karuna (compassion) project - emms international · health system. the karuna project's role...
TRANSCRIPT
KARUNA (COMPASSION) PROJECT
Mid-Term Evaluation
Authors: Dr. Shantidani Minz and Dr. Harika Siddabathula
Project Delivered by: EMMS International and Duncan Hospital
Purpose of the report The purpose of the mid-term evaluation was to assess how well the project is meeting its objectives as per the modified plan and what are the main learning points. Christian Hospital, Chhatarpur and Duncan Hospital, Raxaul are two EHA hospitals with project funding from EMMS with similar broad goals, and the purpose was also to identify common indicators for both.
The questions specified in the TOR for mid-term evaluation were:
Are the objectives/issues stated in the project plan being addressed adequately?
Will the inputs through the project have a long term effect on the health of the community and are these expandable to more areas served by Duncan Hospital?
What are the learning points from this project for project staff and Duncan hospital management and administration that will help project staff to be more relevant and effective in addressing the health needs of the local communities?
Are data for publication and research from the project being captured?
Biographies of the authors Dr. Shantidani Minz, MD, MPH, is a professor of Community Health from the Community Health Department of Christian Medical College (CMC) Vellore. She has worked in rural north India in a mission hospital and with the Christian Medical Association of India and is a faculty in CMC. She has 20 years experience in the field of community health, programmes and training and has been involved with programme evaluations in north and south India.
Dr. Harika Siddabathula (MD) is a resident in Community Medicine in CMC and has worked in rural mission hospitals for 2 ½ years in north India.
Acknowledgments The evaluation team would like to thank EMMS International and Duncan Hospital, Raxaul for the opportunity to evaluate this unique project in one of the most needy districts of Bihar. The team would also like to thank all the staff of Karuna project and other community health projects of Duncan hospital, groups and individuals met, especially the doctors and nurses at the three PHCs for their support and valuable information provided to the team during the course of the evaluation. Special thanks go to Dr. Vandana, Dr. Sharon and Mr. Sumit for their valuable inputs towards planning and interpretation of the findings.
The cover photograph is of the Karuna project team in Duncan Hospital.
2
Contents Purpose of the report ............................................................................................................ 2 Biographies of the authors .................................................................................................... 2 Acknowledgments ................................................................................................................. 2 Contents ............................................................................................................................... 3 Acronyms .............................................................................................................................. 4 Executive Summary .............................................................................................................. 5
Major Findings ................................................................................................................... 5 Recommendations............................................................................................................. 6
Introduction ........................................................................................................................... 8 Project background............................................................................................................ 8 Methodology and limitations ............................................................................................ 11 Context analysis and project planning ............................................................................. 11
Findings .............................................................................................................................. 15 Project implementation and possible modifications .......................................................... 16 Project objectives and assumptions ................................................................................. 18 Implementation, achievements and performance of overall objectives............................. 20 SWOT Analysis and brainstorming by project staff .......................................................... 27
Compliance with EMMS International Operational Framework ............................................ 29 Coherence with the vision and mission of EHA ................................................................ 29 Compliance with overall Operational Framework ............................................................. 29 Sustainability of the initiative ............................................................................................ 29
Learning and Conclusions ................................................................................................... 30 Recommendations .............................................................................................................. 31 Annexes .............................................................................................................................. 33
Annex 1: Terms of Reference .......................................................................................... 33 Annex 2: Methodology ..................................................................................................... 37 Annex 3: Duncan Hospital Community Projects Timeline ................................................ 38 Annex 4: People met during evaluation ........................................................................... 50 Annex 5: Evaluation Programme ..................................................................................... 53
3
Acronyms
ANM - Auxiliary Nurse Midwife
ASHA - Accredited Social Health Activist
AWC - Anganwadi Centre (day care centre run by the government)
AWW - Anganwadi Worker
AYUSH - Physician trained in Indian systems of medicine
CHC - Community Health Centre (Government health care institution)
EHA - Emmanuel Hospital Association
IEC - Information, Education, Communication
ICDS - Integrated Child Development Services
NGO - Non-Governmental Organisation
NRHM - National Rural Health Mission
PO - Project Officer
PHC - Primary Health Centre
RCH - Reproductive and Child Health
SC - Subcentre
SWOT - Strengths, Weaknesses, Opportunities, Threats
VHND - Village Health and Nutrition Day
VHSC - Village Health and Sanitation Committee
4
Executive Summary EHA and EMMS International have worked together to bring transformation in the lives of
people from many underdeveloped parts of North India for a long period. Duncan Hospital
has had a long history of engaging with the local communities based on the needs of the
time and vision of the institution, and currently has eight community health projects in
various stages of their existence. The KARUNA project is the first of its kind where
engagement with the community for improving Maternal and Child Health is linked with
clinical services of the hospital through special funding for increasing the capacity of the
clinical department.
The project plan was modified based on the findings of a situation analysis carried out at the
start of the project. The mid-term evaluation was proposed to assess the progress made and
lessons learned that would influence the future direction of the Karuna project and guide all
projects with community engagement.
Major Findings The project is focussing on a change in key behaviours that lead to demand for preventative
and curative services of the healthcare delivery system under the banner of the National
Rural Health Mission (NRHM), and matching that with quality improvement in the public
health system. The Karuna project's role is facilitatory and catalytic, with Duncan hospital
providing tertiary level clinical services for mothers and children. This is a daunting task in
Purba (East) Champaran District of Bihar, which has never been a focus for development.
Being on the border with Nepal, the blocks close to Duncan Hospital are difficult for
development programmes, with high migration and trafficking and a great shortage of
indigenous workforce for health programmes.
The project's effort towards improving the quality of health services through skills training of
government functionaries has been limited, since few ANM (Auxiliary Nurse Midwife) training
sessions have been done so far. ASHA (Accredited Social Health Activists) and ICDS
(Integrated Child Development Services) workers are more available. Permissions and
access to ANMs is difficult, because of their preoccupation with immunisations in recent
months and because CARE India is currently the official partner in Bihar for quality
improvement. The project is supporting the work of ANM and meeting with the subcentre
level group to improve their knowledge. Input at the PHC level has not been possible and
monitoring of PHC functions has not been done.
5
The activities towards changing key behaviours for healthy lifestyles are done through
community action groups, of which the adolescent boys’ and girls’ groups are the most
promising. Peer educators from adolescent groups are coming forward to address issues
that will result in social change. Community workers at the grassroots level who come from
the target villages are the key change agents.
The referral system for very sick children or complicated pregnant women is working well,
since PHCs refer patients to Duncan Hospital readily. However, the cost of care at Duncan
hospital is a cause of concern and the management is working on a system for providing
concessional treatment to patients from project areas.
Recommendations The government healthcare delivery system is deficient in human resources, infrastructure
and skills in delivering the standard of care set by the NRHM. While the government health
department works towards bridging the gap, many NGOs are involved in supporting the
work. Since Duncan Hospital has contributed for a long time to this district's healthcare and
gained the trust of local people, the Karuna project is well positioned to contribute actively to
change in the health status of the community.
In order to improve the quality of services, the Karuna project will need:
→ To go into a collaborative relationship with other participating NGOs in the district and
the government programme
→ To fill in the gaps that exist in planning, implementing and monitoring field
programmes. Project staff will need to complement the work of ANM and ASHA in the
field.
→ Efforts for community mobilisation and behaviour change need to concentrate on the
groups that are working well and show promise. These groups should be built up as
hubs with skills to initiate newer groups for dissemination of knowledge and skills, and
action. They should also be seen and promoted as agents for challenging the whole
community together for action to achieve health and long-term social change.
6

7
Introduction Project background The Duncan Hospital, Raxaul is a member hospital of Emmanuel Hospital Association
(EHA). It is situated in East Champaran District of Bihar which has amongst the poorest
health and development indicators in India. Being on the border of India and Nepal, this
hospital serves approximately 11 million people from surrounding parts of Bihar and
Southern Nepal. Founded by Dr. H. Cecil Duncan in 1930 and shaped by Drs. Mathew and
Joanna Peacock and by Drs. Trevor and Patricia Strong, this hospital developed into a
referral centre for providing essential medical and surgical services in this remote location. It
was managed by the Regions Beyond Missionary Union until 1974 and later handed over to
EHA.
The hospital has been challenged by the needs of the local community, and many
community projects have evolved over time in response. The relationship with EHA has led
to alignment with the vision and mission of EHA in responding to community needs around
the hospital. EHA has identified focus areas for all its hospitals working in the community,
and so Duncan Hospital’s community initiatives are aligned to these.
The Community Health projects of Duncan hospital have addressed issues such as
immunisation, mental health, community-based rehabilitation, HIV/AIDS, and capacity-
building for improving access to health services. Many of these projects link to the hospital
for referral of patients and technical support. However, Karuna project is the first to have a
defined collaboration with Duncan Hospital’s clinical services and a linkage for improving
maternal and child health care.
EMMS International is a charity based in Edinburgh, Scotland, working with EHA to address
maternal and child health (MCH) in north India. Duncan hospital is the implementing partner
for a time-bound project, Karuna, to improve maternal and child health in three Community
Development Blocks of East Champaran District of Bihar state.
History of Community Health initiatives of the Duncan Hospital Duncan Hospital is situated in a challenging environment. Being at the Indo-Nepal border, it
has been catering to the citizens of both countries, most recently during the massive
earthquake of April 2015. Traditionally, Duncan Hospital has provided high quality obstetric,
surgical and medical care to people from Bihar, UP and Nepal. In many ways it has been the
hospital for complicated cases in this region. The need for high volume clinical services has
lead to a persistent need for more and more doctors and nurses. Alongside this, there has
been awareness of the need to address health issues beyond the boundaries of the hospital.
A summary response of the hospital is presented in Annex 2. It reflects the development of
community health response in the country as a whole, starting with an outreach approach for
8
clinical services, specific disease responses and then widening out to address other
determinants of health such as livelihoods. While community engagement or
communitisation became an important area for NGO workthe to support National Rural
Health Mission, the Duncan Community Health team also addressed vulnerable groups in
society, including the disabled, mentally ill and those at risk of trafficking.
While many issues directly and indirectly related to health are of great concern in this area,
mothers and children of East Champaran District of Bihar continue to be at a disadvantage,
with inadequate preventative and curative services. CHETNA (Centre for Health, Education,
Training and Nutrition Awareness) and RCH (Reproductive and Child Health) projects have
been working in this field, trying different approaches and resulting in improved awareness
and use of services, but most projects have had a limited area for implementation, resulting
in valuable learning but limited impact.
Despite strides made with NRHM and many RCH programmes, quality care during
pregnancy and childbirth and better health of women and children in the region has not yet
been ensured. The Bihar government is collaborating with many NGOs to address this, but
East Champaran still lags behind with poorer health indicators. The Duncan Hospital team
identified as a challenge to build the capacity of the public health system through skills
enhancement and an effective network for referrals, to reduce morbidity and mortality among
mothers and babies.
Uniqueness of the Karuna Project The KARUNA project is envisaged to address two important issues leading to poor health
outcomes for women and children:
1. Lack of good quality health services and
2. Lack of demand for quality health services by the communities.
The project is building on the experiences of earlier community projects to increase
awareness and demand generation for preventative and curative health services and change
in behaviours leading to better health. The strategy combines community organisation and
awareness for positive health through action groups. The expectation is that small
homogenous community groups of older women (mothers-in-law), pregnant women, men
and adolescents will develop into action groups which will ensure promotional, preventative
and appropriate health-seeking behaviours for and by women and children.
In order to meet the demand thus generated, the Karuna project expects to match it with
quality preventative and curative health services, through the combined efforts of the
government health system and Duncan Hospital. Duncan Hospital is currently providing
tertiary level referral care for obstetrics cases and for sick children for many blocks of
districts. The Karuna project’s strategy is to ensure adequate skills for health personnel from
9
primary to higher level, appropriate facilities at each level and a functioning referral system
from the village and PHC to Duncan Hospital, for cases needing this.
This is the first community project addressing capacity-building within Duncan Hospital to
meet the needs generated by a community health project. The project is contributing to the
training of specialists and additional equipment for complicated obstetric and paediatric
patients.
Previous project input in the Karuna project area All three blocks have had some input through previous community projects of Duncan
Hospital. Of the three, Adapur block has had the most input, in the areas of HIV/AIDS, RCH,
Community Based Rehabilitation and trafficking, and Ramgarhwa has had the least input,
even though Champapur clinic has been running in this block for a long time and the school
of nursing makes home visits in this block. (See Annex 3.) The most beneficial effect of
previous projects is the rapport with the community. While Adapur and Raxaul villages are
easier to work with and the relationship with health staff is good, Ramgarhwa is a new area
for the hospital, with new challenges. Duncan Hospital has worked on RCH and VHSC
(Village Health and Sanitation Committee) formation and training in Adapur block for a long
time, under its CHETNA project, and established two RCH clinics there. The RCH nurse in
charge of these RCH clinics was well known in the community and had built a strong
relationship with the government PHC in Adapur. Under the Karuna project, these RCH
clinics were merged and moved to a more central location, at the request of patients. The
RCH clinics run by CHETNA have contributed greatly to the rapport with the community with
government healthcare providers in Adapur.
Relevance of the Karuna Project The current situation of the health system and gaps in human resources and services make
it necessary for Duncan Hospital to contribute to addressing some of these through
supportive action and bridging the gaps in care. East Champaran District has very poor
health indicators, which have not improved even with inputs from the NRHM, as the district
has not been able to implement the recommended changes and upgrade services. Being on
the border brings its own problem of issues with, most recently, the effects of Nepal's and
India’s somewhat confrontational relations. This prevents implementation of many
development activities. Migration is a challenge for government systems, an area to which a
private player like Duncan hospital can contribute significantly. The area has poor roads and
poor transport infrastructure, making healthcare inaccessible to most of the population, and
making it essential for projects to complement the government, to reach remote villages for
health service delivery.
10
Methodology and limitations The Karuna project has been functioning for only one and a half years, and so a deliberate
decision was taken to concentrate on processes rather than on outcomes and indicators.
Therefore, data related to the project was not considered in this evaluation. The final
methodology for the evaluation was decided based on ideas evolving from discussion with
the project leaders and field staff, some of whom have been involved in other community
health projects of Duncan Hospital. The experiences of the hospital’s earlier community
projects was incorporated, to identify and describe the specific contribution of the Karuna
project.
The methodology followed is represented in a flow diagram in Annex 2.
The evaluators reviewed all project documents and reports provided by the project
implementers before the evaluation, to draw up a tentative plan for field work and interaction
with specific groups. After collection of data from the field, the evaluators reviewed the
documents again, to clarify issues, inputs and strategies for interpretation and report writing.
Additional documents, such as maps, data collection format, field reporting format and
monthly reports, were made available for the team when asked.
The evaluators observed facilities for maternal and child care in the 3 blocks’ PHCs, 1
subcentre, 2 ICDS centres, Duncan hospital's Adapur and Champapur centres, and the Out-
Patient and In-Patient facilities at Duncan hospital. We used IPHS (Indian Public Health
Standards) as the guideline for expected standards.
It was found imperative that the Karuna project be seen as a component or a part of Duncan
Hospital's (and EHA's) response to the needs of the larger communities served by the
hospital. For this the evaluators needed to see the larger picture, and Dr. Sharon Cynthia put
together a comprehensive document to decipher this complex picture. (See Annex 3.)
Both evaluators met with the coordinating people, Dr. Vandana Kanth, Dr. Sharon Cynthia
and Mr. Sumit Khalkho for an overview and discussion on the direction of the evaluation.
The evaluation’s final plan was based on their input and that of other project staff,
concerning feasibility of meetings and observations in the three blocks under the project.
Details are given in Annex 4.
Context analysis and project planning Health system in Project Area: Challenges and gaps Purba (east) Champaran District headquarters is in Motihari, which is 40 to 70 km by road
from three block headquarters. The district hospital is located in Motihari. The three blocks in
the project are adjacent to each other, each with a designated block PHC (equivalent to
CHC) and all belonging to Raxaul subdivision. The health infrastructure is poorly developed
in all three blocks, with only one functional PHC in each block, although additional PHCs
11
exist in the official plan. Some conduct Out-Patient services, when doctors can be spared
from their main PHC work.
Each of these blocks has a population close to 200,000, with each ANM covering a
population of nearly 10,000, compared to the recommended 5,000. There is a shortage of
human resources, with 2 to 3 MBBS doctors and 4 PHC nurses per PHC and a shortage of
ANMs for public health work. Although male MPHWs are supposed to work alongside ANMs,
most of these posts are vacant. Subcentre and PHC infrastructure is inadequate. This
results in inadequate coverage of the population by ANM and concentration on a few service
activities such as immunisations and VHND (Village Health and Nutrition Days).
Until recently, immunisation coverage was very low in the project area and the programme
has concentrated on improving it. ANM, AWW and ASHAs come together fortnightly to plan
activities and generate a due list for immunisation. Most of the ANMs are currently occupied
with catching up on a backlog of primary immunisations. This has also become the main
activity for ASHAs who are primarily responsible for making the due list for every VHND and
going house to house to motivate beneficiaries. ASHAs are also responsible for
accompanying women to the 24x7 PHCs which provide delivery care.
ANMs’ time is taken up fully in organising these activities, reporting, attending reviews and
attending training run by many NGOs who are involved with NRHM programmes.
Ayush doctors in PHCs are expected to oversee school health programmes, but are unable
to fill the need of PHCs’ clinical work.
The new PHC building in Adapur has a good space and 30 beds, but additional nursing or
support staff to maintain the structure are not available.
Raxaul is located on the border with Nepal and this border town has a hospital with multiple
specialities. However, complicated cases are referred to Duncan hospital.
Basic training of ANMs is lacking in quality, since they are trained by different private
institutions which lack skills training. Most of them come from other districts, as the
educational achievement of women and girls is very low in East Champaran. This also
results in lower motivation.
Apart from poor infrastructure and quality of services, government PHCs are plagued with
corruption. Patients are required to pay to receive care. This prevents many poor people
going to PHCs.
Preparatory phase and modifications in proposal The first proposal was prepared by Dr. Vandana Kanth with inputs from EMMS. This was
modified subsequently, based on findings of a needs assessment which used qualitative
methods and a baseline survey report which brought out huge gaps in antenatal and child
care. The decision was taken to address behaviours that will lead to long term change in
health status rather than influencing short-term but measurable indicators. Based on the plan
12
of project personnel, the direct target population was reduced. However, training input for
quality improvement in health services was maintained for all government health workers. Hierarchy and responsibilities Dr. Vandana Kanth is the director of the Community Health Department and oversees all
planning, implementation and monitoring of the Karuna project. Dr. Sharon Cynthia and Mr.
Sumit Khalkho are responsible for detailed implementation, monitoring, review and revision
of plans and activities.
RCH nurses support clinics at Adapur and Champapur and the Block team with
implementation of activities at community level, and training of government staff,
complementing service delivery at VHND. They also interact with Duncan Hospital
functionaries for referred patients.
Mobilisers and motivators work as a team for community mobilisation, community education
and implementation of all activities in the 10 villages of the block adopted by the project.
Mobilizers interact with block level government health system functionaries for planning,
collaboration for service delivery and feedback to the PHC team. They attend the block level
meetings at the PHC.
Motivators are voluntary workers from the community. They have designated villages and
may belong to one of the project villages. Male and female motivators tend to work together,
covering 4 to 5 villages rather than individually covering 2 to 3 villages. They are more
comfortable working with same-gender groups. Reporting is primarily done by the motivators
and mobilisers depending on the level of event or activity. Reporting of vital events is done
by the motivators. They are the functional link between project staff, community and the
village-level functionaries, ASHA and AWW.
Mobilisers are supervisory workers in principle, but as the project activities are in the
developing stage, they work mostly along with motivators.
Review of all Community Health Projects of Duncan Hospital to date It was found imperative that the Karuna project be seen as a component or a part of Duncan
Hospital's (and EHA's) response to the needs of the larger communities served by the
hospital. For this the evaluators needed to see the larger picture, and Dr. Sharon Cynthia put
together a comprehensive document to decipher this complex picture. (See Annex 3.)
Persons/groups met Both evaluators met with the coordinating people, Dr. Vandana Kanth, Dr. Sharon Cynthia
and Mr. Sumit Khalkho for an overview and discussion on the direction of the evaluation.
The evaluation’s final plan was based on their input and that of other project staff,
concerning feasibility of meetings and observations in the three blocks under the project.
Details are given in Annex 4.
13

Role of Duncan Hospital The hospital administration is part of planning the needs at hospital level for maternal and
child services. The requirements for equipment and staff were forecast based on current
utilization from the project area and type of service needs. The hospital supports the
Community Health Director with all administrative and management-related responsibilities.
The hospital management team is directly involved in reviewing progress and changes in the
project with the Community Health Director.
Recent plans are to bring all community health projects into a common platform to
complement and support each other. There is also a plan for a common review system,
which has already started.
14
Findings This is the first project linking a community health project to clinical service development or
enhancement at Duncan Hospital. The plans for input to the hospital systems were based on
the experience of the clinical department. Documentation of outputs and related outcome
needs were thought of by the team. The administration of the hospital is tuned towards
bringing the strengths of all community initiatives together and ensuring an active link
between hospital and local communities through community health projects.
The project modification reduced substantially the quantum of proposed activities and
population to be covered. The plan and details of activities were reorganised to follow the
logical framework’s original objectives and strategies. This has made the project more
doable and the objectives more likely to be achieved.
Duncan Hospital and its community health projects have developed a very good rapport with
the government health system and many other departments related to health. The project is
getting involved with skills training of ASHA, ANM and ICDS workers. There are hurdles in
addressing specific gaps in skills of workers and basic equipment to improve the quality of
care, as the need is high.
The healthcare delivery system in Purba Champaran District is not yet developed as per the
recommended standards under NRHM. The population covered by a PHC and ANM is much
more than the target maximum 30,000 and 5,000 respectively. There is a shortage of health
functionaries who belong to the district. Most of the staff are from other districts, creating
additional challenges for workers. Infrastructure development will take a long time.
Many other international and national NGOs are working in Bihar to support NRHM activities.
This is creating extra demands on staff for reporting and creating avenues for monitoring
needs of each. The Karuna project and Duncan Hospital could channel the efforts of all
groups, bringing the required and appropriate level of quality in training, monitoring and
reporting acceptable to all. The challenge is also not to burden staff.
The service delivery component of the Karuna project is supplementing basic MCH care for
a limited population in a few project villages around two centres in Adapur and Champapur.
While high quality of clinical care is provided, some of the components of antenatal care are
not available in the clinics. Linkages with the PHCs and Subcentre functionaries are not
clear. However, referral from PHCs to Duncan Hospital for maternal care is actively done.
Sick children are referred by all government health workers and Karuna project workers to
Duncan Hospital. However, the cost of care is an important deciding factor for most families.
The Karuna project team is skilled and highly motivated. The commitment and involvement
of community motivators is inspiring. The grassroots workers are well accepted and have a
good rapport with the different action groups being organised to build capacity of the
15
communities. Only one project officer is employed full-time in the project and needs to
supervise a wide geographic area and 2 levels of workers. The skills and involvement of
male and female community organisers is different and RCH nurses contribute to this level
of supervision.
Many community action groups are organised for building capacity for better health. There
are different levels of success, with different groups, with the smost active and promising
group being the adolescent boys’ and girls’ groups. There is a possibility of social change
with this change in youth.
Documentation and reporting of activities are done at many levels, but mainly by grassroots
workers (motivators). There are many reports and the need for each needs a review.
All community health projects of Duncan Hospital have different strengths and experiences.
At present each one is working almost independently and sometimes parallel to others in the
field. There is room for sharing capacity and maximising benefit to the community.
Project implementation and possible modifications Skills and Capacity Building for project team
All full-time staff underwent training for updating and upgrading their skills for the needs of
the Karuna project. New staff had in-house training and orientation to the project. Motivators
were trained separately. The teams carried out needs assessment activities in their block to
gather baseline information. This included the baseline survey in approximately 24,000
households and documentation of felt needs using participatory methods. These processes
were useful in orienting staff to the community, their needs and difficulties, barriers to overall
development and challenges for the Karuna project. It also provided an opportunity for
developing data collection skills.
Recommendation: The project needs people with skills in community organization and participatory methods for
improving ownership by the community and health communication. Special training courses
for PO and community mobilizers (who will now be appointed as Community Coordinators)
will help better implementation of the activities.
Development of the baseline and revision in plan and budget A baseline study of over 23,000 households was carried out in all three blocks. The
objectives were to estimate infant, neonatal and maternal deaths in the population and to
study the causes of them. This confirmed the previous understanding of the needs for
changing maternal and child health status. It became clear that health services were not
accessed for preventative maternal care and curative child-care.
There are a few issues regarding the quality of data. 60% of respondents were male
respondents and all information was not collected for all households. Vital information such
16
as total population was not captured in the survey, and as a result some rates cannot be
calculated. Therefore we recommend that the survey results be used only for internal
circulation, planning and monitoring purposes and not for publication.
Modifications were made in the logframe, budget and Gantt chart in February 2015 and June
2015.
Recommendation: Programme data should show the changes in specific indicators so that repeated surveys
are not necessary. If an end line survey is done, it should only look for validating the data on
a sample and in addition study behaviour changes identified as key indicators in the modified
plan.
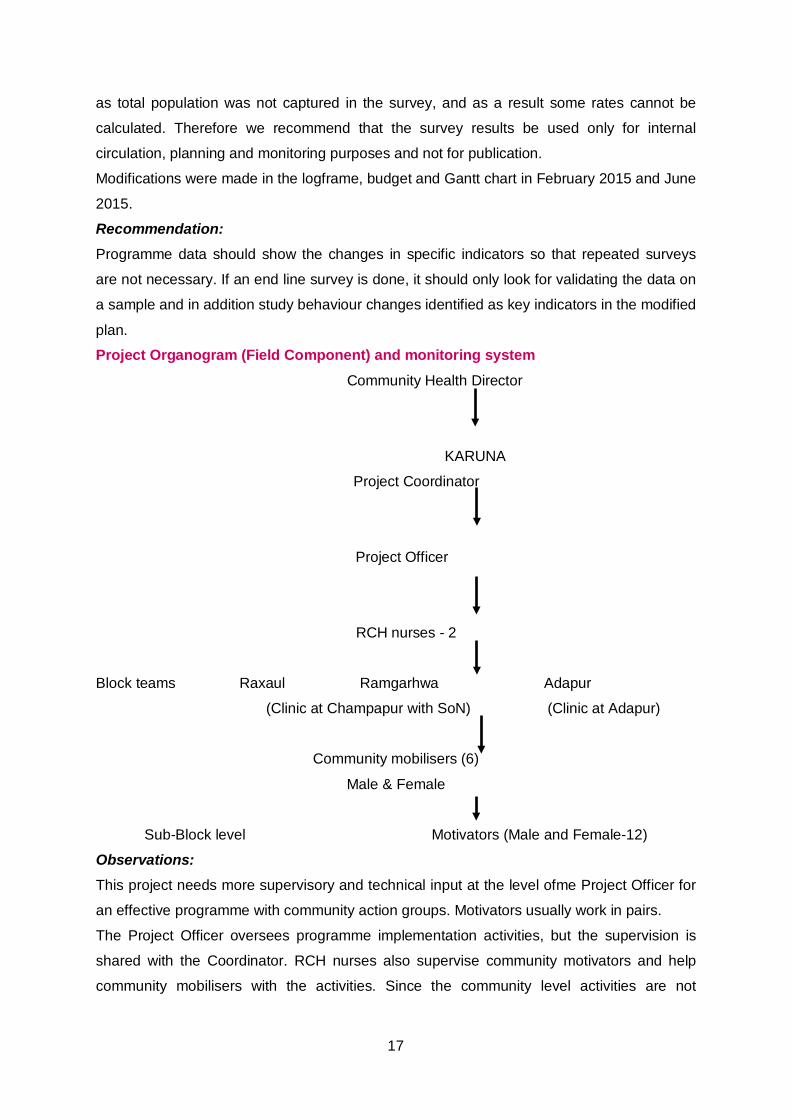
Project Organogram (Field Component) and monitoring system Community Health Director
KARUNA
Project Coordinator
Project Officer
RCH nurses - 2
Block teams Raxaul Ramgarhwa Adapur
(Clinic at Champapur with SoN) (Clinic at Adapur)
Community mobilisers (6)
Male & Female
Sub-Block level Motivators (Male and Female-12)
Observations: This project needs more supervisory and technical input at the level ofme Project Officer for
an effective programme with community action groups. Motivators usually work in pairs.
The Project Officer oversees programme implementation activities, but the supervision is
shared with the Coordinator. RCH nurses also supervise community motivators and help
community mobilisers with the activities. Since the community level activities are not
17
specifically divided between mobilisers and motivators, there is overlap and resulting
confusion in reporting.
Women motivators work with women groups while men work with boys and men.
Vital event reporting is done by the motivators, but there is no formal system of verification or
validation.
Recommendations: Clear responsibility for supervision must be given to different levels of staff. Verification of
vital data collected by the motivator is necessary and can be done by RCH nurses, while
community activity reports must be authenticated by the community organisers. Cause of
death is not collected using verbal autopsy methods, which should be done to monitor
changes in child deaths.
Collaboration with other NGOs Being one of the least developed districts, East Champaran has attracted a large number of
NGOs and international organisations, the leading one being CARE India, which is involved
in skills training to improve the quality of care in health centres and hospitals. There are
many others, including the WHO, Path Finder and UNCEF, who are involved in different
aspects of the NRHM programme. All representatives attend review meetings at the PHC
and visit the field for either monitoring or training activities. There is a difference in level of
skills and commitment of each of the staff at the district level, but each one has a voice at
higher levels in the hierarchy of the heath system that Duncan Hospital lacks.
Recommendation: The Karuna project should take the initiative to bring all of them together and form a network
for exchange of ideas, reduce duplication and work to complement the efforts of each other.
There is a need for advocacy at higher levels for a change in the functioning of the PHC
system, and a need for a better image and removal of corruption. This network can advocate
collectively at all levels, to encourage accountability and quality improvement, which is in any
case everyone’s agenda.
Special efforts need to be made to collaborate with CARE India for skills training of
healthcare workers and for advocacy to address corruption at all levels of healthcare. Since
CARE India is a trusted long-term partner with the Government of Bihar, it carries good
leverage with government organisations.
Project objectives and assumptions The broad objectives of the Karuna project are:
1. To provide good quality maternal and infant care in 3 blocks of East Champaran District
18
a) To network with government stakeholders to facilitate implementation of
government guidelines for antenatal, delivery, postnatal and infant care services in
the PHCs and HSCs in 3 blocks.
b) Capacity-building of government and private healthcare providers in maternal and
child healthcare.
c) Strengthening mother and child healthcare services in Duncan Hospital and the
primary health care services in Duncan Rural Health Centres at Champapur and
Adapur and mobile clinics.
2. To empower communities to adopt recommended behaviours to improve the survival of
mothers and children through awareness-generation and advocacy.
The objectives are in line with the mission and vision of EHA and EMMS International and
there is commitment from Duncan Hospital to consolidate the community engagement efforts
to bring cumulative benefit from all project inputs.
One of the important assumptions was that the Karuna project would be able to engage with
NRHM efforts in improving the quantum and quality of health services. This has been
difficult, since more than one non-governmental organisation is involved in training in various
aspects and components of the NRHM. CARE India is the main partner with NRHM Bihar
for skills development of nurses and ANMs for improvement in quality of care. However, their
effort is to work from the higher level to the lower level of service delivery, resulting in poorer
quality of primary care services while tertiary care services are being upgraded. While there
is wisdom in this approach, a very low quality of services persisting at primary level with non-
existent secondary level care (no functioning CHC) does not develop confidence in people
who need to use the government health system. Project staff have anecdotal information of
language barriers with trainers and more theoretical training than skill building for subcentre
ANMs by CARE. Duncan Hospital is a site for skills training and could offer more
involvement with CARE training. Training of ASHAs has been more possible but all areas of
need cannot be addressed.
The project plan also had a component for monitoring quality at health centres according to
Indian Public Health Standards (IPHS). Without an official agreement or MOU, this role
cannot be played by Duncan Hospital.
Monitoring of changes expected through the Karuna project interventions would not have
been possible if the whole block was covered uniformly with activities. The modified plan
restricts the implementation area to 10 villages in each block, and therefore changes in
these villages collectively can be compared to others. Since the some training input for
health and nutrition workers (ANM, ASHA and AWW) is at the block level with PHC, a
certain level of change is expected in the non-target villages also. This will be reflected in the
change at block and district level indicators.
19
Implementation, achievements and performance of overall objectives MCH Services
I. Training of ICDS and health workers Formal training sessions with health staff and community level nutrition and health workers
are limited. There is difficulty in gaining permission to train ANMs and PHC nurses. ASHAs
are the more willing and enthusiastic group as a whole, but some are uninterested, chosen
arbitrarily and therefore ineffective. AWWs are well trained and knowledgeable. They need
encouragement and acknowledgement of their work to go beyond their call of duty and
collaborate with other functionaries. They are happy to work with the Karuna project, as they
feel appreciated and supported when specific needs for health services arise.
RCH nurses use any opportunity to train the ANMs on care of antenatal women, but this is
usually limited to VHND.
Recommendation: The project could make separate plans for formal and informal training. Informal training in
the field during VHND, visits to AWW and SC could concentrate on skills while formal
training when possible could address programme improvement, information quality, quality
assurance and special skills training. Karuna project leaders need to identify specific
monitoring needs for the government-managed services to which they can contribute and
make a formal agreement for Duncan Hospital to provide services.
Each block team could develop its own list of training gaps to address and follow it, since
each one faces different challenge and barriers.
Depending on the skills and knowledge of mobilizers and motivators, they should start as
training assistants and later take on training of topics related to community organisation,
participation and communication.
II. Collaboration among grassroots functionaries of nutrition and health, and linkage with project
ASHAs, ANM and ICDS workers are brought together at the Health Sub Centre (HSC) level
for training and planning for VHND. This has forced two hitherto independently functioning
programmes to come together. Anganwadi workers are fairly knowledgeable, know their
work and responsibilities and document on a regular basis. However, they may not cover the
whole population. They are now starting to share information but still are not cooperating
well, since ANMs are at a higher level, while ASHA and AWW are at a lower level and have
better knowledge of the community. Community mobilisers and motivators are working on
the ground with these groups, but their involvement is tentative at present. Motivators can be
20
part of village teams, actively working to supplement and complement ASHAs’ and AWWs’
work.
Fortnightly meetings of this group is used as an opportunity by the Karuna project to interact
and add inputs to improve knowledge, assess availability of services and plan for bridging
the gap, such as training ASHA to check blood pressure, and organizing VHND activities
with them.
Recommendation: Government health workers and Karuna project workers are not fully utilising the strengths of
the ICDS programme. Karuna could work to strengthen this linkage and bring them closer to
the community through interaction with Saasbahu and adolescent girls’ groups. Motivators
and mobilisers need to work closely with AWW and plan complementary activities with
beneficiary groups.
Motivators and mobiliser need to work with AWW to reach mothers of small children.
III. Contribution during VHND At present the role of community motivator, mobiliser and RCH nurse during VHND is not
well defined. Raxaul block had additional input through another Duncan Hospital project,
Sexual and Reproductive Health Rights (SRHR), in which intensive input on antenatal
examination, investigations, IFA supply and counselling was given. The ANMs are able to
organise the activities better and able to provide all services with the help of ASHAs and
AWWs. RCH nurses occasionally help in examination of antenatal women, but are in a
dilemma, thinking they might replace ANM rather than build their capacity.
Recommendation: VHND involvement/contribution needs to be planned and accepted by ANM, MOIC.
Mobilisers and motivators must use the opportunity for interpersonal education. RCH nurses
can help in examinations to start with and transfer responsibility over time when the backlog
of immunisations is over.
IV. Referral linkage
Although a formal referral linkage with the government health system may not be possible,
the informal system is active. It was observed that this open referral to Duncan Hospital is
misused by PHC staff. The other barrier to early referral to Duncan hospital for acute care or
severe illness is the cost of care. For a large section of society, the cost of care at Duncan
Hospital is prohibitively high, causing either delay in seeking care or choosing a less
appropriate mode of treatment.
Recommendation: Agreement on a protocol-based referral and encouraging protocol-based management at
PHC will improve the value of referral, reduce delays and reduce inappropriate referrals to
higher centres and Duncan Hospital.
21
The referral system followed by all community health projects of Duncan Hospital should be
uniform and an assessment of patients’ paying capacity with recommendations for
concession should be part of the referral. The hospital needs to develop a feasible plan for
this in consultation with Community Health and Finance departments. There should be a
clear communication to potential beneficiaries for a hassle-free referral. Since the project is
contributing to human resources and equipment at the hospital, a specific indicator showing
improvement in usage of Duncan Hospital’s maternal and child health services is needed to
justify the investment.
Institutional (Duncan Hospital) capacity building
The project aims to support postgraduate training for one doctor, who will return to work in
the community health projects. A suitable candidate has been identified for this. Additional
equipment for obstetrics and paediatric care have also been bought with project funding.
This has enabled the hospital to provide higher quality services for a higher number of
patients coming to Duncan Hospital. An estimated 70% of the patients coming for obstetric
care are from the project blocks. Therefore improving quality of services at the hospital will
directly benefit the community.
Comment: The role of doctors receiving support for training on their return needs to be discussed. While
it is important that they contribute to services in the project area, they will not be competent
in programme-based interventions for maternal or child care. They will require additional
training if they are to help in project management. Therefore, it is recommended that they
be used by the hospital primarily for speciality care and not be given project responsibility. If
any one of them is interested and has a leaning towards community approaches then s/he
may be encouraged to take more responsibilities.
Peripheral Health Centres at Adapur and Champapur Champapur centre building is owned by Duncan Hospital and Adapur health centre is a
rented building. Both have been used as peripheral outreach centres for clinics and use by
other community health projects. The facilities in the centres are adequate for running a
fully-fledged 24-hour dispensary and community centre. Alternatively, they can be used as a
place for community training. At present, both the buildings are underutilized. At present,
Adapur centre is used for conducting a general antenatal clinic and the clientele is from the
surrounding villages, majority Muslim and not necessarily from the project villages. It does
not provide the full range of antenatal services as per NRHM guidelines and requires
patients to buy medicines at hospital cost. This form of service can only be considered an
extension of Duncan Hospital services, not really fulfilling the need for bridging the service
gap in the project population. A service at the community level must be following norms set
by NRHM or higher, and should be available for a minimum or subsidised cost.
22
The location of Champapur centre has more possibilities for being relevant and bridging the
service gap in healthcare of women and children in addition to providing care for other
illnesses, especially of the elderly. This centre was a vibrant place when run around the
clock with availability of trained health professionals and a fair level of care for most
illnesses. Over time, this has changed and it now functions only as a stop for nursing
students going for field practice. Doctor- or nurse-managed clinics in the centre are therefore
not regular, and do not contribute significantly to healthcare of local people.
Recommendation:
Adapur centre is very close to the 30-bed block PHC which has a 24-hour delivery facility.
Therefore, if this centre is maintained, it should identify useful service activity for itself, such
as a high risk antenatal or newborn clinic, or a special clinic for diabetes, hypertension and
similar illnesses which are not yet a priority of the government health system.
Champapur clinic is located in Ramgarhwa block, which is the most backward among the
three project blocks. It could function truly as an extension of Duncan Hospital, with
comprehensive services for specific illnesses. The School of Nursing and the hospital could
develop a relevant model of clinical services that could be provided through this centre as
local people find it difficult to go to PHC or the nearest town for healthcare. This would mean
a specific budgetary allocation and personnel planning by Duncan Hospital. Of the two
centres, Champapur could still play a positive role for improving access to healthcare, but
this will require a policy decision by Duncan Hospital.
Both buildings can be utilized as peripheral centres for all community health project
activities. While new projects are planned by Duncan Community Health Department,
utilization of these centres should be kept in mind. As Ramgarhwa block is relatively
underdeveloped, future projects can be concentrated in this area.
Community empowerment for behaviour change The Karuna project has identified multiple community groups for focusing on behavior
change communication in 26 villages, namely Siswa, Kowadhangar, Parsauna Tapsi, Gadh
Bahuari, Nayakatola, Lakshmipur Lakshmanwa in Raxaul block, Bakhri, Kurmeniya, Koraiya,
Latihanwa, Dhabdhabwa, Bishunpurwa, Pokhariya, Manghurhara, Chikani, Chiljhapti in
Adapur block
Tilkahoni, Belahiya, Kalikapur, Gulariya, Jaitapur, Sakrar, Mushahri, Bahuari, Mangalpur and
Nandlali in Ramgarhwa block. Community organization also takes place through
organization of these smaller groups. The most active and functional of them all are the
adolescent boys’ and girls’ groups and older women’s groups (Saas). The team has found it
difficult to organize new fathers’ groups and develop an active mothers’ group. The reason
for this is migration of young men for long periods of time and younger women (daughters-in-
law) having no voice in the family and community. It is a challenge to form and maintain
23
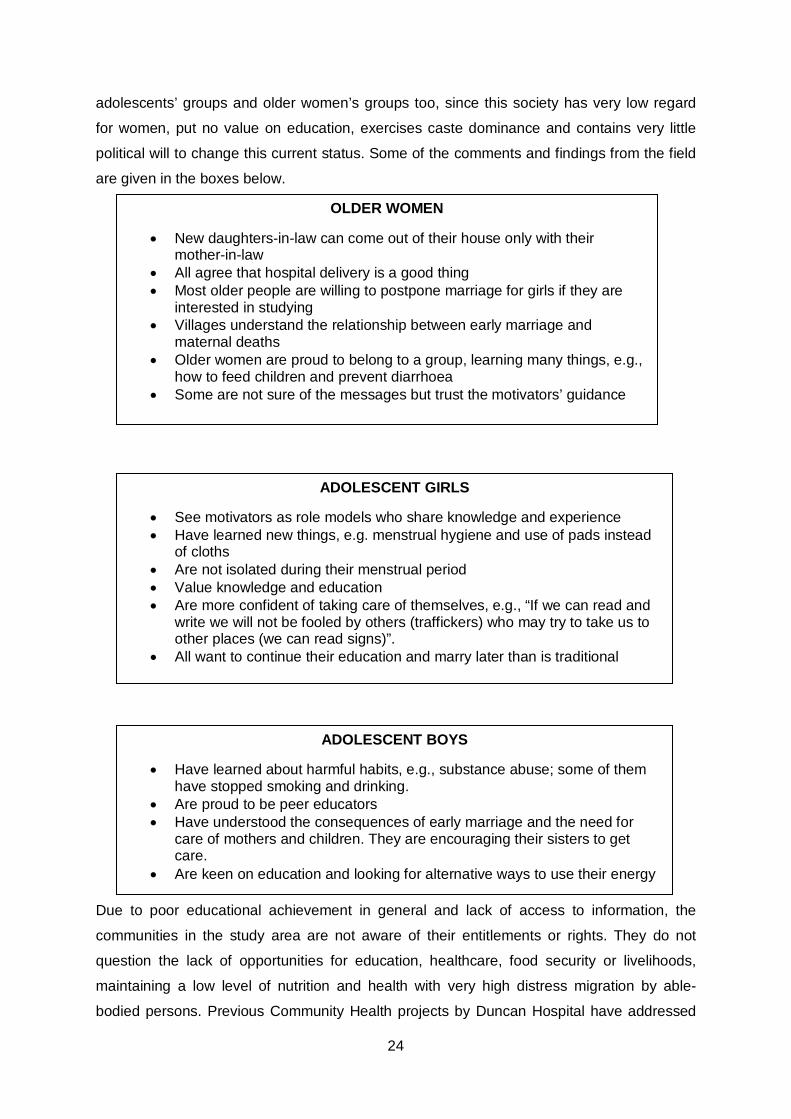
adolescents’ groups and older women’s groups too, since this society has very low regard
for women, put no value on education, exercises caste dominance and contains very little
political will to change this current status. Some of the comments and findings from the field
are given in the boxes below.
Due to poor educational achievement in general and lack of access to information, the
communities in the study area are not aware of their entitlements or rights. They do not
question the lack of opportunities for education, healthcare, food security or livelihoods,
maintaining a low level of nutrition and health with very high distress migration by able-
bodied persons. Previous Community Health projects by Duncan Hospital have addressed
OLDER WOMEN
• New daughters-in-law can come out of their house only with their mother-in-law
• All agree that hospital delivery is a good thing • Most older people are willing to postpone marriage for girls if they are
interested in studying • Villages understand the relationship between early marriage and
maternal deaths • Older women are proud to belong to a group, learning many things, e.g.,
how to feed children and prevent diarrhoea • Some are not sure of the messages but trust the motivators’ guidance
ADOLESCENT GIRLS
• See motivators as role models who share knowledge and experience • Have learned new things, e.g. menstrual hygiene and use of pads instead
of cloths • Are not isolated during their menstrual period • Value knowledge and education • Are more confident of taking care of themselves, e.g., “If we can read and
write we will not be fooled by others (traffickers) who may try to take us to other places (we can read signs)”.
• All want to continue their education and marry later than is traditional
ADOLESCENT BOYS
• Have learned about harmful habits, e.g., substance abuse; some of them have stopped smoking and drinking.
• Are proud to be peer educators • Have understood the consequences of early marriage and the need for
care of mothers and children. They are encouraging their sisters to get care.
• Are keen on education and looking for alternative ways to use their energy
24
some of these issues, but the input has been scattered in many blocks and has reached only
a few villages and beneficiaries. Often there is a lack of continuity in the focus of one project
to the next in the same geographical area. This has resulted in poor sustainability of
changes achieved by individual projects and lack of measurable social change.
Adolescent boys and girls groups have benefitted most from the input of the project. Peer
educators have been identified and trained. There is interest and enthusiasm to embrace the
knowledge imparted through the training sessions. Members of the groups are becoming
vocal and have developed positive self-esteem, and some of them have taken action at the
community and family level to initiate change. Major change is seen in stopping underage
marriages and decisions to continue schooling. The examples of a few bold individuals, both
boys and girls, is an encouragement to others. Older members of the community are
accepting and support such decisions, which is a big change in this society.
Boys and girls are actively seeking ways to build their lives with positive behaviours moving
away from harmful or useless behaviours and practices.
Older women are influential and probably gatekeepers for any positive health-seeking
behaviors for the care of women and children. They also make decisions about their
adolescent sons’ and daughters’ education and marriage. They have a louder voice than
their sons, who may be absent from home or decision-making most of the time. The younger
women do not have a voice in a combined group. It was very difficult to get them to talk in
the large group. Even individually they were not able to repeat any message learned through
activities of the project or ICDS programme. They depend very much on ASHA for any
health service. Motivators in the community are an additional source of information on health
services for them. It is possible that the women motivators have developed a rapport with
this group of women but the evaluators did not have the opportunity to verify this.
Older men, though very influential in community level decision-making, seem to agree with
the older women’s decision to change health-seeking practices. They also are benevolent
towards adolescent boys’ and girls’ decisions on schooling and marriage. So far the project
staff have not faced any resistance from traditional leadership or the older age group in
educating the younger generation on their rights and possibility of different futures.
The organization of the task force has not been easy and in light of the modification of the
project plan, with only 10 target villages per block, the role of the task force is in question.
Ideally, it would help the project implementers in planning and monitoring project activities.
Motivators met by the evaluators were very well accepted in the community and were greatly
appreciated for their contribution, especially to the young people. Some boys and girls
considered them as their role models.
25
Recommendations: The younger generation is ready and eager for change. It would be wise to invest in this
group and give lower priority to young men’s group and the Task Force. Activities to
encourage wider participation, building character and encouraging a competitive spirit could
be brought, in the form of Melas or inter-village competitions, for example, for young people
to showcase their talents. This would also help in giving positive direction to their energy.
Non-functional groups should be either removed from activities or made low priority.
Develop a community-initiated collective action There should be an active move to engage villagers of all ages in discussion to address their
rights, entitlement and access to health and development services. This should be initiated
by the adolescent boys’ and girls’ groups, making it a community effort for change. Ekjut
NGO’s strategy in Jharkhand has been a successful experiment in markedly bringing down
maternal and child deaths, due to community decisions and ownership of the action for
accessing health services.
Social change needs change in the mindset of the powerful, especially when gender issues
are to be addressed. This will need collective decision and action by the whole community.
The process can be tried for MCH care, and if successful can become a vehicle for social
change.
Behavioural change needs an enabling environment, which needs community support. So,
older men who are making most decisions need to be brought into the discussion when older
women are comfortable with this.
Health Communication for behaviour change
The Health Communication strategy is not well defined. Multiple methods and media have
been sporadically used for different groups and for mass health education. As community
action groups are the most receptive, the whole strategy for behaviour change
communication can be focused on them. The project team should study appropriate
messages and media needs and plan specific strategies for this input. Specific indicators for
this component need to be in place before input is planned. Sporadic mass health education
programmes are strongly discouraged, and instead young people in the community should
be used as a vehicle to reach the wider community. They can be formed into health
education groups, taking messages to schools, peers, family and the village.
Documentation and health information system
Currently, a large amount of information is captured in various reports by motivators and
organizers. Apart from vital events, most of the other documentation is only related to
activities such as meetings and visits.
Two sets of indicators need to be developed:
26
1. Informing the change in health status, e.g. births, perinatal deaths, causes of
deaths, outcome of childhood illnesses and maternal deaths.
2. Assessing progress towards achievement of outcomes listed in 1, e.g. sick children
identified and referred by ASHA, motivators and even community members,
community initiatives in making ICDS centres function, near-miss cases
referred and managed in Duncan Hospital, and number of ANMs providing complete
antenatal care package.
We suggest that the project team revisits all process and outcome indicators and retains
only those that will directly lead to outcome indicators even beyond the project period. After
identifying this, the process should be to work backwards and identify the information that
needs to be collected. Some of these will need to be done on a regular basis prospectively
(e.g., births, antenatal care, perinatal deaths and birth weight), while some other indicators
will need only periodic collection of specific information. A set of suggested indicators is
given in a separate document.
SWOT Analysis and brainstorming by project staff The group identified a happy, strong and safe community as a healthy community where
livelihoods are ensured. This project is contributing towards this broad goal. All three block
teams worked on challenges and opportunities for achieving this goal.
Common barriers identified were
• Poor quality of ANMs’ work, non-functional ASHA, dominance and interference
of husbands (AWW, ANM and ASHA).
• Restrictions on girls
• Poor attitude towards girls’ education
• Difficulty of changing attitudes towards care of women
• Too many NGOs
• Entitlements which do not reach the people
• Bribe-taking in PHCs (Specific to Ramgarhwa)
• Inactive and uninterested motivators
• Poor access to communities, e.g. bad roads
• Elections and the monsoon interfere with activities, especially with monitoring
• Unavailability of adequate transport
• Poorly functioning health services
• Lack of equipment in PHCs
Facilitating aspects were:
• Acceptance and support of community, PRI and MOIC
• Ability to work with ASHA, AWW and ANM
27
• Support of CARE and UNICEF
• Change in adolescent girls, now taking decisions about their own lives and
dreaming
• Willingness of parents to change
• Mothers-in-law thinking about their daughters-in-law
• Increasing awareness of some task force members
• Different NGOs working on different issues and so multiple inputs.
28
Compliance with EMMS International Operational Framework Coherence with the vision and mission of EHA EHA has identified specific areas for community engagement. MCH remains one of the
important areas for intervention. Duncan Hospital's community health projects are
addressing some of the key areas of interest, and recent projects have moved to issues
which are not traditionally considered "health", for example human trafficking.
Compliance with overall Operational Framework EMMS International articulates its values and principles very clearly in its policy document
called its Operational Framework. These are translated in the Karuna project through
engaging with the vulnerable (women), government health providers, empowering women
and adolescents who otherwise have no voice, and making quality health care and access to
it a rights issue. EMMS International puts a major emphasis on gender, and sees all its
Maternal and Child Health (MCH) work as concerning primarily gender.
Sustainability of the initiative Sustainability of project activities depends on developing a long-term Duncan-Community
intersection, where an open communication channel is created for communities to develop
their skills in exercising their rights to achieve good health. Duncan Hospital may bring in
different ideas in the form of community projects, but these should all address the basic
need to develop social capital for long-term and sustainable development.
Focus on adolescents is a strategy with a long-term effect on social change, much needed in
this society. Addressing issues of the disabled and mental health issues are also efforts
towards social justice. All community projects of Duncan Hospital should develop a common
agenda for social change and incorporate these in project plans.
29
Learning and Conclusions Duncan Hospital has a long history of engaging with local communities to address needs
arising out of interaction with them. This has lead to a large number of community projects
addressing a range of issues, including inequity, injustice and right to life with dignity in a
small way. The team has gained valuable experience of engaging with the community and
building trust. They are respected and people have faith in programmes initiated by Duncan
Hospital. The Karuna project has gone a step further to address deep-rooted social
behaviours to bring change in ordinary people’s lives and health. This is a difficult task since
the outcome of activities towards this will only be visible in the long term. However, it is a
start and the experience of the Karuna project in changing mindsets and behavior should be
used for all future community initiatives by Duncan Hospital.
• The project is targeting a small number of villages in each block for intensive inputs.
This should be used for learning and fine-tuning strategies. If possible, this lesson
should be extended to other villages through the community action groups.
• East Champaran District will always remain in the peripheries of political interests. It
is in a difficult area, being on the Nepal border. People here will always need non-
governmental organisations to advocate for them, for the foreseeable future.
Therefore, Duncan Hospital’s intervention in the district will always be needed.
• Collaboration with NGOs with different value bases will always be a challenge for an
institution such as Duncan Hospital with a strong Christian ethos. The challenge is to
find the meeting point with such agencies for the benefit of the common man and
woman.
• People are waiting for a change. Developing long-term partnerships with
communities will sustain even a small input by a short-term project. Therefore, short-
term projects should invest in community organisation, building social capital and
trust-based partnerships with local communities.
• The face of a project is identified by the staff and workers. Having a large number of
local workers will increase credibility with local communities and indirectly invest in
capacity building.
30
Recommendations Due to the delay in effective implementation of NRHM programmes in the project district, the
contribution of the Karuna project and Duncan Hospital is needed to bridge the gap.
However, the needs are in the areas of generating demand through community mobilisation,
improving quality of services through training of government functionaries, monitoring
services and bridging the gap in services. This will need the following:
• Develop the current status of good rapport with government health system into a
trust relationship and work with the PHCs for image-building for better utilisation of
public health services. (Improve Quality)
• Work towards forming a collaborative network with other NGOs and the government
health system in the district and leverage good will for Duncan Hospital for better
participation in skills training of government health workers. (Improve Quality)
• Link all community health projects of Duncan Hospital together and with the
communities, to complement and supplement the health services. (Improve access
to Quality Care and better Demand Generation)
• Build on the success in reaching adolescents and youth and invest in this group,
even though the outcomes of this intervention will be seen much later than the
project period. Drop the non-functional, or difficult to reach community groups such
as the new fathers’ group and Task Force. However, joint community action is
needed for improvement of maternal and child care where villagers of all strata and
ages need to be involved. Bring the interested groups of adolescents, older and
vocal women and men, and those who make decisions in the community together
for a joint effort for lasting change in health-seeking behaviour.
• Match the demand for quality healthcare with an efficient and trusted referral system
to public health system (PHCs) and Duncan Hospital
• Review the organisational structure to increase the number of animators
(community motivators), or reorganise their work responsibilities since they are key
to the success of the main objectives. Institute higher level supervision (level of
Project Officer), since there are 3 blocks with different needs. Improve the skills and
supervision of community level workers and redefine RCH nurses’ role to give more
responsibilities based on their knowledge and experience.
• Review the project document, plans and strategies to identify process and outcome
indicators relevant for tracking the efficiency of the inputs and change. Simplify and
restrict documentation of events, programmes and reports from the field to those
required for indicators. Link community data to hospital data.
31

Make a policy decision on involving clinical staff in community projects and improve
involvement of the School of Nursing. Institute a two-way integration of community health
activities and hospital-based work for long-term ownership of community engagement
initiatives by Duncan Hospital staff. Referral and feedback systems, monthly review of
activities by a common group, hospital data feeding into programmes and vice versa will
promote this.
32
Annexes Annex 1: Terms of Reference Terms of Reference for Mid-Term Evaluation of Duncan Hospital’s Karuna (Compassion) – MCH in East Champaran, June 2014-March 2017
1. Introduction/background EMMS International is a charity based in Edinburgh, Scotland, which works to improve
healthcare, through partners in north India, Malawi and Nepal. Its main partner in India is
Emmanuel Hospital Association (EHA), and its largest initiatives with EHA concern Maternal
and Child Health (MCH). This mid-term evaluation is of the above-named project, run from
Duncan Hospital in Raxaul, Bihar.
This project, with direct costs of £343,343, is intended to improve maternal and child health
in three blocks around Duncan Hospital. It is funded from EMMS International’s fundraising.
The purpose of the mid-term evaluation is to find out how well the project is meeting its
objectives, make recommendations to improve it and provide a report to be published by
EMMS International.
The report will be the copyright of EMMS International. EMMS International and Duncan
Hospital will circulate the report to all their staff and key stakeholders of the project, and will
aim to present key findings in conferences and in academic research papers.
2. Scope of mid-term evaluation to be carried out by the consultant 1. Review attached programme documentation. (1 day)
2. In Duncan Hospital, interview the Project Manager (Community Health
Consultant, Dr. Sharon Cynthia), Director of Community Health and Development
at Duncan Hospital (Dr. Vandana Kanth), and any other relevant staff
recommended by Dr. Cynthia and Dr. Kanth, Conduct a Focus Group Discussion
with the whole Karuna team in Duncan Hospital. (1/2 day)
3. View all statistics and relevant documentation in the Karuna office. (1/2 day)
4. Visit at least one village in each of the three blocks in the project area, villages to
be chosen by the evaluator. Include in these visits Duncan Hospital’s Adapur
Clinic. During these site visits, in each block, conduct the following:
a. view all premises relevant to the Project and associated services,
b. interview and hold discussions with staff working on the project,
c. interview government healthcare staff and others involved in the project,
33
d. conduct focus group discussions with each of the groups involved,
including pregnant women/girls, lactating women/girls, fathers, mothers-
in-law, adolescent girls and boys. (3 days)
5. Interview relevant senior government healthcare staff in Raxaul. (1/2 day)
6. Consolidate and analyse data, write draft evaluation report using the format
attached, send to EMMS International and Duncan Hospital for review, and
incorporate feedback into final evaluation report (2.5 days total)
7. Conduct all the above in relation to the attached project documents.
8. Travel from home to Duncan Hospital and back home. (2 days)
Total: 10 working days, to be done within 2 months from start to end.
3. Main purpose and questions to be answered in the report - To what extent is the project meeting its objectives?
- Is the project working to address the issues raised in the baseline survey?
- What have staff learned through working on this project?
- Will systems instituted by the project continue after it, so that health and healthcare
continue to improve?
- Is there scope to replicate the project in other locations covered by Duncan Hospital?
- Could Duncan Hospital usefully institute more advocacy, to improve the project’s
outcomes?
- Has the project yielded data which could be used in research to be presented or
published?
- What changes could help Karuna achieve its objectives better?
4. Fees, expenses and budget A consultant based in India is sought, to minimise costs of travel.
Fees: £100/day = £1,000, to be paid after all work is completed, upon submission of an
invoice. EMMS International will reimburse reasonable public transport, accommodation and
subsistence costs, upon submission of receipts.
Budget = 10 days @ £100 = £1,000 + reasonable expenses. If the evaluation is conducted by an institution, the expenses policy of this institution will be reimbursed. If the consultant is accompanied by a more junior person for learning purposes, that person’s expenses may be reimbursed. 5. Timing
November/December 2015, with report to be finalised within 2 months of start date.
34
6. Logistics
EHA will arrange the consultant’s travel to Duncan Hospital and back home. Duncan
Hospital will provide accommodation and meals for the consultant, and will organise all local
travel needed.
7. Confidentiality and publication The report is for publication, and therefore will comply with EMMS International’s Child and
Vulnerable Adult Protection Policy, in terms of which people to name in the report, and
gaining permission from such people.
EMMS International and Duncan Hospital will distribute the mid-term evaluation report
internally, to relevant stakeholders in India and to potential donors to healthcare in India.
EMMS International will put the mid-term evaluation report on its website and on IATI
(International Aid Transparency Initiative). EMMS International or Duncan Hospital may
present the report at conferences, and will inform the other parties before doing so. Any
party may reference the report, and in so doing will always refer to EMMS International, EHA
and Duncan Hospital as co-implementers.
EMMS International will use the mid-term evaluation report as a learning document amongst
its staff. Duncan Hospital will use the report to debrief all the project’s stakeholders
(including EHA staff, volunteers, government staff, community groups, senior and junior
government health staff) about challenges and successes.
8. Profile of the Consultant An independent consultant with minimal prior experience of Duncan Hospital and the Karuna
staff, who has conducted at least 5 external evaluations, has at least 5 years of experience
of working in community medicine and maternal and child health in India, and has a
demonstrable grounding in and academic knowledge of the issues surrounding gender and
maternal and child health in India.
9. Outputs
• A draft mid-term evaluation report, using the format attached, to be submitted
to EMMS International and Duncan Hospital within a month after the
evaluation visit.
• A final draft of the mid-term evaluation report, still using the format attached,
to be submitted to EMMS International and Duncan Hospital within 2 weeks
after receiving feedback from EMMS International and Duncan Hospital on
the draft evaluation report.
10. Attachments
• Logframe (version revised June 2015), budget (version revised February 2015),
Gantt chart (version revised February 2015), Additional Notes (version revised
35
February 2015) and Project Agreement signed 25th March 2014 between EMMS
International and EHA.
• EMMS International Child and Vulnerable Adult Protection Policy
• EMMS International Operational Framework
• Project baseline survey report
• All quarterly narrative, financial and monitoring reports from Duncan Hospital to
EMMS International, as finalised by EMMS International for language and clarity.
11. Other documents, to be prepared or provided by Duncan Hospital before the evaluation As requested by the consultant.
12. Signatures Consultant Signature
Signed:
Name:
Date:
Position in Organisation:
EMMS International Signature
Signed:
Name: Catherine Ratcliff
Date: 25th October, 2015
Position in Organisation: Director of International Programmes
36
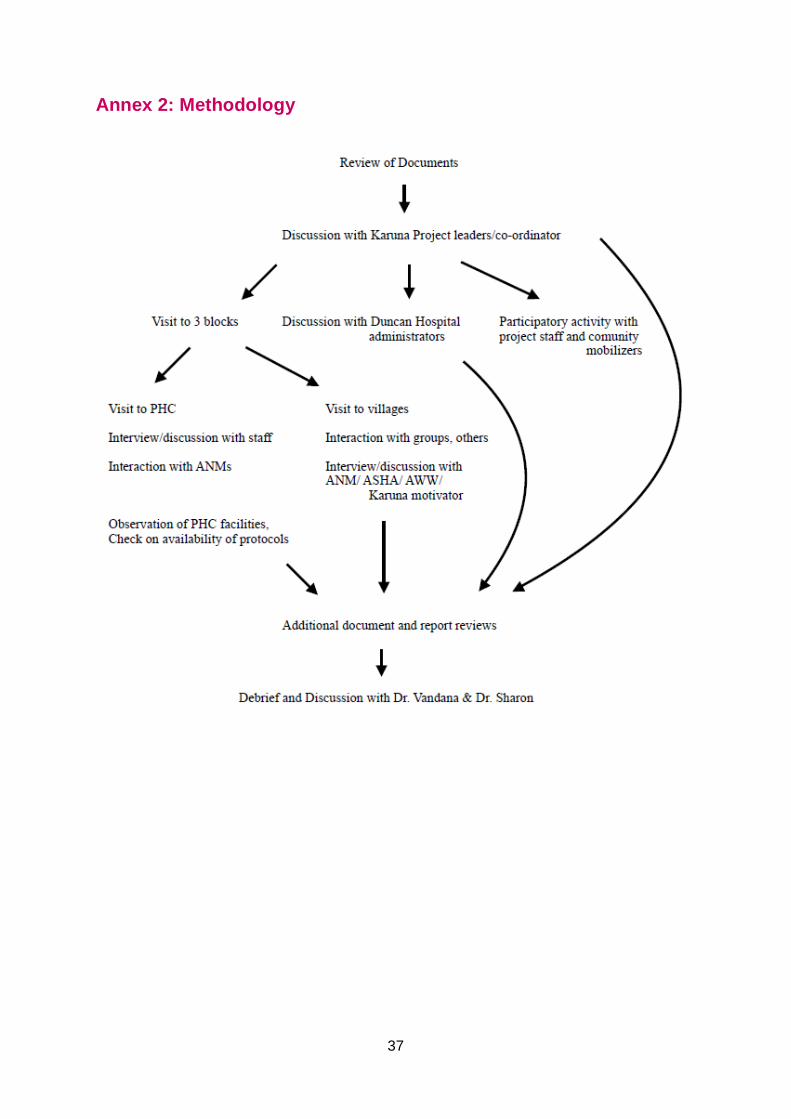
Annex 2: Methodology
37
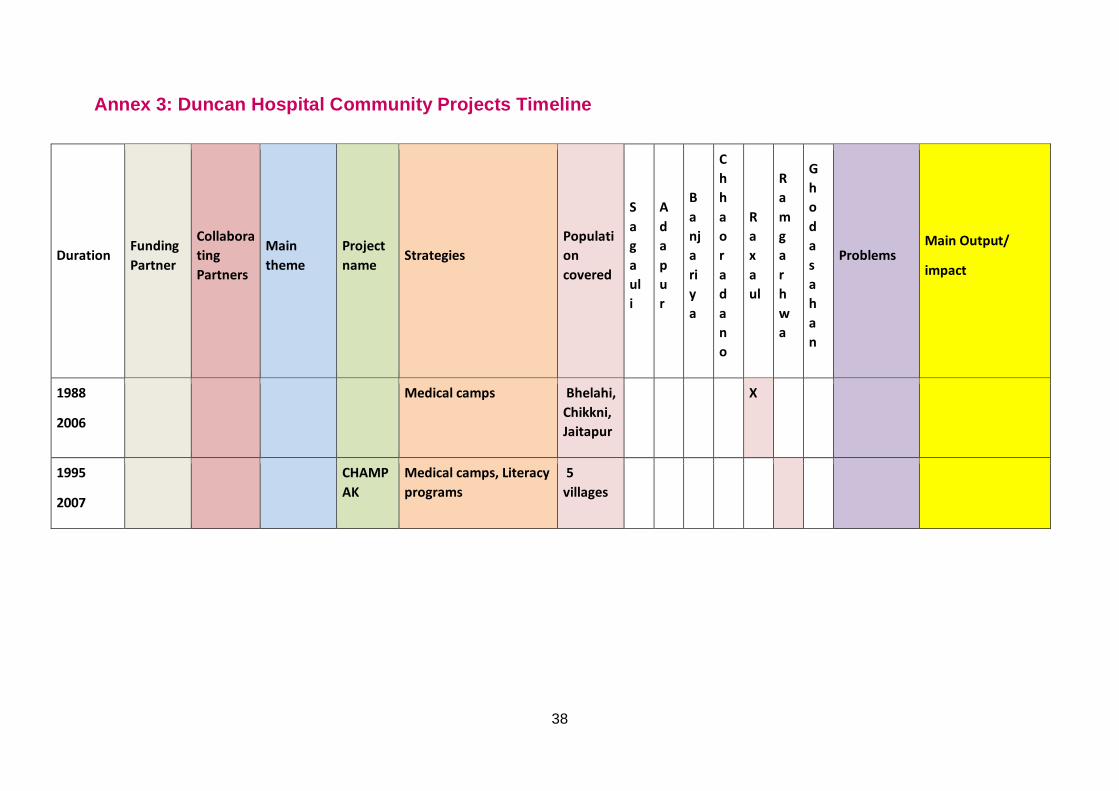
Annex 3: Duncan Hospital Community Projects Timeline
Duration Funding Partner
Collaborating Partners
Main theme
Project name
Strategies Population covered
Sagauli
Adapur
Banjariya
Chhaoradano
Raxaul
Ramgarhwa
Ghodasahan
Problems Main Output/
impact
1988
2006
Medical camps Bhelahi, Chikkni, Jaitapur
X
1995
2007
CHAMPAK
Medical camps, Literacy programs
5 villages
38
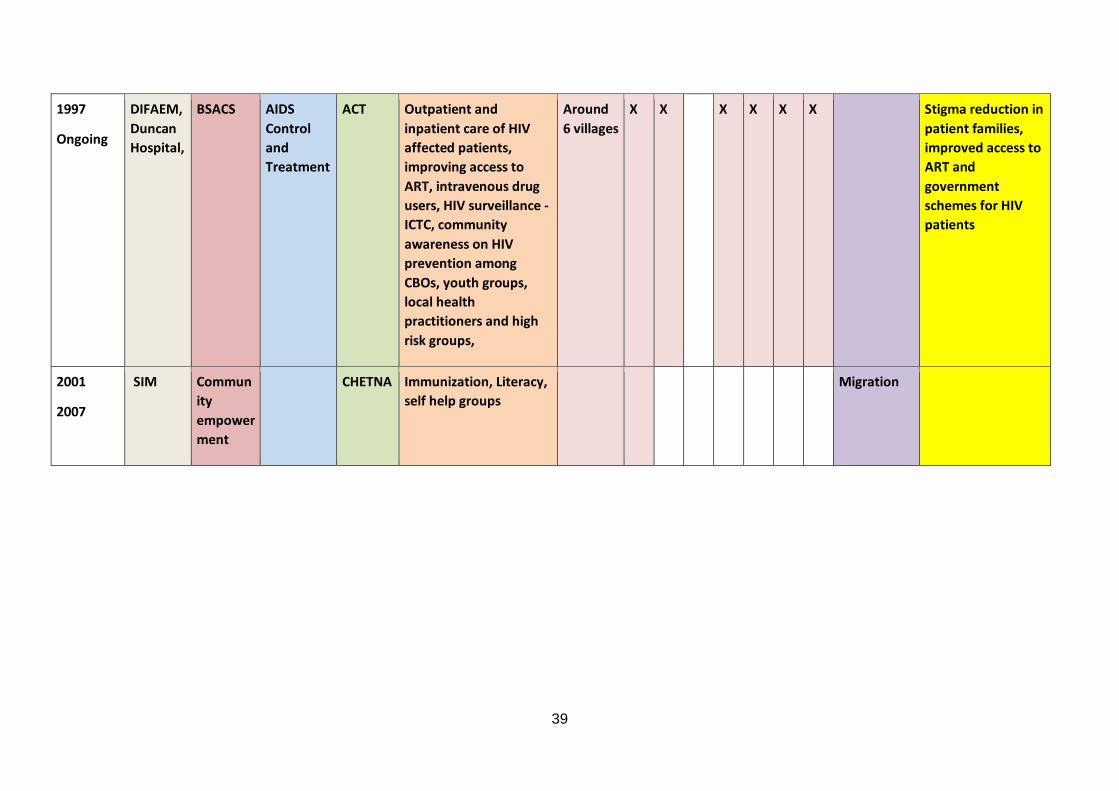
1997
Ongoing
DIFAEM, Duncan Hospital,
BSACS AIDS Control and Treatment
ACT Outpatient and inpatient care of HIV affected patients, improving access to ART, intravenous drug users, HIV surveillance - ICTC, community awareness on HIV prevention among CBOs, youth groups, local health practitioners and high risk groups,
Around 6 villages
X X X X X X Stigma reduction in patient families, improved access to ART and government schemes for HIV patients
2001
2007
SIM Community empowerment
CHETNA Immunization, Literacy, self help groups
Migration
39
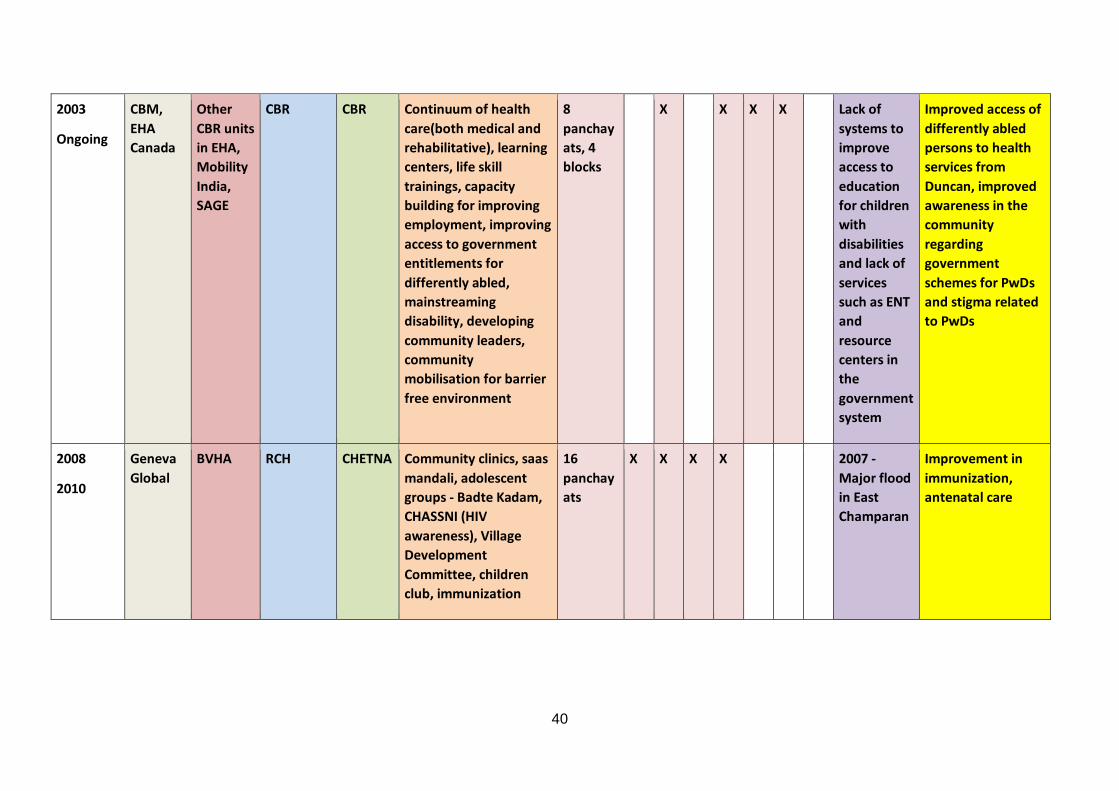
2003
Ongoing
CBM, EHA Canada
Other CBR units in EHA, Mobility India, SAGE
CBR CBR Continuum of health care(both medical and rehabilitative), learning centers, life skill trainings, capacity building for improving employment, improving access to government entitlements for differently abled, mainstreaming disability, developing community leaders, community mobilisation for barrier free environment
8 panchayats, 4 blocks
X X X X Lack of systems to improve access to education for children with disabilities and lack of services such as ENT and resource centers in the government system
Improved access of differently abled persons to health services from Duncan, improved awareness in the community regarding government schemes for PwDs and stigma related to PwDs
2008
2010
Geneva Global
BVHA RCH CHETNA Community clinics, saas mandali, adolescent groups - Badte Kadam, CHASSNI (HIV awareness), Village Development Committee, children club, immunization
16 panchayats
X X X X 2007 - Major flood in East Champaran
Improvement in immunization, antenatal care
40
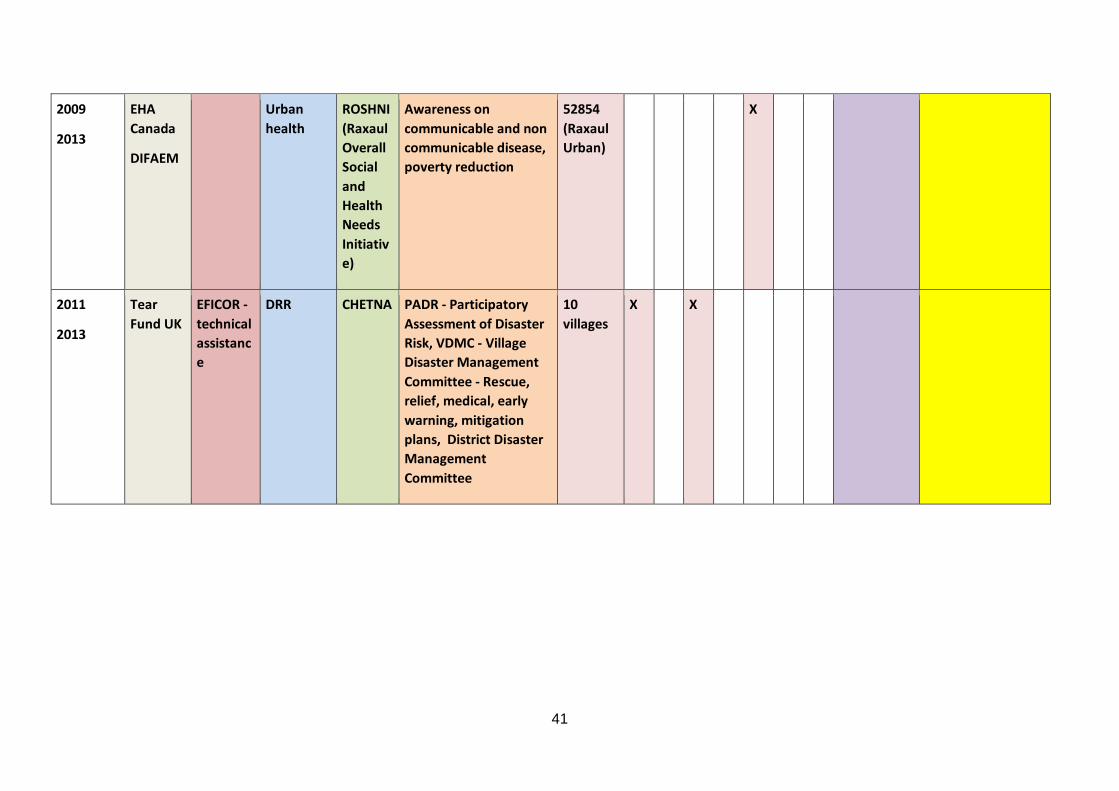
2009
2013
EHA Canada
DIFAEM
Urban health
ROSHNI (Raxaul Overall Social and Health Needs Initiative)
Awareness on communicable and non communicable disease, poverty reduction
52854 (Raxaul Urban)
X
2011
2013
Tear Fund UK
EFICOR - technical assistance
DRR CHETNA PADR - Participatory Assessment of Disaster Risk, VDMC - Village Disaster Management Committee - Rescue, relief, medical, early warning, mitigation plans, District Disaster Management Committee
10 villages
X X
41
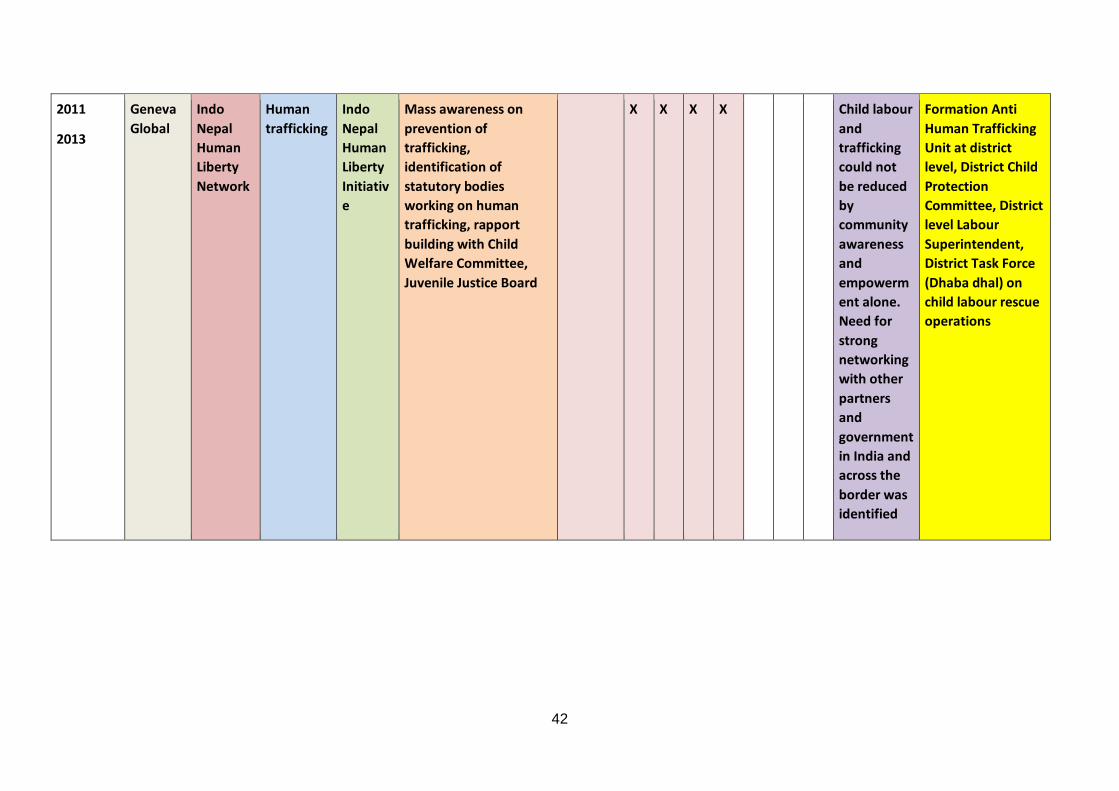
2011
2013
Geneva Global
Indo Nepal Human Liberty Network
Human trafficking
Indo Nepal Human Liberty Initiative
Mass awareness on prevention of trafficking, identification of statutory bodies working on human trafficking, rapport building with Child Welfare Committee, Juvenile Justice Board
X X X X Child labour and trafficking could not be reduced by community awareness and empowerment alone. Need for strong networking with other partners and government in India and across the border was identified
Formation Anti Human Trafficking Unit at district level, District Child Protection Committee, District level Labour Superintendent, District Task Force (Dhaba dhal) on child labour rescue operations
42
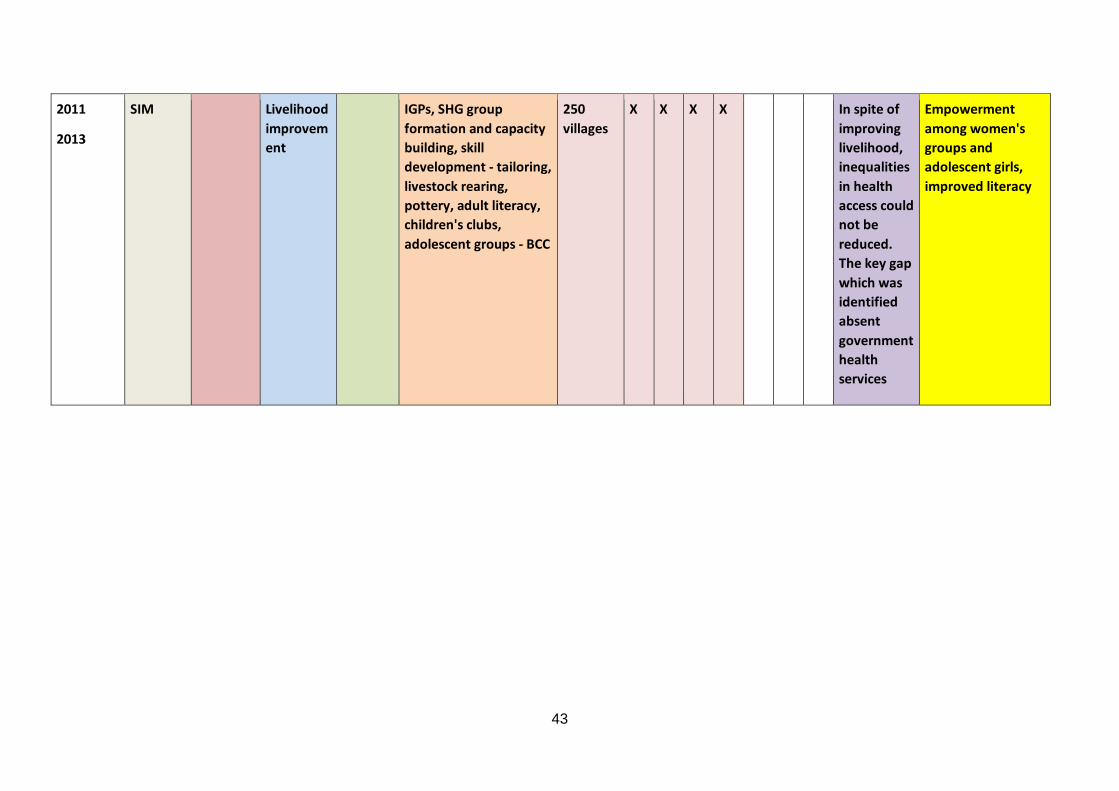
2011
2013
SIM Livelihood improvement
IGPs, SHG group formation and capacity building, skill development - tailoring, livestock rearing, pottery, adult literacy, children's clubs, adolescent groups - BCC
250 villages
X X X X In spite of improving livelihood, inequalities in health access could not be reduced. The key gap which was identified absent government health services
Empowerment among women's groups and adolescent girls, improved literacy
43
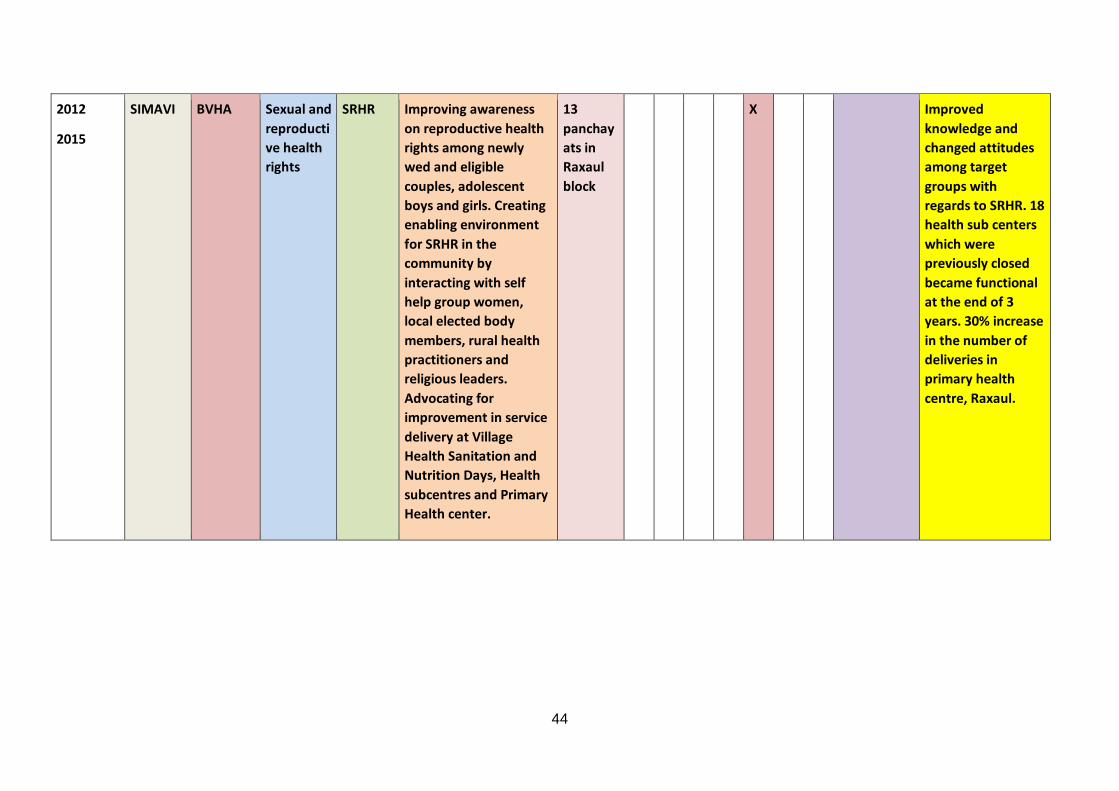
2012
2015
SIMAVI BVHA Sexual and reproductive health rights
SRHR Improving awareness on reproductive health rights among newly wed and eligible couples, adolescent boys and girls. Creating enabling environment for SRHR in the community by interacting with self help group women, local elected body members, rural health practitioners and religious leaders. Advocating for improvement in service delivery at Village Health Sanitation and Nutrition Days, Health subcentres and Primary Health center.
13 panchayats in Raxaul block
X Improved knowledge and changed attitudes among target groups with regards to SRHR. 18 health sub centers which were previously closed became functional at the end of 3 years. 30% increase in the number of deliveries in primary health centre, Raxaul.
44
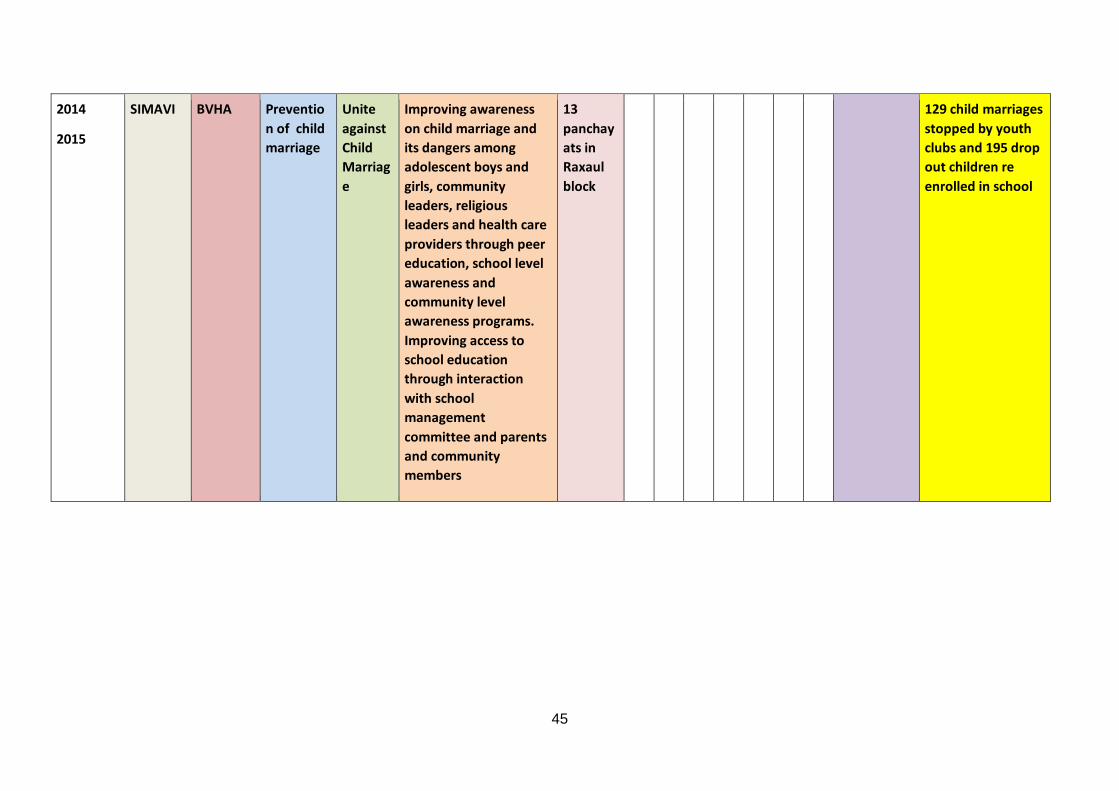
2014
2015
SIMAVI BVHA Prevention of child marriage
Unite against Child Marriage
Improving awareness on child marriage and its dangers among adolescent boys and girls, community leaders, religious leaders and health care providers through peer education, school level awareness and community level awareness programs. Improving access to school education through interaction with school management committee and parents and community members
13 panchayats in Raxaul block
129 child marriages stopped by youth clubs and 195 drop out children re enrolled in school
45
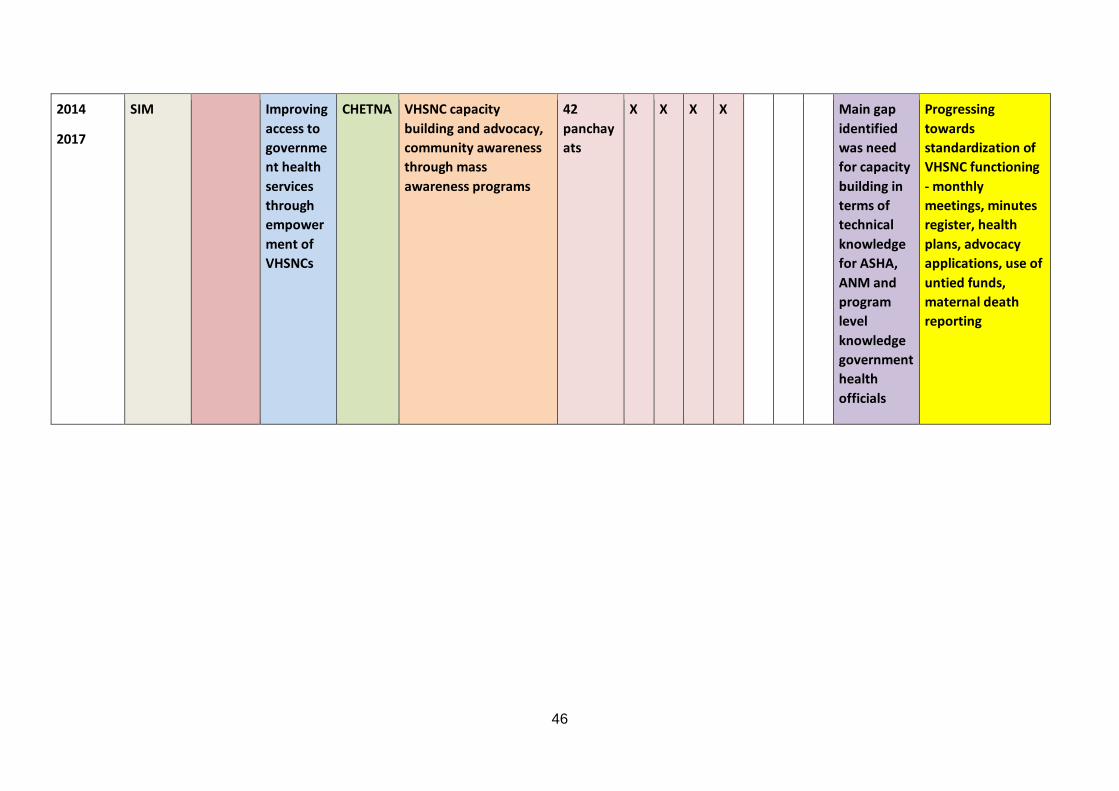
2014
2017
SIM Improving access to government health services through empowerment of VHSNCs
CHETNA VHSNC capacity building and advocacy, community awareness through mass awareness programs
42 panchayats
X X X X Main gap identified was need for capacity building in terms of technical knowledge for ASHA, ANM and program level knowledge government health officials
Progressing towards standardization of VHSNC functioning - monthly meetings, minutes register, health plans, advocacy applications, use of untied funds, maternal death reporting
46
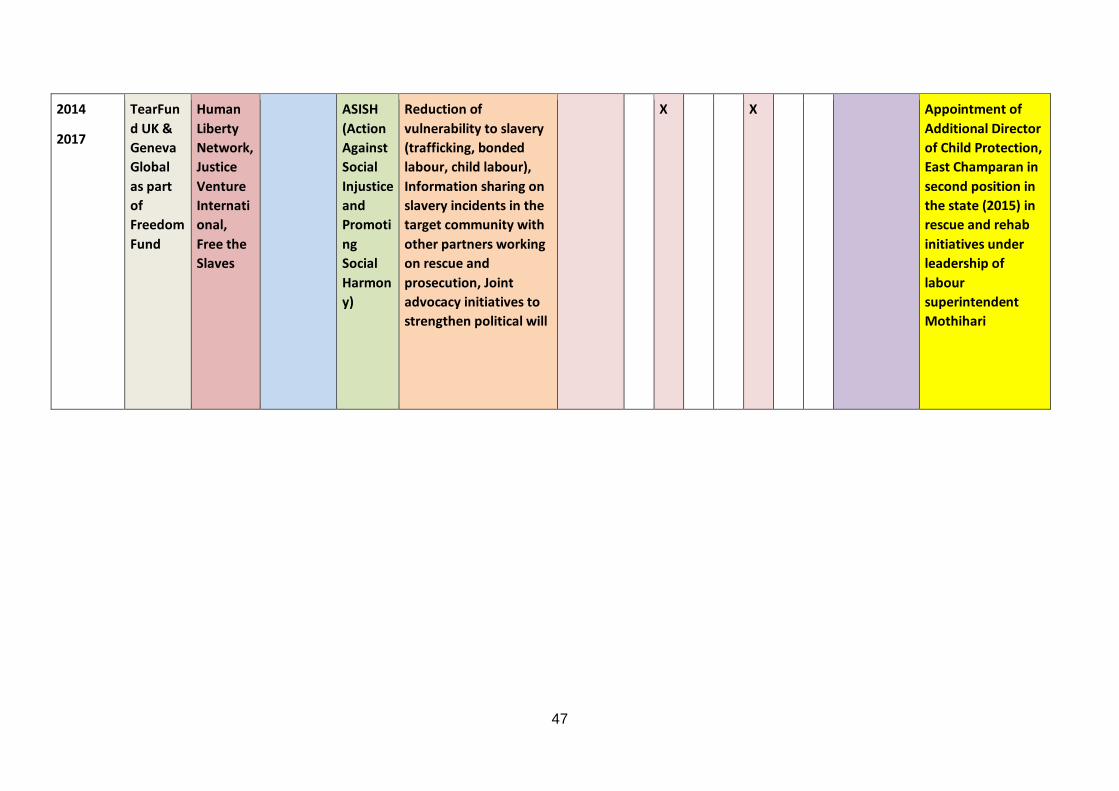
2014
2017
TearFund UK & Geneva Global as part of Freedom Fund
Human Liberty Network, Justice Venture International, Free the Slaves
ASISH (Action Against Social Injustice and Promoting Social Harmony)
Reduction of vulnerability to slavery (trafficking, bonded labour, child labour), Information sharing on slavery incidents in the target community with other partners working on rescue and prosecution, Joint advocacy initiatives to strengthen political will
X X Appointment of Additional Director of Child Protection, East Champaran in second position in the state (2015) in rescue and rehab initiatives under leadership of labour superintendent Mothihari
47
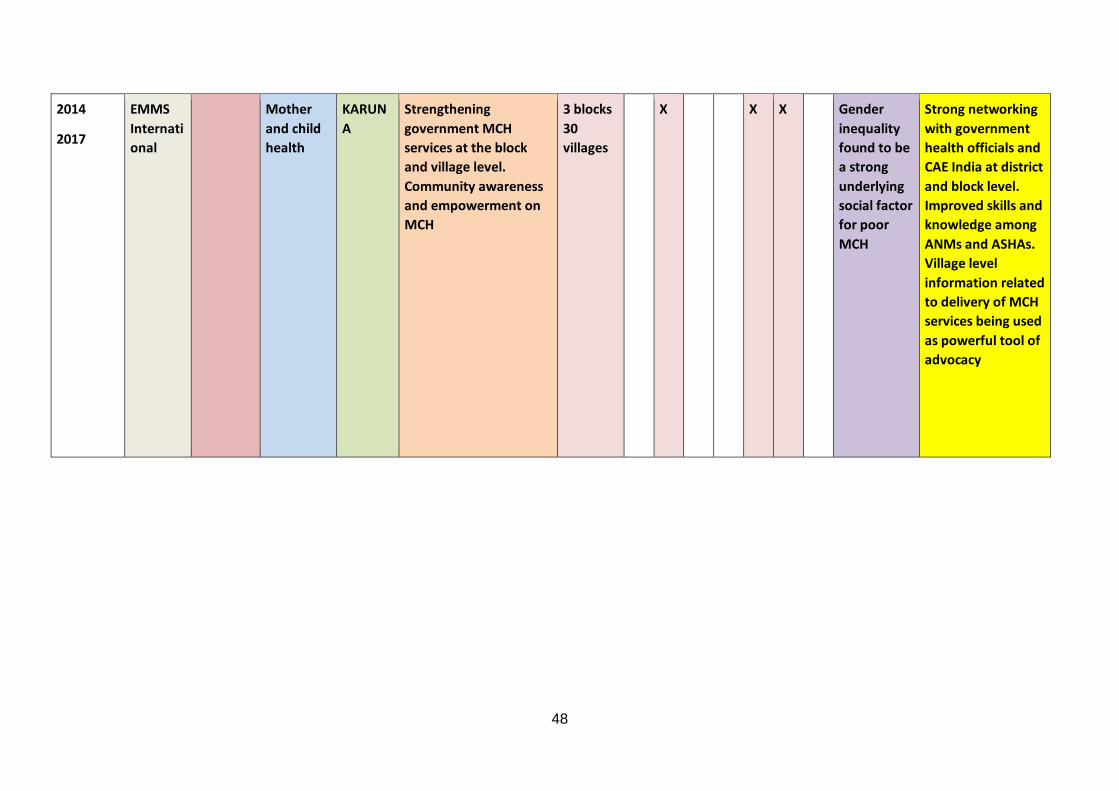
2014
2017
EMMS International
Mother and child health
KARUNA
Strengthening government MCH services at the block and village level. Community awareness and empowerment on MCH
3 blocks 30 villages
X X X Gender inequality found to be a strong underlying social factor for poor MCH
Strong networking with government health officials and CAE India at district and block level. Improved skills and knowledge among ANMs and ASHAs. Village level information related to delivery of MCH services being used as powerful tool of advocacy
48
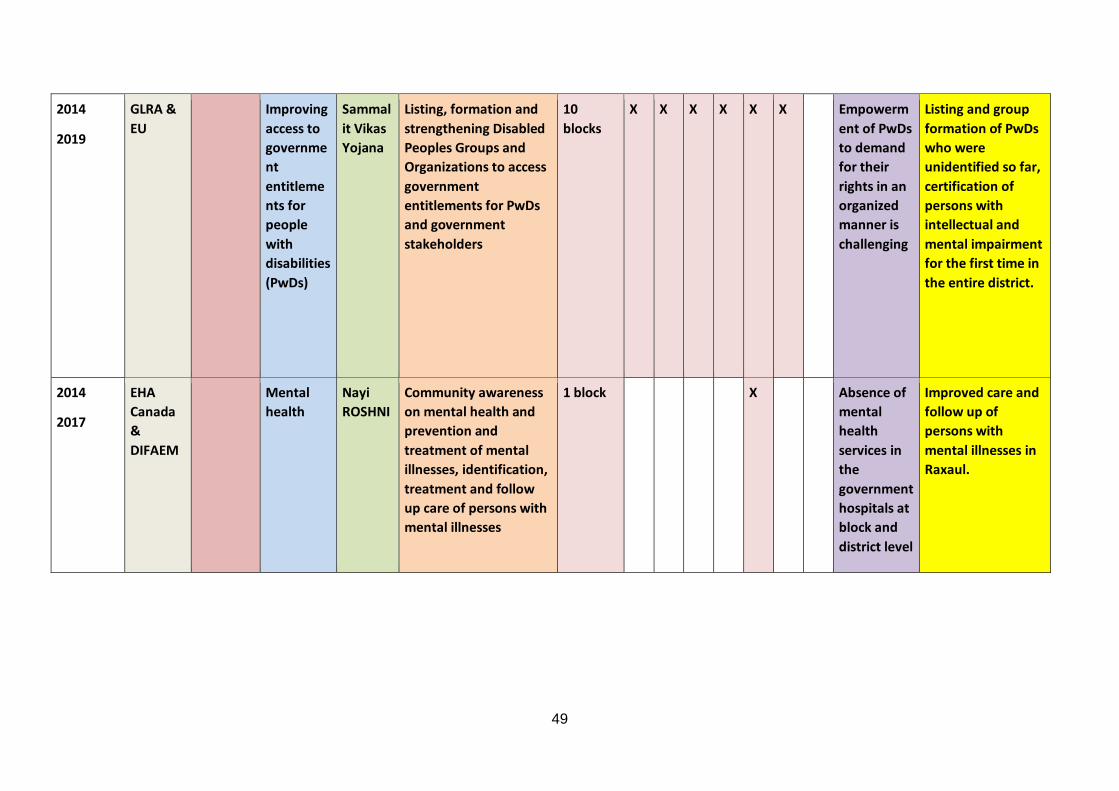
2014
2019
GLRA & EU
Improving access to government entitlements for people with disabilities (PwDs)
Sammalit Vikas Yojana
Listing, formation and strengthening Disabled Peoples Groups and Organizations to access government entitlements for PwDs and government stakeholders
10 blocks
X X X X X X Empowerment of PwDs to demand for their rights in an organized manner is challenging
Listing and group formation of PwDs who were unidentified so far, certification of persons with intellectual and mental impairment for the first time in the entire district.
2014
2017
EHA Canada & DIFAEM
Mental health
Nayi ROSHNI
Community awareness on mental health and prevention and treatment of mental illnesses, identification, treatment and follow up care of persons with mental illnesses
1 block X Absence of mental health services in the government hospitals at block and district level
Improved care and follow up of persons with mental illnesses in Raxaul.
49
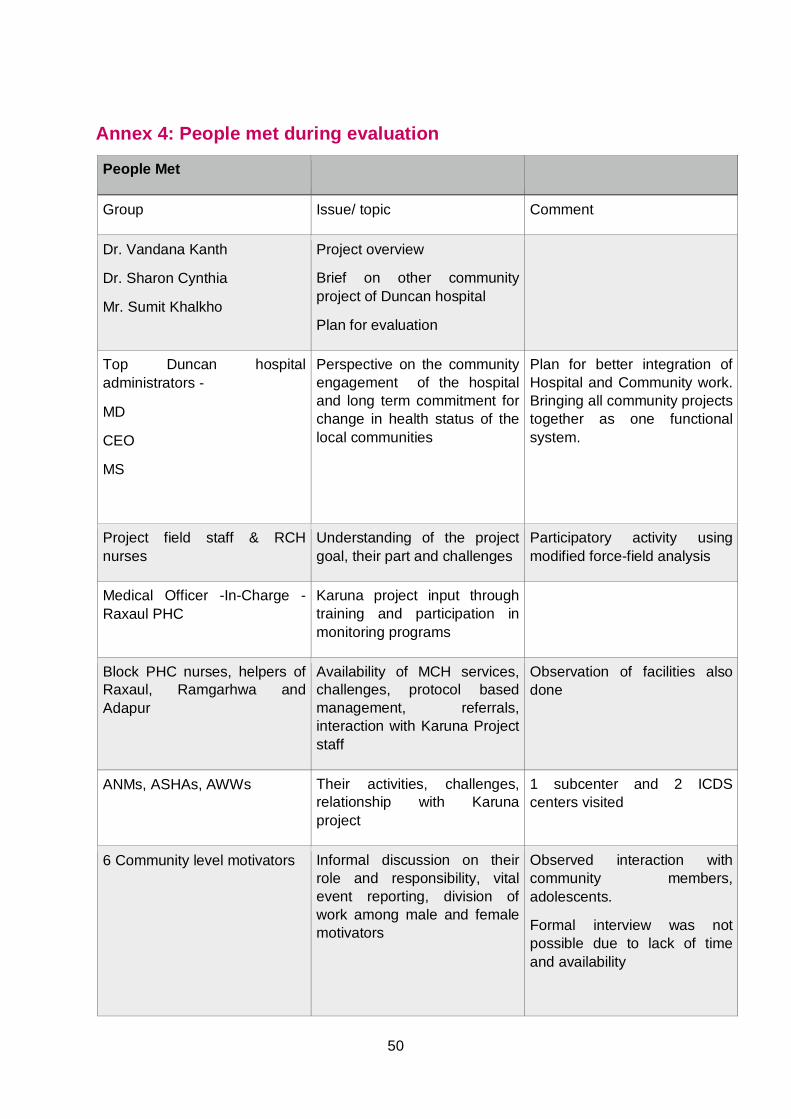
Annex 4: People met during evaluation
People Met
Group Issue/ topic Comment
Dr. Vandana Kanth
Dr. Sharon Cynthia
Mr. Sumit Khalkho
Project overview
Brief on other community project of Duncan hospital
Plan for evaluation
Top Duncan hospital administrators -
MD
CEO
MS
Perspective on the community engagement of the hospital and long term commitment for change in health status of the local communities
Plan for better integration of Hospital and Community work. Bringing all community projects together as one functional system.
Project field staff & RCH nurses
Understanding of the project goal, their part and challenges
Participatory activity using modified force-field analysis
Medical Officer -In-Charge - Raxaul PHC
Karuna project input through training and participation in monitoring programs
Block PHC nurses, helpers of Raxaul, Ramgarhwa and Adapur
Availability of MCH services, challenges, protocol based management, referrals, interaction with Karuna Project staff
Observation of facilities also done
ANMs, ASHAs, AWWs Their activities, challenges, relationship with Karuna project
1 subcenter and 2 ICDS centers visited
6 Community level motivators Informal discussion on their role and responsibility, vital event reporting, division of work among male and female motivators
Observed interaction with community members, adolescents.
Formal interview was not possible due to lack of time and availability
50
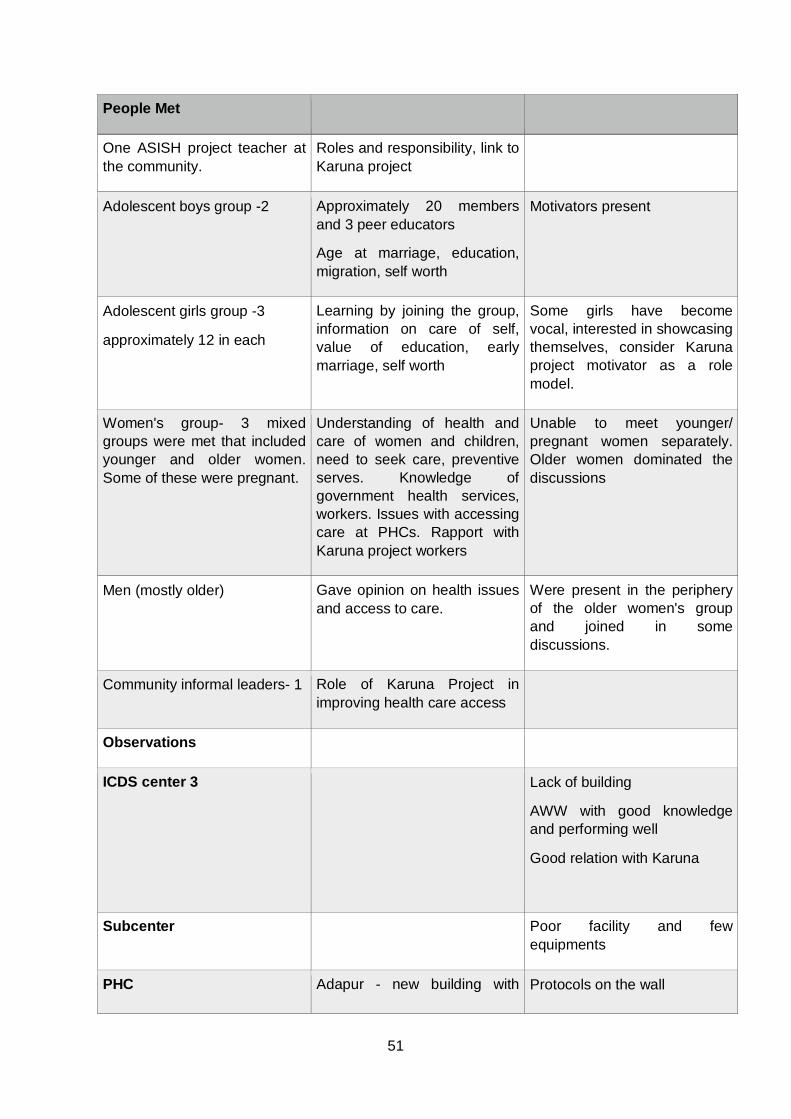
People Met
One ASISH project teacher at the community.
Roles and responsibility, link to Karuna project
Adolescent boys group -2 Approximately 20 members and 3 peer educators
Age at marriage, education, migration, self worth
Motivators present
Adolescent girls group -3
approximately 12 in each
Learning by joining the group, information on care of self, value of education, early marriage, self worth
Some girls have become vocal, interested in showcasing themselves, consider Karuna project motivator as a role model.
Women's group- 3 mixed groups were met that included younger and older women. Some of these were pregnant.
Understanding of health and care of women and children, need to seek care, preventive serves. Knowledge of government health services, workers. Issues with accessing care at PHCs. Rapport with Karuna project workers
Unable to meet younger/ pregnant women separately. Older women dominated the discussions
Men (mostly older) Gave opinion on health issues and access to care.
Were present in the periphery of the older women's group and joined in some discussions.
Community informal leaders- 1 Role of Karuna Project in improving health care access
Observations
ICDS center 3 Lack of building
AWW with good knowledge and performing well
Good relation with Karuna
Subcenter Poor facility and few equipments
PHC Adapur - new building with Protocols on the wall
51
People Met
adequate space, few staff
Ramgarhwa
Raxaul- old building with limited space
New coming up
Ultra sound done by a male technician
Adapur center Use as OP and Chetna project uses for meetings/ lunch stop
Almost opposite Adapur PHC
Champapur center
Duncan hospital faciltities Additional equipments for maternal and child health emergency and acute care are purchased with project finding.
PHC review meeting
Raxual
ANMs, MO-IC and representatives of many NGOs (WHO, CARE, Pathfinders, UNICEF etc. & Karuna project coordinators) also attend
Lot of input in this PHC with equipments, Hb and urine test kits, support in organising VHND etc. Different NGOs monitoring/contributing to different aspects of primary health care
PHC review meeting
Ramgarhwa
ANMs, MO-1, MO-IC, UNICEF rep, CARE rep.
52
Annex 5: Evaluation Programme Day 1, AM The evaluation team had detailed discussions with the Director
of Community Health Department and Project Coordinator, Dr. Sharon, on Day 1. With input from the team, the field visits were finalised.
Day 1, PM, Day 2 and Day 4
Field visits to all three blocks, visit to PHCs, HSC and ICDS centre.
Visit to the Hospital especially maternal and neonatal service.
Informal interaction with doctors’ team.
Day 3 Meeting with Duncan Hospital administrators and project leaders.
Group activity and discussion with the supervisory team.
Day 5 Debriefing and clarifications with project leaders.
53
© EMMS International April 2016
This publication is copyright but the text may be used free of charge for the purposes of advocacy, campaigning, education, and research, provided that the source is acknowledged in full. The copyright holder requests that all such use be registered with them for impact assessment purposes. For copying in any other circumstances, or for re-use in other publications, or for translation or adaptation, permission must be secured and a fee may be charged.
The information in this publication is correct at the time of going to press.
EMMS International 7 Washington Lane Edinburgh EH11 2HA
0131 313 3828 www.emms.org [email protected]
EMMS International is a charity, registered in Scotland (SC032327) and a company limited by guarantee, registered in Scotland (SC224402).
54