intermountain-led cms hospital engagement network falls prevention july 11, 2014 affinity call
DESCRIPTION
Intermountain-led CMS Hospital Engagement Network Falls Prevention July 11, 2014 Affinity Call. Marlyn Conti –Patient Safety Initiatives Manager Intermountain Quality and Patient Safety. Outline for Discussion. Review of data through Q1 2014 - PowerPoint PPT PresentationTRANSCRIPT
Intermountain-led CMS Hospital Engagement Network
Falls PreventionJuly 11, 2014 Affinity Call
Marlyn Conti –Patient Safety Initiatives Manager Intermountain Quality and Patient Safety
Outline for Discussion
• Review of data through Q1 2014• ‘High performers’ – Identify and ask what
they are doing?• Falls recommended metrics• “Just-one-thing” – updated document• 2014 plans for improvement:– Reach out to low performers to provide assistance– Continue Webinars for sharing
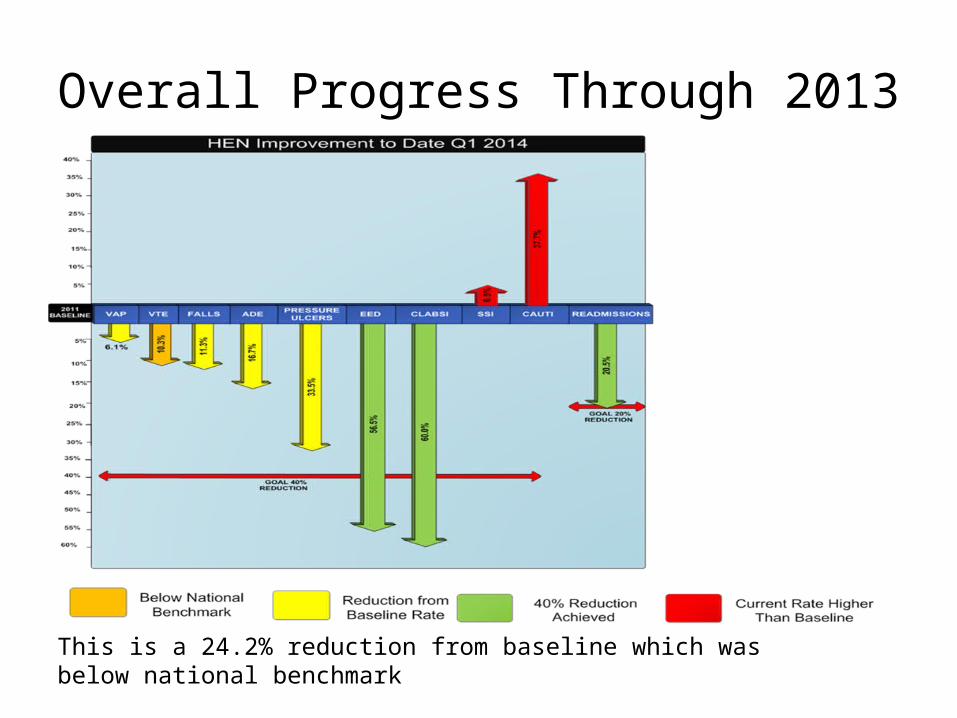
Overall Progress Through 2013
This is a 24.2% reduction from baseline which was below national benchmark
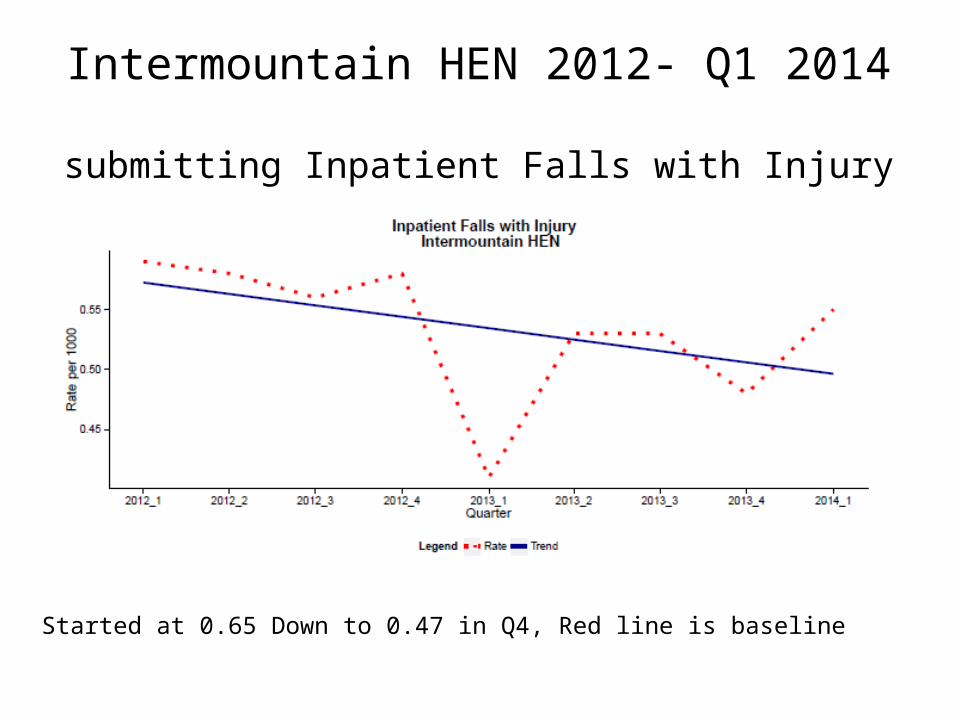
Intermountain HEN 2012- Q1 2014 submitting Inpatient Falls with Injury
Started at 0.65 Down to 0.47 in Q4, Red line is baseline
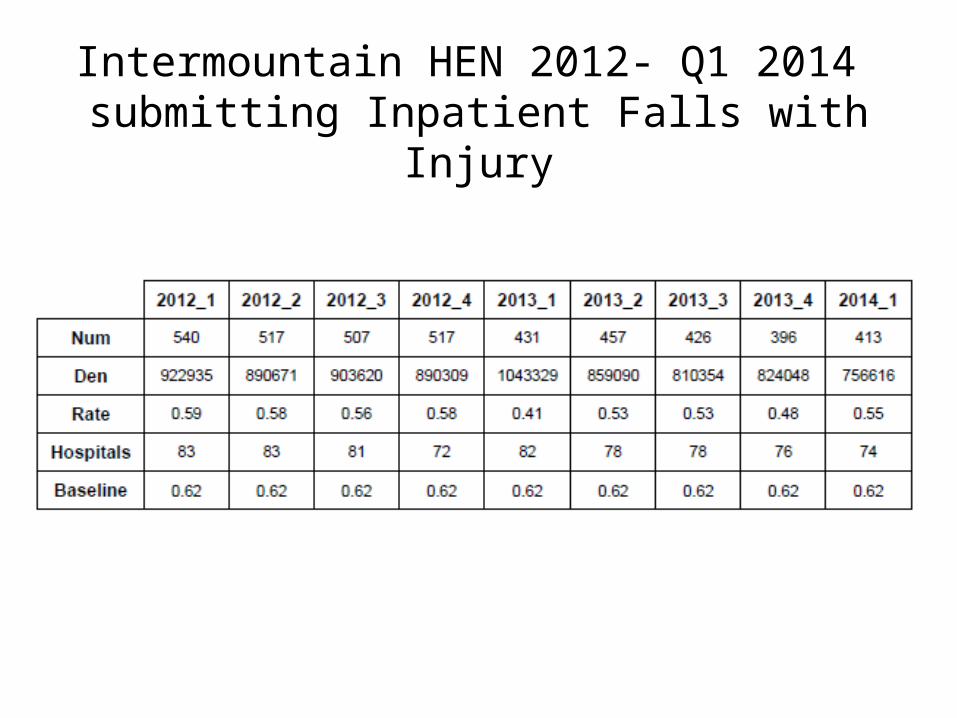
Intermountain HEN 2012- Q1 2014 submitting Inpatient Falls with Injury
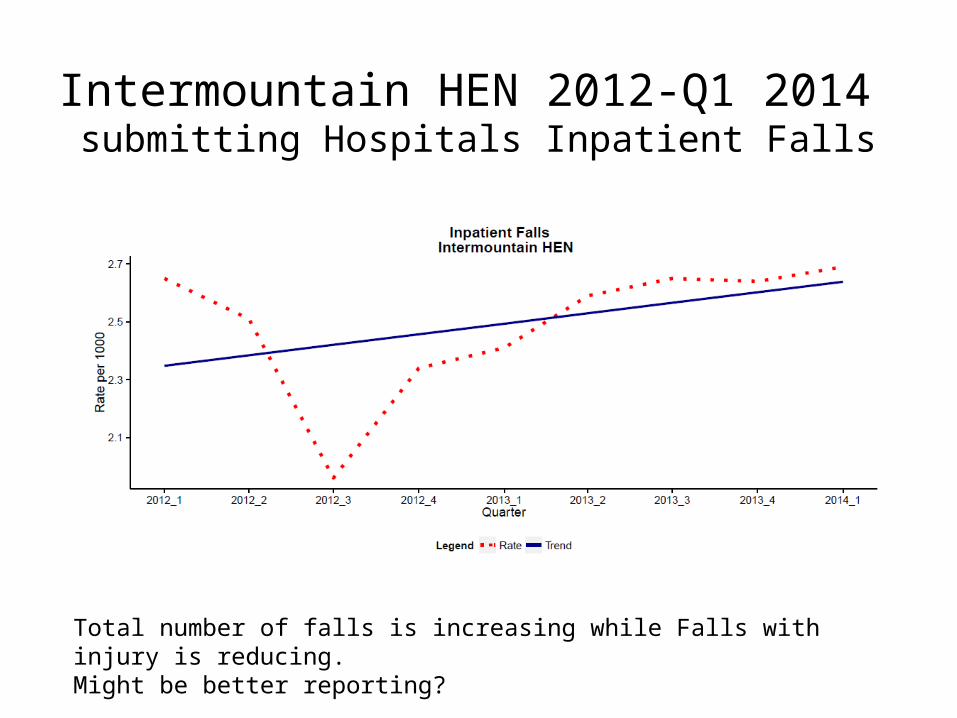
Intermountain HEN 2012-Q1 2014 submitting Hospitals Inpatient Falls
Total number of falls is increasing while Falls with injury is reducing. Might be better reporting?
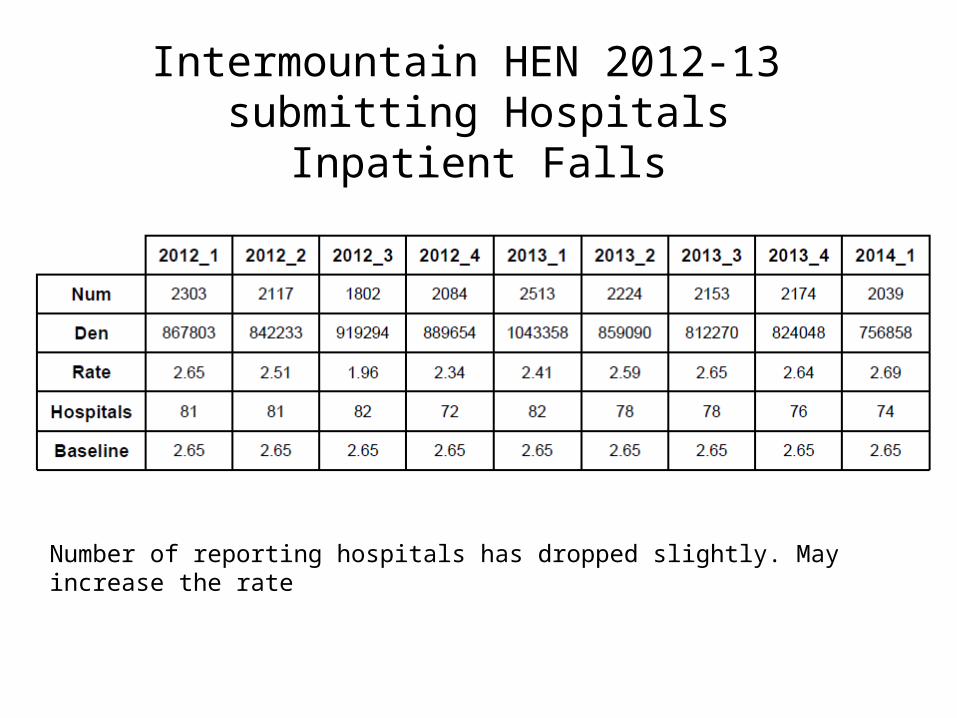
Intermountain HEN 2012-13 submitting Hospitals
Inpatient Falls
Number of reporting hospitals has dropped slightly. May increase the rate
HEN Falls Measures
• Metric specification resource manual http://www.henlearner.org/wp-content/uploads/2012/03/HEN_measure_Feb5.pdf
• Submission schedule: – May 20, 2014: for data through March 2014
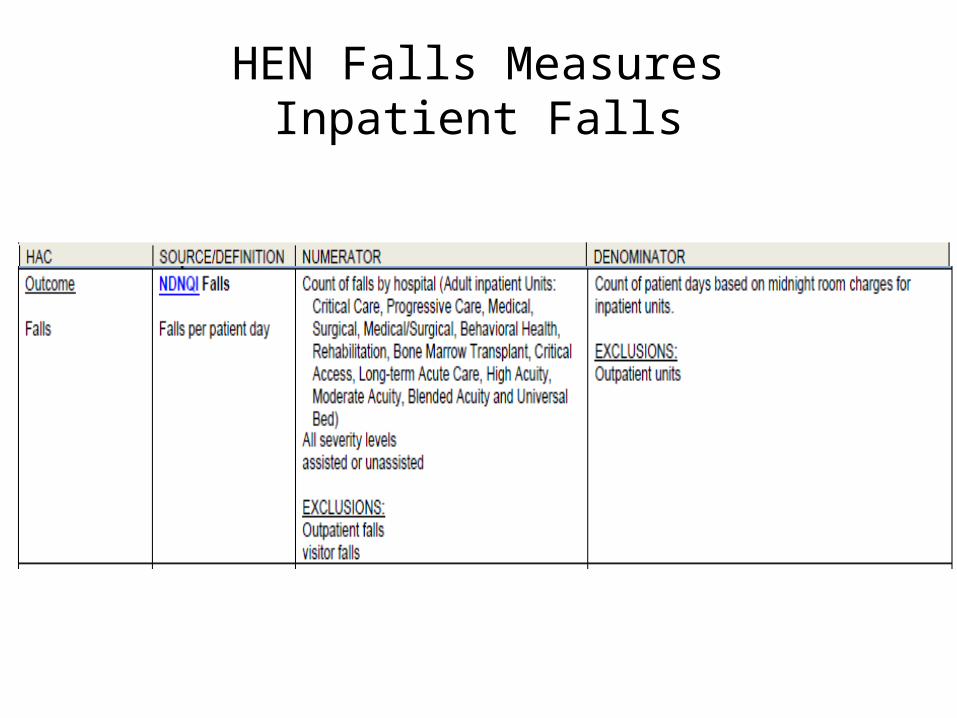
HEN Falls MeasuresInpatient Falls
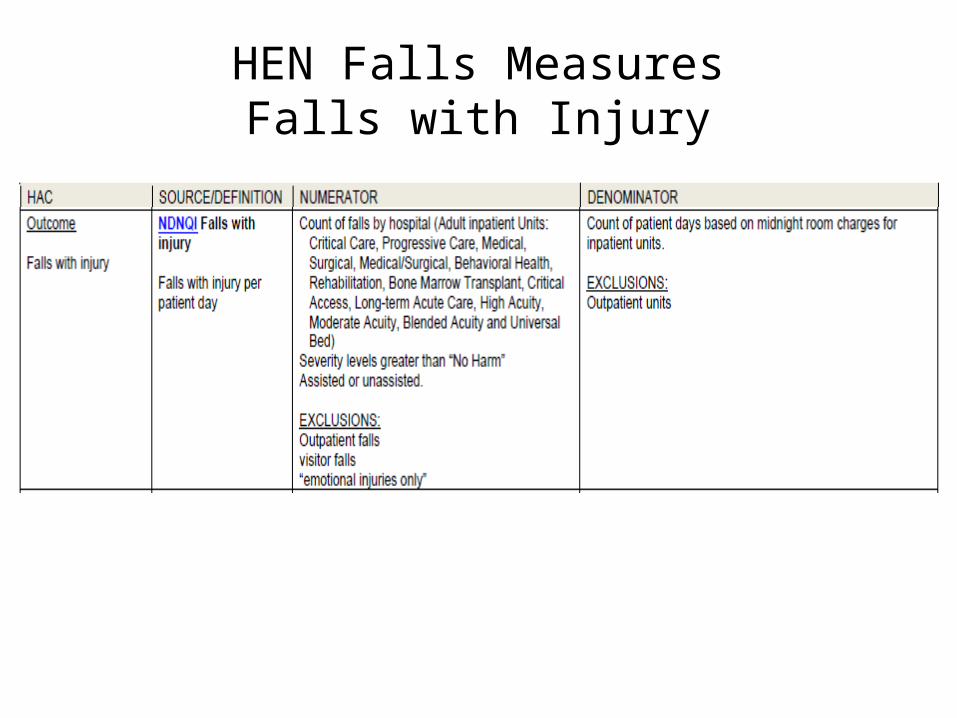
HEN Falls MeasuresFalls with Injury
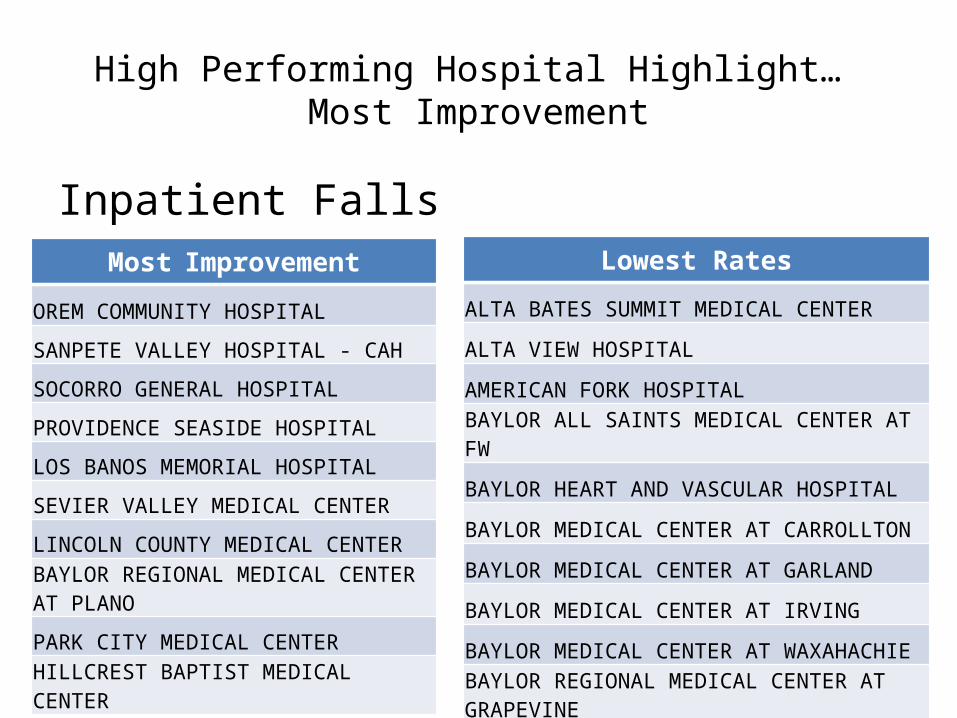
High Performing Hospital Highlight… Most Improvement
Inpatient FallsMost Improvement
OREM COMMUNITY HOSPITAL
SANPETE VALLEY HOSPITAL - CAH
SOCORRO GENERAL HOSPITAL
PROVIDENCE SEASIDE HOSPITAL
LOS BANOS MEMORIAL HOSPITAL
SEVIER VALLEY MEDICAL CENTER
LINCOLN COUNTY MEDICAL CENTERBAYLOR REGIONAL MEDICAL CENTER AT PLANO
PARK CITY MEDICAL CENTER
HILLCREST BAPTIST MEDICAL CENTER
Lowest Rates
ALTA BATES SUMMIT MEDICAL CENTER
ALTA VIEW HOSPITAL
AMERICAN FORK HOSPITAL
BAYLOR ALL SAINTS MEDICAL CENTER AT FW
BAYLOR HEART AND VASCULAR HOSPITAL
BAYLOR MEDICAL CENTER AT CARROLLTON
BAYLOR MEDICAL CENTER AT GARLAND
BAYLOR MEDICAL CENTER AT IRVING
BAYLOR MEDICAL CENTER AT WAXAHACHIE
BAYLOR REGIONAL MEDICAL CENTER AT GRAPEVINE
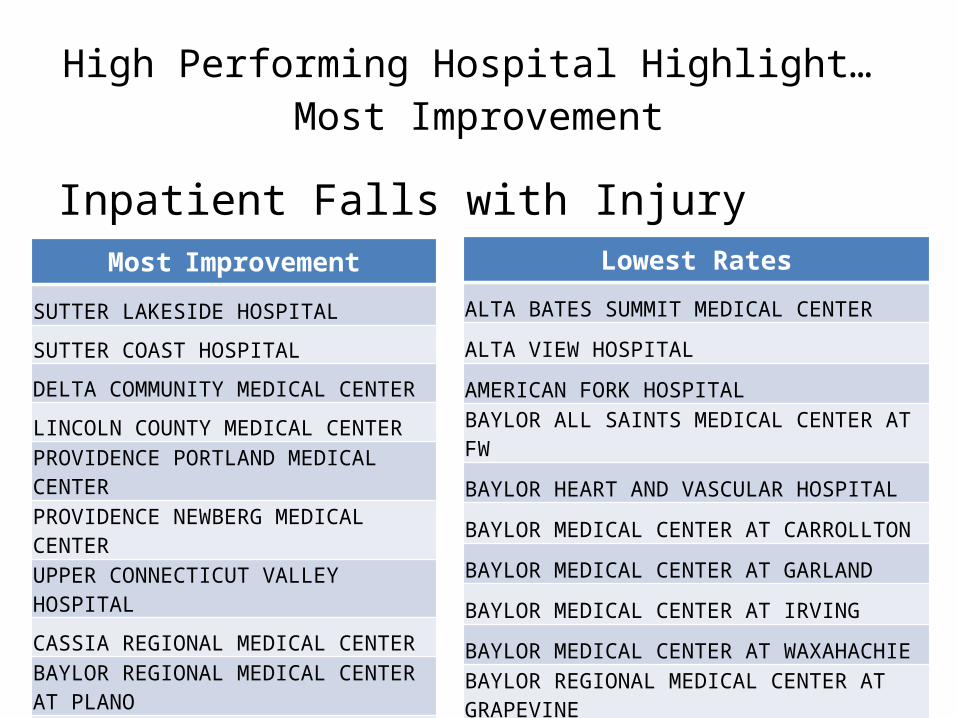
High Performing Hospital Highlight… Most Improvement
Inpatient Falls with InjuryMost Improvement
SUTTER LAKESIDE HOSPITAL
SUTTER COAST HOSPITAL
DELTA COMMUNITY MEDICAL CENTER
LINCOLN COUNTY MEDICAL CENTER
PROVIDENCE PORTLAND MEDICAL CENTER
PROVIDENCE NEWBERG MEDICAL CENTER
UPPER CONNECTICUT VALLEY HOSPITAL
CASSIA REGIONAL MEDICAL CENTERBAYLOR REGIONAL MEDICAL CENTER AT PLANO
PARK CITY MEDICAL CENTER
Lowest Rates
ALTA BATES SUMMIT MEDICAL CENTER
ALTA VIEW HOSPITAL
AMERICAN FORK HOSPITAL
BAYLOR ALL SAINTS MEDICAL CENTER AT FW
BAYLOR HEART AND VASCULAR HOSPITAL
BAYLOR MEDICAL CENTER AT CARROLLTON
BAYLOR MEDICAL CENTER AT GARLAND
BAYLOR MEDICAL CENTER AT IRVING
BAYLOR MEDICAL CENTER AT WAXAHACHIE
BAYLOR REGIONAL MEDICAL CENTER AT GRAPEVINE
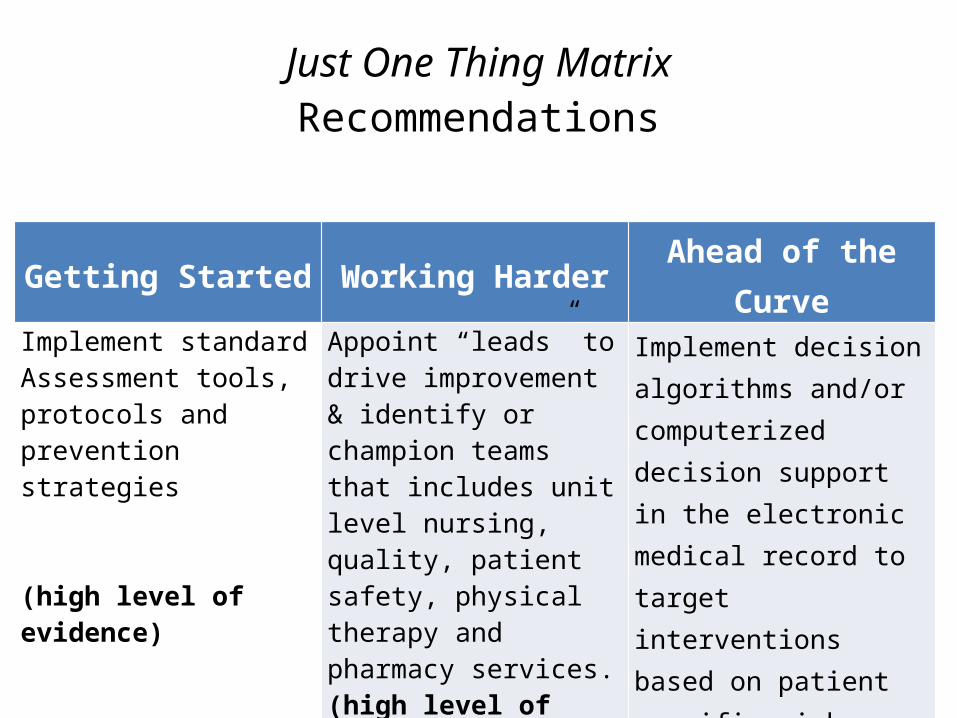
Just One Thing MatrixRecommendations
Getting Started Working Harder Ahead of the Curve
Implement standard Assessment tools, protocols and prevention strategies
(high level of evidence)
Appoint “leads” to drive improvement & identify or champion teams that includes unit level nursing, quality, patient safety, physical therapy and pharmacy services. (high level of evidence)
Implement decision algorithms and/or computerized decision support in the electronic medical record to target interventions based on patient specific risk factors
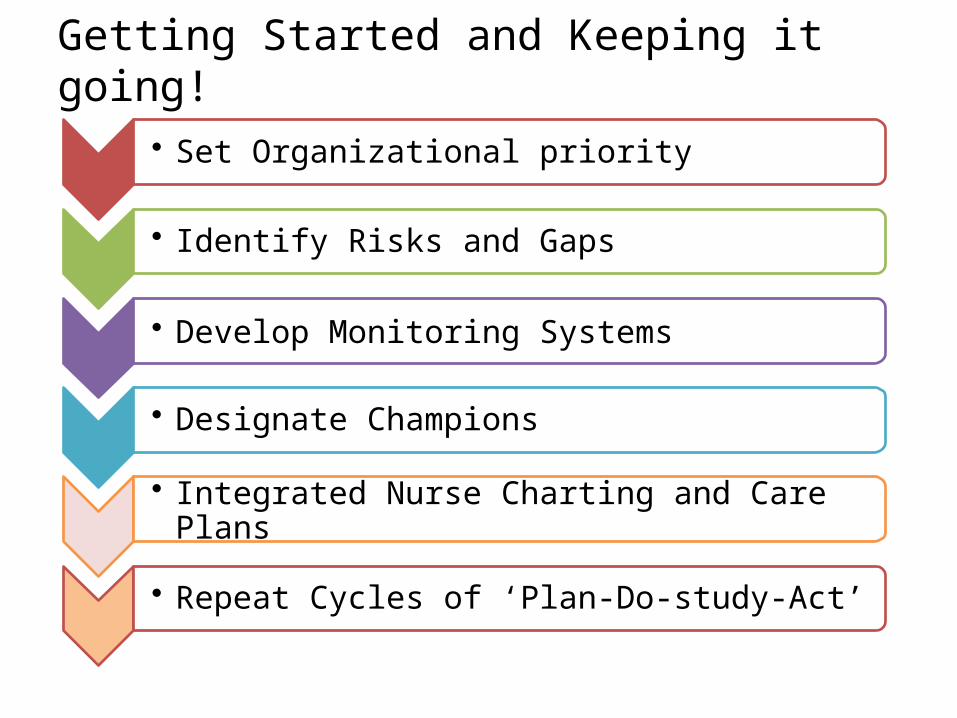
• Set Organizational priority
• Identify Risks and Gaps
• Develop Monitoring Systems
• Designate Champions
• Integrated Nurse Charting and Care Plans
• Repeat Cycles of ‘Plan-Do-study-Act’
Getting Started and Keeping it going!
Fall Event #1Case 1: 9:13:48 AM• Pt noted during rounding sleeping soundly @ 0200, was not woken up. Pt found on
floor by CNA @ 0240. • Pt reports going to the bathroom on her own, took herself off the CPM, SCD, and
went to the bathroom without a walker, stated "I really needed to go to the bathroom, that's why I didn't call," fell backwards and hit her head on the side of the counter. Pt alert and orient before and after fall.
• Pt noted previously using the call light for help, and agreed at the beginning of the shift to call when help is needed, but decided to be noncompliant this time. VS done. No abnormality.
Post fall: • Only noted injury is hematoma to left forehead. Dr. MJ notified, no new orders
given except to monitor patient during the night. Pt re-educated about fall risks, bed alarm activated, sign on door, and monitored frequently. Post fall: Pt re-educated about fall risks, bed alarm activated, sign on door, and monitored frequently.
Fall Event #2Case 2: 12:43:55PM • Aide was sitting at desk documenting end of shift vital signs when patient's
bed alarm went off. Aide stood up look through the doorway and saw patient on knees next to the side of the bed. Bed alarm and side rails were in place at the time of the fall. When asked patient reported he wanted to roll onto his side. Lift was used to return patient to the bed, vital signs obtained RN notified, RN assessed patient, palpated joints. Patient reports pain on palpation of patella and anterior aspect of knees and shins bilaterally.
Post Fall: • MD notified, Family Notified. Could have possibly been prevented if patient
had a sitter in the room. Nursing and CNA staff had repeatedly reinforced to Patient, the hospital safety protocols for ambulation and transfer require staff assistance.
Fall Event #3
Case 3:• You have identified 10 patients on your unit with a high risk for
falls, what intervention do you implement?
• Based on your experience, which interventions are the most effective?
• How would you document the assessment and intervention(s) for
the patient in your EHR?
• What type(s) of performance feedback would be available at the unit level?
Fall Event #4• You are a nurse manager on a 40 bed MedSurg unit with a hospital
mandate to reduce falls with limited resources.
• Issue: Identify patients at risk for falls.
• How would you identify the patients? How would you stratify the individual patient’s risk? Who would screen the patient? What key factors contributed to the decision?
• How would you document the assessment and intervention(s) for the patient in your EHR?
• What type(s) of performance feedback would be available at the unit level?
Fall Event 5
• Budget cuts have forced reduction in the number of patient care techs (PCT) and nursing staff. What tactics would you use to minimize fall risk?
• How would you maintain what you have implemented?
Fall Prevention Best Practice
• Use our HEN bundle to assess practice?
• Or use the Veterans Integrated Service Network 8 (VISN 8) Road Map?
• http://www.mnhospitals.org/Portals/0/Documents/ptsafety/falls/falls-prevention-roadmap.pdf
2014 plans for improvement
• Reach out to low performers to provide assistance.• Held regional workshop in Plano Texas• Shared case studies
• Collect and share best practices across network hospitals • Review/revise 2013 proposed prevention bundle • Conduct participant practice survey
• Next webinar plans? • Questions• Issues• barriers