introducing and sustaining eenc in hospitals: routine...
TRANSCRIPT

E A R L Y E S S E N T I A L N E W B O R N C A R E ( E E N C ) m O d u l E 3
Introducing and sustaining EENC in hospitals: routine childbirth and newborn care


E A R L Y E S S E N T I A L N E W B O R N C A R E ( E E N C ) M O D U L E 3
Introducing and sustaining EENC in hospitals: routine childbirth
and newborn care

WHO Library Cataloguing-in-Publication Data
Introducing and sustaining EENC in hospitals: routine childbirth and newborn care (Early Essential Newborn Care)
1. Infant, Newborn. 2. Infant care – standards. 3. Guideline. 4. Postnatal care.
I. World Health Organization Regional Office for the Western Pacific.
ISBN 978 92 9061 780 8 (NLM Classification: WS 420)
© World Health Organization 2016All rights reserved.
Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press: World Health Organization – 20, avenue Appia – 1211 Geneva 27, Switzerland (tel. +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications – whether for sale or for non-commercial distribution – should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html). For WHO Western Pacific Region publications, requests for permission to reproduce should be addressed to Publications Office, World Health Organization, Regional Office for the Western Pacific, P.O. Box 2932, 1000, Manila, Philippines, fax: +632 521 1036, e-mail: [email protected].
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate borderlines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Cover, photo credit: © WHO/Yoshi Shimizu

CONTENTS
Foreword .................................................................................................................................................................................................................................. v
About the EENC modules .........................................................................................................................................................................................vi
BACKGROUND ......................................................................................................................................................................................................................1
SECTION 1. Review EENC clinical practice ...........................................................................................................................................3
1.1 Exit interviews with postpartum mothers – (Checklist 1) .......................................................................................3
1.2 Chart reviews of postpartum mothers who received an exit interview – (Checklist 2) ........................4
1.3 Observation of delivery practices and environmental hygiene – (Checklists 3a, 3b, 3c) ...................5
1.4 Review of availability of key medicines and supplies for EENC – (Checklist 4) .........................................6
1.5 Review of hospital policies: support of EENC practices – (Checklist 5)..........................................................6
1.6 Review of EENC coaching status of facility staff (Checklist 6).............................................................................7
1.7 Review of hospital impact indicators (Checklists 7a, 7b) ......................................................................................7
SECTION 2. Identify and prioritize EENC strengths and areas for improvement ..............................................8
SECTION 3. Identify priority actions for improving EENC ...................................................................................................10
CHECKLISTS .........................................................................................................................................................................................................................13
CHECKLIST 1. Exit interviews with postpartum mothers..........................................................................................................................14
CHECKLIST 2. Chart reviews of postpartum mothers who received an exit interview ...........................................................16
CHECKLIST 3a. Delivery practice for the breathing baby ............................................................................................................................18
CHECKLIST 3b. Delivery practice for the non-breathing baby ..................................................................................................................20
CHECKLIST 3c. Environmental hygiene ...................................................................................................................................................................22
CHECKLIST 4. Review of availability of key medicines and supplies for EENC ............................................................................24
CHECKLIST 5. Review of hospital policies: support of EENC practices ............................................................................................26
CHECKLIST 6. EENC coaching summary ............................................................................................................................................................28
CHECKLIST 7a. EENC hospital impact indicators ............................................................................................................................................29
CHECKLIST 7b. Progress in EENC hospital impact indicators in the previous 12 months .......................................................30


v
Foreword
WHO, Member States and stakeholders in the Western Pacific Region share a vision for mothers and their children: that every newborn infant have the right to a healthy start in life.
But now one newborn infant dies every two minutes – often needlessly – in the Region.
Together, we have taken bold steps to address this grim statistic, with Member States endors-ing the Action Plan for Healthy Newborn Infants in the Western Pacific Region (2014–2020). The plan aims to improve the quality of care for mothers and babies in health facilities, where the vast majority of children are born in the Region.
We offer five teaching modules of Early Essential Newborn Care, or EENC, starting with the Early Essential Newborn Care Clinical Practice Pocket Guide. Since its release, reviews and research have shown impressive reductions in death, infection and intensive care unit admis-sions in facilities employing EENC.
The current volume, Introducing and sustaining EENC in hospitals: routine childbirth and newborn care, is the third module for improving EENC health provider practices in facilities across the Region.
These modules are critical components of the regional plan of sustained action and strong policies utilizing proven methods for saving money and lives. Already governments, health-care facilities and families are saving precious resources, making health systems more accountable and quality care more attainable.
Together, we must push beyond the era of the Millennium Development Goals and meet the even loftier targets for the Sustainable Development Goals: a global maternal mortality ratio of less than 70 per 100 000 live births with no country above 140; and a neonatal mortality rate of less than 12 per 1000 births in countries.
To reach these ambitious targets, we must work together with Member States and partners to bring improved high-quality EENC to all mothers and newborn infants in every stretch of the Region.
Shin Young-soo, MD, Ph.D.Regional Director

ABOUT THE EARLY ESSENTIAL NEWBORN CARE MODULES
The fi ve Early Essential Newborn Care (EENC) modules support planning, imple-mentation, improvement, and monitoring and evaluation of EENC.
Module Title Primary user level
1 Annual implementation reviews and planning National and subnational
2 Coaching for the First Embrace – Facilitator's GuideNational and subnational facilitators
p 3Introducing and sustaining EENC in hospitals:
routine childbirth and newborn care
Hospital with national support for scale up
4Introducing and sustaining EENC in hospitals:
Kangaroo Mother Care (KMC) for preterm infants
5Introducing and sustaining EENC in hospitals:
managing childbirth and postpartum complications
Module 1 is used at the national and subnational levels to collect data for development of annual and 5-year national strategic plans.
National and subnational facilitators use Module 2 to upgrade skills of health workers provid-ing routine childbirth and newborn care nationwide. In hospitals, EENC teams are formed to regularly assess and improve quality of care using Module 3. Once excellent routine childbirth and newborn care are well established, coaching and quality of improvement for Kangaroo Mother Care (KMC) for preterm infants is done with Module 4. Lastly, management of childbirth and postpartum complications is added using Module 5 (see below).
FACILITATORS GUIDE
Coaching guide for the First Embrace
E A R L Y E S S E N T I A L N E W B O R N C A R E ( E E N C ) M O D U L E 2
M O D U L E 2
Routine childbirth and newborn careINTRODUCING AND SUSTAINING EENC IN HOSPITALS
E A R L Y E S S E N T I A L N E W B O R N C A R E ( E E N C ) M O D U L E 3
M O D U L E 3
Kangaroo mother care (KMC) for preterm infantsINTRODUCING AND SUSTAINING EENC IN HOSPITALS
E A R L Y E S S E N T I A L N E W B O R N C A R E ( E E N C ) M O D U L E 4
M O D U L E 4
Managing childbirth and postpartum complicationsINTRODUCING AND SUSTAINING EENC IN HOSPITALS
E A R L Y E S S E N T I A L N E W B O R N C A R E ( E E N C ) M O D U L E 5
M O D U L E 5
2-day coaching KMC for pre-term infants
Managing complications
Formation of EENCteam
Quarterly EENC assessments through weekly / bi-weekly progress monitoring meetings to improve clinical practice
vi
p

1
This module aims to provide the EENC hospital team with a practical approach to assess and improve the quality of routine childbirth and newborn care. The team will use data from observations, interviews and reviews of charts, policies and hospital registers to complete checklists, identify priorities and develop plans.
PARTICIPANTS
EENC team members include paediatricians, obstetricians, nurses, midwives and infection control, quality improvement and hospital administration staff (maximum of 25). These should include senior staff in key positions as well as mid-level staff to carry out the work. Participants are divided into small groups and collect data using checklists.
TIMING
Six to 13 weeks after the 2-day First Embrace coaching, an initial full EENC quality as-sessment is conducted. Thereafter, regular team meetings are held at least monthly. A day-long EENC quality assessment (Module 3, 4 or 5) is conducted at least twice a year. The EENC team may decide to conduct assessments more frequently, depending on the status and quality of EENC practice.
MATERIALS NEEDED FOR INITIAL FULL EENC QUALITY ASSESSMENT
Module 3 (one per participant); flipchart (1–2) with A1-size paper (10); markers (10), tape.
BACKGROUND

2
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
TABLE 1. Content of the full EENC quality assessment
Quality improvement action
Tasks Tools Method followed in orientation
SECTION 1: Review EENC clinical practice
• Interview postpartum mothers Checklist 1
Data collection in pairs/groups, then summarize in plenary
• Review charts of postpartum mothers Checklist 2
• Observe delivery practice and environmental hygiene
Checklists 3a, 3b, 3c
• Review availability of key medicines and supplies for EENC Checklist 4
• Review hospital policies: support of EENC practices Checklist 5
• Review EENC coaching status of facility staff Checklist 6
• Review hospital impact indicators Checklists 7a, 7b
SECTION 2: Identify and prioritize EENC strengths and areas for improvement
• Identify and prioritize EENC strengths
Table 2Group work per topic, then plenary discussion
• Identify and prioritize EENC areas for improvement
SECTION 3: Identify priority actions for improving EENC
• Develop action steps
Table 3Group work per topic, then plenary discussion
• Assign responsibility
• Review progress regularly

3
Exit interviews with postpartum mothers Checklist 10
Instructions
1. Divide the EENC team into pairs, with each pair conducting at least two exit interviews – one person interviewing and the other recording. Altogether, a minimum of 10 interviews should be conducted. Interviews should be completed before women are discharged.
2. Select a room away from patients and staff for conducting interviews. If this is not possible, locate a quiet corridor or area where the conversation can be more private.
3. Select mothers using these criteria:
– Delivered at least three hours prior to the interview.
– A mix of women with normal vaginal deliveries, assisted deliveries, and caesarean sections (when present) and babies in the neonatal care unit (NCU).
– Have not been admitted for abortion, or had a stillbirth or newborn death.
– If 10 or fewer postpartum mothers meeting the criteria are available, select all mothers.
– If more than 10 postpartum mothers meeting the selection criteria are available, use a random sampling method.1
4. Obtain informed oral consent. State, “We are trying to understand your delivery experi-ence so that we can help improve care for women. Everything you say here will be kept confidential, meaning no one will know you said it. Anytime you want to stop, you may. Your care will remain the same. Do you agree to do this interview?” Record informed consent if given.
1. If more than 20 women meet the selection criteria, consider systematic random sampling. Number the women in the delivery admission register in the order they arrived. Divide the total number of admissions in the register by 10 to �nd the sampling interval (for example, if 40 women meet the criteria, select every fourth women on the list). Start randomly and use the sampling interval to select women from the random start until 10 women have been sampled.
1.1
SECTION 1.
REVIEW EENC CLINICAL PRACTICE

4
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
5. Conduct the exit interview and record in a notebook.
– State: “We would like to start by asking you to describe what happened to you from the moment you went into labour until now.”
– Probe: the silent probe (i.e. maintaining silence even after you feel uncomfortable) with head nods is very effective in allowing women to tell their story. This can be followed by: “so the first thing that happened was… [repeat what was said], what happened next?” Keep probing to fill in the details.
– Write down the “story” of her labour and delivery. Ask her to tell it in her own words. Record the story in a notebook, making special note of responses to questions in Checklist 1 – Exit interviews with postpartum mothers. If by the end, the mother does not tell you specific details spontaneously, then use the questions in Checklist 1. For #12 in Checklist 1, you will need to ask the mother the question as she is unlikely to mention this in her narration. If the mother answers “yes”, ask her to show you the items she has bought herself or received from baby food companies.
– The questions in Checklist 1 should not be used to conduct the interview until the mother has finished telling the story.
6. Extract information from notebook and record in Checklist 1 indicating Y (Yes), N (No), or as otherwise instructed in the questions.
7. In plenary, tally findings from all exit interviews in the summary column of Checklist 1.
Chart reviews of postpartum mothers who received an exit interview Checklist 20
Instructions
1. In pairs, use the identification numbers of the mother and baby to identify the charts of women who already received an exit interview. If mothers’ charts are separate from those of their babies, it may be necessary to review both to complete the chart review.
2. In pairs, complete Checklist 2 – Chart reviews of postpartum mothers who received an exit interview. If data are not recorded in the chart, the response is “NR” (Not Recorded).
3. In plenary, tally the results in the summary column of Checklist 2.
1.2

5
Observation of delivery practices and environmental hygiene
Instructions
Observation of delivery practices Checklists 3a and 3b0
1. Ask delivery and operation room staff to notify the group of pending deliveries and cae-sarean sections. At least five deliveries should be observed. As cases requiring resuscitation are uncommon, participants may not have the opportunity to observe such a delivery.
2. In pairs, move about to get a clear view without obstructing the birth attendant(s), speak-ing or intervening.
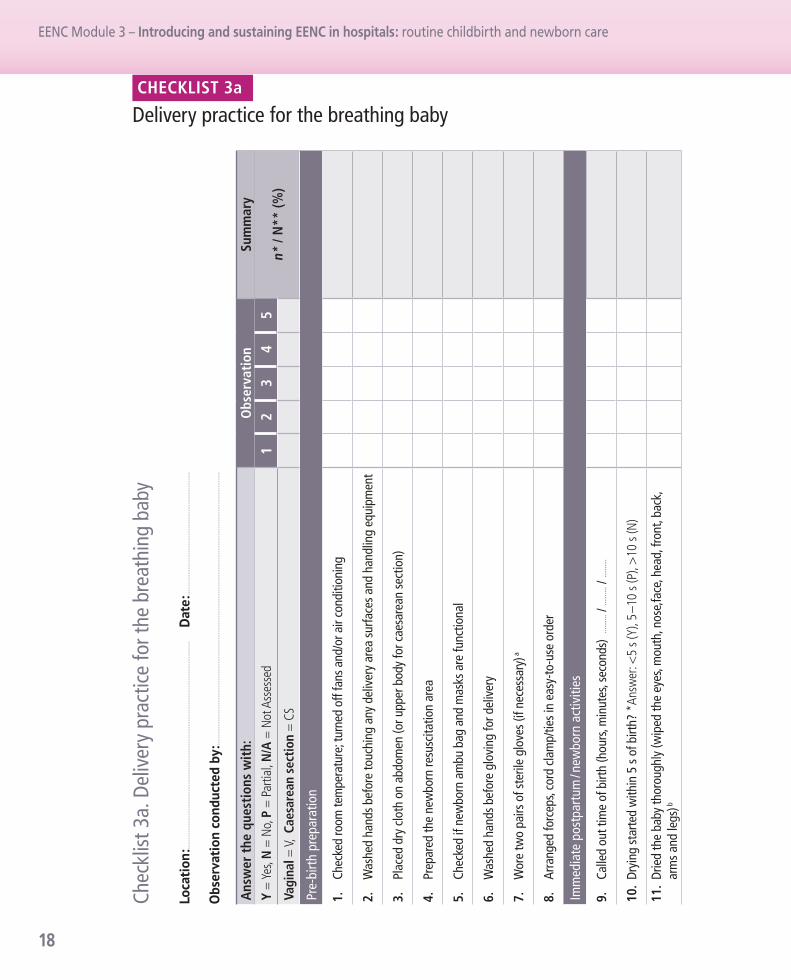
3. Observe the same delivery, record findings individually on Checklist 3a – Delivery practice for the breathing baby or Checklist 3b – Delivery practice for the non-breathing baby as: correctly done (Y = Yes), incompletely done (P = Partial) or not done or done incorrectly (N = No). If a practice is not assessed, indicate N/A and provide details in the “Comments” column.
4. After each observation, score the checklist: 2 points for “Yes”, 1 point for “Partial” and 0 points for “No.” The maximum possible score for delivery of a breathing baby (Checklist 3a) is 42 and non-breathing baby (Checklist 3b) is 60. Upon completion, compare findings in the pair and reconcile differences. Record average scores and score ranges in completed checklists.
5. Give feedback to staff at the end of the delivery away from the mother. Provide positive feedback first, then describe areas for improvement.
Observation of environmental hygiene Checklist 3c0
1. Observe handwashing facilities and toilets for patients, newborn resuscitation areas and supply and equipment in delivery rooms, postnatal care rooms (PNC) and neonatal care units.
2. Complete Checklist 3c – Environmental hygiene.
3. For each aspect of environmental hygiene assessed, record the total number of observa-tions (N) and of these, how many meet the criteria asked (n)?
4. Give feedback to staff at the end of the review on areas for improvement.
1.3

6
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Review of availability of key medicines and supplies for EENC Checklist 40
Instructions
1. Review the list of medicines and supplies by direct observation – staff who work in ante-natal care (ANC), delivery, postnatal care and neonatal care areas are often familiar with the availability of essential medicines, equipment and supplies and can help identify where medicines and supplies are stored and answer key questions.
2. If EENC team members are unsure of the status of some medicines or supplies, determine who should be consulted to determine the status. This may include staff from the relevant section or the hospital pharmacy.
3. Complete Checklist 4 – Review of availability of key medicines and supplies for EENC.
– The WHO definition of normal storage conditions is: “Storage in dry, well-ventilated premises at temperatures of 15–25 °C or, depending on climatic conditions, up to 30 °C”.
– Note items not available on the day of the review and those that have had stock-outs in the previous 12 months. Note problems with storage or functionality of equipment.
– Note whether stock records are available for all items.
Review of hospital policies: support of EENC practices Checklist 50
Instructions
1. Get copies of hospital policies listed in Checklist 5 – Review of hospital policies: support of EENC practices.
Note: national policies are not included unless a written policy is available at the hospital.
2. Record policies seen in Checklist 5 and identify policies currently not available.
3. Determine whether all relevant staff have been oriented on the available written policies.
1.4
1.5

7
Review of EENC coaching status of facility staff Checklist 60
Instructions
1. List the types of health professionals at the hospital involved in childbirth, postnatal and newborn cares in Checklist 6 – EENC coaching summary.
2. Identify the total number of staff for each type of health professional.
3. Identify the total number of staff coached and the number who still need to be coached. Ensure new and trainee staff are included and that staff who have departed are not counted. If any staff members have been coached more than once, count them only once.
4. Decide on a responsible person and time line for completing coaching.
5. Identify resources needed to complete coaching such as manikins, essential supplies or other materials. Discuss sources of support.
Review of hospital impact indicators Checklist 70
Instructions
1. Review data collected for the last 12 months for each hospital impact indicator – indicators are summarized in Checklist 7a – EENC hospital impact indicators.
– Discuss the type of database most suitable for the facility (Excel database, other elec-tronic database). If necessary, discuss adaptation of the database format to facilitate data entry and reporting.
– Discuss problems with collecting data for hospital impact indicators, such as record completeness or case-definitions and possible solutions.
– Discuss and note trends in indicators over the past 12 months (changes in mortality or case-fatality rates, changes in asphyxia, sepsis, prematurity or low-birth weight, and NCU admission rates), and possible reasons for observed trends in Checklist 7b – Progress in EENC hospital impact indicators in the previous 12 months.
– Note data inconsistencies and gaps in the database, and possible reasons and solu-tions for them.
1.6
1.7

8
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Instructions
1. Draw Checklists 1, 2, 3a, 3b, 3c, 4, 5, 6 and 7 on flipcharts and enter the data collected.
2. Draw Table 2 – Identifying and prioritizing strengths and areas for improvement for EENC on another flipchart.
3. Post completed flipcharts of each checklist around the room in order (Checklists 1, 2, 3a, 3b, 3c, 4, 5, 6 and 7).
4. Starting on Checklist 1, identify strengths and gaps including those that have not been re-corded in checklists. Mark the two or three most important gaps, giving consideration to:
– importance to improving EENC clinical practice;
– whether action to address the gap can be taken with existing resources and personnel; and
– whether action to address the gap can be taken in the next three months.
5. Reach consensus on the most important strengths, gaps and underlying reasons. Write them word-for-word on Table 2.
SECTION 2.
IDENTIFY AND PRIORITIZE EENC STRENGTHS AND AREAS FOR IMPROVEMENT

9
TABLE 2. Identifying and prioritizing strengths and areas for improvement for EENC
Areas StrengthsPriority areas
for improvement Underlying reasons
Clinical practice a
Environmental hygiene
Key medicines and supplies
Hospital policies
EENC coaching for staff
Hospital impact indicators
a. Based on data collected from exit interviews, chart reviews, and observations of deliveries.

10
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Purpose
Actions required to address areas needing improvement are developed, based on the underly-ing reasons for gaps identified in the previous step. Responsibilities are allocated to members of the EENC team. Some solutions will be relatively easy to implement with available staff and resources. Others may require the intervention of senior hospital managers or additional resources. Some solutions may require actions outside of the hospital – for example advocacy to improve supply of essential medicines or commodities.
Instructions
1. Draw Table 3 – Priority actions for improving EENC on a flipchart and post next to Table 2. Referring to Table 2, discuss priority actions to address underlying issues, person(s) respon-sible and timing. Leave status blank (it will be updated during subsequent team meetings).
2. Discuss and agree on up to three actions per priority area for improvement. Answer the following questions:
– If we complete our actions, will we improve EENC?
– Can we measure if the action has been completed?
– Can we feasibly complete it within three months? (Or for longer-term priorities, can we substantially start the process within three months?)
3. Write the agreed actions on the flipchart.
4. Agree on the date and time of the next EENC hospital team meeting.
5. Discuss mechanisms to ensure that quarterly EENC assessments are carried out.
SECTION 3.
IDENTIFY PRIORITY ACTIONS FOR IMPROVING EENC

11
TABLE 3. Priority actions for improving EENC
Priority actions Person responsible Time Status date
Clinical practice
Environmental hygiene
Key medicines and supplies
Hospital policies
EENC coaching for staff
Hospital impact data


13
EENC Module 3 Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Checklists
CHECKLIST 1. Exit interviews with postpartum mothers..........................................................................................................................14
CHECKLIST 2. Chart reviews of postpartum mothers who received an exit interview ...........................................................16
CHECKLIST 3a. Delivery practice for the breathing baby ............................................................................................................................18
CHECKLIST 3b. Delivery practice for the non-breathing baby ..................................................................................................................20
CHECKLIST 3c. Environmental hygiene ...................................................................................................................................................................22
CHECKLIST 4. Review of availability of key medicines and supplies for EENC ............................................................................24
CHECKLIST 5. Review of hospital policies: support of EENC practices ............................................................................................26
CHECKLIST 6. EENC coaching summary ............................................................................................................................................................28
CHECKLIST 7a. EENC hospital impact indicators ............................................................................................................................................29
CHECKLIST 7b. Progress in EENC hospital impact indicators in the previous 12 months .......................................................30
A printable Excel file for data entry and automatic calculation of summary information is available at:http://www.wpro.who.int/reproductive_maternal_newborn_child_adolescent/publications/20160901-mca-template.xlsx.

14
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Chec
klist
1. E
xit i
nter
view
s w
ith p
ostp
artu
m m
othe
rs
Que
stio
n M
othe
r nu
mbe
rSu
mm
ary
Ans
wer
the
que
stio
ns w
ith:
Y (=
Yes
) or N
(= N
o)1
23
45
67
89
10n*
/ N
** (%
)
1.
Verb
al in
form
ed c
onse
nt o
btai
ned
2.
Iden
tifyi
ng in
form
atio
n of
mot
her a
nd b
aby
(p
rovi
de h
ere)
3.
Mod
e of
del
iver
y (V
= v
agin
al, C
S =
caes
area
n se
ctio
n)n
CS =
4.
Age
of th
e ba
by (i
n ho
urs)
5.Du
ring
child
birth
:a.
was
the
mot
her a
llow
ed to
sit,
stan
d or
lay
in
the
posit
ion
she
wan
ted?
b.
if y
es, in
wha
t pos
ition
did
she
spen
d m
ost o
f the
tim
e?
c. di
d th
e m
othe
r hav
e a
com
pani
on o
f her
cho
ice?
d. w
as th
e m
othe
r enc
oura
ged
to e
at a
nd d
rink?
e. di
d an
yone
pus
h do
wn
on th
e m
othe
r’s b
elly?
f. w
as a
n en
ema
done
?
6.W
as th
e ba
by b
athe
d?a.
if
yes,
how
long
afte
r birt
h?
<1
h, 1
–6 h
, 7–2
4 h,
≥ 24
hn
≥ 24
h =
7.W
as th
e ba
by p
lace
d in
ski
n-to
-ski
n co
ntac
t with
th
e m
othe
r?
a. h
ow lo
ng a
fter b
irth
(<1,
1–1
0, 1
1–59
, ≥ 60
min
)?n
< 1
min
=
b. h
ow lo
ng d
id th
e ba
by re
mai
n in
uni
nter
rupt
ed
skin
-to-s
kin
cont
act b
efor
e be
ing
sepa
rate
d fro
m
the
mot
her f
or a
ny re
ason
?
(<10
, 10–
29, 3
0–59
, 60–
89, ≥
90 m
in)
n ≥ 9
0 m
in =
c. ha
d th
e ba
by c
ompl
eted
the
first
bre
astfe
ed
(atta
ched
, dee
p su
ckin
g) b
efor
e be
ing
sepa
rate
d
from
the
mot
her?
CHECKLIST 1
Exit interviews with postpartum mothers

15
Que
stio
n M
othe
r nu
mbe
rSu
mm
ary
Ans
wer
the
que
stio
ns w
ith:
Y (=
Yes
) or N
(= N
o)1
23
45
67
89
10n*
/ N
** (%
)
d. w
hy w
as th
e ba
by se
para
ted
from
the
mot
her?
Reas
ons:
e. di
d th
e ba
by re
ceive
imm
edia
te sk
in-to
-ski
n co
ntac
t, no
sepa
ratio
n fo
r at l
east
90
min
and
unt
il th
e fir
st
brea
stfe
ed w
as c
ompl
eted
?
Answ
er Y
onl
y if:
a <
1 m
in, b
≥ 9
0 m
in a
nd c
= Y
8.
Did
the
baby
sta
y w
ith th
e m
othe
r dur
ing
the
entir
e ho
spita
l sta
y (ro
omin
g in
)?
9.Is
the
mot
her b
reas
tfeed
ing?
a. i
f yes
, how
long
afte
r birt
h di
d th
e ba
by fi
rst
brea
stfe
ed?
(<15
, 15–
90, >
90
min
) (at
tach
ed,
deep
suck
ing)
15 <
n <
90
min
=
b. h
ow lo
ng d
id th
e ba
by b
reas
tfeed
the
first
tim
e?n ≥
15 m
in =
c. sin
ce d
elive
ry, w
as th
e ba
by fe
d an
ythi
ng o
ther
th
an b
reas
tmilk
?
n (#
No)
=
d. d
id th
e ba
by re
ceive
ear
ly (w
ithin
15–
90 m
in)
and
exclu
sive
brea
stfe
edin
g?
An
swer
Y o
nly
if: 1
5 <
a <
90
min
and
c =
N10
.If
the
baby
has
bee
n fe
d an
ythi
ng o
ther
th
an b
reas
tmilk
, wha
t was
giv
en?
Flui
ds g
iven
:
11.
Has
the
baby
bee
n fe
d an
ythi
ng fr
om a
bot
tle?
12.
Was
any
thin
g ap
plie
d to
the
cord
stu
mp?
a. i
f yes
, wha
t was
app
lied?
Su
bsta
nces
:
13.
Does
the
mot
her h
ave
infa
nt fo
rmul
a, b
aby
bottl
es,
gifts
or o
ther
pro
duct
s sp
onso
red
by b
aby
food
co
mpa
nies
with
her
at t
he h
ospi
tal?
a. i
f yes
, ask
her
to sh
ow th
em to
you
and
not
e do
wn
the
type
s of p
rodu
cts.
Prod
ucts
:
CHECKLIST 1
Exit interviews with postpartum mothers (continued)
* n =
tota
l num
ber o
f “Y”
(Yes
) res
pons
es u
nles
s oth
erw
ise
spec
i�ed
**N
= to
tal n
umbe
r of m
othe
rs in
terv
iew
ed

16
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Chec
klist
2. C
hart
revi
ews
of p
ostp
artu
m m
othe
rs w
ho re
ceiv
ed a
n ex
it in
terv
iew
Que
stio
n M
othe
r nu
mbe
rSu
mm
ary
Ans
wer
the
que
stio
ns w
ith:
1
23
45
67
89
10n*
/ N
** (%
) Y
(= Y
es),
N (=
No)
, NR
(= N
ot R
ecor
ded)
1.
Iden
tifyi
ng in
form
atio
n of
mot
her a
nd b
aby
(pro
vide
her
e)
2.
Wer
e sy
phili
s te
st re
sults
from
AN
C w
ritte
n in
the
reco
rd?
3.
Was
poi
nt-o
f-car
e ra
pid
HIV
test
ing
done
or H
IV te
st re
sults
fro
m A
NC
writ
ten
in th
e re
cord
?
4.W
as a
par
togr
aph
com
plet
ed c
orre
ctly
? a
a. i
f par
tial o
r no,
spec
ify re
ason
Mai
n re
ason
s:
5.W
as a
rtific
ial r
uptu
re o
f mem
bran
es (a
mni
otom
y) d
one?
a. i
f yes
, wha
t wer
e th
e in
dica
tions
?M
ain
indi
catio
ns:
6.W
as th
e m
othe
r’s la
bour
indu
ced
or a
ugm
ente
d
with
oxy
toci
n?
a. i
f yes
, wha
t wer
e th
e in
dica
tions
?M
ain
indi
catio
ns:
7.W
as th
e ba
by d
eliv
ered
by
caes
area
n se
ctio
n?
a. i
f yes
, wha
t wer
e th
e in
dica
tions
?M
ain
indi
catio
ns:
8.
Was
an
episi
otom
y do
ne?
a. i
f yes
, wer
e re
stric
ted
crite
ria fo
r epi
sioto
my
used
? b
9.W
as IM
oxy
toci
n gi
ven
afte
r del
iver
y?
10.
Wer
e an
y su
bsta
nces
put
on
the
cord
stu
mp,
e.
g. a
lcoh
ol, t
riple
dye
, gen
tian
viol
et?
a. i
f yes
, wha
t was
app
lied?
Mai
n su
bsta
nces
:
CHECKLIST 2
Chart reviews of postpartum mothers who received an exit interview

17
Que
stio
n M
othe
r nu
mbe
rSu
mm
ary
Ans
wer
the
que
stio
ns w
ith:
1
23
45
67
89
10n*
/ N
** (%
) Y
(= Y
es),
N (=
No)
, NR
(= N
ot R
ecor
ded)
11.
Wer
e th
e fo
llow
ing
asse
ssed
with
in 1
hou
r of d
eliv
ery?
a. v
agin
al b
leed
ing
b. f
unda
l hei
ght a
nd u
terin
e co
ntra
ctio
n
c. p
ulse
and
blo
od p
ress
ure
of th
e m
othe
r
d. t
empe
ratu
re o
f the
mot
her
e. d
ange
r sig
ns o
f the
bab
y
12.
Was
rout
ine
eye
care
giv
en w
ithin
90
min
of b
irth?
c
13.
Was
vita
min
K g
iven
bet
wee
n 90
min
and
6 h
of b
irth?
c
14.
Was
hep
atiti
s B
vacc
ine
give
n w
ithin
24
h of
birt
h? c
15.
Was
BCG
vac
cine
giv
en w
ithin
24
hour
s of
birt
h? c
16.
Whi
ch o
f the
follo
win
g w
ere
asse
ssed
with
in 6
hou
rs
of d
eliv
ery?
a. s
econ
d bl
ood
pres
sure
of m
othe
r
b. u
rine
void
c. f
ull p
hysic
al e
xam
of b
aby
a.
P =
par
tial m
ay b
e ap
plic
able
. If t
he a
sses
sor i
s un
able
to d
eter
min
e w
heth
er th
e pa
rtog
raph
has
bee
n fil
led
corr
ectly
, the
ans
wer
sho
uld
be v
alid
ated
w
ith th
e ov
erse
eing
sta
ff m
embe
r/at
tend
ing
phys
icia
n.b.
A
bnor
mal
pro
gres
sion
of la
bour
; non
-rea
ssur
ing
feta
l hea
rt ra
te p
atte
rn; v
acuu
m o
r for
ceps
del
iver
y; s
houl
der d
ysto
cia.
c.
If tim
ing
of a
dmin
istr
atio
n is
not s
peci
fied,
indi
cate
“Y”
and
“TN
S” (t
ime
not s
peci
fied)
.
Chec
klist
2. C
hart
revi
ews
of p
ostp
artu
m m
othe
rs w
ho re
ceiv
ed a
n ex
it in
terv
iew
(con
tinue
d) CHECKLIST 2
Chart reviews of postpartum mothers who received an exit interview (continued)
* n =
tota
l num
ber o
f “Y”
(Yes
) res
pons
es u
nles
s oth
erw
ise sp
eci�
ed**
N =
tota
l num
ber o
f cha
rts r
evie
wed
18
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Chec
klist
3a.
Del
iver
y pr
actic
e fo
r the
bre
athi
ng b
aby
Loca
tion:
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
.. D
ate:
......
......
......
......
......
......
......
......
......
......
......
......
Obs
erva
tion
cond
ucte
d by
: ......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
....
Ans
wer
the
que
stio
ns w
ith:
Obs
erva
tion
Sum
mar
yY
= Y
es, N
= N
o, P
= P
artia
l, N
/A =
Not
Ass
esse
d 1
23
45
n* /
N**
(%)
Vagi
nal =
V, C
aesa
rean
sec
tion
= C
S
Pre-
birt
h pr
epar
atio
n
1.
Chec
ked
room
tem
pera
ture
; tur
ned
off f
ans a
nd/o
r air
cond
ition
ing
2.
Was
hed
hand
s be
fore
touc
hing
any
del
iver
y ar
ea s
urfa
ces
and
hand
ling
equi
pmen
t
3.
Plac
ed d
ry c
loth
on
abdo
men
(or u
pper
bod
y fo
r cae
sare
an s
ectio
n)
4.
Prep
ared
the
new
born
resu
scita
tion
area
5.
Chec
ked
if ne
wbo
rn a
mbu
bag
and
mas
ks a
re fu
nctio
nal
6.
Was
hed
hand
s be
fore
glo
ving
for d
eliv
ery
7.
Wor
e tw
o pa
irs o
f ste
rile
glov
es (i
f nec
essa
ry) a
8.
Arra
nged
forc
eps,
cord
cla
mp/
ties
in e
asy-
to-u
se o
rder
Imm
edia
te p
ostp
artu
m / n
ewbo
rn a
ctiv
ities
9.
Calle
d ou
t tim
e of
birt
h (h
ours
, min
utes
, sec
onds
) ...
......
. / ...
......
. / ...
......
.
10.
Dryi
ng s
tarte
d w
ithin
5 s
of b
irth?
*An
swer
: <5
s (Y)
, 5 –
10 s
(P),
>10
s (N
)
11.
Drie
d th
e ba
by th
orou
ghly
(wip
ed th
e ey
es, m
outh
, nos
e,fa
ce, h
ead,
fron
t, ba
ck,
arm
s an
d le
gs) b
CHECKLIST 3a
Delivery practice for the breathing baby

19
Ans
wer
the
que
stio
ns w
ith:
Obs
erva
tion
Sum
mar
yY
= Y
es, N
= N
o, P
= P
artia
l, N
/A =
Not
Ass
esse
d 1
23
45
n* /
N**
(%)
Vagi
nal =
V, C
aesa
rean
sec
tion
= C
S
Imm
edia
te p
ostp
artu
m / n
ewbo
rn a
ctiv
ities
(con
tinue
d)
12.
Rem
oved
the
wet
clo
th
13.
Plac
ed b
aby
in d
irect
ski
n-to
-ski
n co
ntac
t
14.
Cove
red
baby
’s bo
dy w
ith c
loth
and
hea
d w
ith a
hat
15.
Chec
ked
for a
sec
ond
baby
c
16.
Inje
cted
oxy
toci
n IM
to m
othe
r with
in 1
min
ute
17.
Rem
oved
firs
t (so
iled)
pai
r of g
love
sa
18.
Chec
ked
for c
ord
pulsa
tions
bef
ore
clam
ping
, cla
mpe
d af
ter c
ord
pulsa
tions
st
oppe
d (u
sual
ly 1
–3 m
inut
es)
19.
Plac
ed c
lam
p/tie
at 2
cm
, for
ceps
at 5
cm
, fro
m u
mbi
lical
bas
e
20.
Deliv
ered
pla
cent
a
21.
Coun
selle
d m
othe
r on
feed
ing
cues
(dro
olin
g, m
outh
ope
ning
, ton
guin
g/lic
king
, ro
otin
g, b
iting
han
d, c
raw
ling,
etc
.) –
*Ans
wer
: > 2
cue
s (Y)
, 1–2
cue
s (P)
Tota
l sco
re =
(# Y
es x
2) +
(# P
arti
al)
(m
axim
um s
core
pos
sible
= 4
2)
Aver
age
scor
e =
Scor
e ra
nge
(from
low
est t
o hi
ghes
t) =
a.
If de
liver
y is
by c
aesa
rean
sec
tion
or a
sep
arat
e bi
rth
atte
ndan
t is
avai
labl
e to
han
dle
the
cord
, mak
e a
note
in “
Sum
mar
y”. I
f a s
epar
ate
birt
h at
tend
ant i
s av
aila
ble
to h
andl
e th
e co
rd a
nd u
ses
ster
ile g
love
s w
hen
doin
g so
, sco
re p
ract
ice
as “
Y” (Y
es).
b.
Dedu
ct 5
poi
nts
if su
ctio
ned
unle
ss b
aby
was
drie
d th
orou
ghly
and
bab
y ha
d no
tone
and
am
niot
ic fl
uid
was
mec
oniu
m s
tain
ed.
c.
For c
aesa
rean
sec
tions
, sco
re th
is as
“Y”
(Yes
).
* n =
tota
l num
ber o
f “Y”
(Yes
) res
pons
es u
nles
s oth
erw
ise sp
eci�
ed**
N =
tota
l num
ber o
f obs
erva
tions
Chec
klist
3a.
Del
iver
y pr
actic
e fo
r the
bre
athi
ng b
aby
(con
tinue
d) CHECKLIST 3a
Delivery practice for the breathing baby (continued)

20
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
CHECKLIST 3b
Delivery practice for the non-breathing babyCh
eckl
ist 3
b. D
eliv
ery
prac
tice
for t
he n
on-b
reat
hing
bab
yLo
catio
n:...
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
.....
Dat
e: ...
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
...
Obs
erva
tion
cond
ucte
d by
: ......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
....
Act
ivit
yO
bser
vati
onSu
mm
ary
Y =
Yes
, N =
No,
P =
Par
tial,
N/A
= N
ot A
sses
sed
12
n* /
N**
(%)
Vagi
nal =
V, C
aeas
area
n se
ctio
n =
CS
Pre-
birth
pre
para
tion
1.
Chec
ked
room
tem
pera
ture
; tur
ned
off f
ans a
nd/o
r air
cond
ition
ing
2.
Was
hed
hand
s be
fore
touc
hing
any
del
iver
y ar
ea o
r equ
ipm
ent
3.
Plac
ed d
ry c
loth
on
abdo
men
(or u
pper
bod
y fo
r cae
sare
an s
ectio
n)
4.
Prep
ared
the
new
born
resu
scita
tion
area
5.
Chec
ked
if ne
wbo
rn a
mbu
bag
and
mas
k ar
e fu
nctio
nal
6.
Was
hed
hand
s be
fore
glo
ving
for d
eliv
ery
7.
Wor
e 2
pairs
of s
teril
e gl
oves
(if n
eces
sary
) a
8.
Arra
nged
forc
eps,
cord
cla
mp/
ties
in e
asy-
to-u
se o
rder
Imm
edia
te p
ostp
artu
m / n
ewbo
rn a
ctiv
ities
9.
Calle
d ou
t tim
e of
birt
h (h
ours
, min
utes
, sec
onds
) ....
...... /
......
.... /
......
...
10.
Dryi
ng s
tarte
d w
ithin
5 s
of b
irth?
*An
swer
: < 5
s (Y
), 5–
10 s
(P),
>10
s (N
)
11.
Drie
d th
e ba
by th
orou
ghly
(wip
ed th
e ey
es, m
outh
/nos
e, fa
ce, h
ead,
fron
t, ba
ck, a
rms
and
legs
)
12.
Rem
oved
the
wet
clo
th
13.
Put b
aby
in d
irect
ski
n-to
-ski
n co
ntac
t
14.
Cove
red
baby
’s bo
dy w
ith c
loth
and
hea
d w
ith a
hat
15.
Det
erm
ined
whe
ther
the
baby
was
gas
ping
or n
ot b
reat
hing
16.
Calle
d fo
r hel
p an
d in
form
ed th
e m
othe
r

21
CHECKLIST 3b
Delivery practice for the non-breathing baby (continued)A
ctiv
ity
Obs
erva
tion
Sum
mar
yY
= Y
es, N
= N
o, P
= P
artia
l, N
/A =
Not
Ass
esse
d1
2n*
/ N
** (%
)Va
gina
l = V,
Cae
asar
ean
sect
ion
= C
S
17.
Rem
oved
firs
t (so
iled)
pai
r of g
love
s a
18.
Qui
ckly
cla
mpe
d an
d cu
t cor
d
19.
Mov
ed b
aby
to re
susc
itatio
n ar
ea
20.
Cove
red
baby
qui
ckly
dur
ing
and
afte
r tra
nsfe
r
21.
Posit
ione
d he
ad c
orre
ctly
to o
pen
airw
ays
22.
Appl
ied
face
mas
k fir
mly
ove
r chi
n, m
outh
and
nos
e
23.
Gai
ned
ches
t rise
with
in 1
min
ute
of b
irth b :
......
.... m
in .
......
... s
24.
Sque
ezed
bag
to g
ive
30–5
0 br
eath
s pe
r min
ute
25.
Mai
ntai
ned
good
che
st ri
se th
roug
hout
or t
ook
step
s to
impr
ove
vent
ilatio
n
26.
Afte
r bab
y br
eath
ing
wel
l, st
oppe
d ve
ntila
tion
27.
Retu
rned
to s
kin-
to-s
kin
cont
act,
cove
red
baby
28.
Chec
ked
for a
sec
ond
baby
c
29.
Gav
e ox
ytoc
in IM
to th
e m
othe
r
30.
Deliv
ered
pla
cent
a
31.
Coun
selle
d m
othe
r on
babi
es s
tatu
s fo
llow
ing
resu
scita
tion
and
on fe
edin
g cu
es
*Ans
wer
> 2
cue
s (Y)
, 1–2
cue
s (P)
Tota
l sco
re =
(# Y
es x
2) +
(# P
arti
al)
(m
axim
um s
core
= 6
2) d
Aver
age
scor
e =
Scor
e ra
nge
(from
low
est t
o hi
ghes
t) =
a.
If de
liver
y is
by c
aesa
rean
sec
tion,
or a
sep
arat
e bi
rth
atte
ndan
t is
avai
labl
e to
han
dle
the
cord
, mak
e a
note
in “
Sum
mar
y”. I
f a s
epar
ate
birt
h at
tend
ant i
s av
aila
ble
to h
andl
e th
e co
rd a
nd u
ses
ster
ile g
love
s w
hen
doin
g so
, sco
re p
ract
ice
as “
Y” (Y
es).
b.
O
nly
scor
ed a
s “Y
es”
or “
No”
– N
o: “
Part
ial”
c.
Fo
r cae
sare
an s
ectio
ns, s
core
this
as “
Y” (Y
es).
d.
Dedu
ct 5
poi
nts
if re
susc
itatio
n is
perf
orm
ed w
hen:
(1) t
he b
aby
is no
t br
eath
ing
but
has
mus
cle
tone
and
grim
ace,
and
(2) t
he b
aby
is no
t dr
ied
imm
edia
tely
or
thor
ough
ly (e
ither
not
imm
edia
tely,
not
thor
ough
ly o
r not
at a
ll).
* n =
tota
l num
ber o
f “Y”
(Yes
) res
pons
es u
nles
s oth
erw
ise sp
eci�
ed**
N =
tota
l num
ber o
f obs
erva
tions

22
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Chec
klist
3c.
EN
VIRO
NM
ENTA
L HY
GIE
NE
Deliv
ery
room
, rec
over
y ro
om, n
eona
tal c
are
unit
and
post
nata
l car
e ro
om
Que
stio
nDe
liver
y ro
om(s
)Re
cove
ry
room
(s)
Neo
nata
l ca
re u
nit
PNC
room
(s)
Com
men
ts
Han
dwas
hing
faci
litie
s an
d to
ilets
for p
atie
nts a
1.
Is th
ere
a fil
led
alco
hol h
and
gel d
ispen
ser w
ithin
2 m
of e
very
bed
? (Y
/ N
)
2.
Is a
t lea
st o
ne s
ink
for w
ashi
ng h
ands
ava
ilabl
e fo
r use
in th
e ro
om? b
(Y /
N)
3.
Wha
t is
the
tota
l num
ber o
f sin
ks?
(N)
4.Ho
w m
any
sinks
:
a. a
re c
lean
? (n
/N)
b. h
ave
cont
inuo
us su
pply
of c
lean
, run
ning
wat
er?c (
n/N
)
c. ha
ve so
apd a
vaila
ble?
(n/N
)
d. h
ave
singl
e-us
e to
wel
s ava
ilabl
e? (n
/N)
5.W
hat i
s th
e to
tal n
umbe
r of t
oile
ts fo
r pat
ient
s? (N
)
6.Ho
w m
any
toile
ts:
a. a
re fu
nctio
ning
? (n
/N)
b. a
re c
lean
? (n
/N)
New
born
resu
scita
tion
area
7.
How
man
y ot
her r
oom
s ha
ve a
t lea
st 1
resu
scita
tion
area
set
up?
(N)
8.Ho
w m
any
deliv
ery
beds
hav
e a
resu
scita
tion
area
ava
ilabl
e w
ithin
2 m
? (n
/N)
9.
How
man
y re
susc
itatio
n ar
eas
are
avai
labl
e? (N
)
CHECKLIST 3c ENVIRONMENTAL HYGIENE:
Delivery room, recovery room, postnatal care room and neonatal care unit

23
Que
stio
nDe
liver
y ro
om(s
)Re
cove
ry
room
(s)
Neo
nata
l ca
re u
nit
PNC
room
(s)
Com
men
ts
10.
How
man
y re
susc
itatio
n ar
eas:
a. a
re c
lean
and
dry
? (n
/N)
b. h
ave
new
born
am
bu b
ag a
nd m
ask
avai
labl
e? (n
/N)
Sup
plie
s an
d eq
uipm
ent (
Y/N
)
11.
Are
all s
urfa
ces
free
of c
lutte
r?
12.
Are
new
gar
bage
bag
s us
ed fo
r eac
h de
liver
y?e
13.
Are
shar
ps b
oxes
ava
ilabl
e?
14.
At le
ast 1
met
er s
epar
atio
n be
twee
n be
ds?
15.
Clea
n th
erm
omet
ers
and
stet
hosc
opes
and
use
d fo
r eac
h pa
tient
? (s
epar
ate
equi
pmen
t ded
icat
ed to
eac
h pa
tient
; or s
uppl
ies
for c
lean
ing
inst
rum
ents
ava
ilabl
e?e )
Pro
mot
ion
of b
aby
food
com
pany
pro
duct
s
16.
Are
baby
food
com
pany
mat
eria
ls vi
sible
(pos
ters
, bro
chur
es, s
ticke
rs,
pain
ted
wal
ls, c
loth
ing,
etc
.)
17.
Are
hosp
ital o
rder
s pr
ohib
iting
use
of i
nfan
t for
mul
a an
d ot
her l
inka
ges
with
milk
form
ula
com
pani
es v
isibl
e an
d po
sted
som
ewhe
re in
the
area
?
a.
To u
nder
take
a c
ompl
ete
hand
hyg
iene
ass
essm
ent,
see
‘Han
d Hy
gien
e Se
lf-A
sses
smen
t Fra
mew
ork’
(WHO
, 201
0)b.
If
mor
e tha
n one
room
is av
aila
ble i
n a ca
tego
ry, r
epor
t ava
ilabi
lity i
n eac
h roo
m se
para
tely.
Not
e if a
lcoho
l gel
/han
d rub
is av
aila
ble f
or st
aff u
se bu
t not
for u
se by
patie
nts a
nd fa
milie
s.c.
A
wat
er su
pply
that
is e
ither
pip
ed o
r fro
m o
nsite
stor
age,
with
app
ropr
iate
disi
nfec
tion,
mee
ting
appr
opria
te sa
fety
stan
dard
s for
mic
robi
al a
nd c
hem
ical
con
tam
inat
ion.
d.
Soap
: det
erge
nt-b
ased
pro
duct
s th
at c
onta
in n
o ad
ded
antim
icro
bial
age
nts
or m
ay c
onta
in th
ese
sole
ly a
s pr
eser
vativ
es. I
t may
be
in v
ario
us fo
rms
incl
udin
g ba
r so
ap, t
issu
e, le
af a
nd li
quid
pre
para
tions
.e.
Th
ese
ques
tions
are
pre
fera
bly a
nsw
ered
thro
ugh
obse
rvat
ion.
If it
is n
ot p
ossib
le, t
hen
ask
heal
th st
aff.
Indi
cate
‘(R)
’ nex
t to
answ
ers t
hat w
ere
obta
ined
by a
skin
g st
aff.
CHECKLIST 3c ENVIRONMENTAL HYGIENE
Delivery room, recovery room, postnatal care room and neonatal care unit (continued)

24
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
CHECKLIST 4
Review of availability of key medicines and supplies for EENCCh
eckl
ist 4
. Rev
iew
of a
vaila
bilit
y of
key
med
icin
es a
nd s
uppl
ies
for E
ENC
Avai
labl
e
on th
e da
y
of th
e re
view
? (Y
or N
)
Stoc
k co
nditi
on?
No
expi
red
drug
s?
Equi
pmen
t fun
ctio
nal?
Stoc
k re
cord
s ex
ist?
(Y
or N
)
# St
ock-
outs
in
the
past
12
mon
ths
1.
Mag
nesiu
m s
ulfa
te fo
r sev
ere
pre-
ecla
mps
ia a
nd e
clam
psia
, an
d fe
tal n
euro
prot
ectio
n if
gest
atio
nal a
ge <
32 w
eeks
£ N
orm
al s
tora
ge a
£ N
o ex
pire
d dr
ugs
2.
Oxy
toci
n fo
r IM
and
par
ente
ral u
se –
imm
edia
tely
pos
tpar
tum
–
and
for c
ontro
l of h
aem
orrh
age
£ 2
–8 °
C£
Pro
tect
ed fr
om li
ght b
£ N
o ex
pire
d dr
ugs
3.Co
rtico
ster
oids
for w
omen
of 2
4–34
wee
ks o
f ges
tatio
n at
risk
of
pre
term
del
iver
y c
£ N
orm
al s
tora
ge a
£ P
rote
cted
from
ligh
t b
£ N
o ex
pire
d dr
ugs
4.An
tibio
tics
for p
rete
rm p
rela
bour
rupt
ure
of m
embr
anes
d £
Nor
mal
sto
rage
a
£ P
rote
cted
from
ligh
t b
£ N
o ex
pire
d dr
ugs
5.Fu
nctio
nal n
ewbo
rn a
mbu
bag
and
mas
k (s
izes
0 a
nd 1
) w
ithin
2 m
of e
ach
deliv
ery
bed
6.
Oxy
gen
for n
ewbo
rn u
se
7.CP
AP
8.Fu
nctio
nal a
utoc
lave
9.Re
frige
rato
r
10.
Full
deliv
ery
sets
for d
eliv
ery e
11.
Vita
min
K£
Nor
mal
sto
rage
a
£ P
rote
cted
from
ligh
t b
£ N
o ex
pire
d dr
ugs

25
Avai
labl
e
on th
e da
y
of th
e re
view
? (Y
or N
)
Stoc
k co
nditi
on?
No
expi
red
drug
s?
Equi
pmen
t fun
ctio
nal?
Stoc
k re
cord
s ex
ist?
(Y
or N
)
# St
ock-
outs
in
the
past
12
mon
ths
12.
Hepa
titis
B va
ccin
e£
2–8
°C
£ N
o ex
pire
d dr
ugs
13.
BCG
vac
cine
£
2–8
°C
£ N
o ex
pire
d dr
ugs
14.
Inje
ctab
le a
ntib
iotic
s fo
r man
agem
ent o
f new
born
sep
sis£
Nor
mal
sto
rage
a
£ P
rote
cted
from
ligh
t b
£ N
o ex
pire
d dr
ugs
15.
Baby
cap
s –
and
adeq
uate
clo
ths
for d
ryin
g
16.
Func
tiona
l del
iver
y ta
bles
17.
Surg
ical
glo
ves
18.
At le
ast o
ne ta
ble
or tr
olle
y fo
r set
ting
up:
a. d
elive
ry se
ts
b. r
esus
citat
ion
area
s
a.
Stor
age
in d
ry, w
ell-v
entil
ated
pre
mis
es a
t tem
pera
ture
s of
15–
25 °
C or
, dep
endi
ng o
n cl
imat
ic c
ondi
tions
, up
to 3
0 °C
.b.
O
xyto
cin
(com
pare
d to
met
herg
in) i
s re
lativ
ely
less
ligh
t-se
nsiti
ve b
ut it
is s
till g
ood
prac
tice
to p
rote
ct it
from
ligh
t as
ther
e is
a 7%
loss
in p
oten
cy w
hen
expo
sed
to li
ght i
f sto
red
at 2
1–25
°C.
c.
Re
com
men
ded
whe
n th
e fo
llow
ing
cond
ition
s ca
n be
met
: ges
tatio
nal a
ge a
sses
smen
t can
be
accu
rate
ly u
nder
take
n, p
rete
rm b
irth
is co
nsid
ered
imm
inen
t, th
ere
is no
clin
ical
evi
denc
e of
mat
erna
l inf
ectio
n, a
dequ
ate
child
birt
h ca
re is
ava
ilabl
e, a
nd th
e pr
eter
m n
ewbo
rn c
an re
ceiv
e ad
equa
te c
are
if ne
eded
. d.
Pr
eter
m p
rela
bour
rup
ture
of t
he m
embr
anes
is d
efine
d as
rup
ture
of t
he m
embr
anes
bef
ore
labo
ur h
as b
egun
in a
pre
gnan
cy w
ith a
ges
tatio
nal a
ge o
f les
s th
an
37 w
eeks
.e.
De
fined
loca
lly –
incl
udes
all
mat
eria
ls an
d eq
uipm
ent n
eede
d to
con
duct
a n
orm
al d
eliv
ery.
CHECKLIST 4
Review of availability of key medicines and supplies for EENC (continued)

26
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
CHECKLIST 5
Review of hospital policies: support of EENC practicesCh
eckl
ist 5
. Rev
iew
of h
ospi
tal p
olic
ies:
sup
port
of E
ENC
prac
tices
Polic
y ar
eaDo
es th
e ho
spita
l ha
ve a
writ
ten
polic
ya ?Ha
ve s
taff
been
orie
nted
on
the
polic
ya ?
1.
Com
pani
on a
nd p
ositi
on o
f cho
ice
for a
ll de
liver
ies
2.
Mat
erna
l and
feta
l mon
itorin
g du
ring
labo
ur in
clud
ing
use
of th
e pa
rtogr
aph
3.M
ater
nal a
nd n
ewbo
rn m
onito
ring
afte
r del
iver
y?
4.Im
med
iate
new
born
car
e:
a. i
mm
edia
te a
nd th
orou
gh d
ryin
gb.
ski
n-to
-ski
n co
ntac
t for
a m
inim
um o
f 90
min
utes
5.Al
l rou
tine
care
(e.g
. eye
car
e, v
itam
in K
, im
mun
izat
ions
and
exa
min
atio
ns) d
elay
ed u
ntil
af
ter a
full
brea
stfe
ed
6.N
on-s
epar
atio
n of
mot
her a
nd b
aby
unle
ss u
rgen
t car
e is
requ
ired
– in
clud
ing
elim
inat
ion
of
neo
nata
l nur
serie
s fo
r wel
l bab
ies
7.
No
rout
ine
suct
ioni
ng
8.N
o pl
acin
g su
bsta
nces
on
the
cord
stu
mp
9.N
o pr
e-la
ctea
l fee
ds
10.
No
bath
ing
until
at l
east
24
hour
s afte
r del
iver
y
11.
EEN
C cli
nica
l poc
ket g
uide
/nat
iona
l clin
ical s
tand
ards
ado
pted
and
use
d fo
r all
deliv
erie
s
12.
Infe
ctio
n co
ntro
l pra
ctic
es fo
r del
iver
ies
incl
udin
g:
a. h
andw
ashi
ng p
ract
ices
b. u
se o
f dou
ble
glov
esc.
pro
cess
ing
cont
amin
ated
inst
rum
ents
d. d
isinf
ectio
n of
del
ivery
bed
s, eq
uipm
ent,
surfa
ces,
floor
s and
oth
er it
ems
e. di
stan
ce o
f sep
arat
ion
of p
atie
nt b
eds/
belo
ngin
gsf.
was
te m
anag
emen
t
13.
Corti
cost
eroi
ds fo
r wom
en o
f 24–
34 w
eeks
of g
esta
tion
at ri
sk o
f pre
term
del
iver
y
14.
Antib
iotic
s fo
r pre
term
pre
labo
ur ru
ptur
e of
the
mem
bran
es (p
PRO
M)

27
Polic
y ar
eaDo
es th
e ho
spita
l ha
ve a
writ
ten
polic
ya ?Ha
ve s
taff
been
orie
nted
on
the
polic
ya ?
15.
Antid
ote
for m
agne
sium
sul
fate
toxi
city
for m
anag
emen
t of p
re-e
lam
psia
and
ecl
amps
ia
(10%
cal
cium
glu
cona
te)
16.
Inje
ctab
le a
ntih
yper
tens
ive
for m
anag
emen
t of p
re-e
clam
psia
and
ecla
mps
ia (H
ydra
lazin
e 5
mg)
17.
Inje
ctab
le a
ntib
iotic
s fo
r man
agem
ent o
f man
ual r
emov
al o
f the
pla
cent
a (a
mpi
cilli
n or
firs
t-ge
nera
tion
ceph
alos
porin
)18
. KM
C fo
r pre
term
bab
ies
wei
ghin
g ≤
2000
g a
t birt
h in
clud
ing
feed
ing
with
bre
ast m
ilk
and
mon
itorin
g fo
r com
plic
atio
ns
19.
Stan
dard
cas
e-m
anag
emen
t gui
delin
es fo
r the
man
agem
ent o
f new
born
sep
sis
20.
Crite
ria fo
r ind
ucin
g or
aug
men
ting
labo
ur
21.
Crite
ria fo
r con
duct
ing
caes
area
n se
ctio
ns
22.
Rest
ricte
d cr
iteria
for c
ondu
ctin
g ep
isiot
omy
for v
agin
al d
eliv
erie
s
23.
Stab
iliza
tion
of n
ewbo
rns
incl
udin
g pr
even
tion
of h
ypot
herm
ia, h
ypog
lyca
emia
, hyp
oxae
mia
, ap
noea
and
infe
ctio
n pr
ior t
o tim
ely
refe
rral
24.
For b
abie
s w
ith re
spira
tory
dist
ress
:
a. o
xyge
nb.
con
tinuo
us p
ositi
ve a
irway
pre
ssur
e (C
PAP)
25.
Care
of s
erio
usly
ill n
ewbo
rn in
fant
s
26.
Patie
nt–s
taff
ratio
s fo
r:
a. d
elive
ry ro
om
b. p
ostp
artu
m w
ard
c. n
eona
tal c
are
unit
27.
Proh
ibiti
on, p
rom
otio
n, sa
les,
and
use
of in
fant
form
ula
or a
ny li
nkag
es w
ith fo
rmul
a co
mpa
nies
in
the
facil
ity
28.
Fam
ily p
lann
ing
coun
selli
ng b
efor
e di
scha
rge
29.
Rout
ine
repo
rting
of s
tillb
irths
, mat
erna
l dea
ths
and
new
born
dea
ths
a.
If ho
spita
l pol
icie
s ar
e no
t ava
ilabl
e, c
heck
for a
vaila
bilit
y of
writ
ten
natio
nal p
olic
ies
at th
e ho
spita
l and
if s
taff
wer
e or
ient
ed o
n it.
CHECKLIST 5
Review of hospital policies: support of EENC practices (continued)

28
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
Type of health professional
Total #Total
coachedStill to coach
Person responsible for coaching
TimelineOther
resources needed
Total
CHECKLIST 6
EENC coaching summary

29
Indicator Data by yearCountry target
20202015 2016 2017 2018 2019
1. Neonatal care unit / nursery admission rate
2. Proportion of newborn infants by weight:
• < 1000 g
• 1000–1499 g
• 1500–1999 g
• 2000–2499 g
• 2500–3500 g
• > 3500 g
3. Proportion of newborn infants delivered at the facility classified with newborn sepsis a
4. Proportion of newborn infants delivered at the facility classified with birth asphyxia b
5. Newborn mortality rate stratified by weight:
• < 1000 g
• 1000–1499 g
• 1500–1999 g
• 2000–2499 g
• 2500–3500 g
• > 3500 g
6. Case-fatality rate (% registered cases dying)
a. Preterm c newborn infants
b. Low-birth-weight d newborn infants
c. Newborn sepsis
d. Newborn asphyxia
a. Bacterial sepsis of the newborn: ICD-10 P36 (including codes P36.0 – P36.9 bacterial sepsis of known cause or sepsis of unknown cause).
b. Birth asphyxia is defined as newborn infants who are gasping or not breathing at 1 minute of age. c. Preterm newborn infants are live births less than 37 completed weeks gestation (ICD-10 P07.2 and ICD-10 P07.3).d. Low-birth weight is defined as < 2500 g.
CHECKLIST 7a
EENC hospital impact indicators

30
EENC Module 3 – Introducing and sustaining EENC in hospitals: routine childbirth and newborn care
IndicatorAre data
available? Y or N
Details of observed trend
Reasons for observed performance
Neonatal care unit / nursery admission rate
Proportion of newborn infants by birth weight
Proportion of newborn infants with sepsis
Proportion of newborn infants with asphyxia
Newborn mortality by birth weight
Case-fatality rate for sepsis
Case-fatality rate for asphyxia
Case-fatality rate for preterm babies
Case-fatality rate for low-birth-weight babies
CHECKLIST 7b
Progress in EENC hospital impact indicators in the previous 12 months

