lines
48h 24h
Cells were exposed to KPT330 at IC50 dose
and p53 accumulation was evaluated at 24h
by Western Blot
Exposure to KPT-330 for 24h reduces the expression of multiple proteins in DLBCL cell lines
Exposure to KPT330 results in nuclear entrapment of mRNA encoding key oncogenic proteins in DLBCLs
Cells were exposed to KPT330 (0.5 µM) for 24 h and subsequent cellular fractionation was performed by differential
centrifugation. mRNA transcript for each gene were determined by RT-qPCR. Nuclear/Cytoplasm mRNA ratio in treated
vs. untreated cells was computed by using total cellular RNA for each condition as calibrator
LY1
- + - + - +
Toledo DoHH2
Experiment plan:
- 5 NSG mice engrafted in both flanks per group
- Treatment started at tumor size of 50-70 mm3
- Mice received 5 somministrations of KPT330 and one
somministration of CHOP
- Tumor volume and weight were evaluated every two
days
XPO1 inhibition by KPT330 impairs the repair of doxorubicin-induced DNA damage in Toledo cells
Doxorubicin 4 hours Doxorubicin 4 followed by 4h recovery
XPO1 inhibition by KPT-330 impairs doxorubicin-induced cell cycle arrest in Toledo cells
Cells were pretreated with KPT330 (IC50, 0.2 uM) for 24h and then exposed to Doxorubicin (IC50, 1.2 uM) for 4h.
DNA damage was assessed by alkaline comet assay at the end of the 4h Doxorubicin treatment or after allowing cells
to recover for additional 4 hours.
Ctrl KPT330 Doxorubicin Doxorubicin + KPT330
Cells were treated with KPT330 (IC50, 0.2 µM) and Doxorubicin (IC50, 1.2 µM) alone or in combination for 24h. After treatment
cell cycle profile was determined by Propidium Iodide staining and subsequent flow cytometry analysis
p<0.0001
30000
20000
10000
0
Mon$ Wed$ Fri$
Group A vehicle vehicle vehicle
Group B KPT330 7.5 mg/Kg KPT330 7.5 mg/Kg vehicle
Group C vehicle vehicle CHOP
Group D KPT330 7.5 mg/Kg KPT330 7.5 mg/Kg CHOP
AU
C
β-ACTIN
β-ACTIN
β-ACTIN
KPT330
(0.5 µM)
LY1
- + - + - +
Toledo DoHH2 • XPO1 is required for proliferation and survival of double/triple hit lymphomas
• XPO1 regulates the nuclear export of transcripts encoding key lymphomagenesis drivers, such as
MYC and BCL6; thus, exposure to KPT330 results in nuclear entrapment of MYC and BCL6
transcripts and subsequent reduction in protein expression
• XPO1 regulates the nuclear export of transcripts encoding members of DNA damage response
and repair pathways, such as CHEK1 and RAD51; thus, exposure to KPT330 results in nuclear
entrapment of CHEK1 and RAD51 transcripts and subsequent reduction in protein expression
• KPT-330 pretreatment increases the effectiveness of first line chemotherapy (CHOP) in vivo in a
triple-hit patient-derived xenograft model
Mutation and constitutive expression of MYC, BCL2 and/or BCL6 (double and triple-hit
lymphomas) defines a subsets of diffuse large B-cell lymphoma (DLBCL) patients with particularly
poor outcome due to chemo-refractory disease, a prognosis that cannot be overcome with
intense chemotherapy.
Exportin 1 (XPO1/CRM1) is a well characterized mammalian export protein that facilitates the
transport of large macromolecules including RNAs and proteins across the nuclear membrane to
the cytoplasm.
XPO1 binds to a diverse array of protein cargos through their canonical leucine-rich nuclear export
signals (NES) domain. XPO1 exports many tumor-suppressor proteins and thus acts as a proto-
oncogene by removing oncosuppressor protein from the nucleus, where they are active, to the
cytoplasm.
XPO1 overexpression is common in solid tumors and hematologic malignancies and
correlates with poor prognosis and resistance to therapy.
Hypothesis
DLBCL cell lines
Toledo
DoHH2
SUDHL-4
OCI-Ly1
OCI-Ly10
SUDHL-6
HBL-1
SC-1
K422
In vitro: In vivo:
Patient-Derived
Xenograft
Double hit DLBCL
XPO1 amplification
Stage IVb
IPI:4
Chemo-refractory
(relapse within 3
months)
In vitro experiments:
Viability: fluorescent assay based on the reduction of
resazurin into resorufin (Cell Titer Blue)
Cell Cycle Profile: Propidium Iodide Staining and
subsequent Flow Cytometry analysis
Protein expression: SDS-PAGE and Western Blot Analysis
mRNA expression in nuclear vs. cytoplasm: cellular
fractionation by differential centrifugation followed by RNA
isolation and RT-qPCR
DNA damage repair kinetic: Alkaline Comet Assay
XPO1 inhibitor: KPT-330 (a.k.a. Selinexor, Karyopharm) –
Selective Inhibitor or Nuclear Export (SINE)
Since double-triple hit lymphomas are characterized by the concomitant deregulation of multiple
oncogenic pathways, we hypothesize that XPO1 may be an effective target for these tumors as
it simultaneously impacts multiple oncogenic mechanisms
We also hypothesize that inhibition of XPO1 by the selective small molecule KPT-330 may also
revert the chemo-refractory status of aggressive lymphomas.
Sustained Response (CR 2 years) Relapsed/Refractory

Presented at the 20th Congress of the European Hematology Association, Vienna, Austria 2015 42
• 31% ORR and 51% DCR for all evaluable DLBCL patients
• 43% ORR and 71% DCR for evaluable DLBCL patients on study ≥ 1 month
• ORR and DCR are equivalent across DLBCL origin or subtype
• Duration of response was >9 months
• Responses were also observed in “double-hit” DLBCL
Best Responses in DLBCL patients
CategoryTotal
EvaluableORR CR PR SD PD DCR
All Patients 39* 31% 4 (10%) 8 (21%) 8 (21%) 19 (49%) 51%
Patients on study ≥ 1 Month 28 43% 4 (14%) 8 (29%) 8 (29%) 8 (29%) 71%
OriginDe novo 28 25% 3 (11%) 4 (14%) 6 (21%) 15 (54%) 46%
Transformed 11 45% 1 (9%) 4 (36%) 2 (18%) 4 (36%) 64%
SubtypeGCB 14 43% 3 (21%) 3 (21%) 5 (36%) 3 (21%) 79%
non-GCB 4 25% 1 (25%) -- 3 (75%) -- 100%
*Three patients were non-evaluable for response due to consent withdrawal with lack of disease assessment prior to one cycle on study.
Responses (as of 1-June-2015) were adjudicated according to the International Working Group Response Criteria for Non-Hodgkin’s
Lymphoma (NHL) 2007 based on interim unaudited data. ORR=Objective Response Rate (CR+PR), CR=Complete Response, PR=Partial
Response, SD=Stable Disease, PD=Progressive Disease, DCR=Disease Control Rate (CR+PR+SD) GCB=Germinal Center B Cell.
GCB/non-GCB subtypes were not defined for all patients.
Allpatients

Presented at the 20th Congress of the European Hematology Association, Vienna, Austria 2015 43
• OS and PFS for all DLBCL pts was 4.6 and 1.7 months, respectively
• Patients with objective responses had greatly increased OS and PFS
Overall and Progression Free Survival in DLBCL
0 3 6 9 12 15 18 21 24 27 30 330
20
40
60
80
100
Time (months)
Ov
era
ll o
r P
rog
res
sio
n F
ree
Su
rviv
al (%
)
All DLBCL patients
OS (4.6 mo)
OS 42
PFS 42
25
12
13
8
10
6
7
5
1
1
6
5
3
2
2
1
PFS (1.7 mo)
0 3 6 9 12 15 18 21 24 27 30 330
20
40
60
80
100
Time (months)
Ov
era
ll S
urv
iva
l (%
)
OS (CR/PR vs SD/PD)
SD/PD (3.5 mo)
CR/PR (>10 mo)
p < 0.0001HR=0.12
CR/PR 12
SD/PD 27
12
13
10
4
8
3
6
2
5
1
3
1
1
1
6
1
2
1
0 3 6 9 12 15 18 21 24 270
20
40
60
80
100
Time (months)
Pro
gre
ss
ion
Fre
e S
urv
iva
l (%
)
CR/PR vs SD/PD
SD/PD (1.2 mo)
CR/PR (24 mo)
p < 0.0001HR=0.06
CR/PR 12
SD/PD 27
10
3
8
1
5
1
4
1
3
1
1
1
2
1
Patientsat risk

Presented at the 20th Congress of the European Hematology Association, Vienna, Austria 2015
Domande al gruppo di lavoro
• Terapia di mantenimento nel Linfoma Mantellare
del giovane post ASCT?
• Terapia di salvataggio nel Linfoma di Hodgkin:
ruolo dei farmaci non chemioterapici e ruolo
Bendamustina?
• Come migliorare il salvataggio dei DLBCL?

Acknowledgments
G. Benevolo
C. Boccomini
B. Botto
A. Castellino
C. Ciochetto
A. Chiappella
M. Nicolosi
L. Orsucci
P. Pregno
P. Riccomagno
Lymphoma Team
Hematology Torino
FIL Secretary Alessandria
All FIL Centers
Biostatistics Torino
Trial Office Modena