ivp interpretation dr. jaturat kanpittaya. introduction ivp has long been cornerstone of imaging ivp...
TRANSCRIPT
IVP IVP INTERPRETATIONINTERPRETATION
Dr. Jaturat Kanpittaya Dr. Jaturat Kanpittaya
Introduction Introduction • IVP has long been IVP has long been cornerstonecornerstone of imaging of imaging
evaluation of urinary tract disease evaluation of urinary tract disease
• Global , Global , importantimportant in diagnosis of KUB in diagnosis of KUB diseasedisease
• Evaluation in hematuria , stone disease , Evaluation in hematuria , stone disease ,
post therapeutic evaluation of stone post therapeutic evaluation of stone
• Good technique , Good technique , understanding limitationunderstanding limitation , ,
basic rule of interpretation basic rule of interpretation
• Relate with other imaging modality Relate with other imaging modality
U/S , CT , MRI U/S , CT , MRI
Contrast materialContrast material
•Excrete by glomerular Excrete by glomerular filtration filtration
•Concentration in the Concentration in the postglomerular nephron postglomerular nephron
and progressive and progressive opacification opacification
Of the urinary tract Of the urinary tract
Standard procedure for IVPStandard procedure for IVP• Scout film ( technique 65-75 kVp , level )Scout film ( technique 65-75 kVp , level )
• NephrotomogramNephrotomogram (1-3 min film ) (1-3 min film )
• 5 min KUB film 5 min KUB film
• Abdominal compression Abdominal compression
• PyelographicPyelographic image ( 10 min film )image ( 10 min film )
• Ureter-bladderUreter-bladder image image
( release compression , 15 min film , ( release compression , 15 min film ,
supine , prone , oblique , upright )supine , prone , oblique , upright )
• BladderBladder image ( delay , oblique , post image ( delay , oblique , post void ) void )
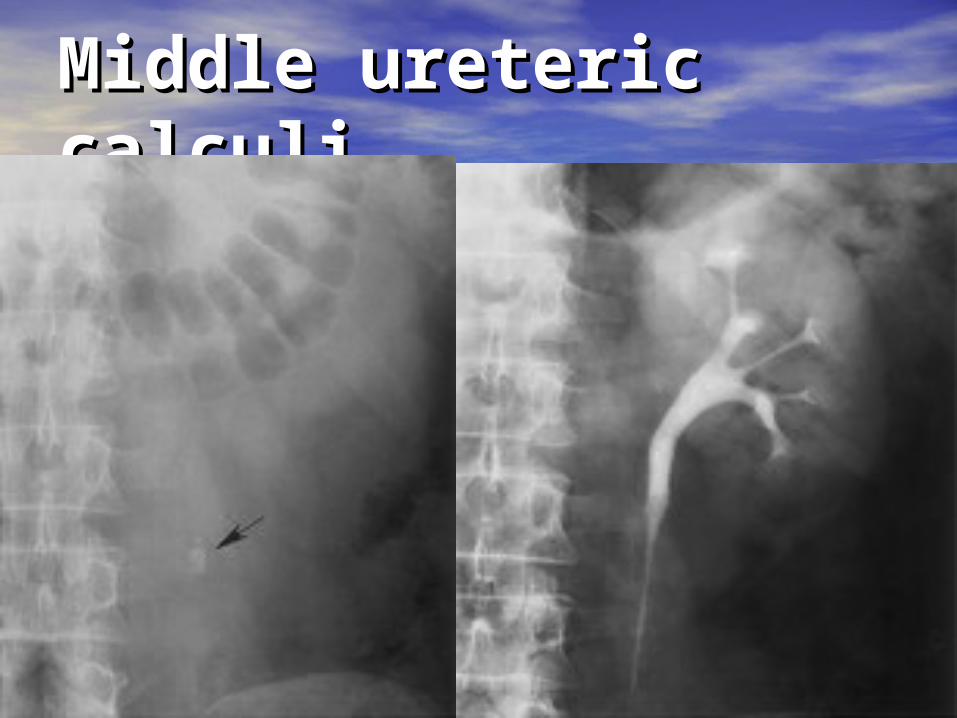
Middle ureteric Middle ureteric calculicalculi
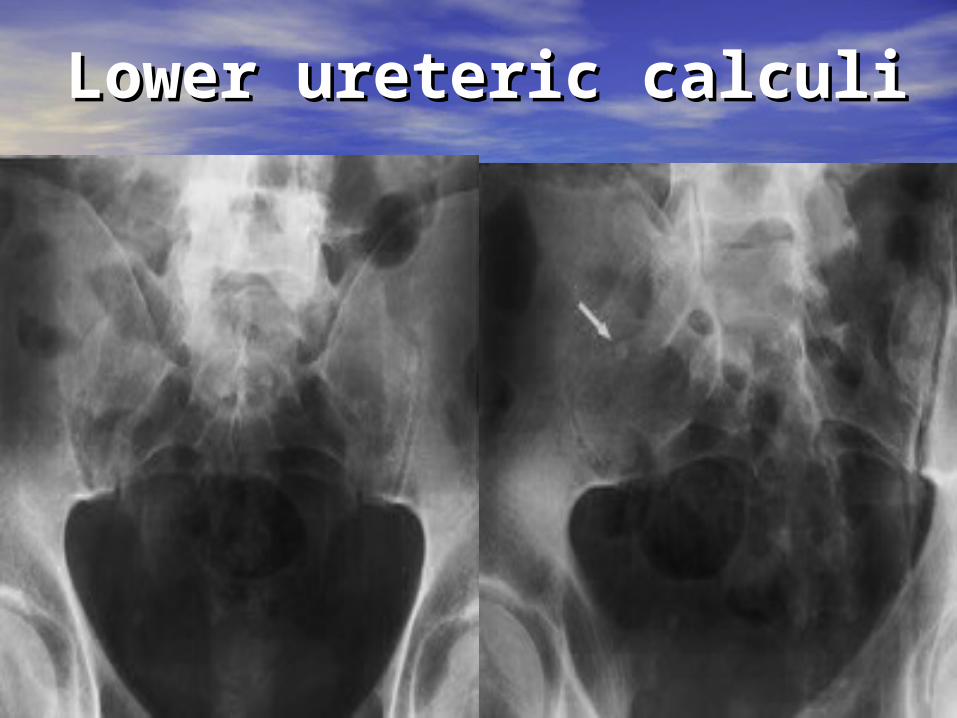
Lower ureteric calculiLower ureteric calculi
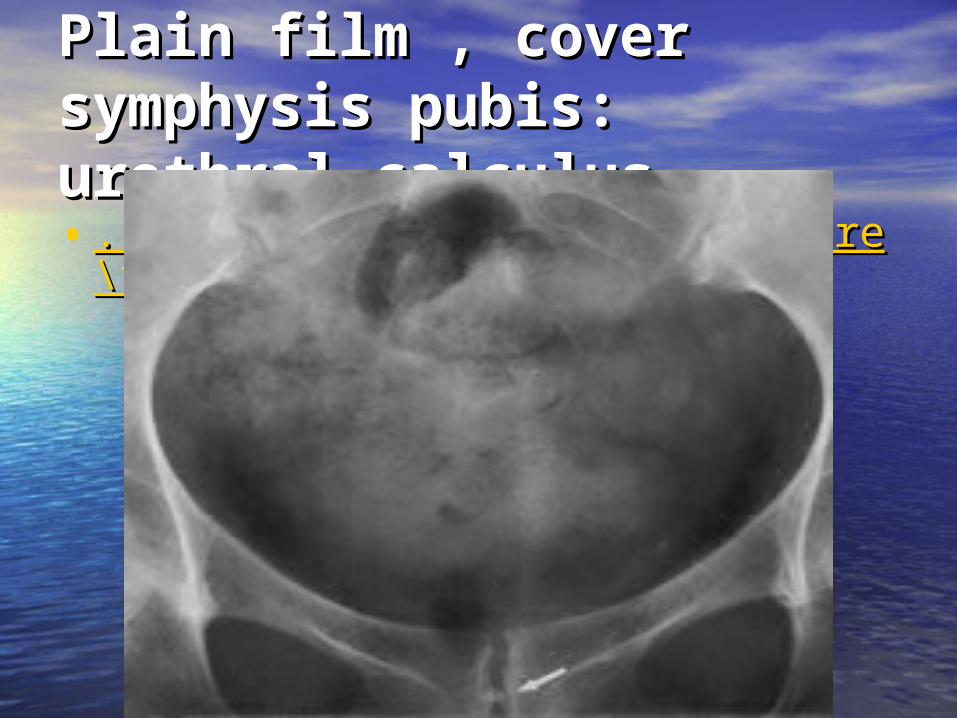
Plain film , cover Plain film , cover symphysis pubis: symphysis pubis: urethral calculusurethral calculus • ..\Intravenous Urography\Figure\f1.gif..\Intravenous Urography\Figure\f1.gif
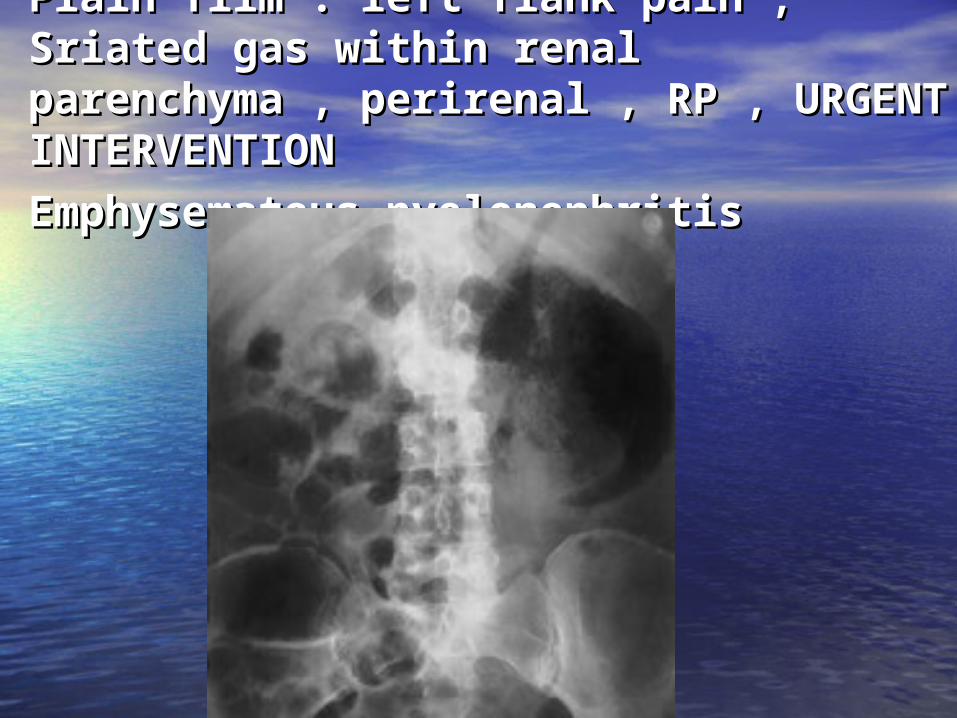
Plain film : left flank pain ,Plain film : left flank pain ,Sriated gas within renal parenchyma , Sriated gas within renal parenchyma , perirenal , RP , URGENT perirenal , RP , URGENT INTERVENTIONINTERVENTION
Emphysematous pyelonephritisEmphysematous pyelonephritis
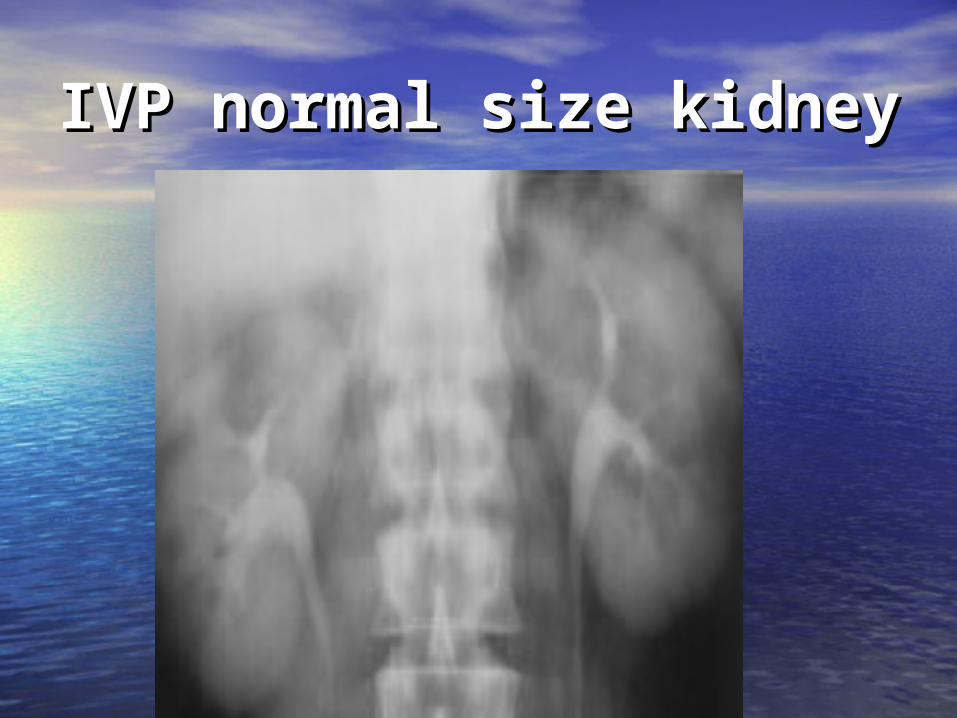
IVP normal size kidneyIVP normal size kidney
Abdominal compression Abdominal compression • Optimal evaluation of ureter and Optimal evaluation of ureter and
pelvicalyceal system , distension of pelvicalyceal system , distension of collecting system collecting system
• Contraindication; Contraindication; *Presence of obstruction *Presence of obstruction *Abdominal aortic aneurysm *Abdominal aortic aneurysm *Abdominal mass *Abdominal mass *Recent abdominal surgery *Recent abdominal surgery *Severe abdominal pain *Severe abdominal pain *Suspected of urinary tract trauma *Suspected of urinary tract trauma *Urinary diversion or renal transplant*Urinary diversion or renal transplant
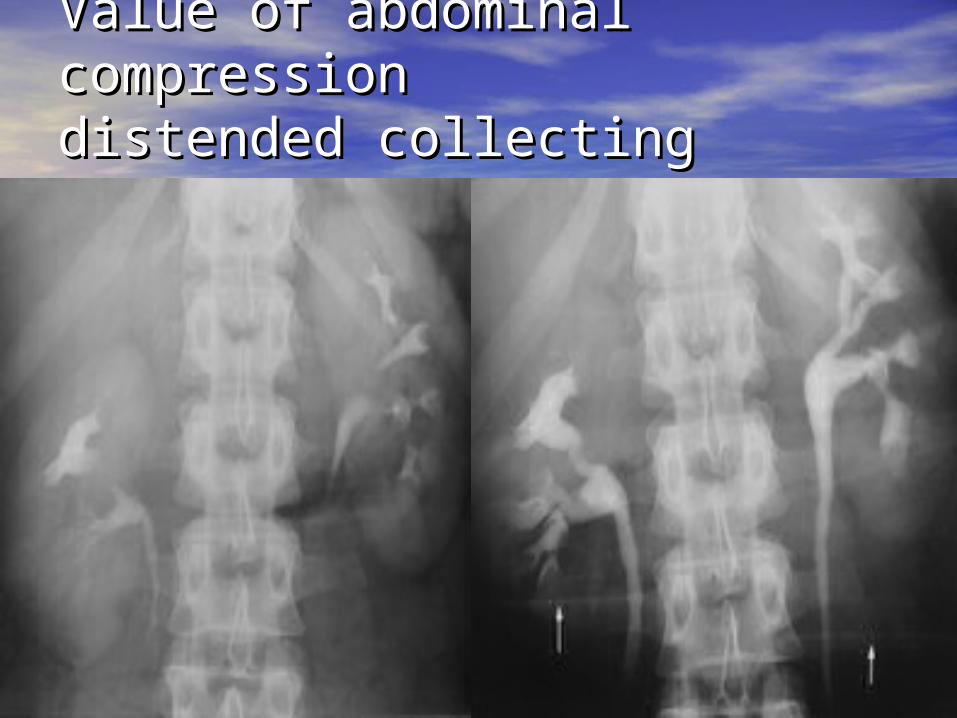
Value of abdominal Value of abdominal compressioncompressiondistended collecting system distended collecting system
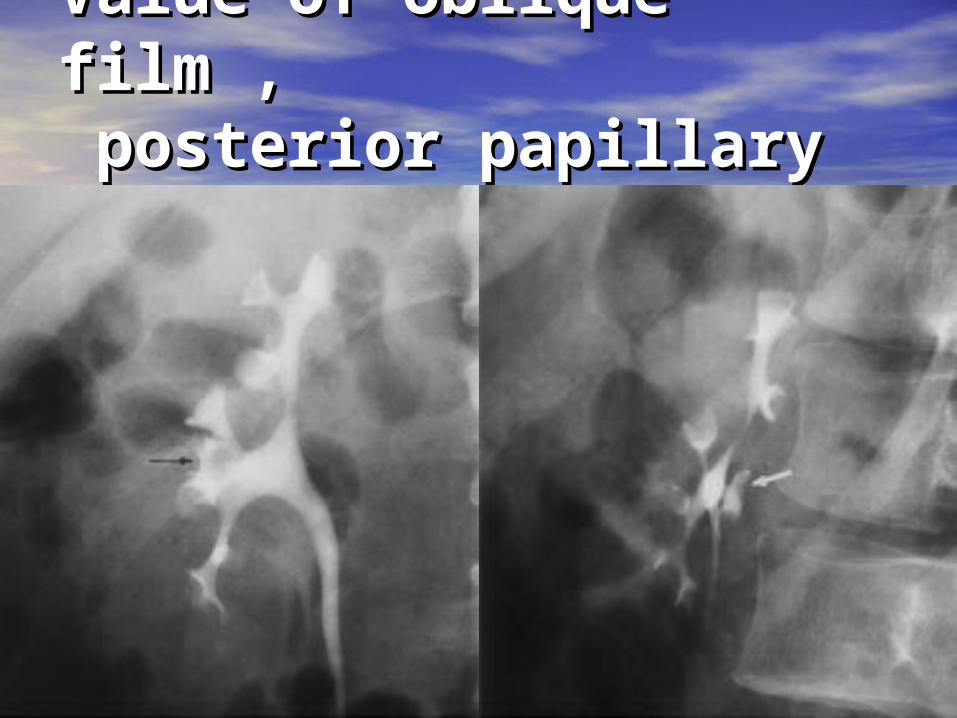
Value of oblique film ,Value of oblique film , posterior papillary tip posterior papillary tip
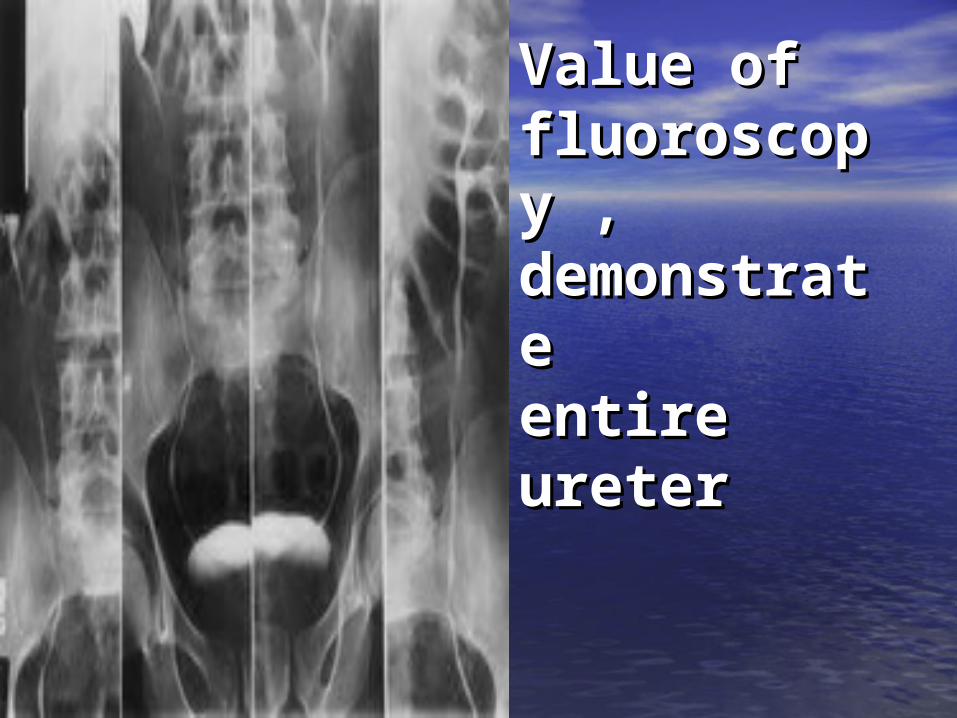
Value of Value of fluoroscopfluoroscopy , y , demonstrademonstrate te entire entire ureterureter
Bladder imageBladder image
•Distend and opacity , oblique Distend and opacity , oblique image , evaluate bladder image , evaluate bladder disease disease
•Post void image may be useful Post void image may be useful
for evaluate filling defect for evaluate filling defect
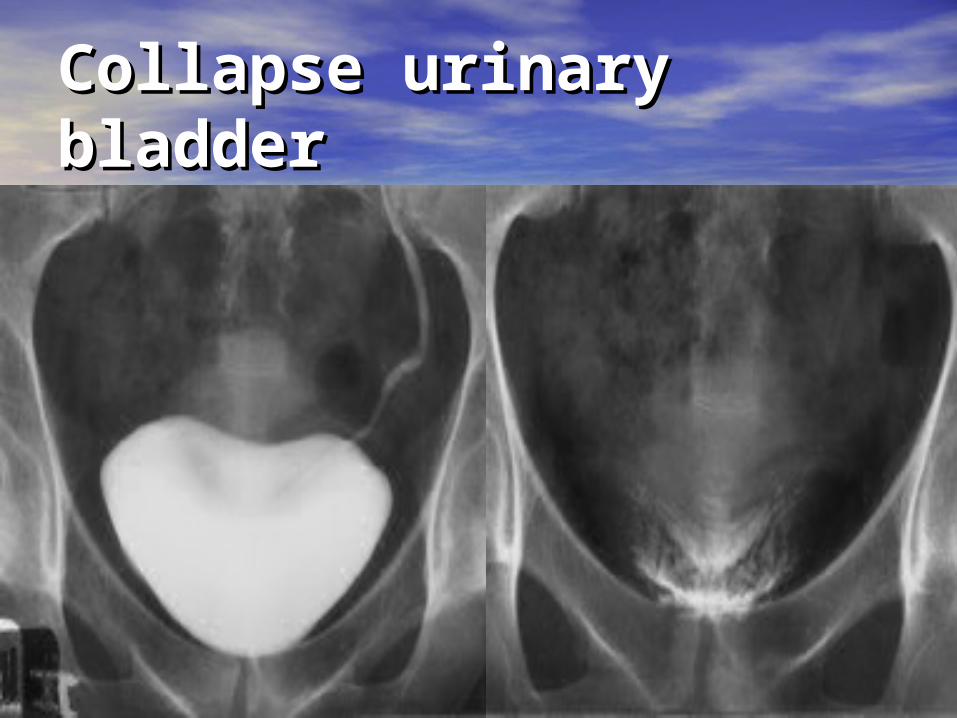
Collapse urinary Collapse urinary bladderbladder
Urographic interpretationUrographic interpretation
• Nephrotomographic phaseNephrotomographic phase; ;
Evaluate renal parenchyma , smooth Evaluate renal parenchyma , smooth contour, contour,
renal size ( 9-13 cm )renal size ( 9-13 cm )
• Pyelographic and ureteric imagePyelographic and ureteric image; ;
Evaluate renal collecting system Evaluate renal collecting system
• Bladder imageBladder image ; ;
Early , delay , post void film assess Early , delay , post void film assess bladder bladder
pathology pathology
Renal sizeRenal size
• Related with age Related with age
• 9-13 cm in length (cephalocaudal)9-13 cm in length (cephalocaudal)
• Kidney slightly larger in men than womenKidney slightly larger in men than women
• LK >RK 0.5 cm LK >RK 0.5 cm
• Significant discrepanciesSignificant discrepancies
RK >1.5 cm larger than LKRK >1.5 cm larger than LK
LK >2 cm larger than RK LK >2 cm larger than RK
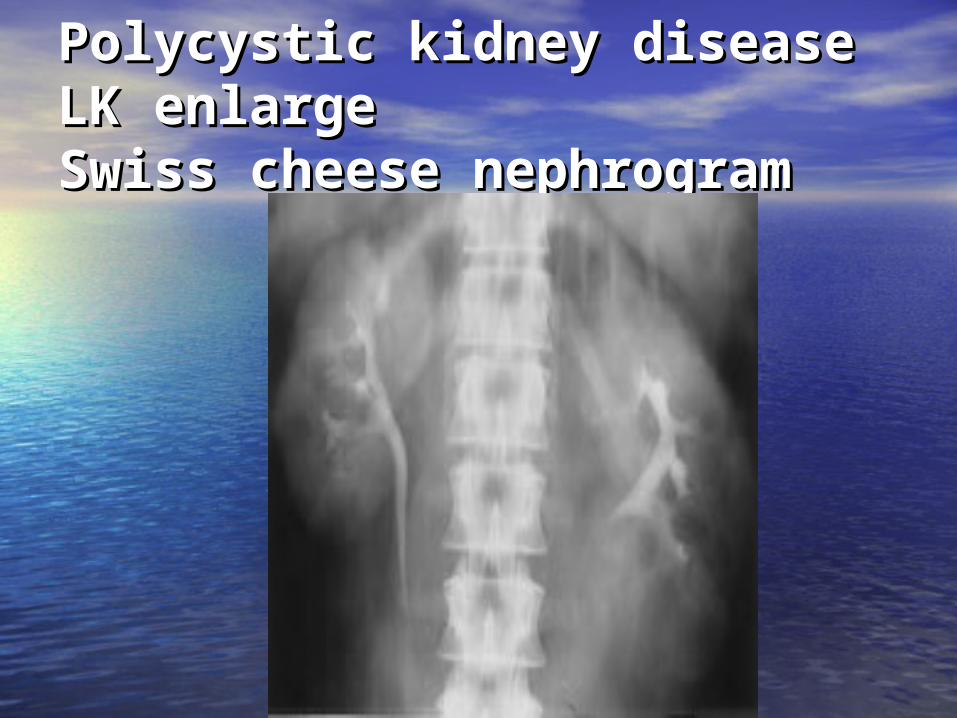
Polycystic kidney diseasePolycystic kidney diseaseLK enlarge LK enlarge Swiss cheese nephrogramSwiss cheese nephrogram

Renal contour abnormalityRenal contour abnormality
• Contour abnormality associate with change Contour abnormality associate with change in in
parenchymal thickness ( parenchymal thickness ( interpapillary interpapillary lineline ) )
interprete underlying collecting system interprete underlying collecting system
• Parenchymal thicknessParenchymal thickness : :
average 3-3.5 cm polar region average 3-3.5 cm polar region
2-2.5 cm interpolar region 2-2.5 cm interpolar region
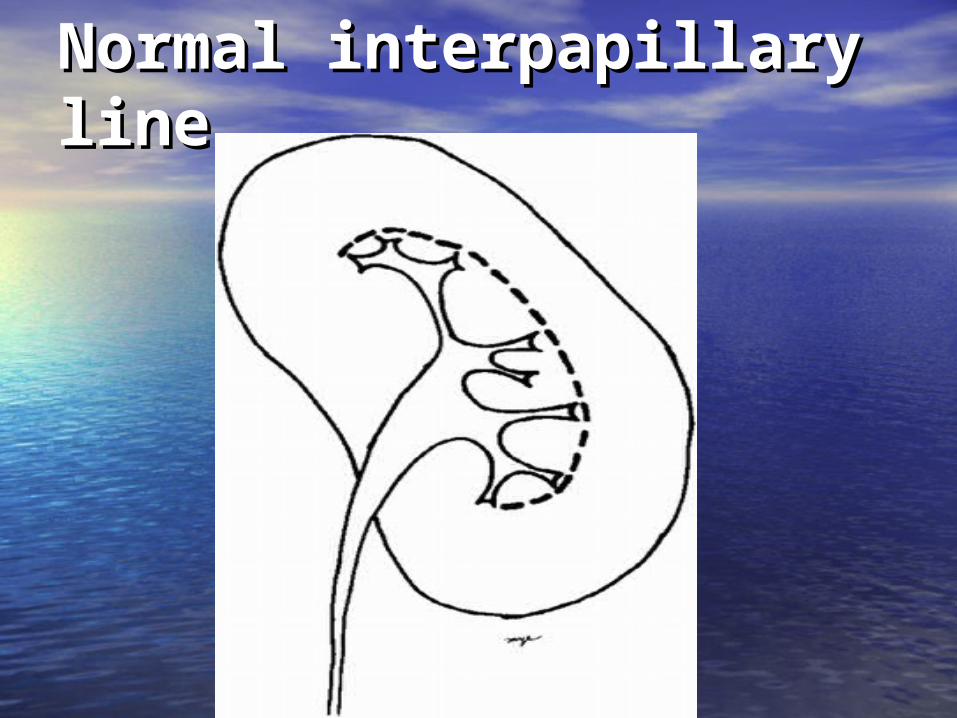
Normal interpapillary Normal interpapillary lineline
Parenchymal thickness Parenchymal thickness • Indentation or increase thicknessIndentation or increase thickness : : * Congenital anatomic variation * Congenital anatomic variation * Predictable location * Predictable location • Increase parenchymal thicknessIncrease parenchymal thickness , , calyceal distortioncalyceal distortion : : * Mass * Mass • Decrease parenchymal thicknessDecrease parenchymal thickness , , calyceal changescalyceal changes : : * Post inflammation * Post inflammation * Stone–relate scar* Stone–relate scar• Parenchymal loss , without calyceal Parenchymal loss , without calyceal
distortiondistortion:: * Renal infarction * Renal infarction
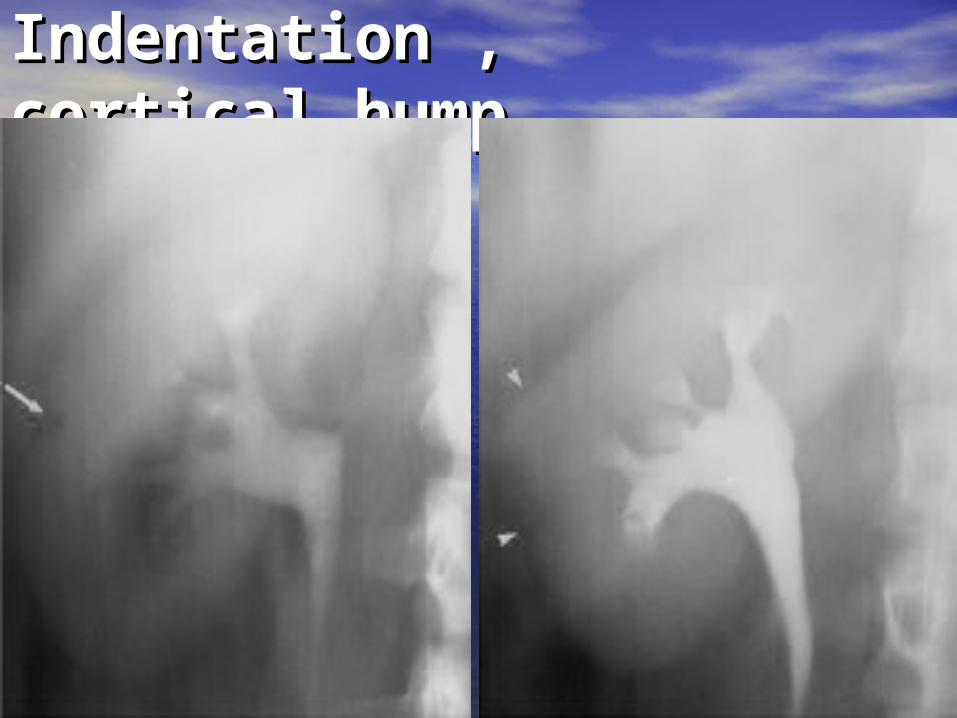
Indentation , cortical Indentation , cortical hump hump
Nephrotomographic Nephrotomographic imageimage
•Require adequate Require adequate
* Renal blood flow * Renal blood flow
* Normal parenchymal excretory * Normal parenchymal excretory
functionfunction
* Normal venous outflow* Normal venous outflow
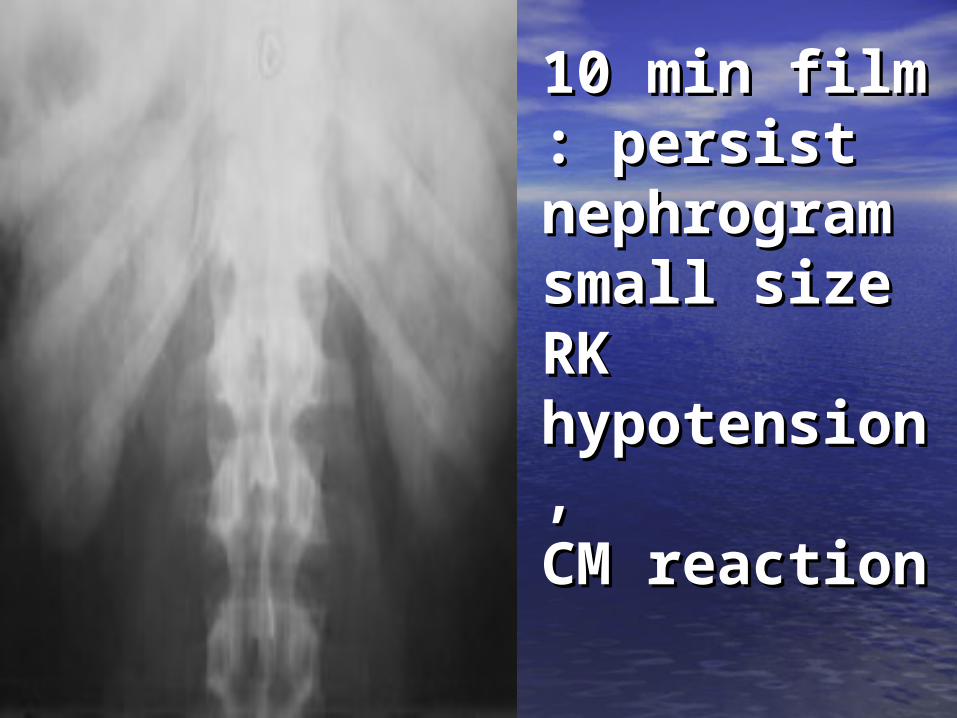
10 min 10 min film : film : persist persist nephrogramnephrogramsmall size small size RK RK hypotensiohypotension , n , CM reaction CM reaction

Renal artery stenosis RK Renal artery stenosis RK nephrotomogram , 15 minnephrotomogram , 15 min small size RK with decrease small size RK with decrease density density
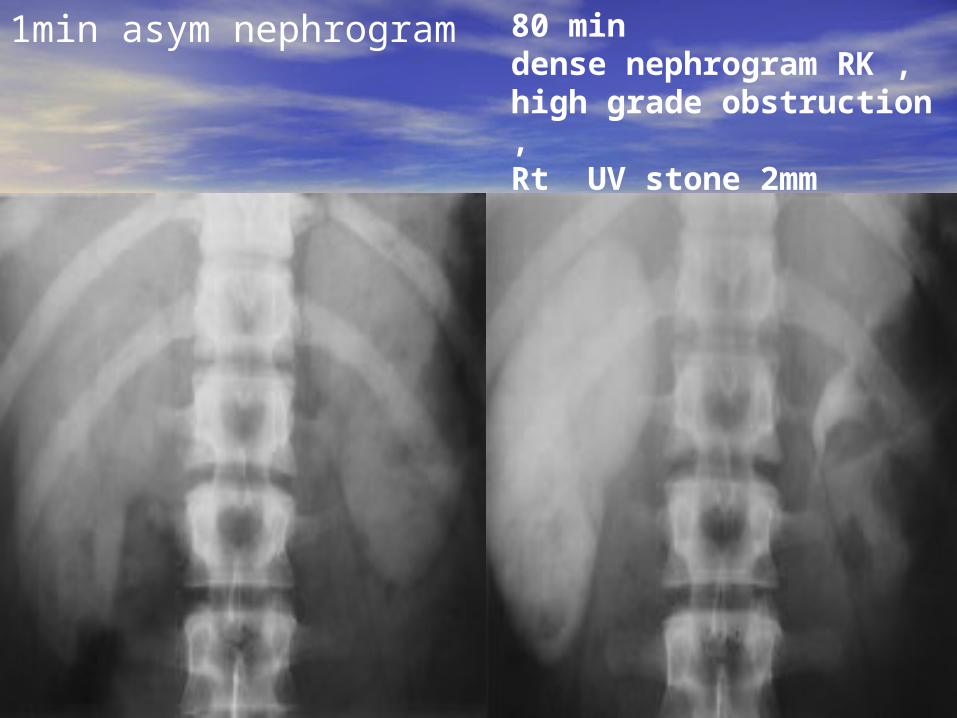
1min asym nephrogram 80 min dense nephrogram RK , high grade obstruction , Rt UV stone 2mm
Nephrotomogram Nephrotomogram • Absence of nephrotomographic Absence of nephrotomographic
enhancement within the lesion :enhancement within the lesion :
suggest a suggest a simple cystsimple cyst , ,
parenchymal parenchymal beaking beaking ( margin of unenhanced tissue )( margin of unenhanced tissue )
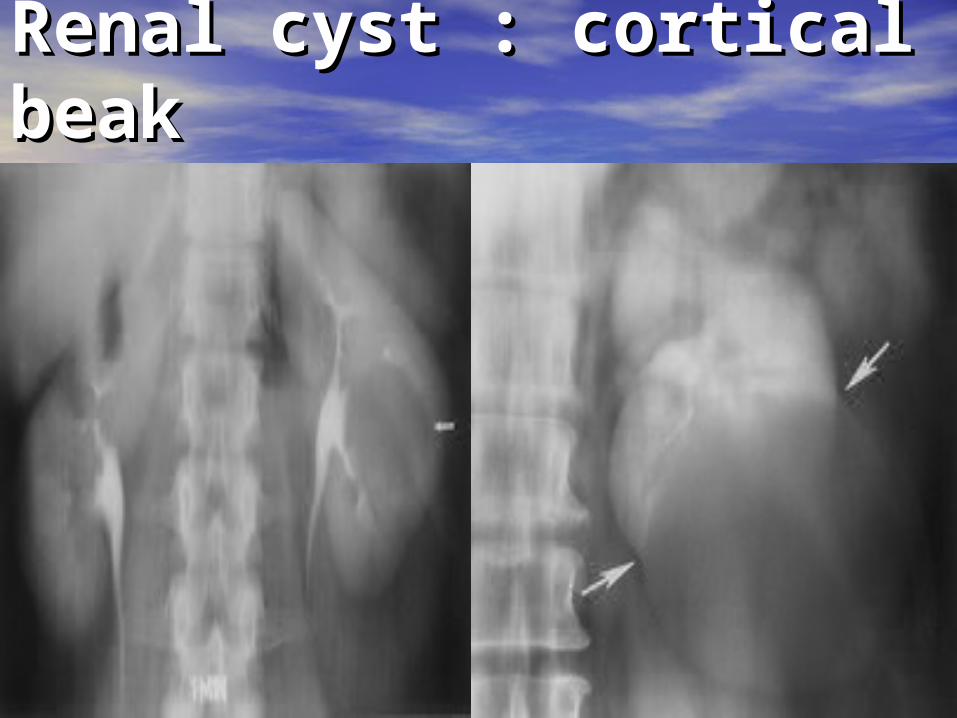
Renal cyst : cortical Renal cyst : cortical beak beak
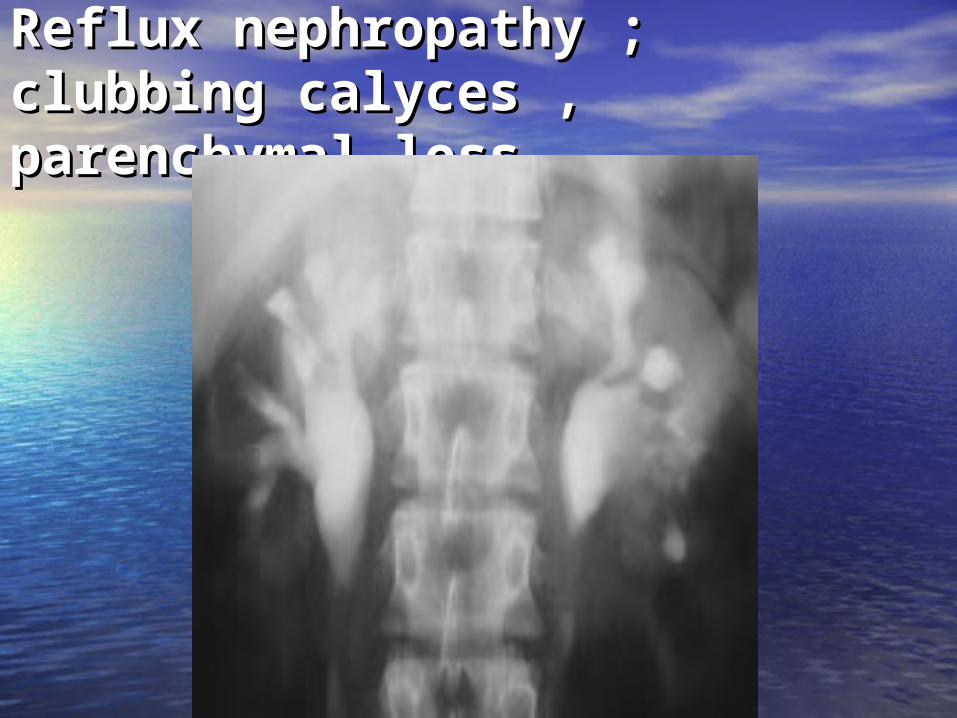
Reflux nephropathy ;Reflux nephropathy ;clubbing calyces , clubbing calyces , parenchymal lossparenchymal loss
MassMass
•Increase parenchymal Increase parenchymal thickness thickness
•Calyceal distortion Calyceal distortion
•Double contour at tomography Double contour at tomography
•CT is suggested for solid lesionCT is suggested for solid lesion
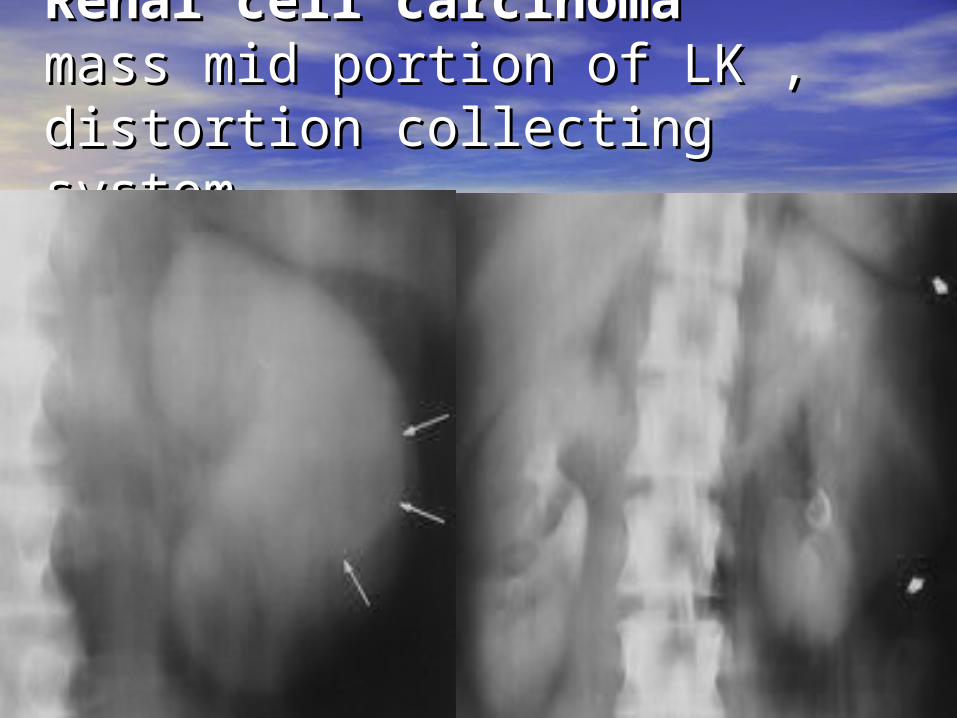
Renal cell carcinomaRenal cell carcinoma mass mid portion of LK , mass mid portion of LK , distortion collecting system distortion collecting system
Position of kidney Position of kidney • RK is lower than LK ( liver )RK is lower than LK ( liver )
• Vertical axis parallel upper 1/3 of Vertical axis parallel upper 1/3 of psoaspsoas
•Alteration of axis and positionAlteration of axis and position : :
* Congenital renal anomaly * Congenital renal anomaly
* Abdominal or RP mass* Abdominal or RP mass
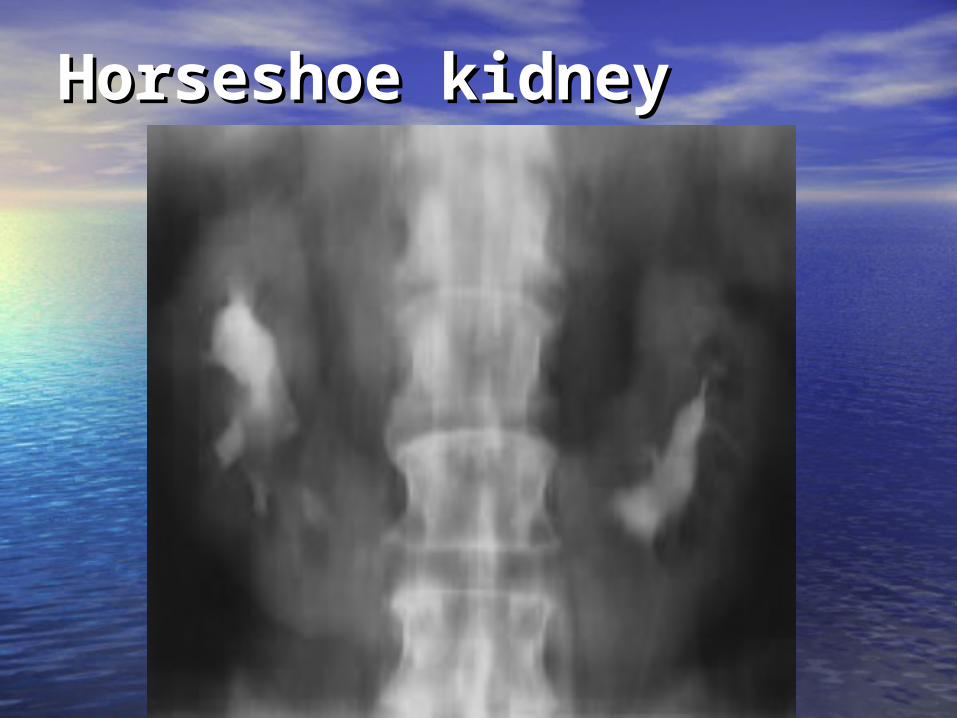
Horseshoe kidneyHorseshoe kidney
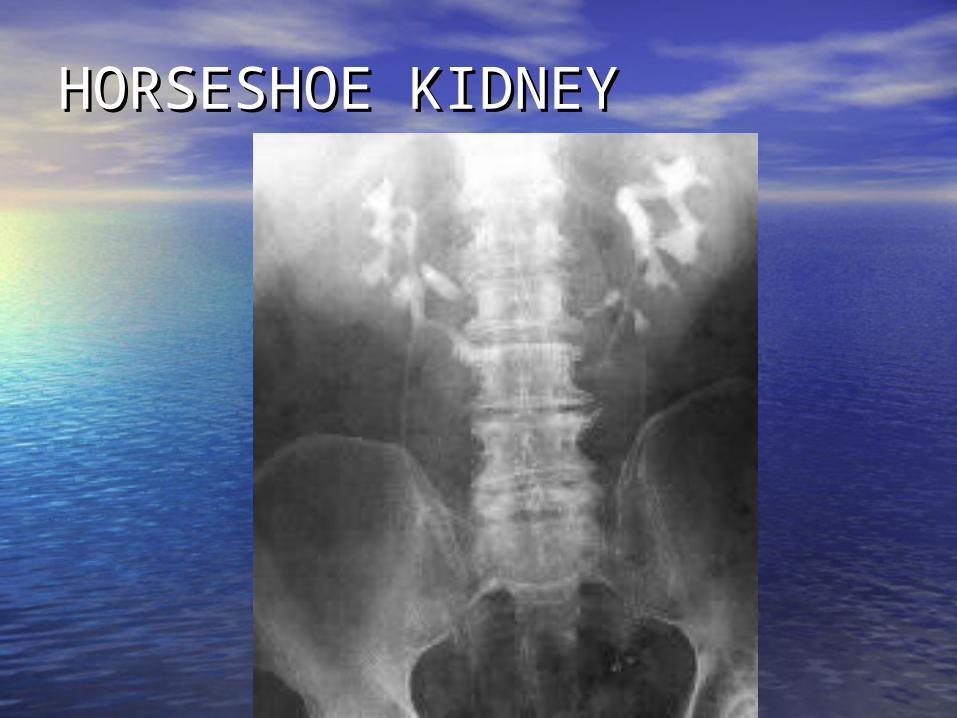
HORSESHOE KIDNEY HORSESHOE KIDNEY
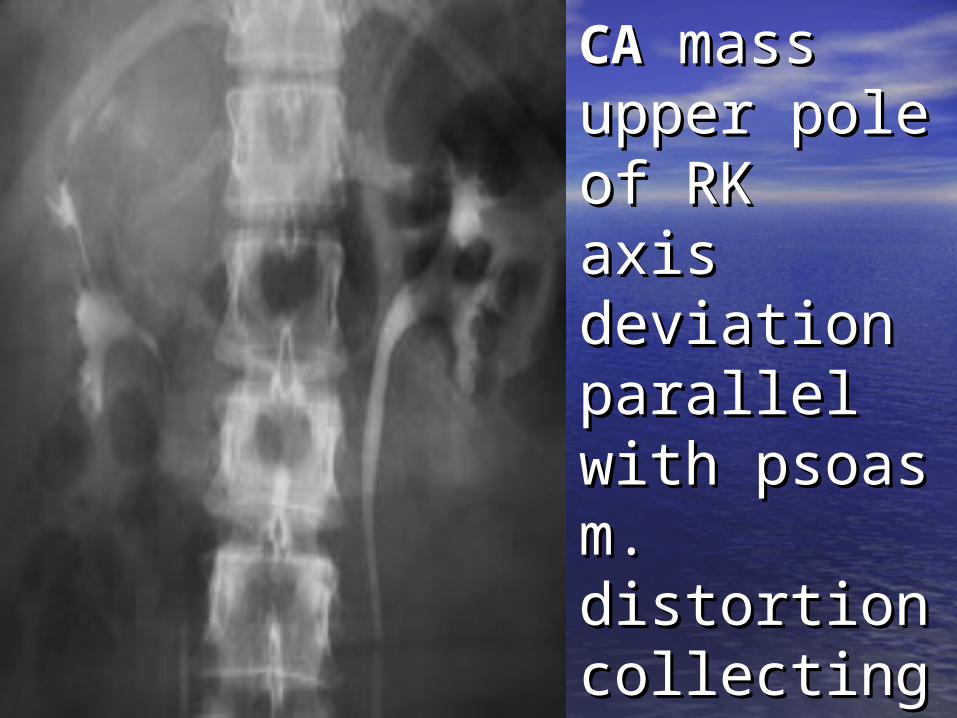
Renal cell Renal cell CACA mass mass upper pole upper pole of RK of RK axis axis deviation deviation parallel with parallel with psoas m. psoas m. distortion distortion collecting collecting system system
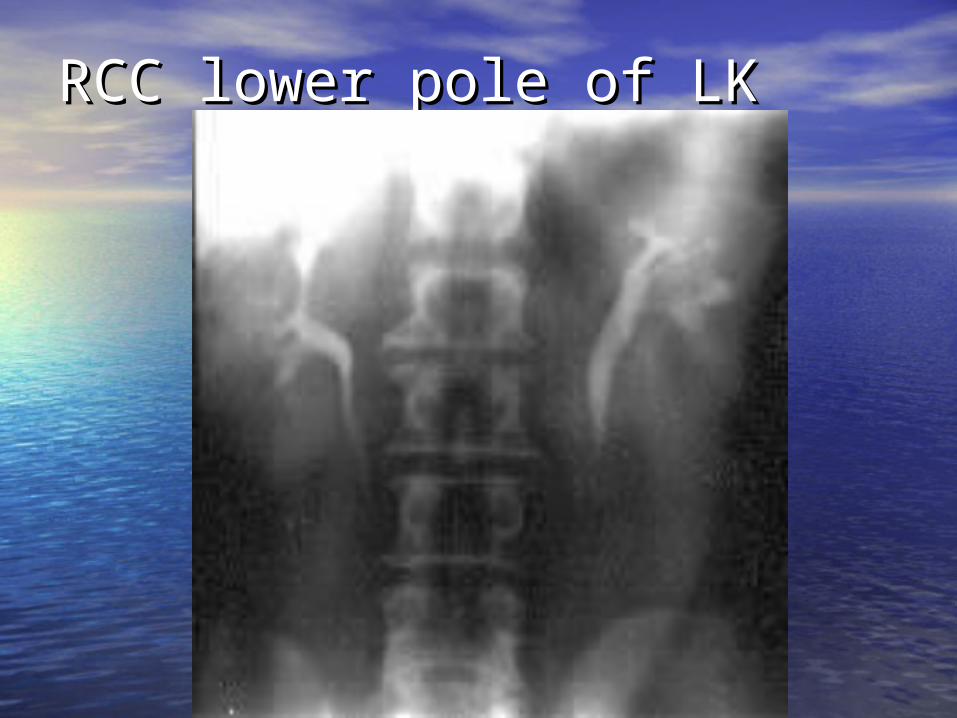
RCC lower pole of LK RCC lower pole of LK
Pyelographic and ureteric Pyelographic and ureteric imageimage
• IVP , CT urogram good for IVP , CT urogram good for evaulation of collecting system , evaulation of collecting system ,
urothelium-line surface:urothelium-line surface:
* TCC urinary tract * TCC urinary tract
* Pyelitis cystica* Pyelitis cystica
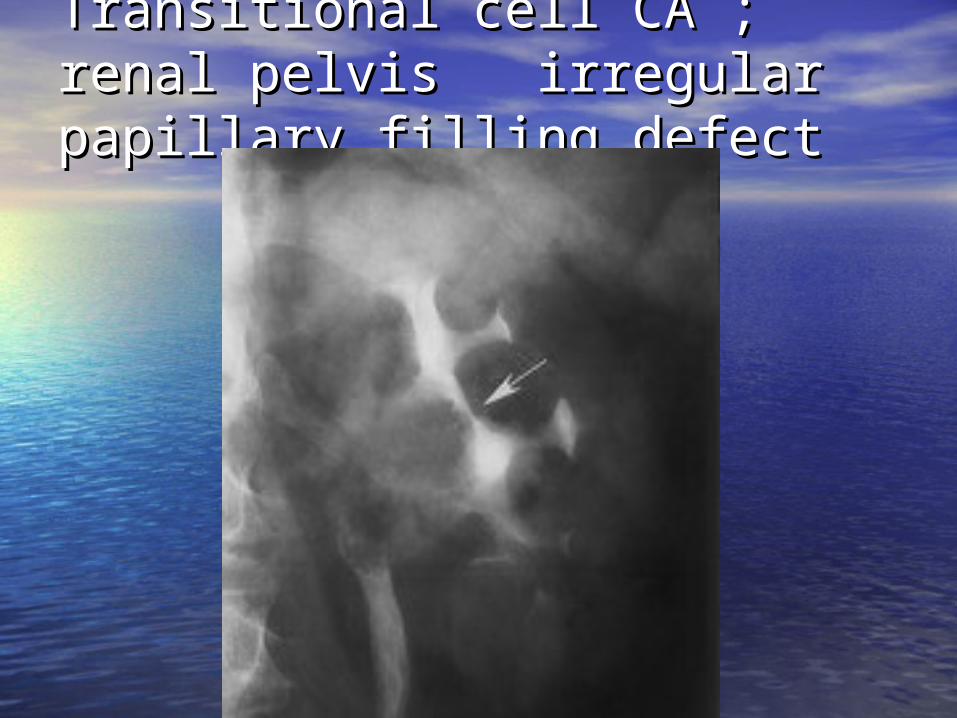
Transitional cell CA ; renal Transitional cell CA ; renal pelvis irregular papillary pelvis irregular papillary filling defectfilling defect
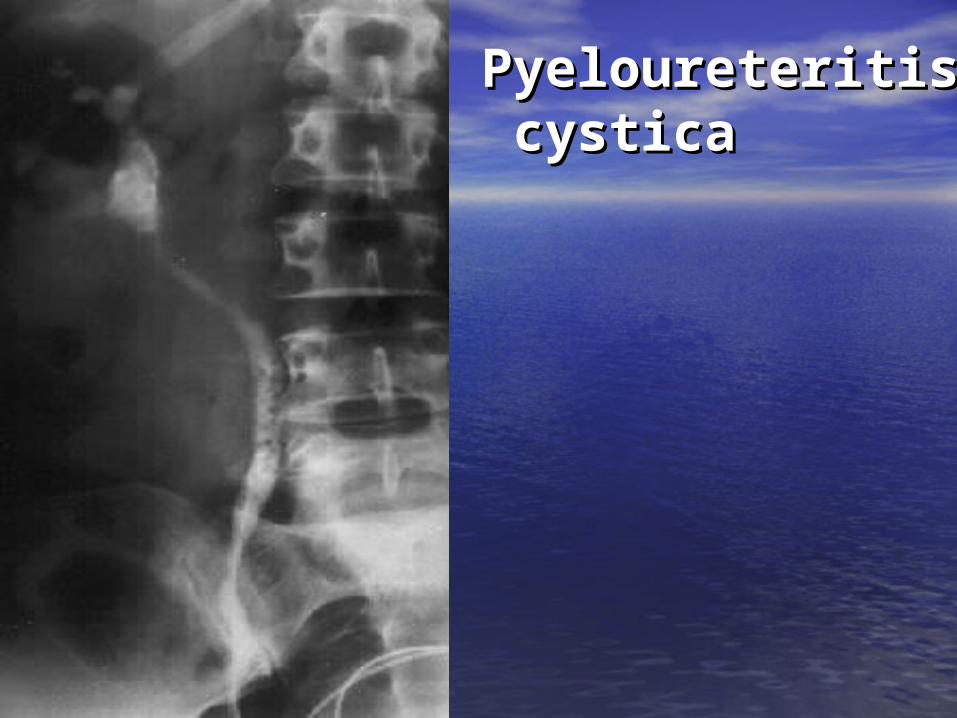
Pyeloureteritis Pyeloureteritis cysticacystica
CalycesCalyces
• Compound calyces : polar region Compound calyces : polar region
• Simple papillae , classic calices : Simple papillae , classic calices : interpolar interpolar
• Obstruction : Obstruction :
* Round forniceal margin , * Round forniceal margin ,
* Loss of papillary impression , * Loss of papillary impression ,
* Clubbing calices* Clubbing calices
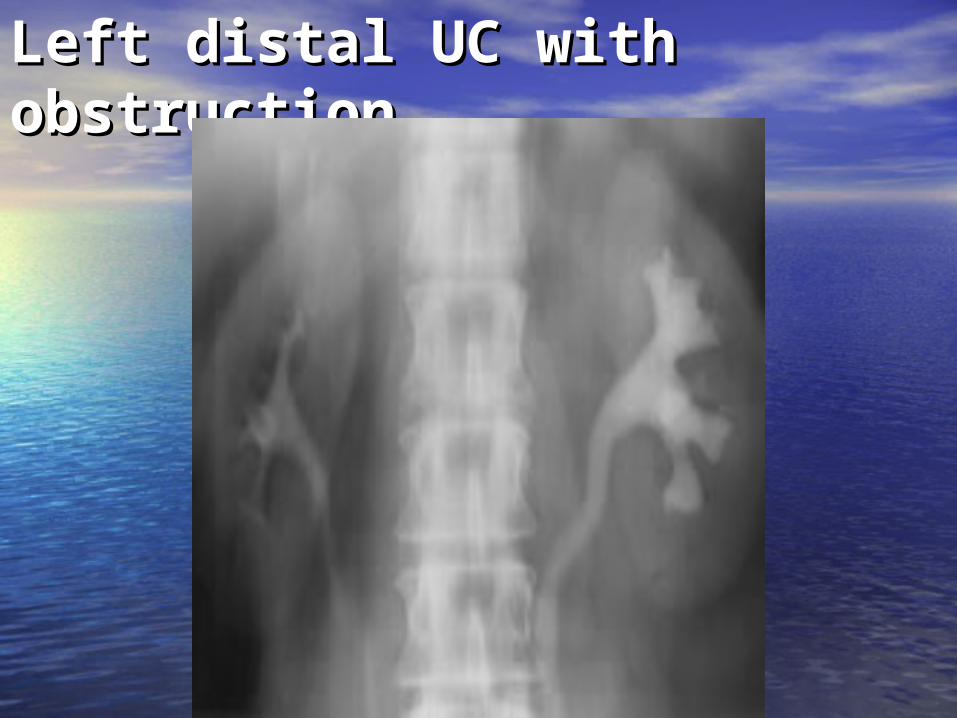
Left distal UC with Left distal UC with obstructionobstruction
PapillaePapillae
•Papillary blush Papillary blush
•Contrast within papillae Contrast within papillae
•Tubular ectasia : Tubular ectasia :
Medullary sponge Medullary sponge kidneykidney
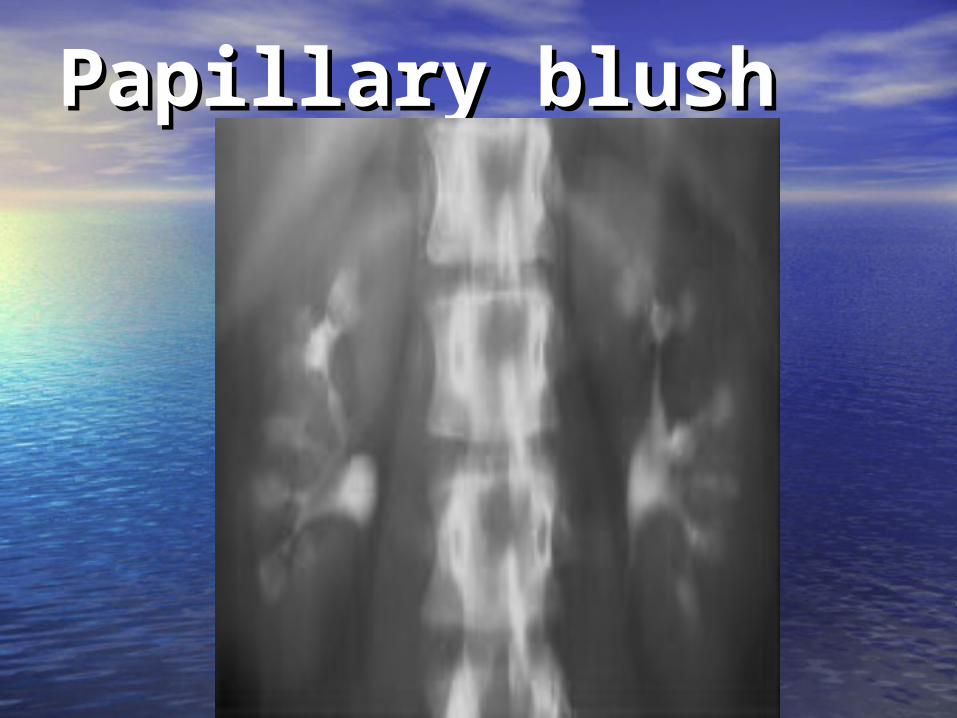
Papillary blushPapillary blush
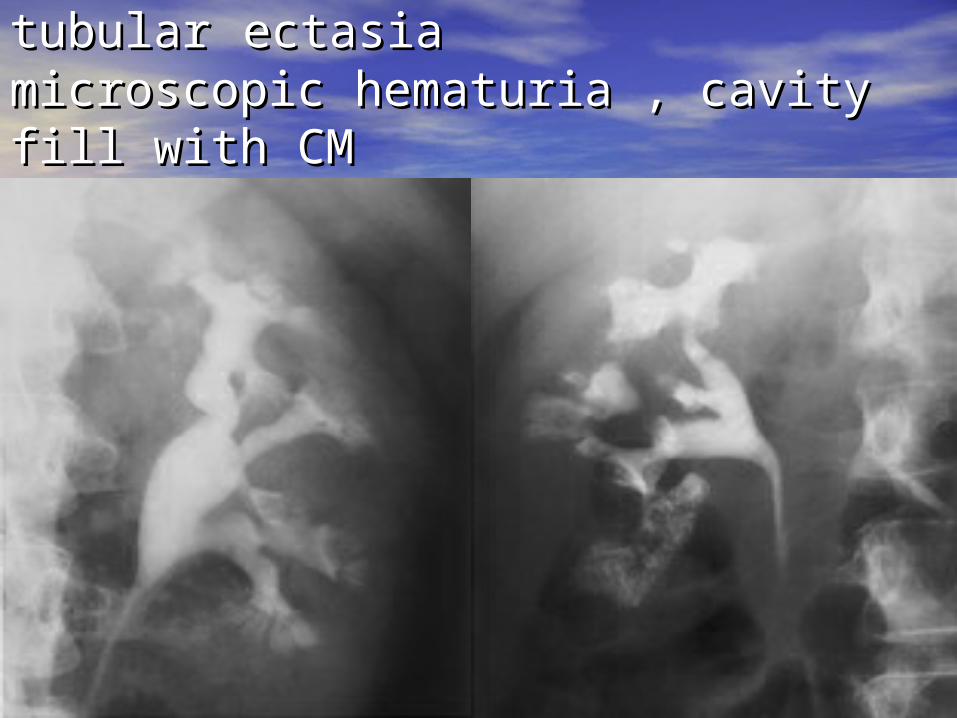
Medullary sponge kidney; tubularMedullary sponge kidney; tubular ectasiaectasiamicroscopic hematuria , cavity fill with microscopic hematuria , cavity fill with CMCM“ growing calculus sign ““ growing calculus sign “
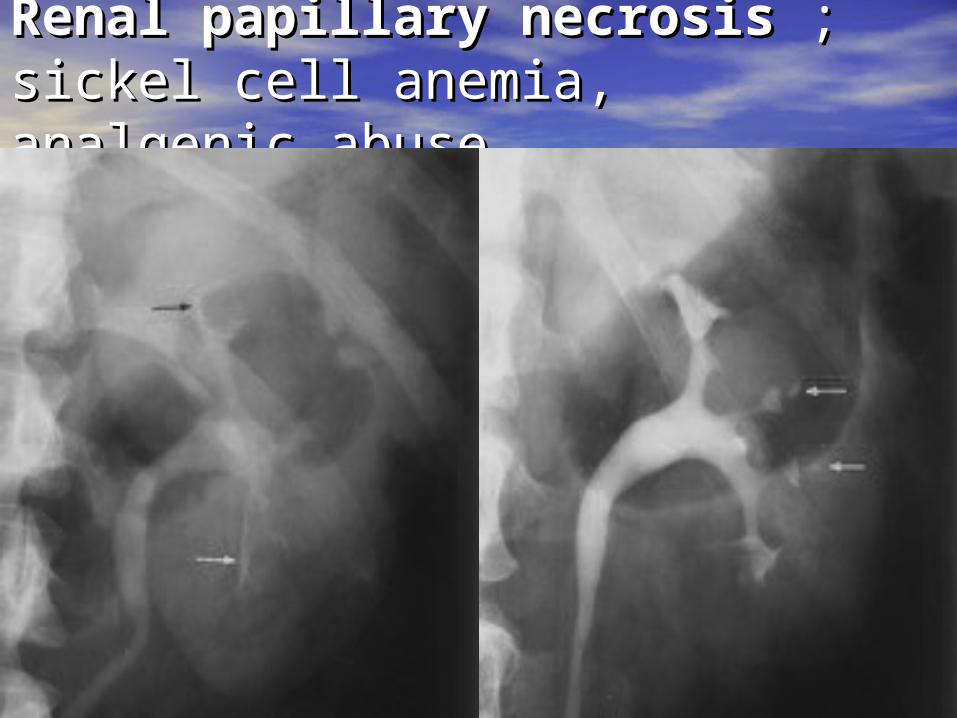
Renal papillary necrosisRenal papillary necrosis ; ;sickel cell anemia, analgenic sickel cell anemia, analgenic abuseabuse
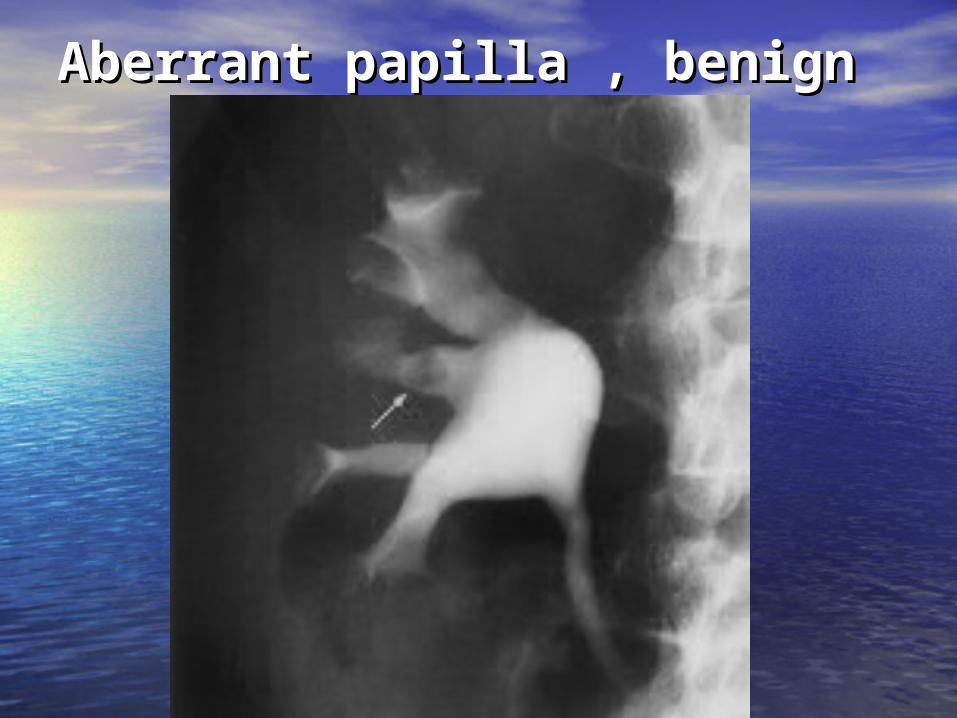
Aberrant papilla , benignAberrant papilla , benign

Calyceal diverticulum with Calyceal diverticulum with stonestone
Phantom calixPhantom calix
•Usually number of calices 7-14Usually number of calices 7-14
•Phantom calix : Phantom calix :
* Benign -TB * Benign -TB
* Malignant process -* Malignant process -OncocalixOncocalix
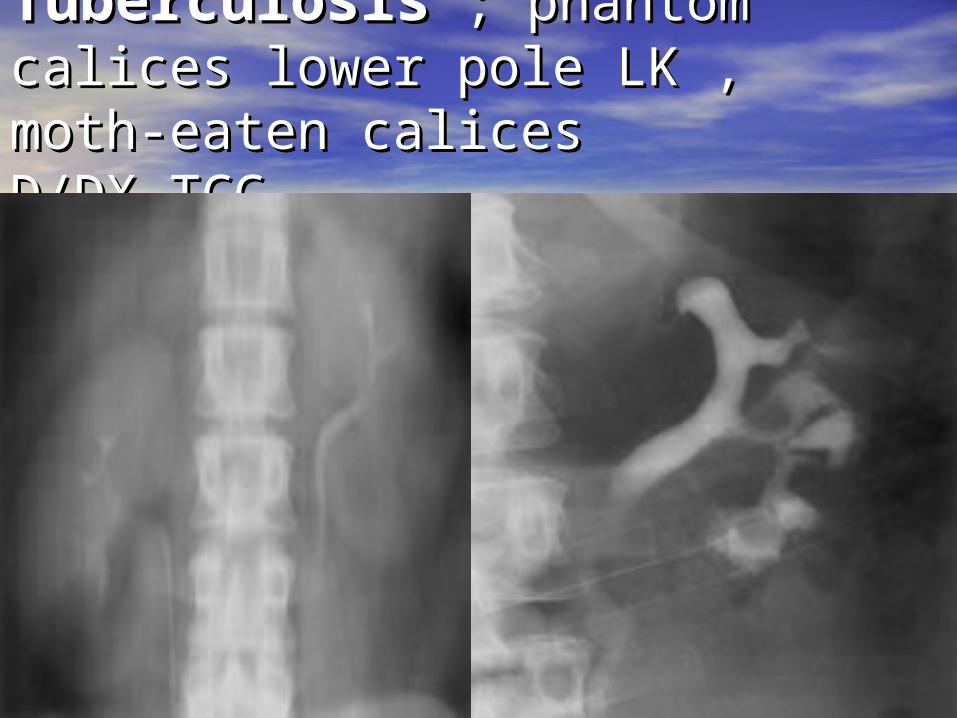
TuberculosisTuberculosis ; phantom ; phantom calices lower pole LK , moth-calices lower pole LK , moth-eaten caliceseaten calicesD/DX TCCD/DX TCC
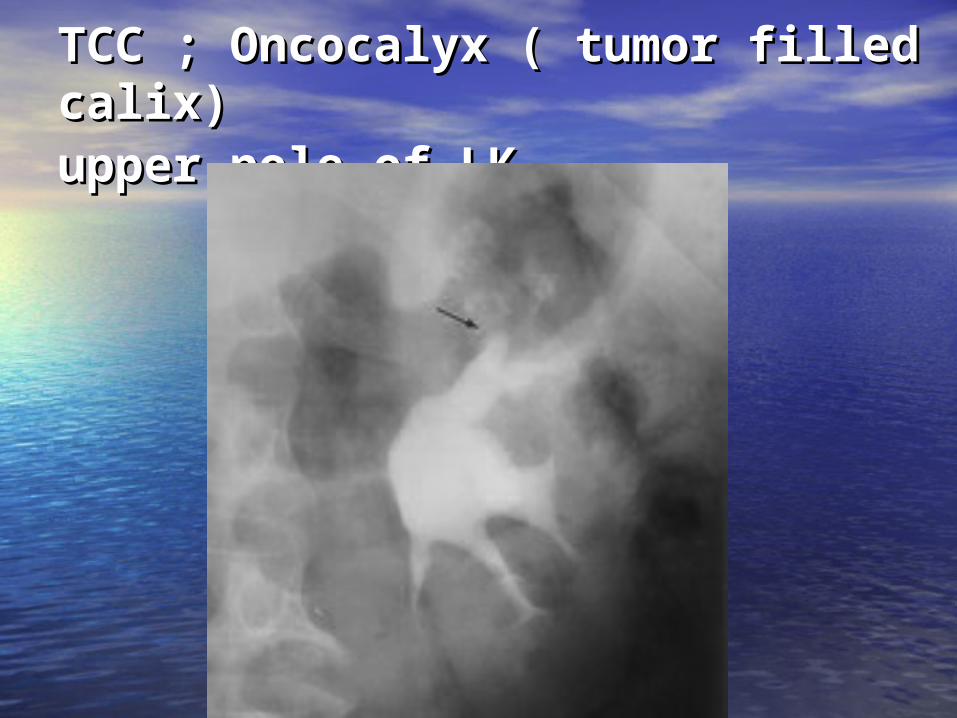
TCC ; Oncocalyx ( tumor filled TCC ; Oncocalyx ( tumor filled calix)calix)upper pole of LKupper pole of LK
Impression on collecting Impression on collecting systemsystem
•Vascular compression Vascular compression
•Renal sinus cyst Renal sinus cyst
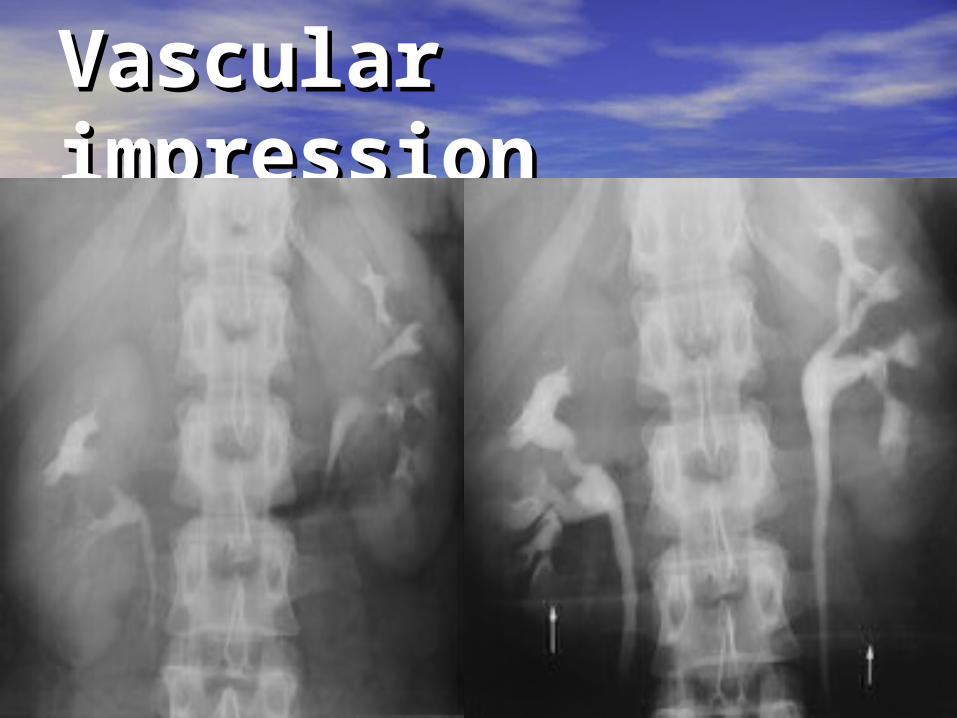
Vascular Vascular impressionimpression
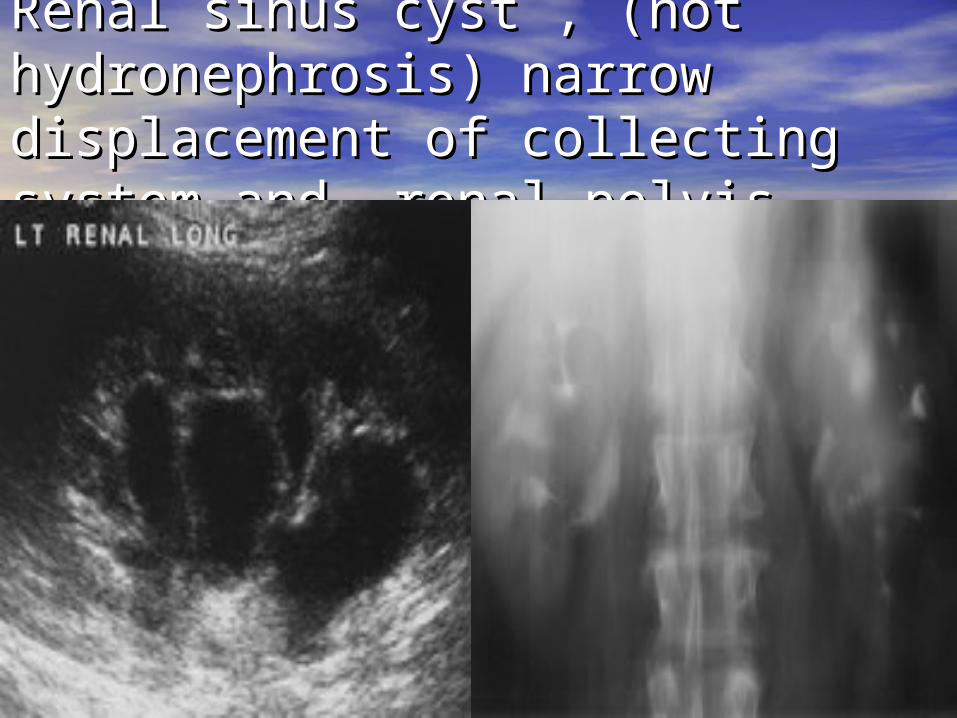
Renal sinus cyst , (not Renal sinus cyst , (not hydronephrosis) narrow hydronephrosis) narrow displacement of collecting system displacement of collecting system and renal pelvisand renal pelvis
UreterUreter• Segmental nonvisualization of Segmental nonvisualization of
ureter due to peristalsis ureter due to peristalsis
• Persistence column of contrast Persistence column of contrast along course of ureter on several along course of ureter on several
image indicate image indicate obstruction :obstruction :
collecting system dilatationcollecting system dilatation

Stone at right Stone at right UV junction , UV junction , edema edema interureteric interureteric ridge ( normal ridge ( normal < 3mm )< 3mm )
Ureteric courseUreteric course
• From renal pelvis , lateral to psoas m. From renal pelvis , lateral to psoas m.
• About L3 pass ventral to psoas m.About L3 pass ventral to psoas m.
• Upper RP course , pass along lateral ½ of Upper RP course , pass along lateral ½ of transverse process of upper lumbar transverse process of upper lumbar vertebrae vertebrae
• Cross anterior to iliac vessel ( medial )Cross anterior to iliac vessel ( medial )
• Pelvic course , parallel inner margin of Pelvic course , parallel inner margin of iliac bone and enter bladder at UV iliac bone and enter bladder at UV junction junction
Abnormal ureteric Abnormal ureteric coursecourse
• Medial deviation of ureter : Medial deviation of ureter :
* Overlying pedicle, medial to * Overlying pedicle, medial to pedicle pedicle
* Separation of ureter <5 cm* Separation of ureter <5 cm
• Lateral deviation :Lateral deviation :
* Ureter lie >1cm beyond tip of * Ureter lie >1cm beyond tip of
transverse process transverse process
• Abrupt changes in ureteric courseAbrupt changes in ureteric course
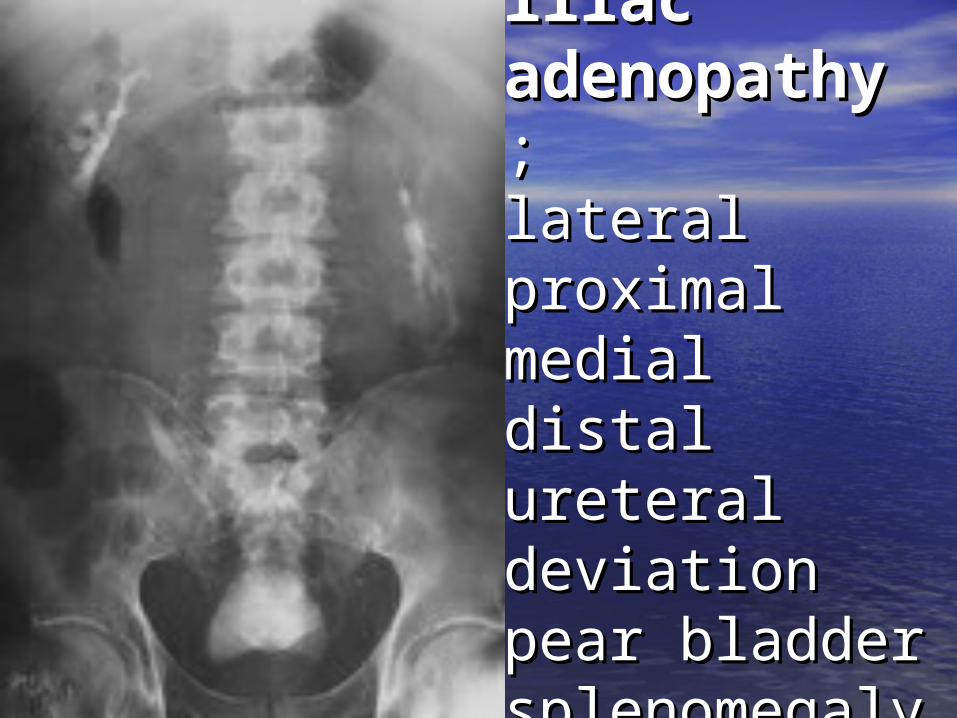
RP and iliac RP and iliac adenopathyadenopathy ; ; lateral lateral proximal proximal medial distal medial distal ureteral ureteral deviationdeviationpear bladder pear bladder splenomegaly splenomegaly
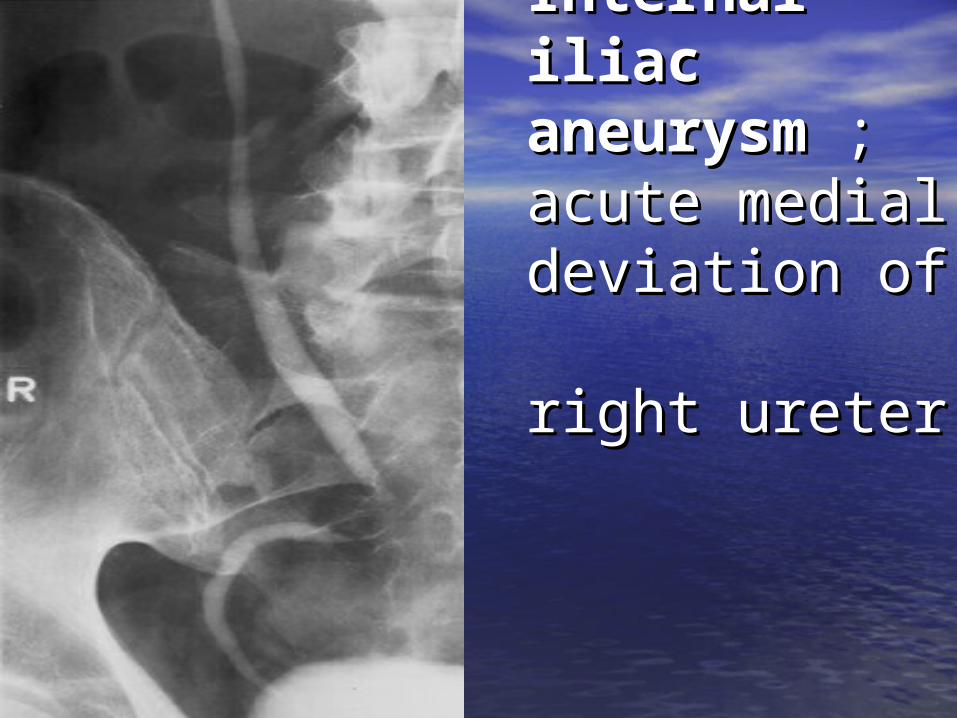
Internal iliac Internal iliac aneurysmaneurysm ; ; acute medial acute medial deviation of deviation of right ureterright ureter
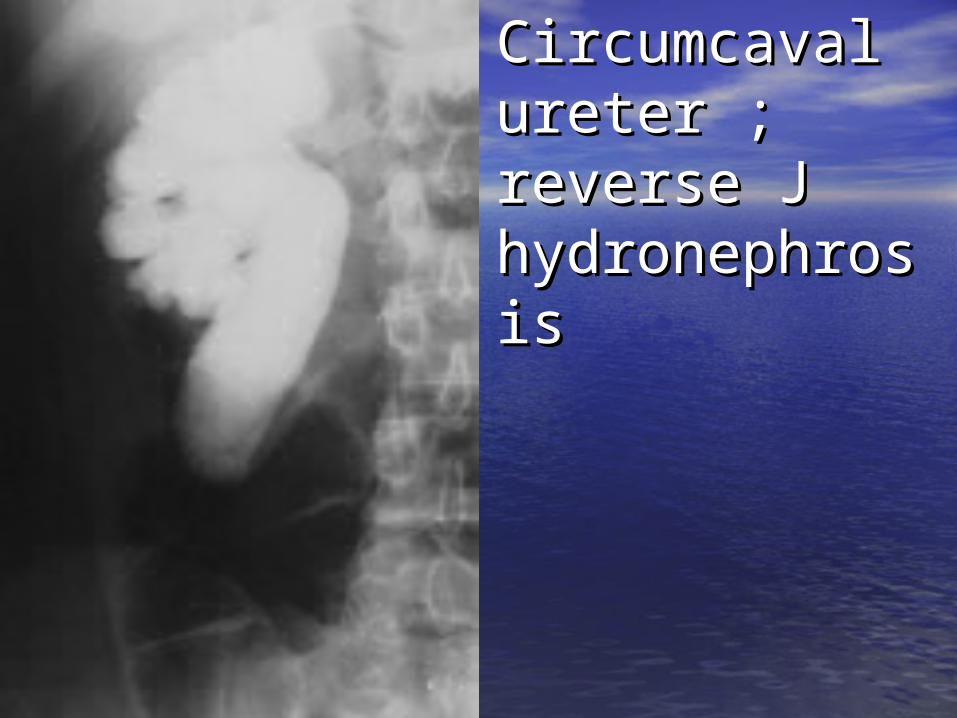
Circumcaval Circumcaval ureter ; ureter ; reverse J reverse J hydronephrosihydronephrosis s
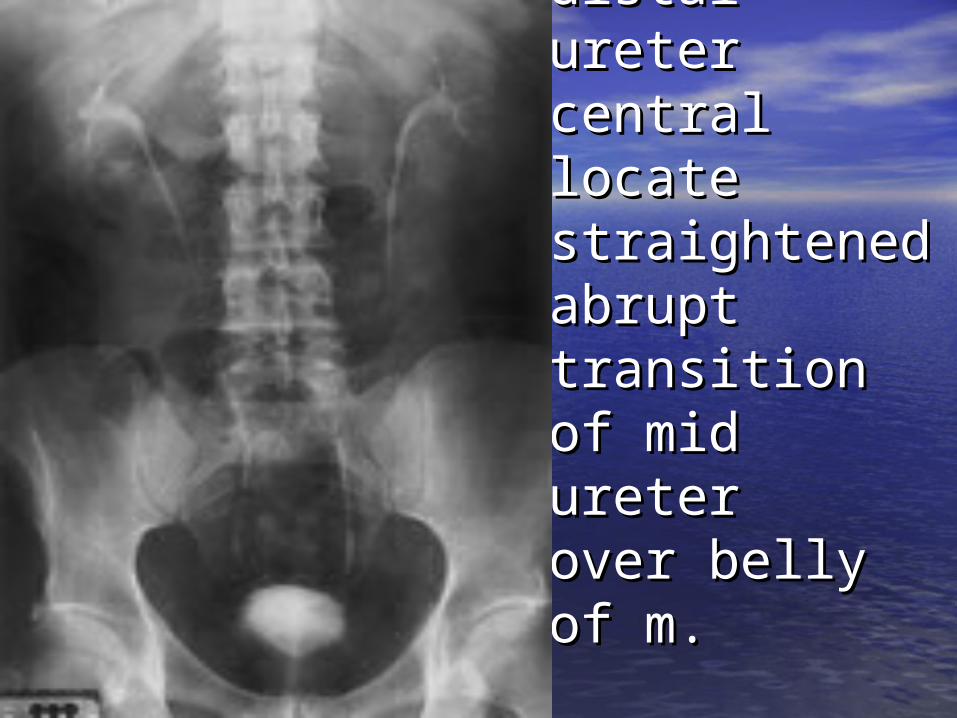
Psoas Psoas musclemusclehypertrophyhypertrophy::distal ureter distal ureter central locate central locate straightenedstraightenedabrupt abrupt transition of transition of mid uretermid ureterover belly of over belly of m. m.
Ureteric diameterUreteric diameter• Diameter > 8 mm consider dilatation Diameter > 8 mm consider dilatation
:: * Obstruction * Obstruction * Ureterocele* Ureterocele * Nonobstructive dilatation , * Nonobstructive dilatation , high urine flowhigh urine flow ( fluid diuresis , DI ) ( fluid diuresis , DI ) * Reflux * Reflux * Inflammatory process * Inflammatory process
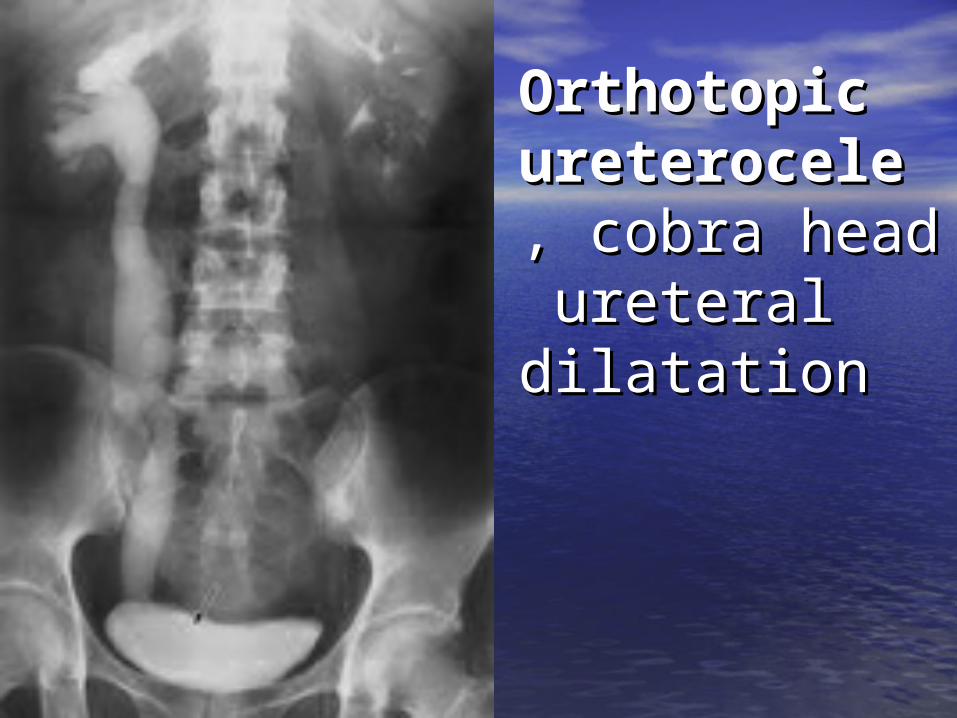
Orthotopic Orthotopic ureteroceleureterocele , , cobra head cobra head ureteral ureteral dilatation dilatation
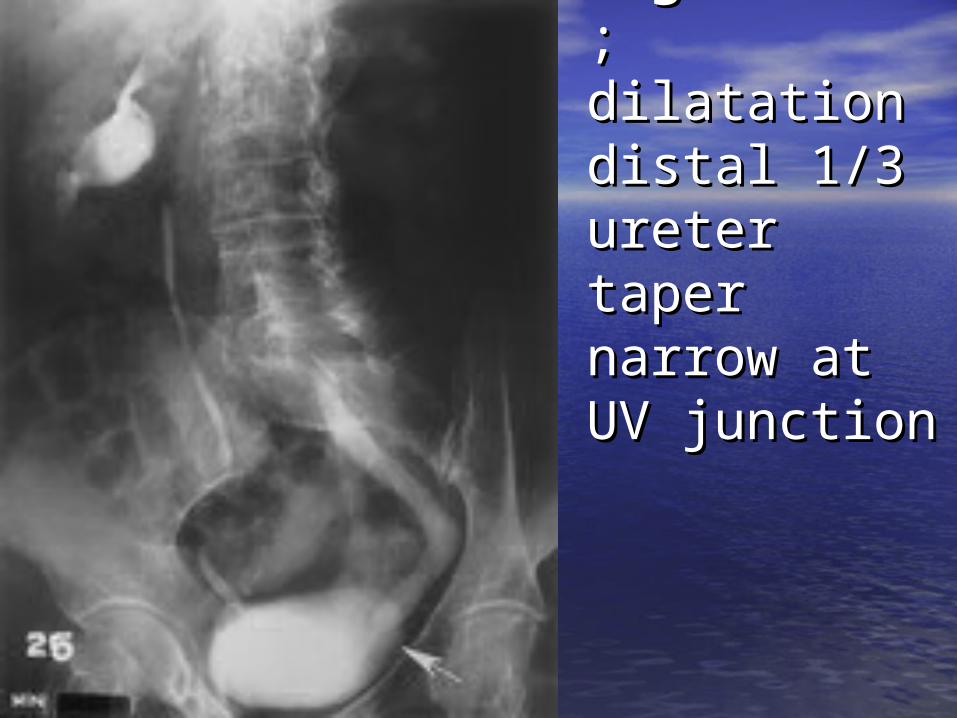
MegaureterMegaureter ;;dilatation dilatation distal 1/3 distal 1/3 ureter taper ureter taper narrow at UV narrow at UV junctionjunction
UreterUreter
• Normal peristalsis Normal peristalsis
• Anatomic narrowing :Anatomic narrowing :
* UPJ junction * UPJ junction
* Iliac vs transition * Iliac vs transition
* UV junction * UV junction
• Vascular impression of gonadal Vascular impression of gonadal vein , prominent in femalevein , prominent in female

Ureteric Ureteric nothchingnothchingextrinsic extrinsic vascular vascular narrowing narrowing gonadal gonadal veinvein
Ureter Ureter •Ureteral pseudodiverticulaUreteral pseudodiverticula : :
narrow with outpouching ureteric narrow with outpouching ureteric wallwall
increase of TCCincrease of TCC , , especially in especially in bladderbladder
•Ureteric filling defectUreteric filling defect : :
TCC , patient present with hematuriaTCC , patient present with hematuria
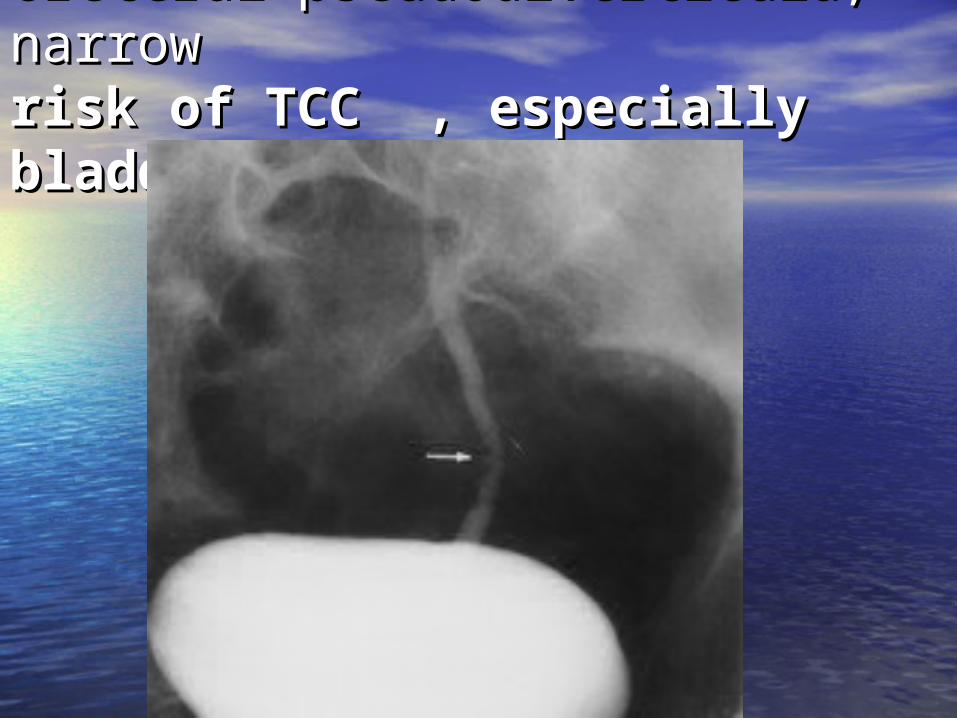
Ureteral pseudodiverticula, Ureteral pseudodiverticula, narrow narrow risk of TCC , especially risk of TCC , especially bladderbladder
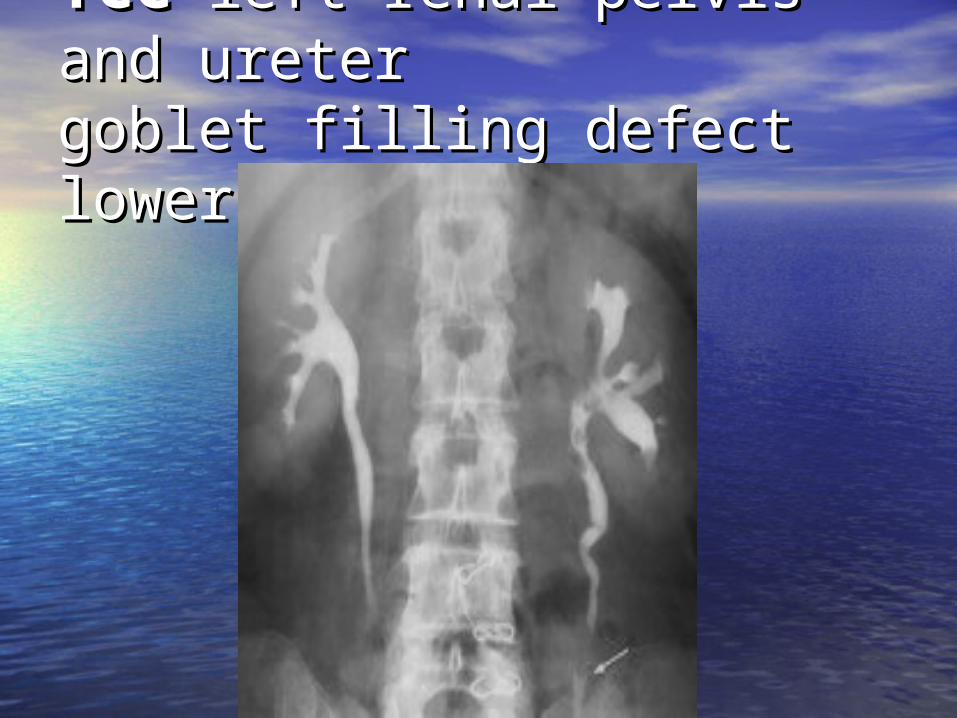
TCCTCC left renal pelvis and left renal pelvis and ureter ureter goblet filling defect lower goblet filling defect lower ureterureter

TCC TCC distal ureter with filling distal ureter with filling defect on fluorocopy , persist defect on fluorocopy , persist hematuria hematuria
Bladder imageBladder image
• 15-30 min or delay film distend 15-30 min or delay film distend lumenlumen
evaluate the bladder , wall thicken evaluate the bladder , wall thicken
• Post void film may be helpful for Post void film may be helpful for evaluation mucosal lesion evaluation mucosal lesion
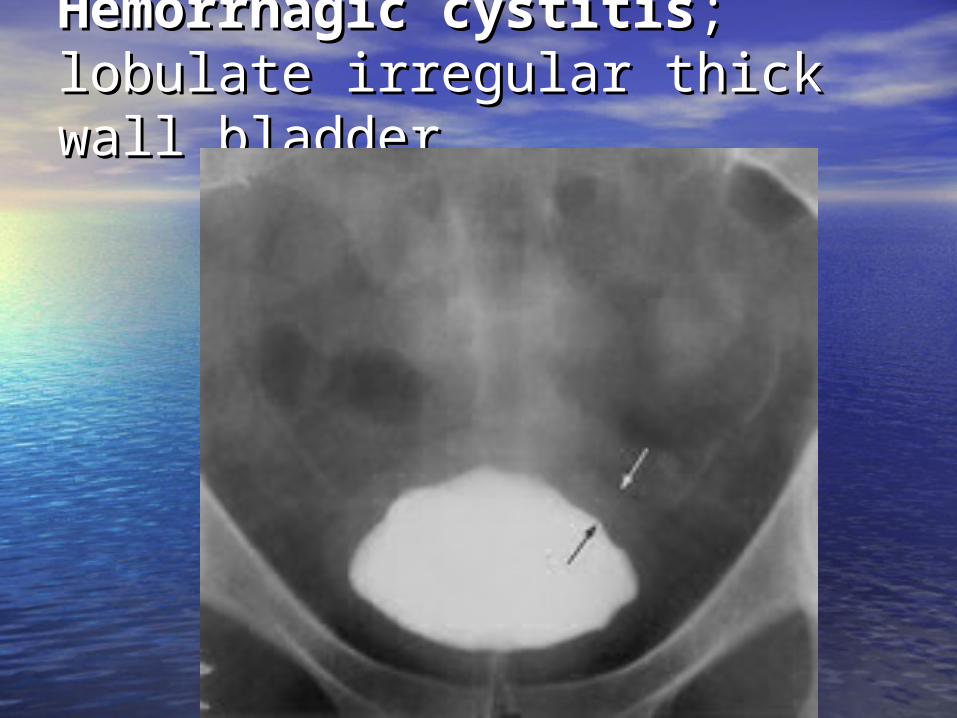
Hemorrhagic cystitisHemorrhagic cystitis; ; lobulate irregular thick wall lobulate irregular thick wall bladder bladder
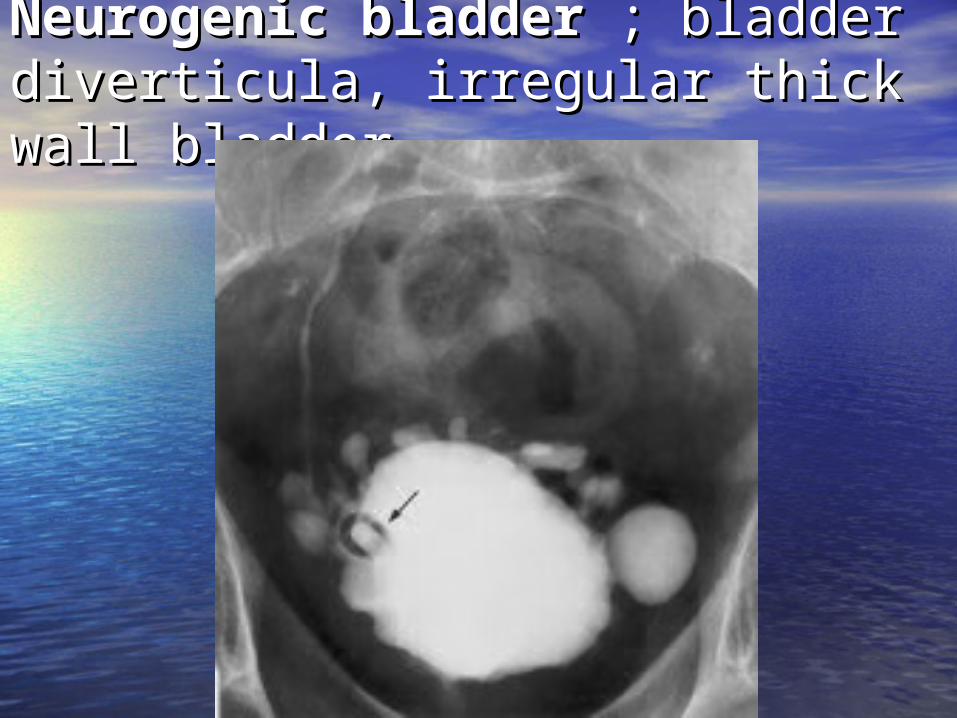
Neurogenic bladderNeurogenic bladder ; bladder ; bladder diverticula, irregular thick wall diverticula, irregular thick wall bladder bladder
BladderBladder
• Bladder is tether only at the Bladder is tether only at the lower aspect of anatomic pelvislower aspect of anatomic pelvis
• Position and appearance can be Position and appearance can be
significant distort by significant distort by
* Mass ( intrinsic , extrinsic )* Mass ( intrinsic , extrinsic )
* Hematoma * Hematoma
* Pelvic lipomatosis * Pelvic lipomatosis
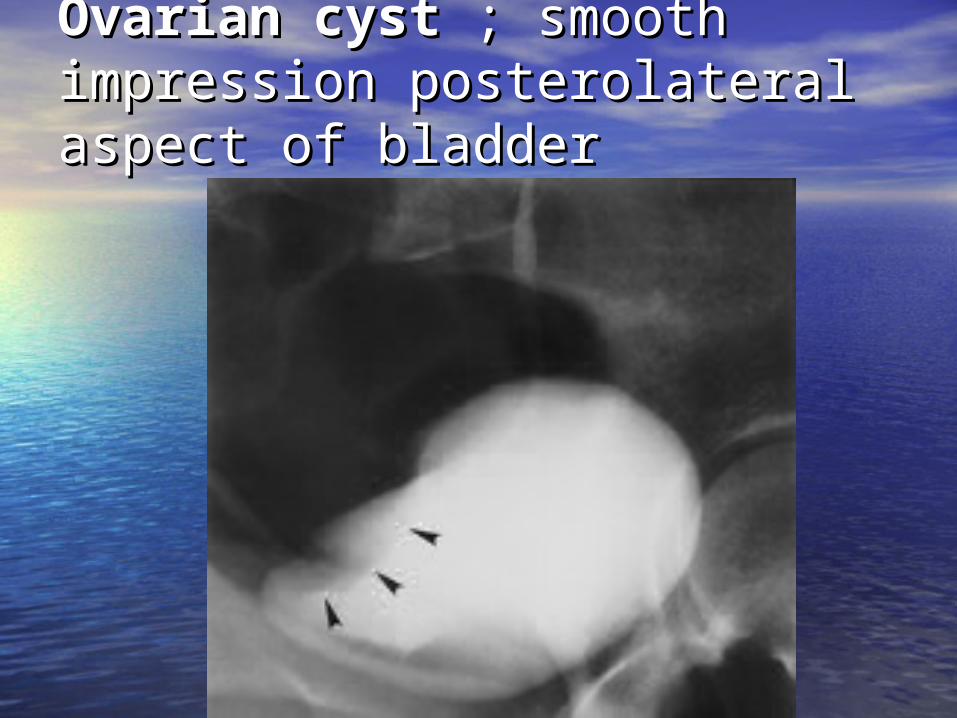
Ovarian cystOvarian cyst ; smooth ; smooth impression posterolateral impression posterolateral aspect of bladder aspect of bladder

Pelvic Pelvic traumatraumahematomahematomapear deviate, pear deviate, elongate elongate bladder , bladder , blood clot blood clot in lumenin lumen
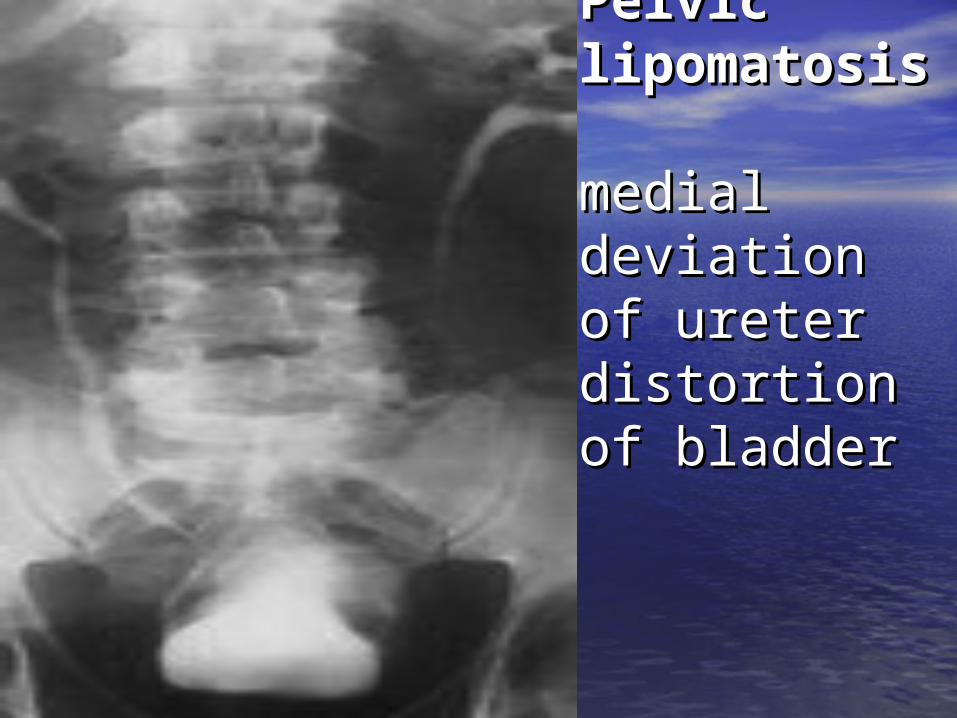
Pelvic Pelvic lipomatosislipomatosis medial medial deviation of deviation of ureter ureter distortion of distortion of bladderbladder
Bladder outlet Bladder outlet obstructionobstruction
• Bladder base defect ( prostatic disease) Bladder base defect ( prostatic disease) with bladder wall irregular thickened ,with bladder wall irregular thickened ,
contour abnormality with cellule or contour abnormality with cellule or diverticulum formation diverticulum formation
* Cellule – early herniation of bladder * Cellule – early herniation of bladder mucosa mucosa
usually as wide as tall usually as wide as tall
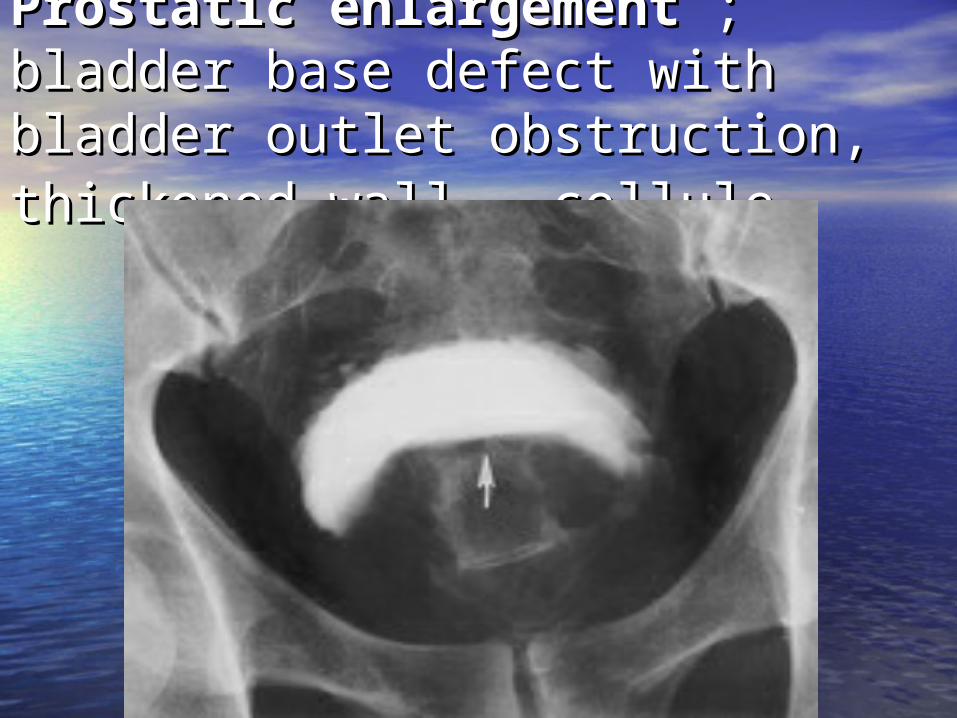
Prostatic enlargementProstatic enlargement ; ; bladder base defect with bladder bladder base defect with bladder outlet obstruction, thickened wall , outlet obstruction, thickened wall , cellulecellule
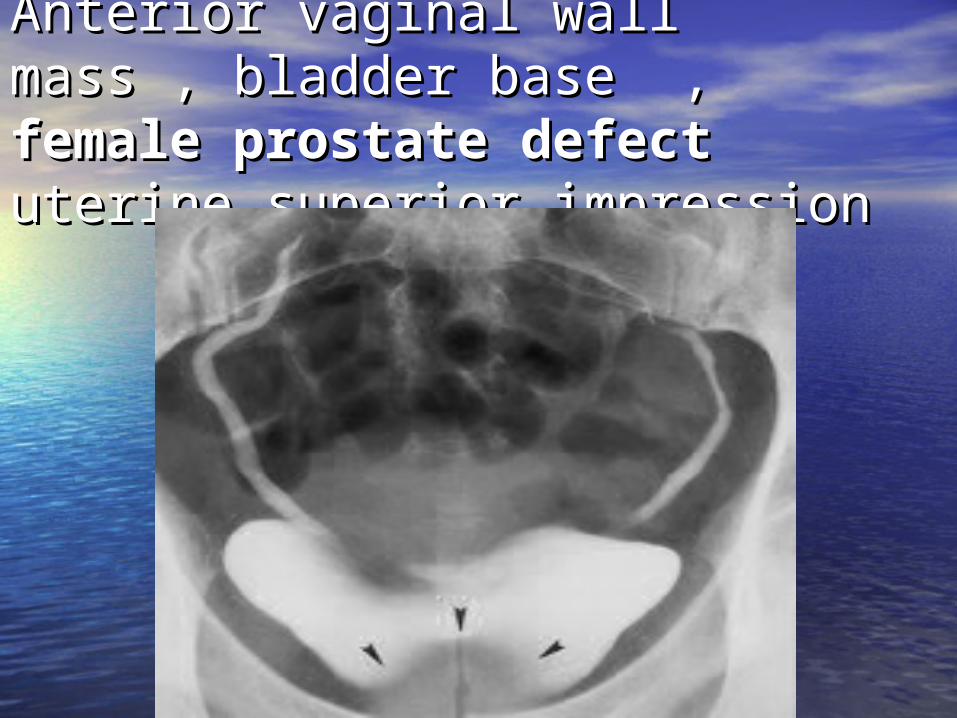
Anterior vaginal wall mass , Anterior vaginal wall mass , bladder base , bladder base , female female prostate defectprostate defectuterine superior impression uterine superior impression

Bladder Bladder
•Early filling image and Early filling image and post void film :post void film :
most sensitive image most sensitive image for evaluate filling for evaluate filling defectdefect
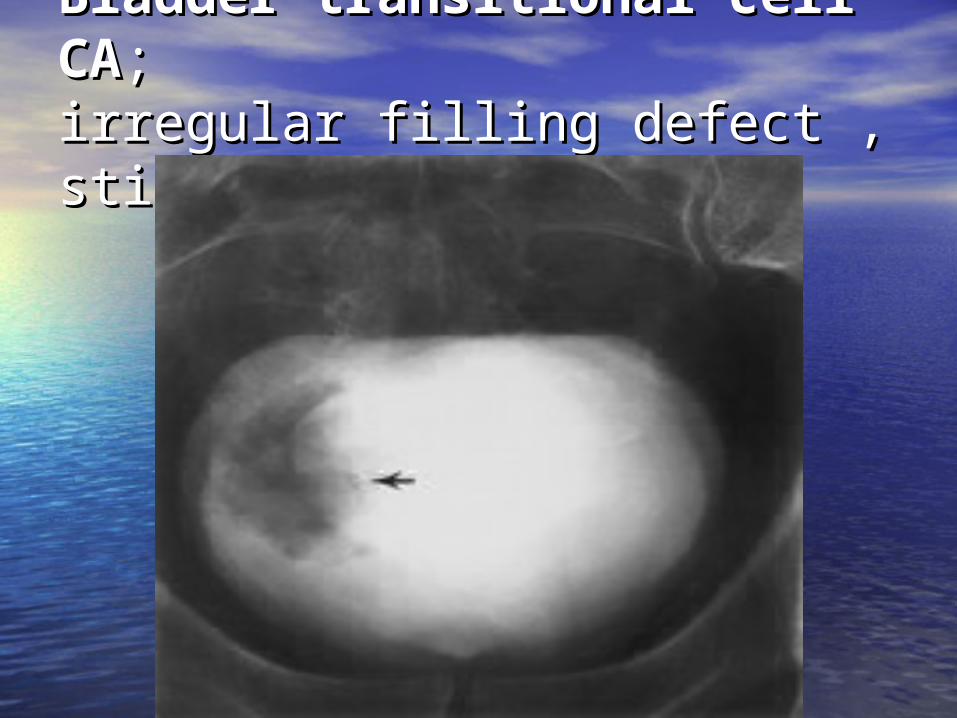
Bladder transitional cell CABladder transitional cell CA;;irregular filling defect , stipple irregular filling defect , stipple signsign
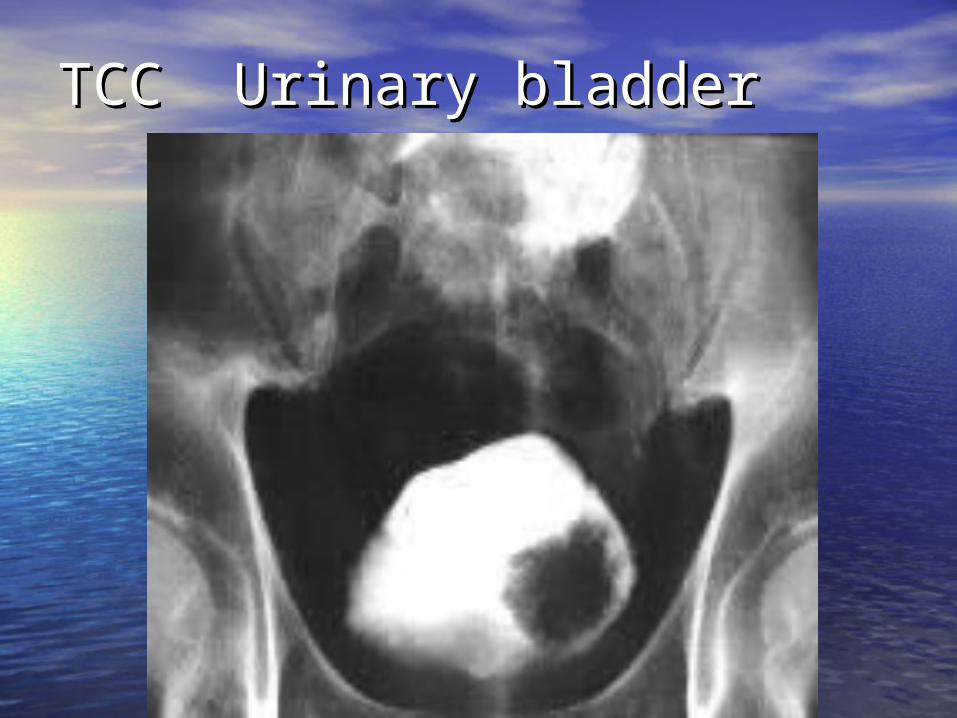
TCC Urinary bladder TCC Urinary bladder
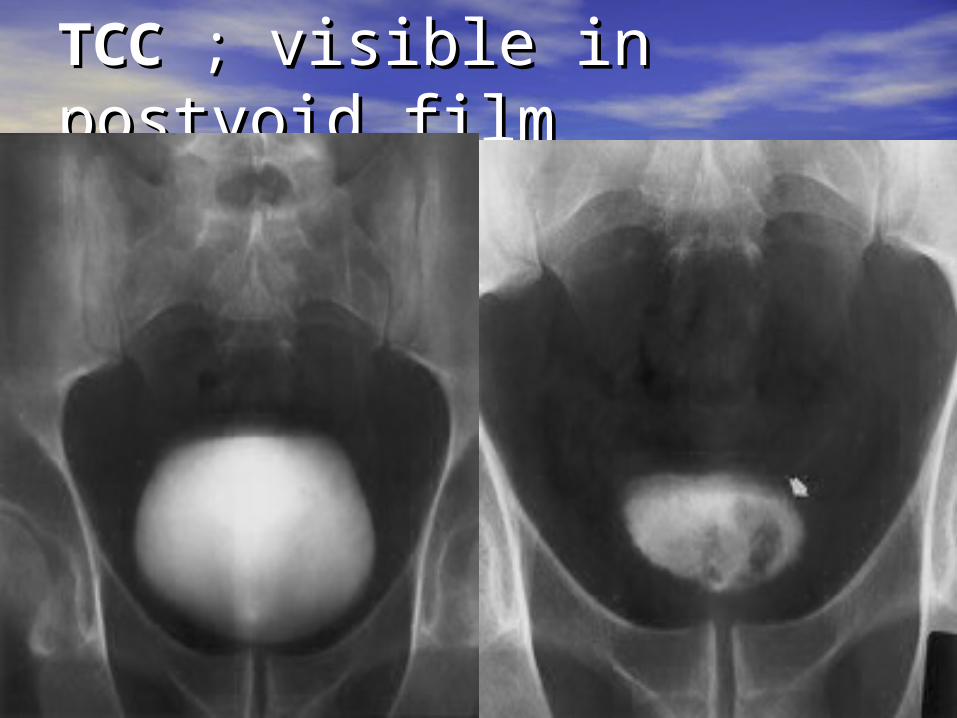
TCCTCC ; ; visible in postvoid visible in postvoid filmfilm
ConclusionConclusion• Tailored urographic study allow Tailored urographic study allow
*Optimal visualization of urinary *Optimal visualization of urinary tract tract
*Provide diagnostic detail *Provide diagnostic detail
• Important :Important :
* Good technique * Good technique
* Understanding limitation * Understanding limitation
* Basic rule of interpretation * Basic rule of interpretation
* Correlate with other imaging * Correlate with other imaging modalitymodality

Thanks youThanks you