investigational medicinal product dossier omega-3 …
TRANSCRIPT
PURPOSE IMPD, version 1, February 5th 2016 1 of 46
INVESTIGATIONAL MEDICINAL PRODUCT DOSSIER
Omega-3 fatty acids and placebo
Version 1, dated February 5th 2016
Authors:
Matthijs Bossong
Gregor Berger
Conrad Vissink
Hugo Schurgast
Inge Winter
PURPOSE IMPD, version 1, February 5th 2016 2 of 46
TABLE OF CONTENTS
LIST OF TABLES .................................................................................................................. 4
1. INTRODUCTION……….. ................................................................................................... 5
2. CHEMICAL PHARMACEUTICAL DATA… ....................................................................... 6
2.1.P MEDICINAL PRODUCT… ............................................................................................ 6
2.1.P.1 Description and Composition of the Medicinal Product .......................................... 6
2.1.P.2 Pharmaceutical Development ................................................................................ 6
2.1.P.2.1 Components of the Medicinal Product ......................................................... 6
2.1.P.2.2 Medicinal Product ........................................................................................ 7
2.1.P.2.3 Manufacturing Process Development .......................................................... 7
2.1.P.2.4 Container Closure System ........................................................................... 7
2.1.P.2.5 Microbiological Attributes ............................................................................. 7
2.1.P.2.6 Compatibility ................................................................................................ 7
2.1.P.3 Manufacture .......................................................................................................... 7
2.1.P.3.1 Manufacturer(s) ........................................................................................... 7
2.1.P.3.2 Batch Formula ............................................................................................. 8
2.1.P.3.3 Description of Manufacturing Process and Process Controls ....................... 8
2.1.P.3.4 Controls of Critical Steps and Intermediates ................................................ 8
2.1.P.3.5 Process Validation and/or Evaluation .......................................................... 8
2.1.P.4 Control of Excipients ............................................................................................. 8
2.1.P.4.1 Specifications .............................................................................................. 8
2.1.P.4.2 Analytical Procedures .................................................................................. 9
2.1.P.4.3 Validation of Analytical Procedures ............................................................. 9
2.1.P.4.4 Justification of Specifications ....................................................................... 9
2.1.P.4.5 Excipients of Human or Animal Origin ......................................................... 9
2.1.P.4.6 Novel Excipients .......................................................................................... 9
2.1.P.5 Control of Medicinal Product ................................................................................. 9
2.1.P.5.1 Specifications .............................................................................................. 9
2.1.P.5.2 Analytical Procedures ................................................................................ 10
2.1.P.5.3 Validation of Analytical Procedures ........................................................... 10
2.1.P.5.4 Batch Analyses .......................................................................................... 10
2.1.P.5.5 Characterization on impurities ................................................................... 10
2.1.P.5.6 Justification of Specification(s) .................................................................. 10
2.1.P.6 Reference Standards .......................................................................................... 10
2.1.P.7 Container Closure System................................................................................... 11
PURPOSE IMPD, version 1, February 5th 2016 3 of 46
2.1.P.8 Stability.... ........................................................................................................... 11
2.1.P.8.1 Stability testing parameters ....................................................................... 11
2.1.P.8.2 Stability testing storage ............................................................................. 11
2.1.P.8.3 Stability testing scope ................................................................................ 12
2.2 NON-CLINICAL PHARMACOLOGY, PHARMACOKINETICS AND TOXICOLOGY ..... 13
2.2.1 Acute single dose toxicity ....................................................................................... 13
2.2.2 Repeated dose toxicity ........................................................................................... 13
2.2.3 Genotoxicity / Carcinogenicity ................................................................................. 15
2.2.4 Reproductive and developmental toxicity ................................................................ 17
2.2.5 List of studies Conducted & References ................................................................. 18
2.2.6 References ............................................................................................................. 19
2.3 CLINICAL DATA ........................................................................................................... 20
2.3.1 Clinical pharmacology............................................................................................. 20
2.3.2 Clinical pharmacokinetics ....................................................................................... 22
2.3.3 Human exposure .................................................................................................... 23
2.3.4 Overall risk and benefit assessment ....................................................................... 23
2.3.5 Conclusion .............................................................................................................. 23
2.4 OVERALL RISK AND BENEFIT ASSESSMENT .......................................................... 25
2.4.1 PUFAs and potential adverse effects in UHR ......................................................... 25
2.4.2 PUFAs and potential adverse effects in schizophrenia ........................................... 25
2.4.3 Specific adverse effects of PUFAs .......................................................................... 25
2.4.4 Risks versus benefits of PUFAs in emerging psychosis .......................................... 27
2.5 CONCLUSION ............................................................................................................... 27
APPENDIX 1 ....................................................................................................................... 32
APPENDIX 2 ....................................................................................................................... 33
APPENDIX 3 ....................................................................................................................... 34
APPENDIX 4 ....................................................................................................................... 35
APPENDIX 5 ....................................................................................................................... 36
APPENDIX 6 ....................................................................................................................... 39
APPENDIX 7 ....................................................................................................................... 42
APPENDIX 8 ....................................................................................................................... 45
PURPOSE IMPD, version 1, February 5th 2016 4 of 46
LIST OF TABLES
Table 1 Qualitative composition of omega-3 capsules ........................................................... 6
Table 2 Qualitative composition of placebo capsules ............................................................. 6
Table 3 Release and Shelf-life Specification Product with active substance .......................... 9
Table 4 Release and Shelf-life Specification Placebo .......................................................... 10
Table 5 Stability testing parameters and methods ............................................................... 11
Table 6 Stability testing schedule of withdrawals ................................................................. 12
Table 7 Studies examining EPA/DHA repeated dose toxicity ............................................... 14
Table 8 Studies examining EPA/DHA genotoxicity / carcinogenicity .................................... 15
Table 9 Studies examining EPA/DHA reproductive and developmental toxicity ................... 17
Table 10 List of referenced non-clinical studies on omega-3 fatty acids ............................... 18
PURPOSE IMPD, version 1, February 5th 2016 5 of 46
1. INTRODUCTION
This Clinical Trial Application presents information relating to omega-3 capsules containing 180
mg of EPA, 120 mg of DHA and 1.9 mg mixed tocopherols (antioxidant), as well as placebo
capsules. Omega-3 is being investigated in subjects at ultra-high risk for developing psychosis,
for the prevention of clinical transition to psychosis.
Omega-3 fatty acids are used worldwide as nutritional supplements with important physical and
psychosocial health benefits and has been studied elaborately in (the prevention of) various
disease states, ranging from cardiovascular disease to psychosis. Pre-clinical data demonstrate
very low level of oral toxicity of omega-3 fatty acids.
Due to the generally high level of overlap between IMPDs and Investigator Brochures, and the
resulting cross referencing between the documents, it has been decided to combine both
documents in the current IMPD.
PURPOSE IMPD, version 1, February 5th 2016 6 of 46
2. CHEMICAL PHARMACEUTICAL DATA
2.1.P MEDICINAL PRODUCT
2.1.P.1 Description and Composition of the Medicinal Product
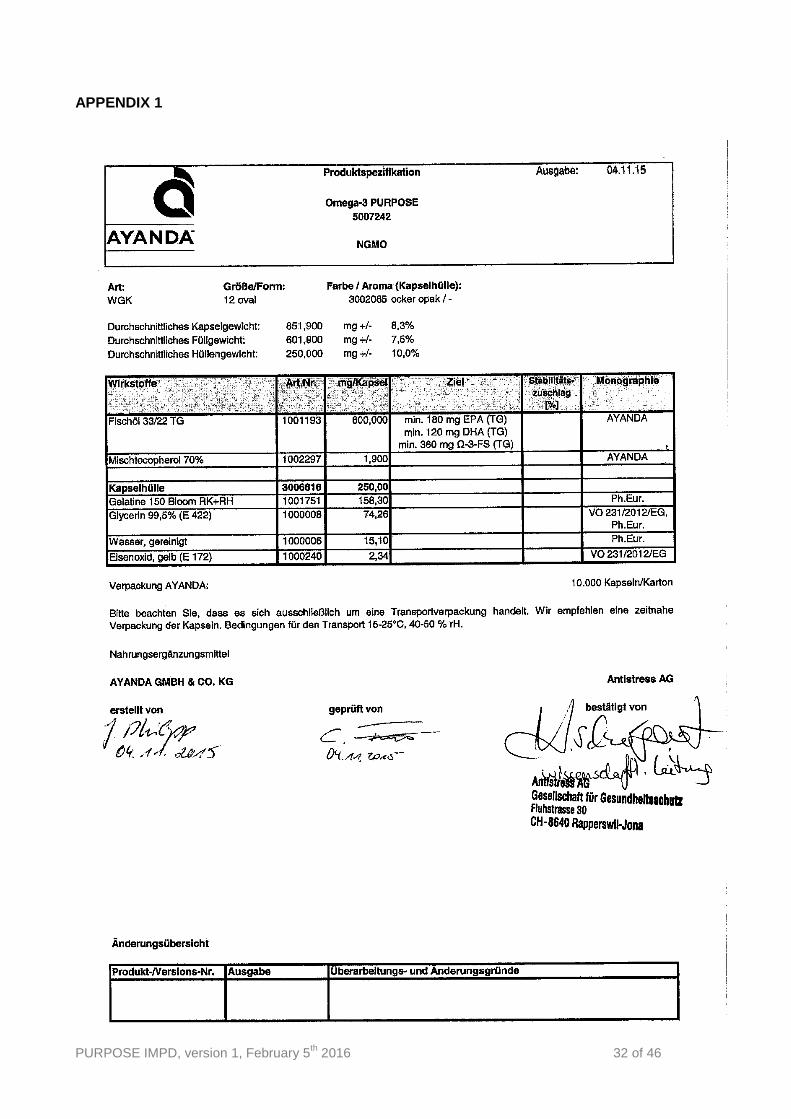
Omega-3 capsules of 600 mg, containing 180 mg of EPA, 120 mg of DHA, 60 mg of other
omega-3 fatty acids and 1.9 mg mixed tocopherols (antioxidant), as well as placebo capsules.
The qualitative composition of the verum capsules is listed in Table 1. Please also see Appendix
1.
Table 1 Qualitative composition of omega-3 capsules
Component Reference to
standards Function
Fish oil 33/22 TG In house Active ingredient
Mixed tocopherol In house Active ingredient
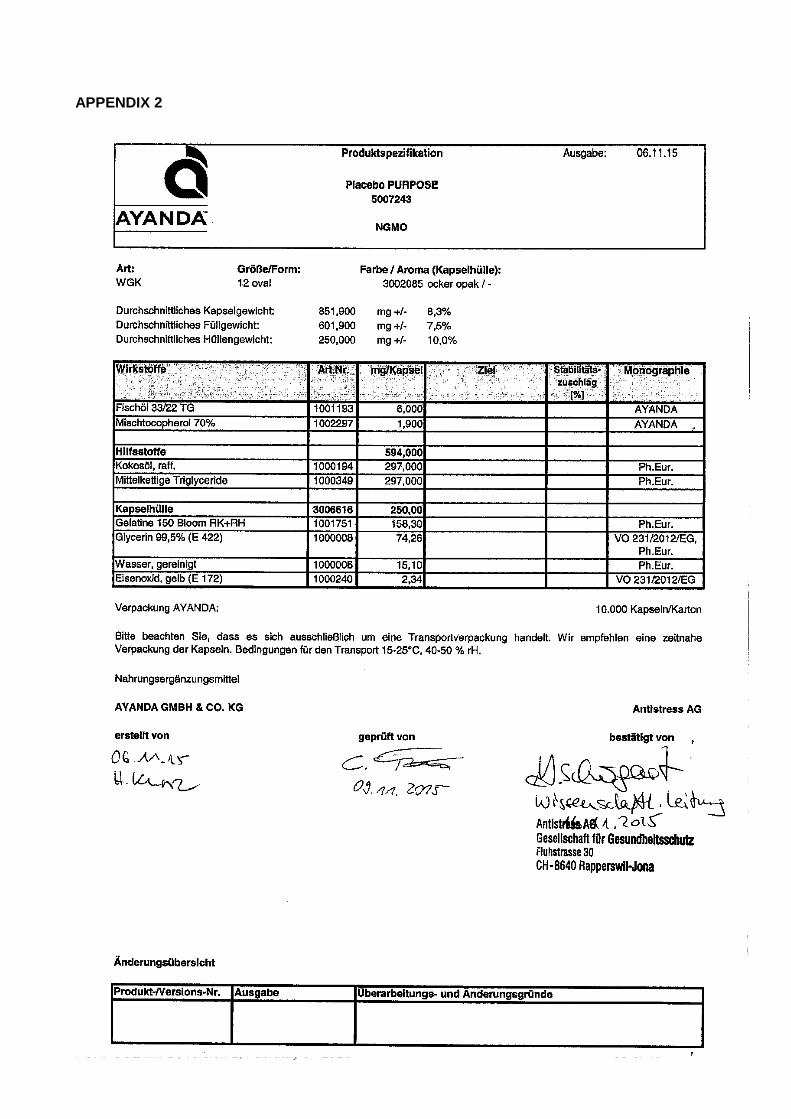
The qualitative composition of the placebo capsules is listed in Table 2. Please also see
Appendix 2.
Table 2 Qualitative composition of placebo capsules
Component Reference to
standards Function
Fish oil 33/22 TG In house Active ingredient
Mixed tocopherol In house Active ingredient
Coconut oil Ph. Eur. Active ingredient
Medium-chain triglyceride Ph. Eur. Active ingredient
2.1.P.2 Pharmaceutical Development
The gel capsules with verum and placebo which are used for the present study have been used
in a clinical trial conducted by Amminger et al. (2010) in a similar subject population.
2.1.P.2.1 Components of the Medicinal Product
The mixed tocopherol (vitamin E) is a common addition to omega-3 fatty acid capsules, and
has been added to the placebo as well, in order to align the content of the capsules on
factors which may influence pharmacokinetics/-dynamics and/or therapeutic effect. Fish oil
is added to the placebo capsule in order to prevent unblinding due to differences in smell
PURPOSE IMPD, version 1, February 5th 2016 7 of 46
and taste compared to the verum capsule. Placebo capsules will contain a 1:1 combination
of coconut oil and medium chain triglycerides because it does not contain polyunsaturated
fatty acids and has no impact on omega-3 fatty acid metabolism.
2.1.P.2.2 Medicinal product
No additional relevant information applicable.
2.1.P.2.3 Manufacturing Process Development
The manufacturing process development is described in detail in section 2.1.P.3.3.
2.1.P.2.4 Container Closure System
The capsules will be packed in customized polyethylene bags or in tubular film made
of Polyethylene for the transport to ACE Pharmaceuticals in the Netherlands, where
the capsules will be bottled using 400 ml (dark brown) glass bottles with a pressure
seal lid.
2.1.P.2.5 Microbiological Attributes
Not applicable.
2.1.P.2.6 Compatibility
Not applicable.
2.1.P.3 Manufacture
2.1.P.3.1 Manufacturer(s)
Manufacturing and QP release:
AYANDA GmbH & Co. KG
Am Huenengrab 20
16928 Pritzwalk
Germany
QP release:
Antistress / Burgerstein
Fluhstrasse 30
8640 Rapperswil-Jona
Switzerland
PURPOSE IMPD, version 1, February 5th 2016 8 of 46
Packaging, blinding, labeling and QP release:
ACE Pharmaceuticals BV
Schepenveld 41
3891 ZK Zeewolde
The Netherlands
Phone +31 36 5227201
Fax +31 36 5229096
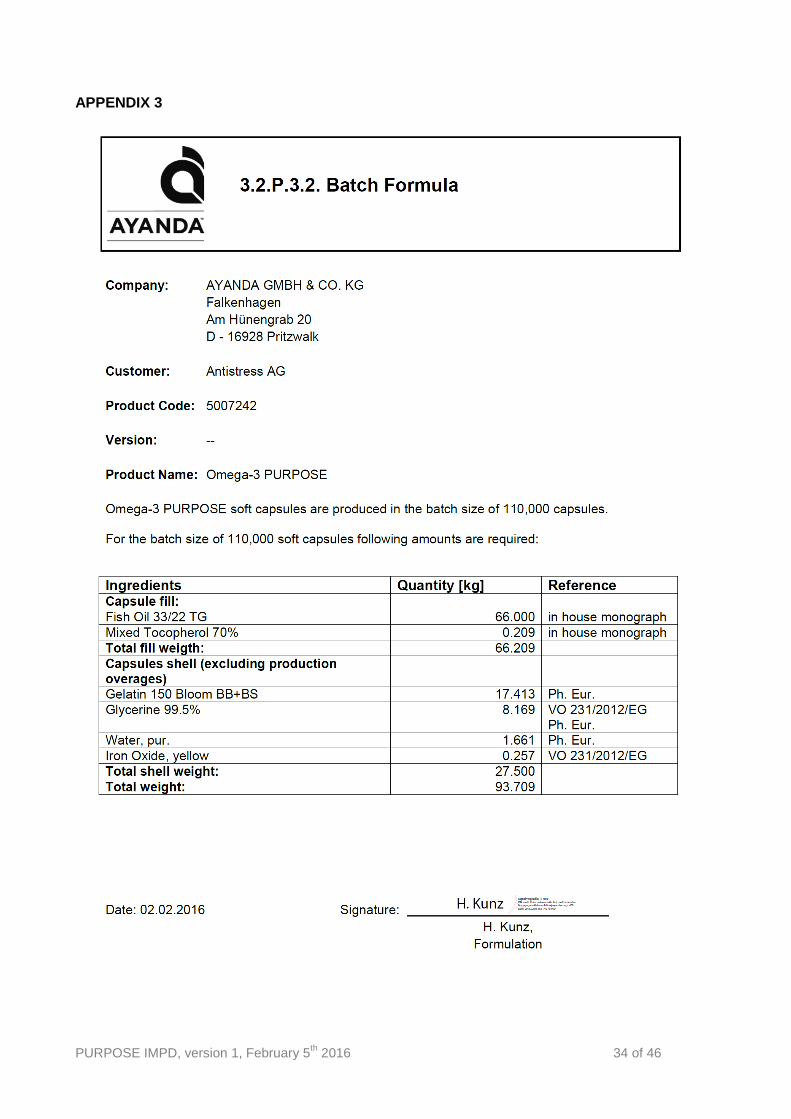
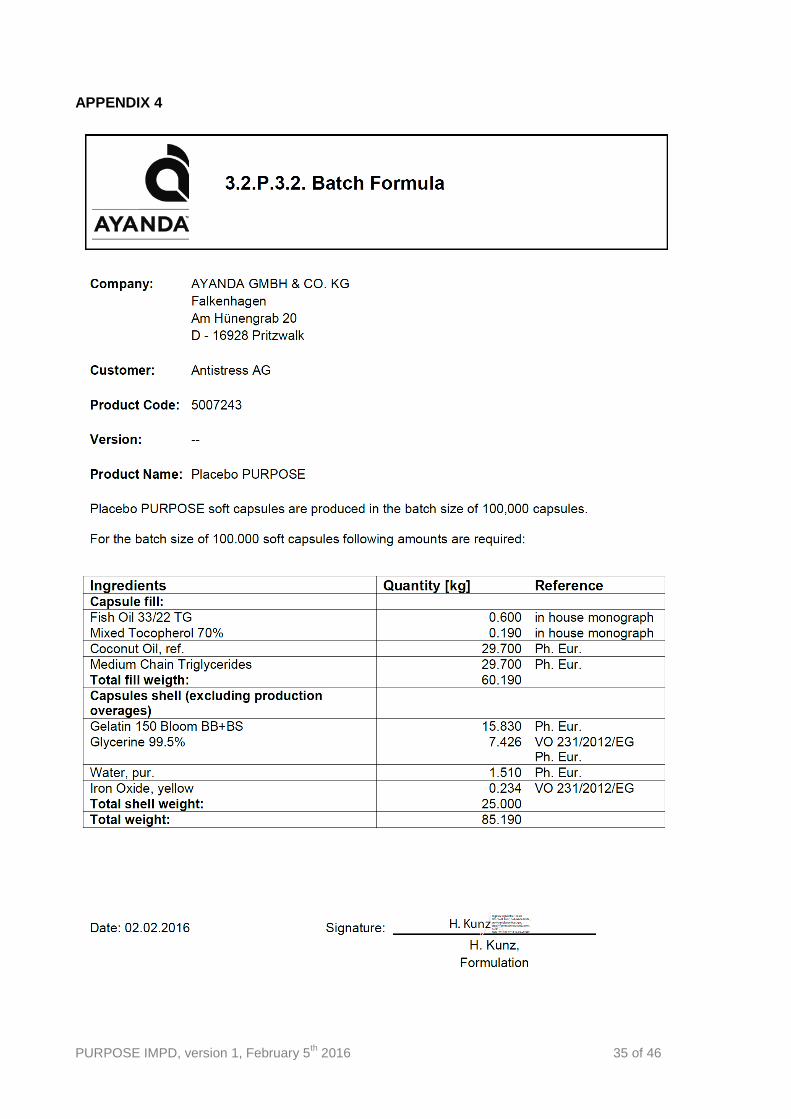
2.1.P.3.2 Batch Formula
Please see Appendix 3 and 4 for the batch formula of omega-3 and placebo capsules,
respectively.
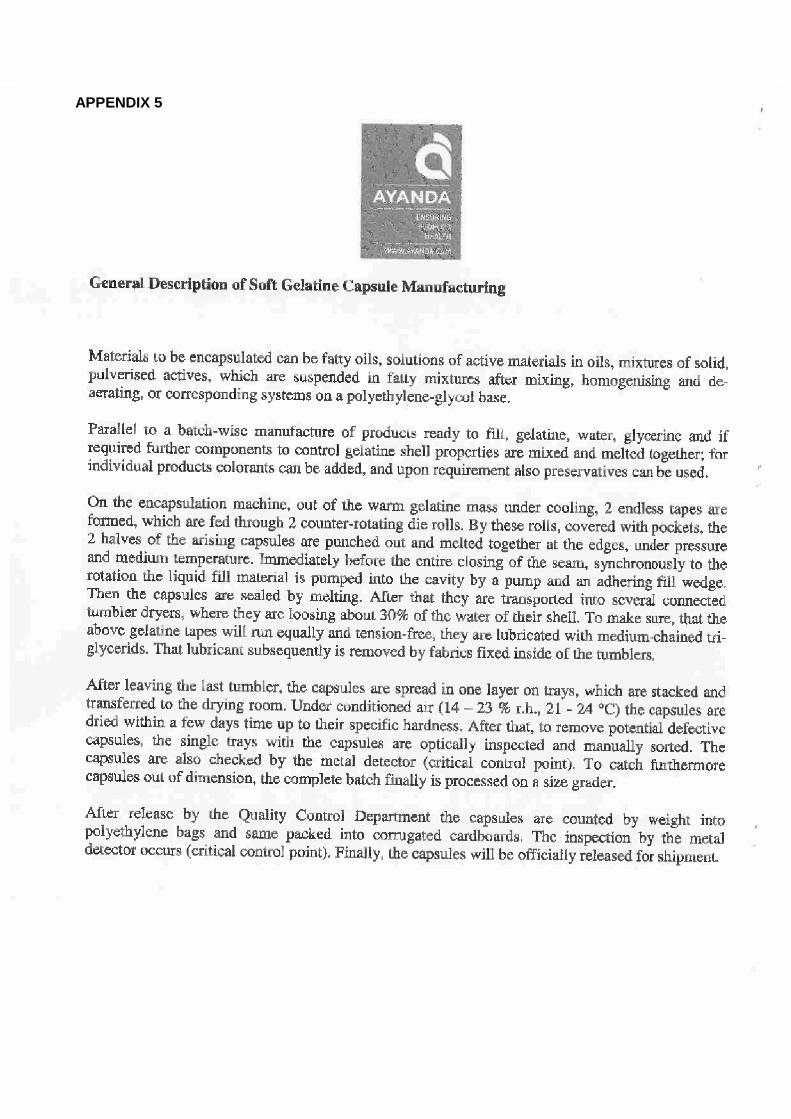
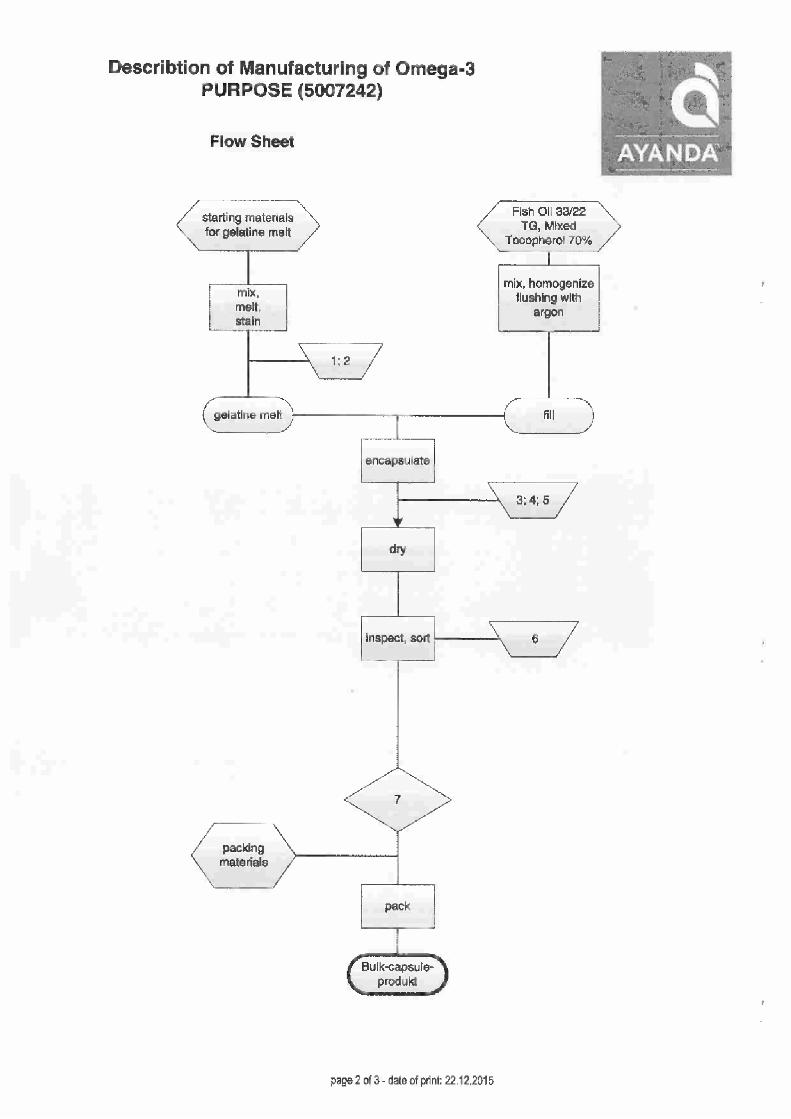
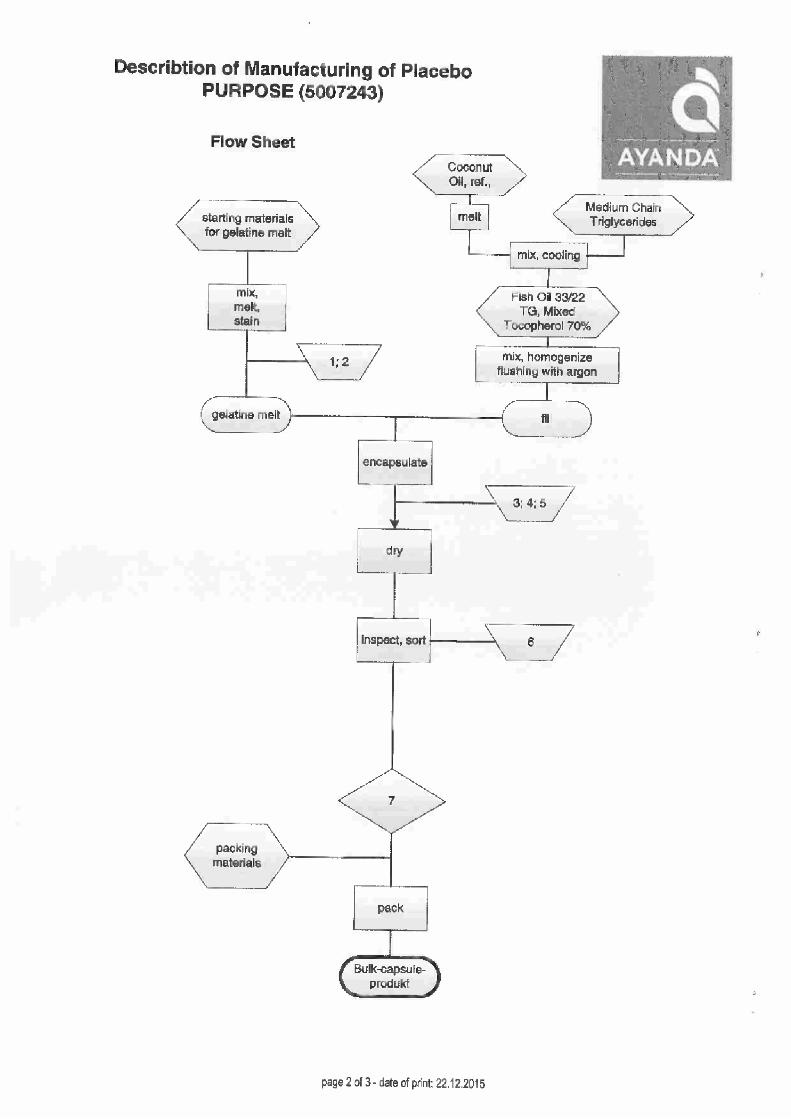
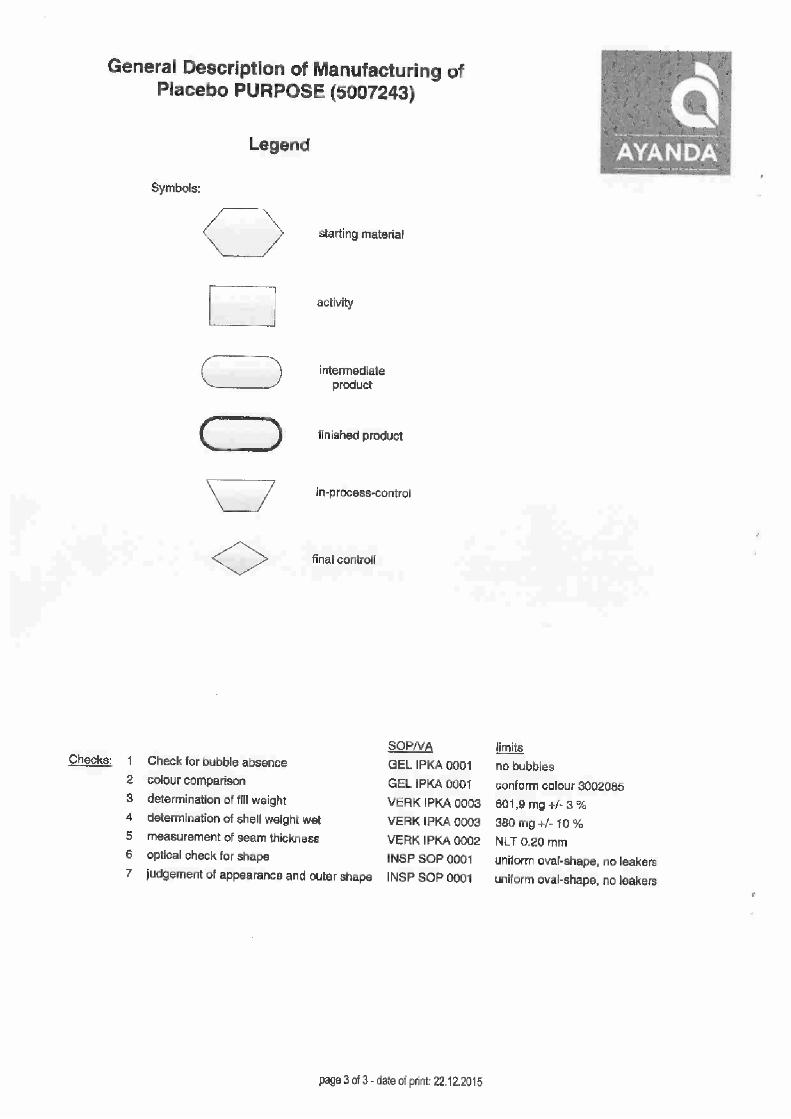
2.1.P.3.3 Description of Manufacturing Process and Process Controls
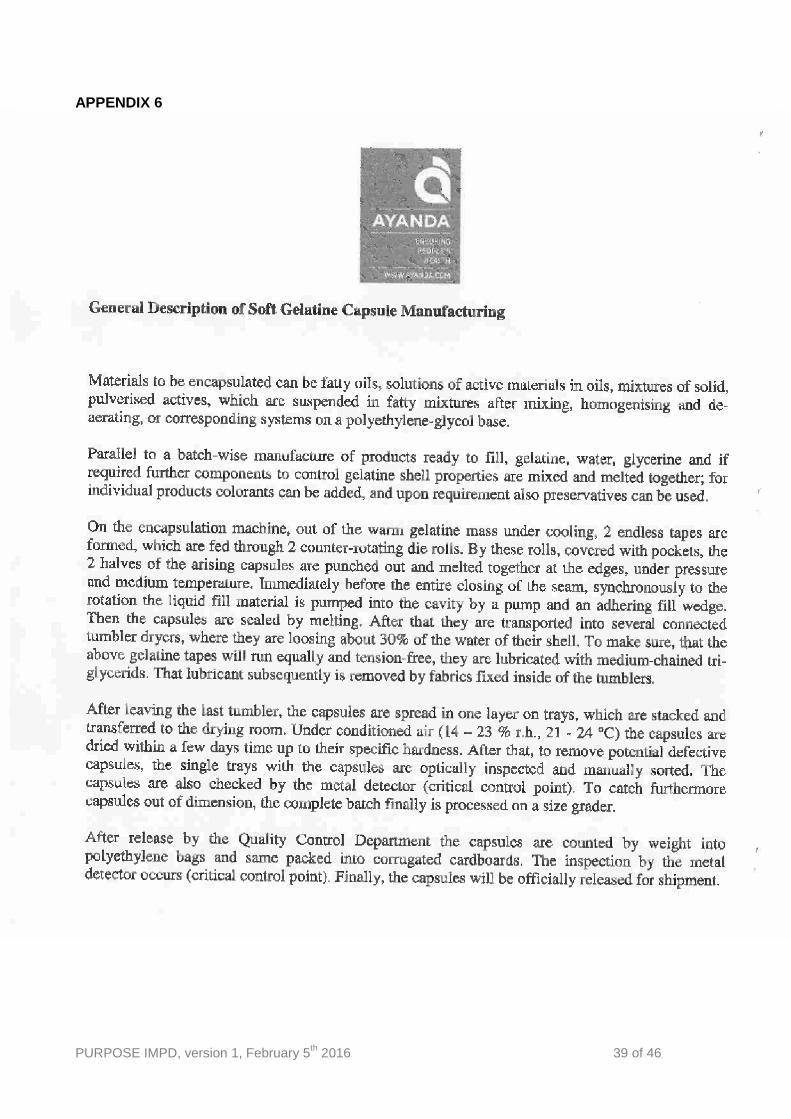
Please see Appendix 5 and 6 for a general description of the manufacturing process as well
as a flow chart mentioning the in-process controls for omega-3 fatty acids and placebo,
respectively.
2.1.P.3.4 Controls of Critical Steps and Intermediates
Please see Appendix 5 and 6 for a general description of the manufacturing process as well
as a flow chart mentioning the in-process controls for omega-3 fatty acids and placebo,
respectively.
2.1.P.3.5 Process Validation and/or Evaluation
The currently manufactured product Omega-3 Purpose (item code: 5007242; batch
number: 30016995) has not been validated. Production of soft gelatin capsules with an oil
mixture filling is a well-established procedure at Ayanda GmbH & Co. KG. The used
equipment is qualified and the staff is well trained. Additionally, the manufacturing site in
Germany is certified according to EU-GMP rules, International Featured Standard and
Global Standard for Food Safety. The parameters on the certificate of analysis are within
the specification.
2.1.P.4 Control of Excipients
2.1.P.4.1 Specifications
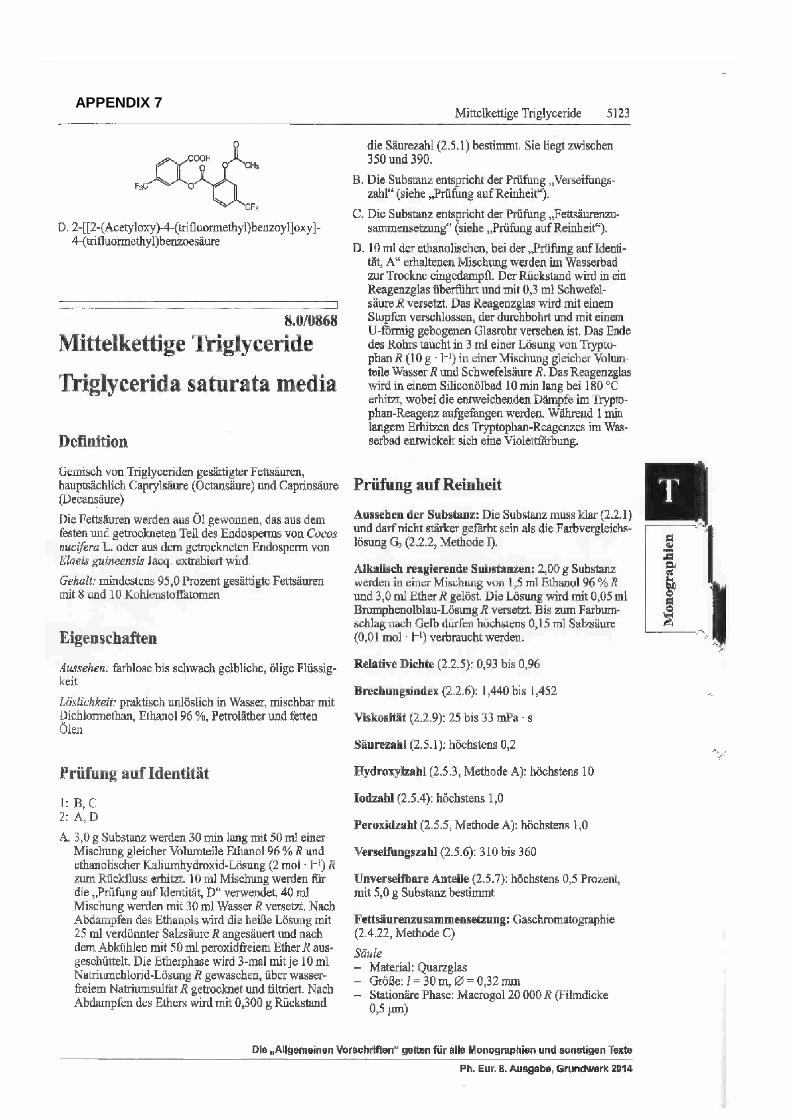
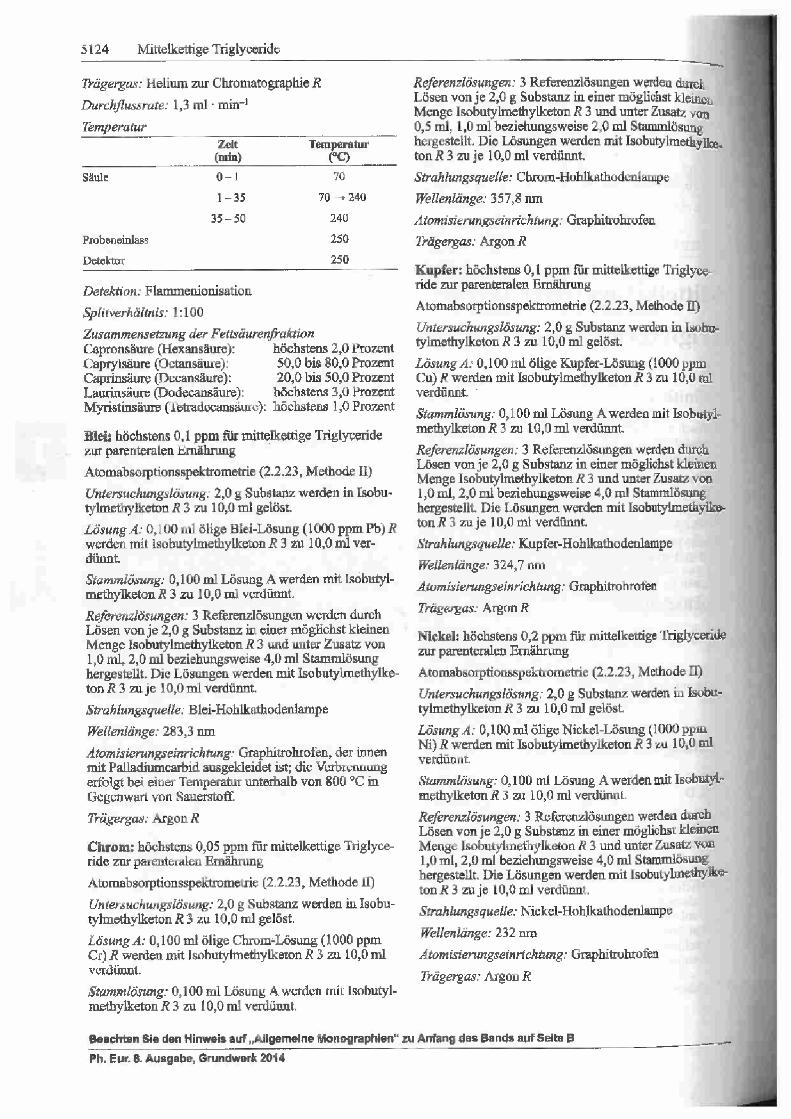
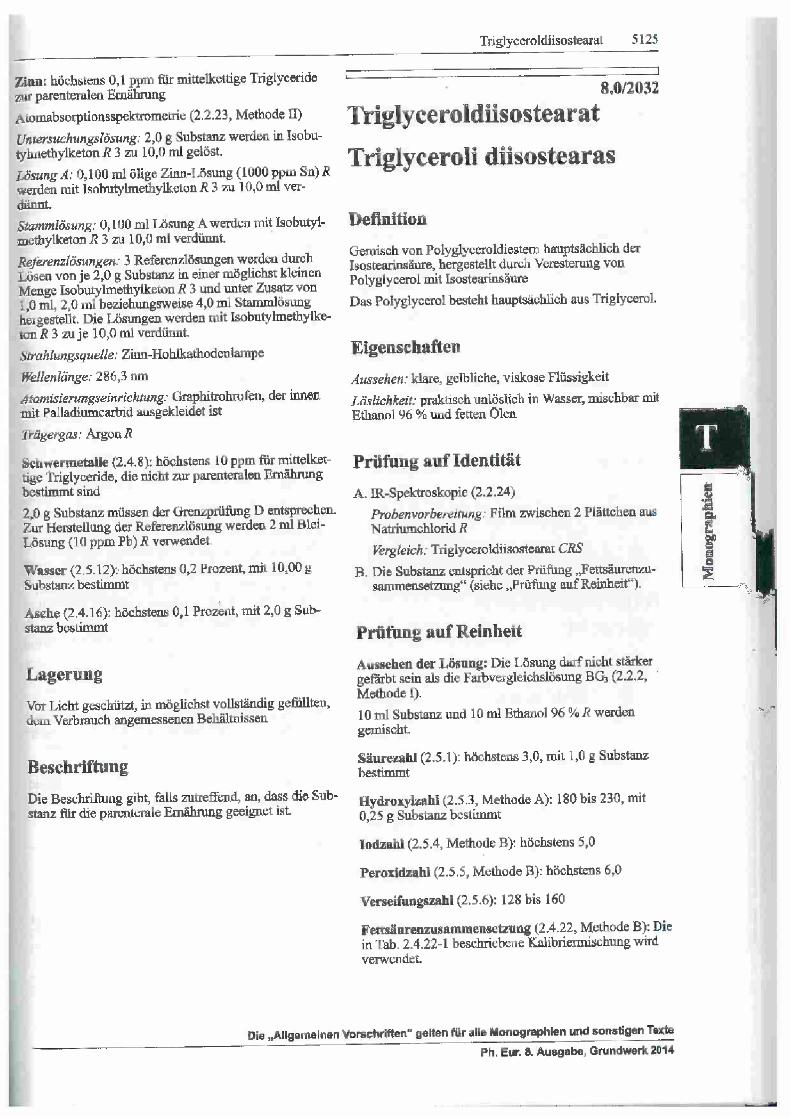
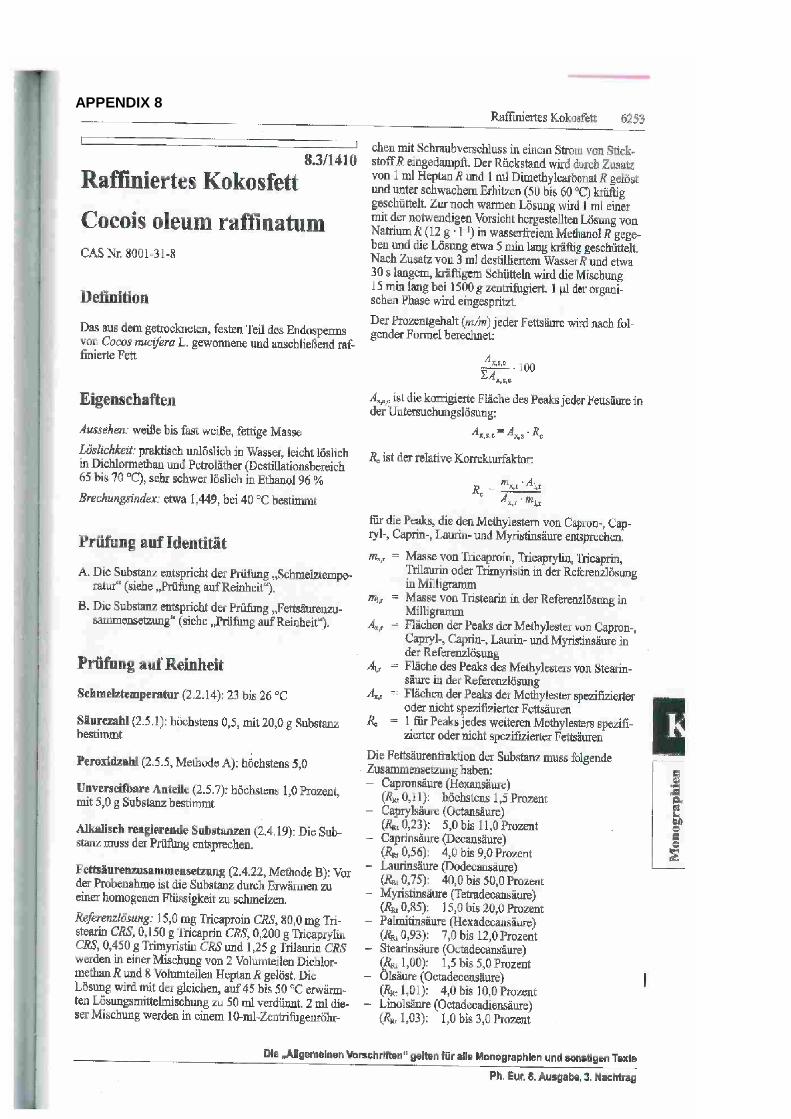
Please see Appendix 7 and 8 for the Ph. Eur. monographies of the excipients medium
chain triglycerides and coconut oil (version 8.3) used in our products. All raw materials are

PURPOSE IMPD, version 1, February 5th 2016 9 of 46
Ph. Eur. Grade and are tested according to Ph. Eur. methods or with validated methods, if
applicable.
2.1.P.4.2 Analytical Procedures
The analytical procedures are available on request.
2.1.P.4.3 Validation of Analytical procedures
All Ph. Eur. methods used for our standard analytical regime are per se regarded as
validated.
2.1.P.4.4 Justification of Specifications
Not applicable.
2.1.P.4.5 Excipients of Human or Animal Origin
Not applicable.
2.1.P.4.6 Novel Excipients
Not applicable.
2.1.P.5 Control of Medicinal Product
2.1.P.5.1 Specifications
Table 3 Release and Shelf-life Specification Product with active substance
Test item Method Acceptance Criteria
Description Visual observation 12 oval clear, slightly yellow soft gel capsule
ID GC, Ph.Eur. 2.2.28 Retention times of EPA/DHA complies with CRS
Uniformity of filling mass Ph.Eur. Complies
Assay GC, Ph.Eur. 2.2.28 Min. 180 mg EPA (TG) Min. 120 mg DHA (TG) Min. 360 mg Omega3 (TG) Shelf life spec.: Min. -10%
Peroxide Value PH.Eur. 2.5.5 Max. 5 Shelf-life spec.: for Information
Anisidine Value PH.Eur. 2.5.36 Max. 20 Shelf-life spec.: for Information
Disintegration Ph.Eur. 2.9.1 max. 30 min
PURPOSE IMPD, version 1, February 5th 2016 10 of 46
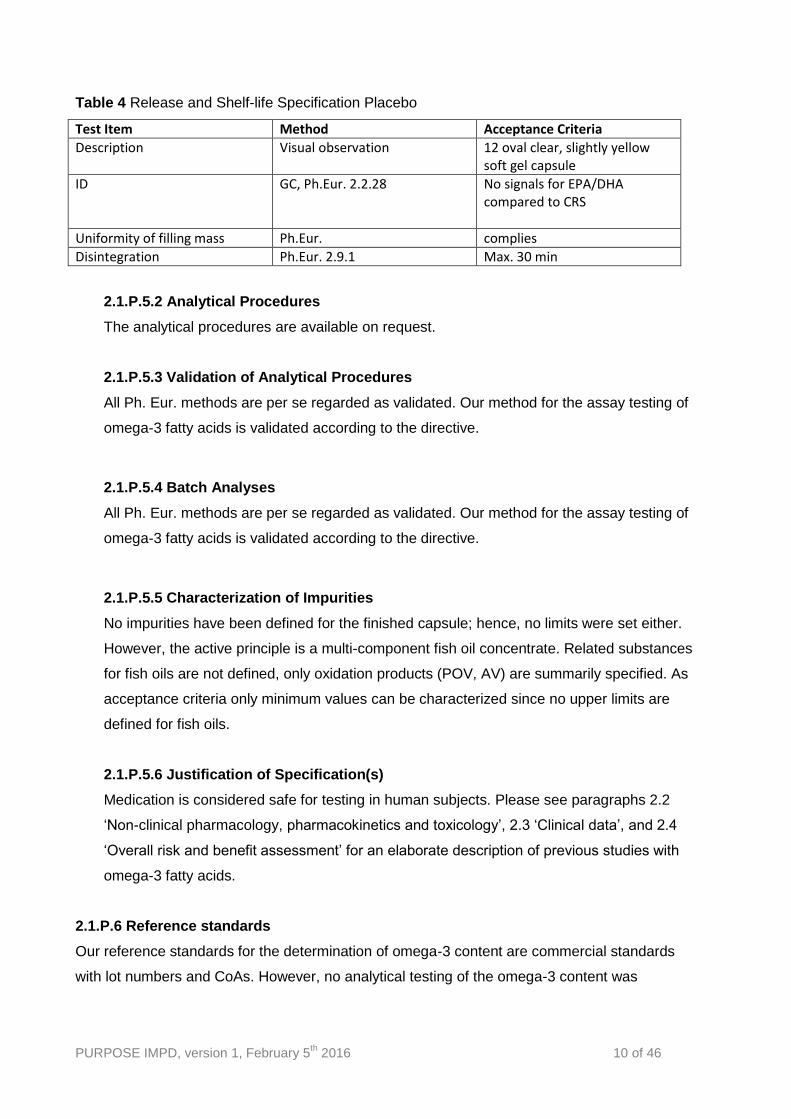
Table 4 Release and Shelf-life Specification Placebo
Test Item Method Acceptance Criteria
Description Visual observation 12 oval clear, slightly yellow soft gel capsule
ID GC, Ph.Eur. 2.2.28
No signals for EPA/DHA compared to CRS
Uniformity of filling mass Ph.Eur. complies
Disintegration Ph.Eur. 2.9.1 Max. 30 min
2.1.P.5.2 Analytical Procedures
The analytical procedures are available on request.
2.1.P.5.3 Validation of Analytical Procedures
All Ph. Eur. methods are per se regarded as validated. Our method for the assay testing of
omega-3 fatty acids is validated according to the directive.
2.1.P.5.4 Batch Analyses
All Ph. Eur. methods are per se regarded as validated. Our method for the assay testing of
omega-3 fatty acids is validated according to the directive.
2.1.P.5.5 Characterization of Impurities
No impurities have been defined for the finished capsule; hence, no limits were set either.
However, the active principle is a multi-component fish oil concentrate. Related substances
for fish oils are not defined, only oxidation products (POV, AV) are summarily specified. As
acceptance criteria only minimum values can be characterized since no upper limits are
defined for fish oils.
2.1.P.5.6 Justification of Specification(s)
Medication is considered safe for testing in human subjects. Please see paragraphs 2.2
‘Non-clinical pharmacology, pharmacokinetics and toxicology’, 2.3 ‘Clinical data’, and 2.4
‘Overall risk and benefit assessment’ for an elaborate description of previous studies with
omega-3 fatty acids.
2.1.P.6 Reference standards
Our reference standards for the determination of omega-3 content are commercial standards
with lot numbers and CoAs. However, no analytical testing of the omega-3 content was
PURPOSE IMPD, version 1, February 5th 2016 11 of 46
performed on the delivered batch. Please note that this will be part of the stability program
(paragraph 2.1.P.8).
2.1.P.7 Container Closure System
The gel capsules used in the clinical trial will be packed in dark brown glass bottles, which are
closed with a pressure seal lid in order to maximize stability of the capsules as well as possible
(i.e. minimize exposure to light and air). The bottles will be packed in cardboard boxes to further
protect the capsules from light.
2.1.P.8 Stability
All commercially available omega-3 fatty acid products manufactured by Antistress / Burgerstein
have been proven stable for a period of 36 months, assessed with the stability testing methods
as described below. They never experienced any problems in guaranteeing the stability of their
capsules for a period of 36 months.
Stability testing needs to be done for the current batch of capsules, and will be performed by
SGS Institut Fresenius GmbH, Berlin, Germany. By accelerated stability testing of the verum
capsules stored at 40°C/75%RH, a 24-month stability of samples can be assessed within six
months. All tests will be carried out at SGS’ laboratories accredited according to
DIN/EN/ISO/IEC 17025. Climatic chambers for controlled stability storage are referring to GMP
conditions. Please note that 1) stability studies on verum capsules will be initiated prior to the
start of the clinical trial to ensure stability of capsules, and 2) there are no reasons to expect that
the placebo product will undergo changes in physical characteristics or degradation.
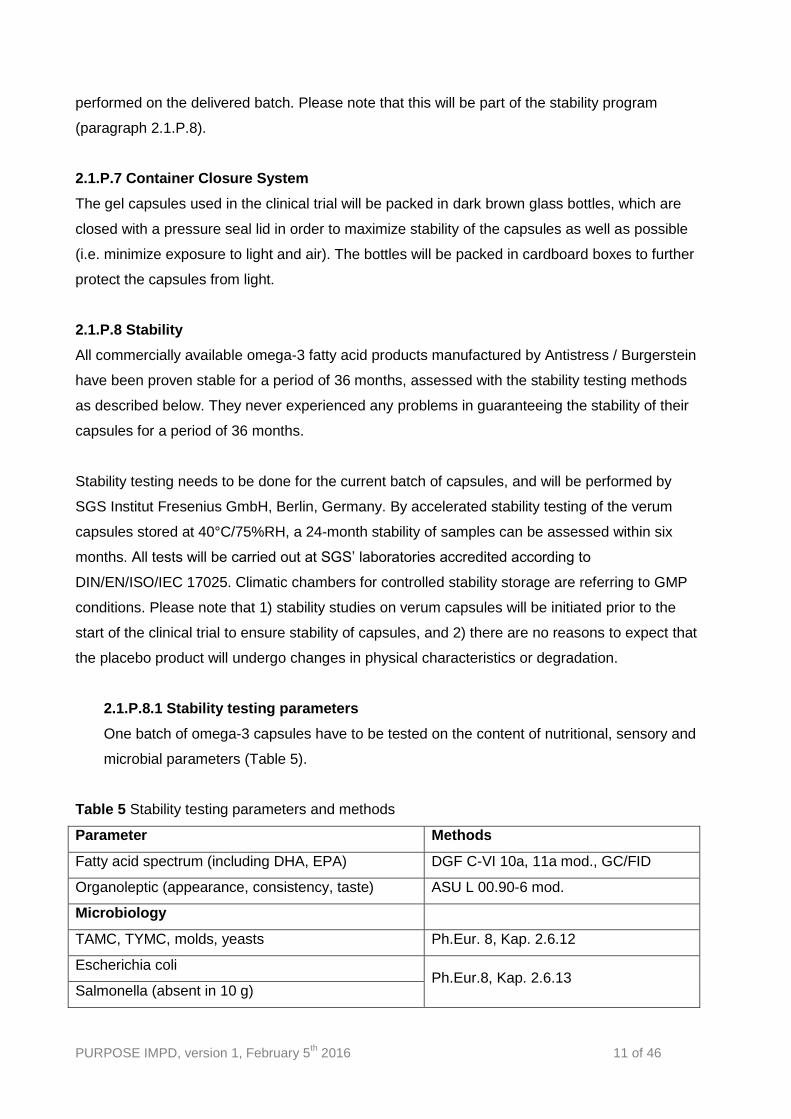
2.1.P.8.1 Stability testing parameters
One batch of omega-3 capsules have to be tested on the content of nutritional, sensory and
microbial parameters (Table 5).
Table 5 Stability testing parameters and methods
Parameter Methods
Fatty acid spectrum (including DHA, EPA) DGF C-VI 10a, 11a mod., GC/FID
Organoleptic (appearance, consistency, taste) ASU L 00.90-6 mod.
Microbiology
TAMC, TYMC, molds, yeasts Ph.Eur. 8, Kap. 2.6.12
Escherichia coli Ph.Eur.8, Kap. 2.6.13
Salmonella (absent in 10 g)
PURPOSE IMPD, version 1, February 5th 2016 12 of 46
Staphylococcus aureus (absent in 1 g)
Bile-tolerant gram-negative bacteria
2.1.P.8.2 Stability testing storage
Samples are checked upon arrival at SGS on its completeness and compliance with the
documentation provided by the client and on its sound condition. Each single sample
including packaging is labelled. Samples are stored under controlled conditions regarding
room temperature, stress conditions and protected from light. Stability storage referrers to
GMP conditions with continuous 24/7 control of temperature and documentation. Under the
assumption of a shelf life of 24 months the stability study is set up for a speeded period of
time (6 month). Samples for analysis are taken from the chamber at distinct points of time
(removal at t=X months).
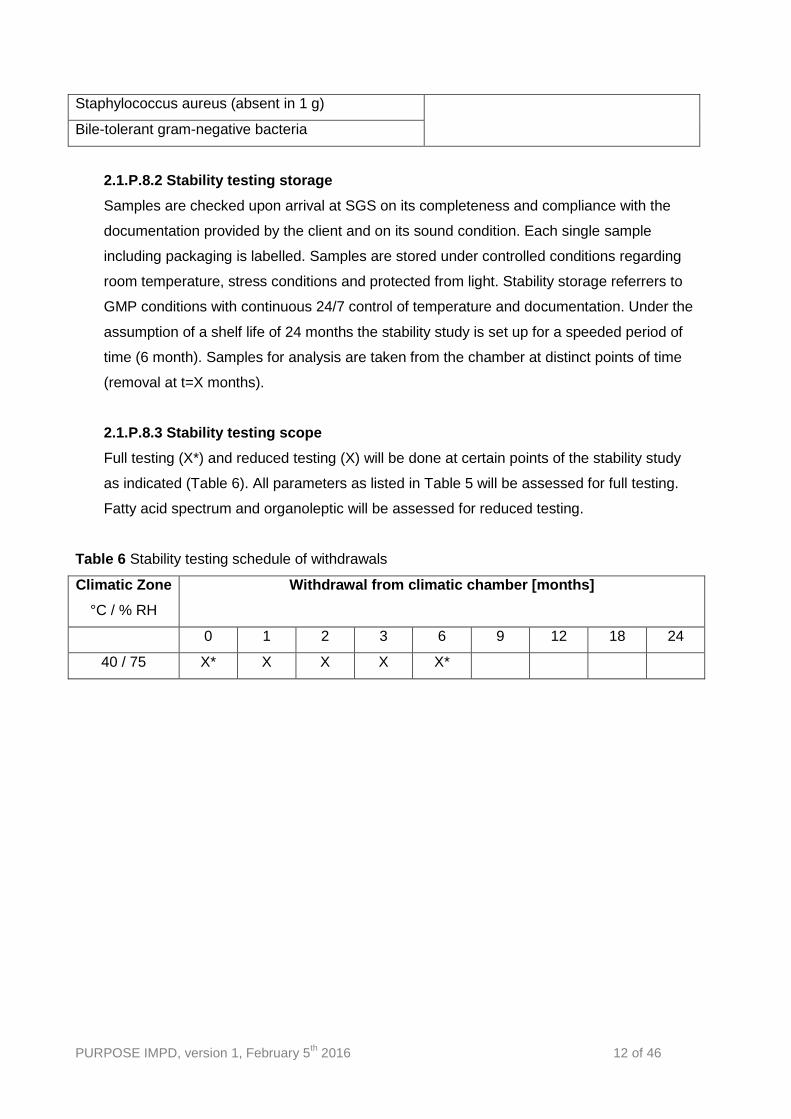
2.1.P.8.3 Stability testing scope
Full testing (X*) and reduced testing (X) will be done at certain points of the stability study
as indicated (Table 6). All parameters as listed in Table 5 will be assessed for full testing.
Fatty acid spectrum and organoleptic will be assessed for reduced testing.
Table 6 Stability testing schedule of withdrawals
Climatic Zone
°C / % RH
Withdrawal from climatic chamber [months]
0 1 2 3 6 9 12 18 24
40 / 75 X* X X X X*
PURPOSE IMPD, version 1, February 5th 2016 13 of 46
2.2 NON-CLINICAL PHARMACOLOGY, PHARMACOKINETICS AND TOXICOLOGY
In addition to the non-clinical and clinical pharmacology, pharmacokinetics and toxicology as
described in paragraphs 2.2 and 2.3 of this IMPD, we would like to emphasize that additional
information is publically available in the Summary of Product Characteristics of registered
products containing EPA/DHA such as for example Omacor ®
(https://www.medicines.org.uk/emc/medicine/10312/SPC/Omacor/).
2.2.1 Acute single dose toxicity
No acute single dose toxicity studies for eicosapentaenoic acid (EPA) and docosahexaenoic
acid (DHA) were identified in the literature.
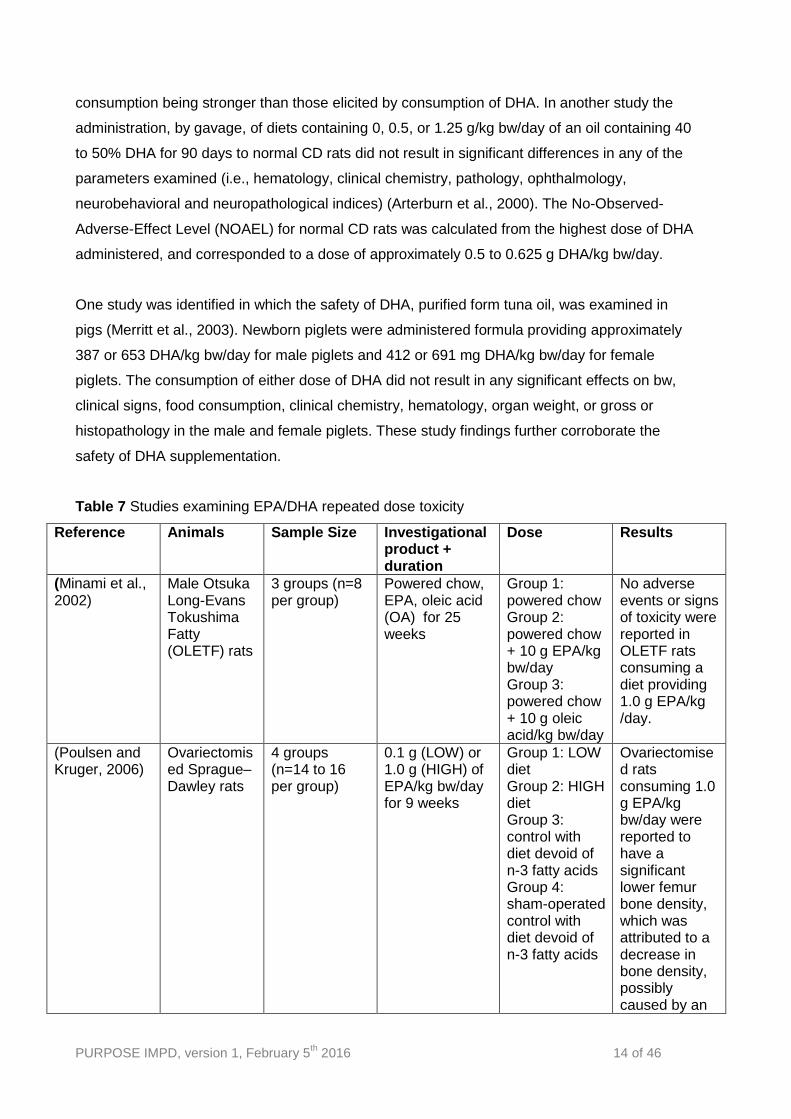
2.2.2 Repeated dose toxicity
Several animal studies were identified in which the safety of EPA and DHA consumption was
examined (Table 7). In one study, 5-week-old male Otsuka Long-Evans Tokushima Fatty
(OLETF) rats (which are used to model Type 2 diabetes) were provided with diets containing 1.0
g EPA/kg body weight(bw)/day, 1.0 g oleic acid/kg bw/day or a non-supplemented rat chow diet
until they were 30 weeks of age (Minami et al., 2002). No adverse events or signs of toxicity
were reported in OLETF rats consuming a diet providing 1.0 g EPA/kg bw/day. Moreover,
consumption of the EPA-containing diet had beneficial effects on various lipid and biochemical
parameters, causing significant reductions in plasma TG levels and abdominal fat accumulation,
and significantly improving insulin resistance. Thus, EPA was found to have a potentially
beneficial role in improving insulin sensitivity in Type 2 diabetes.
In another animal study, diets containing corn oil, corn oil and 0.1 g EPA/kg bw/day, or corn oil
and 1.0 g EPA/kg bw/day were fed to ovariectomised rats for 9 weeks (Poulsen and Kruger,
2006). No significant differences were noted between the bone breaking strength and serum
type-1 collagen concentrations of the treatment and control rats. Ovariectomised rats
consuming 1.0 g EPA/kg bw/day were reported to have a significant lower femur bone density,
which was attributed to a decrease in bone density, possibly caused by an increase in bone
resorption. In contrast to these findings, the administration of EPA to older women (mean age
79.6 years) had beneficial effects on bone density (Kruger et al., 1998).
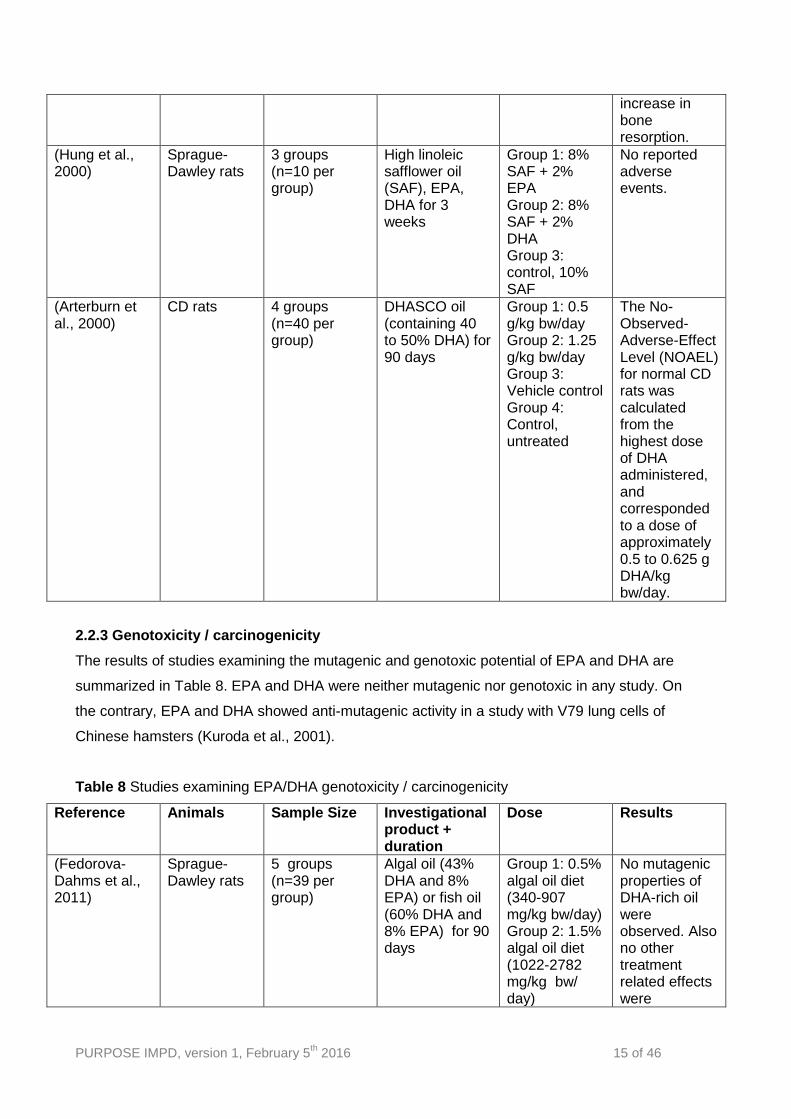
The administration of a diet containing 2% EPA or DHA ethyl esters, representing a dose of
approximately 1,000 mg/kg bw/day, to normal Sprague-Dawley rats for 3 weeks did not result in
any adverse events (Hung et al., 2000). In contrast, consumption of EPA and DHA had
beneficial effects on lipid metabolism and leukotriene synthesis, with the effects elicited by EPA
PURPOSE IMPD, version 1, February 5th 2016 14 of 46
consumption being stronger than those elicited by consumption of DHA. In another study the
administration, by gavage, of diets containing 0, 0.5, or 1.25 g/kg bw/day of an oil containing 40
to 50% DHA for 90 days to normal CD rats did not result in significant differences in any of the
parameters examined (i.e., hematology, clinical chemistry, pathology, ophthalmology,
neurobehavioral and neuropathological indices) (Arterburn et al., 2000). The No-Observed-
Adverse-Effect Level (NOAEL) for normal CD rats was calculated from the highest dose of DHA
administered, and corresponded to a dose of approximately 0.5 to 0.625 g DHA/kg bw/day.
One study was identified in which the safety of DHA, purified form tuna oil, was examined in
pigs (Merritt et al., 2003). Newborn piglets were administered formula providing approximately
387 or 653 DHA/kg bw/day for male piglets and 412 or 691 mg DHA/kg bw/day for female
piglets. The consumption of either dose of DHA did not result in any significant effects on bw,
clinical signs, food consumption, clinical chemistry, hematology, organ weight, or gross or
histopathology in the male and female piglets. These study findings further corroborate the
safety of DHA supplementation.
Table 7 Studies examining EPA/DHA repeated dose toxicity
Reference Animals Sample Size Investigational product + duration
Dose Results
(Minami et al., 2002)
Male Otsuka Long-Evans Tokushima Fatty (OLETF) rats
3 groups (n=8 per group)
Powered chow, EPA, oleic acid (OA) for 25 weeks
Group 1: powered chow Group 2: powered chow + 10 g EPA/kg bw/day Group 3: powered chow + 10 g oleic acid/kg bw/day
No adverse events or signs of toxicity were reported in OLETF rats consuming a diet providing 1.0 g EPA/kg /day.
(Poulsen and Kruger, 2006)
Ovariectomised Sprague–Dawley rats
4 groups (n=14 to 16 per group)
0.1 g (LOW) or 1.0 g (HIGH) of EPA/kg bw/day for 9 weeks
Group 1: LOW diet Group 2: HIGH diet Group 3: control with diet devoid of n-3 fatty acids Group 4: sham-operated control with diet devoid of n-3 fatty acids
Ovariectomised rats consuming 1.0 g EPA/kg bw/day were reported to have a significant lower femur bone density, which was attributed to a decrease in bone density, possibly caused by an
PURPOSE IMPD, version 1, February 5th 2016 15 of 46
increase in bone resorption.
(Hung et al., 2000)
Sprague-Dawley rats
3 groups (n=10 per group)
High linoleic safflower oil (SAF), EPA, DHA for 3 weeks
Group 1: 8% SAF + 2% EPA Group 2: 8% SAF + 2% DHA Group 3: control, 10% SAF
No reported adverse events.
(Arterburn et al., 2000)
CD rats 4 groups (n=40 per group)
DHASCO oil (containing 40 to 50% DHA) for 90 days
Group 1: 0.5 g/kg bw/day Group 2: 1.25 g/kg bw/day Group 3: Vehicle control Group 4: Control, untreated
The No-Observed-Adverse-Effect Level (NOAEL) for normal CD rats was calculated from the highest dose of DHA administered, and corresponded to a dose of approximately 0.5 to 0.625 g DHA/kg bw/day.
2.2.3 Genotoxicity / carcinogenicity
The results of studies examining the mutagenic and genotoxic potential of EPA and DHA are
summarized in Table 8. EPA and DHA were neither mutagenic nor genotoxic in any study. On
the contrary, EPA and DHA showed anti-mutagenic activity in a study with V79 lung cells of
Chinese hamsters (Kuroda et al., 2001).
Table 8 Studies examining EPA/DHA genotoxicity / carcinogenicity
Reference Animals Sample Size Investigational product + duration
Dose Results
(Fedorova-Dahms et al., 2011)
Sprague-Dawley rats
5 groups (n=39 per group)
Algal oil (43% DHA and 8% EPA) or fish oil (60% DHA and 8% EPA) for 90 days
Group 1: 0.5% algal oil diet (340-907 mg/kg bw/day) Group 2: 1.5% algal oil diet (1022-2782 mg/kg bw/ day)
No mutagenic properties of DHA-rich oil were observed. Also no other treatment related effects were

PURPOSE IMPD, version 1, February 5th 2016 16 of 46
Group 3: 5% algal oil diet (3466-8322 mg/kg bw/day) Group 4: Control, fish oil diet (3511-7155 mg/kg bw/day) Group 5: Control, basal diet
observed. Therefore, the highest Algal oil dose was considered NOAEL.
(Blum et al., 2007)
Sprague-Dawley rats
8 groups (n=10 to 30 per group)
Combination of fish oil (containing 26.7% DHA and 11.4% EPA) and DHA-algal (containing 45% DHA) for 90 days or 90 days + an additional 4-week recovery period (no treatment).
Group 1: 2000 mg/kg fish oil Group 2: 1500 mg/kg fish oil + 500 mg/kg DHA-algal oil Group 3: 1000 mg/kg fish oil + 1000 mg/kg DHA-algal oil Group 4: 2000 mg/kg DHA-algal oil Group 5: Control Group 6: 2000 mg/kg fish oil + 4 week recovery Group 7: 2000 mg/kg DHA-algal oil + 4 week recovery Group 8: Control + 4 week recovery
In the 90-day toxicity study no toxicologically significant side effects were observed in genotoxicity- and chromosomal aberration studies, following oral administration of DHA oil, both fish and algal derived. The highest dose of 2000 mg/kg bw/day was considered NOAEL.
(Abril et al., 2003)
Growing pigs (mixed breed of Landrace and Large White)
5 groups (n=29 per group)
Dried DHA-rich microalgae, DRM, (containing 22.3% DHA) added to the diet for 120 days.
Group 1: 1.10% DRM Group 2: 1.10% DRM on day 79-106 and 0.39% DRM on day 107-120 Group 3: 3.30% DRM on day 79-106 and 1.17% DRM on day 107-120 Group 4: 5.51% DRM on day 79-106
No treatment-related adverse effects were observed in these commercial strains of swine.

PURPOSE IMPD, version 1, February 5th 2016 17 of 46
and 1.94% DRM on day 107-120 Group 5: Control
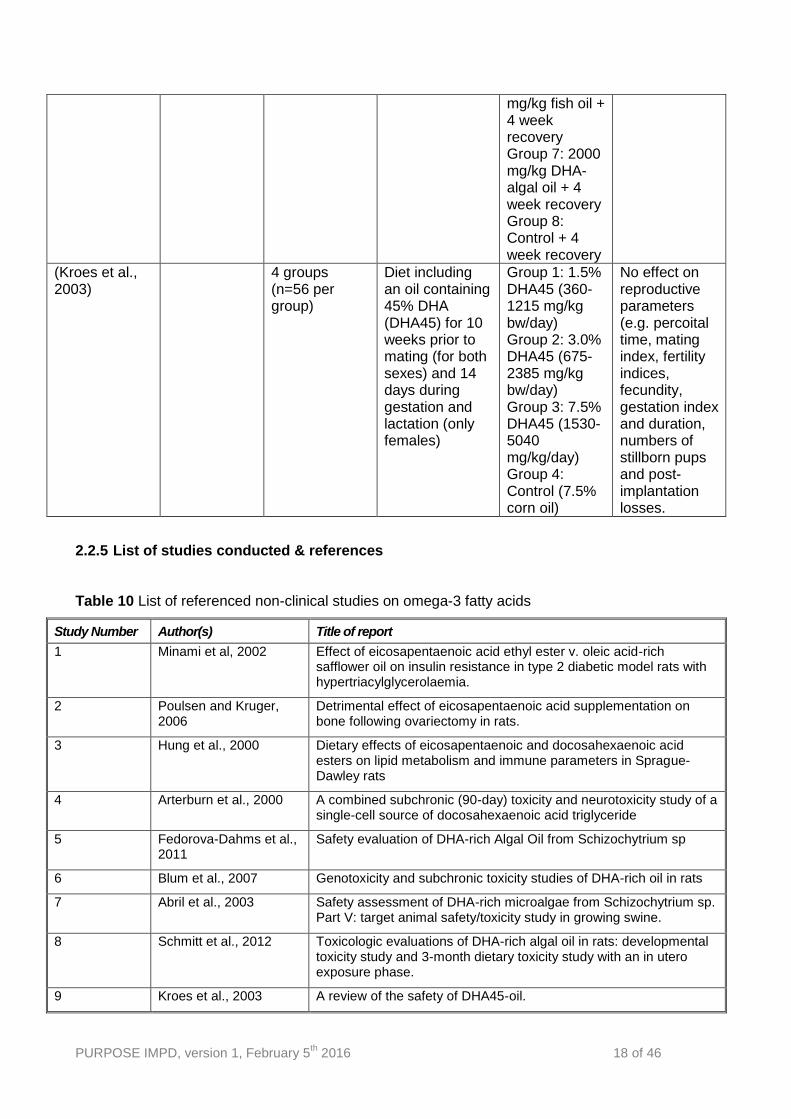
2.2.4 Reproductive and developmental toxicity
Table 9 summarizes available literature on reproductive and developmental toxicity. Overall no
effect on developing animals were observed related to EPA and DHA consumption.
Table 9 Studies examining EPA/DHA reproductive and developmental toxicity
Reference Animals Sample Size Investigational product + duration
Dose Results
(Schmitt et al., 2012)
Sprague-Dawley rats
5 groups (n=60 per group)
DHA rich oil (42% DHA, total omega-3 fatty acid concentration of 44%) or fish oil (DHA 26-27% and EPA content of 6-7%). Treated for 89-91 days in males en 75-77 days in females. Male and female offspring were exposed for 106-107 and 110-111 consecutive days, respectively.
Group 1: Fish oil Group 2: Fish oil Group 3: DHA rich oil Group 4: DHA rich oil Group 5: Control, basal diet
There was an absence of maternal and developmental toxicity. Also postnatal survival and development were not different with the control group. The highest dose, 2000 mg/kg bw/day, was considered the NOAEL.
(Blum et al., 2007)
Sprague-Dawley rats
8 groups (n=10 to 30 per group)
Combination of fish oil (containing 26.7% DHA and 11.4% EPA) and DHA-algal (containing 45% DHA) for 90 days or 90 days + an additional 4-week recovery period (no treatment).
Group 1: 2000 mg/kg fish oil Group 2: 1500 mg/kg fish oil + 500 mg/kg DHA-algal oil Group 3: 1000 mg/kg fish oil + 1000 mg/kg DHA-algal oil Group 4: 2000 mg/kg DHA-algal oil Group 5: Control Group 6: 2000
There were no adverse effects reported related to DHA-containing oil consumption.
PURPOSE IMPD, version 1, February 5th 2016 18 of 46
mg/kg fish oil + 4 week recovery Group 7: 2000 mg/kg DHA-algal oil + 4 week recovery Group 8: Control + 4 week recovery
(Kroes et al., 2003)
4 groups (n=56 per group)
Diet including an oil containing 45% DHA (DHA45) for 10 weeks prior to mating (for both sexes) and 14 days during gestation and lactation (only females)
Group 1: 1.5% DHA45 (360-1215 mg/kg bw/day) Group 2: 3.0% DHA45 (675-2385 mg/kg bw/day) Group 3: 7.5% DHA45 (1530-5040 mg/kg/day) Group 4: Control (7.5% corn oil)
No effect on reproductive parameters (e.g. percoital time, mating index, fertility indices, fecundity, gestation index and duration, numbers of stillborn pups and post-implantation losses.
2.2.5 List of studies conducted & references
Table 10 List of referenced non-clinical studies on omega-3 fatty acids
Study Number Author(s) Title of report
1 Minami et al, 2002 Effect of eicosapentaenoic acid ethyl ester v. oleic acid-rich safflower oil on insulin resistance in type 2 diabetic model rats with hypertriacylglycerolaemia.
2 Poulsen and Kruger, 2006
Detrimental effect of eicosapentaenoic acid supplementation on bone following ovariectomy in rats.
3 Hung et al., 2000 Dietary effects of eicosapentaenoic and docosahexaenoic acid esters on lipid metabolism and immune parameters in Sprague-Dawley rats
4 Arterburn et al., 2000 A combined subchronic (90-day) toxicity and neurotoxicity study of a single-cell source of docosahexaenoic acid triglyceride
5 Fedorova-Dahms et al., 2011
Safety evaluation of DHA-rich Algal Oil from Schizochytrium sp
6 Blum et al., 2007 Genotoxicity and subchronic toxicity studies of DHA-rich oil in rats
7 Abril et al., 2003 Safety assessment of DHA-rich microalgae from Schizochytrium sp. Part V: target animal safety/toxicity study in growing swine.
8 Schmitt et al., 2012 Toxicologic evaluations of DHA-rich algal oil in rats: developmental toxicity study and 3-month dietary toxicity study with an in utero exposure phase.
9 Kroes et al., 2003 A review of the safety of DHA45-oil.
PURPOSE IMPD, version 1, February 5th 2016 19 of 46
2.2.6 References
Abril R., Garrett J., et al. (2003) Safety assessment of DHA-rich microalgae from Schizochytrium sp. Part V: target animal safety/toxicity study in growing swine. Regul Toxicol Pharmacol 37(1), 73-82.
Arterburn L.M., Boswell K.D., et al. (2000) A combined subchronic (90-day) toxicity and neurotoxicity study of a single-cell source of docosahexaenoic acid triglyceride (DHASCO oil). Food Chem Toxicol 38(1), 35-49.
Blum R., Kiy T., et al. (2007) Genotoxicity and subchronic toxicity studies of DHA-rich oil in rats. Regul Toxicol Pharmacol 49(3), 271-284.
Fedorova-Dahms I., Marone P.A., et al. (2011) Safety evaluation of DHA-rich Algal Oil from Schizochytrium sp. Food Chem Toxicol 49(12), 3310-3318.
Hung P., Gu J.Y., et al. (2000) Dietary effects of eicosapentaenoic and docosahexaenoic acid esters on lipid metabolism and immune parameters in Sprague-Dawley rats. Biosci Biotechnol Biochem 64(12), 2588-2593.
Kroes R., Schaefer E.J., et al. (2003) A review of the safety of DHA45-oil. Food Chem Toxicol 41(11), 1433-1446.
Kruger M.C., Coetzer H., et al. (1998) Calcium, gamma-linolenic acid and eicosapentaenoic acid supplementation in senile osteoporosis. Aging (Milano) 10(5), 385-394.
Kuroda Y., Shima N., et al. (2001) Desmutagenic and bio-antimutagenic activity of docosahexaenoic acid and eicosapentaenoic acid in cultured Chinese hamster V79 cells. Mutat Res 497(1-2), 123-130.
Merritt R.J., Auestad N., et al. (2003) Safety evaluation of sources of docosahexaenoic acid and arachidonic acid for use in infant formulas in newborn piglets. Food Chem Toxicol 41(6), 897-904.
Minami A., Ishimura N., et al. (2002) Effect of eicosapentaenoic acid ethyl ester v. oleic acid-rich safflower oil on insulin resistance in type 2 diabetic model rats with hypertriacylglycerolaemia. Br J Nutr 87(2), 157-162.
Poulsen R.C., Kruger M.C. (2006) Detrimental effect of eicosapentaenoic acid supplementation on bone following ovariectomy in rats. Prostaglandins Leukot Essent Fatty Acids 75(6), 419-427.
Schmitt D., Tran N., et al. (2012) Toxicologic evaluations of DHA-rich algal oil in rats: developmental toxicity study and 3-month dietary toxicity study with an in utero exposure phase. Food Chem Toxicol 50(11), 4149-4157.
PURPOSE IMPD, version 1, February 5th 2016 20 of 46
2.3 CLINICAL DATA
2.3.1 Clinical pharmacology
The role of polyunsaturated fatty acids (PUFAs) and their metabolites for the cause and
treatment of psychotic disorders are widely discussed. Controlled studies are usually small and
still seem to yield conflicting results (1,2). The efficacy as an augmenting agent in chronic
schizophrenia seems to be small or not present (3), however epidemiological data, as well as
some recent controlled studies in emerging psychosis point towards possible preventive effects
of PUFAs in early and very early stages of psychotic disorders (4, 5) and some potential
secondary or tertiary beneficial long-term effects in later, more chronic stages, in particular for
metabolic or extra-pyramidal side effects.
The clinical staging model for psychotic and severe mood disorders proposed by Patrick
McGorry (6) reflects that very notion of the differentiation between earlier and milder clinical
phenomena and progressing, more chronic manifestations of an illness. This model, which is
considered for inclusion in the DSM-V (7), suggests three risk stages before onset of full
threshold first episode psychosis. Evolving clinical and neurobiological knowledge on high-risk
stages generally seems to support the clinical staging model. The potential role of PUFAs for
brain maturational processes, the regulation of synaptic plasticity and myelination have not yet
been explored in these early stages of emerging psychotic disorders.
Physiological role of PUFAs
Neuronal membrane bilayers are largely made up of phospholipids and cholesterol.
Phospholipids consist of a glycerol or sphingosine backbone with 3 carbon molecules. A
phosphate molecule and a hydrophilic head group, such as choline, ethanolamine, inositol or
serine are attached to the 3-position. Hydrocarbon tails ranging from 16 to 24 carbon molecules
are attached to the 1- and 2 positions. These hydrocarbon tails are called fatty acids. Fatty acids
can be either saturated or unsaturated if they contain one (monounsaturated) or more
(polyunsaturated) double bonds. Typically, fatty acids attached to the 1-position are saturated
and the ones attached to the 2-position are unsaturated. The number of double bonds, i.e. the
degree of unsaturation influences membrane fluidity.
Polyunsaturated fatty acids (PUFAs) can be classified into omega-3 and omega-6 fatty acids.
The terms omega-3 (n-3) and omega-6 (n-6) specify the location of the first double bond from
the methyl end of the molecule. Mammals have lost the ability to introduce a double bond
beyond carbon 9, thus humans cannot synthesize these fatty acids de novo. Therefore, the
parent molecules of n-3 and n-6 PUFAs, alpha-linolenic acid (ALA, 18:3 n-3) and linoleic acid
PURPOSE IMPD, version 1, February 5th 2016 21 of 46
(LA, 18:2 n-6), are termed essential fatty acids (EFAs); they have to be obtained through dietary
intake and hold important physiological functions. In the liver, EFAs serve as substrates for
further conversion to long-chain PUFAs (LC-PUFAs) with higher number of carbon atoms and
double bonds. The synthesis of LC-PUFAs from the parent substrates ALA and LA is a multi-
stage process involving desaturases and elongases, where n-3 PUFAs and n-6 PUFAs
compete for the same enzymes.
The conversion rates from ALA and LA are limited in humans, wherefore some LC-PUFAs, such
as arachidonic acid (AA, 20:5, n-6) and eicosapentaenoic acid (EPA, 20:5, n-3) need to be
mainly ingested with AA and EPA-rich foods. Dietary sources of ALA are nuts and seeds, such
as walnuts, flaxseed and rapeseed oil; sources of the LC-PUFAs such as EPA and DHA include
fatty fish (e.g. salmon), certain white fish, shellfish and other seafood, as well as some animal
products depending on the animals’ diet (8, 9). In early life, breast milk also constitutes a source
of intake (10). LA and all other n-6 PUFAs are ingested with plant and vegetable seeds and oils,
such as margarines as well as those included in processed foods.
PUFAs and inflammatory mediators
AA and EPA act as precursors for eicosanoids such as prostaglandins (PGs), thromboxane (Tx)
and leukotriens (LTs). Prostaglandins can be synthesized after the release of fatty acids from
membrane phospholipids. Eicosanoids regulate a number of cellular processes.
Phospholipases
Phospholipids are broken down by different types of phospholipases (A1, A2, B, C, D). In the
brain, phospholipases A2 (PLA2) and C play the most important role. PLA2 are key enzymes in
regulating the AA content in the cell membrane, as well as the release and production of
bioactive lipids in general. In short, omega-3 LC-PUFAs are potentially anti-inflammatory agents
and influence the PLA2 catalyzed eicosanoid metabolism.
PUFAs and the brain
AA and DHA are concentrated in the grey matter of the human brain and account for 20% of the
membrane fatty acids. EPA and DHA exert different physiological effects on neuronal cell
membranes. DHA has been shown to alter densities of dopamine, serotonin and muscarinic
receptors, whereas EPA affects the brain through its function as a precursor for eicosanoids.
These PUFAs are particularly important for the specific properties and functions of neuronal
cells since their availability determines the phospholipid structure and structure in turn impacts
function. Other processes regulated by PUFAs (11) include brain development (12), synaptic
PURPOSE IMPD, version 1, February 5th 2016 22 of 46
functioning (13), regulation of corticotrophin-releasing hormone (14), prevention of neuronal
apoptosis (15, 16), neurite growth (17), gene expression (18), as well as neuronal migration,
pruning and synaptic plasticity (13). The balance of specific type of PUFAs also affects
inflammatory processes: EPA as well as ALA supplementation (19) has been shown to reduce
the production of pro-inflammatory cytokines (20, 21).
Direct effects of omega-3 fatty acids on the brain can be measured in vivo with magnetic
resonance imaging (MRI) by measuring brain water proton transverse relaxation times (T2),
which is an index of the water in neuronal tissues. Reduced neuronal health is thought to be
associated with T2 increases (22). Indeed, preclinical findings on neuroprotective properties of
EFAs are supported by studies in patients with bipolar disorders (23) and first episode
psychosis (FEP) using T2 relaxation time (22).
Fish intake, cognition and early brain development
Regarding the importance of PUFAs for brain development, maternal fish and seafood
consumption of less than 340g per week during pregnancy has been reported to increase the
risk for a low IQ and deficient neurodevelopmental outcomes in childhood (24). Some (25, 26)
but not all (27-29) studies have yielded findings of protective effects of EFAs in pregnancy and
breastfeeding against schizophrenia and related disorders. Some of the negative findings were
population-based studies, whereas the positive ones rather investigated high-risk populations
with family histories of schizophrenia, very premature birth, birth complications, viral infections
or extreme malnutrition. Possibly, the protective role of EFAs in breastmilk might be relevant
only for risk populations.
2.3.2 Clinical pharmacokinetics
In vivo comparison of three dosages (3 g, 6 g, 12 g) of two different fish oil preparations in terms
of plasma concentrations of their major active components eicosapentaenoic acid (EPA) and
docosahexaenoic acid (DHA) has been quoted most often when describing the
pharmacokinetics of omega-3 fatty acids. The plasma accumulation was measured during 28
days of ingestion and an equally long wash out period. Data were scrutinized for bioavailability
in order to distinguish between the efficiency of the two preparations. Rapid increases in EPA
and DHA plasma concentrations can be demonstrated at all dosages during a 28-day ingestion
period. EPA accumulated more during ingestion of high than of low dosages of fish oil. DHA
revealed almost identical increases and peak values in plasma concentrations in all subgroups.
The present data demonstrate dose dependent increases of EPA concentrations whereas DHA
plasma concentrations are comparable in all dosages investigated. Measurable EPA and DHA
plasma concentration levels are inappropriate means to explain clinical effectiveness. These
PURPOSE IMPD, version 1, February 5th 2016 23 of 46
results were found in both commercially available fish oil preparations. Direct comparison of
both preparations revealed no differences in bioavailability (30). EPA and DHA are absorbed
largely via the lymph. It is apparent that EPA and DHA ethyl esters are hydrolyzed during
absorption from the small intestine (31) and re-esterified mainly into triglycerides for transport in
the chylomicrons in lymph (31, 32). Elaborate evidence for high oral bioavailability is available,
for instance, from an excretion study in which less than 10% of the dose of radioactive carbon
(14C)-labelled EPA ethyl ester or DHA ethyl ester was excreted in faeces over 7 days.
2.3.3 Human exposure
Polyunsatured omega-3 fatty acids (PUFA) are essential for normal brain development. Cell
biological and molecular studies suggest that omega-3 fatty acids modulate membrane fluidity
(33), dopaminergic (34), glutamatergic (35) and serotonergic (36) neurotransmission. PUFA can
also regulate gene expression (37), influencing synaptic plasticity and function (38). Preclinical
studies suggest that omega-3 fatty acids have neuroprotective properties (39, 40). Animal and
human studies show that omega-3 PUFA are crucial during the embryonic stage, early postnatal
life and childhood (41). PUFA are thus relevant to neurodevelopment, neurodegeneration and
behavioural neurobiology, all factors proposed as playing a pivotal role in the genesis of
schizophrenia (42).
The precursors of omega-3 fatty acids (alpha-Linolenic acid ALA) and omega-6 fatty acids
(Linoleic acid LA) are essential fatty acids (EFAs) meaning that humans cannot synthesize them
de novo. Humans have to supply EFAs through diet similar to vitamins. The source of the
omega-3 LC-PUFAs is mainly oily fish, e.g. salmon or sardines, whereas the precursor ALA is
also present in plant oils, such as canola oil, nut oils, or algae oils. A range of epidemiological
and experimental studies provide some evidence for a link between cardiovascular disorders,
metabolic syndrome or depressive disorders that are all proposed to be associated with an
increase in proinflammatory cytokines and a deficiency in omega-3 fatty acids. The latter may
have direct implications for prevention and treatment (43, 44).
Omega-3 fatty acids and psychotic disorders
The “membrane hypothesis “ of schizophrenia (45, 46) was originally based on early findings of
lipid alterations in the cerebrospinal fluid or peripheral cell membranes of patients with
schizophrenia (42) and of a prostaglandin–deficit syndrome (mainly metabolites of arachidonic
acid or eicosapentaenoic acid) (47). There is also evidence suggesting decreased omega-3
fatty acid levels during the early phases of schizophrenia, in blood cell membranes of
antipsychotic-naïve first episode patients (48). Imaging methods such as magnetic resonance
spectroscopy have allowed researchers to investigate membrane turnover in the living human
PURPOSE IMPD, version 1, February 5th 2016 24 of 46
brain, confirming significant membrane abnormalities in schizophrenia (49, 50), independent of
treatment (51, 52).
Although there is only limited evidence supporting that EPA augmentation of antipsychotic
medication in established psychosis improves symptomatic outcome (53), they may exert
positive effects as a preventive agents, in particular during the pre-psychotic phases. A recent
study has confirmed a mixture of EPA and DHA significantly reduces transition rates in subjects
at ultra-high risk for psychosis (54) pointing to a potential neuroprotective effect of omega-3 fatty
acids supplementation in at risk mental states. There is growing evidence suggesting that the
emergence of psychosis is associated with subtle structural (for a review see (55)), functional
(for reviews see (56, 57)) and neurochemical (mostly involving dopamine and glutamate, for
reviews see (58, 59)) alterations which may ultimately lead to the onset of frank psychosis. The
potential underlying mechanism of the therapeutic action of omega-3 fatty acids during the pre-
psychotic phases may be neuroprotective, e.g. via modulation of the antioxidative intracellular
defense (35), antiapoptotic actions (60) or be the result of a direct interaction between EPA and
glutamatergic neurotransmission (for a review on omega-3 fatty acid interventions in early
psychosis see (42)).
Published omega-3 fatty acids RCTs in minors with psychiatric conditions
The available scientific literature concerning effects of omega-3 fatty acids in children with
psychiatric conditions is limited to childhood-onset depression and attention deficit and
hyperactivity disorders (ADHD). Studies in adolescents include an RCT first-episode psychosis
(5), as well as an RCT in adolescents at ultra-high risk for psychosis (4). The latter concerned
an RCT in 81 adolescents at ultra-high risk (UHR) for developing a psychotic disorder (mean
age 16.4) that used 1.2g of an EPA-enriched omega-3 fatty acids oil as a sole agent (4). 27.5%
in the placebo group progressed towards a first psychotic episode compared to only 4.9% in the
omega-3 fatty acids group. This pilot study has recently been replicated but study results are not
available yet (the NEURAPRO study (61)). The use of omega-3 fatty acids in prevention of
mental disorders is promising, yet an avenue to be further explored.
PURPOSE IMPD, version 1, February 5th 2016 25 of 46
2.4 OVERALL RISK AND BENEFIT ASSESSMENT
2.4.1 PUFAs and potential adverse effects in UHR
Only one study has investigated the effects of supplementation with omega-3 PUFAs as
treatment in UHR individuals (4). Thus, the only data regarding the safety of omega 3 PUFAs
are derived from this trial. Applying the Udvalg for Kliniske Undersogelser scale (UKU) to detect
adverse effects, frequency and intensity of possible side effects in the omega-3 FA condition
were not different from placebo. Although not statistically different from the placebo group, the
following adverse effects were reported in the omega-3 group: diarrhoea, nausea/vomiting,
tension/inner unrest, depression, concentration difficulties, emotional indifference, tension
headache, reduced duration of sleep, increased fatigability. All but “increased fatigability”
occurred – nonsignificantly - less frequently in the omega-3 group Not listed are side effects
that occurred with a prevalence of less than 5% in the omega-3 or in the placebo group.
2.4.2 PUFAs and potential adverse effects in schizophrenia
Additional data regarding adverse effects of omega-3 PUFAs supplementation are available
from add-on treatment trials in patients suffering a first episode of psychosis or in chronic
schizophrenia patients. Generally, the assessments of adverse effects in these trials varied
between structured assessments (e.g. UKU) and spontaneous patient reports. In Fenton and
colleagues’ omega-3 PUFA supplementation RCT patients with schizophrenia/schizoaffective
disorder of the verum condition showed upper respiratory infection (8/43 patients, 19%) and
diarrhoea (8/43 patients 19 %) (62). A lower dose of omega-3 PUFAs (600mg EPA/DHA) in
Arvindakshan and colleagues’ open-label study was not associated with any gastrointestinal
problems, but 5 of 33 patients did drop out due to the fishy odour of the capsules (63). Taken
together, the following common but clinically rarely significant side effects were reported here:
mild nausea or diarrhoea, fishy eructation and loose stool (53, 64, 65).
2.4.3 Specific adverse effects of PUFAs
Further data regarding safety issues are available from trials performed in patients with
schizophrenia, other psychiatric and somatic illnesses and the general population.
PUFAs and bleeding time
There is evidence that the intake of omega-3 PUFAs is associated with a prolonged bleeding
time in healthy men (66) and in both healthy men and women (66-68). A literature review by
Knapp suggested that the prolongation of bleeding time is usually modest and there have been
no reports of clinically significant bleeding (69). A statement by the FDA (70) confirmed that fish
oils can significantly prolong bleeding time but a dose of up to 3g/d EPA/DHA is considered as
PURPOSE IMPD, version 1, February 5th 2016 26 of 46
safe (71). According to a study by Emsley and colleagues (72) in chronic schizophrenia patients
a dose of 2g/day EPA caused a significant increase in bleeding time, but remained in the high
end of the normal range and was not associated with clinically relevant bleeding complications.
Since patients with schizophrenia and other psychoses have been shown to be at increased risk
for cardiovascular conditions and mortality (73), a slightly prolonged bleeding time within normal
range as well as other metabolic effects of PUFAs (outlined below) are discussed as being even
beneficial.
PUFAs and metabolic parameters
There is sound evidence from studies in healthy populations and in individuals with lipid
metabolism disorders that omega-3 LC-PUFAs are effective in lowering triglycerides (TG) levels
(74-76). Only one trial explicitly investigated metabolic effects of EPA in patients with chronic
schizophrenia (72). This study evaluated the effects of 2g/day EPA vs. placebo on weight gain,
total cholesterol, HDL, LDL and TG levels, on fasting blood glucose and additionally on tardive
dyskinesia (TD) over a period of 12 weeks with a 40-week open extension phase. The results
point to a significant, but clinically probably only slightly relevant increase in Body Mass Index
(BMI) in the EPA group (baseline 24.5 to end of treatment 25.2 kg/m2; p = 0.0001). With respect
to total cholesterol, HDL, LDL and TG levels, the findings depict a significant decrease in total
cholesterol levels as well as in HDL levels, but there were changes in neither LDL nor in TG
plasma levels (77). Fasting blood glucose increased at trend level. Meta-analytical data of
studies in individuals who were either healthy, had diabetes, hypertension or dyslipidemia, or
cardiovascular disease, show that omega-3 LC-PUFAs do not seem to have relevant effects on
blood glucose (78, 79). At the moment, no published data regarding PUFAs and metabolic
parameters are available in patients with UHR for psychosis.
PUFAs and cardiovascular factors
Epidemiological studies suggest benefits of omega-3 PUFAs on cardiovascular health (80, 81).
Indeed, the American Heart Association recommends 1g/d of EPA/DHA for secondary
cardiovascular disease prevention (76, 82). No valid data are yet available in patients with
schizophrenia. However, it is well known that patients with schizophrenia and other psychiatric
disorders are at increased risk for cardiovascular disease as a consequence of a higher
prevalence of the metabolic syndrome (83). Therefore, positive omega-3 PUFA
supplementation effects in patients with emerging psychosis might not only arise from protection
against transition to acute psychosis, but there may also be a gain from the potential to prevent
metabolic and cardiovascular detriments (84).

PURPOSE IMPD, version 1, February 5th 2016 27 of 46
Other common but clinically rarely relevant side effects of n-3 fatty acid supplementation include
mild nausea, mild diarrhoea, fishy eructation and exacerbation of asthma in aspirin-sensitive
patients (85). Only two of available treatment trials in patients at UHR, with a FEP or chronic
schizophrenia report differences in adverse effects with n-3 LC-PUFAs supplementation (62,
64): they report gastrointestinal symptoms and upper respiratory infections.
2.4.3 Risks versus benefits of PUFAs in emerging psychosis
Taken together, one promising aspect of omega-3 PUFAs is that there seem to be no reports of
relevant deleterious side effects in humans, even at high doses. However, the differential effects
on lipid parameters described above are noteworthy and need further clarification. As
mentioned, the slight risk of prolonged bleeding time is outweighed by the benefits. Aside from
the benefit that treatment with omega-3 PUFAs may prevent or at least delay the onset of
psychotic disorders in UHR groups, a notable benefit is that treatment with omega-3 PUFAs
also significantly reduced positive, negative, and general symptoms on the positive and
negative syndrome scale (PANSS) and improved functioning (4) .
2.5 CONCLUSION
The current stage of knowledge based on the most recent trial of indicated prevention in UHR
groups holds promise that treatment with omega-3 PUFAs may prevent or at least delay the
onset of psychotic disorder. As replication studies are still underway, conclusions in terms of
clinical effectiveness are still preliminary. In contrast, in terms of safety issues evidence from the
RCT in UHR individuals and a variety of studies in schizophrenia patients, strongly suggests
PUFAs are safe and well-tolerated by young people at ultra-high risk of psychosis. Omega-3
PUFAs have been shown to be safe even when used in relatively high doses, and except for
mild gastrointestinal symptoms they are presumed to be free of clinically relevant adverse
events (86). Nevertheless, clinicians should be aware of possible increases in bleeding time.
Although a statement by the FDA (70) reported that fish oils can significantly prolong bleeding
time and a dose of up to EPA/DHA of 3g/d was considered as safe, clinical trial evidence does
not support relevant increases in bleeding time, not even in patients treated with anti-platelet or
antithrombotic agents (71). Generally, tolerability of n-3 LC-PUFAs can be assumed as being
very good. When balancing risks and benefits of omega-3 PUFA supplementation, it is
important to note that additionally to the common positive effects on the cardiovascular and
other systems omega-3 PUFAs might also unfold neuroprotective properties (87) which are of
particular interest in the field of indicated prevention and psychosis research.
PURPOSE IMPD, version 1, February 5th 2016 28 of 46
References 1. Schachter HM, Kourad K, Merali Z, Lumb A, Tran K, Miguelez M. Effects of omega-3 fatty acids on
mental health. Evid Rep Technol Assess (Summ). 2005(116):1-11. 2. Irving CB, Mumby-Croft R, Joy LA. Polyunsaturated fatty acid supplementation for schizophrenia.
Cochrane Database Syst Rev. 2006;3:CD001257. 3. Fusar-Poli P, Crossley N, Woolley J, Carletti F, Perez-Iglesias R, Broome M, et al. White matter
alterations related to P300 abnormalities in individuals at high risk for psychosis: an MRI-EEG study. J Psychiatry Neurosci. 2011;36(1):100083.
4. Amminger GP, Schafer MR, Papageorgiou K, Klier CM, Cotton SM, Harrigan SM, et al. Long-chain omega-3 fatty acids for indicated prevention of psychotic disorders: a randomized, placebo-controlled trial. Arch Gen Psychiatry. 2010;67(2):146-54.
5. Berger GE, Proffitt TM, McConchie M, Yuen H, Wood SJ, Amminger GP, et al. Ethyl-eicosapentaenoic acid in first-episode psychosis: a randomized, placebo-controlled trial. J Clin Psychiatry. 2007;68(12):1867-75.
6. McGorry PD, Nelson B, Goldstone S, Yung AR. Clinical staging: a heuristic and practical strategy for new research and better health and social outcomes for psychotic and related mood disorders. Can J Psychiatry. 2010;55(8):486-97.
7. Woods SW, Walsh BC, Saksa JR, McGlashan TH. The case for including Attenuated Psychotic Symptoms Syndrome in DSM-5 as a psychosis risk syndrome. Schizophr Res. 2010;123(2-3):199-207.
8. Sinclair AJ, Murphy KJ, Li D. Marine lipids: overview "news insights and lipid composition of Lyprinol". Allerg Immunol (Paris). 2000;32(7):261-71.
9. Torres IC, Mira L, Ornelas CP, Melim A. Study of the effects of dietary fish intake on serum lipids and lipoproteins in two populations with different dietary habits. Br J Nutr. 2000;83(4):371-9.
10. Cunnane SC, Francescutti V, Brenna JT, Crawford MA. Breast-fed infants achieve a higher rate of brain and whole body docosahexaenoate accumulation than formula-fed infants not consuming dietary docosahexaenoate. Lipids. 2000;35(1):105-11.
11. Freeman MP, Hibbeln JR, Wisner KL, Davis JM, Mischoulon D, Peet M, et al. Omega-3 fatty acids: evidence basis for treatment and future research in psychiatry. J Clin Psychiatry. 2006;67(12):1954-67.
12. Uauy R, Dangour AD. Nutrition in brain development and aging: role of essential fatty acids. Nutr Rev. 2006;64(5 Pt 2):S24-33; discussion S72-91.
13. Bazan NG. Lipid signaling in neural plasticity, brain repair, and neuroprotection. Molecular neurobiology. 2005;32(1):89-103.
14. Hibbeln JR, Bissette G, Umhau JC, George DT. Omega-3 status and cerebrospinal fluid corticotrophin releasing hormone in perpetrators of domestic violence. Biol Psychiatry. 2004;56(11):895-7.
15. Kim HY, Akbar M, Kim KY. Inhibition of neuronal apoptosis by polyunsaturated fatty acids. J Mol Neurosci. 2001;16(2-3):223-7; discussion 79-84.
16. Kim HY, Akbar M, Lau A. Effects of docosapentaenoic acid on neuronal apoptosis. Lipids. 2003;38(4):453-7.
17. Calderon F, Kim HY. Docosahexaenoic acid promotes neurite growth in hippocampal neurons. J Neurochem. 2004;90(4):979-88.
18. Jump DB. Dietary polyunsaturated fatty acids and regulation of gene transcription. Curr Opin Lipidol. 2002;13(2):155-64.
19. Caughey GE, Mantzioris E, Gibson RA, Cleland LG, James MJ. The effect on human tumor necrosis factor alpha and interleukin 1 beta production of diets enriched in n-3 fatty acids from vegetable oil or fish oil. Am J Clin Nutr. 1996;63(1):116-22.
20. Calder PC. N-3 polyunsaturated fatty acids and inflammation: from molecular biology to the clinic. Lipids. 2003;38(4):343-52.
21. James MJ, Gibson RA, Cleland LG. Dietary polyunsaturated fatty acids and inflammatory mediator production. Am J Clin Nutr. 2000;71(1 Suppl):343S-8S.
22. Wood SJ, Cocchi L, Proffitt TM, McConchie M, Jackson GD, Takahashi T, et al. Neuroprotective effects of ethyl-eicosapentaenoic acid in first episode psychosis: a longitudinal T2 relaxometry pilot study. Psychiatry research. 2010;182(2):180-2.
23. Hirashima F, Parow AM, Stoll AL, Demopulos CM, Damico KE, Rohan ML, et al. Omega-3 fatty acid treatment and T(2) whole brain relaxation times in bipolar disorder. The American journal of psychiatry. 2004;161(10):1922-4.
PURPOSE IMPD, version 1, February 5th 2016 29 of 46
24. Hibbeln JR, Davis JM, Steer C, Emmett P, Rogers I, Williams C, Golding J. Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet. 2007;369(9561):578-85.
25. McCreadie RG. The Nithsdale Schizophrenia Surveys 16: Breastfeeding and schizophrenia, preliminary results and hypotheses. Br J Psychiatry. 1997;170:334-7.
26. Peet M, Poole J, Laugharne J. Infant feeding and the development of schizophrenia. Schizophr Res. 1997;24:255-6.
27. Makrides M, Gibson RA, McPhee AJ, Yelland L, Quinlivan J, Ryan P. Effect of DHA supplementation during pregnancy on maternal depression and neurodevelopment of young children: a randomized controlled trial. JAMA. 2010;304(15):1675-83.
28. Leask SJ, Done DJ, Crow TJ, Richards M, Jones PB. No association between breast-feeding and adult psychosis in two national birth cohorts. Br J Psychiatry. 2000;177:218-21.
29. Sasaki T, Okazaki Y, Akaho R, Masui K, Harada S, Lee I, et al. Type of feeding during infancy and later development of schizophrenia. Schizophrenia research. 2000;42(1):79-82.
30. Marsen TA, Pollok M, Oette K, Baldamus CA. Pharmacokinetics of omega-3-fatty acids during ingestion of fish oil preparations. Prostaglandins Leukot Essent Fatty Acids. 1992;46(3):191-6.
31. Ishiguro J, Tada T, Ogihara T, Ohzawa N, Murakami K, Kosuzume H. Metabolic disposition of ethyl eicosapentaenoate and its metabolites in rats and dogs. J Pharmacobiodyn. 1988;11(4):251-61.
32. Chen IS, Subramaniam S, Cassidy MM, Sheppard AJ, Vahouny GV. Intestinal absorption and lipoprotein transport of (omega-3) eicosapentaenoic acid. J Nutr. 1985 115(2):219-25.
33. Valentine RC, Valentine DL. Omega-3 fatty acids in cellular membranes: a unified concept. Prog Lipid Res. 2004;43(5):383-402.
34. Ohara K. The n-3 polyunsaturated fatty acid/dopamine hypothesis of schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(2):469-74.
35. Berger GE, Wood SJ, Wellard RM, Proffitt TM, McConchie M, Amminger GP, et al. Ethyl-eicosapentaenoic acid in first-episode psychosis. A 1H-MRS study. Neuropsychopharmacology. 2008;33(10):2467-73.
36. Yao JK, Magan S, Sonel AF, Gurklis JA, Sanders R, Reddy RD. Effects of omega-3 fatty acid on platelet serotonin responsivity in patients with schizophrenia. Prostaglandins Leukot Essent Fatty Acids. 2004;71(3):171-6.
37. Deckelbaum RJ, Worgall TS, Seo T. n-3 fatty acids and gene expression. Am J Clin Nutr. 2006;83(6 Suppl):1520S-5S.
38. Heinrichs SC. Dietary omega-3 fatty acid supplementation for optimizing neuronal structure and function. Mol Nutr Food Res. 2010;54(4):447-56.
39. Zhang W, Hu X, Yang W, Gao Y, Chen J. Omega-3 polyunsaturated fatty acid supplementation confers long-term neuroprotection against neonatal hypoxic-ischemic brain injury through anti-inflammatory actions. Stroke. 2010;41(10):2341-7.
40. Palacios-Pelaez R, Lukiw WJ, Bazan NG. Omega-3 essential fatty acids modulate initiation and progression of neurodegenerative disease. Mol Neurobiol. 2010;41(2-3):367-74.
41. Ryan AS, Astwood JD, Gautier S, Kuratko CN, Nelson EB, Salem N, Jr. Effects of long-chain polyunsaturated fatty acid supplementation on neurodevelopment in childhood: a review of human studies. Prostaglandins Leukot Essent Fatty Acids. 2010;82(4-6):305-14.
42. Berger GE, Wood SJ, Pantelis C, Velakoulis D, Wellard RM, McGorry PD. Implications of lipid biology for the pathogenesis of schizophrenia. The Australian and New Zealand journal of psychiatry. 2002;36(3):355-66.
43. Simopoulos AP. Omega-3 fatty acids in inflammation and autoimmune diseases. J Am Coll Nutr. 2002;21(6):495-505.
44. Simopoulos AP. Omega-3 fatty acids in health and disease and in growth and development. Am J Clin Nutr. 1991;54(3):438-63.
45. Horrobin DF, Glen AI, Vaddadi KS. The membrane hypothesis of schizophrenia. Schizophrenia research. 1994;13(3):195-207.
46. Horrobin DF. The membrane phospholipid hypothesis as a biochemical basis for the neurodevelopmental concept of schizophrenia. Schizophrenia research. 1998;30(3):193-208.
47. Smesny S. Prostaglandin-mediated signaling in schizophrenia. Int Rev Neurobiol. 2004;59:255-71. 48. Reddy RD, Keshavan MS, Yao JK. Reduced red blood cell membrane essential polyunsaturated
fatty acids in first episode schizophrenia at neuroleptic-naive baseline. Schizophrenia bulletin. 2004;30(4):901-11.
49. Reddy R, Keshavan MS. Phosphorus magnetic resonance spectroscopy: its utility in examining the membrane hypothesis of schizophrenia. Prostaglandins Leukot Essent Fatty Acids. 2003;69(6):401-5.
PURPOSE IMPD, version 1, February 5th 2016 30 of 46
50. Stone JM. Imaging the glutamate system in humans: relevance to drug discovery for schizophrenia. Curr Pharm Des. 2009;15(22):2594-602.
51. Pettegrew JW, Keshavan MS, Panchalingam K, Strychor S, Kaplan DB, Tretta MG, Allen M. Alterations in brain high-energy phosphate and membrane phospholipid metabolism in first-episode, drug-naive schizophrenics. A pilot study of the dorsal prefrontal cortex by in vivo phosphorus 31 nuclear magnetic resonance spectroscopy. Arch Gen Psychiatry. 1991;48(6):563-8.
52. Fukuzako H, Fukuzako T, Hashiguchi T, Kodama S, Takigawa M, Fujimoto T. Changes in levels of phosphorus metabolites in temporal lobes of drug-naive schizophrenic patients. The American journal of psychiatry. 1999;156(8):1205-8.
53. Fusar-Poli P, Berger G. Eicosapentaenoic acid interventions in schizophrenia: meta-analysis of randomized, placebo-controlled studies. J Clin Psychopharmacol. 2012;32(2):179-85.
54. Amminger GP, Schafer MR, Papageorgiou K, Klier CM, Cotton SM, Harrigan SM, et al. Long-chain omega-3 fatty acids for indicated prevention of psychotic disorders: a randomized, placebo-controlled trial. Archives of General Psychiatry. 2010;67(2):146-54.
55. Fusar-Poli P, Borgwardt S, Crescini A, D'Este G, Kempton M, Lawrie S, et al. Neuroanatomy of Vulnerability to Psychosis: A Voxel-Based Meta-Analysis. Neurosci Biobehav Rev. 2010.
56. Smieskova R, Fusar-Poli P, Allen P, Bendfeldt K, Stieglitz R, Drewe J, et al. Neuroimaging predictors of transition to psychosis – A systematic review and meta-analysis. Neuroscience and Biobehavioural Reviews. 2010:Feb 6 Epub.
57. Fusar-Poli P, Perez J, Broome M, Borgwardt S, Placentino A, Caverzasi E, et al. Neurofunctional correlates of vulnerability to psychosis: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2007;31(4):465-84.
58. Howes OD, Montgomery AJ, Asselin M, Murray R, Grasby P, McGuire P. Molecular imaging studies of the striatal dopaminergic system in psychosis and predictions for the prodromal phase of psychosis. Br J Psychiatry. 2007;s51:s13-s8.
59. Brugger S, Davis JM, Leucht S, Stone JM. Proton magnetic resonance spectroscopy and illness stage in schizophrenia--a systematic review and meta-analysis. Biol Psychiatry. 2011;69(5):495-503.
60. Sinha RA, Khare P, Rai A, Maurya SK, Pathak A, Mohan V, et al. Anti-apoptotic role of omega-3-fatty acids in developing brain: perinatal hypothyroid rat cerebellum as apoptotic model. Int J Dev Neurosci. 2009;27(4):377-83.
61. Markulev C, McGorry PD, Nelson B, Yuen HP, Schaefer M, Yung AR, et al. NEURAPRO-E study protocol: a multicentre randomized controlled trial of omega-3 fatty acids and cognitive-behavioural case management for patients at ultra high risk of schizophrenia and other psychotic disorders. Early Interv Psychiatry. 2015.
62. Fenton WS, Dickerson F, Boronow J, Hibbeln JR, Knable M. A placebo-controlled trial of omega-3 fatty acid (ethyl eicosapentaenoic acid) supplementation for residual symptoms and cognitive impairment in schizophrenia. The American journal of psychiatry. 2001;158(12):2071-4.
63. Arvindakshan M, Ghate M, Ranjekar PK, Evans DR, Mahadik SP. Supplementation with a combination of omega-3 fatty acids and antioxidants (vitamins E and C) improves the outcome of schizophrenia. Schizophrenia research. 2003;62(3):195-204.
64. Peet M, Horrobin DF. A dose-ranging exploratory study of the effects of ethyl-eicosapentaenoate in patients with persistent schizophrenic symptoms. Journal of psychiatric research. 2002;36(1):7-18.
65. Peet M, Brind J, Ramchand CN, Shah S, Vankar GK. Two double-blind placebo-controlled pilot studies of eicosapentaenoic acid in the treatment of schizophrenia. Schizophr Res. 2001;49(3):243-51.
66. Thorngren M, Gustafson A. Effects of 11-week increases in dietary eicosapentaenoic acid on bleeding time, lipids, and platelet aggregation. Lancet. 1981;2(8257):1190-3.
67. Ahmed AA, Holub BJ. Alteration and recovery of bleeding times, platelet aggregation and fatty acid composition of individual phospholipids in platelets of human subjects receiving a supplement of cod-liver oil. Lipids. 1984;19(8):617-24.
68. Wojenski CM, Silver MJ, Walker J. Eicosapentaenoic acid ethyl ester as an antithrombotic agent: comparison to an extract of fish oil. Biochim Biophys Acta. 1991;1081(1):33-8.
69. Knapp HR. Dietary fatty acids in human thrombosis and hemostasis. Am J Clin Nutr. 1997;65(5 Suppl):1687S-98S.
70. Department of Health and Human Services USoAFaDA. 1997 Contract No.: 21 CFR Part 184 (Docket No. 86G-0289).
71. Harris WS. Expert opinion: omega-3 fatty acids and bleeding-cause for concern? Am J Cardiol. 2007;99(6A):44C-6C.
PURPOSE IMPD, version 1, February 5th 2016 31 of 46
72. Emsley R, Niehaus DJ, Oosthuizen PP, Koen L, Ascott-Evans B, Chiliza B, et al. Safety of the omega-3 fatty acid, eicosapentaenoic acid (EPA) in psychiatric patients: results from a randomized, placebo-controlled trial. Psychiatry Res. 2008;161(3):284-91.
73. Scorza FA, Cysneiros RM, Terra VC, Scorza CA, Cavalheiro EA, Ribeiro MO, Gattaz WF. Omega-3 consumption and sudden cardiac death in schizophrenia. Prostaglandins Leukot Essent Fatty Acids. 2009;81(4):241-5.
74. Jacobson TA, Glickstein SB, Rowe JD, Soni PN. Effects of eicosapentaenoic acid and docosahexaenoic acid on low-density lipoprotein cholesterol and other lipids: a review. J Clin Lipidol. 2012;6(1):5-18.
75. Harris WS, Miller M, Tighe AP, Davidson MH, Schaefer EJ. Omega-3 fatty acids and coronary heart disease risk: clinical and mechanistic perspectives. Atherosclerosis. 2008;197(1):12-24.
76. Kris-Etherton PM, Harris WS, Appel LJ. Fish consumption, fish oil, omega-3 fatty acids, and cardiovascular disease. Circulation. 2002;106(21):2747-57.
77. Wei MY, Jacobson TA. Effects of eicosapentaenoic acid versus docosahexaenoic acid on serum lipids: a systematic review and meta-analysis. Curr Atheroscler Rep. 2011;13(6):474-83.
78. Balk EM, Lichtenstein AH, Chung M, Kupelnick B, Chew P, Lau J. Effects of omega-3 fatty acids on serum markers of cardiovascular disease risk: a systematic review. Atherosclerosis. 2006;189(1):19-30.
79. Hartweg J, Perera R, Montori V, Dinneen S, Neil HA, Farmer A. Omega-3 polyunsaturated fatty acids (PUFA) for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2008(1):CD003205.
80. Massaro M, Scoditti E, Carluccio MA, Campana MC, De Caterina R. Omega-3 fatty acids, inflammation and angiogenesis: basic mechanisms behind the cardioprotective effects of fish and fish oils. Cell Mol Biol (Noisy-le-grand).56(1):59-82.
81. Massaro M, Scoditti E, Carluccio MA, Campana MC, De Caterina R. Omega-3 fatty acids, inflammation and angiogenesis: basic mechanisms behind the cardioprotective effects of fish and fish oils. Cell Mol Biol (Noisy-le-grand). 2010;56(1):59-82.
82. Breslow JL. n-3 fatty acids and cardiovascular disease. Am J Clin Nutr. 2006;83(6 Suppl):1477S-82S.
83. Brown S, Birtwistle J, Roe L, Thompson C. The unhealthy lifestyle of people with schizophrenia. Psychol Med. 1999;29(3):697-701.
84. Scorza FA, Cysneiros RM, Cavalheiro EA, Arida RM, de Albuquerque M. Omega-3 fatty acids and sudden cardiac death in schizophrenia: if not a friend, at least a great colleague. Schizophr Res. 2007;94(1-3):375-6.
85. Fenton WS, Hibbeln J, Knable M. Essential fatty acids, lipid membrane abnormalities, and the diagnosis and treatment of schizophrenia. Biol Psychiatry. 2000;47(1):8-21.
86. Freeman MP, Hibbeln JR, Wisner KL, Brumbach BH, Watchman M, Gelenberg AJ. Randomized dose-ranging pilot trial of omega-3 fatty acids for postpartum depression. Acta Psychiatr Scand. 2006;113(1):31-5.
87. Berger GE, Dell`Olio M, Amminger GP. Neuroprotection in emerging psychotic disorder. Early Interv Psychiatry. 2007;1(1):114-27.
PURPOSE IMPD, version 1, February 5th 2016 32 of 46
APPENDIX 1
PURPOSE IMPD, version 1, February 5th 2016 33 of 46
APPENDIX 2
PURPOSE IMPD, version 1, February 5th 2016 34 of 46
APPENDIX 3
PURPOSE IMPD, version 1, February 5th 2016 35 of 46
APPENDIX 4
PURPOSE IMPD, version 1, February 5th 2016 36 of 46
APPENDIX 5
PURPOSE IMPD, version 1, February 5th 2016 37 of 46

PURPOSE IMPD, version 1, February 5th 2016 38 of 46
PURPOSE IMPD, version 1, February 5th 2016 39 of 46
APPENDIX 6
PURPOSE IMPD, version 1, February 5th 2016 40 of 46
PURPOSE IMPD, version 1, February 5th 2016 41 of 46
PURPOSE IMPD, version 1, February 5th 2016 42 of 46
APPENDIX 7
PURPOSE IMPD, version 1, February 5th 2016 43 of 46
PURPOSE IMPD, version 1, February 5th 2016 44 of 46
PURPOSE IMPD, version 1, February 5th 2016 45 of 46
APPENDIX 8

PURPOSE IMPD, version 1, February 5th 2016 46 of 46