jc prcamio and protect trial
TRANSCRIPT
JOURNAL CLUB
15-05-2017


INTRODUCTION
• Ventricular tachycardia (VT) is a medical condition, with an extremely variable clinical presentation, from being almost asymptomatic to producing cardiac arrest.
• When the clinical condition of the patient is not compromised (i.e. blood pressure is maintained and there are no overt signs of heart failure) VT is usually referred to as ‘stable’ or ‘well tolerated’.
• Stable VT requires prompt intervention for termination because haemodynamic instability and deterioration leading to collapse can develop at any time.
• Termination can be achieved with :
electrical cardioversion,
antiarrhythmic medications,
pacing techniques.

• INTRAVENOUS PROCAINAMIDE AND AMIODARONE are drugs of choice for the treatment of haemodynamically stable VT with a class II recommendation.
• Controlled trials with amiodarone have been performed in various clinical contexts (i.e. hypotensive VT or cardiac arrest) and procainamidehas been compared with other antiarrhythmic drugs, but no controlled prospective trial have focused in comparing these two agents in well tolerated VT.
• The PROCAMIO is a multicentre, prospective and randomized study that compares the safety and efficacy of intravenous procainamide and amiodarone in the acute treatment of wide QRS complex monomorphic tachycardias (presumably VT) which are haemodynamically well tolerated.
• The majority of wide QRS complex tachycardias presenting at Emergency Departments are in fact VTs, even if the haemodynamic tolerance is acceptable. As such, the present trial refers to ‘WIDE QRS COMPLEX TACHYCARDIA (probably of ventricular origin)’ rather than to ‘VT’, assuming some uncertainty in diagnosis.

METHODS

STUDY DESIGN
• Patients were randomly assigned in an open-labelled fashion to receive either intravenous procainamide(single dose 10 mg/kg over 20 min) or intravenous amiodarone (single dose 5 mg/kg over 20 min) with a 1:1 ratio.
• The study period was 40 min from infusion initiation (20 min for drug administration and 20 min following administration).
• There was an observation period of 24 h after the end of the study period.

PATIENT SELECTION
• INCLUSION CRITERIA:a. Age ≥18 years.b. Regular wide QRS
tachycardia requiring medical attention.
c. Rate ≥120 bpm.d. Good hemodynamic
tolerance (blood pressure >90, no dyspnea at rest or angina, no hypoperfusion).
• EXCLUSION CRITERIA:a. Treatment with either
intravenous amiodarone or intravenous procainamideduring the previous 24 hours
b. Poor hemodynamic tolerance requiring urgent termination
c. Presence of irregular tachycardia.
d. Tachycardia believed to be supraventricular tachycardia
e. Contraindications to the drugs under study.

DEFINITIONS AND TREATMENTS
• MAJOR CARDIAC ADVERSE EVENTS were defined as follows:
1. Clinical signs of peripheral hypoperfusion.
2. Heart failure signs: dyspnoea at rest and/or orthopnoea associated with signs of pulmonary congestion (presence or increase of rales and/or decrease in blood oxygen saturation).
3. Severe hypotension defined as SBP≤70 mmHg if the pre-treatment SBP was ≤100 mmHg or SBP≤80 mmHg if the pre-treatment SBP was > 100 mmHg.
4. Tachycardia acceleration of >20 bpm of its mean value.
5. Appearance of fast polymorphic VT.
• Drug infusion was stopped by protocol if any of the following occurred:
(i) termination of the tachycardia during the infusion period;
(ii) complete administration of the amount of drug programmed; and
(iii) presence of a major cardiac adverse event.
Response to treatment was evaluated as follows:
1. Termination was defined as conversion to the patient’s known or presumed usual heart rhythm (e.g. sinus, atrial fibrillation) within the study period.
2. If the tachycardia terminated within 20 min of drug infusion initiation and recurred within 20 min following infusion ending, then the treatment was considered unsuccessful.
STUDY ENDPOINTS
• The primary endpoint of the study was to compare the incidence of major cardiac adverse events between both treatments.
• Secondary endpoints were the following:
(i) to compare the efficacy of both drugs in relation to the acute termination of the tachycardia episode.
(ii) to compare the incidence of total adverse events during the observation period.

SAMPLE SIZE CALCULATIONS
• The sample size calculation for this study had significant uncertainties.
• There was only one randomized trial with intravenous procainamide in tolerated VT, with considerable adverse events and observational studies with small number of patients had reported extremely good tolerance of intravenous amiodaroneso it was hypothesized by investigators 20% and 5% adverse event rate in the procainamide and amiodarone groups.

• Based on these assumptions, 302 patients were needed to detect a difference of 15% in major adverse events between both groups
• After nearly 6 years including patients at 2 participating Centres, 74 patients had been randomized and a trend towards a decrease in inclusion rate was observed.

STATISTICAL ANALYSIS
• Summary statistics for continuous variables was recorded as means and standard deviations, as well as medians.
• Comparisons between the two treatment groups were performed with the Wilcoxon rank-sum test.

RESULTS

Summary of patient recruitment and results.


PRIMARY END POINTS


Odds ratio and confidence intervals of adverse eventsand tachycardia termination of procainamide patients compared
with amiodarone patients. AE, adverse events; MCAE, major cardiacadverse events; SP, study period (40 min); OP, observation
period (24 h).

SECONDARY END POINTS

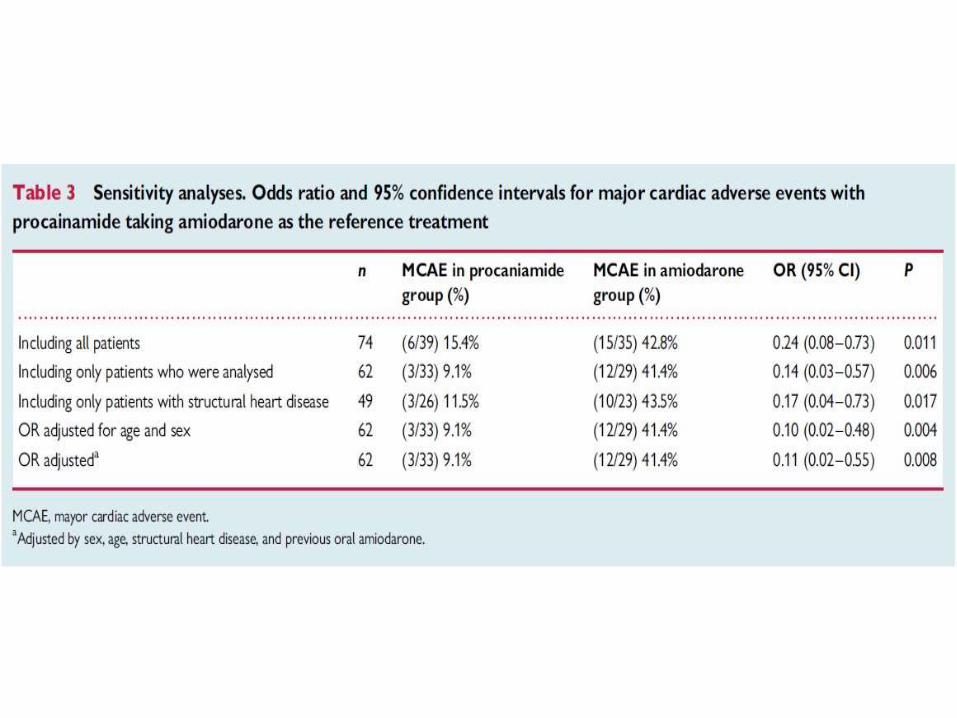
SUBGROUP ANALYSIS IN PATIENTS WITHSTRUCTURAL HEART DISEASE

DISCUSSION
• This study shows for the first time in a randomized controlled trial that when iv procainamide and amiodarone, at usual clinical doses, are compared for the acute treatment of spontaneous episodes of well-tolerated wide QRS complex tachycardias, presumably VT:
Procainamide is associated with less major cardiac adverse events;
Procainamide is more efficacious in terminating the tachycardia episode;
Findings equally apply to the subgroup of patients with structural heart disease.

COMPARISON WITH PREVIOUS AVAILABLEINFORMATION
• In one study which compared procainamide and amiodaronein a retrospective multicentre historical cohort trial in 90 patients, amiodarone caused severe hypotension requiring emergency electrical cardioversion in 6%.
• One additional series which used intravenous amiodaronewas a retrospective single cohort analysis which identified 41 patients that received 300 mg, severe hypotension requiring emergency electrical cardioversion occurred in 7/41 cases (17%).

• But in this study - 41% major cardiac adverse events in the amiodarone arm.
• Possible explanation can be that in this study symptoms were prespecified and levels of hypotension were considered a major event, whereas in retrospective trials major adverse events were recognized by the need of electrical cardioversion.
• Retrospective nature of these studies posed limitations too.
47 patients (52%) in one study had received anotherantiarrhythmic drug and the mean dose was 2.0 mg/kg in patients in whom amiodarone was ineffective, smaller than the 5 mg/kg used in this trial;
In another study the duration of the drug infusion lasted up to 60 min.

• Retrospective nature of these studies posed limitations too.
47 patients (52%) in one study had received anotherantiarrhythmic drug and the mean dose was 2.0 mg/kg in patients in whom amiodarone was ineffective, smaller than the 5 mg/kg used in this trial;
In another study the duration of the drug infusion lasted up to 60 min.
• The information regarding procainamide for the acute termination of spontaneous well-tolerated sustained VT is even more limited.
• In various retrospective studies, major cardiac adverse events occurred in 13% and 17% while in this study it was 9%.
• Efficacy was reported in 76% and 57% in retrospective studies and in 80% in a prospective study which is consistent with the figure of 67% VT termination in this study.

SELECTEDDOSAGES AND ADMINISTRATION
• The duration of infusion chosen was 20 min.
• Dose of amiodarone was 5 mg/kg infused during 20 min, approximating 300 mg.
• Dose of procainamide 10 mg/kg infused over 20 min.

UNEXPECTED FINDINGS?
• Investigators did not expect such a high incidence of major adverse effects in the amiodarone arm since in the various studies e.g by Leak et al reported on using a bolus of 150 mg of amiodarone in 11 critically ill patients and stated that ‘hypotension, cardiac failure and bradyarrhythmias were not induced by this treatment’.
• Similarly, in severely hypotensive recurrent VT, amiodaroneproduced less hypotension than bretilium in another study.
• So investigators hypothesized that if amiodarone was safe in these very sick patients it was going to be so in the stable patientwith tolerated VT.
• But ,in retrospect, some findings can explain results:
When the arrhythmia is immediately life threatening, an antiarrhythmic action can produce such a benefit that overcomes potential adverse effects.
In studies performed during resuscitation all patients had previously received intravenous catecolamines(adrenaline).
In critically ill patients most were receiving catecolamines: these drugs may have counteracted the hypotensive effects of amiodarone.

LIMITATIONS
1. The study included less number of patients that were required according to sample size calculations since ;
a. Extension of emergency protocols to treat these patients on the ambulance; in these protocols only amiodarone was allowed, precluding participation in the trial;
b. Fast turnover of medical personnel at emergency departments.
2. The study design was randomized but not blinded.

CONCLUSIONS
• In this randomized prospective study comparing intravenous procainamide and amiodarone for the treatment of the acute episode of sustained monomorphic well-tolerated wide QRS tachycardia (probably VT), procainamide therapy was associated with less major cardiac adverse events and a higher proportion of tachycardia termination within 40 min.

• Left anterior descending (LAD) artery supplies 45% to 55% of the left ventricle mass.
• Therefore, patients with LAD disease are thought to be at higher risk for future cardiovascular events.
• Location of the lesion in the proximal LAD identifies a higher risk subset of patients in whom the need for, and the method of, revascularization should be further discussed.

• The data comparing outcomes after revascularization for proximal LAD versus nonproximal LAD are limited.
• It is not well understood whether the presence of LAD narrowings requiring revascularization still remains today a predictor of adverse outcome after percutaneous coronary intervention (PCI) with a drug-eluting stent (DES) and with current medical therapy.
• Therefore, investigators aimed to compare long-term outcomes in patients with or without target lesions in the proximal LAD.

• Investigators analyzed the 4-year outcomes in 8,709 patients who underwent coronary artery stenting in PROTECT (Patient Related Outcomes with EndeavorVersus Cypher Stenting Trial), classified according to lesion location within or outside the proximal LAD.

METHODS
• PROTECT was an open-label, multicenter trial that randomized patients undergoing elective, unplanned, or emergency procedures in native coronary arteries to the Endeavor zotarolimus-eluting stent (E-ZES) or the Cypher sirolimus-eluting stent (C-SES)
• The trial involved 196 participating hospitals in 36 countries across 5 continents and was conducted between May 21, 2007, and December 22, 2008.
• The present study included all patients from the PROTECT trial and compared the cohort of patients who received at least 1 stent in the proximal LAD with those who received stents only in nonproximalLAD locations.
• Proximal LAD was defined according to the Coronary Artery Surgery Study classification : end of left main to the first large septal or first diagonal, whichever is most proximal.
PROCEDURE
• Antiplatelet therapy with aspirin and clopidogrel (75 mg) or another thienopyridine derivative was started 3 days before the procedure or through a loading dose (clopidogrel 300 to 600 mg or its equivalent for other thienopyridine) for patients not yet taking these medications.
• During the procedure, 96.7% of patients were treated with clopidogrel, 0.27% were treated with ticlopidine, and 5.72%received another antiplatelet/antithrombin drug.
• Post-procedure, aspirin was prescribed indefinitely, and thienopyridine therapy was prescribed for a minimum of 3 months and up to 12 months , or for longer at the physician’s discretion.

DEFINITIONS
• Major adverse cardiac events (MACE) included all-cause death, MI (Q-wave and non–Qwave), emergent coronary artery bypass graft (CABG) surgery, or repeat clinically indicated target lesion percutaneous or surgical revascularization.
• Target vessel failure (TVF) included death, target vessel MI (Q-wave and non–Q-wave), or clinically driven target vessel revascularization by percutaneous or surgical methods.
• Target lesion failure included death from cardiac causes, target vessel MI,and target lesion revascularization.

• Patients were defined as “complex” if they met at least 1 of the following clinical or lesion characteristics:
1. Renal insufficiency or failure (defined as creatinine ≥140 mmol/l [1.6 mg/dl]),
2. Left ventricular ejection fraction <30%, the occurrence of an acuteMI within the previous 72 h,
3. >1 lesion per vessel,
4. ≥2 vessels with stents,
5. Lesion measuring >27 mm,
6. Bifurcation,
7. Bypass grafts,
8. In-stent restenosis,
9. Unprotected left main artery,
10. Lesions with thrombus, or total occlusion (pre-procedure TIMI [Thrombolysis In Myocardial Infarction] flow grade 0).

STATISTICAL ANALYSIS.
• Dichotomous and categorical variables were reported as counts and percentage.
• Continuous variables were reported as mean SD and were compared with a 2-sample Student t test.
• All analyses were performed according to the intention-to-treat principle in the entire enrolled study population.
• The incidence of clinical outcomes was calculated using the Kaplan-Meier method and compared using the log-rank test

RESULTS





4-YEAR CUMULATIVE INCIDENCE OF EVENTS STRATIFIED BY PROXIMAL LAD PATIENTS VERSUS NONPROXIMAL LAD
Based on Kaplan-Meier analysis: (A) major adverse cardiac events (MACE); (B) cardiac death; (C) target vessel failure (TVF); (D) stent thrombosis; CI ¼ confidence
interval; HR ¼ hazard ratio; LAD ¼ left anterior descending.

4-YEAR CUMULATIVE INCIDENCE OF EVENTS STRATIFIED BY PROXIMAL LAD PATIENTS VERSUS NONPROXIMAL LAD
Based on Kaplan-Meier analysis: (A) major adverse cardiac events (MACE); (B) cardiac death; (C) target vessel failure (TVF); (D) stent thrombosis; CI ¼ confidence
interval; HR ¼ hazard ratio; LAD ¼ left anterior descending.

DISCUSSION
• In this prospective, multinational, multicenter, randomized study with DES for single-vessel and multivessel disease, there was no difference in the rates of death, MACE, or TVF at 4 years according to intervention at a proximal LAD or nonproximal LAD lesion site.
• The occurrence of the predefined primary endpoint—namely, stent thrombosis—was not dependent on whether a proximal LAD or nonproximal LAD site was treated with a DES.
• However, stenting of proximal LAD lesions was associated with significantly higher rates of MI compared with stenting of nonproximal LAD lesions.

• Results are consistent with an analysis of the COURAGE (Clinical Outcomes Utilizing Revascularization and Aggressive DruG Evaluation) trial, in which disease in the proximal LAD did not influence death or MI.
• Two relatively large meta-analyses examining the method of revascularization of the proximal LAD location have not shown differences in mortality, MI, or stroke between PCI and CABG

• These studies which were followed for 4 and 5 years respectively used bare metal stents in the PCI arm and demonstrated a 3-fold increase in recurrent angina and a 5-fold increase in repeat revascularization with PCI as compared with CABG.
• In the metaanalysis performed by Kapoor et al. , the 5-year repeat revascularization rate of patients undergoing CABG for isolated proximal LAD disease was 7.3% at 5 years, compared with 33.5% in their PCI arm, whereas in the current study the TVF rate was 14.8% at 4 years
• There are no randomized studies comparing the long-term outcomes of PCI with CABG for isolated proximal LAD lesions.
• Hannan et al. examined the New York Percutaneous Coronary Interventions Reporting System for patients who underwent CABG surgery and received DES for isolated proximal LAD disease.
• Among 715 of 5,340 patients (13.4%), they reported no differences in mortality or in a combination of mortality, MI, and/or stroke using propensity-matched comparisons; however, CABG patients had significantly lower repeat revascularization rates.

• This study is a post hoc, nonrandomized comparison; all patients underwent PCI and no patient underwent CABG.
• Yet investigators found that outcomes in >2,500 patients treated with DES in the proximal LAD were similar to the outcomes of >6,100 patients with lesions in other coronary arteries, which currently are treated ad hoc and do not require further discussion before decision and intervention

STUDY LIMITATIONS
• The comparison of patients with and without a proximal LAD target lesion was a post hoc analysis.
• Investigators could not exclude the presence of unmeasured selection bias.
• There are several known and unknown confounders with significant impact on the endpoints, and even sophisticated statistical methods cannot eliminate potential selection bias.
• Investigators do not have information regarding heart failure and quality of life, as an event in the proximal LAD may be associated with greater myocardial damage than one in other coronary artery locations.

CONCLUSIONS
• The discussion of how best to treat the patient with a proximal LAD lesion remains a topic of debate .
• In the present study, investigators found that long-term outcomes for MACE, mortality, and TVF were similar regardless of whether the target lesion was in the proximal LAD or not.
• The nonsignificant interaction between stent type (E-ZES vs. C-SES) and lesion location (proximal LAD vs. nonproximal LAD) suggests that these results are independent of stent type.
• This finding may suggest that proximal LAD lesion may not confer a substantial additional risk in the DES era.

• WHAT IS KNOWN? Proximal LAD artery involvement significantly impacts the recommendations for revascularization.
• WHAT IS NEW? In patients treated with drug eluting stents in the proximal LAD, the 4-year event rate was similar to patients treated in other coronary artery tree locations.
• WHAT IS NEXT? In the DES era, proximal LAD no longer confers a different prognosis than other lesion sites.