journal reading 2006-10-13 present by dr. 陳志榮. the banff 97 working classification of renal...
Post on 19-Dec-2015
220 views
TRANSCRIPT
Journal Reading2006-10-13
Present by Dr.陳志榮

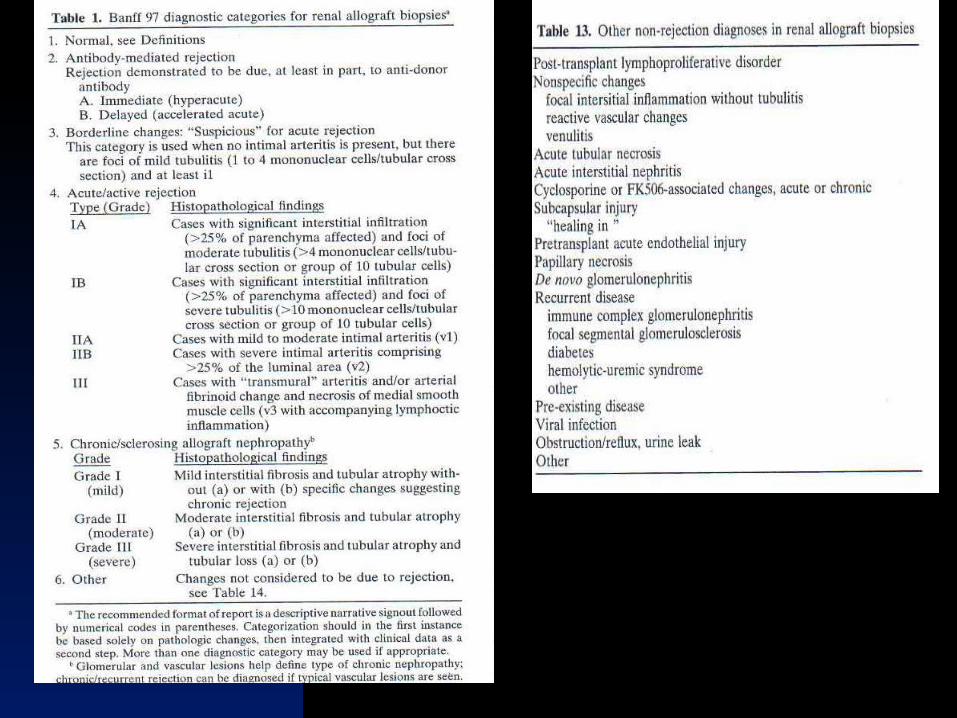
The Banff 97 Working Classification of Renal Allograft Pathology
Racusen LC, Solez K, Colvin RB, Bonsib SM, Castro MC, Cavallo T, Croker BP, Demetris AJ, Drachenberg CB, Fogo AB, Furness P, Gaber LW, Gibson IW, Glotz D, Goldberg JC, Grande J, Halloran PF, Hansen HE, Hartley B, Hayry PJ, Hill CM, Hoffman EO, Hunsicker LG, Lindblad AS, Yamaguchi Y, et al.
Johns Hopkins University School of Medicine, Baltimore, Maryland, USA. [email protected] ~ kidney International,55(2),1999, 713-23
Introduction
Standard interpretation to guide therapy and clinical trials.
Banff schema and Collaborative Clinical Trials in Transplantation (CCTT)

Method and Materials
Analysis of data using Banff classification.
Publication of and experience of the CCTT modification.
International conferences. Data from recent studies of impact
of vasculitis on transplant outcome.
Result
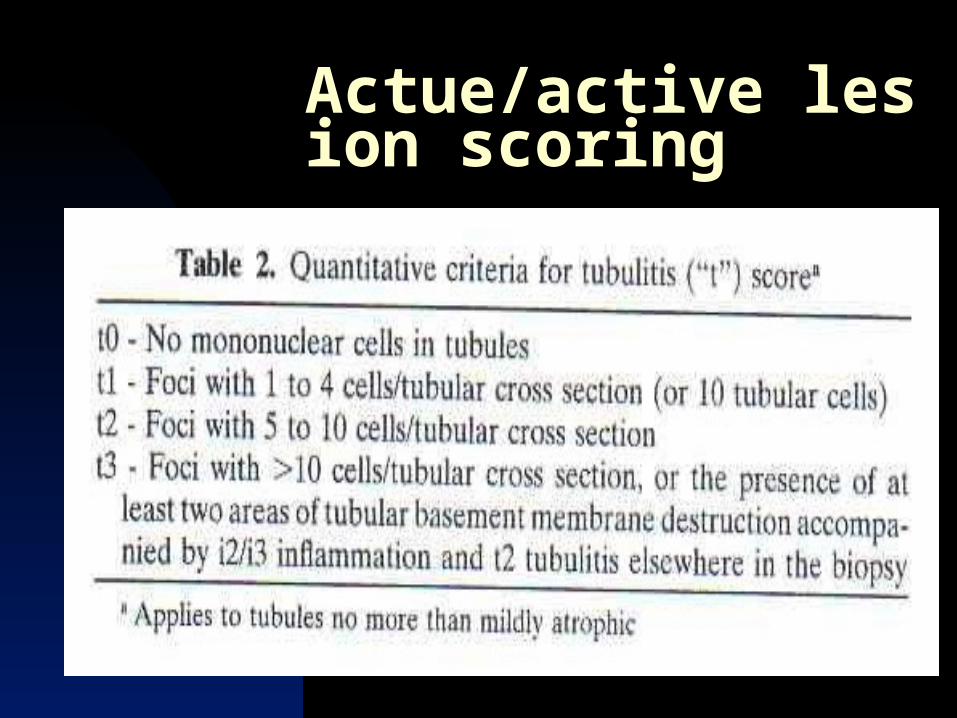
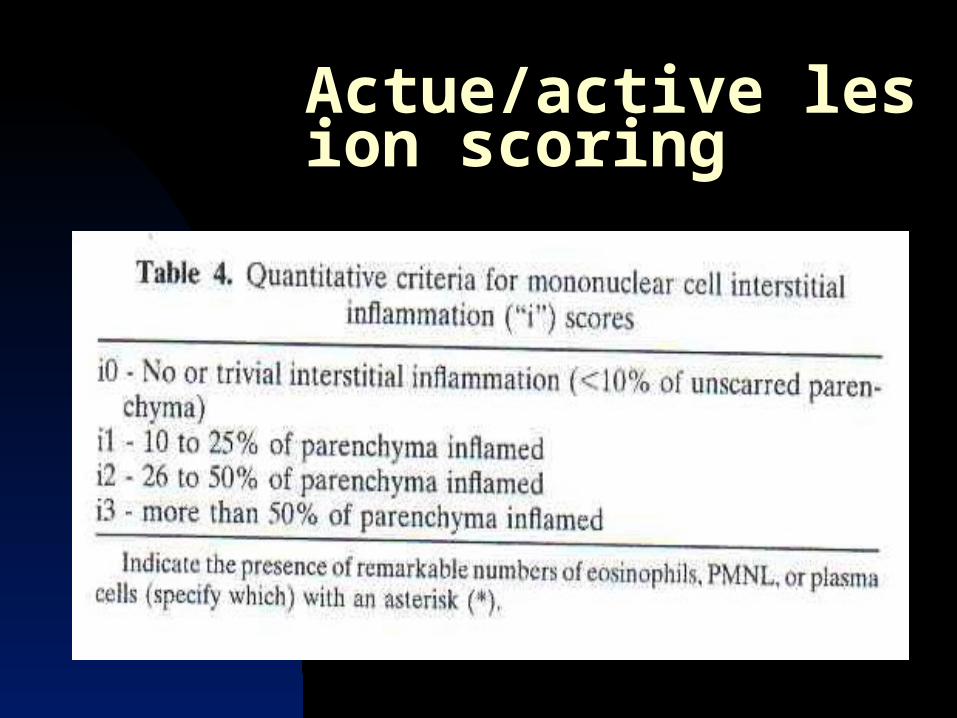
Specimen adequacy. Semiquantitative method. Actue/active lesion scoring. Tubulitis, intimal arteritis, interstitial infla
mmation, glomerulitis. Chronic/sclerosing lesion scoring. Interstitial fibrosis, tubular atrophy, allog
raft glomerulopathy, mesangial matrix increase.
Actue/active lesion scoring
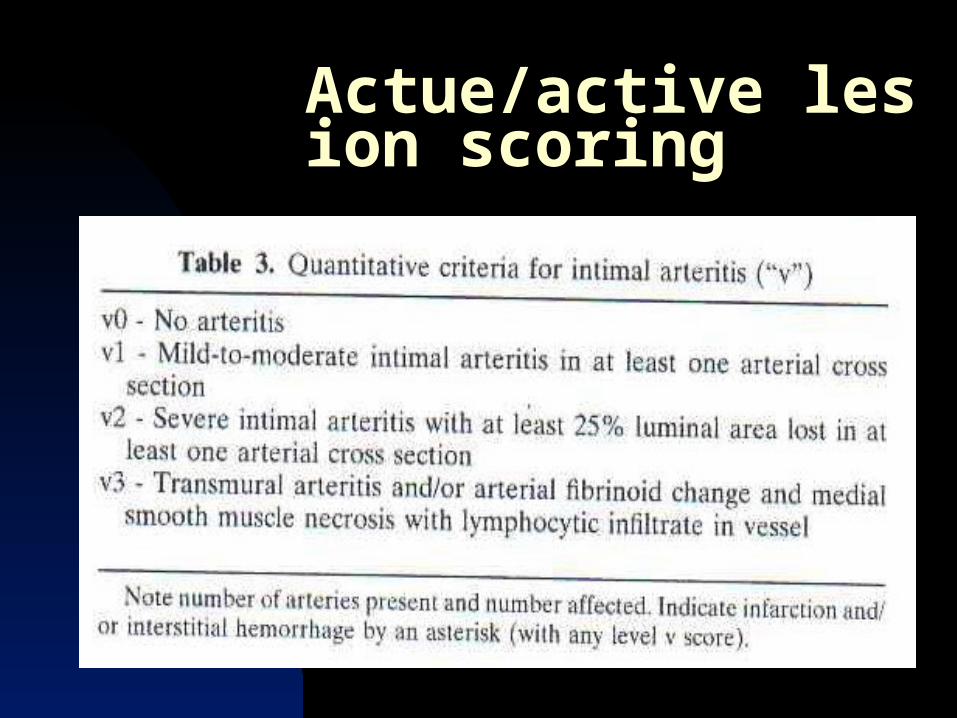
Actue/active lesion scoring Intimal artertitis:
Lymphocytic infiltration beneath the endothelium.
Arteritis: Inflammation in the media and/or
with fibrinoid necrosis of vessel wall.
Actue/active lesion scoring
Actue/active lesion scoring

Actue/active lesion scoring

Actue/active lesion scoring
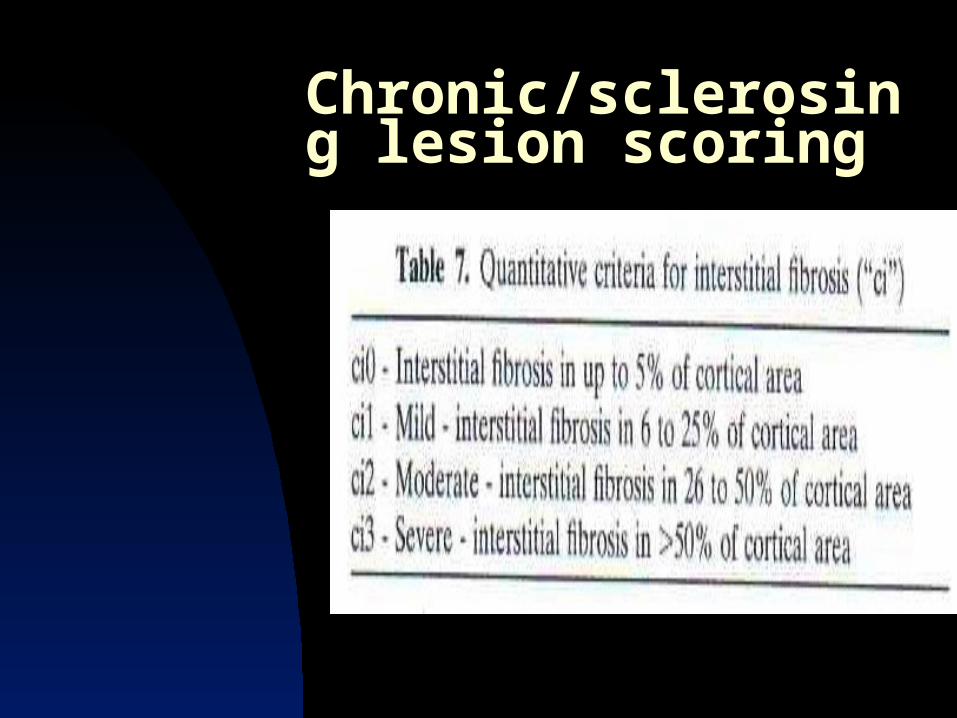
Chronic/sclerosing lesion scoring
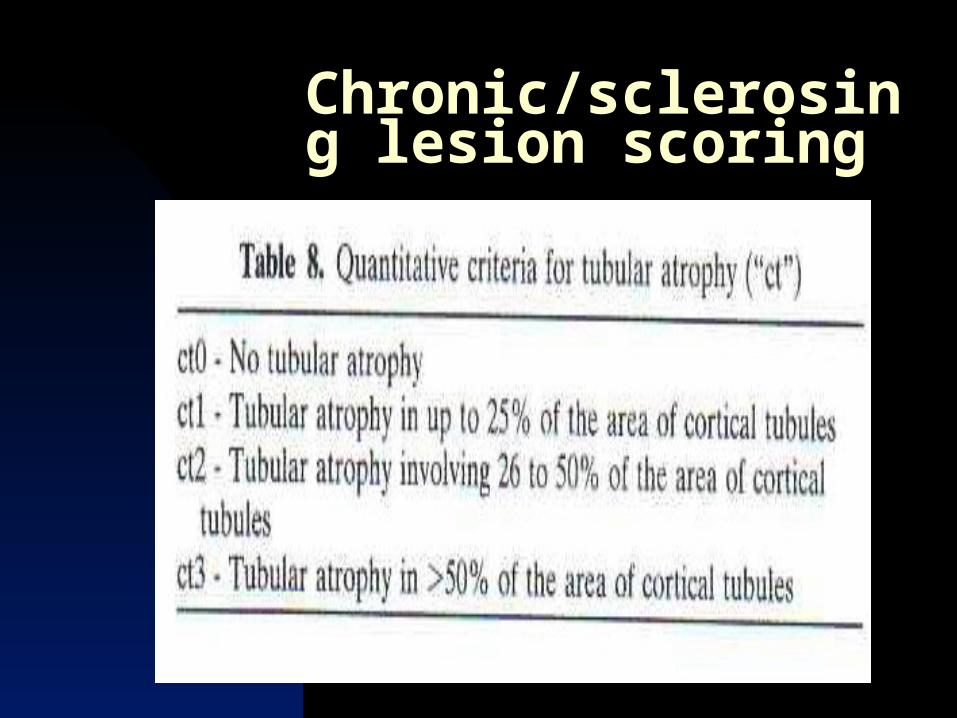
Chronic/sclerosing lesion scoring
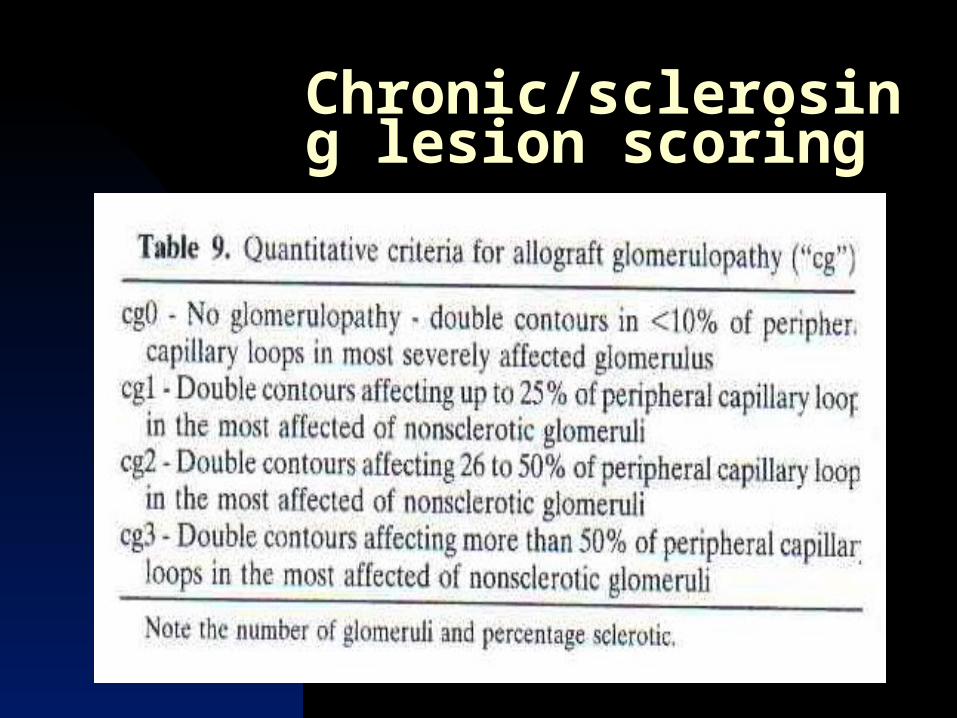
Chronic/sclerosing lesion scoring

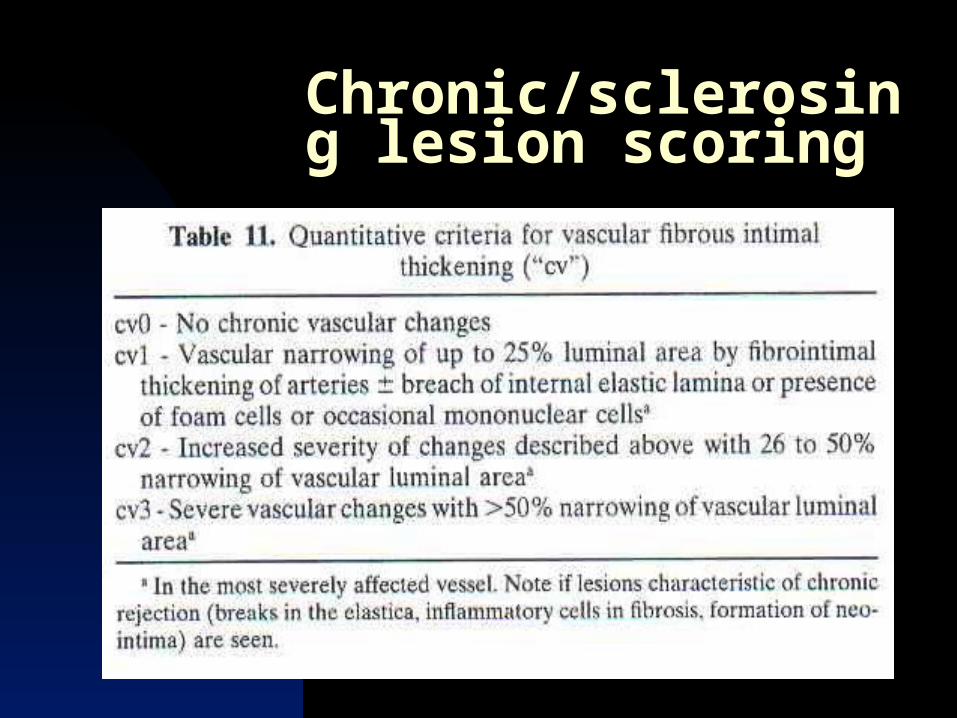
Chronic/sclerosing lesion scoring
Chronic/sclerosing lesion scoring
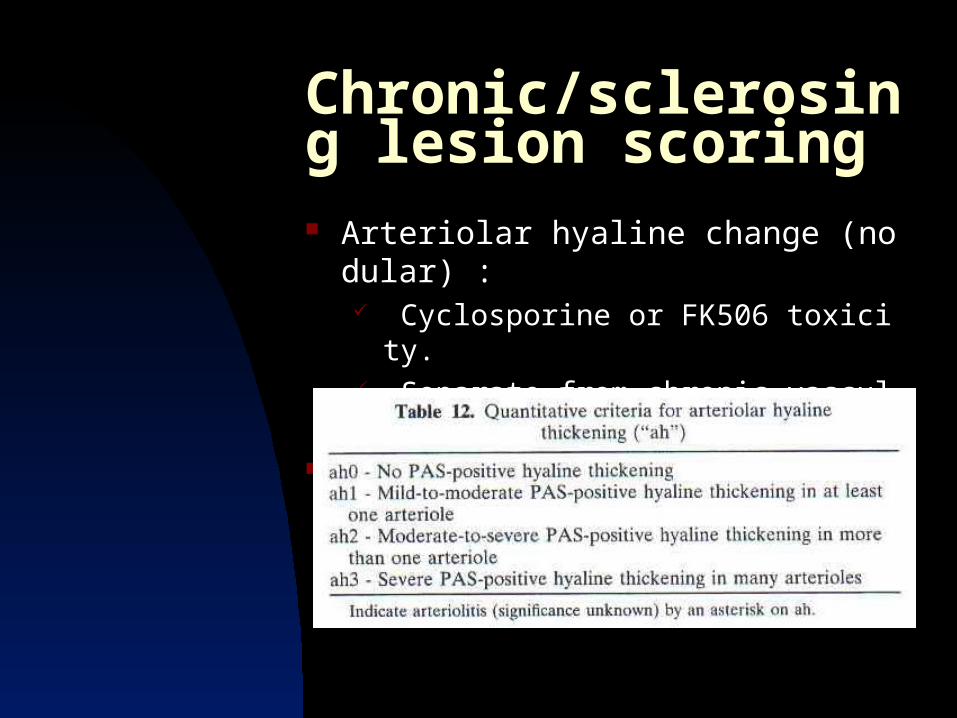
Chronic/sclerosing lesion scoring Arteriolar hyaline change (nodular) :
Cyclosporine or FK506 toxicity. Separate from chronic vascular change.
Arteriolar hyalinosis (ah) score
Discussion
Historical review Finkelstein et al.,1976 (pre-cyclosp
orine era). Banfi et al. Matas et al., 1983 Banff classification,1991 (Banff 93)
Discussion Vasculitis in renal allograft:
Poorer response to therapy and/or outcome.
Intimal arteritis ± fibrinoid necrosis. Roche mycophenolate mofetil stud
y: 87 biopsies=> allograft loss rate. Nickeleit et al: less responsive to st
eroid.

Discussion Interstitial inflammation
I2t2 for diagnosis of rejection is likely appropriate.
Rush et al.: 1/3 asmptomatic patient (subclinical rejection) had i2t2 lesions with a less than 10% change in serum creatinine but had good treatable response.
borderline rejection i1t1 i1t2=>? Significance for rejection.
Correlate with clinical finding. With decreased function=>therapay. With stable function=> no therapy.

Discussion
Antibody-mediated component Widespread endothelial injury. Fibrinoid changes of vessel wall. Glomerular and small vessel throm
boses. Infarctions. Glomerulitis. Polymorphonuclear leukocytes in p
eritubular capillaries.

Discussion Other disease processes
Polymorphonuclear leukocyte (PMNL) in interstitium and tubular lumina.
Aucte bacterial infection. PMNL in peritubular and glomerula
r capillaries. Severe acute endothelial injury and
possible antibody-mediated rejection.
Eosinphils. Hypersensitivity reaction.

Discussion
Viral infection Megalic cells, nuclear smudging, in
tranuclear or cytoplasmic inclusions.
Cytomegalovirus, polyoma virus, adenovirus etc.
Colvin: relatively severe tubular cell injury and mild inflammation raises the possibility.
Discussion
Post-transplant lymphoproliferative disorder (PTLD) Immunoblasts, plasma cell, large cl
eaved/noncleaved cells and small round lymphocyte.
Nuclear atypia, EBV association, B cell preponderant.
D/D: rejection.

Discussion
Cyclosporine Tubular vacuolization. Microvascular toxicity: glomerular
and arterioles.
Discussion
Diagnosis==>prediction of allograft function and outcome.
Early intervention. Molecular study.

How to handle the renal transplant biopsy
D’Agati, Jennette,Silva edn.Non-neoplastic kidney diseases, Atlas of non-tumor pathology, first series, fascicle 4, 2005,p668
Materials: Two cores of tissue.
focal in early stages Glomeruli: 10≧ Arteries 2≧

Processing: Majority of specimen.
Light microscopic examination. (as renal biopsy routine)
Small portion. immunofluorescence study.
EM examination. not general reserved.
Light microscopic examination Three H&E slides. Three PAS or silver stained slides.
Glomerulitis or tubulitis, arteriolar hyaline, double contours of glomerular capillaries.
One Masson trichrome stained slide.
Interstitial fibrosis. Each section:3-4 microns.
Immunofluorescence study: C4d: routine use to exclude acute
humoral rejection. ? Full panel in early transplant peri
oid. IgM, IgG, IgA, C3,C1q,fibrinogen, k
appa and lambda light chain.
Rapid processing: Same day. Formalin-fixed. Frozen section is less reliable.

Allograft renal transplant routine protocol in WanFang Hospital.

Thank you for your attention!