insulin initiation optimising glycaemic control and weight dr c rajeswaran consultant physician...
Post on 19-Dec-2015
225 views
TRANSCRIPT

Insulin initiation
OPTIMISING
Glycaemic control and Weight
Dr C RajeswaranConsultant Physician
Diabetes & EndocrinologyMid Yorkshire NHS Trust

UKPDS: A 1% decrease in HbA1c is associated with a reduction in complications
Stratton IM et al. BMJ 2000; 321: 405–412.
12% Stroke*** p<0.0001
** p=0.035
1%
HbA1c
Microvascular complications e.g. kidney disease and blindness *
37%
Amputation or fatal peripheral blood vessel disease*
43%
Deaths related to diabetes*21%
Heart attack*14%

Glycaemic control and body weight
Weight gain appears unavoidable when patients with Type 2 diabetes are commenced on insulin
Calculations of average weight gain are that for every 5 mmol/l reduction in fasting glucose, or a 2.5% fall in HbA1c, approximate weight gain is 5 kg (Makimattila et al, 1999)
Body weight increases by 2Kg for each percentage point decrease in HbA1C during the first year1
1.Makimattila et al Diabetologia 1999;42;406-412

Glycosuria is known to occur once fasting glucose levels reach around 10-12 mmol/l,
and if treatment with insulin is delayed until this time, weight gain is likely to occur.
Gain in weight mainly represents an increase in fat mass, which enhances insulin resistance and increases the risk of obesity related complications.
Makimattila S, Nikkila K. Yki-Jarvinen H (1999) Causes of weight gain during insulin therapy with and without metformin in patients with type II diabetes mellitus. Diabetologia 42: 406-12
Insulin in Type 2 Diabetes is aimed at
inhibition of hepatic glucose output
And
improvement of peripheral glucose utilisation
Causes of weight gain with treatment ?
Insulin and weight• Reduced glycosuria
• Anabolic action of insulin
• Fluid retention
• Hypoglycaemia and increased calorie consumption
• Excess insulin administration
• Combination of obesity and muscle impairment: 'sarcopenic obesity'.

Metabolic Consequences of Weight Gain
Patients with T2 DM often have many other comorbid conditions increasing their risk for macrovascular events.
Weight gain may have further deleterious metabolic consequences, such as worsening hypertension, lowering HDL-C, and raising LDL-C.[1,2]
Blood pressure control and lipid control have both been shown to reduce cardiovascular events in patients with type 2 DM.
1.Yki-Jarvinen H, Ryysy L, Kauppila M, et al. Effect of obesity on the response to insulin therapy in noninsulin-dependent diabetes mellitus. J Clin Endocrinol Metab. 1997;82:4037-4043. 2.United Kingdom Prospective Diabetes Study Group. Tight blood pressure control and risk of macrovascular and microvascular complications in type 2 diabetes: UKPDS 38. BMJ. 1998;317:703-713.

Adjusted odds ratio for death, by metabolic category for 51-61years age group
Diabetes 2.63
Obesity 0.78
Obesity and diabetes 6.81
Oldridge et al, Jr of clinical Epidemiology 54(2001);928-934

Insulin secretion
Adapted from Riddle et al. Diabetes Care. 1990;13:676-686.
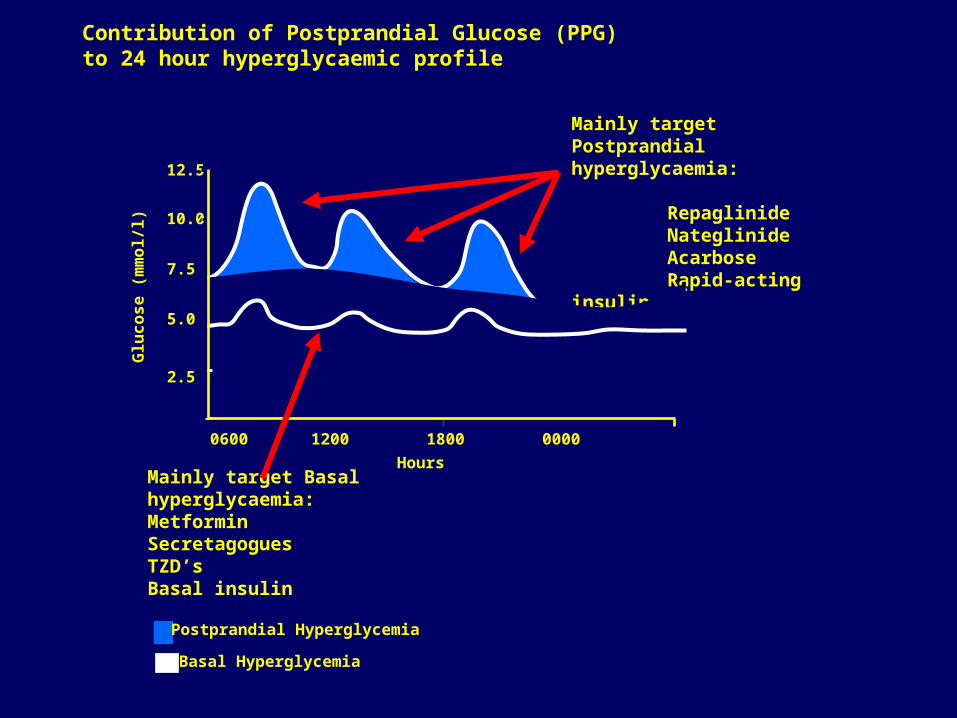
Contribution of Postprandial Glucose (PPG) to 24 hour hyperglycaemic profile
Mainly target Basal hyperglycaemia:MetforminSecretagogues TZD’sBasal insulin
Mainly target Postprandial hyperglycaemia:
RepaglinideNateglinide AcarboseRapid-acting insulin
Glu
co
se
(m
mo
l/l) 10.0
5.0
00600 1200
Hours
1800 0000 0600
7.5
12.5
2.5
Basal Hyperglycemia
Postprandial Hyperglycemia

As patients get closer to HbA1c target, the need to manage PPG increases
Monnier L, et al. Diabetes Care. 2003;26:881-885.
30%40% 45% 50%
70%60% 55% 50%
70%
30%
>10.2 10.2-9.3 9.2-8.5 8.4-7.3 <7.3
% C
on
trib
uti
on
to
Hb
A1c
HbA1c Range (%)
0
20
40
60
80
100
Fasting Plasma Glucose (FPG)
Post Prandial Glucose (PPG)

How Do We Minimize Weight Gain Associated With Insulin Therapy?
Patients who are started on insulin treatment may take away mixed messages about dietary control and think that they can increase their calorie intake on insulin; this results in excessive weight gain.
Lifestyle intervention should be reinforced with initiation of insulin therapy.
Medical Nutrition therapy

Metformin and insulin
Metformin appears to have an insulin-sparing effect and reduces weight gain with insulin treatment.
Studies using a combination of 2g metformin with bedtime isophane insulin, as opposed to twice-daily isophane insulin, showed that the insulin requirements in the metformin group were reduced by 47% and there was 45% less weight gain (Makimattila et al, 1999).
This reduction in weight gain seemed to be due to reduced energy intake in those on metformin.
Patients with T2DM should remain on metformin when they convert to treatment with insulin.

Repaglinide with insulin
In a RCT, use of repaglinide resulted in a reduction in HbA1c compared to twice daily insulin group (1.8% versus 1% drop)
and weight gain (2.2 kg versus 2.9 kg),
but less insulin was required in the repaglinide group (Davies et al, 2002).
Repaglinide in combination with bedtime insulin and metformin produces a significantly greater fall in HbA1c compared with the twice-daily insulin or night time insulin and metformin.
Davies MJ, Howe J, Jarvis J at al (2002) Use of the combination of insulin and the prandial glucose regulator repaglinide in patients with type 2 diabetes mellitus. Diabetic Medicine 19(2): 25

One injection
Intermediate-acting insulin or long-acting analog at bedtimePremixed formulation before dinner
Two injections
Breakfast and dinner: premixed formulationBreakfast and dinner: short-acting or rapid-acting plus NPH or long-acting insulin analog
Three injections
Add a short- or rapid-acting insulin injection at lunchtime to a 2-injection premixed regimenAdd a third premix injection at lunchtime to a 2-injection premixed regimenMove the intermediate- or long-acting insulin analog to bedtime with short-acting or rapid-acting insulin analog at breakfast and dinner
Multiple injections
Short-acting or rapid-acting insulin analog at each meal with an intermediate- or long-acting at bedtime
Insulin pump
Insulin regimes: Multiple options

•If FPG is elevated, start with long-acting (basal) insulin;
•If PPG is elevated, rapid-acting (prandial or bolus) can be used; and
If FPG and PPG are elevated, any of the following would be appropriate:
•Oral agents with basal insulin
•Premixed insulin analogs
•Basal/bolus as in multiple daily injections (MDI) or an insulin pump.
Initiating Insulin: Basic RecommendationsNo set formula......