leading the best care...always! campaign dena van den bergh, michele youngleson, gary kantor,...
TRANSCRIPT

Leading the Best Care...Always!
Campaign
Dena van den Bergh, Michele Youngleson, Gary Kantor, Yolanda Walsh
May 10th 2011
Cape Town

Agenda
• Welcome• Introductions• Best Care…... Always! (BCA)• A framework for leading BCA• Fundamentals of the QI approach• Measuring for BCA• LUNCH• QI in action• Next steps

Introducing Best Care.. Always!
Dena van den Bergh

The BCA Quality Improvement approach
• Not just protocol• Focus on the implementation gap• All learn all teach• Learning by doing

Accelerating change and improvement through networking and collaboration.
Expert Meeting and
Planning Group formed
Learning session
1
Learning session
2
Repeated improvement
cycles:
Repeated improvement
cycles:
Learning session
3
18 -24 months
Mentoring and support

Framework for Leading Improvement

3,4,5: Will, Ideas and Execution
Nolan TW. Execution of Strategic Improvement Initiatives to Produce System-Level Results. IHI Innovation Series white paper. Cambridge, MA: Institute for Healthcare
Improvement; 2007. (Available on www.IHI.org)
Will
Ideas Execution

Next Steps
• Hospital visits (data)• Learning sessions
─LS#1 May 25• Monthly mentoring meetings with quality
champions• More hospital visits

Learning Session #2
Carol R. Haraden, PhD • Vice President, Institute for Healthcare Improvement (IHI) • Lead: Safer Patients Initiative (UK)• Lead: Scottish Patient Safety Alliance • Executive lead: IHI Patient Safety Officer Executive Development Program • Institute of Medicine Committee on Engineering Approaches to Improve
Health Care• Associate editor for the journal Quality and Safety in Health Care.
October/November 2011+ Breakout session for CEOs

The Burden of Healthcare-Associated Infection
Prof Shaheen Mehtar
UIPC, TBH & SUN
Cape Town

Situation Analysis of LMI countries
• Rates of HAI are higher in LMI countries• IPC programmes are poorly supported• Little accountability by Health Care Workers• Clinical commitment essential - Duty of Care

Comparative data- HIC and LMIC Burden of endemic health care associated infection in developing countries: systematic review and
meta analysis- B Allegranzi et al, Lancet, 2011, 377: 228-41
HAIs are at least 3 x more common in LMI countries

Crude HAI Infection Rate: TBH. Impact of an established IPC programme
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q42006 2007 2008 2009 2010
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
5.0
4.3
3.9 4.0
3.6
4.4
3.7
3.1
3.6
4.4
3.3
1.5
2.4
3.63.5
3.13.3
2.8 2.7
2.4
2.8
Crude Infection Rates
Infection Rates

Comparing TBH to meta-analysis
Site Meta analysisMedian/1000 device days
TBH / 1000 patient days
VAP 28 ETA 1- 3
CR BSI 18 CVP & B/C 0.5-1.3
SSI 1.2-23.6/1000 surg op
NO DATA

The impact of Healthcare Associated Infections on the
hospitals

The impact of HAIs on the hospitals
• Mortality and morbidity• Lab and pharmacy costs• Antibiotic use• Bed occupancy• Work load

The impact of HAIs on your hospital
• Fill in the column graphs (per hospital)- peripheral vascular catheter-associated infection
(PVCAI)- central line-associated bloodstream infection
(CLABSI)- ventilator-associated pneumonia (VAP)- catheter-associated urinary tract infection (CAUTI)- surgical site infection (SSI)
• Fill in the scale – hand hygiene (each individual

The fundamentals of the Quality Improvement
approach used in BCA

Changing View of Quality
We are perfect!
NO ACTION
Get rid of the bad apples
M&M
Quality Assurance
REACTION
Incident reporting
“Standards”

Patients get “recommended care” ~ 50% of the time.
Adverse events occur in 10% of hospital patients.─ 50% are preventable.─ 7.5% of these patients die.
...the gap between evidence and practice
20
NEJM 2003; 348:2635-2645
Qual Safety in Health Care 2008;17:216-223

Changing View of Quality
We are perfect!
NO ACTION
Get rid of the bad apples
System thinking
M&M
Quality Improvement
Quality Assurance
REACTION PROACTIVE
“Quality”Safe
EffectiveTimely
EquitablePatient-centred
Efficient
Improvement Science
Incident reporting
“Standards” Process Improvement

Quality Improvement requires two Types of Knowledge
Subject Matter Knowledge
Subject Matter Knowledge: Professional, content, evidence based knowledge.
Improvement Knowledge (Deming): The interaction of the theories of systems, our ‘theory of knowledge’, variation in measurement, and psychology.
Improvement Knowledge
‘What’
‘How’

Improvement
Improvement Knowledge
Subject Matter Knowledge
Improvement: develop effective changes that lead to an improvement.
Langley: Improvement Guide p76
‘Where’
‘How’
‘What’

Improvement Knowledge
Subject Matter Knowledge
Improvement Knowledge
W.E. Deming (1900-1993)
System of Profound Knowledge

Improvement Knowledge
Subject Matter Knowledge
4 fields of interaction - theories of systems - our ‘theory of knowledge’ - psychology of change- variation in measurement
Improvement Knowledge

Complex Dynamic Systems
• Step 1 – Everyone stand up• Step 2 – Without speaking; pick two
people but don’t say who they are or point at them (Keep it a secret)
• Step 3 - Move to be equidistant from both of the people
• Step 4 – Move one person and repeat

The power of the system
Step 1: Pick a number
from 3 to 9
Step 2: Multiply your number by 9
Step 3:Add 12 to the
number from step 2
Step 7: Write down thename of a city
that begins with your letter
Step 4: Add your 2
digits together
Step 5:Divide # from step 4
by 3 to get a 1 digit number
Step 6:Convert your
Number to a letter:1=A 2=B 3=C 4=D 5=E 6=F 7=G 8=H 9 = I
Step 8: Go to the next Letter: A to B, B to C, C to D,
etc.
Step 9: Write down the nameof an animal (not bird,
fish, or insect) that begins with your letter
from Step 8
Step 10:Write down the color of
your animal
Do you have a 2-digit Number?
NO
YES
Output:
Color____________
Animal___________
City__________

Understanding Systems
“Every system is perfectly designed to achieve the results it gets” Paul Batalden
Paul B. Batalden, MD, Professor of Pediatrics, of Community and Family MedicineThe Dartmouth Institute for Health Policy and Clinical Practice at The Dartmouth Medical School.

Hand washing practice in the PICU
from a Report of a participative observational study done during
January and March 2006Candice Bonaconsa and Minette Coetzee
Child Nurse Practice Development Initiative
Prof Andrew Argent, Red Cross Hospital

Actual x 100 = %
Opportunity
How we did this:
Calculating the % of hand washing

Comparitive Table of Hand Washing - Bed Space
24%
38%
7%
75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Docters Nurses Other Visitors
Goal 90%

Time Opportunities Used Opportunities %10:00-11:00 12 2 16.711:15-12:15 11 2 18.221:30-22:30 14 3 21.422:30-23:30 7 1 14.314:15-15:15 11 1 9.115:20-16:20 7 3 42.910:45-11:45 28 5 17.911:45-12:45 10 2 20.010:30-11:30 15 3 20.011:30-12:30 8 3 37.511:30-12:30 15 1 6.712:30-13:30 10 1 10.013:30-14:30 5 2 40.014:30-15:30 8 1 12.515:30-16:30 4 0 0.014:00-15:00 19 1 5.315:00-16:00 9 0 0.012:00-13:00 16 1 6.313:00-14:00 10 0 0.0
elsewhere in the hospital …

Forces in the system keeping hand washing rates where they are
Time
A B
Lewin K (1951)Field Theory in Social ScienceNew York: Harper

Understanding Systems
“Every system is perfectly designed to achieve the results it gets” Paul Batalden
“All improvement needs a change
Not all change is an improvement”
Paul B. Batalden, MD, Professor of Pediatrics, of Community and Family MedicineThe Dartmouth Institute for Health Policy and Clinical Practice at The Dartmouth Medical School.

Improvement Knowledge
Subject Matter Knowledge
4 fields of interaction - theories of systems - our theory of ‘knowledge’- psychology of change- variation in measurement
Improvement Knowledge

Theory of knowledge
Our understanding of why things are the way they are.
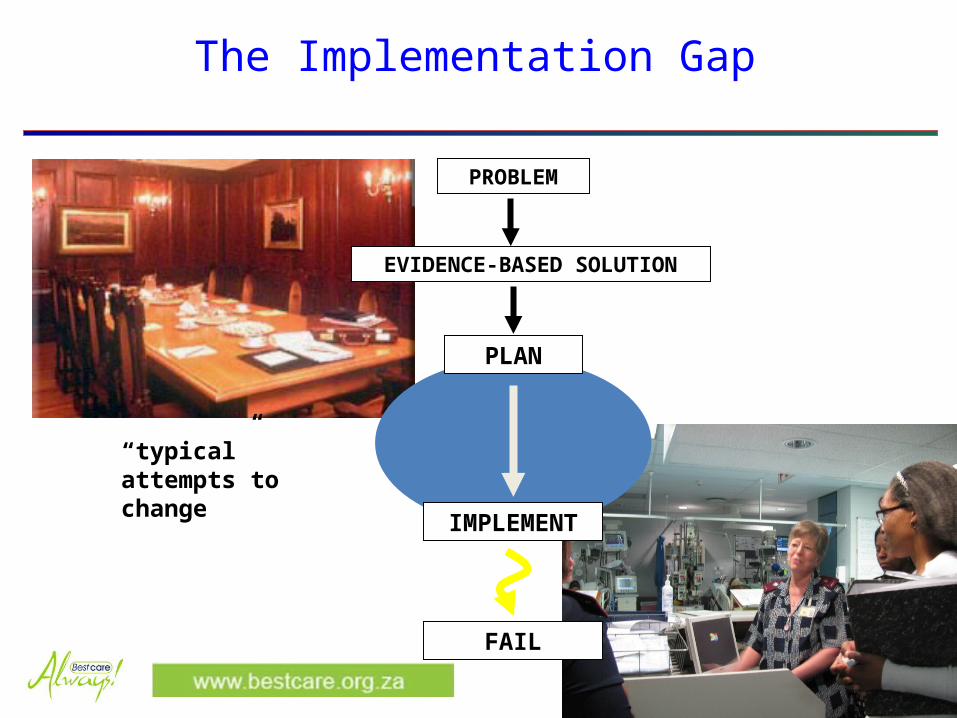
The Implementation Gap
PLAN
IMPLEMENT
FAIL
PROBLEM
EVIDENCE-BASED SOLUTION
“typical” attempts to change
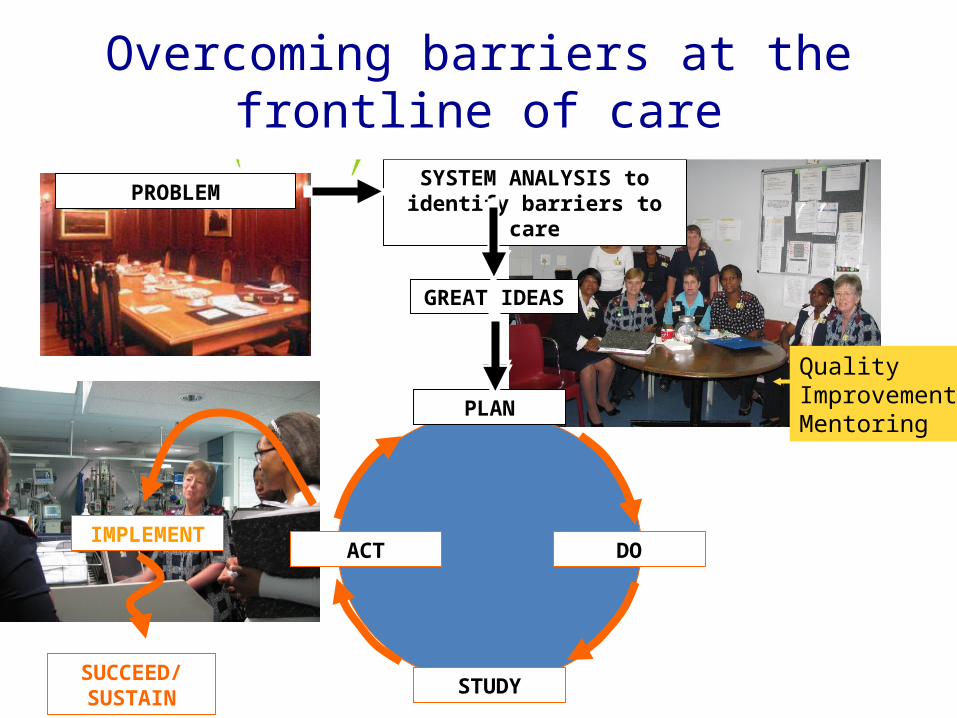
GREAT IDEAS
SYSTEM ANALYSIS to identify barriers to care
DO
STUDY
ACTIMPLEMENT
SUCCEED/ SUSTAIN
PROBLEM
PLAN
Overcoming barriers at the frontline of care
QualityImprovementMentoring

Model for Improvement
What can we change that will result in an improvement?
PLAN
DO
STUDY
ACT
How will we know that a change is an improvement?
What are we trying to accomplish?
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT

Improving many parts of the system at once
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
Bundle 1 Bundle 2Unit 1 Unit 2
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT
PLAN
DO
STUDY
ACT

Improvement Knowledge
Subject Matter Knowledge
4 fields of interaction- theories of systems - our theory of ‘knowledge’- psychology of change- variation in measurement
Improvement Knowledge

Psychology of Change
Population
Innovators
Source: E. Rogers. Diffusion of Innovation
Early Adopters
Early Majority Late Majority
Traditionalists

Improvement Knowledge
Subject Matter Knowledge
4 fields of interaction - theories of systems - our theory of ‘knowledge’- psychology of change- variation in measurement
Improvement Knowledge

Understanding Variation
• Walter Shewhart’s (1891-1967) – understanding variation through Statistical Process Control (SPC)

Flip a coin
1 2 3 4 5 6 7 8 9 10 11 12 13 14 150
2
4
6
8
10
12
# heads up in 10 flips of a coin
Consecutive turns
# h
ead
s u
p

July Aug Sep Oct
5/7 13/8 7/9 5/10
5/7 9/9 8/10
6/7 12/9 15/10
11/7 15/9 19/10
25/7 20/10
27/7 21/10
25/10
ICU: Date of VAP infections 2010

MeasurementCommon mistakes• Using bar graphs rather than run charts• Not enough data points (12 at least to
understand normal variation)• Not making allowances for normal
variation when interpreting data• Not measuring trends over a long enough
period - cut off at year end or financial year end

Reacting to Variation

Measuring forBest Care….Always!

Measurement
• Builds will• Assesses impact• Drives improvement• Keeps the project alive• Sustains the gains

Measurement
• Data must be visually appealing and accessible─Owned and used at the frontline of care─Routinely reviewed at monthly management
meetings • An active, encouraging feedback loop from
management to frontline staff

Measurement
Leaders need to know
i) what measures are being used for ─ incidence of HAIs─ bundle compliance (implementation of
bundles)
ii) how data is being presented
iii) how to─ interpret the data─ respond to the data

Measurement for BCA
• Outcome measures (HAIs)• Process measures (bundle compliance)• Balancing measures• Morbidity and mortality reviews

Outcome measures
• the incidence of HAIs• impact of changes made

Infection Rates
• Total number of infective cases per 1,000 device days:
Total No. of VAP cases
Ventilator daysX 1,000
Numerator
Denominator
Good for aggregate data but high variation for units when events are rare (<10%)

Oct-08
Nov-08
Dec-08
Jan-09
Feb-09
Mar-09
Apr-09
May-09
Jun-09Jul-0
9
Aug-09
Sep-09
Oct-09
Nov-09
Dec-09
Jan-10
Feb-10
Mar-10
Apr-10
May-10
Jun-10Jul-1
0
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
0.00
1.00
2.00
3.00
4.00
5.00
6.00
7.00
8.00
5.57
3.85
5.66
4.21
7.17
4.955.22
2.01 2.10 2.01
3.222.93
3.36
2.58
3.12
2.46
3.48
2.90 2.98
2.082.33
2.17
1.57
2.05
1.67
0.570.85
CLABSI - Infection Rates Per 1000 Central Line DaysLife Healthcare Group - Oct 2008 to Sept 2010
CLABSI-Rate Mean
Upper control limit Lower control limit
Step change after implementation of reporting system and training on BCA in all acute hospitals
Step change after cross functional workshops in ICU's to implement bundle compliance improvement ac-tions and to increase the involvement of Unit Managers in the process
57

Welsh Safety Calendar
IDeveloped by Annette Bartley, Welsh 1000 Lives Campaign


Measuring rare events
Events that occur < 10% of the time

Measuring rare events –days between events
Neonatal deaths – Malare Health Centre, 5’s Alive! Project, Ghana

Date of infection
# Days since last infection
Days Be-tweenInfection
Sequence of Infections

IMeasuring rare events and time-between measures. James Benneyan IHI

Number of infections against annual target
Laurel SimmonsAssoc. Dir. for Quality ImprovementStockport NHS Foundation Trust
Target - 6for the year
(Set for eachHospital forEach HAIby DOH)

Dashboard of measures
Eastern sub-district HIV/AIDS Improvement project reportMarch 2009

Process measures
• Bundle compliance drives the improvement• Target must be set at 95% for each bundle
element and therefore the whole bundle (reliability theory)

Mar
-09
Apr-
09
May
-09
Jun-
09
Jul-0
9
Aug-
09
Sep-
09
Oct
-09
Nov-
09
Dec-
09
Jan-
10
Feb-
10
Mar
-10
Apr-
10
May
-10
Jun-
10
Jul-1
0
Aug-
10
-
2.00
4.00
6.00
8.00
10.00
12.00
14.00
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
11.97 12.00 12.66
12.35 11.83 11.82
8.28
12.96
9.78 9.94
6.70
9.06 8.58
10.01
9.17
7.16
5.63
8.61
69%
82%
77%
71%
86%88%
91% 91% 91%89% 89%
92%88%
93% 93% 92% 93%
80%
Ventilator Associated Pneumonias- Bundle Compliance and Infection Rate
Mar 09 - Aug 10
Infection Rate VAP
67
Bundle compliance

A Framework for Leading Best Care….Always!

Framework for Leading Improvement

Leading BCA
Dr Hannes LootsRegional Clinical ManagerWestern Cape RegionMedi-Clinic Southern Africa
(9 mins)