interventions in stroke-evidence based management
TRANSCRIPT

1Copyright © 2015 Dr. Vipul Gupta . All rights reserved. 1
Head, Neurointerventional Surgery &Interventional NeuroradiologyNEUROVASCULAR & STROKE CENTRE,Medanta-The Medicity
Dr Vipul Gupta
Interventions in stroke:Interventions in stroke:Evidence based managementEvidence based management

2Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Neurovascular diseases…Stroke…. Third most common cause of death Most common reason for disability Appx. 1 in 4 people die within 1 year 30%–50% do not regain functional
independence Annual incidence rate of stroke in India
currently is 145 per 100,000 population 10 - 15% occur in < 40 years
WHO estimates suggest that by 2050, 80% stroke cases in the world would occur in low and middle income countries mainly India and China
3Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
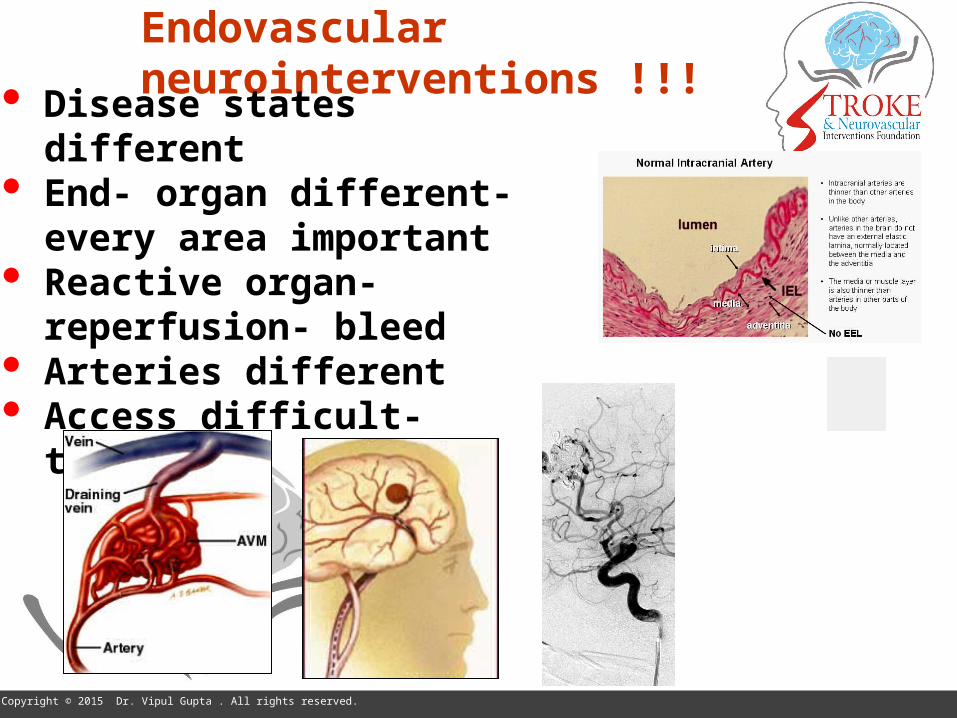
Endovascular neurointerventions !!!
Disease states different End- organ different- every area
important Reactive organ- reperfusion-
bleed Arteries different Access difficult- tortuosity
6Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Neurointerventions…
SAH- aneurysms, vasospasm Intracerebral hemorrhage- AVMs TIA- major vessel stenosis E/C & I/C Stroke- revascularization
Diagnosis- Imaging Interventional hardware Integrated approach

7Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
ISCHAEMIC stroke- brain attack
Penumbra
• At 60 min, about 90%• At 2 h about 80 %• At 3 h about 60% and • At 4.5 h about 40% of patients
Thereafter ?• Maybe 30% at 9 h • And less than 20% beyond 12 h
8Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
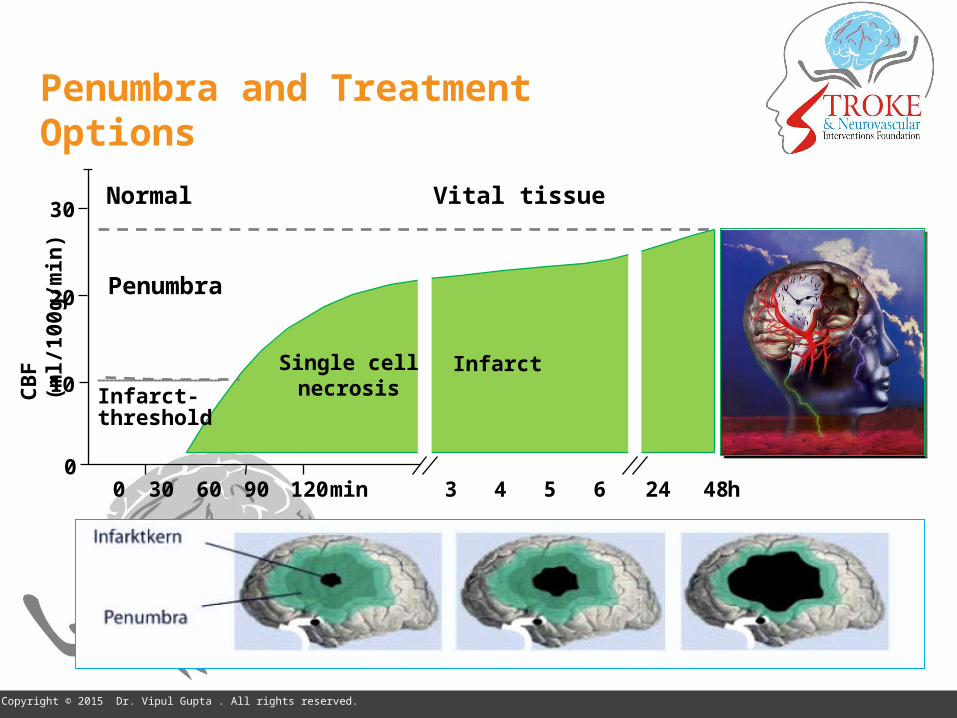
Penumbra and Treatment Options
0
10
20
30
min
CB
F (m
l/100
g/m
in)
300 9060 4120 5 6 24 48h
Infarct-threshold
Penumbra
Normal Vital tissue
InfarctSingle cellnecrosis
3
9Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
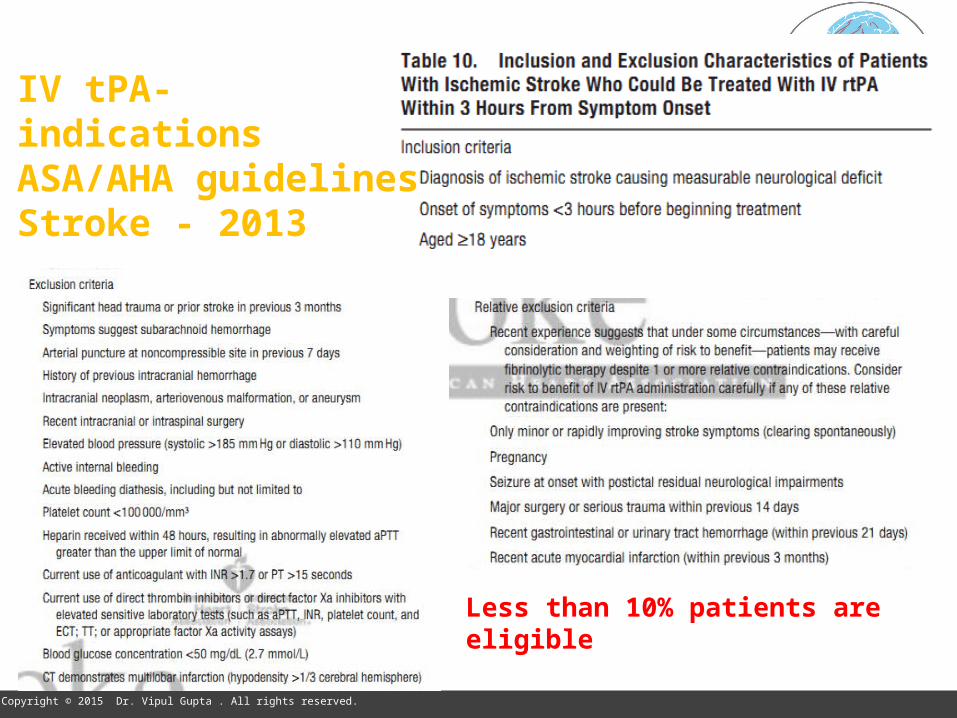
IV tPA- indicationsASA/AHA guidelinesStroke - 2013
Less than 10% patients are eligible
10Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Issues with IV tPA
Time factor Large vessel disease Time to recanalize C.I. – anti-coagulants, recent surgery, wake-up strokes…. < 5 % qualify
11Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
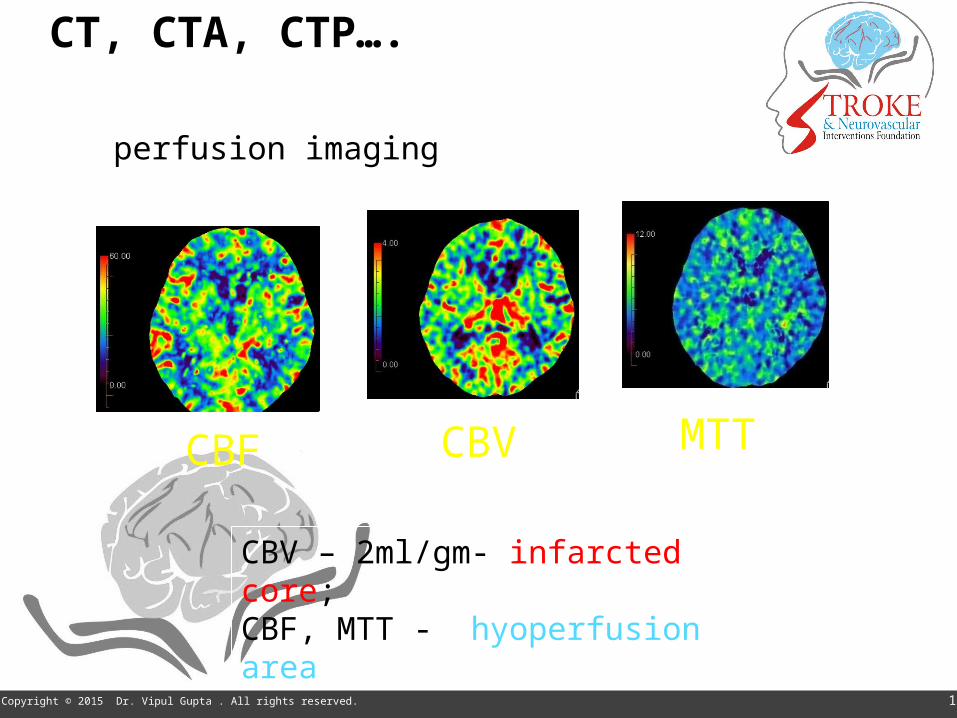
CT, CTA, CTP….
CT perfusion imaging
MTTCBF CBV
CBV – 2ml/gm- infarcted core; CBF, MTT - hyoperfusion area
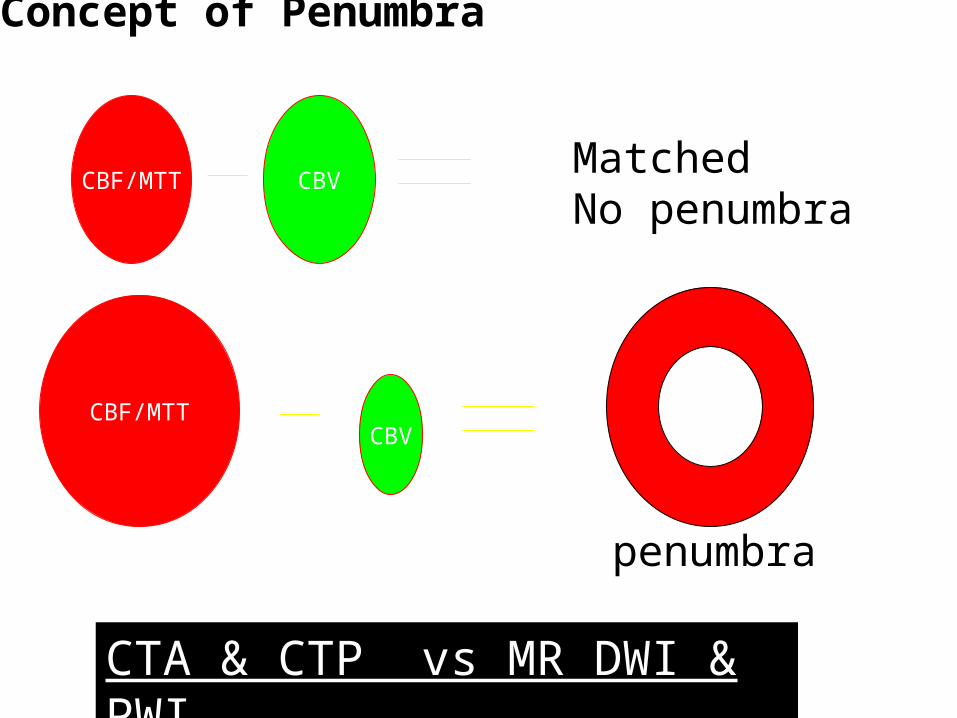
Concept of Penumbra
CBF/MTT CBVMatchedNo penumbra
CBF/MTTCBV
penumbra
CTA & CTP vs MR DWI & PWI
13Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Imaging approaches for case selection
NCCT (ASPECTS)- NIHSS NCCT & CTA, CTA-SI NCCT, CTA & CTP MRI-DWI, (MRA, PWI)
What information is needed?• Bleed• Infarct core – is critical 70-
100 ml• Major vessel occlusion• Tissue at risk- penumbra
Time, imaging interpretation, unstable patients

17Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Evidence – 2014-2015
IMS-III, MR RESCUE & Synthes – failed- no appropriate imaging and old devices Recent trials – imaging for MVO & stent- retreviers MR CLEAN – strongly positive ESCAPE – stopped bcs of efficacy EXTEND –IA – positive DRAMATIC CHANGE IN MGT OF STROKE

MR CLEAN(Netherlands)
ESCAPE(CANADIAN)
EXTEND IA(AUSTRALIAN)
SWIFT PRIME(USA)
REVASCAT(SPANISH)
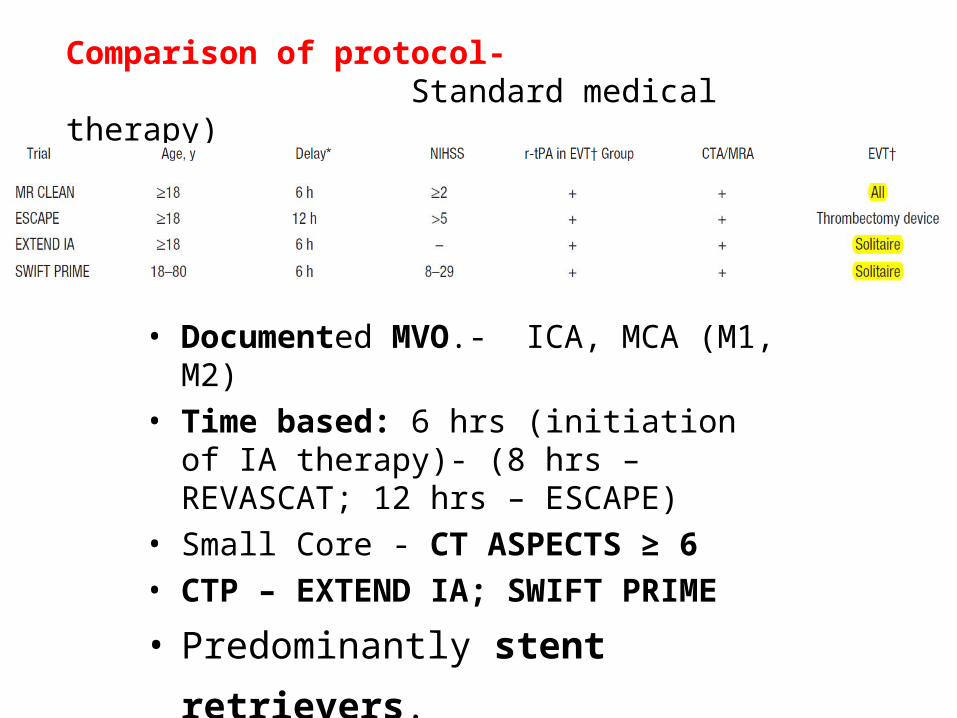
Comparison of protocol- Randomised (Intervention Vs Standard medical therapy)
• Documented MVO.- ICA, MCA (M1, M2)• Time based: 6 hrs (initiation of IA therapy)-
(8 hrs – REVASCAT; 12 hrs – ESCAPE)• Small Core - CT ASPECTS ≥ 6• CTP – EXTEND IA; SWIFT PRIME
• Predominantly stent retrievers. • 86.1 to 100% (100 % in EXTEND IA &
SWIFT PRIME)• (NIHSS scores were 17 (interquartile range,
13–21)
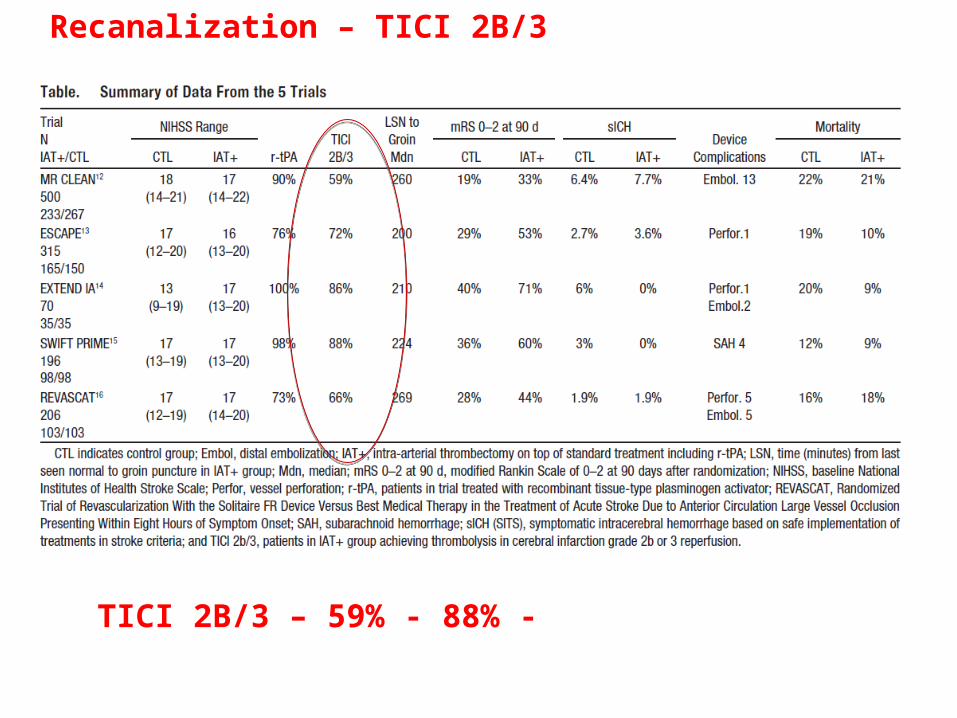
TICI 2B/3 – 59% - 88% - (previous trials 25%, 41%)
Recanalization – TICI 2B/3
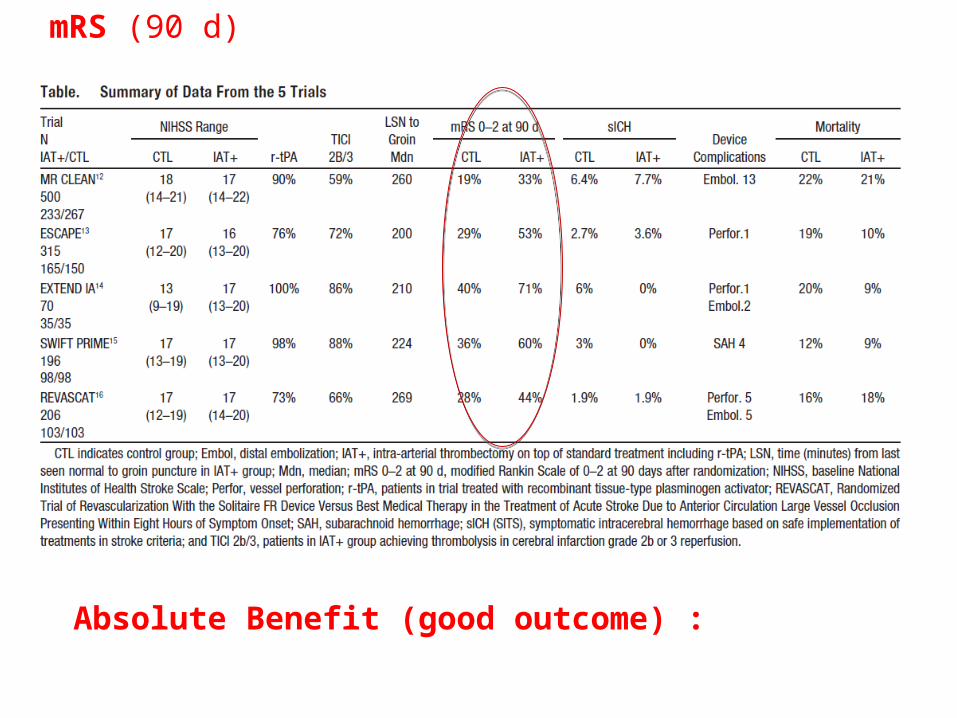
Absolute Benefit (good outcome) : 13.5% to 31.4%(Statistically significant)
mRS (90 d)
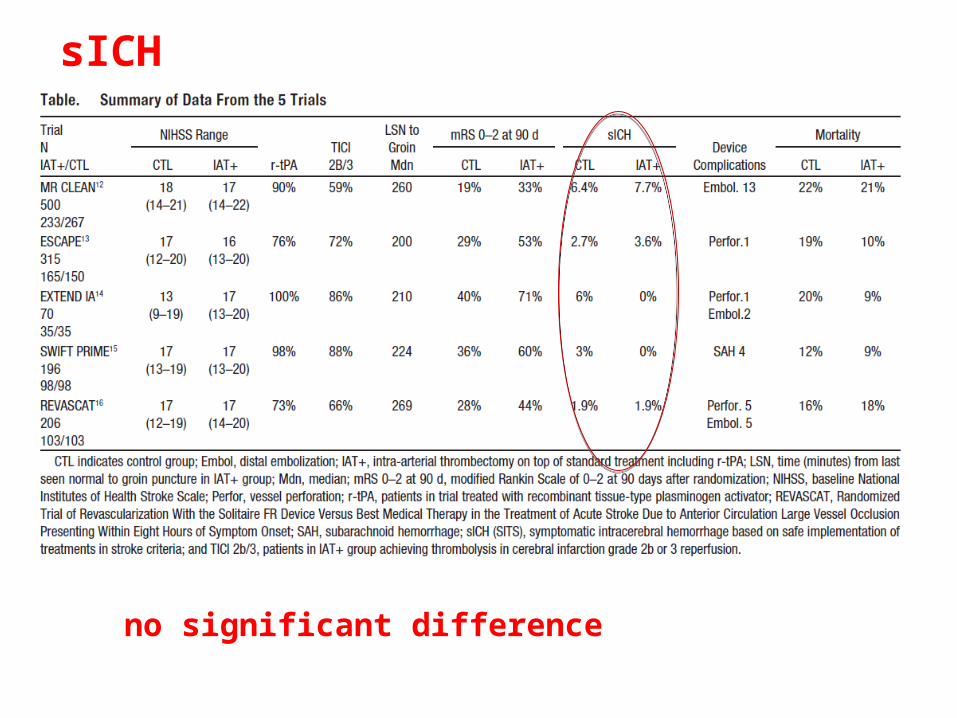
no significant difference
sICH
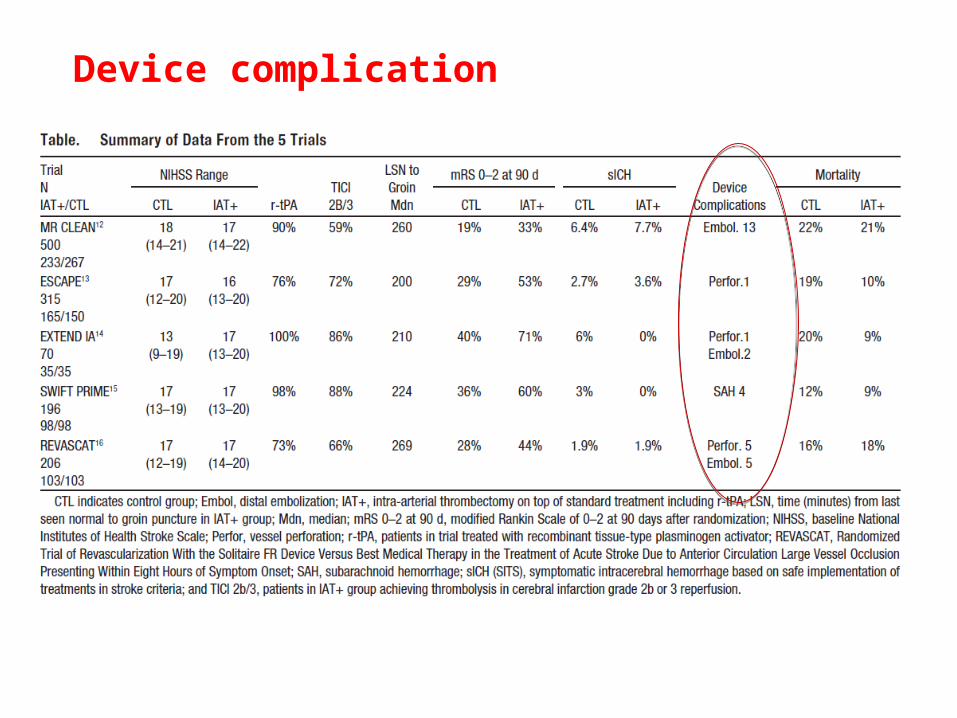
Device complication
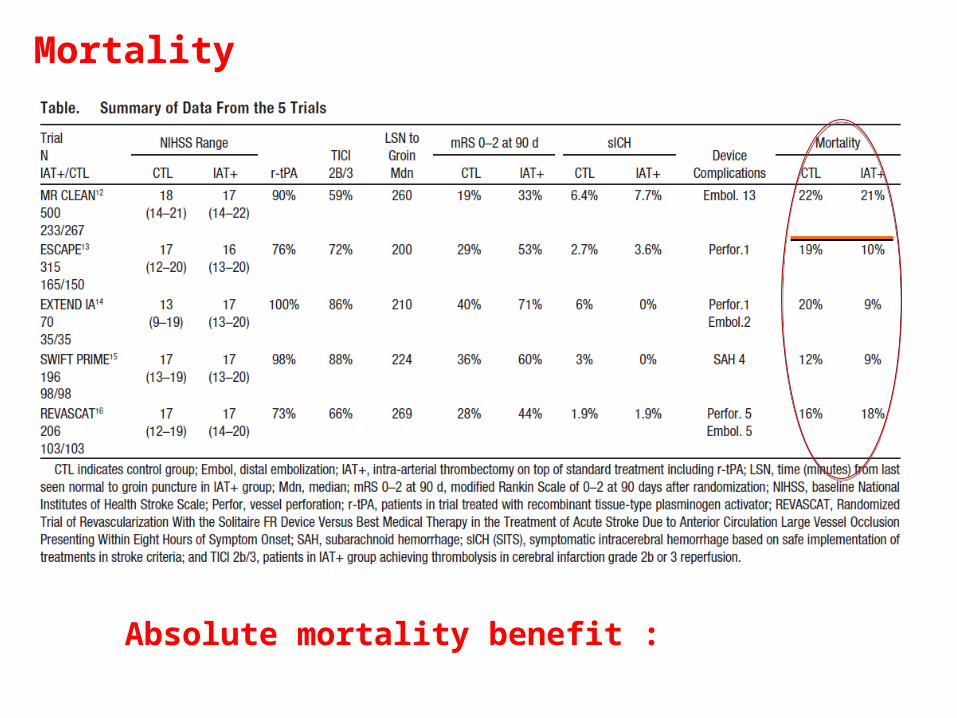
Absolute mortality benefit : 8.6%(Statistically significant in ESCAPE)
Mortality

Comparison of NNT:
EVT: NNT (benefit) - 3.1 to 4.2 (excluding MR CLEAN)
IV tPA ( 3 – 4.5 hours) – 13.8 (ECASS – 3)
Primary PCI (prevent re-infarction) – 33
26Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
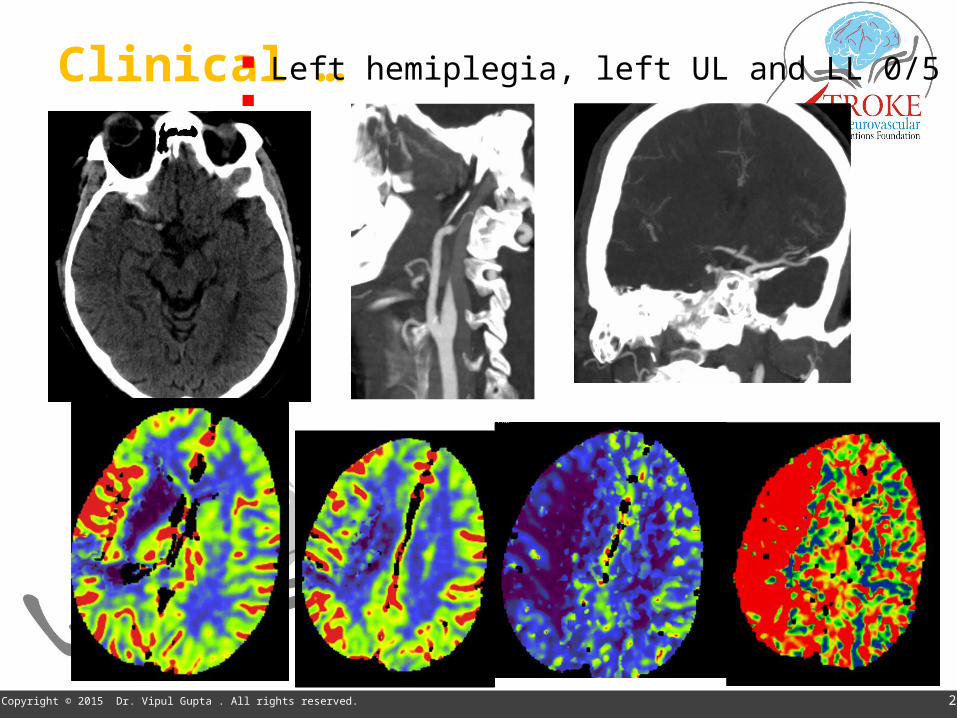
Clinical … Left hemiplegia, left UL and LL 0/5 5:14AM
27Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
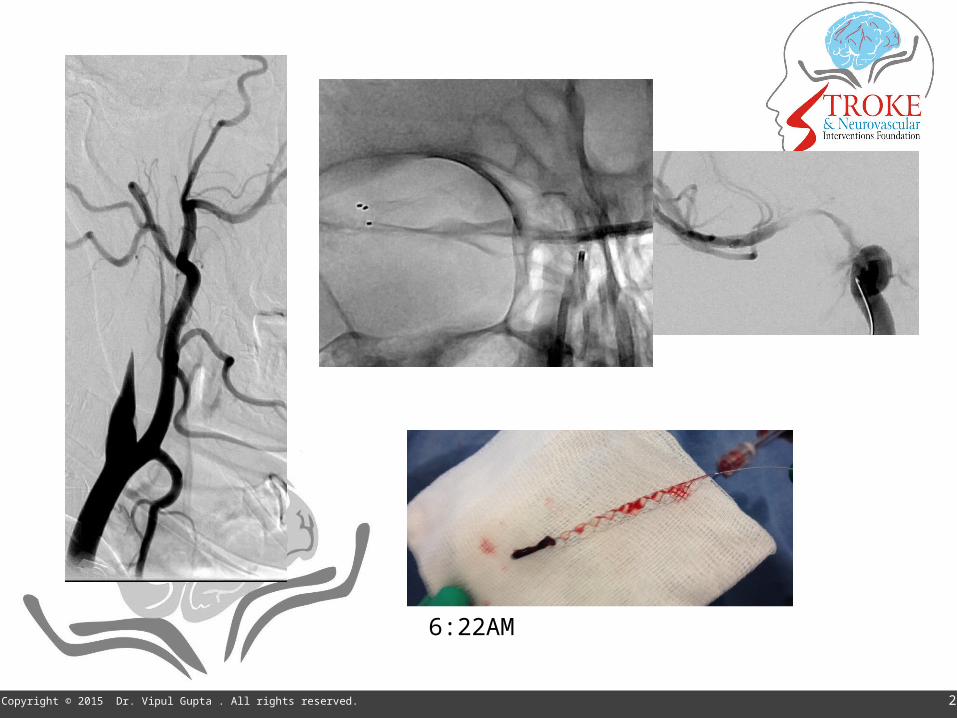
6:22AM
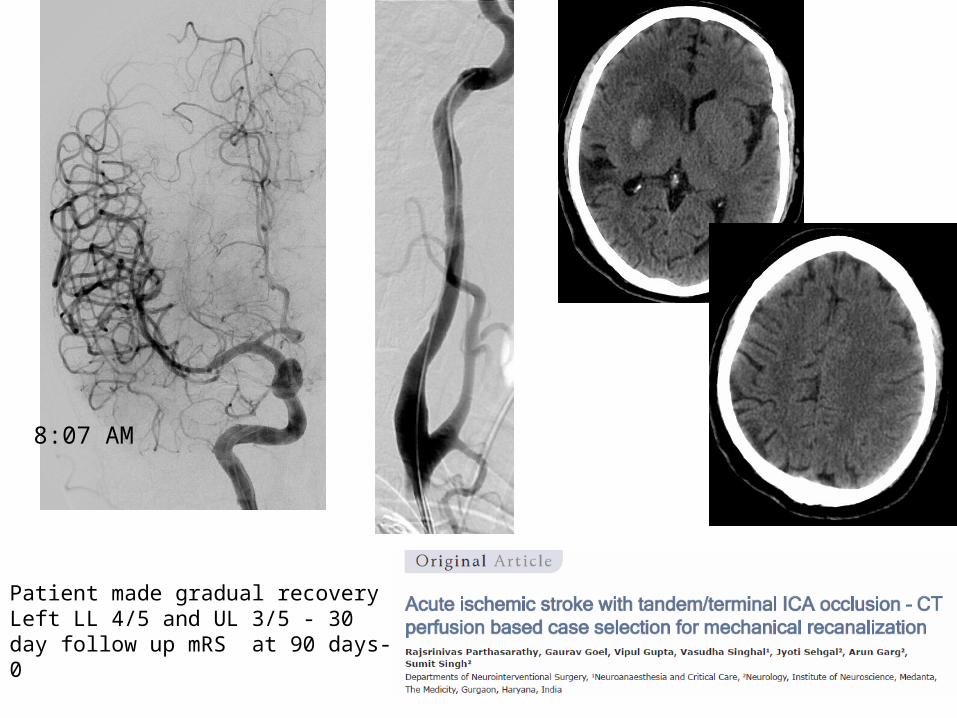
8:07 AM
Patient made gradual recoveryLeft LL 4/5 and UL 3/5 - 30 day follow up mRS at 90 days- 0
29Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
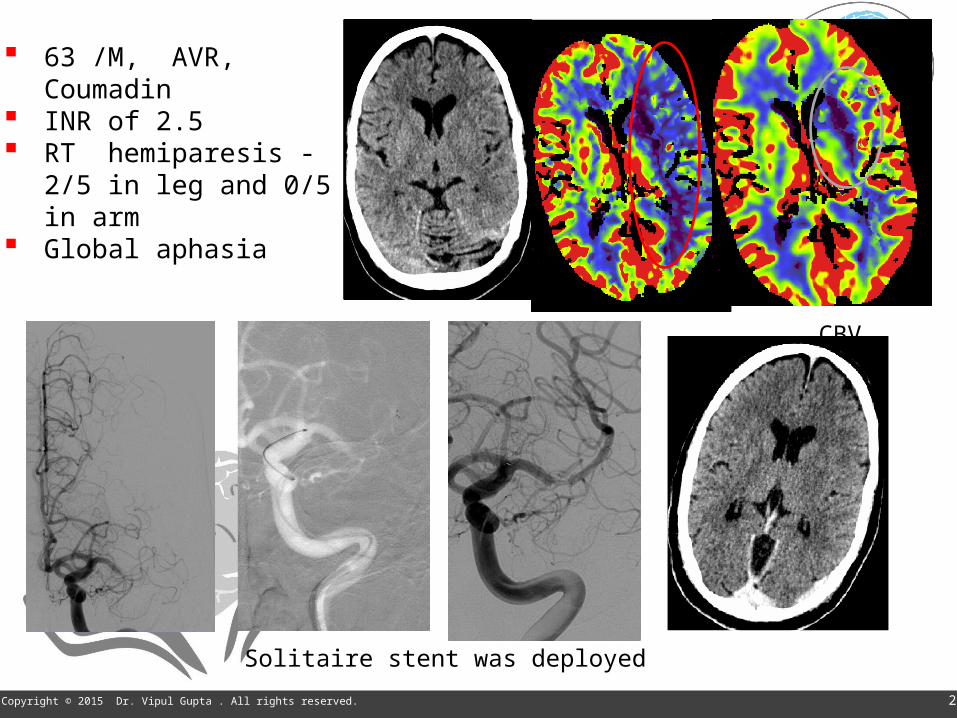
63 /M, AVR, Coumadin INR of 2.5 RT hemiparesis - 2/5 in leg
and 0/5 in arm Global aphasia
CBF CBV
Solitaire stent was deployed
30Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Patient presented with in 2 hours
Futile IV tpa

AHA/ ASA guideline 2015:Patients should receive endovascular therapy with a stent retriever if they meet all the following criteria (Class I; Level of Evidence A). (New recommendation):
prestroke mRS score 0 to 1 acute ischemic stroke receiving intravenous r-tPA within 4.5
hours of onset causative occlusion of the internal carotid artery or proximal
MCA (M1) age ≥18 years NIHSS score of ≥6 ASPECTS of ≥ 6 treatment can be initiated (groin puncture) within 6 hours of
symptom onset
AHA/ ASA guideline:Carefully selected patients with anterior circulation occlusion who have contraindications to intravenous r-tPA, endovascular therapy with stent retrievers completed within 6 hours of stroke onset is reasonable (Class IIa; Level of Evidence C).
Carefully selected patients with acute ischemic stroke in whom treatment can be initiated (groin puncture) within 6 hours of symptom onset and who have causative occlusion of the M2 or M3 portion of the MCAs, anterior cerebral arteries, vertebral arteries, basilar artery, or posterior cerebral arteries (Class IIb; Level of Evidence C)
Waiting after IV tPA not required (Class III)

Beyond 6 hours – Should you consider MT?
ESCAPE: up to 12-hours – positive trial
6 hours49 patientsrate ratio, 1.7; (95% CI, 0.7 to 4.0)
Not significant; however few numbers.
REVASCAT: upto 12 hours, positive trial
Data not provided.

35Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
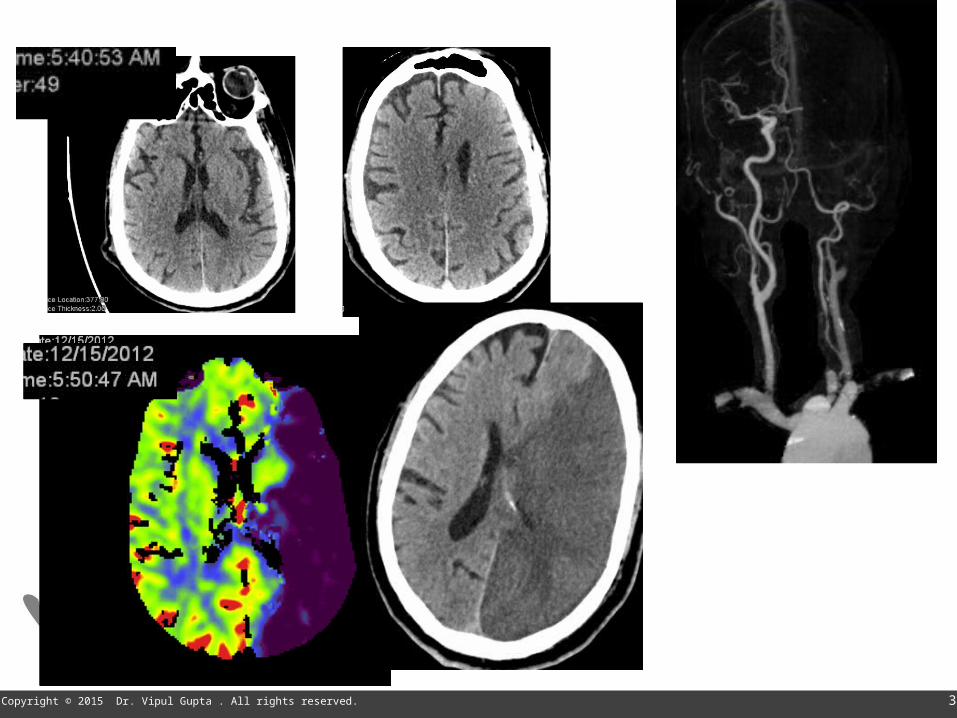
• 60 years old female.Acute onset left hemiparesis and left facial weakness; CT Brain , CTP and CTA done 6 1/2 hours after ictus.
38Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
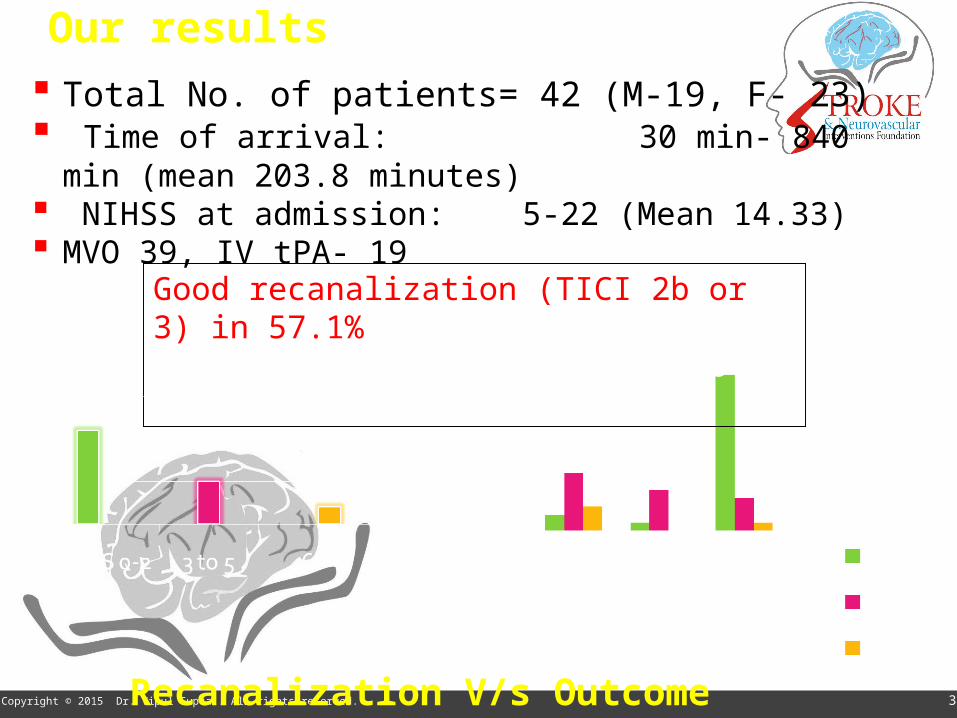
Our results Total No. of patients= 42 (M-19, F- 23) Time of arrival: 30 min- 840 min (mean 203.8 minutes) NIHSS at admission: 5-22 (Mean 14.33) MVO 39, IV tPA- 19
Good recanalization (TICI 2b or 3) in 57.1%mRS 0-2 =52.3%, 3-5 = 34.4%, 6 = 9.5%)
Recanalization V/s Outcome
39Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
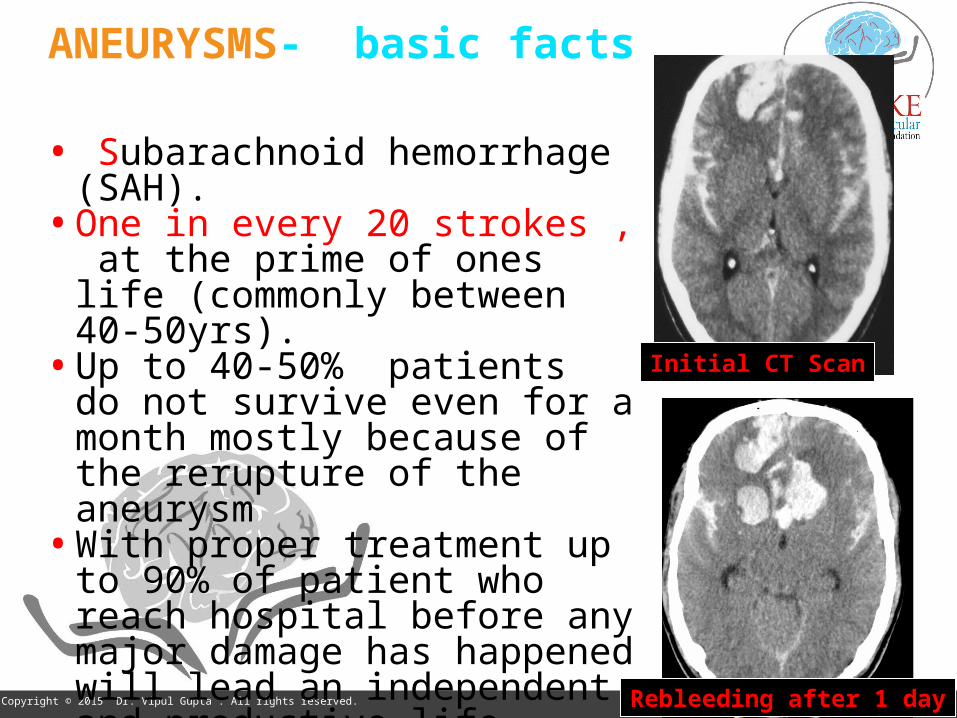
ANEURYSMS- basic facts
• Subarachnoid hemorrhage (SAH).• One in every 20 strokes , at the
prime of ones life (commonly between 40-50yrs).
• Up to 40-50% patients do not survive even for a month mostly because of the rerupture of the aneurysm
• With proper treatment up to 90% of patient who reach hospital before any major damage has happened will lead an independent and productive life
Initial CT Scan
Rebleeding after 1 day

40Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Clipping vs coiling… Initially Surgically inappropriate Tremendous changes in last 15-yrs
Cerebral Aneurysms-
• Image-guidance (3-D , Dyna-CT)• Coil, catheter, balloons, stents • Drugs- aspirin, clopidogrel,
abciximab• Appx. 90% by endovascular • Intra-arterial vasospasm mgt.
• HELP and Cerecyte studies – mRS 0-2 in 87% (80% in ISAT)
41Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
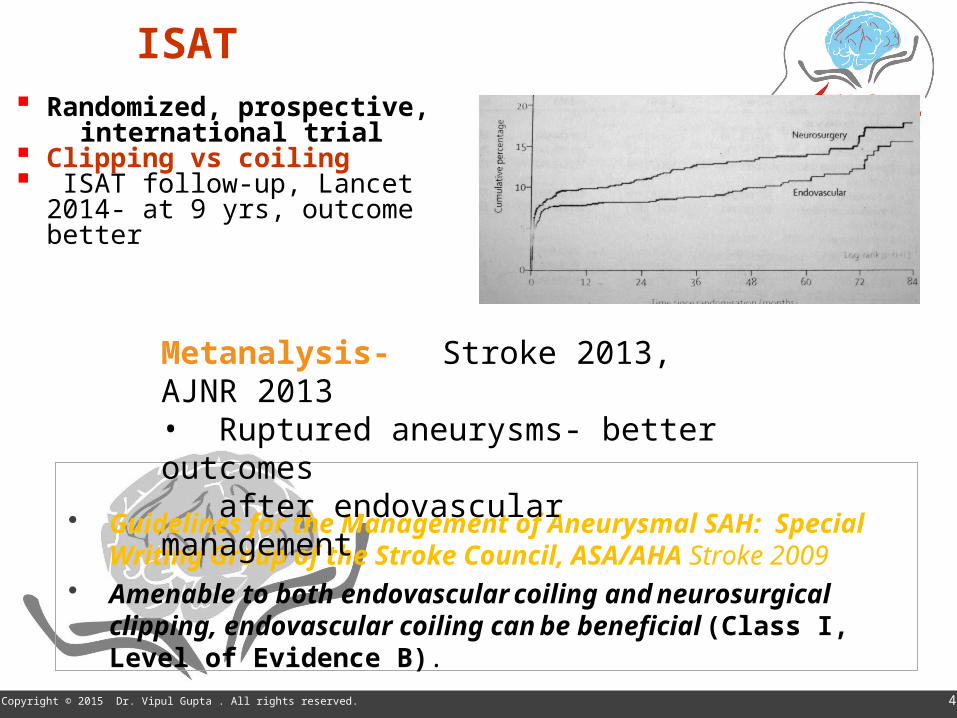
ISAT Randomized, prospective, international trial Clipping vs coiling ISAT follow-up, Lancet 2014- at 9 yrs,
outcome better
Guidelines for the Management of Aneurysmal SAH: Special Writing Group of the Stroke Council, ASA/AHA Stroke 2009
Amenable to both endovascular coiling and neurosurgical clipping, endovascular coiling can be beneficial (Class I, Level of Evidence B).
Metanalysis- Stroke 2013, AJNR 2013• Ruptured aneurysms- better outcomes after endovascular management
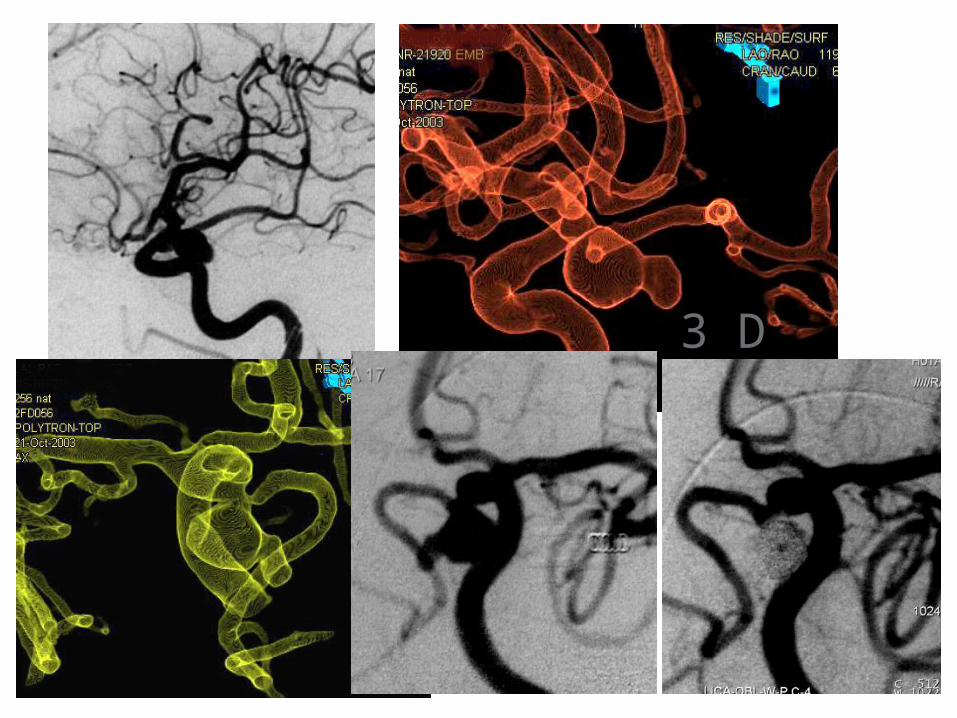
3 D

Broad neck aneurysmBroad neck aneurysm
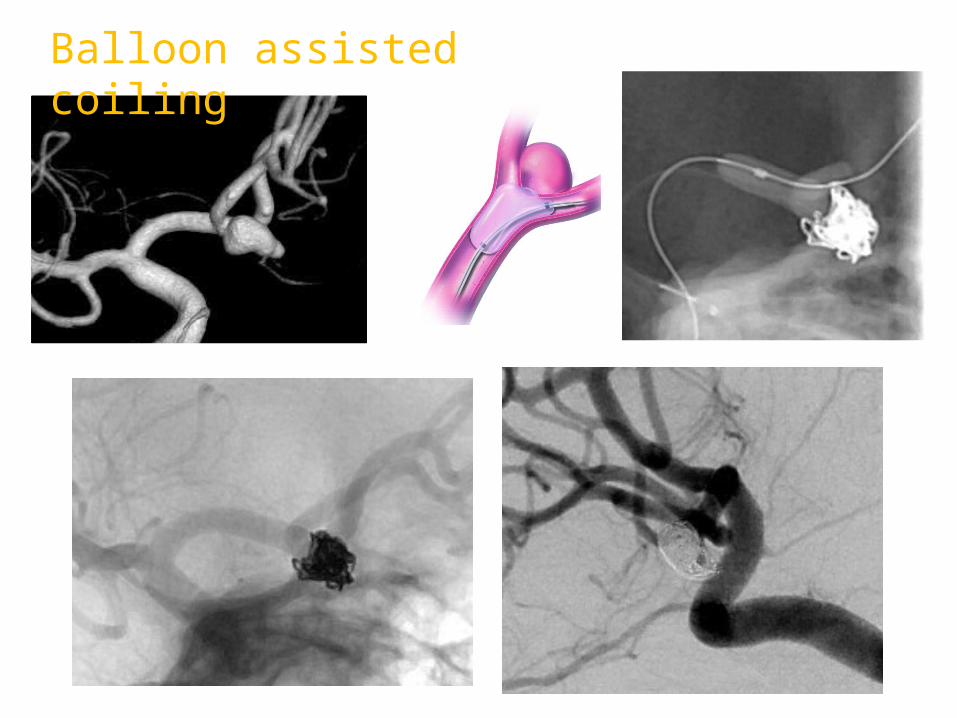
Balloon assisted coiling
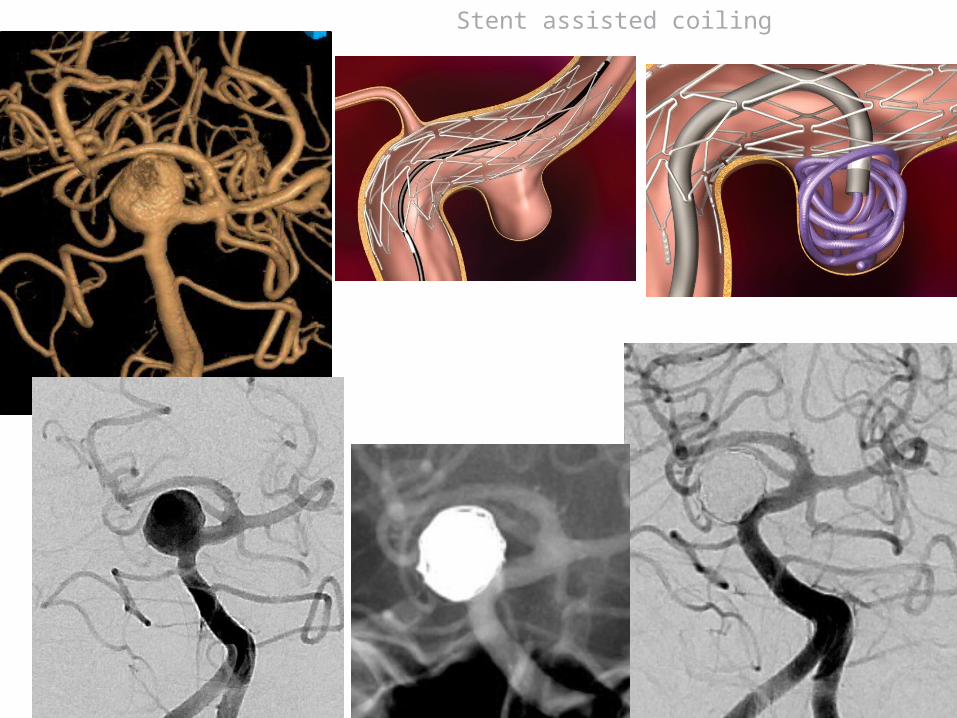
Stent assisted coiling
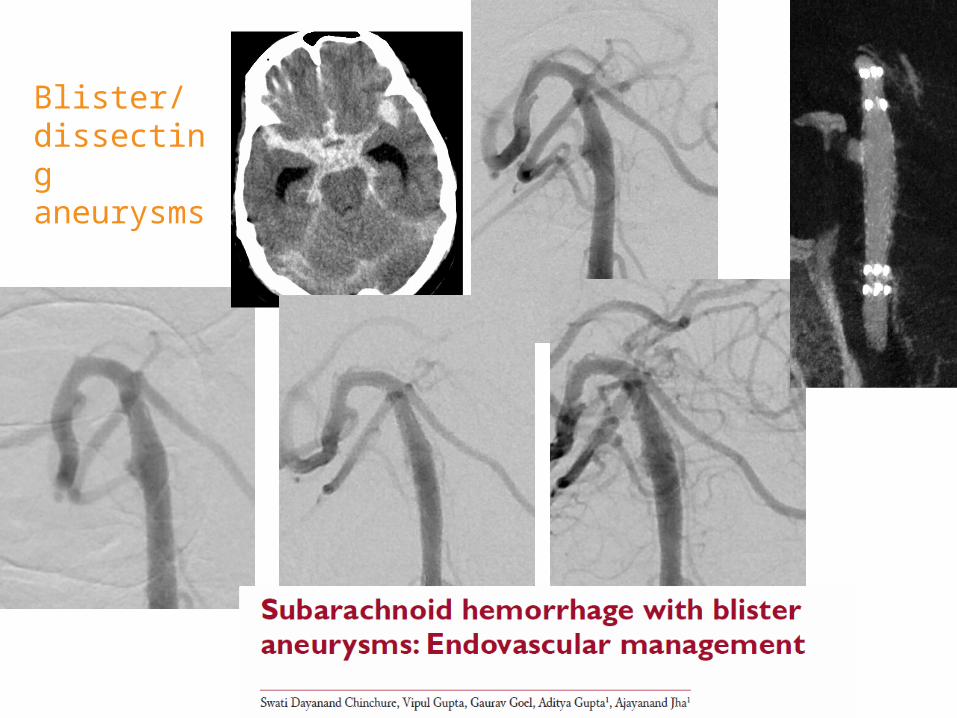
Dissecting blister aneurysm – poor gradeEVD
2-overlapping Enterprise stents 6-months follow-up
Blister/dissecting aneurysms
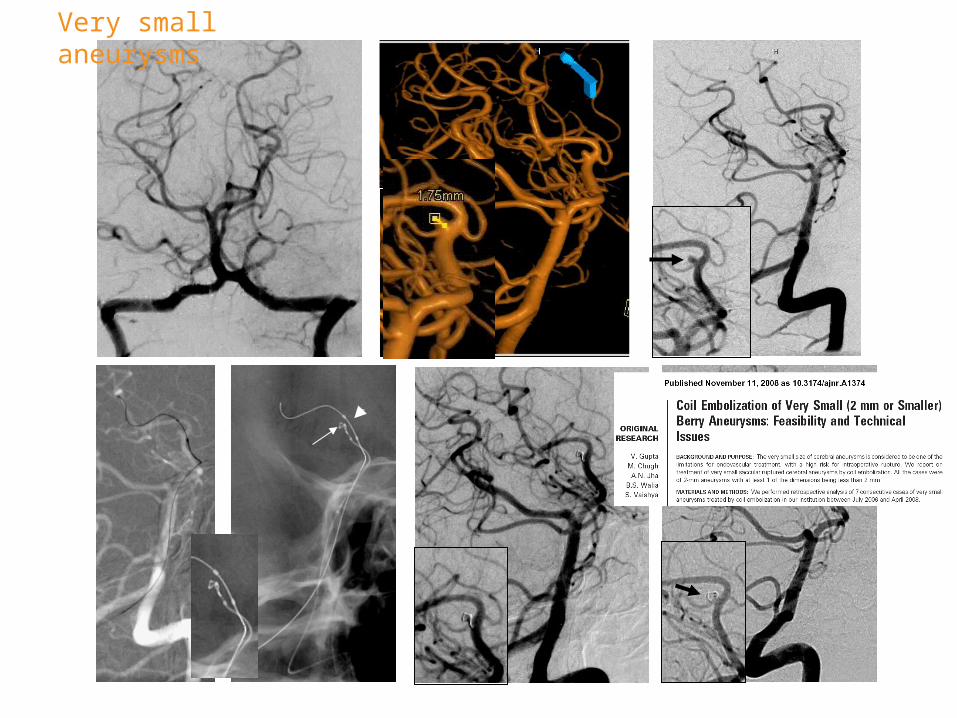
Very small aneurysms
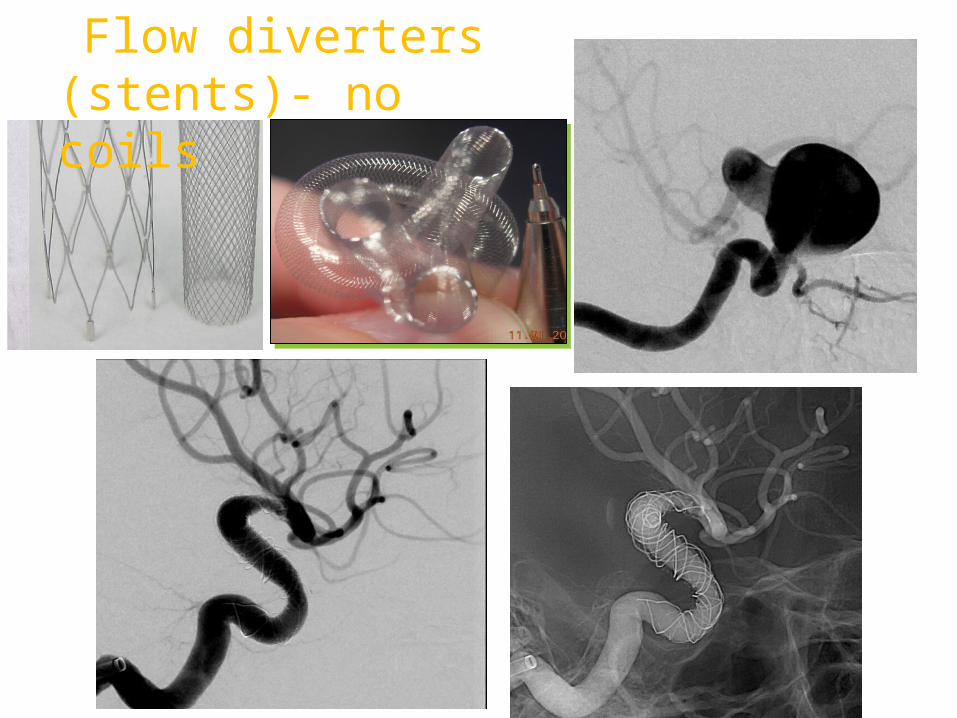
Flow diverters (stents)- no coils
50Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
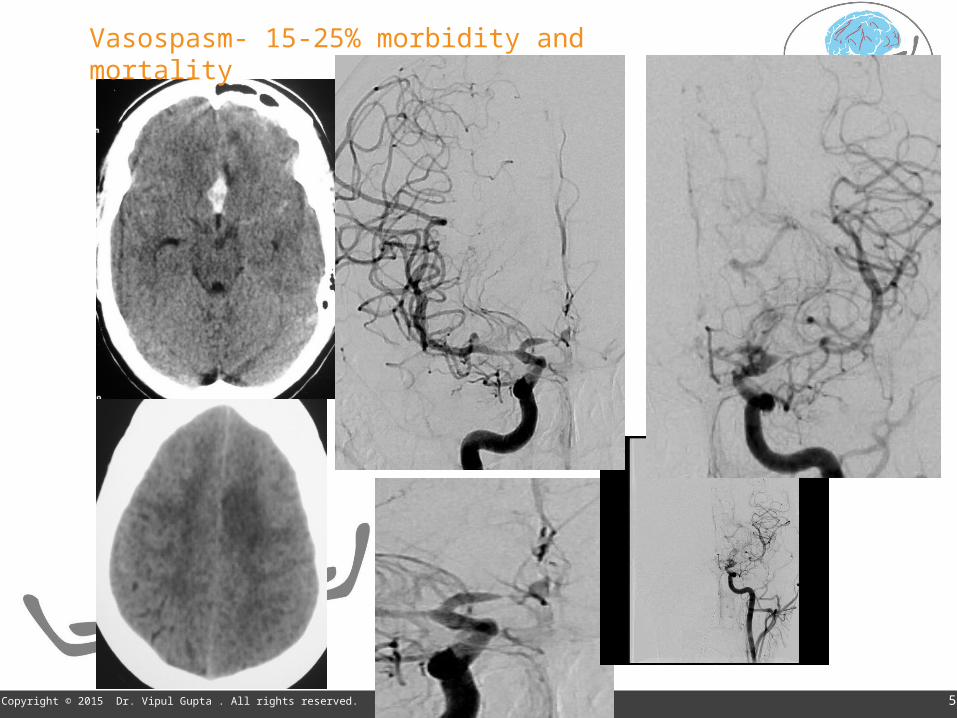
Vasospasm- 15-25% morbidity and mortality
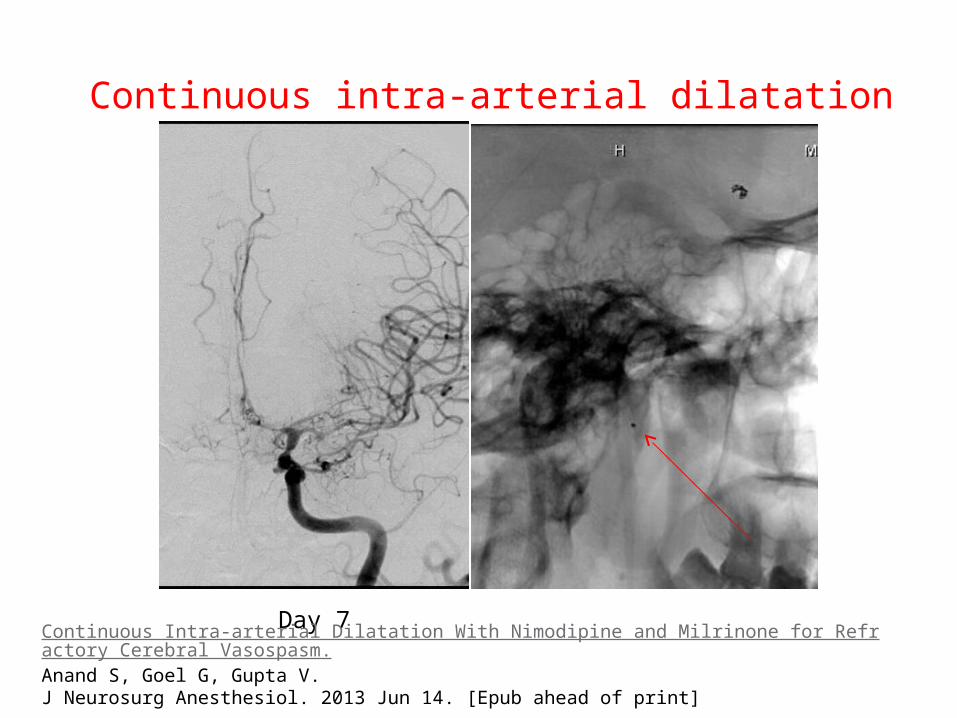
Day 7
Continuous intra-arterial dilatation
Continuous Intra-arterial Dilatation With Nimodipine and Milrinone for Refractory Cerebral Vasospasm.Anand S, Goel G, Gupta V.J Neurosurg Anesthesiol. 2013 Jun 14. [Epub ahead of print]
54Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Our protocol Interventionist part of
neurosurgery team DSA & if possible embolization Neuro lab with 3D, CT NS ICU monitoring (TCD/CTP). Vasospasm- IAVD N- 706 (Sept 2014) Data of consecutive patients

55Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Our protocol Interventionist part of
neurosurgery team DSA & if possible embolization Neuro labwith 3D, CT NS ICU monitoring (TCD/CTP). Vasospasm- IAVD N- 540 (Jan 2014)
EmbolizationSurgery
91%
9%
Good outcomeFNDMortality
Mgt. outcome in good grade patients- 90 % mRS 0-2
56Copyright © 2015 Dr. Vipul Gupta . All rights reserved. 56
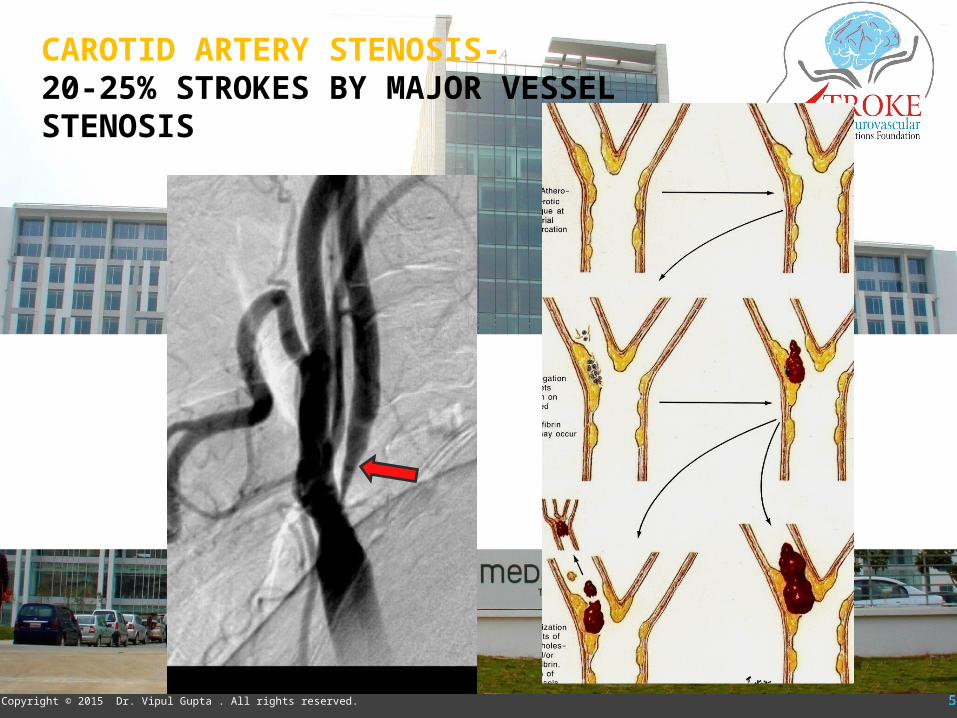
CAROTID ARTERY STENOSIS- 20-25% STROKES BY MAJOR VESSEL STENOSIS

Symptomatic Stenosis Symptomatic Stenosis • Non-invasive >70% Non-invasive >70% • Catheter angiography >50% Catheter angiography >50% • Peri-procedural risk <6%Peri-procedural risk <6%
Asymptomatic Stenosis Asymptomatic Stenosis • >70% Stenosis>70% Stenosis• Periprocedural complication risk is low Periprocedural complication risk is low • Life expectancy >5 yrLife expectancy >5 yr• >80% stenosis- tend to be treated>80% stenosis- tend to be treated
Revascularization indications-Revascularization indications- ASA/AHA guidelines 2011ASA/AHA guidelines 2011
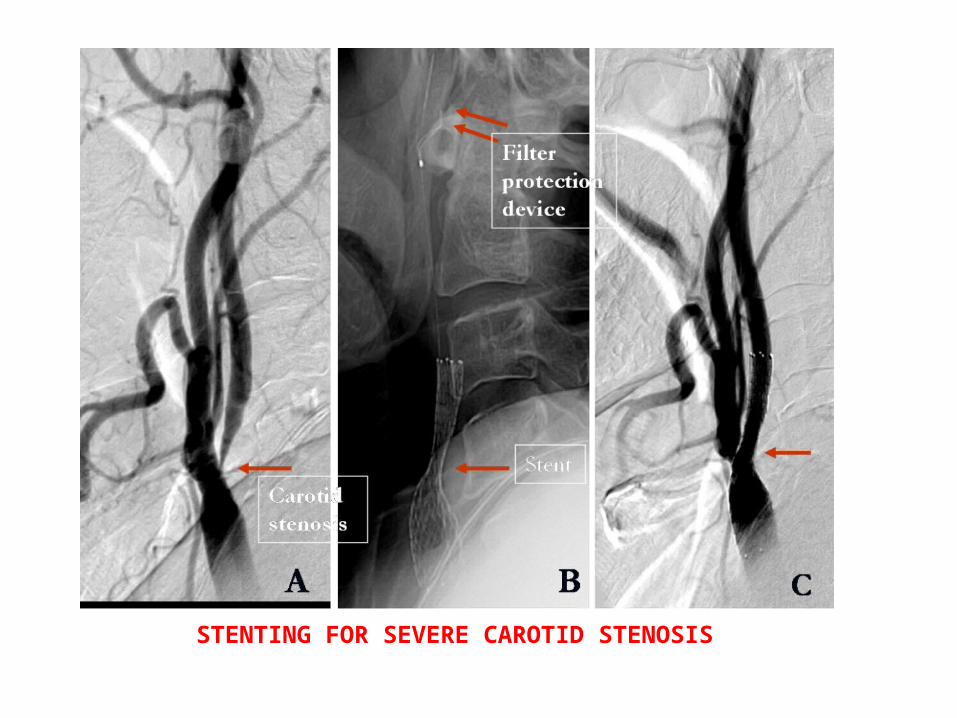
STENTING FOR SEVERE CAROTID STENOSIS
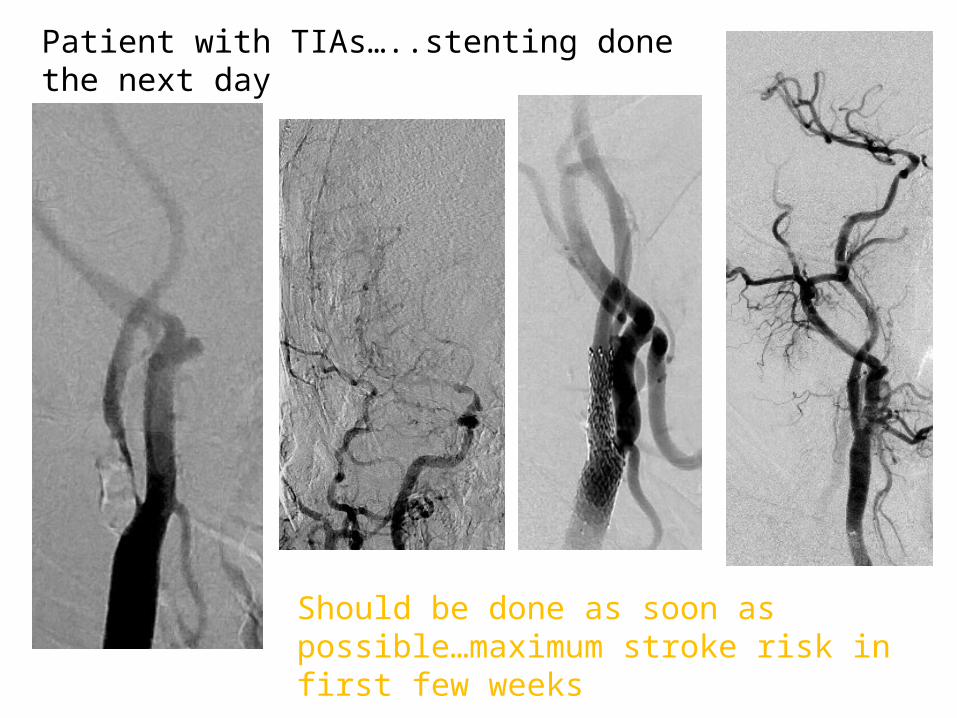
Patient with TIAs…..stenting done the next day
Should be done as soon as possible…maximum stroke risk in first few weeks

61Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
CAS vs CEA- CREST – NEJM 2011
•2502 patients- Outcome largely same•More MI in surgery ; more minor strokes in CAS•Stenting better in 70yrs and less age group •Nerve palsies not included in end-points•Less than 1% major stroke
ASA/AHA guidelines 2014- Endarterectomy and stenting are alternatives (Class I evidence)<70 yrs, stenting may be preferable

62Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
• Microemboli• Plaque morphology• Vasomotor reactivity• Silent infarcts • Progression
63Copyright © 2015 Dr. Vipul Gupta . All rights reserved. 63
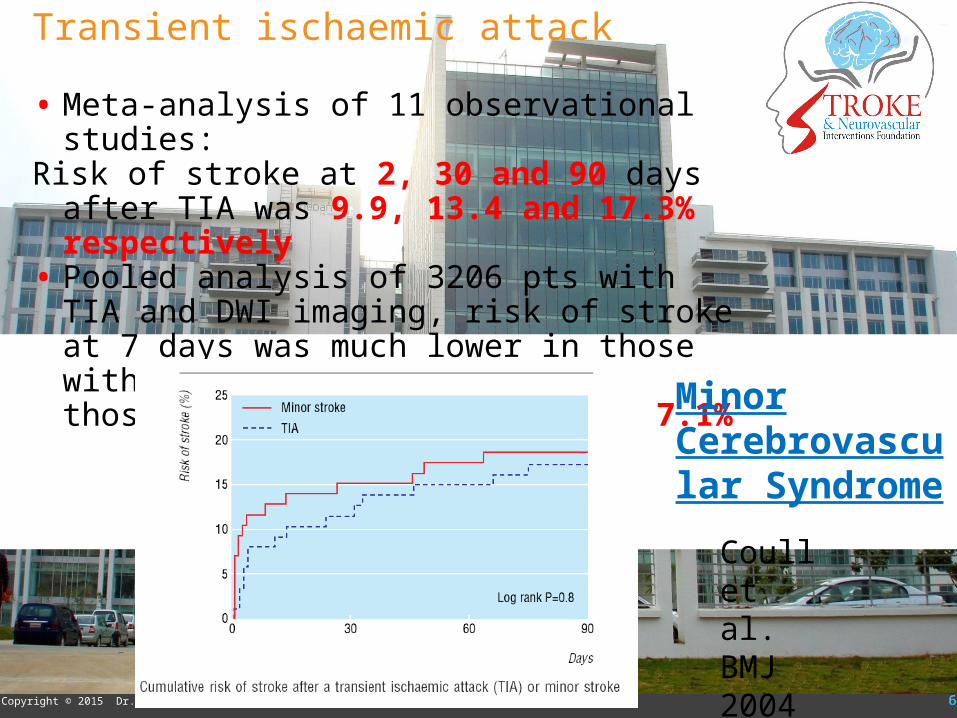
Transient ischaemic attack
• Meta-analysis of 11 observational studies: Risk of stroke at 2, 30 and 90 days after TIA was 9.9,
13.4 and 17.3% respectively• Pooled analysis of 3206 pts with TIA and DWI
imaging, risk of stroke at 7 days was much lower in those without infarction compared to those with infarction: 0.4% vs 7.1%
Coull et al. BMJ 2004
Minor Cerebrovascular Syndrome
64Copyright © 2015 Dr. Vipul Gupta . All rights reserved. 64
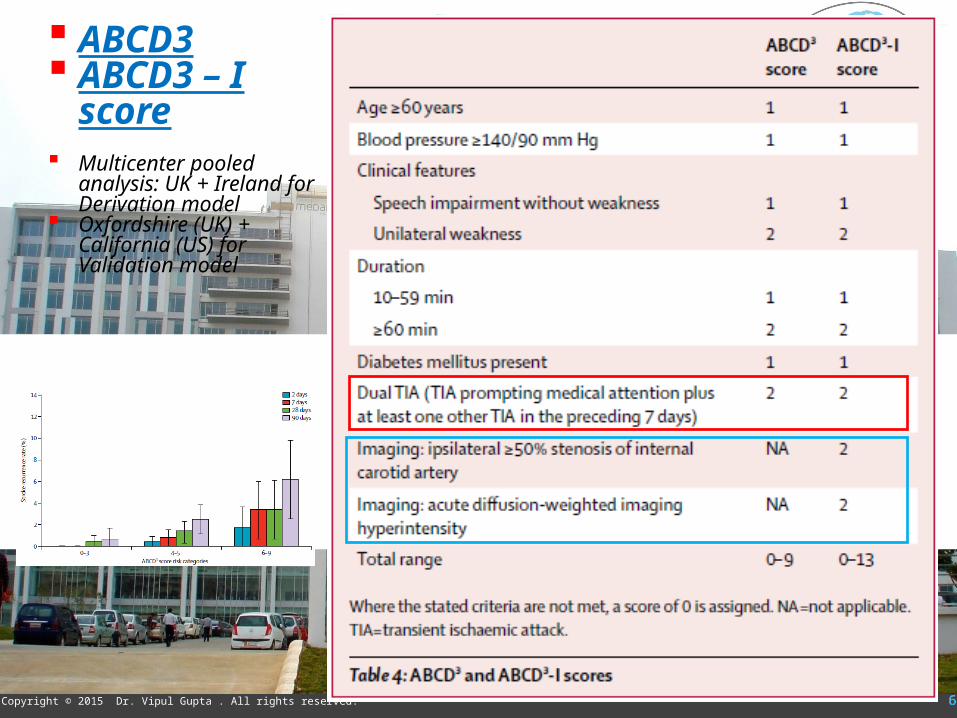
ABCD3 ABCD3 – I score Multicenter pooled analysis:
UK + Ireland for Derivation model
Oxfordshire (UK) + California (US) for Validation model
65Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
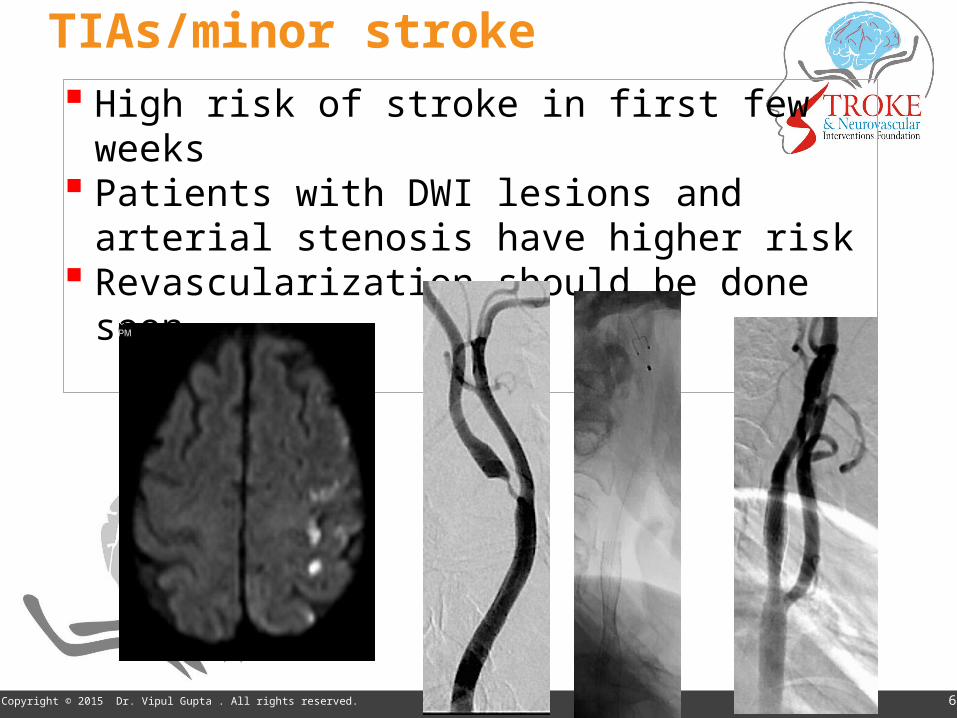
TIAs/minor stroke High risk of stroke in first few weeks Patients with DWI lesions and arterial stenosis have
higher risk Revascularization should be done soon
66Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
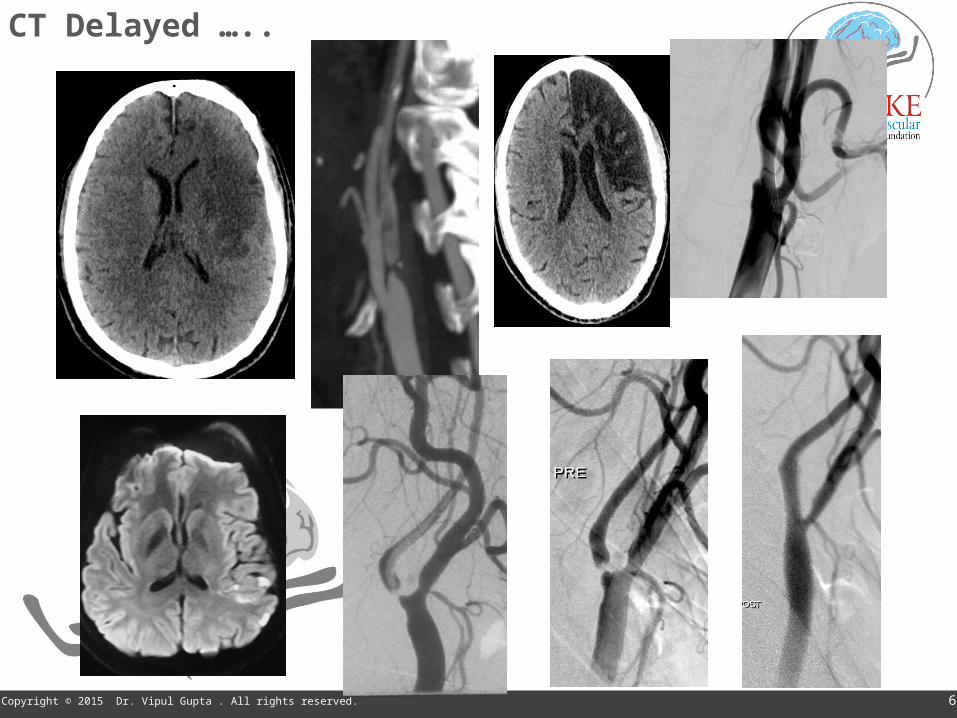
CT Delayed …..

Intracranial atherosclerosis Intracranial arterial stenosis is responsible for 6%
to 10% of ischemic strokes in whites and 22% to 26% of ischemic strokes in Asians
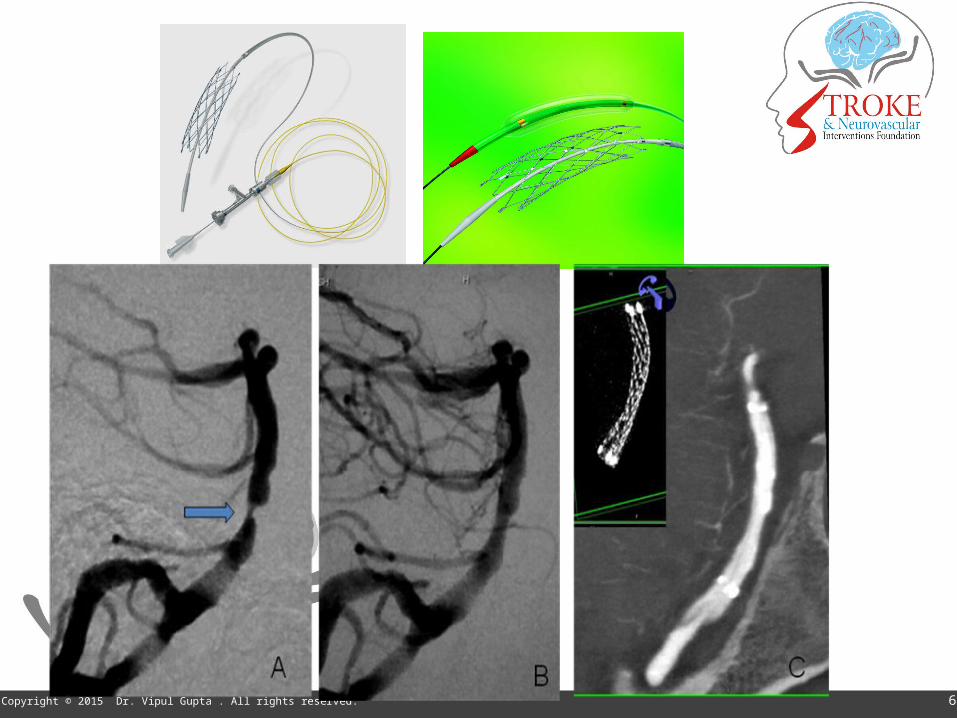
SAMPRIS Trial- stenting not to be done as routine in acute stroke
•Recurrent symptom•Subocclusive stenosis
68Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
69Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
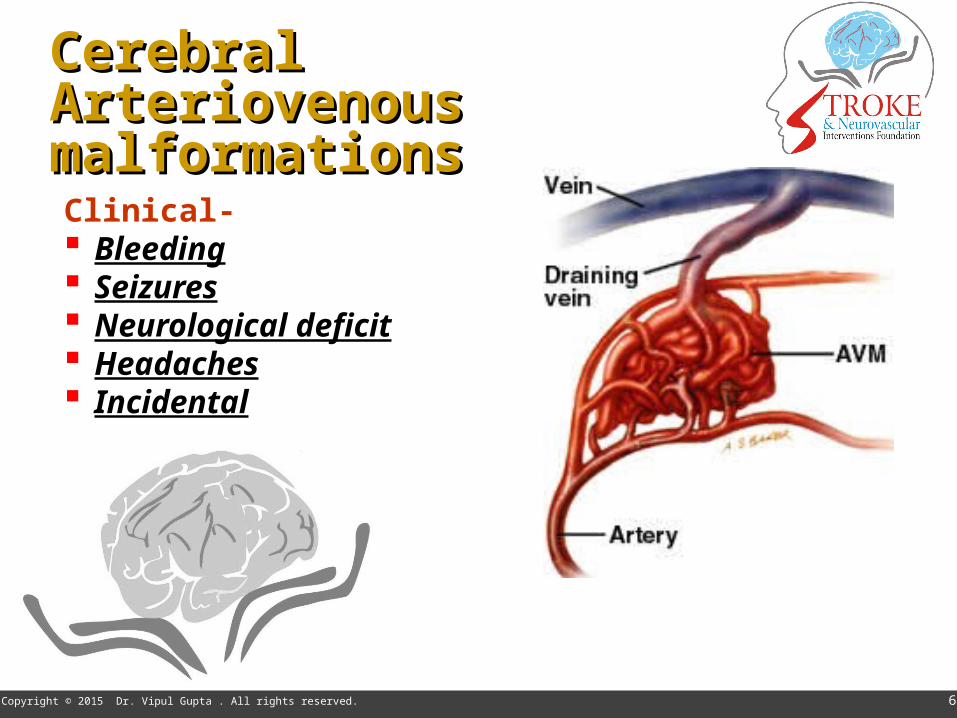
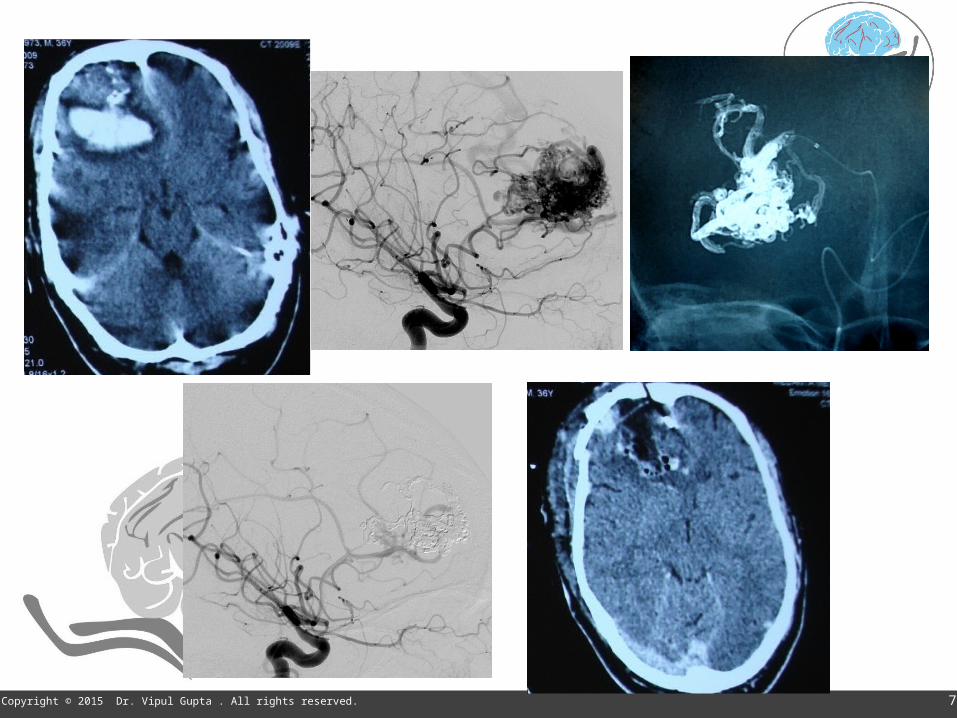
Clinical- Bleeding Seizures Neurological deficit Headaches Incidental
Cerebral Cerebral Arteriovenous Arteriovenous malformationsmalformations

70Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
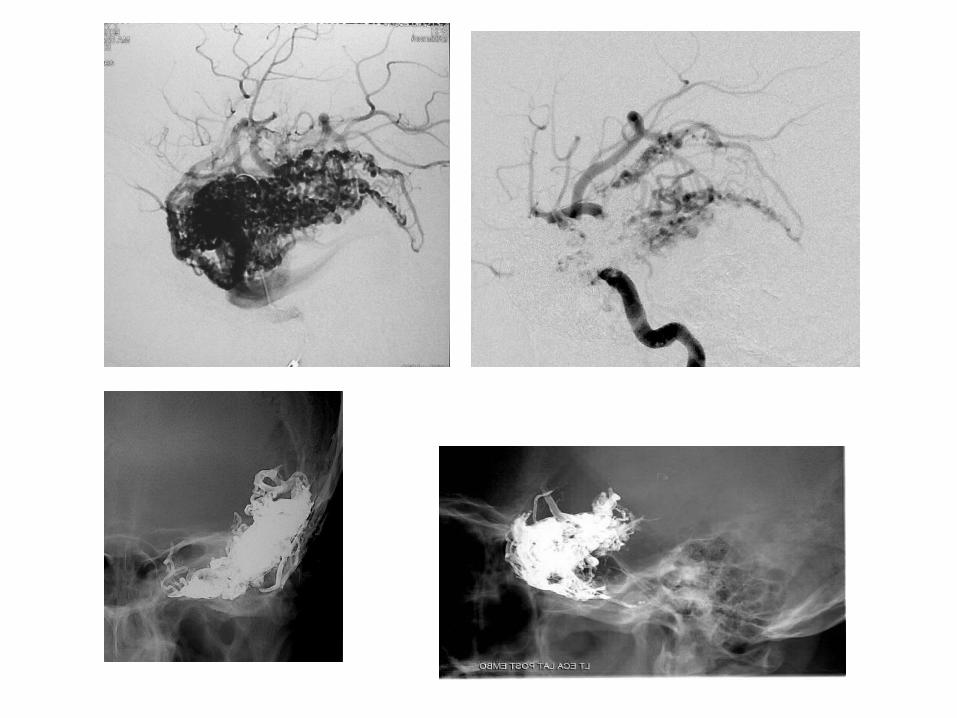
AVM- treatment options
Embolization Radiosurgery (Gamma Knife, LINAC, Cyberknife) Surgery
Embolization Glue (NBCA) vs Onyx embolization
71Copyright © 2015 Dr. Vipul Gupta . All rights reserved.




77Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Conclusion
Advances in Neuroimaging and neurointervention
Critical role in mgt of SAH-aneurysm, Acute stroke, TIA- carotid stenosis, ICH-AVMs
Latest trials have proven the role in acute stroke
Neurointerventionist, neurologist, neurosurgeon and radiologist as a team
78Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Exciting time in neurosciences …
Interventional treatment methods for diseases like epilepsy, parkinsonism, headaches …..
Image guidance in neurosurgery Radiosurgery – Gamma Knife , Cyberknife Minimally invasive spine and brainsurgery Rapid evolution in approach Multidisciplinary , team approach

79Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
For more information on:STROKE & NEUROVASCULAR INTERVENTIONS:
URL:www.sanif.co.in
Facebook:https://www.facebook.com/strokeawarenessindiahttps://www.facebook.com/vipul.gupta.35175
Twitterhttps://twitter.com/drvipulgupta25
LinkedINhttps://in.linkedin.com/pub/dr-vipul-gupta/51/8a1/25a
YouTubeChannel: Stroke & Neurovascular Interventionswww.youtube.com/c/StrokeNeurovascularInterventionsfoundation
Dr Vipul Gupta
80Copyright © 2015 Dr. Vipul Gupta . All rights reserved.
Thank You