ischemic colitis. introduction caused by a reduction in intestinal blood flow from the mesenteric...
TRANSCRIPT

Ischemic Colitis
Introduction Caused by a reduction in intestinal blood
flow from the mesenteric vasculature Arises from occlusion, vasospasm and/or
hypoperfusion Consequences can include sepsis, bowel
infarction, and death

Introduction, cont. Most frequently
affecting the elderly Types:
Non-gangrenous: 85%; transient, resolves
Severe gangrenous: 15%; life-threatening


Anatomy of the Colon Superior Mesenteric Artery
arises from the aorta at L1 or L2 supplies entire small intestine except for the
proximal duodenum 4 branches
inferior pancreaticoduodenal middle colic right colic ileocolic arteries

Anatomy of the Colon, cont. Inferior Mesenteric
Artery arises from the aorta
3 cm proximal to the aortic bifurcation at L3
Branches: left colic artery sigmoid arteries superior rectal artery
Anatomy of the Colon, cont. Ischemic damage to the rectum is rare
because it gets collateral flow from IMA and iliac arteries.
Colon has collateral circulation, but weak points exist: narrow terminal branches supply the splenic
flexure and the rectosigmoid junction these watershed areas are most prone to
ischemia during hypotension


Pathophysiology of Colonic Ischemia Non-occlusive ischemia
affects the watershed areas of the colon
Left colon affected in 75% of patients
Only 25% affects the splenic flexure
Rectum is less than 5%
Pathophysiology of Colonic Ischemia
Aortoiliac surgery post-op rate of colonic
ischemia is 1-7% risk factors include older
age, renal disease, prior colectomy, longer cross-clamping time
risk reduction techniques are not effective

Pathophysiology of Colonic Ischemia Cardiopulmonary bypass
rare, but lethal complication high mortality rate increased severity risk factors include long op
times, inotropes, intraaortic balloon pumps
Pathophysiology of Colonic Ischemia Myocardial infarction
“Ischemic colitis was described in 14 of 100 patients who underwent a colonoscopy within a mean of 15 days after an MI.”
Hemodialysis due to atherosclerosis, diabetes, HD-induced
hypotension

Pathophysiology of Colonic Ischemia Acquired and hereditary
thrombotic conditions unclear if any patients
with colonic ischemia should undergo evaluation for hypercoagulability based on limited data
younger patients should be worked up

Clinical Manifestations Abdominal pain Mild to moderate rectal bleeding or bloody
diarrhea Three progressive clinical stages
Hyperactive phase: soon after hypoperfusion or occlusion; severe pain; conservative measures
Paralytic phase: pain diminishes, but becomes diffuse Shock phase: electrolyte imbalances occur,
dehydration, requires surgery
Diagnosis DDx: infectious colitis,
IBD, diverticulitis, carcinoma,
Labs: increased lactate, LDH, CPK or amylase may indicate advanced tissue damage
Increased WBC may indicate gangrenous necrosis

Diagnosis Plain abdominal x-ray:
non-specific; only valuable in advanced cases if present, portend a worse prognosis
CT scan: typical findings include thickening of the
bowel in segmental pattern generally nonspecific and may be normal
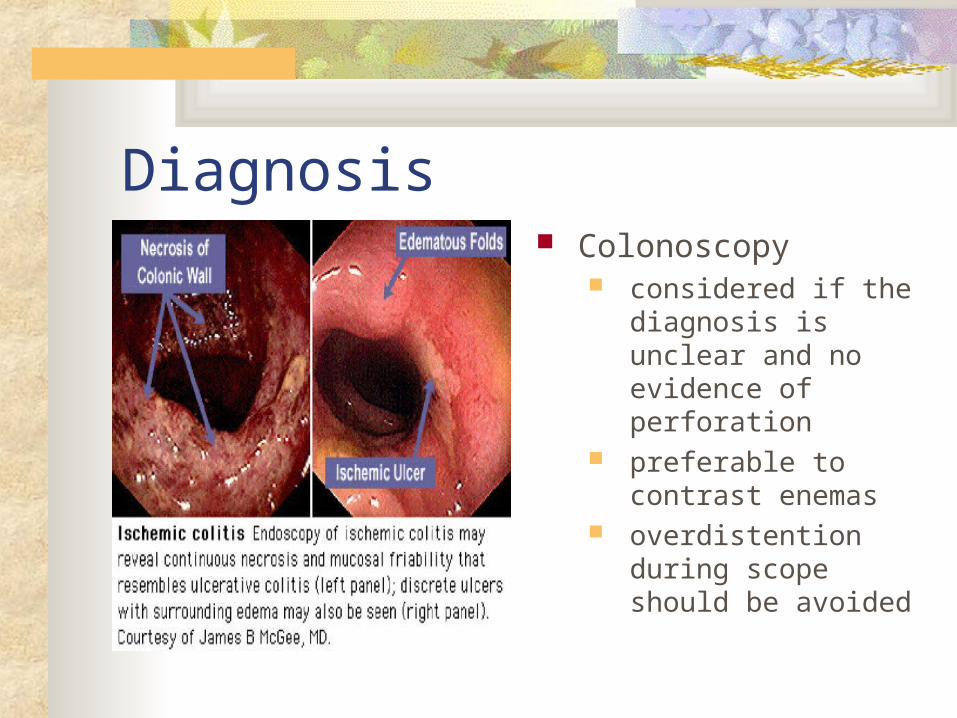
Diagnosis Colonoscopy
considered if the diagnosis is unclear and no evidence of perforation
preferable to contrast enemas
overdistention during scope should be avoided

Diagnosis Colonoscopy, cont.
Findings: pale mucosa petechial bleeding hemorrhagic nodules cyanotic mucosa “single-stripe sign” rectal sparing

Severe redness, swelling, and almost a bluish appearance is seen in the wall of the bowel. This is a very severe case of ischemic colitis. It may and may not heal and often when it does heal, it heals with scarring.

Diagnosis Barium enema
abnormalities are segmental and transient
‘thumbprinting’ is most suggestive and is seen early in the disease; seen in 75% of cases of non-gangrenous ischemia

Barium enema showing stricture formation
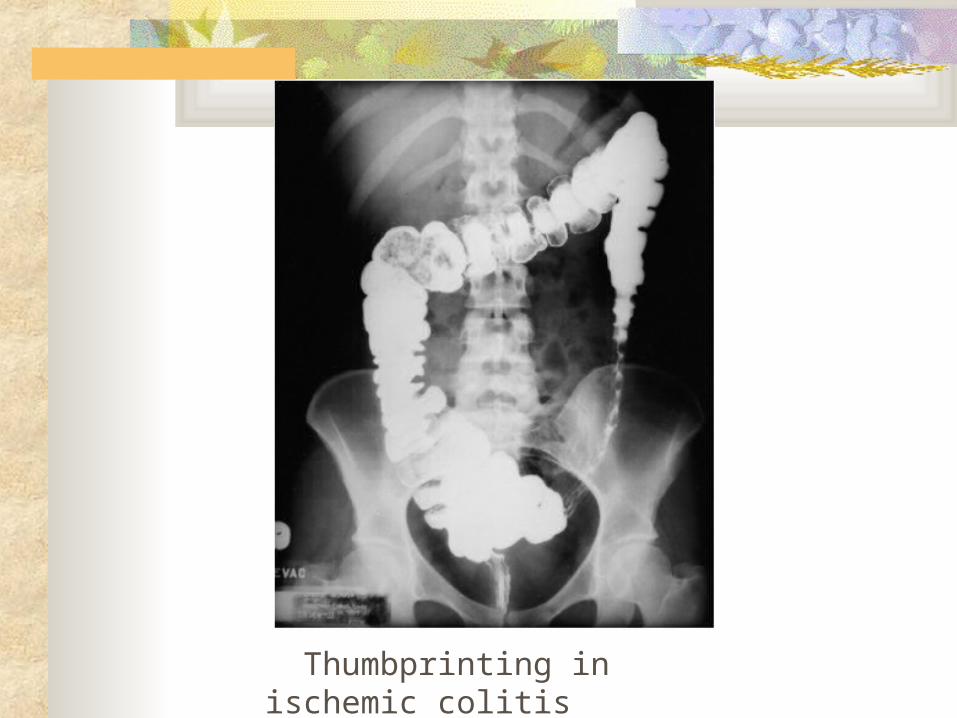
Thumbprinting in ischemic colitis

Diagnosis Angiography
rarely helpful in most cases, colonic blood flow will have
returned already may be indicated if other studies cannot
exclude acute proximal mesenteric ischemia not always available; many contraindications

Diagnosis Laparoscopy
useful for a “second” look
however, pneumoperitoneum greatly effects mesenteric blood flow

Diagnosis MRA
pathologic conditions of the mesenteric vessels that can be identified with this technique include: stenosis or occlusion of the proximal mesenteric
arteries aneurysms portal hypertension vascular invasion by carcinoma
Treatment Embolectomy, or
endarterectomy are only rarely used
depends on type and severity of ischemic colitis

Treatment, cont. Non-occlusive ischemia
supportive care which includes IVF, bowel rest
broad spectrum abx for severe cases NGT if ileus is present vasodilators are not recommended if pt deteriorates, laparotomy and segmental
resection are indicated

Treatment, cont. Colonic infarction
require surgical intervention bowel preps can precipitate perforation or
toxic dilatation despite surgery, mortality following large
bowel infarction is as high as 50 to 75 percent
Prognosis Depends on the severity and comorbidities non-occlusive types improve within one or
two days gangrenous ischemia is associated with a
mortality rate as high as 50 to 70 percent anticoagulation tx is only indicated in pts with
mesenteric venous thrombosis or cardiac embolization

Summary Majority of pts develop
non-gangrenous ischemia which usually resolves
Bloody diarrhea appears within 24 hours of the acute abdominal pain
Dx based on H&P, xray, or endoscopy

Summary Angiography or laparoscopy are rarely needed MRA more recently introduced to r/o mesenteric
arterial or venous disease Treatment is generally supportive in the absence
of colonic gangrene or perforation IVF, Abx, bowel rest Hypercoag w/up for younger pts with recurring
ischemia is recommended