la specificità del cardiopatico anziano con poli zuccalà ...c3%83%c2%a0.pdf · • pressione...
TRANSCRIPT
La specificità del cardiopatico anziano con poli‐morbosità
Giuseppe Zuccalà
Key points:1‐ Evidence‐Based Medicine nel cardiopatico anziano2‐ Reazioni avverse da farmaco nel cardiopatico
anziano3‐ La valutazione multidimensionale

Medical practice: the new way
The past two decades have urged physicians to become familiar with
the data from RCT, systematic reviews, meta-analyses.
Dr.Sackett called for a new approach to the practice of medicine. The
era was born of
EVIDENCE BASED MEDICINE

Age 61±11 71±7 67±10 61±10 65±12 63±11
ACE-i ACE-i vs AR-AT1 AR-AT1 ß-block. Anti-Aldost. Digoxin
Metanalysis ELITE II VAL-HeFT Metanalysis RALES DIGPts 12763 Pts 3150 Pts 5011 Pts 9711 Pts 822 Pts 3397
Males (%) 81% 70% 71% 73% 73% 78%
NYHA III-IV no IV 48% 40% (III) 46% 95% 33%
Characteristics of Patients Enrolled in Randomized Clinical Trials on CHF
Comorbidity no no no no no no
Disability no no no no no no

Caratteristiche associate alla diagnosi di scompenso cardiaco in 32.243 pazienti (Studio GIFA)
CHF(n= 3.704)
Controlli(n= 28.539)
Donne 1.943 (53%) 14.131 (50%)
Età (anni) 78 ± 10 66 ± 18 *
Farmaci 9 ± 6 5 ± 4 *
Patologie 5 ± 2 3 ± 2 *
Diabete 735 (20%) 4.403 (15%) *
Score Charlson 2,3 ± 1,5 1,4 ± 1,9 *
* p < 0,0001

Proportion of the NHF population (20,338) meeting all enrollment criteria of clinical trials of pharmacological agents known to prolong life in patients
with heart failure.
%
Masoudi FA. Am Heart J 2003
0
5
10
15
20
25
30
35
65-69 70-74 75-79 80-84 85 +
SOLVDMERITRALES

EBM and Geriatrics
•Frail elderly are systematically excluded from RCTs•Those included are “superfit”, “young- old” randomized patients• A new form of EBM is in place:
EVIDENCE “BIASED” MEDICINE

Trial sull’ipertensione nell’anziano precedenti l’HYVET
Trial Età media Risultati
The Medical Research Council (MRC) 70 Non effetti sulla mortalità
The European Working Party on High Blood Pressure in the Elderly (EWPHE)
72 Non benefici negli >80
The Swedish Trial in Old Pateints with Hypertension (STOP-Hypertension)
76 Non benefici negli >80
The Systolic Hypertension in the Elderly Program (SHEP)
71 Non effetti sulla mortalitànegli >80
The Systolic Hypertension in Europe (Syst-Eur)
70 Mortalità↑ negli >80 trattati

- Bias di selezione dei pazienti;
- Incompleta definizione delle variabili confondenti;
- Insufficiente conoscenza della terapia antipertensiva effettivamente utilizzata (es. nel Syst-Eur alcuni partecipanti assumevano anche enalapril e/o idroclorotiazide; il trattamento di altri partecipanti era ignoto);
- Definizione variabile del target del trattamento (es, nello SHEP un soggetto con una pressione al baseline di 219 mmHg era considerato trattato con successo se arrivava ad un livello di 195 mm Hg).
Fattori confondenti da considerare:

Differenze tra la popolazione dello studio SHEP e le popolazioni di pari età nei siti di arruolamento
0
5
10
15
20
25
Demenza Depressione Disabilità
SHEP Popolazioni generali
%

Prevalenza di ipertensione e deficit cognitivo (AMT < 7) nei 32.242 anziani arruolati nello studio GIFA.
0
10
20
30
40
50
60
< 65 65-74 75-84 85 +
IpertensioneDeficit cognitivo

Caratteristiche associate alla diagnosi di ipertensione arteriosain 32.243 pazienti (Studio GIFA)
Ipertensione(n= 8.208)
Controlli(n= 24.035)
Età (anni) 72 ± 12 69 ± 17 *
Farmaci 7 ± 6 6 ± 4 *
Patologie 4 ± 2 3 ± 2 *
Diabete 1.864 (23 %) 3.251 (13 %) *
AMT† < 7 1.131 (25 %) 3.745 (30 %) *
BPCO 1.053 (13 %) 3.442 (14 %)
Score Charlson 1,5 ± 1,5 1,4 ± 1,8
* p < 0,0001† Abbreviated Mental Test

Fattori associati all’uso di antipertensivi
nell’Health, Aging, and Body Composition Study (Health ABC)
Fumo Alcol
Verdura Caffè
Scolarità Introito economico
Estrogeni Esercizio fisico
Relazioni sociali Obesità
Polivitaminici Depressione
Colesterolemia Anemia
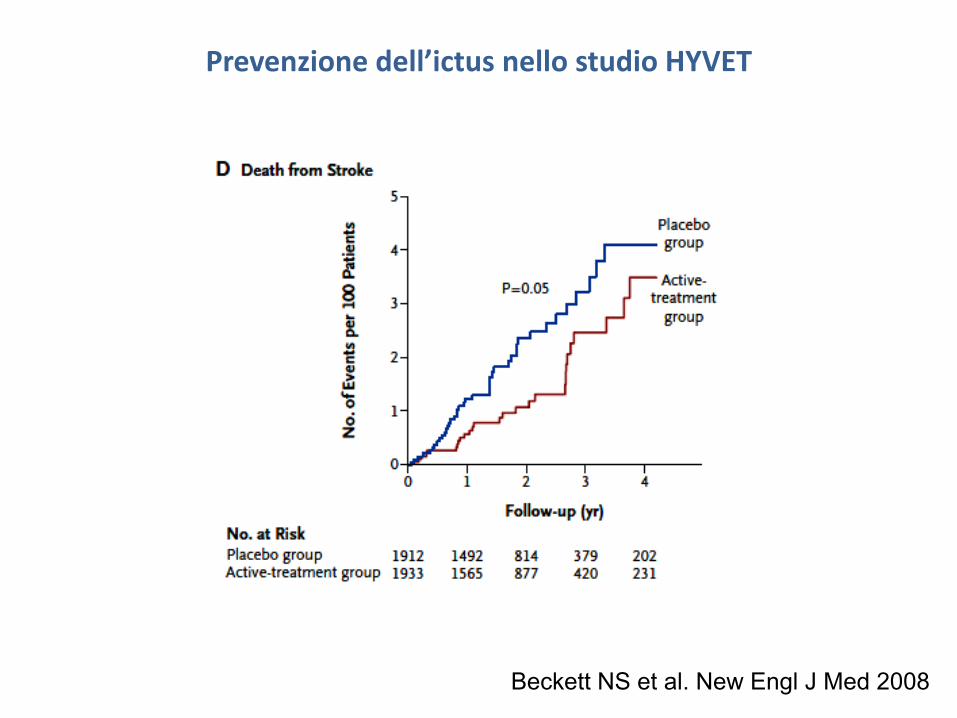
Beckett NS et al. New Engl J Med 2008
Prevenzione dell’ictus nello studio HYVET

Prevenzione dell’ictus nello studio HYVET
Beckett NS et al. New Engl J Med 2008

Criteri di ammissione all’HYVET; trattamento.
• Età ≥ 80 anni;
• Pressione arteriosa (4 misurazioni; terapia antipertensiva sospesa per 2 mesi) ripetutamente compresa tra 160 e 199 mm Hg.
• Trattamento con placebo vs. indapamide (1,5 mg), più eventualmente perindopril (2 o 4 mg) o placebo, più eventualmente altro antipertensivo, a discrezione dei medici.
• Obiettivo ottimale: Pressione arteriosa <150/80 mm Hg.

Sarwat I. JAMA. 2004
Systolic Hypertension in Older Persons
“Treatment of SH in older patients with SBP of at least 160 mm Hg is
supported by strong evidence. The evidence available to support
treatment of patients to the level of 140 mm Hg or those with baseline
SBP of 140 to 159 mm Hg is less strong; thus, these treatment
decisions should be more sensitive to patient preferences and
tolerance of therapy.”

Tulner LR et al. Am J Geriatr Pharmacother 2009
Treatment of Hypertension in an Elderly OutpatientPopulation in the Netherlands

Associazione tra numero di farmaci assunti ed incidenza di ADR
Carbonin P et al. J Am Geriatr Soc 1991

Butt TF et al. J Hum Hypertens 2010
Managing hypertension in the very elderly:effect of adverse drug reactions (ADRs) on achieving targets
In 64 out of 100 patients the ambulatory blood pressure monitoring confirmed poor blood pressure control. Despite this, 26 of these patients had an antihypertensive either stopped, and /or reduced or left unchanged at clinic because of documented adverse drug reactions (ADRs)... antihypertensive agents were either stopped, and or reduced because of ADRs in half the patients from the well-controlled group.
This study highlights the difficulties of treating patients of 80 years and over with antihypertensives even when the target blood pressure is relatively modest (150mmHg). Almost half the patients had documented ADRs, which limited further intervention in 40 out of 100, or had very low blood pressure that necessitated withdrawal of therapy (4 patients) to avoid troublesome postural symptoms... implementation of the HYVET recommendations in clinical practice may be difficult.

Duprez DA et al. J Hum Hypertens 2009
Aliskiren for Geriatric Lowering of Systolic Hypertension: a randomized controlled trial

Peters R et al. Lancet Neurol 2008
Incident dementia and blood pressure lowering in theHypertension in the Very Elderly Trial cognitive function
assessment (HYVET‐COG)

Zuccalà G et al. Neurology 2001.
<120 120-129130-139 140-149 150-159160-169 ≥170
0.5
1
2
Systolic blood pressure (mm Hg)
Odd
s ra
tio
Ipotensione e deficit cognitivo – associazione selettiva negli anziani con scompenso cardiaco

Georgiadis D, Eur Heart J 2000
Cerebrovascular reactivity is impaired in patients with cardiac failure

Raymond I. et al. Heart. 2003
Prevalence of impaired left ventricular systolic function and heart failure in a middle aged and elderly urban population segment of
Copenhagen.
“Asymptomatic cases accounted for 44.0% of all cases of systolic dysfunction in the male population and only 9.1% in the female population.”

Survival according to cognitive impairment among 1,113 older patients with heart failure
Zuccalà G et al, Am J Med 2003
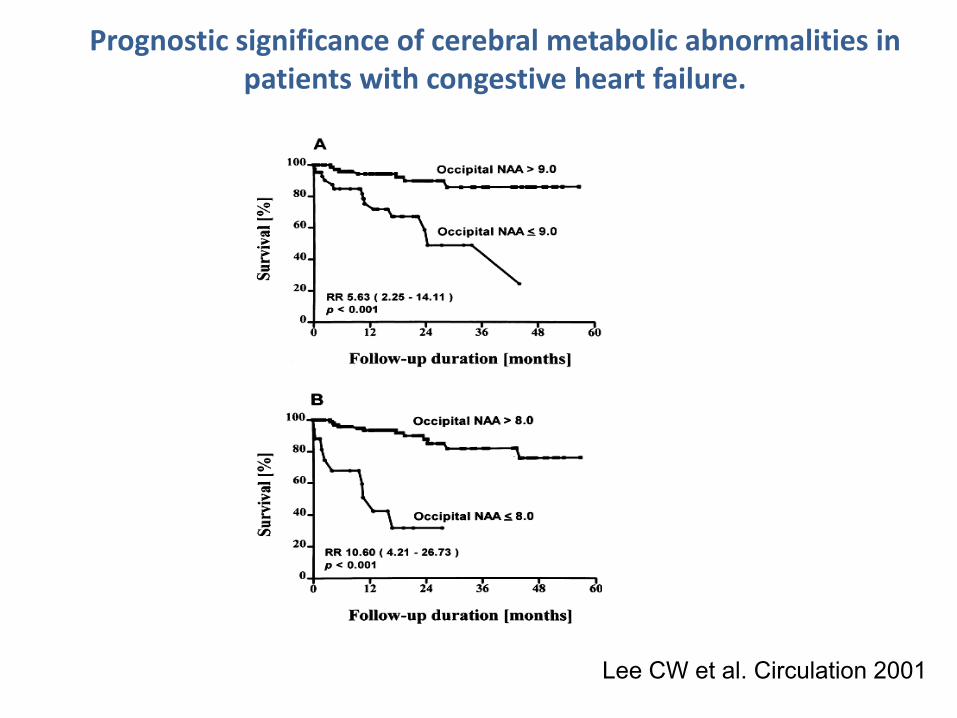
Lee CW et al. Circulation 2001
Prognostic significance of cerebral metabolic abnormalities in patients with congestive heart failure.

Cohn JN. N Engl J Med 2001
A RANDOMIZED TRIAL OF THE ANGIOTENSIN‐RECEPTOR BLOCKERVALSARTAN IN CHRONIC HEART FAILURE

Progress in heart failure management? Lessons from the real world
“In these findings, we see the reason… for concern that our clinical trials
are leaving gaps in our knowledge… several factors may contribute to this
finding in the elderly, including… reduced responsiveness or tolerance to
treatments”.
Konstam MA. Circulation 2000

National Trends in Outcomes Among Elderly Patients with Heart Failure
“We found no substantial improvement in mortality and hospital
readmission during the 1990s among elderly patients hospitalized with
heart failure. These findings suggest that recent innovations in heart failure
management have not yet translated into better outcomes in this
population.”
Kosiborod M Am J Med 2006

La definizione di anziano “fragile” secondo le linee guida SIGG‐SIMI.
“…soggetti di età avanzata o molto avanzata, cronicamente affetti da
patologie multiple, con stato di salute instabile, frequentemente disabili,
in cui gli effetti dell’invecchiamento e delle malattie sono spesso
complicati da problematiche di tipo socio-economico. ”

Ferrucci L et al. Circulation 2001
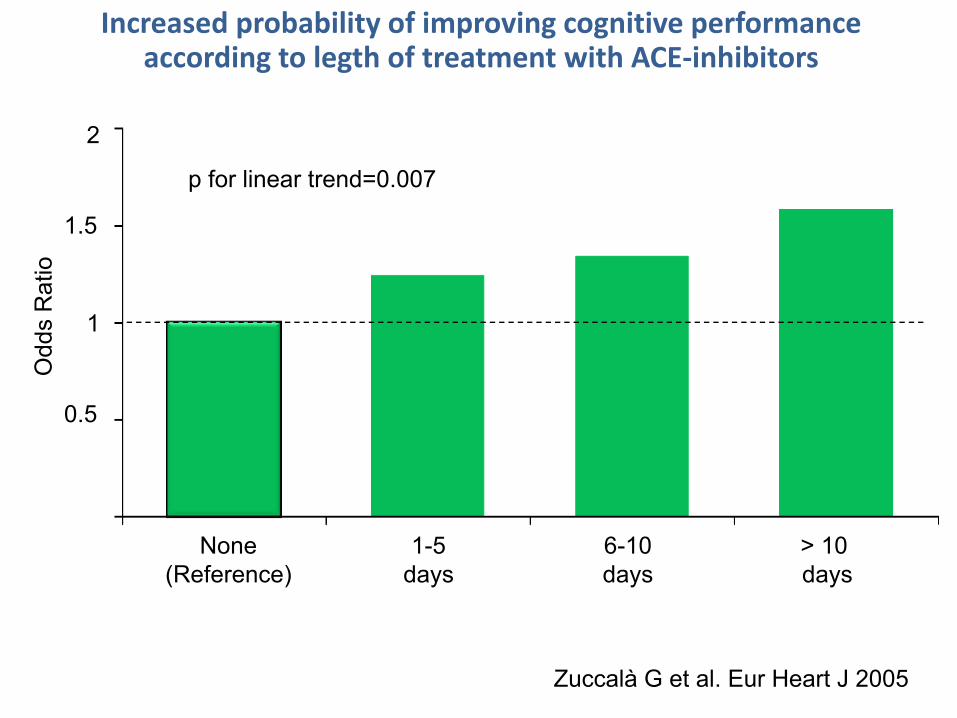
> 10 days
6-10days
1-5days
None(Reference)
p for linear trend=0.007
Odd
s R
atio
0.5
1
1.5
2
Increased probability of improving cognitive performance according to legth of treatment with ACE‐inhibitors
Zuccalà G et al. Eur Heart J 2005

Odd
s R
atio
p for linear trend=0.001
0
0,5
1
1,5
2
None(reference)
Low dose High dose
Increased probability of improving cognitive performance according to increasing dosages of ACE‐inhibitors
Zuccalà G et al. Eur Heart J 2005

Variazioni della funzione cognitiva nello SCOPE in rapporto al trattamento con Candesartan in soggetti con funzione cognitiva
normale o ridotta al baseline
Skoog I. Am J Hypertens 2005;18:1052

Lou M et al. Sustained blockade of brain AT1 receptors before and after focalcerebral ischemia alleviates neurological deficits and reduces neuronal injury, apoptosis, and inflammatory responses in the rat. J Cereb Blood Flow Metab2004.
Dai W et al. Blockade of central angiotensin AT1 receptors improvesneurological outcome and reduces expression of AP-1 transcription factors afterfocal brain ischemia in rats. Stroke 1999.
Li J, Culman J et al. Angiotensin AT2 receptor protects against cerebralischemia-induced neuronal injury. FASEB J 2005.
Fournier A et al. Cerebroprotection mediated by angiotensin II – a hypothesissupported by recent randomized clinical trials. J Am Coll Cardiol 2004.

Zuccalà G et al. Eur Heart J 2005

Laudisio A. et al. Drugs & Aging 2009
Unadjusted
Age- and sex-adjusted
Full adjusted
No CHFCHF
1 2 3
Probability (Odds Ratios, 95% CI) of improving cognitive performance according to starting treatment with digoxin
in 1590 older patients with heart failure

Kilander L et al. Stroke 1998
“Men with atrial fibrillation who were treated with digoxin…performed
markedly better than those without treatment… The difference
remained highly significant after adjustment for 24-hour diastolic blood
pressure, heart rate, and diabetes. Ejection fraction did not differ…”.
Atrial fibrillation is an independent determinant of low cognitive function

Watta M et al. Life Sci 2004
“A close relationship between Na, K-ATPase activity and
neurotransmitter release has been demonstrated…Ouabain, a
selective and specific Na, K-ATPase inhibitor, increases acetylcholine,
5-hydroxytryptamine, and catecholamine release…”.
Endobain E, a brain Na+, K+ ‐ATPase inhibitor, decreases norepinephrine uptake in rat hypothalamus
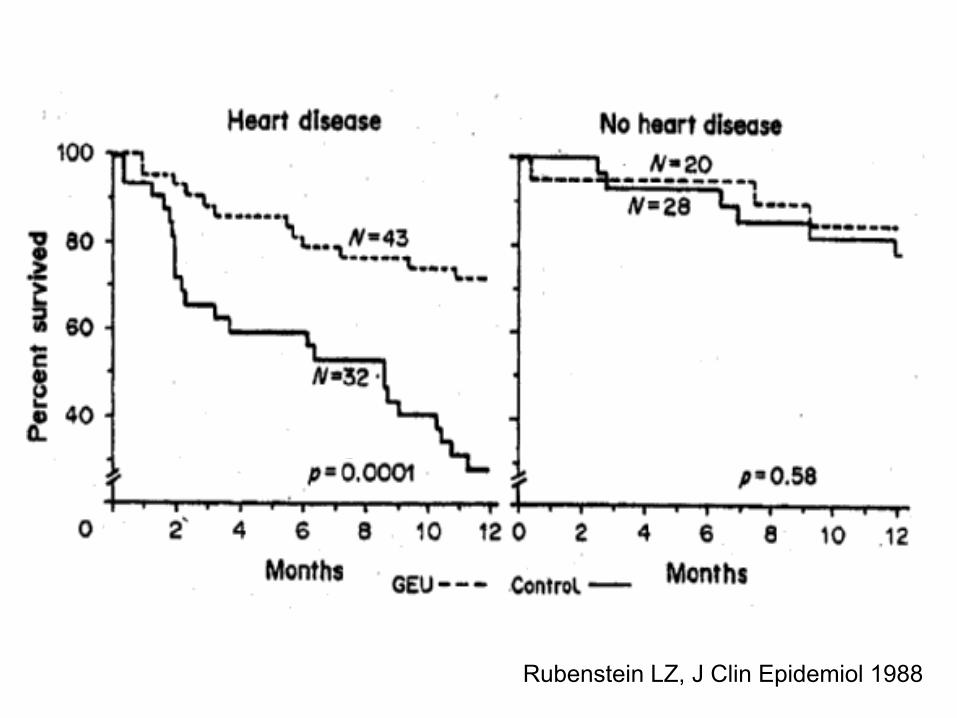
Rubenstein LZ, J Clin Epidemiol 1988

Geriatric Conditions and Subsequent
Mortality in Older Patients With Heart Failure
%
Chaudhry. SI et al. JACC 2010

interRAI NationsNordic Countries
Iceland, Norway, Sweden, Denmark, Finland
EuropeNetherlands, Germany, UK, Switzerland, France, Poland,
Italy, Spain, Estonia,Czech Republic
Far East/Pacific RimJapan, South Korea, Taiwan,
Hong Kong, Australia, New Zealand, China
Middle EastIsrael
North AmericaCanada
US

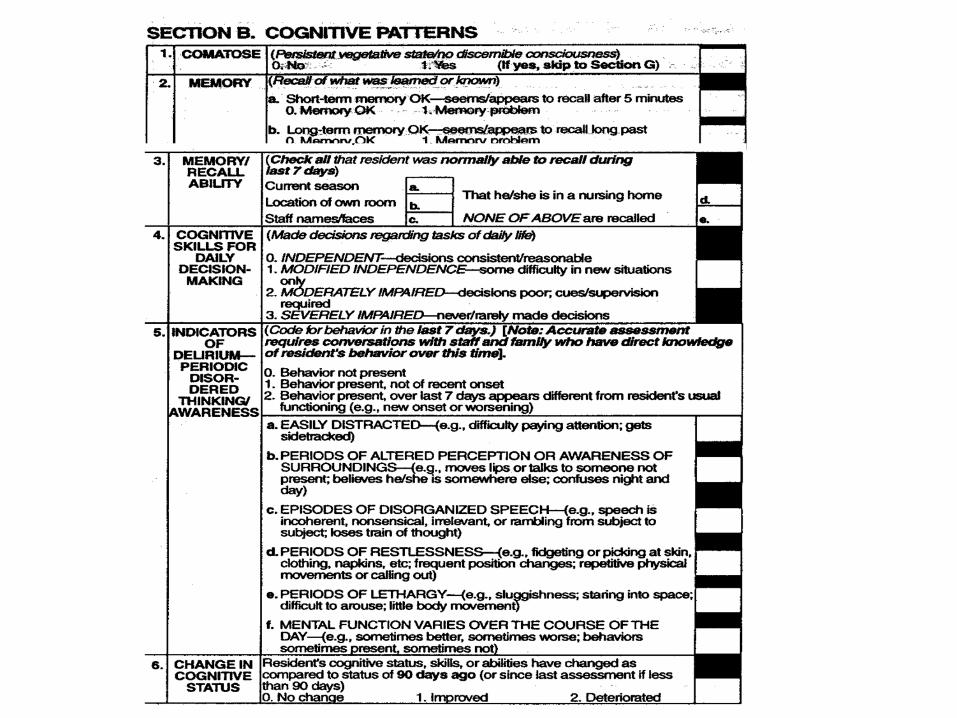
AREE VALUTATE DA VAOR
Stato cognitivo Stato confusionale acuto
Comunicazione Sfera visiva
Umore/comportamento Benessere psicosociale
Capacità funzionale Continenza
Mezzi di contenzione Stato nutrizionale
Stato oro‐dentale Decubiti
Attività Sondino naso‐gastrico
Uso di psicofarmaci Cadute

Potentially Inappropriate Medication UseAmong Elderly Home Care Patients in Europe
“Combining all 3 sets of criteria, we found that 19.8% of patients in the
total sample used at least 1 inappropriate medication… Potentially
inappropriate medication use was associated with patient's poor
economic situation, polypharmacy, anxiolytic drug use, and
depression. Negatively associated factors were age 85 years and
older and living alone. ”
Fialova D et al. JAMA 2005

Potentially Inappropriate Medication UseAmong Elderly Home Care Patients in Europe
Fialova D et al. JAMA 2005

Venkitachalam L. JACC. 2010
Stepping Outside of the Heart ‐ Using Nontraditional Patient Characteristics to Understand and Improve Outcomes
“Chronic diseases in the elderly, especially HF, must be recognized as
occurring within a complex construct of unique medical, behavioral,
psychosocial, and economic factors that requires a holistic approach
that should be individually tailored to meet each patient’s needs and
expectations.”