jurnal plastic surg - medicinal leeches for the treatment of venous congestion and hematoma
DESCRIPTION
JournalTRANSCRIPT

© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811 JDDG | 11˙2010 (Band 8)
JDDG; 2010 • 8:881–888 Submitted: 23.3.2010 | Accepted: 10.5.2010
Keywords• medicinal leeches• Hirudo medicinalis• venous congestion• hematoma• complication• plastic reconstructive surgery
SummaryBackground: Leeches were used for medical purposes as long as 2 000 yearsago in ancient Egypt. In recent years the use of medicinal leeches becamerather popular again, e. g. to improve blood circulation in ischemic tissue afterreconstructive plastic surgery.Patients and Methods: In a single center, retrospective study 23 consecutivecases were analyzed in which medicinal leeches had been used therapeuticallyafter plastic reconstructive surgery. All cases were categorized regarding theindication for leech therapy, the onset, the duration, the number of leeches andthe number of sessions.Results: Among the group of patients there were 7 female and 16 male patientswith a mean age of 73 ± 14 years (48–94 years) altogether. The main indicationswere venous congestion (12/23; 52 %) and hematoma (9/23; 39 %). Two caseswere diagnosed with a necrosis of the tip of the flap and therefore receivedleech therapy (2/23; 9 %). The average number of leeches was 2.6 leeches/session,the number of sessions was 1.7 ± 0.8. 20/23 patients (87 %) showed a restitutioad integrum after leech therapy, in 3/23 patients (13 %) a necrosis of the tip ofthe flap could not be prevented. A clinical improvement was noticed after anaverage of 1.1 ± 0.3 days. Conclusions: The early application of medicinal leeches can improve localhemodynamic conditions. Leech therapy is a simple and effective method; thecost efficiency of the treatment is high.
Medicinal leeches for the treatment of venouscongestion and hematoma after plasticreconstructive surgery Friederike Riede1*, Wolfgang Koenen1*, Sergij Goerdt1, Heimo Ehmke2, Jörg Faulhaber1
(1) Department of Dermatology, Venereology and Allergy, Medical Faculty Mannheim of the University of Heidelberg,University Medicine Mannheim, Mannheim, Germany
(2) Department of Physiology, Center of Experimental Medicine, University Hospital Eppendorf, Hamburg, Germany
*Both authors contributed equally to this paper.
IntroductionMedicinal leeches (Hirudo medicinalis)have been used for over 2000 years totreat a variety of medical complaints. Atthe end of the 20th century new therapyconcepts took the place of leech therapy[1, 2]. With microvascular surgery tech-niques there has been a renaissance inthe use of medicinal leeches in recentyears. One main indication here is theimprovement of tissue circulation afterreconstructive procedures. Weinberg
et al., for example, were able to showthat leeches are a dependable method torelieve acute venous congestion [3].Leeches also have been used successfullyto save various free skin grafts [3]. An important factor oin this therapeu-tic effect is hirudin, which is found inleech saliva. Hirudin is a polypeptidecontaining 65 amino acids with a molecular weight of about 7 kD.Hirudin has a selective affinity tothrombin and thus inhibits the conver-
sion of fibrinogen to fibrin [1]. In themeantime recombinant hirudin is avail-able for a wide range of therapeutic indications, for example recombinanthirudin has been licensed in Germanysince 1997 for the therapy of HIT (heparin-induced thrombocytopenia)type II [4]. In addition to hirudin thesaliva of leeches contains other pharmacologically active substancessuch as hyaluronidase and protease inhibitors which promote spreading of
DOI: 10.1111/j.1610-0387.2010.07473.x Original Article 881

the anticoagulant in the wound. The re-lease of an additional vasodilator (in theform of an antihistamine) possibly leadsto the observed prolongation of bleed-ing time after the end of the blood mealof the leech [1].Venous congestion denotes a situationwhere venous drainage of tissue is highlyimpaired or even totally blocked whilearterial inflow is unimpaired. As a resultoutward filtration in the capillary bed increases and finally arterial inflow alsodeclines. Clinical features of venous stasis are dark discoloration, edema andoverheating of the affected tissue. Venous stasis is a serious complicationafter microsurgical reconstructive proce-
dures such as flaps, free grafts and tissuereplantation. Without therapy stasisresults in ischemia which – depending onseverity – can lead to tissue necrosis [5]. The goal of this study was to examine theclinical course after use of leeches afterplastic/ reconstructive procedures. Onthe basis of 23 clinical cases, the effec-tiveness of therapeutic application ofmedicinal leeches is analyzed. Target pa-rameters were the indication for medici-nal leech therapy, the postoperative dayof onset and the number of therapy rep-etitions. Further, the number of leechesused per session, the improvement ofsigns and symptoms and the latency pe-riod were analyzed.
Patients, materials and methodsPatientsIncluded in this study were 23 consecu-tive patients treated for skin cancer between 2006 and 2009 in the Depart-ment of Dermatology, Venereology and Allergy at University MedicineMannheim. After micrographically controlled excision followed by plasticreconstruction medical leeches were em-ployed in the postoperative course due tocomplications. During the study period,flaps displaying signs of venous conges-tion were routinely treated with medici-nal leeches. The number of documentedcases thus equals the rate of stasis com-plications in 4 years.
882 Original Article Leeches in complications after plastic reconstructive surgery
JDDG | 11˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811
Table 1: Patient and tumor characteristics.
Abbreviations: w = woman; m = man; SD = standard deviation.
Patient Gender Age (years) Tumor Location Plastic reconstructive procedure
1 m 70 Melanoma Temple Advancement and rotation flap
2 m 79Chondrodermatitis nodu-laris helicis
Ear Tissue expansion
3 m 79 Lentigo maligna Cheek Cheek rotation flap
4 w 68 Basal cell carcinoma Nose U-plasty
5 m 77 Basal cell carcinoma Nose Transposition flap
6 m 53 Basal cell carcinoma Nose Pedicled forehead flap
7 m 48 Basal cell carcinoma Nose Pedicled forehead flap
8 m 76 Basal cell carcinoma Nose Advancement and rotation flap
9 m 80 Basal cell carcinoma Nose Transposition flap
10 w 54 Basal cell carcinoma Cheek Subcutaneous pedicled island flap
11 m 94 Squamous cell carcinoma Lower lip Bernard flap
12 w 84 Basal cell carcinoma Nose U-plasty
13 m 57 Basal cell carcinoma Nose Advancement and rotation flap
14 m 50 Basal cell carcinoma Nose Transposition flap
15 m 87 Basal cell carcinoma Lower Lid Cheek rotation flap
16 m 56 Basal cell carcinoma Cheek Advancement and rotation flap
17 w 89 Basal cell carcinoma Nose Transposition flap + full-thickness graft
18 w 79 Basal cell carcinomaMedial canthus of the eye
Subcutaneous pedicled island flap
19 m 82 Basal cell carcinoma Upper lip Advancement and rotation flap
20 w 94 Squamous cell carcinoma Cheek Transposition flap
21 m 85 Basal cell carcinoma Ear Advancement flap
22 m 69 Basal cell carcinoma Nose Advancement flap
23 w 76 Squamous cell carcinoma Lip Bernard-Freeman-Fries-plasty
Mean ± SD 16 /7 73 ± 14
↓
†

70 % ethanol and disposed of with theclinic’s medical waste. For application of the medicinal leechthe site was scarified with a lancet or asterile canula until blood emerged. Thenthe animals were applied using atrau-matic tweezers. After application theleeches were covered with moist gauzeand the lighting in the treatment roomwas dimmed. Therapy was over when theleech fell off by itself. No special tech-nique was employed to fix the leech.
ResultsPatients and tumor characteristics Of the 23 patients included 7/23 (30 %)were female, 16/23 (70 %) were male.Men were thus more frequently affectedin our group of patients. At the time of surgery the average age ofthe women was 78 years (54–94 years)
Leeches in complications after plastic reconstructive surgery Original Article 883
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811 JDDG | 11˙2010 (Band 8)
Materials and methodsOnly patients with defect closure in theface who developed clinical complicationsduring their inpatient stay following flaps
were included in this retrospective study.These included either flaps displayingsigns of venous congestion up to superfi-cial necroses or hematomas. The followingdata were recorded: date of surgery, age,gender, time point of leech application,number of sessions, number of leeches ap-plied per session as well as clinical responseto treatment. The data were recorded intabular form and the mean ± standard de-viation determined. For safety reasons allpatients received prophylactic antibiosiswith cefuroxime (500 mg 2 � 1 tablet) orin case of penicillin allergy with clin-damycin (300 mg 3 � 1 tablet).All medicinal leeches were obtained from the firm Biebertaler Blutegelzucht(Biebertaler Blutegelzucht GmbH,Biebertal, Germany) and were kept atroom temperature in tap water. After thetreatment the leeches were killed with
Figure 1: Summary of preoperative risk factors.Depicted are the coincidence of diabetes (DMType 2: diabetes mellitus type 2), administrationof anticoagulation (PHEN: phenprocoumon,ASS: acetylsalicylic acid, CLO: clopidogrel) andnicotine abuse.
Table 2: Summary of treatment results.
Abbreviation: SD = standard deviation.
Patient IndicationStart of treat-ment (dayspostop.)
Number ofsessions (n)
Number ofleeches persession (n)
Restitutio adintegrum vs.flap failure
Clinical improve-ment (days afterleech application)
1 Venous congestion 7 3 3 Healed 2
2 Hematoma 3 1 2 Healed 1
3 Venous congestion 2 1 5 Healed 1
4 Necrosis 2 3 3 Partial necrosis –
5 Hematoma 3 3 3 Healed 2
6 Venous congestion 5 2 2 Healed 1
7 Venous congestion 2 2 2 Healed 1
8 Hematoma 3 1 3 Healed 1
9 Venous congestion 3 1 4 Healed 1
10 Venous congestion 1 1 2 Healed 1
11 Venous congestion 2 1 3 Healed 1
12 Venous congestion 1 2 2 Healed 1
13 Venous congestion 2 1 2 Healed 1
14 Hematoma 2 1 2 Healed 1
15 Hematoma 2 3 2 Healed 1
16 Venous congestion 2 2 3 Partial necrosis –
17 Hematoma 5 1 3 Healed 1
18 Hematoma 1 1 1 Healed 1
19 Hematoma 3 2 2 Healed 1
20 Venous congestion 1 2 2 Healed 1
21 Hematoma 3 3 2 Healed 1
22 Necrosis 2 1 2 Partial necrosis –
23 Venous congestion 3 1 4 Healed 1
Mean ± SD 2.6 ± 1.5 1.7 ± 0.8 2.6 ± 0.9 1,1 ± 0,3

and of the men 71 years (48–89 years).The average age of the total group was73 ± 14 years (48–94 years). Of 23 tumors 17/23 (74 %) were basalcell carcinomas, 3/23 (13 %) squamouscell carcinomas and 1/23 (4 %) each amelanoma, chondrodermatitis nodularishelicis or lentigo maligna. Of the tumors11/23 (48 %) were located in the regionof the nose, 5/23 (20 %) on cheeks andtemple, 3/23 (13 %) were on the upperor lower lips, 2/23 (9 %) were in the pe-riorbital region and 2/23 (9 %) on theears (Table 1). The analysis of further predisposing riskfactors showed no correlation betweenthe occurrence of venous congestion andfactors such as diabetes mellitus (2/23;9 %) or nicotine abuse (2/23; 9 %). Pa-tients with anticoagulation (11/23;phenprocoumon or vitamin K antago-nist [n = 5], acetylsalicylic acid [n = 5],clopidogrel [n = 1]) constituted 48 % ofall cases, which deviates from regular col-lectives of all surgical patients, with finalnumbers being lacking. A review of riskfactors is presented in Figure 1.
Treatment resultsClosure was achieved by various localflaps listed in Table 1. The dominant in-dication was venous congestion (stasis)(12/23; 52 %) or a hematoma (9/23;39 %). In two cases medicinal leecheswere applied due to a necrosis of the tipof the flap (2/23; 9 %) (Table 2). Therapy was initiated on average2.6 ± 1.5 days postoperatively. The meannumber of leeches applied was2.6 leeches per session. The number ofsessions of leech therapy per patient was1.7 ± 0.8. In 12/23 (52 %) cases only asingle session was needed, in 6/23(26 %) two sessions were performed, in5/23 (22 %) patients three sessions wererequired (Table 2). Restitutio ad integrum after treatmentwas observed in 20/23 (87 %) patients.Improvement occurred after a mean of1.1 ± 0.3 days, with 18/23 (78 %) dis-playing clinical improvement after oneday of treatment, while in 2/23 (9 %)improvement was only seen after thesecond day. In 3/23 (13 %) patientsmedicinal leech application did notlead to clinical improvement andnecrosis of the tip of the flap occurred(Table 2).Representative clinical cases are shown inFigures 2 and 3.
884 Original Article Leeches in complications after plastic reconstructive surgery
JDDG | 11˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811
Figure 2: A 94-year-old patient with venous congestion of the distal part of the flap one day afterreconstruction of a lower lip defect using a Bernard flap (a). Treatment of venous congestion withthree medicinal leeches (b). Significant discoloration of the flap tip one day after treatment (c).Clinical appearance four days (d) and two months (e) after treatment with medicinal leeches.

DiscussionIn the present study the patient collectiveconsists of 7 women and 16 men with amean age of 73 years (48–94 years). Ofnote is the unequal gender distributionof about 1 : 3 (women : men) which isprimarily unexplained. A random pa-tient constellation would be a conceiv-able explanation, but for such a devia-tion the number of patients includedseems too large. An unequal distributionof the genders in the collective of surgicalpatients could also be excluded. Gender-specific hormonal causes are also con-ceivable. This hypothesis is supported byrecently published data showing that in amouse model estradiol-17ß has protec-tive effects with regard to the develop-ment of necrosis of the tip of the flap [6]. In the patient collective presented ther-apy was initiated after 2.6 days. The pa-
tients were treated on average with1.7 sessions with 2.6 leeches per session.Data in the literature as well as our ownclinical observations suggest that thetherapeutic effectiveness is all the greaterthe sooner that medicinal leech therapyis started [7]. Physiological understand-ing of hemodynamics in the flaps in ob-structive situations underscores the ne-cessity of early intervention, in case oftotal blockade of venous drainage evenwithin 8 hours [8]. We are therefore ofthe opinion that medicinal leechesshould be applied as early as possible, op-timally within the first 24 hours. Thenumber of leeches applied and the num-ber of sessions must be adapted to thesize of the flap and the degree of venouscongestion. This demand is also sup-ported by a recently published experi-mental study on rats [9].
The dominant indications for the use ofmedicinal leeches on the studied patientcollective were venous congestion andhematomas. Due to blockage of venousdrainage venous congestion results in anincreased hydrostatic pressure in the cap-illaries and thus effective filtration pres-sure. As a consequence of increased out-ward filtration increasing amounts of fluidenter the surrounding tissue. The result-ing increase in interstitial pressure re-duces transmural pressure in the supply-ing arteriole resulting in vasodilation anda further increase in capillary pressure.With maximum precapillary vasodila-tion vasomotion, which is important forreabsorption, may be impaired thusgreatly promoting the further develop-ment of local edema [10]. Additionally,there can be a disturbance of lymphaticdrainage as well as an activation of inflam-matory processes (adhesion molecules,etc.) (Figure 4). Therapy with medicinalleeches probably targets several of thesepathophysiological mechanisms. It reducesvenous congestion by providing for an al-ternative drainage for the congested bloodand thus allows for arterial reperfusion ofthe capillary bed [3]. The increased perfu-sion can maintain physiological prerequi-sites in the affected tissue allowing forpreservation of tissue vitality up to neovascularization. Without therapy ischemia develops in the congested tissueand, depending on the severity of ischemia, this can lead to necrosis of thetissue [5]. In addition to an active reduc-tion of blood in congested tissue by theblood meal of the leech indirect effectsoccur by means of passive bleeding fromthe bite site after the leech falls off [11–14].In one of the few experimental studiesConforti and coworkers were able torecord characteristics of the medicinalleech in the treatment of venous conges-tion in a porcine model. The mean vol-ume of a blood meal was 2.45 ml; themean time of leech application per ses-sion was 70.9 minutes. The passiveblood loss per leech after two hours wason average 2.2 ml and after 4 hours onaverage 2.5 ml, thus comparable to theamount of the active blood meal [5]. The practical use of the medicinal leechis uncomplicated. To keep the leech inthe treatment area various techniques arediscussed in the literature. In addition tothe use of syringes [15, 16], plastic bags,opsite dressings [17] and even surgicalsuture material are recommended [18].
Leeches in complications after plastic reconstructive surgery Original Article 885
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811 JDDG | 11˙2010 (Band 8)
Figure 2: Continued.
In this study the leeches were only cov-ered with a gauze compress and the light-ing in the treatment room dimmed. The most dangerous complication of me-dicinal leech therapy is an infection withAeromonas hydrophila. This bacterium isfound in the intestinal flora of the leechand can cause wound infection up to sep-sis [19]. With the use of prophylactic an-tibiosis – as also recommended in the lit-erature – this complication was notobserved in the study collective [20]. An-ecdotal reports are made in the literatureof relevant anemia [20, 21] often follow-ing multiple applications of leeches. Withexception of prolonged bleeding times ofup to two days in one case, no bleedingcomplications were observed in the studycollective. The occurrence of postoperative surgicalcomplications in reconstructive surgeryis rare with correct indications and per-formance and is directly related to theexperience of the surgeon [22]. The pa-tients for this study were recruited overfour years from a total of about 24,000surgical procedures, reflecting the lowrate of venous congestion as a complica-tion. In economic terms the use of me-dicinal leeches is highly efficient. Treat-ment costs for a medicinal leech are4.35 € plus value added tax and ship-ping. For an average treatment the costfor materials is about 15 € and for per-sonnel about 8 €. Compared with thecost of a prolonged inpatient stay ofabout 250 € per day, surgical revisionswith operating room costs of over 8 €
per minute or the cost of modern wounddressing of about 70 € per week or fol-low-up surgical procedures, the cost ofmedicinal leeches is negligible. As an alternative to medicinal leeches“pin-pricking” of flaps with venous con-gestion or grafts is common. In our opin-ion this procedure is indicated only formoderate venous congestion as the shortbleeding time makes it inferior to medic-inal leech therapy. Scientific studies onthis question are still lacking. A some-what more experimental treatment op-tion is hyperbaric oxygen therapy. Gamp-per and coworkers were able tosignificantly reduce local flap failure withsecondary venous ischemia in an animalmodel with hyperbaric oxygenation [23].
ConclusionsThe present study demonstrated thatmedicinal leeches provide an elegant and
886 Original Article Leeches in complications after plastic reconstructive surgery
JDDG | 11˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811
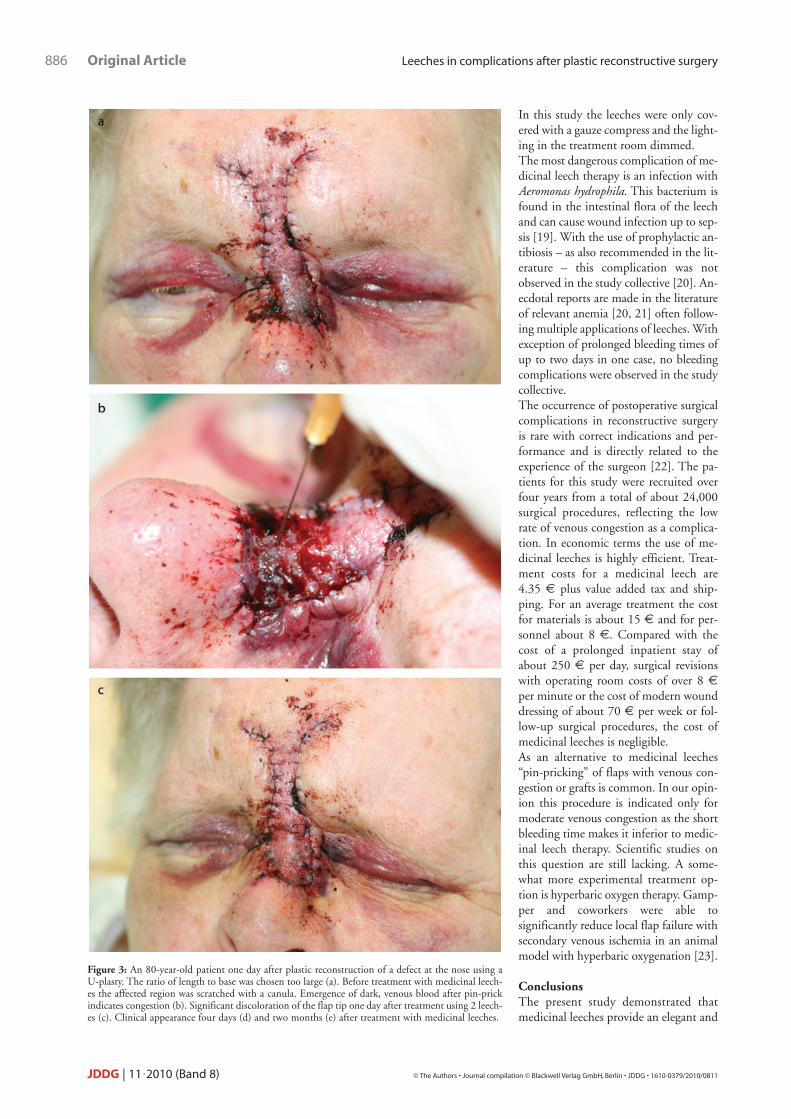
Figure 3: An 80-year-old patient one day after plastic reconstruction of a defect at the nose using aU-plasty. The ratio of length to base was chosen too large (a). Before treatment with medicinal leech-es the affected region was scratched with a canula. Emergence of dark, venous blood after pin-prickindicates congestion (b). Significant discoloration of the flap tip one day after treatment using 2 leech-es (c). Clinical appearance four days (d) and two months (e) after treatment with medicinal leeches.

promising therapy option to treat venouscongestion and hematomas after plasticsurgery. In the patient collective studiedin 87 % of cases there was a restitutio adintegrum. Only in three patients was theuse of medicinal leeches unable to pre-vent the development or progression ofnecrosis of the tip of the flap. For the treatment of venous congestionmedicinal leeches are a sensible – even isnot established – therapy form due totheir ability to reduce venous stasis and,for a limited period of time, improve lo-cal hemodynamic conditions in flaps.Due to the low therapy costs and thehigh effectiveness this treatment is verycost-efficient. In addition, high follow-up costs of postoperative complicationscan be prevented. Medicinal leechesshould be applied early, if possible within
24 hours. The number of leeches re-quired as well as the number of sessionsdepends on the size of the affected areaand the clinical severity. <<<
Conflicts of interestNone.
Friederike Riede
Correspondence toDr. Jörg FaulhaberDepartment of Dermatology, Venereologyand AllergyUMM – University Medicine MannheimMedical Faculty Mannheim of the University of HeidelbergTheodor-Kutzer-Ufer 1–3D-68167 Mannheim, GermanyTel.: +49-621-383-2280Fax: +49-621-383-3815E-mail: [email protected]
References1 Wells MD, Manktelow RT, Boyd JB,
Bowen V. The medical leech: an old tre-atment revisited. Microsurgery 1993;14: 183–6.
2 Adams SL. The medical leech: A pagefrom the annelids of internal medicine.Ann Intern Med 1988; 109: 399–405.
3 Weinfeld AB, Yuksel E, Boutros S,Gura DH, Akyurek M, Friedman JD.Clinical and scientific considerations inleech therapy for the management ofacute venous congestion: an updatedreview. Ann Plast Surg 2000; 45:207–12.
4 Kleinschmidt S, Seyfert UT. Die Heparin-induzierte Thrombopenie(HIT) Bedeutung für Anästhesie undIntensivmedizin. Anästhesist 1999; 48:771–85.
5 Conforti ML, Connor NP, Heisey DM,Hartig GK. Evaluation of performancecharacteristics of the medicinal leech(Hirudo medicinalis) for the treatmentof venous congestion. Plast ReconstrSurg 2002; 109(1): 228–35.
6 Toutain CE, Brouchet L, Raymond-Letron I, Vicendo P, Bergès H, Favre J,Fouque MJ, Krust A, Schmitt AM,Chambon P, Gourdy P, Arnal JF, Len-fant F. Prevention of skin flap necrosisby estradiol involves reperfusion of aprotected vascular network. Circ Res2009; 104(2): 245–54.
7 Utley DS, Koch RJ, Goode RL. The failing flap in facial plastic and reconstructive surgery: role of the me-dicinal leech. Laryngoscope 1998; 108:1129–35.
8 Kerrigan CL, Wizman P, Hjortdal VE,Sampalis J. Global flap ischemia: acomparison of arterial versus venousetiology. Plast Reconstr Surg 1994;93(7): 1485–95.
9 Schlaudraff KU, Bezzola T, MontandonD, Pepper MS, Pittet B. Mixed
Leeches in complications after plastic reconstructive surgery Original Article 887
© The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811 JDDG | 11˙2010 (Band 8)
Figure 3: Continued.

arterio-venous insufficiency in randomskin flaps in the rat: is the applicationof medicinal leeches beneficial? J SurgRes 2008; 150: 85–91.
10 Levick JR, Michel CC. Microvascularfluid exchange and the revised Starlingprinciple. Cardiovascular Res 2010Mar 3. [Epub ahead of print].
11 Hayden RE, Phillips JG, McLear PW.Leeches: objective monitoring of alte-red perfusion in congested flaps. ArchOtolaryngol Head Neck Surg 1988;114(12): 1395–9.
12 Smoot EC 3rd, Debs N, Banducci D,Poole M, Roth A. Leech therapy andbleeding wound techniques to relievevenous congestion. J Reconstr Micro-surg 1990; 6(3): 245–50.
13 Smoot EC, Ruiz-Inchaustegui JA, RothAC. Mechanical leech therapy to relievevenous congestion. J Reconstr Micro-surg 1995; 11(1): 51–5.
14 Nowak G, Schrör K. Hirudin – thelong and stony way from an anticoagu-
lant peptide in the saliva of medicinalleech to a recombinant drug andbeyond. A historical piece. ThrombHaemost 2007; 98(1): 116–9.
15 Azari K, Fisher C. A simple device for theapplication of medicinal leeches. PlastReconstr Surg 2008; 122: 168e–169e.
16 Chan WY, Carter LM, Wales CJ. Leechcontrol: a cheap and simple method.Ann Plast Surg 2006; 57(1): 120–1.
17 Geishauser M, Schmiedl S, KnoblochK, Vogt PM, Gohritz A. Teach the leechthe site to bite: another technical tip totame hirudo medicinalis. Plast Recon-str Surg 2009; 124(2): 671.
18 Granzow JW, Armstrong MB, PanthakiZJ. A simple method for the control ofmedicinal leeches. J Reconstr Micro-surg 2004; 20(6): 461–2.
19 Ardehali B, Hand K, Nduka C, Hol-mes A, Wood S. Delayed leech-borneinfection with Aeromonas hydrophilia inescharotic flap wound. J Plast ReconstrAesthet Surg 2006; 59(1): 94–5.
20 Whitaker IS, Kamya C, Azzopardi EA,Graf J, Kon M, Lineaweaver WC. Pre-venting infective complications follo-wing leech therapy: is practice keepingpace with current research? Microsur-gery 2009; 29(8): 619–25.
21 Haycox CL, Odland PB, Coltrera MD, Raugi GJ. Indications and com-plications of medicinal leech therapy. JAm Acad Dermatol 1995; 33(6):1053–5.
22 Felcht M, Faulhaber J, Linder AS, Go-erdt S, Koenen W. Impact of the surge-on’s experience on the postoperativeoutcome – a retrospective analysis ofnon-melanoma skin cancers of the headand neck region. J Dtsch Dermatol Ges2010; 8: 167–73.
23 Gampper TJ, Zhang F, Mofakhami NF,Morgan RF, Amiss R, Hoard MA, An-gel MF. Beneficial effect of hyperbaricoxygen on island flaps subjected to se-condary venous ischemia. Microsur-gery 2002; 22(2): 49–52.
888 Original Article Leeches in complications after plastic reconstructive surgery
JDDG | 11˙2010 (Band 8) © The Authors • Journal compilation © Blackwell Verlag GmbH, Berlin • JDDG • 1610-0379/2010/0811
Figure 4: Pathophysiological concept of venous congestion (Hydrostatic PressureCAP: hydrostatic pressure in capillaries; Effective filtration pressureCAP:effective filtration pressure in capillaries).

Copyright of Journal der Deutschen Dermatologischen Gesellschaft is the property of Wiley-Blackwell and its
content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.