june 7, 2013 surviving change in the 21 st century florida association of blood banks annual meeting...
TRANSCRIPT

June 7, 2013
Surviving Change in the 21st CenturyFlorida Association of Blood Banks Annual MeetingRichard R. Gammon, MDMedical Director

2
Learning Objectives
• Discuss past model of blood center operations
• Cover current challenges
• Give an overview of current and future opportunities

SECTION ONEPast Model of Blood Center Operations
3

Ancient Times
• Prehistoric man– Left drawings of
himself pierced by arrows
– Aware of blood– Fearful as life flowed
red out of body of animal or enemy
Cave of Lascaux
Rossi’s Principles of Transfusion Medicine. 2009

Blood has Mystical Qualities
• Romans – Fountain of youth– Medea prepares
cauldron of sacrificed black sheep
– Gives to Jason’s father Aeson
– His hair and beard…assumed the blackness of youth…limbs of vigour and robustnessBullfinch’s Mythology

Middle Ages
• 1492 Pope Innocent VIII on deathbed
• Physician used blood drawn from three boys 10 years of age to save life
• All died-no blood received

First Animal-to-Human Transfusion
• June 15, 1667 – Jean Baptiste Denis
• Blood of lamb administered to 15 year-old boy – less impurities
• Boy had fever and lethargy– Symptoms relieved
by transfusion of 9 oz of blood

Denis’ Experience
• Performed transfusions on 3 additional patients
• Number 2 survived, but 3 and 4 did not
• Patient 4 – 34 year-old Anthony du Mauroy– Experienced bouts of maniacal behavior– Transfused blood of a calf two times

The Fate of Mr. du Mauroy
• Two months later he began to experience maniacal behavior
• Wife sought transfusion therapy• Transfusion could not be accomplished and
patient died the next day• Wife tried to extort money from Denis or
threatened a malpractice lawsuit• Denis refused and an investigation was
launched

…and the Answer Is?
• Madame du Mauroy had poisoned her husband with arsenic
• Judgment April 17, 1668– Denis was exonerated– Madame du Mauroy was held for trial– Transfusion should not be performed unless
approved by the Physicians of the Parisian Faculty

1700s-Early 1800s
• Within 10 years transfusion banned from England and France
• Leeches for phlebotomy common– Contributed to death
of George Washington
Death of Washington by Howard Pyle

The Beginnings
• Early 1800s• James Blundell
– London obstetrician
• Noted frequency of death after delivery

The Beginnings
• Performed 10 transfusions– 5 were successful
• Developed devices to facilitate transfusion
• Against animal transfusions
Blundell’s Gravitator

The Victorian Era
• Media used for transfusion– Milk
• Cows• Goats• Human milk
– Abandoned when saline became available
Adler J. 1892

Era of Modern Blood Banking
• 1900– Karl Landsteiner
discovered ABO System
• 1913– Reuben Ottenberg– Describes
compatibility testing– O as “universal”
Dr. Landsteiner

Wars and Technology
• Anticoagulants– Sodium citrate -
WW I– ACD - WW II
• Indirect transfusion -- WWII– Blood collected
now – Transfused later Soldier Receives Transfusion

Wars and Technology – WW I
Battlefield Blood Bank

Transfusion WW I
Blood Brothers- L'Illustration – 11/21/1914

War and Technology-World War II
• US begins “Plasma for Britain” project
• Dr. Charles Drew heads project
• 14 million units collected by war’s end

The Rise of the Community Blood Center
• 1937 Dr. Bernard Fantus established first blood storage facility
• Cook County Hospital in Chicago
• Blood bank– Save in one place – Obtain as needed

The Rise of the Community Blood Center
• 1941 – Irwin Memorial Blood
Bank opens– First US community
blood bank

Blood Centers The Early Days
Donor Room Laboratory
Blood Centers The Early Days
23

The Creation of Components
• 1960s– Move to
component therapy/plastics
– Allows extended storage
– Multiple products from one donation

Derivative Therapy
• WW II – Cohn develops cold ethanol method of plasma fractionation– Albumin, fibrinogen, globulin become available
• Clotting factor concentrates– 1965 Pool discovered Factor VIII could be
harvested from cryoprecipitate– Hemophiliacs benefited greatly-reduced
disability

Volunteerism
• 1962– Connection made between paid donations
and posttransfusion hepatitis
• 1970– 1970 January designated as National
Volunteer Donor Month– US moves to all volunteer donor base

The 1980s
• Discovered that HIV could be transmitted in blood – 20 month infant
• Up to 1% of single-donor unit transfusions were infected with HIV
• Public confidence in blood supply at all-time low
• Concern with slow action by regulatory/professional associations

The late 20th/Early 21st Century
• Improved testing methods
• Nucleic Acid Testing Introduced – HIV (1999)– Hepatitis C (1999)– West Nile Virus (2003)– Hepatitis B (2012)

2010s
• Error reduction– Barcodes/RFID– iTrace – FDA
clearance 05/29/13
• Emerging pathogens– Hemovigilance– Pathogen Inactivation
• Cellular Therapies• Blood management
http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm354186.htm 05/13

SECTION TWO
Current Challenges

Paradigm Shift
B. Grigsby ABC Meeting 08/11
32
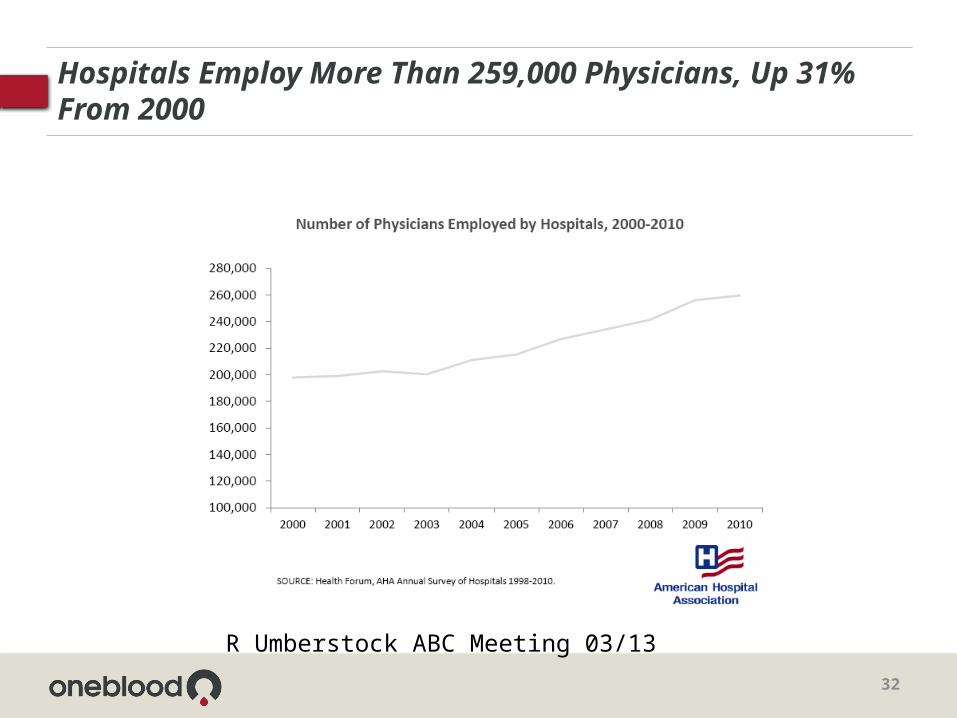
Hospitals Employ More Than 259,000 Physicians, Up 31% From 2000
R Umberstock ABC Meeting 03/13

33
Adapting to Change

34
Adapting to Change

35
More Change…

36
Affordable Care Act

37
Seizing Opportunity
Seizing Opportunity
38

39
Diversification
J Fredericks. ABC Meeting 03/12

Diversification - Transplantation
40

Diversification – Transfusion Medicine
41

SECTION THREEOpportunities – Current and Future

Role of the Blood Center
ABC Webinar 12/08/10

44
Processing Services

45
Cord Blood Processing and Banking

46
The Possibilities

47
Cumulative Stem Cell Trials Worldwide

Cell therapy companies & their products
~300 therapeutic companies with ~250 cell-based therapies in the market or in some stage of clinical development. These therapies can be roughly broken down into the following stages*:~110 Phase I ~70 Phase II~30Phase III ~40 Commercial (marketed in at least one country)
Only ~1/3 of the therapies currently marketed (~13) required and received regulatory approval. In contrast, an estimated 90% of the therapies in development are “products” requiring pre-market approval.
__________________________________________________________________________________
* Note that these numbers are limited to industry-sponsored trials and may not capture fully products in early-stage trials where industry “sponsorship” is less than transparent.
ABC Webinar 0212

Have the fundamentals changed?
• Cell therapy is here – instances of it being routine clinical practice & commercial
• There has been incremental success• CT is now very much a part of individual, corporate,
academic, policy, and financial consciousness• CT is now part of routine clinical practice and commercial
products• Emerging metrics of a maturing industry (e.g., players,
orgs, FDA, etc.)• On financial sector’s radar• Now working on second generation (not first generation)
products.
– Very little of this was true 10 year’s ago.

50
Today’s Market

51
Raw Cellular Material Collection

52
Storage and Logistics

53
Regulatory

US blood centers: strengths / opportunities
• In 2011 independent blood centers grew cell therapy business from almost nothing to ~2,000 collections in ~35 sites generating >$3M in revenue on track to do ~$6M in 2012.
• The growth to-date is exclusively from patient-donor collections.
• This market is growing rapidly

55
US blood centers: strengths/opportunities
• Other cell-based opportunities exist (more-to-less synergistic):• Custom allogeneic collections (e.g.., cells from diseased
patients)• Blood products (e.g.., plasma, etc.)• Post-collection minimal manipulation cell processing
(separation/isolation)• Collection from cell sources such as cord blood, bone marrow• Stem cell or tissue banking - cord blood, cord tissue, adult
stem cell, tissue• Manufacturing• Collection/processing of other cell sources such as adipose,
cadaveric, tissue• Technology (e.g.., device or biologic) development /
distribution• Out-patient clinics (clinical infusion)

US blood centers: advantages
• A cohesive independent blood center network:• Represents one the largest single network of collection
centers in the world• Represents the most collection centers with experience
collecting for cell therapies• Is comprised of centers staffed by personnel
accustomed to working in an environment requiring strict regulatory compliance
• ISBT128-compliant• Offers centralized contracting, training, implementation
and ongoing central support regarding customer service, data tracking, etc..
• Most commercially and technically flexible network of centers

US blood centers: weakness / threats
• Competitors are hungry for this business.
Academic centers (sourcing and manufacturing) American Red Cross (dispersed sourcing and future
manufacturing) Fresenius (dispersed sourcing (therapeutic apheresis
arm)) HemaCare (dispersed sourcing) AllCells, Inc. (sourcing – single site) Synergy BioSolutions (sourcing – single site) Key Biologics, LLC (sourcing – single site) Lonza (sourcing – single site and manufacturing) PCT (manufacturing – sourcing in future)

US blood centers: impact of healthcare trends
Increasing financial pressures on healthcare
Cell therapy is big business now Core business declining volume &
diminishing margins while novel areas represent double-digit CAGR = success will go to the nimble
Lines between blood and cells and synthetics are blurring

Key drivers to success?
• Cohesion. Centralized administration and access for customers.
• Identifying leading centers for beta implementations / R&D.
• Having and demonstrating expertise with emerging technologies / systems.
• Demonstrating commitment to being commercially flexible and service-oriented.
• Participating in the field’s leadership & executive network

60
Where Might We Go In 10 years?

61
Summary

62
Provenge - Background
Harm et al. ASFA meeting 2012

PROVENGE Processing
• Process repeated three times• Full course is typically completed in one month
63
64
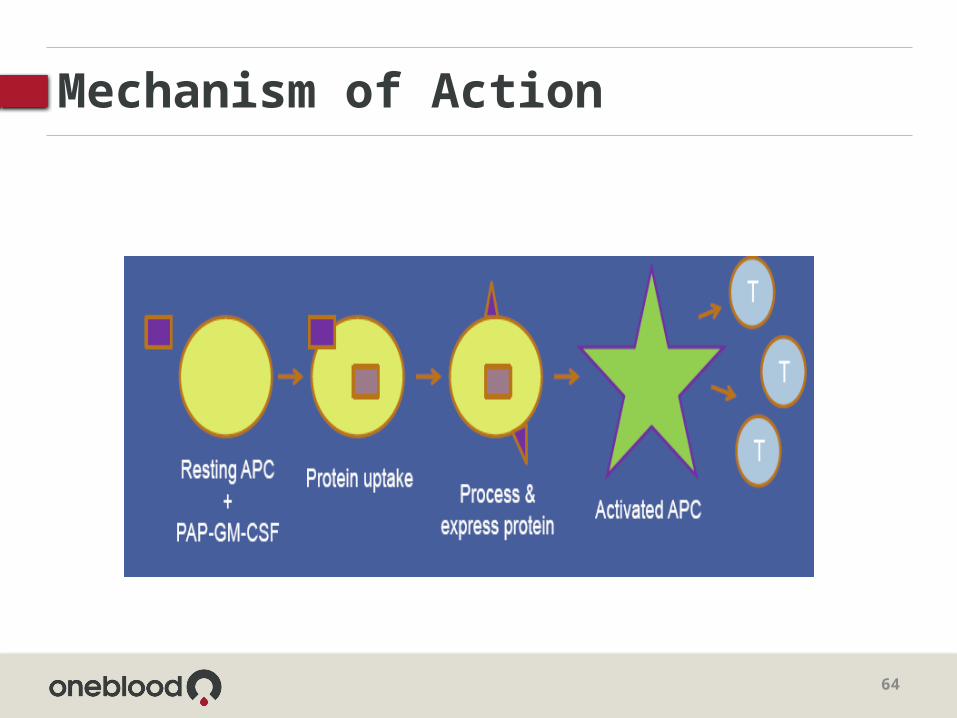
Mechanism of Action

65
Mononuclear Cell Collection

66

67
Patient Demographics

68
Results: Scheduling

69
Scheduling
70
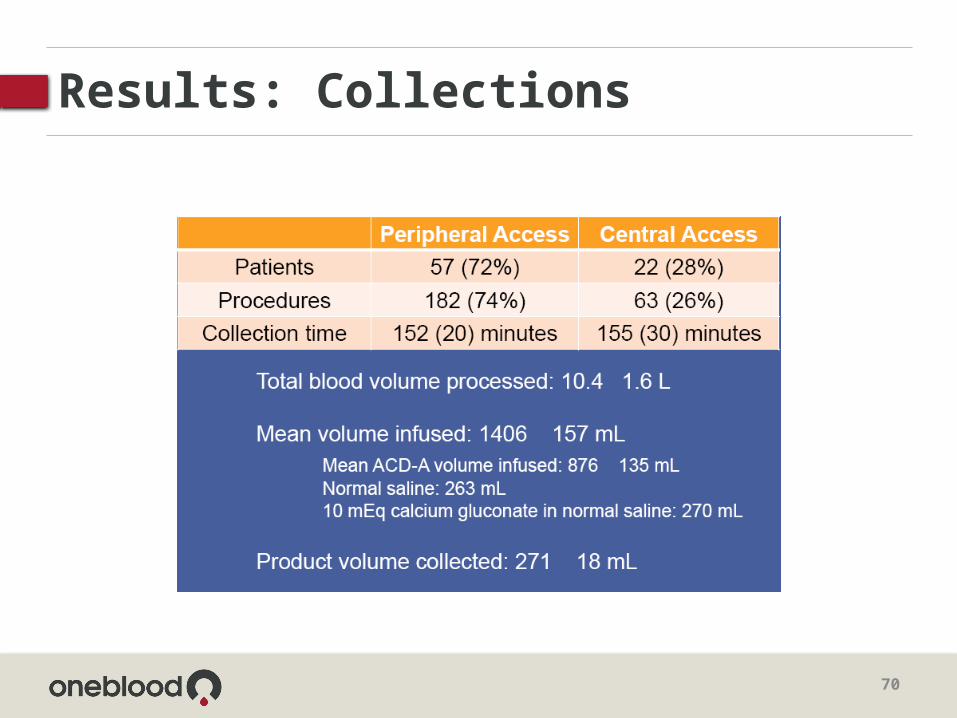
Results: Collections

71
Conclusions

Sports Medicine- Hope or Hype?
• Claims by athletes and doctors that increased popularity of PRP began winter of 2009
• Two leading football players
• Recovered quickly and went on to play in the Super Bowl
Troy Polamalu
Hines Ward
USA Today 06/29/11NY Times09/07/11

More Questions Than Answers
• Testimonials from athletes and their doctors are not credible evidence
• Most injuries eventually recover on their own, so if a patient has a treatment and then gets better, would the person have recovered at the same time anyway? Or did the treatment actually slow the healing process?
• There is no way to know without a study that compares patients who were randomly assigned to have a treatment with a matched control

Costs
• Hundreds to thousands of dollars per injection
• Fails to heal, doctors often inject again and again
• Insurers usually do not pay, so patients pay out of their own pocket

Current Studies
• Contradicting data are available in the literature with regards to PRP in wound healing
• Reported that the PRP injection in patient with Achilles tendinopathy did not result in greater improvement in pain and activity as compared to placebo injected with saline
Transfusion Medicine Reviews 2010; 24: 218-24JAMA 2010; 303: 144-49

76
Current Studies – New Zealand
• 53 adults (mean age 49, 53% men) with symptoms of unilateral mid-portion Achilles tendinopathy for at least three months.
• Participants were excluded if they had a history of previous Achilles tendon rupture or surgery or had undergone previous adjuvant treatments such as injectable therapies, glycerol trinitrate patches, or extracorporeal shockwave therapy
BMJ 2013;346:f2310 doi: 10.1136/bmj.f2310 041813

77
Results
• 26 participants were randomly assigned to the treatment group
• 27 to the control group• 50 (94%) completed the six month study,
with 25 in each group• Clear and clinically worthwhile improvements
in the VISA-A score were evident at six months in both the treatment (change in score 18.7, 95% confidence interval 12.3 to 25.1) and control (19.9, 13.6 to 26.2) groups.

78
Results
• Overall effect of treatment was not significant (P=0.689) and the 95% confidence intervals at all points precluded clinically meaningful benefit or harm
• There was no significant difference between groups in secondary outcomes or in the levels of compliance with the eccentric calf strengthening program .
• No adverse events were reported.

79
Conclusions
• The administration of two unguided peritendinous autologous blood injections one month apart, in addition to a standardized eccentric training program , provides no additional benefit in the treatment of mid-portion Achilles tendinopathy.

Current Studies
• Activity of platelet-derived factors present in PRP could depend upon– Quality of the PRP– Quality of wound– Type of wound– Physiologic conditions of the patients
(age)– Other comorbidities– Use of prescription drugs

Conclusions
• Premature to conclude that the variable results obtained using PRP are due to its inefficacy
• A large number of randomized clinical trials are essential to establish the importance and role of PRP under diverse conditions

82
Conclusions
• Clinicians and patients often want a magic bullet, and autologous blood products seem to satisfy many requirements of different parties
• They are easy to obtain and prepare, they seem to be safe and ethically and socially acceptable
• They are not doping, they are hyped by the media, and they allow large profit margins.BMJ 2013;346:f2979 doi: 10.1136/bmj.f2979 (Published 10 May 2013)

83
Conclusions
• But do they actually work? • Despite the findings of well
conducted studies that suggest that they probably do not, it seems likely that they will continue to be widely used

84
Blood Center Approach
• Could be opportunity
• Proceed with caution
• Ensure you have protocol
• Establish way to recoup costs

Other Opportunities
• Mononuclear cells for in vitro use
• HPC collection and processing– NMDP and private facilities
85
T. Foster – Webinar 04/23/13

86
Phase III Clinical Trials
• Refractory angina and chronic myocardial ischemia
• Renal cell carcinoma• Multiple sclerosis• Prostate cancer
– Similar to Provenge but with some important variations

87
Phase III Clinical Trials
• Glioblastoma• Recurrent glioblastoma• Alzheimer’s disease
– Utilize plasma exchange for treatment

88
Cell Therapy Opportunities

Blood ManagementProgram Evolution
S. Benitez- Santana. Blood Management Summit 11/10

Cost of Allogeneic Blood
Transfusion 2010; 50: 753-65

Beneficiaries of Blood Management
• Ordering of appropriate blood components
• Distribution, handling, and dispensing of blood components
• Administration of blood components• Monitoring effects of blood
components on patients
Guidelines for Patient Blood Management. AABB Press 2011

Sample Collection
• Surprisingly high proportion of pretransfusion testing specimens are mislabeled or contain blood from a patient other than the one identified on the specimen label– 1 in 165 samples being mislabeled – 1 in 1986 samples with wrong blood in tube errors
• The samples with labeling errors or omissions are 40-times more likely to be of a different ABO type than the intended recipient

Blood Administration Practice
• Institutional policies and procedures must list the steps that should be taken before the initiation of a transfusion – Physician’s order for the component and any
special instructions regarding its preparation or administration
– Informed consent– Patient identification – Unit identification (number, product type, blood
type, product modifications, and expiration date)– Confirmation of correct association of unit to
patient

Blood Administration Practice
• The risk of death as a result of mistransfusion from labeling or omission errors exceeds that of hepatitis C or human immunodeficiency virus (HIV)J. Carson. Ann Int Med 03/26/12

Blood Administration Practice
• Comprehensive “systems” approach is applied to all aspects of patient, sample, and unit identification to minimize risk of errors
• Advocate the use of routine audits to monitor the effectiveness of processes to ensure appropriate and accurate labeling and identification www.blogszebra.com 06/13

Evaluating and Reporting Adverse Effects of Transfusion
• System to track and identify trends in adverse transfusion reactions and to ensure periodic auditing of such reactions
2009 NBCUS
The Transfusion Committee
AABB Audioconference 05/19/10
Peer Review
• Assess whether deviations from the transfusion guidelines are clinically justified
• Reveal practice patterns of over- and under-use that may benefit from an intervention to improve practice

Peer Review
• May lead the transfusion committee to question whether the guidelines are appropriate or should be modified
• Effective system of detecting new problems– Any detected problems should be
reported to the transfusion committee for further exploration

One Center’s ApproachCleveland Clinic
• Noted continuing high blood product utilization – Transfusion of 2+ units of PRBCs common for
patients with Hgb>10 g/dL
• Unreliable blood product usage data– Difficult to assign blood product orders to
specific physicians to identify usage
• Implemented CPOE inpatient data (Epic)– Revised blood order practice
Parker B. Blood Management Summit 11/10
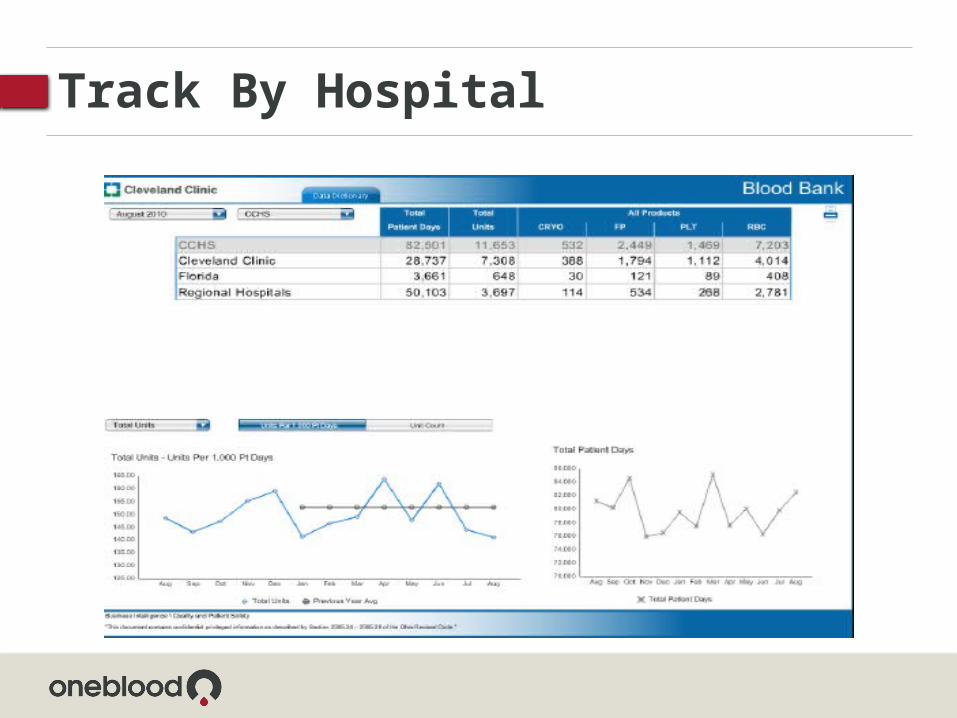
Track By Hospital

Track by Department

Track By Physician

Blood Waste Management

Wastage
• Examined and tracked • Involve a minimal
number of components• Most often involves
products with shelf-lives of 24 hours or less
• Temperature-controlled containers outside of the blood bank – Monitored for proper
storage conditions
2009 NBCUS

Conclusions
• Blood management and utilization is a comprehensive program in transfusion therapy
• Based on the concept of continuous
improvement and centered on the patient

Conclusions
• Consideration of many factors – Patient’s status– Laboratory results– Evidence-based criteria– Defined outcomes– Physician and facility history
• Key to the development of a blood management strategy
• Improves quality and advances patient safety

A Donor Center: Attracting Donors Who Do Not Wish To See Blood
Transfusion 2013; 53: 13
