lambeau antero‐latéral de cuisse · 1 lambeau antero‐latéral de cuisse altf ou de la lente et...
TRANSCRIPT
1
Lambeau Antero‐latéral De CuisseALTF
Ou de la lente et longue évolution des lambeaux cutanés
• Lambeau antero-latéral de cuisse (ALTF) =– première description 1984 (Song)
– Popularisation mondiale 20 ans après
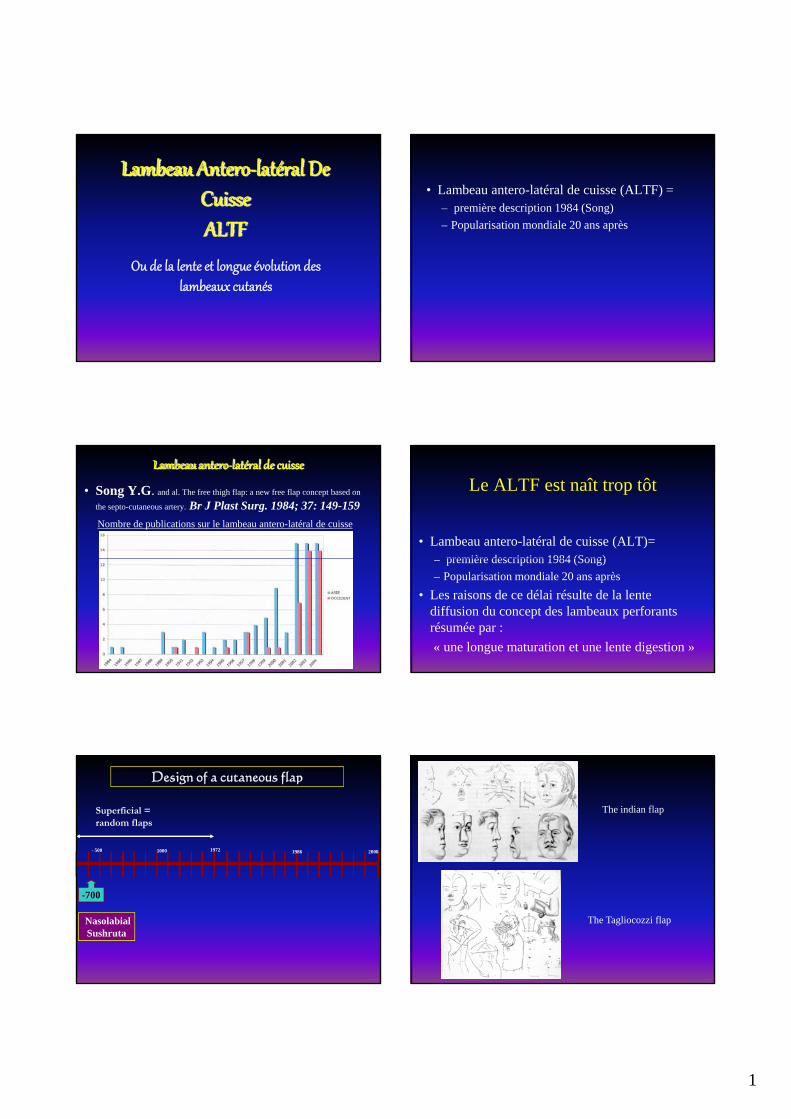
Lambeau antero‐latéral de cuisse
• Song Y.G. and al. The free thigh flap: a new free flap concept based on
the septo-cutaneous artery. Br J Plast Surg. 1984; 37: 149-159
Nombre de publications sur le lambeau antero-latéral de cuisse
Le ALTF est naît trop tôt
• Lambeau antero-latéral de cuisse (ALT)=première description 1984 (Song)– première description 1984 (Song)
– Popularisation mondiale 20 ans après
• Les raisons de ce délai résulte de la lente diffusion du concept des lambeaux perforants résumée par :
« une longue maturation et une lente digestion »
1000 19861972- 500 2008
Design of a cutaneous flap
Superficial = random flaps
-700
Nasolabial Sushruta
The indian flap
The Tagliocozzi flap

2
Design of a cutaneous flap
• For 3000 years = superficialsuperficial– random flap
• 2/1 ratio• Arc of rotation• 4 basic drawings
ADVANCEMENT TRANSLATION
TRANSPOSITION ROTATION
1000 19861972- 500 2008
Planning of cutaneous flap
Superficial = random flaps
Deep = axial flaps
-700
Nasolabial Sushruta
1972
Mc GregorGroin flap
Axial flow flap
Design of a cutaneous flap
• 1972 = deep, following source vessel– Axial flap
• 1972 Mc Gregor = the conceptg p
• The era of musculo-cutaneous flaps
1000 19861972- 500 2008
Planning of a cutaneous flap
Superficial = random flaps
Deep = axial flaps
Superficial = perforator flaps
-700
Nasolabial Sushruta
1972
Mc GregorGroin flap
Axial flow flap
Taylor
1980
NakajimaClassification of vessels
for the skin
1986
Design of a cutaneous flap
• 1990 = superficial – According with the anatomy of vessels for the
skin• The result of fundamental and clinical work on skin
vascularisation
• The era of perforator flaps
– Result during this last century of :• fundamental anatomical work
• Clinical evolution

3
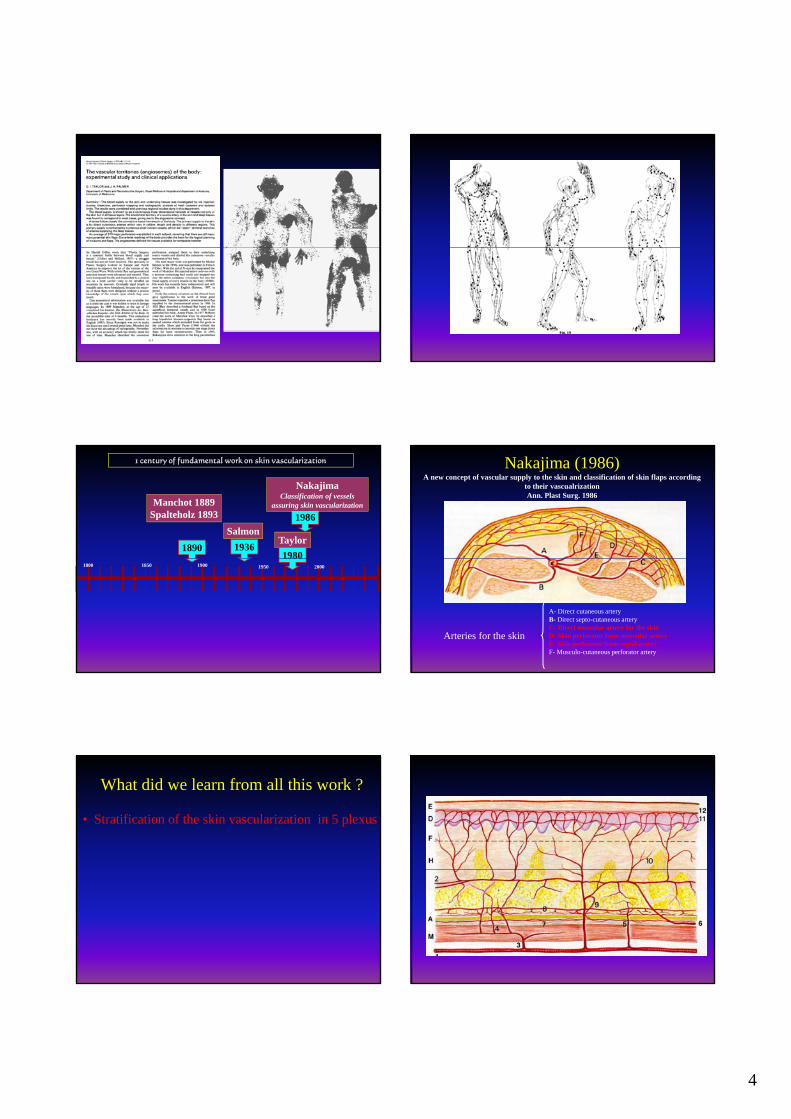
1890
Manchot 1889Spalteholz 1893
1 century of fundamental work on skin vascularization
1800 1900 19501850 2000
1890
Manchot 1889Spalteholz 1893
1936
Salmon
1 century of fundamental work on skin vascularization
1800 1900 19501850 2000
1890
Manchot 1889Spalteholz 1893
1936
Salmon
1980
Taylor
1 century of fundamental work on skin vascularization
1800 1900 19501850 2000
4
1890
Manchot 1889Spalteholz 1893
1936
Salmon
1980
Taylor
1986
NakajimaClassification of vessels
assuring skin vascularization
1 century of fundamental work on skin vascularization
1800 1900 19501850 2000
Nakajima (1986)A new concept of vascular supply to the skin and classification of skin flaps according
to their vascualrizationAnn. Plast Surg. 1986
A- Direct cutaneous arteryB- Direct septo-cutaneous arteryC- Direct muscular artery for the skinD- Skin perforator from muscular arteryE- Skin perforator from septal arteryF- Musculo-cutaneous perforator artery
Arteries for the skin
What did we learn from all this work ?
• Stratification of the skin vascularization in 5 plexus

5
What did we learn from all this work ?
• Stratification of the skin vascularization in plexus
• 3D organization = Angiosome concept– 61 territories = based on 61 main source vessels
– 442 perforators over 0 5 mm442 perforators over 0.5 mm
What did we learn from all this work ?
• Stratification of the skin vascularization in plexus
• 3D organization = Angiosome concept
– 61 territories = based on 61 main source vessels
– 442 perforators over 0.5 mm
• Skin paddle design = survival of the entire flap
What did we learn from all this work ?Survival of the entire skin paddle
The skin territory
The source vessel
The Perforator
What did we learn from all this work ?
• Stratification of the skin vascularization in plexus
• 3D organization = Angiosome concept
– 61 territories = based on 61 main source vessels
– 442 perforators over 0.5 mm
• Skin paddle design = survival of the entire flap– The subcutaneous network
Sub-cutaneous network
• Long running sub-cutaneous vessels (limbs)

6
Sub-cutaneous network• Long running sub-cutaneous vessels (limbs)
• Sensitive nerves accompanied by pedicle = neuro-cutaneous flap
What did we learn from all this work ?
• Stratification of the skin vascularization in plexus
• 3D organization = Angiosome concept
– 61 territories = based on 61 main source vessels
– 442 perforators over 0.5 mm
• Skin paddle design = survival of the entire flap– The subcutaneous network
– The capture rule
The capture rule• Interconnection of all angiosomes by:
– Choke arteries
– Oscillating veins
Choke arteries & oscillating veins
The capture rule• Interconnection of all angiosomes by:
– Choke arteries
– Oscillating veins
• Responsible for the Capture phenomena:p p p– Anatomic Cutaneous Arterial & Venous Territory
– Hemodynamic Cutaneous Arterial & Venous Territory
– Potential Cutaneous Arterial & Venous Territory
Vascular territories

7
Survival of the entire skin paddleThe sub-cutaneous network
IV
Survival of the entire skin paddleThe capture rule
IVIIII II
What did we learn from all this work ?
• Stratification of plexus in the skin
• 3D organization = Angiosome concept
– 61 territories = based on 61 main source vessels
– 442 perforators over 0.5 mm
• Skin paddle design = survival of the entire flap– The subcutaneous network
– The capture rule
– The perforasome concept
Perforasome conceptSaint-Cyr PRS 124 2009
• 1 principle = each perforator is linked with adjacent through direct & indirect communication
Perforasome conceptSaint-Cyr PRS 124 2009
• 1 principle = each perforator is linked with adjacent through direct & indirect communication
• 2 principle = Flap design according with connecting vesselsconnecting vessels– Limbs = longitudinal
– Trunk = perpendicular
Perforasome conceptSaint-Cyr PRS 124 2009
• 1 principle = each perforator is linked with adjacent through direct & indirect communication
• 2 principle = Flap design according with connecting vessels
– Limbs = longitudinal
Trunk = perpendicular– Trunk = perpendicular
• 3 principle = preferential filling within the same angiosome

8
Perforasome conceptSaint-Cyr PRS 124 2009
• 1 principle = each perforator is linked with adjacent through direct & indirect communication
• 2 principle = Flap design according with connecting vessels
– Limbs = longitudinal
– Trunk = perpendicular
• 3 principle = preferential filling within the same angiosome
• 4 principle = – direction of vascularization of a joint perforator
is away from the joint
– Intermediate perforator is multidirectional
What did we learn from all this work ?
• Stratification of plexus in the skin
• 3D organization = Angiosome concept
– 61 territories = based on 61 main source vessels
– 442 perforators over 0.5 mm
Ski ddl d i i l f h i fl• Skin paddle design = survival of the entire flap
– The subcutaneous network
– The capture rule
– The perforasome concept
• Classification of vessels for the skin
Vessels for the skin
• 3 types of vessels vascularising the skin:1. Direct path to the skin
2. Perforating vessels but dissectable
3. Perforating vessels but undissectable A- Direct cutaneous arteryB- Direct septo-cutaneous arteryC- Direct muscular artery for the skin
Direct
A- Direct cutaneous artery
Ex: groin flap vascularized by superficial circonflexe iliac pedicle
B- Direct septo-cutaneous
Forearm flap vascularized by radial pedicle

9
A- Direct cutaneous arteryB- Direct septo-cutaneous arteryC- Direct muscular artery for the skin
F- Musculo-cutaneous perforator artery
Direct
Undirectundissectable
F- Musculo-cutaneous perforator artery
Pectoralis major flap vascularized by acromio-thoracic pedicle
A- Direct cutaneous arteryB- Direct septo-cutaneous arteryC- Direct muscular artery for the skin
D- Skin perforator from muscular arteryE- Skin perforator from septal artery
F- Musculo-cutaneous perforator artery
Direct
Undirectundissectable
Undirectdissectable
D- Skin perforator from muscular artery
DIEP flap vascularized by the deep inferior epigastric pedicle
D & E- Skin perforator from muscular & septal artery
Antero-lateral thigh flap vascularized by the anterior lateral circonflexe
femoral artery
To concludeThe history of skin flaps can be
summarized by A l t ti d d t i th• A longue maturation needed to acquire the fundamental bases of blood circulation and skin vascular anatomy and an long digestion by the practitioner for their application in the medical practice of flap surgery

10
Manchot, 1889 Salmon, 1936 Morris & Taylor, 2006
Manchot, 1889Whetzel, Plast. Reconstr. Surg., 1992
Morris,Perforator flaps, 2006
1984 1986 1989-1994 1993-1998
Pourquoi le lambeau antero‐latéral de cuisse est‐il né trop tôt ?
Articlede Song
Classificationde Nakajima
1989 - Concept de lambeau perforant DIEP flap (Koshima)
1994 – DIEP flap et reconstruction mammaire (Allen)
Travaux de Kimata et Koshima
Lambeau antero‐latéral de cuisse:Travaux fondamentaux sur son anatomie vasculaire
• Les articles à retenir:– Xu. Applied anatomy of the antero-lateral femoral flap. 1988– Koshima. The anterolateral thigh flap: variations in its vascular pedicle. 1989– Zhou. Clinical experience and surgical anatomy of 32 free anterolateral thigh flap
transplantation. 1991– Koshima. Free combined composite flaps using the lateral circonflex femoral system for
repair of massive defects of the head and neck regions: an introduction to chimeric flap
principle. 1993– Kimata. Versatility of the free anterolateral thigh flap for reconstruction of head and neck defects.
1997– Kimata. Anatomic variations and technical problems of the anterolateral thigh flap: A report of 74
cases. 1998
Lambeau antero‐latéral de cuisse:Travaux fondamentaux sur son anatomie vasculaire
• Les articles à retenir:– Xu,1988; Koshima,1989; Zhou, 1991, Koshima,1993; Kimata, 1997;
Kimata, 1998
• Les rectifications principales des approximations de Song:– Variations de l’origine de la perforante septo-cutanée directe (type B):
• Naît de la branche descendante de la LCFA 25 %
• Naît directement de la fémorale profonde 30 %
• N’existe pas 45 %
– Variations du type de perforantes cutanées:• Septo-cutanée directe (type B) 18 %
• Musculaire (type C & D) et septo-cutanée indirecte (type E) 82 %

11
Lambeau antero‐latéral de cuisseNotions anatomiques fondamentales
Intermuscular septum LCFA
Branchedescendante
Rectus femoris
Vastus lateralis
Lambeau antero‐latéral de cuisseNotions anatomiques fondamentales
Origine de la perforante cutanée
84.5 % 14 % 1.5 %
98.5 %
Naissance des perforantes cutanées: principalement à la moitié de la cuisse
Lambeau antero‐latéral de cuisseNotions anatomiques fondamentales
Lambeau antero‐lateral de cuisseTechnique chirurgicale
Variation dans la technique de fermeture cutanée
Lambeau antero‐latéral de cuisseTechnique chirurgicale

12
Lambeau antéro‐latéral de cuisseClassification
1- Zone donneuse: peau de la région antero-latérale de la cuisse2- Composition du lambeau: Fascio-cutané
– Fascio-cutané : fin et plastique +/- dépend du patient et du sexe. Utilisé comme un lambeau ultra-fin
• Taille de la palette cutanée: 20 x 12 pour une fermeture directe– Musculo-cutané avec le muscle vaste externe– Composite ou chimérique avec tissus du voisinage (rectus antérieur, TFL,
crête iliaque)
Lambeau antéro‐latéral de cuisseClassification
Lambeau antero-latéral composite
Lambeau antéro‐latéral de cuisseClassification
1- Zone donneuse: peau de la région antero-latérale de la cuisse2- Composition du lambeau: Fascio-cutané
– Fascio-cutané : fin et plastique +/- dépend du patient et du sexe. Utilisé comme un lambeau ultra-fin
• Taille de la palette cutnée: 20 x 12 pour une fermeture directe– Musculo-cutané avec le muscle vaste externe– Composite ou chimérique avec tissus du voisinage (rectus antérieur, TFL, crête
iliaque)3- Type de vascularisation: pédicule LCFA, branche descendante
– Direct septo-cutanée (type B) ou perforante septo-cutanée (type E)– Direct cutanée d’une artère musculaire (type C) ou perforante d’une artère
muusculaire (type D)4- Type de transfère :
– Pédiculé en îlôt vasculaire (longueur du pédicule de 10 à 20 cm) à flux antérograde (reconstruction abdominale) ou à flux rétrograde (reconstruction du genou)
– Libre (reconstruction de la tête et cou, autres régions ayant de besoin d’une vaste palette cutanée
5- Préparation préopératoire: aucune
• Couverture de pertes de substance cutanée:– Joue et larges pertes de substance cervico-faciale
– Abdomen
Lambeau antéro‐latéral de cuisseIndications
– Membres
• Reconstruction de la cavité buccale:– Reconstruction de la langue
• Reconstruction complexe tridimentionnelle de la tête et du cou comme lambeau composite
Lambeau antéro‐latéral de cuisseExemples de cas cliniques
Sarcome radio‐induit de la joue: exérèse transfixiante

13
Composite flap with rectus femoris
Type E perforator
Collateral for rectus femoris
Métastase pariétale cancer du col de l’utérus
• F 45 ans
• PDS 7 x 14 cmabdomenabdomen
• Lambeau musculo-cutané de vaste externe
• Pédiculé

14
1 an post-opératoire
Adénocarcinome récidivant de la tempe
• F 63 ans
• PDS 8 x 13 cmfosse temporale
• Comblement et couverture

15
• F 33 ans
• PDS abdominale
8 x 10 cm
Tumeur de Darrier Ferrand aine droite
• Lambeau sensible (nerf cutané fémoral latéral controlatéral)