inf'ormation to users - open...
TRANSCRIPT

MALINGERING: THE USE OF A PSYCHOLOGICAL TESTBATTERY TO DETECT TWO KINDS OF SIMULATION
(FAKING, BENDER-GESTALT, DISSIMULATION, MMPI).
Item Type text; Dissertation-Reproduction (electronic)
Authors Schretlen, David John
Publisher The University of Arizona.
Rights Copyright © is held by the author. Digital access to this materialis made possible by the University Libraries, University of Arizona.Further transmission, reproduction or presentation (such aspublic display or performance) of protected items is prohibitedexcept with permission of the author.
Download date 28/06/2018 17:08:01
Link to Item http://hdl.handle.net/10150/183871

INF'ORMATION TO USERS
This reproduction was made from a cop~ d manuscript sent to us for publication and microfilming. While the most advanced technology has been used to photograph and reproduce this manuscript. the quality of the reproduction is heavily dependent upon the quality of the material submitted. Pages in any manuscript may have indistinct print. In all cases the best available copy has been filmed.
The following explanation of techniques 1s provided to help clarify notations which may appear on this reproduction.
1. Manuscripts may not always be complete. When it is not possible to obtain missing pages. a note appears to indicate this.
2. When copyrighted materials are removed from the manuscript. a note appears to indicate this.
3. Oversize materials (maps. draWings. and charts) are photographed by sectioning the original. beginning at the upper left hand comer and continuing from left to right in equal sections with small overlaps. Each oversize page is also filmed as one exposure and is available. for an additional charge. as a standard 35mm slide or in black and white paper format. *
4. Most photographs reproduce acceptably on positive microfilm or microfiche but lack clarity on xerographic copies made from the microfilm. For an additional charge. all photographs are available in black and white stan,dard 35mrn slide format. *
*For more information about black and white slides or enlarged paper reproductions. please contact the Dissertations Customer Services Department.
U-M-I Dissertation Information Service
University Microfilms International A Bell & Howell Information Company . 300 N. Zeeb Road, Ann Arbor, Michigan 48106


8623860
Schretlen, David John
MALINGERING: THE USE OF A PSYCHOLOGICAL TEST BATTERY TO DETECT TWO KINDS OF SIMULATION
The University of Arizona
University Microfilms
International 300 N. Zeeb Road, Ann Arbor, MI48106
PH.D. 1986


MALINGERING: THE USE OF A PSYCHOLOGICAL TEST BATTERY
TO DETECT TWO KINDS OF SIMULATION
by
David John Schretlen
A Dissertation Submitted to the Faculty of the
DEPARTMENT OF PSYCHOLOGY
In Partial Fulfillment of the Requirements For the Degree of
DOCTOR OF PHILOSOPHY
In the Graduate College
THE UNIVERSITY OF ARIZONA
1 986

THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE
As members of the Final Examination Committee, we certify that we have read
the dissertation prepared by ___ D~av __ i_d_J __ oh~n~_S~ch~r~e~t~le~n~ ____________________ ___
entitled Malingering: The Use of a Psychological Test Battery to
Detect Two Kinds of Simulation
and recommend that it be accepted as fulfilling the dissertation requirement
for the Degree of Ph.D. ----------------------------------------------------------
Date
Date
Date
Date
Date
Final approval and acceptance of this dissertation is contingent upon the candidate's submission of the final copy of the dissertation to the Graduate College.
I hereby certify that I have read this dissertation prepared under my direction and recommend that it be accepted as fulfilling the dissertation requirement.
r-Y-It Date
----------------------------_._----- .

STATEMENT BY AUTHOR
This dissertation has been submitted in partial fulfillment of requirements for an advanced degree at The University of Arizona and is deposited in the University Library to be made available to borrowers under rules of the Library.
Brief quotations from this dissertation are allowable without special permission, provided that accurate acknowledgement of source is made. Requests for permission for extended quotation from or reproduction of this manuscript in whole or in part may be granted by the head of the major department or the Dean of the Graduate College when in his or her judgement the proposed use of the material is in the interests of scholarship. In all other instances, however, permission must be obtained from the author.
SIGNED:
..... _ .. __ .--------------------------------------------

For Claire Marie, Whose Laughter I Shall Never Forget
-----------------------------------------------------------------------

ACKNOWLEDGEMENTS
Gaining entrance into the numerous institutional settings
required to complete this research was greatly facilitated by the
following people, to whom I am most grateful: Dr. Rodney Jilg,
Department of Economic Services, Developmental Disabilities Division;
Dr. August Johnson, Chief Psychologist, Tucson Veterans Administration
Medical Center; and especially Mr. Sam Sublett, Warden, Arizona
Correctional Training Center, Rincon Unit.
To Dr. Hal Arkowitz, whose guidance in every step of the design,
execution and analysis of this experiment made it possible, I wish to
express my appreciation. His careful examination of my thinking and
meticulous attention to each revision of the manuscript essentially
informed the final production.
Finally, I wish to acknowledge my parents and my sister for
their steady support, their joy over my small accomplishments, and their
example of continuing growth.
iv
--- --------------

TABLE OF CONTENTS
CHAPTER
I INTRODUCTION.
History.
Munchausen's Syndrome
Ganser Syndrome •
Hysteria.
Depth of Psychopathology.
Scope of the Problem.
Overview of Malingering Research •
Intelligence Tests.
Summary •
Personality Tests •
Minnesota Multiphasic Personality Inventory •
Detection Strategies and Validity •
Summary •
Bender Gestalt.
Summary •
Purpose
Development of the Malingering Scale.
Use of a Test Battery •
Enhancing External Validity •
Type of Disorder Simulated.
v
PAGE
1
3
3
4
5
6
9
12
13
19 ' .. ~ ,.
21
22
22
30
31
34
35
35
36
37
39

CHAPTER
II
III
IV
METHOD.
Subjects
Procedure.
Materials and Scoring.
Hypostheses.
RESULTS
Subject Characteristics.
Instrumentation.
Experimental Manipulations
Major Findings
Tests of Specific Hypotheses
DISCUSSION.
APPENDIX A.
APPENDIX B.
APPENDIX C.
APPENDIX D.
APPENDIX E.
REFERENCES •
vi
PAGE
40
40
42
44
48
50
50
50
55
57
65
71
80
84
85
89
90
91
. ------ -----------------------------------------------------------------------.----

LIST OF TABLES
TABLE
1 A Comparison of the Three Most-Frequently Cited MMPI Indices Used to Identify Malingered Protocols ••
2 Design of the Present Study ••
3 Demographic Characteristics of Experimental Subjects (Expressed in Group Means and Percentages
4 Inter-Rater Reliability Estimates for Six Aspects of Bender Gestalt Drawings
5 Intercorrelation Matrix of Bender Gestalt Scores
6 Means and Standard Deviations (in Parentheses) on the MMPI
PAGE
27
41
51
52
54
Validity Scales and on the Goldberg Psychoticism Index • • 56
7 Mean Number of Correct Responses on Each Malingering Scale Subtest.
8 Discriminating Power of the Discriminant Functions
9 Significance of the Discriminant Functions • •
10 Discriminant Functions Analysis Classification Results
11 Standardized Discriminant Function Coefficients ••••
12
13
14
Discriminant Functions Evaluated at Group Means (Centroids) • • •
Means and Standard Deviations (in Parentheses) for' the Bender Gestalt Malingering Criteria. •
Comparison of Hit Rates (Percent of Group Correctly Classified) for Discriminant Analyses Based on Individual Tests Versus the Test Battery • • • • • •
vii
58
61
61
63
64
66
69
70

ABSTRACT
Malingering refers to the voluntary production of false or
greatly exaggerated symptoms in pursuit of an obviously recognizable
goal. Numerous studies have shown that psychological tests can detect
persons faking various mental disorders; however, the majority of these
are plagued by methodological flaws that seriously limit their validity
and generalizability. The present study employed a contrasted-groups
design that allowed for a rigorous test of the hypothesis that a battery
of psychological tests can detect persons given a financial incentive to
fake insanity or mental retardation. In addition to using two tests
previously employed in simulation research (MMPI and Bender Gestalt), an
instrument whose sole purpose is to differentiate malingerers from
genuinely impaired adults was developed for validation in this study.
This pen-and-paper test (the Malingering Scale) consists of 90
arithmetic, vocabulary, information and abstraction items, and requires
20 minutes to complete.
One hundred male adults were divided into five groups of 20
subjects. Two groups consisted of genuinely impaired subjects (either
mentally retarded or psychotic inpatients). The other three groups were
drawn from a population of prison inmates. Two of the latter groups
were offered a financial incentive for successful simulation of a mental
disorder (either mental retardation or "insanity") while the fifth group
consisted of inmate controls (answering honestly).
viii
-- - - - -- -- -------------------------------------------------------

ix
The test battery was administered to all subjects and scored by
examiners who wer~ naive to the purpose of the study. A series of item
analyses established the internal consistency of the Malingering Scale
and identified those items which best differentiate malingerers from the
genuinely impaired. These items were assembled into scoring keys for
subjects faking each condition. All test scores were then entered into
a series of discriminant function analyses which confirmed the
hypothesis that the battery provided more powerful discrimination of
subject groups than any single test. Overall, 84% of subjects were
accurately classified into their respective group, and 96% of subjects
were correctly identified as either malingering or not malingering. The
most powerful single instrument proved to be the Malingering Scale.
Directions for future research, including the necessity for cross
validation of the Malingering Scale, were discussed.

CHAPTER I
INTRODUCTION
In the 1980 Diagnostic and statistical manual of mental
disorders (3rd ed.), or DSM III, the American Psychiatric Association
(APA) rejected the notion that malingering constitutes a mental
disorder. Rather, the essential feature of malingering is described as
the "voluntary production and presentation of false or greatly
exaggerated physical or psychological symptoms." These symptoms do not
necessarily reflect an underlying psychopathology, but are "produced in
pursuit of a goal that is obviously recognizable with an understanding
of the individual's circumstances." Examples of such goals include: the
avoidance of military induction or undesirable work, evasion of criminal
prosecution, and the procurement of drugs or financial compensation.
The differentiation of malingering from conversion and other
somataform disorders is based on the clinician's judgement that observed
symptoms are voluntarily produced (in contrast, for example, to
"hysterical blindness") and manifested in the presence of an obviously
recognizable goal. Malingering must also be differentiated from
factitious disorders, possibly a more subtle differentiation.
Like malingering, factitious disorders are also "characterized
by physical or psychological symptoms that are under voluntary control."
However, unlike malingering, such symptoms are produced in the absence
of any recognizable goal, and the differentiation is based on this
1
-- - --- -------

2
distinction. Here, the symptom picture is considered to reflect a
mental disorder because the patient's simulation of illness has a
compulsive quality which renders him unable to refrain from the
factitious production. One example of factitious disorder is
"MunchausE!U's Syndrome," which is described below. Thus, factitious
symptoms are regarded as "voluntary" in the sense that they are
deliberate and purposeful, although the individual suffering from a
factitious disorder is regarded as lacking the control required to not
feign illness.
The range of contexts in which malingering occurs is very broad.
Broader still is the range of illnesses which have reportedly been
malingered. Spanning centuries of history are reports of individuals
who have faked illnesses ranging from sensory and motor deficits, such
as blindness or paralysis, to physical ailments, such as dysentary,
anemia, and cardiac arrhythmia, and of course mental disorders (Garner,
1939; Jones & Llewellyn, 1917).
The purpose of this study is to develop a psychological test
whose sole function is to detect persons who are malingering either of
two mental conditions: "insanity" or mental retardation. The
discriminatory power of this Malingering Scale will be evaluated in
conjunction with two widely-used psychological tests, the Minnesota
Multiphasic Personality Inventory (MMPI) and the Bender Visual Motor
Gestalt Test (Bender "Gestalt). In addition, the response patterns of
subjects faking each condition will be compared in order to determine if
the simulation of one disorder is more easily detected than the other,
and if any systematic differences between their test response patterns
emerge.

3
History
The view endorsed by the APA is particularly significant given
the difference of opinions surrounding just what types of simulation
should be included under the rubric "malingering." Probably everybody
has escaped an onerous responsibility by malingering at some time or
another. The youngster who complains of a stomach ache in order to skip
school fits the strictest definition of malingering. But when does this
type of behavior, which few would consider very harmful, become
"malingering"? In the DSM III this issue is addressed by excluding
certain disorders. Two clinical syndromes that have been identified by
various writers as forms of malingering are specifically excluded from
the current definition. One such illness is called Munchausen's
Syndrome.
Munchausen's Syndrome
The term "Munchausen' s Syndrome" was coined by Asher (1951).
Following an extensive review of the literature, Ireland, Sapira and
Templeton (1967) outlined eight features commonly cited in case studies:
(1) feigned severe illness of a dramatic and emergency nature, the symptoms of which mayor may not be borne out by physical examination; (2) factitious evidence of disease, surreptitiously produced by interference with diagnostic procedures or by selfmutilation; (3) evidence of many previous hospital procedures, particularly laparotomy scars and cranial burr holes; (4) pathological lying; (5) aggressive, unruly behavior and a "mixture of truculence and evasiveness in manner" (Asher, 1951); (6) departure' from the hospital against medical advice; (7) a background of many hospitalizations and extensive travel; and (8) the absence of any readily discernible ulterior motive. (p. 579)

4
Asher (1951) had previously described several of these
characteristics, but felt that the most remarkable feature is that such
patients, unlike malingerers who gain some definite end, "seem to gain
nothing except the discomfiture of unnecessary investigation or
operations." Instead of seeking some recognizable goal, the simulation
of illness seen in Munchausen patients is 'believed to derive from an
intrapsychic need to assume the "patient" role (APA, 1980).
Ganser Syndrome
In 1898 Ganser described this disorder (cited in Anderson,
Trethowan, & Kenna, 1956) the essential feature of which he regarded as
the symptom known as "vobeireden." The term "vobeireden," often called
"the symptom of approximate answers," actually translates as "talking
past the point." It was originally described by Moeli in 1888 who, upon
questioning patients with this condition, characteristically found in
their responses that "the answer is wrong, it is true, but it bears some
relationship to the sense of the question and shows that the sphere of
appropriate concepts had been touched (cited in Anderson et a1., 1956,
p. 14). Thus, when asked to solve a problem such as "3 times 8," the
patient might respond "25." When asked to name the capital of France,
the patient might answer, "London."
One might ask, by what process are "approximate answers"
produced? It is generally assumed that such responses are the result of
a patient's conscious attempts to appear less intelligent or more
disorganized than he actually is. Thus, when asked a question, the
patient silently thinks of the correct or appropriate answer, if he
knows it, but then subverts this answer in order to produce an incorrect
-- "-' - ............ _-_ .. _---_ .... _-.. ----------------------------- --_ .. - ... _._-----_.

5
response. In so doing, however, the patient is unable to depart from
the "sphere of appropriate concepts," presumably because he has become
ensnared in a mental set or einstellung.
Somewhat more controversy has surrounded the question of whether
to regard Ganser Syndrome as a separate disorder or simply as one form
of malingering, than the same question in regard to Munchausen's
Syndrome. Wertham (1969), for example, dismissed Ganser Syndrome as a
"hysterical pseudostupidity which occurs almost exclusively in jails and
in old-fashioned psychiatric textbooks. It is now known to be almost
always due more to conscious malingering than to unconscious
stupefaction" (p.191). Nevertheless, as noted previously, Ganser
Syndrome is considered a mental disorder in the DSM III (where it is
classified as a Factitious Disorder) when Ganser features are evidenced
in the absence of an obviously recognizable goal. Of course, this does
not preclude the possibility that a malingerer will evidence
"vobeireden" in his simulation of various mental conditions.
Hysteria
Finally, it should be noted that the various somataform
disorders listed in DSM III are regarded as mental disorders on the
grounds that the physical symptoms observed in patients with these
disorders are not under voluntary control. Here the question is not
whether hysteria and malingering represent different disorders, but how
the two can be differentiated. That is, the difficulties inherent in
differentiating hysteria from true malingering are complicated by the
possibility that malingering and hysteria may well occur in varying
admixtures in the same individuals (Hender~Dn & Gillespie, 1941).

6
Depth of Psychopathology
Parallel to the controversy over just what kinds of simulation
should be considered malingering is another historical disagreement over
the degree of psychopathology reflected in the act of malingering. From
one perspective malingering is viewed as indicative of fairly severe
mental disorder.
Bleuler (1924) wrote that "those who simulate insanity with some
cleverness are nearly all psychopaths and some are actually insane"
(p.191). Eissler (1951) felt that "malingering is always the sign of a
disease often more severe than a neurotic disorder because it concerns
an arrest of development at an early phase" (p. 252). Others have
suggested that malingering may occur in individuals suffering from a
wide variety of mental disordero, including neuroses, psychoses,
personality disorders, mental retardation, and extreme fear states
(Flicker, 1956; Hofling, 1975; Moersch, 1944).
In contrast, Jones and Llewellyn (1917) argued that malingering
does not necessarily imply that the individual has a mental disorder.
Rather, they wrote:
The etiology of malingering is the etiology of Deceit; the motives for both are unchanging, perennial as the passions of mankind •••• It is therefore in the moral and ethical sphere that the ultimate origins of malingering are to be sought, in the gamut of human passions -- ambition, revenge, fear, greed reinforced or dictated by poverty, ignorance, weakness of mind or frame. (p. 11)
Szaz (1957) would probably agree with their view, and has argued
further that malingering does not meet the criteria of a diagnosis at
all. In fact, he felt that the malingering cannot be given rational
meaning as a psychopathological syndrome and should be eliminated as an

7
item in the differential diagnosis of various mental disorders. Wertham
(1969) also endorsed this view in the following:
I have done research on the simulation of mental disease for a long time and found out a number of curious things. There is a strange, entirely unfounded, superstition even among psychiatrists that if a man simulates insanity there must be something wrong with him in the first place. As if a sane man would not grasp at any straw if his life is endangered by the electric chair! (p. 49).
Debate over the degree of psychopathology inherent in
malingering may continue; however, in the official nomenclature of the
APA, malingering is not listed as a mental disorder, but as a condition
that is not attributable to a mental disorder. It is regarded as more
likely to occur among persons with Antisocial Personality Disorder. In
sum, we have seen that malingering is not to be confused with either
Gasner Syndrome or Munchausen, nor is it to be regarded as a mental
disorder at all. The malingerer must be differentiated from the
hysteric, yet individuals with any of these disorders may also at times
consciously produce or exaggerate symptoms for some desired end. That
is, the neurotic may exploit his pre-existing illness by exaggerating
the symptom picture for some desired end.
Then what precisely is malingering? As yet, there is probably
no adequate answer to this question. It is clearly stated in the DSM
III that individuals with antisocial personality disorder are more prone
to malinger than others, when faced with an opportunity to do so. Yet
not a single study using psychological test instruments to empirically
verify this claim has been reported in the literature. Moreover,
clinicians of considerable stature have simply concluded that
malingerers are no more than "liars" and "scoundrels" regardless of

8
whether or not their "lying" is superimposed on some "unrelated" mental
disorder. The question is further complicated when one considers the
context in which an act of malingering occurs. Who would condemn the
prisoner of war who succeeds in concealing tactical information or
secures his own release by feigning illness? Does such behavior
consitute malingering? Clearly we must consider the context of the act
to understand its meaning. Perhaps further consideration must be given
to the "obvious recognizability" of the goal, as well. In reference to
the latter Menninger (1935) reminds us that "behavior cannot be
understood in terms of conscious intentions alone; unless one considers
the unconscious motives which determine an act one cannot understand the
significance of the act to the actor" (p. 509).
The range of behaviors subsumed under the rubric of malingering
is often broadened even further by those writers who include
dissimulation, that is, the conscious effort to "fake good" or appear
more adjusted than one actually is, in order to obtain some desired end,
such as a job. Many authors consider dissimulation to be the "other
side" of the malingering process, and military psychiatrists have often
reported seeing dissimulation more frequently than malingering proper.
Because of the many unanswered questions about the nature of
malingering, the need for further research to help define the parameters
(such as the "who," "how," and "for what goals") that characterized
these phenomena is self-evident. As we shall see in the next section,
however, simulation research is further warranted by the social costs
associated with ignorance about the problem of malingering.
---------------------. _._- . -_. ---------_ ....

9
Scope of the Problem
DSM III gives no indication of the prevalence of malingering.
This is not surprising in light of the widely differing estimates
reported in the literature. Jung (1903) reported that only 0.13% of
8,430 hospital admissions at Burgholzli were diagnosed as malingering.
Reports from various military psychiatric settings (Brussel and Hitch,
1943; Flicker, 1956; Sund, 1970) suggest that the prevalence in these
settings may range from 0.03% to 7%.
The military is but one stage, however, upon which the
malingerer may enact his pretense. Even if one assumes a low incidence,
the cost of hospitalizing individuals feigning illness to obtain
medication, food, or shelter can mount rapidly. Yet in spite of this
fact, recent incidence rates for malingering in hospital admissions have
not been reported.
The possibility of malingering also presents special problems to
the legal system in various situations. Two such situations are
Worker's Compensation law for "mental injuries" and damages for
"emotional distress" in tort law. Every jurisdiction in the country has
worker's compensation law, which applies in nearly all industrial
injuries to guarantee that workers receive compensation for injuries
that arise "out of and in the course of employment." Merrikin, Overcast
and Sales (1982) reviewed the status of worker's compensation law in
each of the fifty states, the District of Columbia, and the federal
system regarding three legally distinct types of work-related injuries
that are frequently litigated. They found that where a work-related
"physical" cause results in a mental injury, all jurisdictj.ons treat the
---------------------------------- .... --

10
full disability as compensable. All but one treat as fully compensable
those accidents wherein a "mental" cause results in a physical injury
(e.g., fear aroused by one's proximity to a potentially fatal accident
results in a heart attack). However, it was found that tremendous legal
confusion surrounds the type of accident wherein it is claimed that a
"mental" cause results in a mental injury. Only twenty-five
jurisdictions were found to allow compensation for such mental-mental
injuries in the event of sudden onset; only fifteen percent were found
to award compensation for gradual onset mental injuries. In short, the
authors argue, courts and legislatures are wary of a "compensatory
scheme which is pregnant with possibilities for malingering," and
conclude:
Until psychological research develops accurate techniques for identifying malingering in compensation cases, ••• courts and legislatures will continue to make compensation decisions which are based not on the actual presence or absence of a work-connection, but rather on artificial causation criteria, outright bans on compensation for gradual onset mental injuries, or legal allocations of the burden of proving work-connection. (p. 386).
Miller, Overcast and Sales (1984) conducted a similar review of
tort law regarding recovery of damages for "emotional distress." Tort
law includes that body of civil law which deals with remedies for
private wrong-doing. The authors argue that due inpart to the
difficulties inherent in differentiating between genuine and malingered
claims for emotional distress, there is substantial variation among
jurisdictions in their approaches to handling such claims. To deal with
the uncertainly of these claims, courts have relied upon various
artificial tests to determine the genuineness of emotional distress
claims. Early tests required physical impact on the injured party,

11
while later tests required the presence of the ~laintiff in a vaguely
specified "zone of danger," or that the alleged emotional distress was
"foreseeable" under the circumstances. The authors conclude that the
"special skills and knowledge possessed by psychologists should be
brought to bear on the development of accurate and legally relevant
techniques for differentiating between spurious and genuine claims of
emotional distress" (p. 13).
The specter of malingering is also raised in other legal
settings. In his work on forensic psychiatry, Davidson (1965) reported
that, of the various psychiatric disorders, the only ones likely to be
malingered
deficiency.
have little
are amnesias, psychoses, psychoneuroses, and mental
He argues further that since psychoneurosis and amnesia
bearing on a defendant's responsibility, malingered
psychosis or mental deficiency are more frequently encountered in
criminal cases. It seems quite possible, therefore, that some
proportion of defendants who enter pleas of "Incompetent to Stand Trial"
(1ST) or "Not Guilty by Reason of Insanity (NGRI) malinger precisely
these conditions.
On the basis of a national mail survey, Steadman, Monahan,
Hartstone, Davis, and Robbins (1982) reported that there were 6,420
patients admitted to various mental health and "specialty" institutions
across the United States in 1978 as 1ST. From this figure they
extrapolated that approximately 25,000 defendants had been evaluated for
competency in this time period. One can only guess how many of the
18,500 defendants found "competent" to stand trial had tried to malinger
"incompetence. " These authors also report that 1,625 patient had been

12
admitted to hospitals as NGRI during the same time period, and cite
three studies which found that the acquittal rates for defendants
entering a plea of NGRI ranged from 1% to 25%. Thus, between 75% to 99%
of defendants who plead NGRI were convicted; how many were malingering?
In short, from medical to legal settings, the malingering of
various mental disorders presents problems of considerable social
import. With worker's compensation law making further inroads into
compensation for "mental injuries" (Merrikin, Overcast, & Sales, 1982),
and the substantial number of criminal defendants entering pleas of 1ST
and NGRI, it has become imperative to determine the accuracy with which
clinicians can identify malingerers, and to improve upon this accuracy,
where possible. Numerous studies on the detection of malingering have
been conducted, especially since World War II, which indicate that
psychological tests can be helpful in identifying certain kinds of
malingering. However, in order to draw any definite conclusions, it
will be necessary to review and critically evaluate the research in this
area.
Overview of Malingering Research
Generally, the designs employed in these studies represent three
levels of sophistication. The first level essentially consists of case
studies. These "uncontrolled" studies invariably present findings that
are based on one or more subjects who were either "suspected" or "known"
malingerers.
The largest number of reported investigations consist of
"partially controlled" studies. In this category are studies which
compared the test results of an "experimental" group of subjects who

13
were either instructed to fake a mental disorder or who were "suspected"
of malingering, against the test scores of another group. Often the
second group was comprised of normal subjects answering honestly (i.e.,
a normal control), though many studies used genuinely disordered
subjects answering honestly (i.e., a criterion group). Some studies
even used a second experimental group given different instructions, such
as "fake good," for comparison with their malingering group.
Finally, a limited number of third level or "fully controlled"
studies were found. In these studies, each of three groups were used:
an experimental group ("suspected" malingerers or subjects who were
instructed to malinger), a criterion group (mentally disordered subjects
who answered honestly), and a normal control group (answering honestly).
The present review will discuss studies on the simulation of mental
disorders that were reported between 1943 to the present, and that used
psychological tests as a basis for their findings. These may be divided
into two broad categories: those which relied primarily on intelligence
tests, and those which employed other personality measures, such as the
MMPI and the Bender-Gestalt test.
Intelligence Tests
Nine studies (Anderson, Trethowan, & Kenna, 1956; Bash & Alpert,
1980; Crowley, 1952; Goldstein, 1945; Heaton, Smith, Lehman & Vogt,
1978; Hunt, 1946; Hunt & Older, 1943; Pollaczek, 1952; and Wachspress,
Berenberg & Jacobson, 1953) on the use of intelligence tests to detect
malingerers have been reported in the literature. In reviewing these
studies, it is apparent that the major impetus for devising strategies
to identify malingerers on this basis came from military settings, where

14
large numb~rs of recruits are routinely screened with brief intelligence
tests. Five of the nine studies utilized military personnel in their
samples, and all nine were reported after World War II.
Only one of these studies (Wachpress, et a1., 1953) is of the
case study variety. These authors reported descriptive findings on
psychological tests administered to three army recruits who were
suspected of malingering psychotic conditions. On intelligence tests,
it was found that "grossly irrational" responses depressed the raw
scores of each recruit's protocol. One patient was reported to answer,
"London is in France," and that "the capital of Italy is Prague." It
should be noted that, while these responses may be "grossly irrational,"
they are also examples of vobeireden." The authors also found marked
inconsistency of intellectual functioning across tests. For example,
one patient obtained a Wechsler-Bellevue IQ estimate of 57, while his IQ
estimate based on the Rorschach was well within the normal range.
Four studies were of the partially controlled variety; that is,
none of these included a control group for comparison. Such a group
serves to insure that subjects instructed to fake a disorder, such as
mental retardation, do indeed alter their test performance in response
to this experimental manipulation. Instead, each of these studies
compared the test results of one or more groups instructed to malinger a
mental disorder with those of a criterion group of genuinely disturbed
individuals. Such a design permits one to estimate the accuracy (i.e.,
the hit rate) of a given test instrument for differentiating such
groups. However, such a design fails to demonstrate that any obtained
group differences are due to the effects of a response set to malinger,

15
rather than to the simple fact that "malingering" subj ects are not
mentally disordered. Heaton, et al. (1978) compared the WAIS results of
an experimental group instructed to fake a "head injury" whith those of
a group of "nonlitigating head trauma patients." Although it was shown
that the malingering subjects did fake deficits on the WAIS, their IQ
estimates (and all of their subtest scores except Similarities) did 'not
differ significantly from those of the head trauma patients. Item
analyses were not conducted in this study.
Hunt and Older (1943) and Pollaczek (1952) compared the results
of subjects faking "feeble-mindedness" with those of genuinely retarded
subjects on various IQ screening instruments. Hunt (1946) later
compared the test results obtained from subj ects faking
"feeble-mindedness" in his earlier study with those of two schizophrenic
groups. In each of these studies, item analyses were undertaken to
examine the patterns of inter-item scatter in response accuracy produced
by each subject group. These analyses are based on the assumption that
"the malingerer is not familiar with the complete picture of the disease
he is simulating, and hence is unable to duplicate it" (Hunt & Older,
1943, p .250) •
In the Hunt and Older (1943) and Pollaczek (1952) studies it was
hypothesized that malingerers would fail more of the easy items and pass
more of the hard items than mentally deficient subjects. To test this
hypothesis, the percentage of malingerers and "feeble-minded" subjects
passing each test item was recorded. Hunt and Older found that more
"feeble-minded" than malingering subj ects passed the two easier items,
while this pattern was reversed on eight more difficult items. These

16
investigators did not statistically evaluate the obtained differences in
response scatter. Pollaczek essentially replicated this study using a
different test, the CVS abbreviated intelligence scale. However, she
did statistically evaluate the obtained differences using a series of t
tests, and found that 17 out of 37 items significantly differentiated
her college students who faked "stupidity" from a group of mentally
retarded adults. Finally, Hunt (1946) demonstrated that the pattern of
response scatter produced by malingerers was different than that
produced by schizophrenics, although he again failed to use inferential
statistics to evaluate these differences. Briefly, he found that far
more schizophrenic subjects passed the easy items than malingering
subjects, but there were few between-group differences on the more
difficult items.
The remaining four studies were found to represent fully
controlled design. That is, each included at least one experimental,
one criterion, and one control group. Anderson, et al. (1956)
contrasted the interview and test data of an experimental group
instructed to "feign mental abnormality" with those of a normal control
group and two criterion groups, consisting of "pseudo-dementia" and true
dementia patients. Unfortunately, these investigatqrs reported almost
no quantitative analysis of the data. It was reported that "contrasting
the responses of each group to each one of the 32 questions on memory,
orientation, &c., in relation to the whole performance, few significant
differences emerge" (Anderson, et al., 1956, p. 518). However, normal
subjects were reported to make a "substantial number" of errors
resembling "simple approximate answers of the 'two-and-two-make-five'

17
kind," but that "gross 'vobeireden,' e.g. calling coins 'discs and
ovals' ••• were not given by normal subjects" (p. 518).
Bash and Alpert (1980) compared the test results of an
experimental group of inpatients who had been diagnosed by two
psychiatrists as "malingering hallucinatory schizophrenia" with those of
a nonpsychotic
consisting of
inpatient control group and two criterion groups
hallucinatory and non-hallucinatory schizophrenic
inpatients. In a series of planned comparisons using a one-way ANOVA,
each of six subtests scored for "approximate answers" significantly
differentiated "malingerers" from non-malingerers. These six subtests
included Arithmetic, Block Design, Digit Span, Picture Arrangement,
Information, and Picture Completion. For each of these an "approximate
answers" scoring procedure was devised. On Arithmetic items, for
example, an answer of one above or below the correct response (such as
4 + 3 = 6 or 8) earns a score of +1. The "approximate answers" score
for each subjects on the six subtests was calculated and transformed
into a standard score based on the distribution of all subjects. Using
these standard scores, together with their "malingering" scores on
several other tests used in the study (Rorschach, Bender Gestalt,
Listening Task, and Betts Test), subjects were diagnosed as either
malingerers or non-malingerers. The correlation (phi coefficent)
between test diagnosis and previous psychiatric diagnosis was found to
equal .89. Cross tabulation indicated that the composite test score
produced a hit rate of 87% with 1% false positives. Only four
malingerers were incorrectly identified as genuinely disturbed, with one
non-malingerer misdiagnosed as faking.

18
In the study by Crowley (1952), a series of chi-square tests
indicated that 20 out of 25 test items significantly differentiated
subj ects faking "feeble-mindedness" from genuinely retarded subj ects.
She based her analyses on group differences in response accuracy or
inter-item "scatter," as did Pollaczek (1952) and others. She
introduced a minor variation to this strategy by examining differences
in the "distribution of credits earned" on test items, with each items
being scored ), 1, or 2 points.
Finally, Goldstein (1945) invited one group of subjects to
purposely fail an army intelligence screening test as if they were
trying "to evade Army service." He compared their test results with
those of a criterion group who actually failed the test and with a
control group who passed the examination. He too based the item
analyses on response "scatter." That is, he recorded the percentage of
malingerers and genuine test failures passing each item and then
calculated the raw differences in percentages. He then incorporated
those items showing the greatest percentage differences into a series of
scoring keys. By weighting items according to the size of the
differences, he developed several different keys which were then applied
to his groups. The "optimal" cutoff score was set at that point which
allowed for the least amount of overlap between-his malingering and test
failure groups. The best scoring key correctly identified 96% of the
malingering subjecfs with 16% false positives (genuine test failures
misidentified as faking).
To cross validate both the scoring key and the "optimal" cutoff
score, Goldstein then compared the test results of a second group of

19
recruits instructed to malinger "feeble-mindedness" with those of
another group of genuine test failures. In this cross validation he
obtained a hit rate of 98% with 14% false positives. It should be noted
that, although the rate of false positives associated with Goldstein's
key is undesirably high, there is no way of knowing whether or not some
of the men in his genuine test failure groups had actually been
malingering. If some of his criterion group subj ects had actually
failed the test intentionally, then his obtained false positive rate
would surely be an overestimate, thus making his scoring key even more
accurate than was reported.
In only one study (Goldstein, 1945) was an investigation of
reliability of the malingering test conducted. This researcher used a
split-half method with Spearman-Brown correction to assess the
reliability of his malingering scoring key for the Army Visual
Classification Test. He obtained an r=.91 for the test across all three
groups, and an r=. 73 for the optimal scoring key. However, Goldstein
pointed out that this reliability of the malingering key for the control
and "test failure" groups, whose reliability coefficients approached
zero. This finding was expected; their malingering scores should, by
definition, be uncorrelated.
Summary. In review, it is evident that all five of the nine
studies which sought to identify subjects simulating mental retardation
clearly demonstrated the adequacy of intelligence measures for making
this differentiation. Additionally, the variety of intelligence tests
used across studies lends cross validation to the underlying detection
strategies, especially the comparison of response "scatter." On the

20
basis of those studies in whi~h··rhit '"rates w'ere reported, it app~ars that
even' tr!:.f "intelLigence tests can be used to accurately identify 84% to
98% of normal subjects instructed to fake mental retardation, and to
accurately identify 84% to 90% of subjects who are genuinely retarded.
Unfortunately, while the hit rates obtained in some of these
studies are quite high, a number of methodological limitations restrict
the external validity of their findings. The present study was designed
to overcome many of these limitations. Howe~er, since the majority of
these problems are common to studies using personality as well as
intelligence tests, a discussion of their impact will follow a review of
the studies which used other instruments for detecting malingerers.
An interesting finding in at least one study (Hunt & Older, "
1943) is that subjects simulating mental deficiency were frequently
found to give bizarre or grossly illogical responses to test questions,
apparently reflecting their misunderstanding of the nature of mental
retardation. This, of course, suggests the possibility of using "
personality tests to detect subjects faking retardation, a strategy
which has not previously been employed. It is possible that a
combination of intelligence and personality tests may yield higher hit
rates, perhaps with fewer false positives than any single intelligence
measure scored for malingering.
Four of the nine studies employed intelligence tests to detect
subjects simulating a mental disorder other than retardation. In three
of these, qualitative examination of test responses revealed that such "
measures may effectively identify subjects simulating schizophrenia
(Bash & Alpert, 1980), various psychotic reactions (Wachspress, et al.,
..

21
1953) and "mental abnormality" (Anderson, et a1., 1956). In the fourth
study (Heaton, et al., 1978) it was shown that, with the exception of
Digit Span, the subscale and full scale WAIS scores of truly
head-injured subjects were not significantly different .. from those
simulating head injury. However, it should be noted that these authors
did not examine response "scatter" or "approximate answers," the two
types of item analyses which have proven to be the most effective for
the determination of malingering. ..
Personality Tests
In general, personality tests have been used to detect a broader
range of malingered pathology than intelligence tests, including:
psychosomatic disorders, .neuroses, psychoses" organic conditions, and
even "dissimulation," the concealment of pathology (Dahlstrom, et a1.,
1972). Inasmuch as the dissimulator attempts to conceal abnormalities
or character flaws in order to obtain some desired end, many writers
have argued that it should be considered' a form of malingering.
Nevertheless, research on dissimulation will not be reviewed here for
two reasons. First, the DSM III definition of malingering excludes the
problem of dissimulation. Second, the literature on dissimulation, by
virtue of its magnitude and complexity, warraftts a separate review. The
studies to be reviewed here will include those which relied primarily on
the Bender Gestalt or the MMPI for detecting subjects faking a mental
disorder.
"
----------------------~---------~--. ---

22
Minnesota Multiphasic Personality Inventory "
Thirteen studies using the MMPI to detect subjects malingering
various conditions have been reported since the development of this
instrument. None of these have been of the uncontrolled or case study
variety. Seven studies were of the partially controlled type. Of "
these, four (Cofer, Chance & Judson, 1949; Exner, McDowell, Pabst,
Stackman & Kirk, 1963; Gendreau, Irvine & Knight, 1973; and Meehl &
Hathaway, 1946) employed nearly identical repeated measures designs in
which the results of a group simulating mental disorder were compared "
with the re-test results of the same subjects answering honestly. Two
of the partially controlled studies (Heaton, Smith, Lehman & Vogt, 1978;
Shaw & Matthews, 1965) compared subjects faking neurological deficits
with genuinely impaired subjects. The seventh study (Harvey & ",
Sipprelle, 1976) failed to include either a criterion group or a control
group, but simply compared the test results of one group instructed to
"fake good" with those of another group instructed to "fake bad." The
other six studies (Anthony, 1971; Gough, 1947, 1950, 1954; Grow, McVaugh '\
& Eno, 1980; Hunt, 1948) used fully controlled designs. In each of
these studies the test results of at least one group instructed to fake
a mental disorder (or to "fake bad") were compared with those produced
by genuinely disordered and normal control groups who were given "
standard instructions.
Detection Strategies and Validity. Numerous strategies for
detecting malingered performance on the MMPI have been described. Early
in the development of this test it was discovered that neither the L nor
the K scale effectively identified profiles in which subj ects

23
intentionally presented themselves in an unfavorable or abnormal manner
(Meehl & Hathaway, 1946). However, the F scale has proven to be quite
useful for this task. In their original demonstration of this, Meehl &
Hathaway (1946) asked 54 adult males to take the MMPI twice, once under
standard conditions and a second time with the instructional set to
"obtain adverse scores without giving themselves away." Using the F raw
score cutoff of 15, 96% of the faked protocols were correctly
identified. Unfortunately, the number of false positives was not
reported.
Gough (1946) believed that clinical scale profiles could be used
to differentiate authentic from exaggerated MMPI protocols. He reported
that the signs of an exaggerated profile include marked elevations on
Hs, D, Hy, Sc, and Pt scales. However, in a subsequent study Gough
(1947) found that subjects faking "severe psychoneuroses" produced
marked elevations on scales Sc, Pa, Pd, and D. He described the latter
subject's profiles as erratic and jagged, multiphasic, of irregular "
elevation and positive slope," in contrast to those produced by genuine
psychotics, which he described as "diphasic, of moderate elevation, and
with approximately co-equal peaks" (p. 220). More importantly, Gough
also observed that, regardless of what disorder was simulated, F scores
were elevated and the K scores were depressed. This led him to
investigate the F, K and F-K raw score difference as empirical indices
for differentiating faked from legitimate profiles. With the exception
of K score the results of these investigations are presented below in
Table 1. Data on the K scale scores are' excluded from this table
because the K scale, by itself, has proven to be a very poor index of

24
malingering (although it shows promise as an index of "faking good").
Like Meehl and Hathaway (1946), Gough found that the K scale failed to
detect malingering; his optimal K cutoff score identified only 45% of
the malingered profiles.
In a subsequent, fully controlled investigation of the F-K raw
score difference as an index of malingering, Gough (1950) compared 319
"simulated profiles" (most of which were donated by other investigators)
with 1,773 "authentic profiles." As shown in Table 1, he found that an
F-K cutoff score of 9 or greater correctly identified 75% of the
simulated profiles as faked, with only 3% false positives (authentic
profiles misidentified as faked). More interestingly, Gough calculated
the hit rates and false positive rates produced by every F-K cutoff
score from 0 to 16 for each of the eight subgroups which comprised his
criterion group. This data shows that the optimal cutoff score clearly
depends upon the nature of the criterion ~ used. For example, Gough
found that an F-K cutoff score of 6 or greater correctly identified 81%
of his malingerers. However, while this cutoff score misidentified less
than 2% of his control subjects (960 normal adults) as faking, it also
misidentified 9% of his criterion subjects (803 mentally disordered
adults) as faking. Further, among a group of psychopaths and a group of
psychotics, this same cutoff score (F-K=6) would produce false positive
rates of 45% and 39%, respectively. In short, he found that it is much
easier to differentiate malingerers from normal adults than from
genuinely disturbed adults, and that it is most difficult to
differentiate malingerers from severely disturbed adults, such as
psychopaths and psychotics.
--------------------.~--.- _._---_._----_.- .---

25
In a partially controlled investigation of the F raw score as an
index of malingering, Cofer, et al. (1949) compared the test results of
college students faking "emotional disturbance" with normal controls.
None of the malingerers obtained F raw scores of less than 20.
According to Gough (1950, p. 409), Cofer stated in a personal
communication than an F-K raw score difference of 5 or greater correctly
identified all of the malingered protocols, with no false positives.
Hunt (1948) also investigated the F-K index with a fully
controlled study in which he compared the results of college males and
prison inmates who were instructed to fake "abnormality" with their own
retest scores when given standard instructions and with the protocols of
193 psychiatric patients given standard instructions. As shown in Table
1, Hunt found that an F-K cutoff score of 11 or greater correctly
identified 87% of the malingered profiles. Not suprisingly, more
psychiatric patients (12%) than normal control subjects (8%) were
misclassified as malingering.
Then, in 1954, Gough reported the results of a large, fully
controlled study in which he devised the Dissimulation scale (Ds). To
construct this scale, Gough compared the response patterns of 111 normal
adults instructed to "fake a psychoneurotic reaction" with those of 176
actual psychoneurotics. For each item, the proportion of malingerers
who answered "true" was compared with the proportion of neurotics who
also answered "true. " The difference of
statistical significance for 74 items
cross-validated these items by comparing
these proportions reached
(Ds scale) • Gough then
the Ds scores of 354
malingerers with those of 915 psychiatric patients and 507 high school
---- ----------- -------------------------------------- --- ------ - -----.-----------

26
students answering honestly. The results are shown in Table 1. Again,
not surprisingly, the percentage of psychiatric patients who were
misclassified as malingering (6%) was higher than the percentage of high
school students who were mistakenly identified as malingering (2%).
Exner, et ale (1963) compared the relative accuracy of the F raw
score, F-K index, and Ds scale for differentiating the profiles of 25
students who were told to "appear sufficiently deviant to be exempt from
some social responsibility" with their own retest scores when given
standard ins truc tions. As shown in Table 1, all three indices were
remarkably effective.
While these early investigators were examining the utility of
the F, K, and F-K indices, Wiener (1948) pursued a different approach.
He divided the items on each MMPI scale into "obvious" and "subtle"
categories. Although his work was directed primarily toward the
identification of subjects who were faking "good," several later
investigators applied scores on the Subtle and Obvious item scales to
the task of identifying malingerers.
The first such application was reported by Anthony (1971). He
obtained the protocols of 40 Air Force men with nonpsychotic diagnoses,
then retested the same subjects under an instructional set to
"exaggerate on the test whatever difficulties had brought them into the
clinic." He then matched 32 of the "exaggerated" profiles (clinical
scales only) with protocols on file to compose a criterion group for
comparison. In comparing the 40 standard profiles with the 40
exaggerated ones, Anthony reported that a cutoff score of 45 on the
Subtle items scale produced a hit rate of 90% with 10% false positive.

27
Table 1
A Comparison of the Three Most-Frequently Cited
MMPI Indices Used to Identify Malingered Protocols
F (raw) F-K (raw) Ds scale
Comparison Cut- Hit Cut- Hit Cut- Hit Investigator Group off rate off rate off rate
Anthony, 1971 control 10 73% 0 75% 21 78%
criterion 30 34% 18 38% 30 63%
Cofer et a1., control 20 100% 5 100% 1949
Exner et a1., control 12 100% 12 96% 20 100% 1963
Gendreau control 34 100% 24 100% 96% et a1., 1973
Gough, 1947 psychotic 26 73% 16 82%
neurotic 14 64% 4 64%
Gough, 1950 combined 9 75%
Gough, 1954 control 35 93%
criterion 35 93%
Grow et al. , control 15 100% 7 98% 35 86% 1980
criterion 15 75% 7 81% 35 56%
Hunt, 1948 control 11 87%
criterion 11 87%
Meehl & control 15 96% Hathaway, 1946

28
A cutoff score of 100 on the Obvious items scale yielded a hit rate of
86% with 15% false positives. Unfortunately, it was considerably more
difficult to differentiate the exaggerated profiles from the "matched"
ones. Using a cutoff score of 36 for Subtle items, only 41% of the
exaggerated protocols could be identified, with 28% of the "matched"
criterion group profiles misidentified as faked. Using a cutoff score
of 170 on the Obvious items produced a slightly higher hit rate, 56%,
but this was accompanied by a false positive rate of 38%. Like most
recent investigators, Anthony compared the effectiveness of several
different detection strategies. An inspection of Table 1 reveals that
these findings for the Subtle and Obvious scales were more promising
than those for the F, F-K and Ds scales. These results are unusual; in
no other study has the use of Wiener's scales proven more effective for
identifying malingerers than the F, F-K or Ds scales.
Gendreasu, et al. (1980) compared the protocols of 24 adult male
prison inmates who took the MMPI on three occasions, with instructions
to answer honestly, give a "good impression," and give a "bad
impression." Although the cutoff score was not reported, these
investigators found that the Obvious items scale produced a hit rate of
88%; the false positive rate was not reported. As shown in Table 1,
however, the hit rates obtained by using the three most common indices
were considerably higher.
Grow, et al. (1980) reported the findings of two experiments.
First, the results of a group instructed to malinger "psychopathology of
one form or another" were compared with the results of a normal control
group to investigate the effectiveness of various malingering indices

29
using selected cutoff ·scores. Then, in a cross validation study the
protocols of 16 psychiatric patients who were "suspected of faking bad
on the MMPI" were compared with those of 14 patients who were believed
to have taken the MMPI in a "legitimate fashion." In the first
expe:L"imel1t it was reported that a cutoff score of 100 on the Obvious
ftems scale identified 48% of the malingering subjects with no false
positives reported for the control subjects. Using a cutoff score of 45
on the Subtle items scale produced a hit rate of 38%, with a false
positive rate of 14%. Upon cross validation, however, these scales
fared even more poorly. Using the same cutoff scores, only 25% of the
"suspected" malingerers w'ere identified with the obvious items (with 0%
false positives) while 44% were identified with the Subtle items (with
8% false positives). As shown in Table 1, the best indices for
detecting malingerers in these two experiments were the F raw score
using a cutoff of 15, the F-K raw score differences using a cutoff of 7,
and the Ds scale with a cutoff of 35.
Harvey and Sipprelle (1976) employed neither a control group nor
a criterion group, but instead compared a group instructed to fake "good
adjustment" with a group instructed to malinger poor adjustment. These
authors reported that Subtle items scores were significantly higher than
Obvious item scores for subjects faking good adjustment, while the
reverse of this pattern was shown for subjects faking poor adjustment.
In addition, malingerers obtained significantly higher scores on Subtle
items and significantly lower scores on Obvious items than subj ects
instructed to fake good adjustment. These researchers did not report
hit rates for these scales, nor did they report quantitative analyses of

30
the effectiveness of other malingering indices. They did find that the
Land K scales failed to differentiate the two groups, but that the F
scale detected both groups "very accurately."
Finally, Shaw and Matthews (1965) reported on the development of
a 17-item "pseudo-neurologic scale" to identify subjects who were
"suspected of simulating a neurological deficit." Their study compared
32 "suspected" malingerers with 32 brain damaged subjects by item
analyzing the Hs, Hy and Pd scales using roughly half of the subjects
from each group. The optimal cutoff score correctly identified 81% of
the "suspected" malingerers, with a false positive rate of 25%. In
cross validating the derived scale using their remaining subjects, 67%
of 18 "suspected" malingerers were correctly identified, with a false
positive rate of 22%.
None of the studies reported reliability data, or employed
designs which would permit analysis of test-retest reliability
estimates. However, those investigators who did use within subj ects
designs, wherein the instructional sets were counterbalanced for order,
consistently found that the order in which response sets were presented
to the subjects did not influence the nature of changes induced by the
instructional set.
Summary. On the basis of these thirteen studies it is evident
that normal subjects can simulate mental abnormality on the MMPI, and
that such malingered profiles can be accurately differentiated from
nonpathological ones. The detection strategies which appear to be most
effective are the F raw scores, the F-K raw score difference, and the
Dissimulation scale (Ds) developed by Gough.

31
In general, malingerers can be more easily differentiated from
normal subjects answering honestly than from genuinely disturbed
subjects answering honestly. This trend can be seen in Table 1 where it
is evident that hit rates are typically higher when malingerers are
compared with controls than with criterion group subjects. Yet, in
practice, malingerers must usually be differentiated from the genuinely
disordered. That is to say, when there is a question of malingering,
the clinician is seldom asked, "does this person appear to be abnormal
or normal"? Rather, the question is more likely to be whether or not a
given person t s abnormal appearance is genuine. Presently, there is
insufficient data to infer from which diagnostic categories (e.g.,
neurotics vs. psychotics) malingerers can be most accurately
differentiated.
As shown by these thirteen studies, the MMPI has been used to
detect several kinds of psychological malingering, including: "bad
impressions," psychoneuroses, psychoses, and brain damage, although it
has never been applied to the task of detecting malingered mental
retardation. Yet, as suggested in the review of intelligence test
studies, there is some anecdotal evidence suggesting that subjects who
are feigning mental retardation may display neurotic or psychotic
behavior as part of their deception. The present study will investigate
the utility of the MMPI for detecting malingered mental retardation.
Bender Gestalt
In her original monograph, Bender (1938) included the drawings
of a "confessed" malingerer, two prisoners who presented with "Ganser
symptoms," and four normal adults who were asked to "simulate mental
.- _ .... _---- .. ----._-- ---'

32
deficiency. " Her discussion of these protocols involved a description
of several features which she believed to be characteristic of the
malingered test performance. Her investigation thus constituted a case
study design with qualitative descriptions of the types of drawing which
(she concluded) should arouse suspicion of malingering. Regarding one
of these protocols, she notes that in an effort to inhibit his
intelligence, "the simulator has succeeded only in inhibiting his
impulses so that the drawings are small and inhibited" (p. 151).
Elsewhere she observed that "where the figures are distorted it is
accomplished by changing the relationship or direction of details. This
could be done only by first perceiving the correct gestalt and changing
a detail secondarily" (pp. 151-152). On several malingered protocols
Bender noted a tendency to simplify the symbols but strengthen the
gestalt. Finally, on one particularly transparent simulation, it was
noted that several complex details were actually added to the drawings.
On the basis of such features, which serve to betray the malingerer,
Bender concluded that "even when human beings lie with their
consciousness, they tell the truth with their unconscious" (p.150).
The Bender Gestalt test was also used in the study by Anderson,
et ale (1956) that was described previously. However, while the study
was fully controlled, only 13 of the 18 subjects who were instructed to
malinger actually took the Bender Gestalt, and the authors did not
report using it with subj ects in the other groups. Although it was
reported that 9 of the 13 malingerers produced "abnormal" records, the
criteria for making these judgements were not articulated. Instead, the
results of one subject were described qualitatively. Several features

33
of this description seem consistent with the observations of Bender.
For example, it was reported that Card A was drawn with the diamond half
imposed on the circle. Card 1 was drawn as a single unbroken straight
line, and Card 2 was reduced to a single wavy line. On Card 4 the
subject reproduced a wave line, but drew a wavy square above it, joined
by a bar, while Card 8 was "a mass of childish scribble." (p. 520).
In the fully controlled study by Bash and Alpert (1980) that was
described earlier, the Bender Gestalt test was included in a battery of
tests that was administered to each subject. Bash and Alpert
operationalized the features that Bender (1938) had originally described
as characteristic of malingered drawings. These features were then
taken as criteria (to be described below) for scoring the test
protocols. Each subject's "malingering score" on the Bender Gestalt was
included with his other test results in the series of discriminant
functions described earlier. Bash and Alpert reported hit rates for the
discriminant functions, but did not report the hit rates associated with
the Bender Gestalt itself, nor did they report the hit rate of any
individual test, for that matter. However, a planned comparison of the
Bender Gestalt malingering scores for "suspected" malingerers versus the
three comparison groups revealed highly significant differences, leading
these investigators to conclude that the Bender Gestalt is a "good
discriminator."
Bruhn and Reed (1975) reported a fully controlled study in which
college students took the Bender Gestalt twice; once with standard
instructions and a second time with instructions to simulate brain
damage. Their protocols were then compared with those produced by

34
genuinely brain damaged (craniocerebral trauma) subjects. The entire
procedure was piloted in order to establish the sorting criteria used by
an ABPP clinical psychologist, and then repeated with two additional
judges. Additionally, the effectiveness of two scoring systems
(Pascal-Suttell and Canter) were investigated. In the pilot study
neither scoring system showed any utility at all for differentiating
malingerers from genuinely brain damaged subjects, despite their
effectiveness for differentiating organics from normals. Thus, a Canter
cutoff score of 9 accurately identified 78% of the normals without
misclassifying a single organic, but only detected 3 of the 18
malingerers. However, in both the pilot and main studies, each of three
judges wer,e able to differentiate malingered protocols from those of
normal and genuinely organic subjects. Taken together, the three judges
produced an average hit rate of 93%, with 14% of the organics' protocols
misclassified as malingered (false positives). Unfortunately, these
investigators did not describe the features which betrayed the
malingered drawings; thus, it is impossible to tell the degree to which
their judgement criteria matched Bender's original observations.
Summary.
test may be a
These four reports suggest that the Bender Gestalt
useful instrument for detecting various types of
psychological malingering, including: brain damage, mental retardation,
and schizophrenia. However, Bender's original suggestions for the
evaluation of malingering have been operationalized only once (Bash &
Alpert, 1989), and have never been cross validated. Yet the consensus
of findings implies that a careful delineation of the features which
characterize malingered Bender Gestalt performance may prove to be of

35
considerable clinical utility. The present study involved a validation
of Bender's original scoring recommendations as operationalized by Bash
and Alpert.
Purpose
In this study, two groups of subjects took a series of
psychological tests on which they were instructed to respond "as if"
they were suffering from a mental disorder (i. e., to "fake" a mental
disorder). Their responses were then compared with those of three other
groups who took the same tests but were given standard instructions.
Two of the latter three groups consisted of mentally disturbed subjects,
while the third consisted of control subjects. The test results of
these five groups were compared in order to determine how well the
psychological tests would detect those subjects who were instructed to
"fake" a mental disorde::. In essence, this study is quite similar to
the majority of previous research on simulation. However, it also
differs from previous studies in several important ways.
Development of the Malingering Scale
A major purpose of the present study was to develop and validate
a brief, pencil-and-paper test whose sole function is to detect persons
malingering mental disorders. The absence of such an instrument has
severely limited simulation research in the past. Previous studies have
typically adpated standard psychological tests such as the MMPI or
Rorschach to the task of detecting malingerers, primarily because the
body of research on faking has been conducted with the aim of answering
questions about test validity (e.g., can the Rorschach be faked?).
- ._ .. _---_.-----_._ .. _--_._----------------------------- _. __ ._--- - --------------

36
Consequently, simulation research conducted over the last 35
years has relied almost exclusively on the use of personality tests for
detecting all types of psychologicaL malingering. Yet, evidence from
research conducted during and immediately after World War II (e. g. ,
Goldstein, 1945) suggests that subjects malingering certain disorders,
such as mental deficiency, can be better detected with specially-adapted
intelligence tests than with standard instruments.
best of these tests are either obsolete or not
Unfortunately, the
available today.
Further, the widely-used Wechsler Intelligence Scales are probably not
well suited to the development of a test for malingering because the
Wechsler scales contain too few easy items and because the items are
arranged in an obvious heirarchical order of difficulty. It is the
malingerers' failure to accurately judge item difficulty which permits
their detection. For this reason, in devising an effective test for
detecting malingerers, Goldstein (1945) recommends the inclusion of many
easy items arranged in a scrambled sequence. This requires the would-be
malingerer to make numerous judgements about item difficulty with a
minimum of cues about the actual (normative) difficulty of each item.
The Malingering Scale validated in the present study consists of 90
intelligence test items, many of which were adapted from existing
intelligence tests.
Use of a Test Battery
A second purpose of this study is to develop and validate a
battery of tests for detecting malingerers. Previous research indicates
that many simulators are able to elude detection (e.g., Gough, 1947).
It may be that some of these subjects "figure out" how to avoid

37
detection on a particular test. If this is so, then a battery of tests
on which the response demands vary (e.g., structured vs. projective;
personality vs. intelligence), may prove to be more effective in
detecting malingerers than any single instrument. The present study
employed a battery of psychological tests that includes a structured
personality test (MMPI), a projective personality test (Bender Gestalt),
and a test consisting of intelligence test items (the Malingering Scale
developed for this study.).
In one fully controlled study using a test battery, Bash and
Alpert (1980) discovered that the accuracy with which patients suspected
of malingering schizophrenia could be detected was considerably greater
using a battery of tests specially scored for malingering than using any
single test instrument. Although this finding has not been cross
validated, Heaton, et al. (1978) also reported finding higher hit rates
using a battery of tests than by using the MMPI alone for identifying
subjects faking neurological deficits.
Enhancing External Validity
A third general aim of the present study was to limit the number
of analog features that characterized the subject selection and
experimental procedures. Previous research has frequently employed
unrepresentative subjects, such as college students, who are given a
contrived instructional set, such as "give your worst impression" with
no real incentive for disguising their malingering.
Very few studies have drawn subjects from populations in which
the prevalence of malingering is believed to be higher than that found
in the general population. The present study employed prison inmates in

38
experimental and control groups to reduce the analog factor of subject
selection, and thus enhance the external validity of any significant
findings. The reason for selecting prison inmates to comprise the
experimental and control groups derives from the DSM III observation
that "suspicion of malingering is aroused by the presence of an
Antisocial Personality Disorder" (APA, 1980, p. 331). This conditon is
undoubtedly more prevalent among prison inmates than college students.
Additional relevant demographic differences between prison inmates and
college student
ethnicity. All
groups include age, sex, educational level, and
of these differences limit the generalization of
findings obtained in previous analog studies to the response patterns
which may be produced by the criminal who is malingering a mental
disorder in the hopes of evading criminal prosecution or conviction.
The majority of previous simulation research has employed
designs with other analog factors, extending well beyond the use of
unlikely populations. Studies in this area typically recruit subjects
to participate in an experiment, then assign them to one of several
groups. Those in the experimental group are usually instructed to fake
a mental disorder, as though they were seeking some imaginary reward,
such as evading military induction.
In considering these procedures, the question arises, is it
possible to design an experiment in which the reward contingencies can
be made to resemble those faced by individuals who actually malinger
outside of the laboratory? The present study implemented a design in
which subjects were confronted with a set of reward contingencies that
very nearly replicate the type of circumstances in which malingering is

39
likely to occur, thereby reducing the analog factors which have plagued
earlier malingering research.
Type of Disorder Simulated
The fourth general purpose of this study was to compare the
response patterns of subj ects who are simulating two different mental
disorders: mental retardation versus "insanity." One question to be
answered was whether subj ects malingering one of these disorders are
more easily detected than subjects malingering the other. A related
question asks which test most accurately detects subjects simulating
each type of disorder. These questions are of obvious clinical
-significance in that the answers to them may well dictate what specific
tests or type of tests should be included in a test battery for making a
determination of malingering. More broadly, if it is found that
subjects malingering mental deficiency are as easily identified with the
various tests at those faking "insanity," then there would be a stronger
basis for comparing the results of previous studies which used different
response sets in their experimental instructions.

CHAPTER II
METHOD
Subjects
A total of 100 male adults between the ages of 18 to 65
constituted five groups of twenty subjects each. Group I (MR) consisted
of subjects classified as mildly to moderately mentally retarded (i.e.,
IQ values ranging from 30 to 69), and who lived in semi-independent
satellite housing in Tucson, Arizona. Group II (Psy) consisted of
psychiatric inpatients drawn from the Tucson Veterans Administration
Medical Center who obtained scores which fell in the "psychotic" range
(Le., 50 and above) of Goldberg's (1965) Psychoticism index of the
MMPI. In his report of the cross validation of this scale, Goldberg
(1965) showed that a cutoff score of 50 accurately differentiated 74% of
861 adult males who were independently diagnosed as either psychotic or
neurotic. Thus, groups I and II comprised the "criterion" groups, the
genuinely disordered subjects who were given standard instructions at
the time of testing.
Subjects in Groups III, IV and V were drawn from the population
of prison inmates who were serving their sentences at the Arizona
Correctional Training Facility (ACTF), a medium security prison in
Tucson, Arizona. Group III subjects were instructed to fake mental
retardation (MgMr), while those in Group IV were instructed to fake a
psychotic condition (MgPSY). Group V subjects, serving as an inmate
40

41
control group, were given standard instuctions (i.e., with no
instructions to fake in any way), just like the genuinely disordered
subjects in Groups I and II.
All five groups were to be matched on the variables of age, sex,
and ethnic backg:t'ound. Additionally, with the obvious exception of
mentally retarded subjects, the groups were matched on educational level
and IQ. An IQ screening test (the Shipley Institute of Living Scale)
was given to the psychotic and prison inmate subjects to insure that
none had an IQ estimate which fell below 80 (the lower bound of the Low
Average range). The files of all inmates who participated in the study
were examined to screen out those who were diagnosed as suffering from a
psychotic illness at the time of testing. The present study is depicted
in Table 2.
Table 2
Design of the Present Study
Mentally Psychotic
Retarded Inpatients Prison Inmates
Answer Answer Malinger Malinger Answer
Honestly Honestly Retardation Insanity Honestly
Group I Group II Group III Group IV Group V
N = 20 N = 20 N = 20 N = 20 N = 20

42
Procedure
Depending upon the experimental condition in which they served,
subj ects were recruited in one of several ways. Initially, however,
every subject who volunteered to participate in the study indicated this
by signing a Subject's Consent form (Appendix A). At that time all
subjects (except the genuinely retarded) were asked to complete the
Shipley Institute of Living Scale (an IQ screening test). Each
subject's WAIS Full Scale IQ was estimated from this test using the
tables supplied by Paulson and Lin (1970) to insure that the
non-retarded subjects had rQs of 80 or above. In fact, the non-retarded
subjects were found to have IQ estimates ranging from 80 to 122. The IQ
estimates of mentally retarded subjects were obtained from their
Department of Economic Security, Division of Developmental Disabilities
patient files. In fact, the retarded subjects had IQ estimates that
ranged from a low of 13 to a high of 64. Finally, as explained in the
Subject's Consent forms found in Appendix A, at the time of screening,
each subject (or subject's guardian) was invited to participate (or give
permission for their ward to participate) in a psychological experiment
that was being conducted "in order to collect information about how
different people answer a recently-developed psychological test."
Group I (retarded) subjects were then asked to take two
psychological tests (i.e., the Bender Gestalt and the Malingering Scale)
which require approximately one hour of time altogether. They were paid
$2.00 for their participation. These subjects were not given the MMPI
because it was judged to be too difficult a task for them. Subject~ in
Group II (psychotic inpatients) wre also asked to complete the same two
-------------------- ----- --- -----------

43
psychological tests, although it was estimated that they would complete
the tests in 20-30 minutes. Because patients admitted to the Tucson
VAMC are frequently given the MMPI as part of the initial evaluation,
their MMPI results were automatically available to the experimenter when
patients agreed to participate in the study. Only those patients whose
MMPI revealed a Goldberg scale of 50 or greater were invited to
participate. It should be noted that the Goldberg scale involves a
linear transformation of five clinical scales; it does not include the
validity scales, which were ignored at the time of initial screening.
To fill Groups III, IV and V, all ACTF inmates were notified of
an opportunity to earn $2.00 by participating in a psychological
experiment (as described by the ACTF Subject's Consent form in Appendix
A). After the initial screening, 20 volunteers were selected at random
for assignment to an inmate control group (Group V). These subjects,
like those in the two criterion groups were asked to do their best and
answer test questions honestly.
Then, forty additional volunteers were assigned to Groups III
and IV (fake retardation and fake insanity) and subjected to a
deception. These men were informed that no further subjects were needed
for the original study, but that they were invited to participate in
another experiment. These men were then given a second ACTF Subject's
Consent form that described an experiment in which the subject was asked
to fake a mental disorder while taking some psychological tests. The
consent form explained that any inmate who could successfully fake a
specified mental disorder (either retardation or insanity), without
being detected by an experimenter who later examines their test results,

44
would be awarded $15. The exact wording of these instructions may be
found in Appendix A. Thus, subj ects in Groups III and IV were faced
with a set of reward contingencies which approximate those faced by bona
fide malingerers, viz., a high reward for successful deception, but
little or none for unsuccessful attempts. However, in order to insure
their continued cooperation, all subjects in the two malingering groups
were assured of $2.00 for participating, regardless of whether or not
they were detected. As with the other three groups, these subjects were
assured that all their test results would be kept confidential and that
their participation in the study would not affect their treatment at the
institution.
After consenting to participate in the "second" study, the forty
subjects who constituted Groups III and IV were given more detailed
instructions about the nature of their task. These instructions, which
were read aloud to the subjects, may be found in Appendix B.
The subjects in Groups III, IV and V were all administered the
MMPI, Bender Gestalt and Malingering Scale. After receiving their
instructions from the experimenter, subjects were tested by one of two
research assistants who were led to believe that the sole purpose of the
present study was to collect data on an IQ screening test and were
unaware that the study concerned malingering in any way.
Materials and Scoring
The two most commonly-used and most accurate faking scales
reported for the MMPI (F and F-K) were calculated for each protocol. On
the Bender-Gestalt test, six features of each subject's drawings were
scored for malingering. These features were those originally described

45
by Bender (1938) as characterizing the drawings of malingerers. Bash
and Alpert (1980) operationalized these features for their investigation
of malingerers, and concluded that the Bender Gestalt proved to be an
extremely sensitive test for identifying malingerers. No attempt to
cross validate these findings, however, has been conducted to date.
The six features which comprise the Bender Gestalt malingering
index include the following: 1) Inhibited figure size: each figure
that was completely covered by a 1 1/4" X 1 1/4" square of paper
received a score of +1; 2) Changed position: each figure whose position
was changed while the form remained good was scored +1; 3) Distorted
relationship: each figure which contained correctly reproduced parts
that were misplaced in relationship to one another were scored +1; 4)
Complex additions: each figure that contained additional complex detail
was scored +1; 5) Gross simplifications: each figure that was grossly
simplified received a score of +1; and 6) Inconsistent form quality:
each test protocol that contained at least one grossly simplified and
one high level drawing was scored +1. These scoring criteria differ
from those used by Bash and Alpert in two details. First, whereas Bash
and Alpert (1980) added one criterion (number of designs recalled) to
those described by Bender, this was not scored in the present study
because the test was administered only once to my subjects. Second,
whereas Bash and Alpert used a 1" Xl" square of paper to score each
item for inhibited size, I used a 1 1/4" X 1 1/4" square of paper
because almost none of the subjects drew even a single figure smaller
that 1" Xl".

46
The third instrument employed used was the Malingering Scale
that was developed for this study (see Appendix C). It is a
pencil-and-paper test consisting of 90 items, and it requires about 20
minutes to complete. In content, it is similar to an intelligence test,
with subtest designed to assess the subject's general fund of knowledge,
arithmetic ability, vocabulary and abstract reasoning. The majority of
items are easy enough to be passed by any person of average
intelligence. The rationale for selecting specific items to be included
in the Malingering Scale was provided by Golstein (1945) who devised a
set of scoring keys to be used with the Army Visual Classification Test
for detecting inductees who tried to malinger "feeblemindedness." He
advised that a malingering scale should be characterized by, "1. a
liberal sprinkling of easy items; 2. items of varying degrees of
difficulty; 3. a scrambled sequence" (p. 118).
Two subtests of the Malingering Scale, Information and
Arithmetic, are administered verbally by the examiner, in much the same
way as the Wechsler Intelligence Scale subtests with the same names. In
fact, many of these items were drawn from the Wechsler scales. The
Vocabulary and Abstraction subtests may be completed without the aid of
an examiner. The items on these two scales are of the mUltiple choice
variety, but there are only two choices from which the subject selects
his answer for each item. On each scale the items are scored 0 or +1;
there are no time requirements, nor are bonus points given for speed.
After scoring the Malingering Scale protocols for a~l groups, a
series of chi squares were conducted to select those items which
maximally differentiated between subjects in the various conditions •
.... _---_.-----.. _ .. -.. _--_._---------------------

47
That is, the proportion of retarded subjects who passed each item was
compared with the proportion of subjects faking retardation who passed
each item. Those items which differentiated between the two groups with
a probability of .05 or less were assembled into the Malingering
Retardation (MgR) "key. " In the same way, items which significantly
differentiated between psychotic inpatients and subjects faking
"insanity" were assembled into the Malingering Insanity (MgI) "key."
The rationale for doing these analyses has been described by Hunt and
Older (1943) while the procedures have been described by Golc;lstein
(1945). Both are predicated on the finding that malingerers and
genuinely mentally deficient subjects produce different patterns of
inter-item scatter, that is, malingerers err in their judgements about
item difficulty. As a result, they tend to fail some of the items which
nearly all mentally deficient subjects pass, and pass some of the items
which nearly all of the mentally deficient subjects fail. It is these
items which comprise the MgI and MgR keys. The final MgI key consisted
of 39 items, while the final MgR key consisted of 24 items (specific
items are listed in Appendix D).
Each subject's total scores were obtained by summing the number
of correct responses on each subtest. Scores for the MgI and MgR keys
were calculated by summing the number of items answered in the direction
that signifies malingering. All scores were then entered as predictive
variables in a discriminant function analysis. This allowed for a
statistical comparison of each predictor variable's relative strength
for differentiating between the groups.

48
Hypotheses
First it was hypothesized that subjects faking either
retardation (Group III) or insanity (Group IV) would score significantly
higher on the F and F-K raw score indices of malingering on the MMPI
than genuine psychotics (Group II) or the inmate controls (Group V).
These comparisons were included as a replication and cross validation of
previous studies which have consistently found that subjects faking
"bad" or "poor adjustment" and so forth obtain scores on these MMPI
indices which are elevated above those produced by normal and mentally
disordered persons.
Second, it was hypothesized that malingering subjects would
obtain significantly higher scores on each of the "malingering criteria"
described for the Bender-Gestalt test than subjects in the other three
groups. This hypothesis was based on the finding of Bash and Alpert
(1980) that subjects suspected of malingering schizophrenia produced
more of these malingering features in their drawings than either
psychotic or non-psychotic control subjects.
Third, it was hypothesized that a discriminant function based on
scores derived from all three instruments (MMPI, Bender-Gestalt and
Malingering Scale) would yield a higher hit rate than any single test.
This was based on the findings of Bash and Alpert (1980) and Heaton, et
al. (1978) which indicated that test batteries were more effective for
identifying malingerers than any single test.
Fourth, it was hyposthesized that subjects faking mental
retardation would obtain scores on the Goldberg Psychoticism index that
are higher than those obtained by inmate controls. Similarly, it was

49
hypothesized that subjects faking "insanity" would obtain lower overall
scores on the Malingering Scale (an intelligence test) than the inmate
controls. Thes,e twin hypotheses were based on reports that subj ects
simulating emotional
unintelligent, while
disorders often present themselves as
those simulating mental deficiency often give
grossly illogical or bizarre responses on intelligence tests, apparently
due to their misconceptions about the nature of these disorders (Hunt &
Older, 1943; Wachspress, 1953).
CHAPTER III
RESULTS
Subject Characteristics
Efforts to match subjects were successful for all variables
except age. Chi square analysis revealed no significant association
between experimental condition and race, (12, N=100)=14.50, n.s.
Further, a series of one-way Anovas revealed no significant differences
between experimental groups (excluding retardates) on education,
F(3,76)=2.09, n.s., or on estimated IQ, F(3,76)=1.91, n.s. In comparing
the age of subjects across experimental conditions, a one-way Anova
revealed that efforts to match on age failed, F(4,95)=13.25, p <.01.
Demographic characteristics of the sample are shown in Table 3.
Instrumentation
As described previously, six dimensions of each Bender Gestalt
protocol were scored by two research assistants who were trained on a
set of 20 faked protocols obtained from college students, and who were
naive with regard to the nature of the study. With the exception of a
single dimension, "changed position," estimates of inter-rater
reliability were acceptably high. Pearson correlation coefficients,
calculated on the scores obtained from two ratings of 35 randomly
selected protocols, are presented in Table 4.
50

Table 3
Demographic Characteristics of Experimental Subjects
(Expressed in Group Means and Percentages)
Race
Condition Age Educ IQ Wht Hisp Blk Other
Control 31 10.5 101 65% 15% 10% 10%
Fake Retarded 24 11.7 103 60% 10% 20% 10%
Fake Insanity 33 12.2 108 75% 20% 5% 0
Actual Retarded 31 47 80% 20% 0 0
Psychotic 45 12.3 101 85% 5% 10% 0
Total 33 11.7 103 73% 14% 9% 4%
Mentally retarded subjects excluded from Educ.
51
-------------------- --- -- ----------

Table 4
Inter-Rater Reliability Estimates for
Six Aspects of Bender Gestalt Drawings
Scoring Pearson Correlation
Diminished Size .95
Changed Position .66
Distorted Relationship .71
Complex Additions .78
Gross Simplifications .93
Inconsistent Form Quality 74% agreement
52
._-------------------- ------- ----- ------------- ---

53
An intercorrelation matrix was also computed (using the entire
data set) in order to assess the degree of independence underlying these
dimensions of the Bender Gestalt. As shown in Table 5, with the
exception of Changed Position, which is highly correlated with
Diminished Size and with Distorted Relationship, the intercorrelations
are acceptably low. This finding suggests that all of the Bender
Gestalt indices except Changed Position measure reasonably distinct
aspects of a subject's drawings. Thus, all but Changed Position (which
also had the lowest inter-rater reliability) were retained for
subsequent analyses.
The Malingering Scale was subjected to a series of item analyses
in order to determine its psychometric characteristics. Data bearing on
its validity will be discussed below under "Maj or Findings." Of
importance here is the finding that all four subtests of the Malingering
Scale displayed remarkably high internal consistency. Using the Kuder
Richardson (formula 1120) method to assess internal consistency, the
following reliability estimates (based on N=100) were obtained:
Arithmetic, .97; Information, .95; Vocabulary, .92 and Abstraction, .88.
It was hypothesized that some items would prove to be
particularly effective in discriminating malingerers from genuinely
impaired subjects. In order to test this hypothesis, the percentage of
malingering psychotic versus genuinely psychotic subjects who correctly
answered each item were compared using chi square analyses. Those items
which discriminated between the groups with an associated probability of
p <.05 constituted the Malingering Insanity, or MgI key. This entire
process was then duplicated using scores obtained from the genuinely

54
Table 5
Intercorrelation Matrix of Bender Gestalt Scores
Changed Distorted Complex Grossly
Position Relationship Additions Simplified
Diminished Size .52 .37 .06 -.13
Changed Position .49 .34 .12
Distorted Relationship .24 -.17
Complex Additions -.05
p< .01

55
retarded and malingering retarded subjects. The latter comparisons
resulted in the development of the other scoring key, referred to as the
Malingering Retardation or MgR key.
The Malingering Insanity key consists of 39 items scored +1 for
each correct response. Lower scores suggest malingering. The
Malingering Retardation key consists of 24 items. On 16 of these items
correct responses are score +1; on the remaining 8 items, incorrect
responses are scored +1 (indicating that malingerers failed the item
more frequently than retardates). On this key, higher scores suggest
malingering. The exact items, and the direction in which they are
scored are listed in Appendix 1. Naturally, for clinical purposes, the
examiner may wish to sum the number of incorrect scores on the MgI key
so that high scores on both keys suggest faking and low scores on both
keys denote genuine pathology. A comparison of each group's performance
on these keys will be presented under "Major Findings."
Experimental Manipulations
The results show that subjects understood and followed the
instructions which they were given. Those instructed to fake "insanity"
produced marked elevations on every clinical scale (except Mf) of the
MMPI, including elevations on the Goldberg Psychoticism Index that
greatly exceeded those produced by the genuine psychotics. Group means
and standard deviations on the MMPI clinical scales are listed in
Appendix E. The means and standard deviations on the validity scales
and the Goldberg Psychoticism Index are presented in Table 6.

Table 6
Means and Standard Deviations (in Parentheses) on the MMPI
Validity Scales and on the Goldberg Psychoticism Index
Score Control Psychotic
L 52 (7.9) 49 (7.5)
F 74 (17.9) 86 (13.4)
F (raw) 13 (7.3) 19 (6.1)
K 53 (7.3) 47 (9.4)
K (raw) 14 (3.9) 10 (4.9)
F-K raw -1 (9.3) 9 (9.0)
Goldberg 69 (16.3) 71 (18.5)
Malinger
Retardation
58 (12.3)
112 (24.5)
28 (9.2)
53 (9.0)
14 (4.8)
14 (11.3)
100 (23.2)
Malinger
Insanity
54 (9.1)
128 (21. 6)
34 (8.5)
46 (8.0)
10 (4.2)
24 (9.5)
108 (32.7)
56

57
Similarly, subjects who were instucted to malinger retardation
succeeded in lowering their overall scores on the Malingering Scale
significantly below those of the control psychotic subjects. A
comparison of group performance is shown in Table 7. The control and
psychotic subjects answered nearly every item correctly, while retarded
subjects failed the majority of items. Malingerers performed at a level
intermediate between the retardates and the other subjects. These
findings indicate that the subjects who were instructed to malinger
mental retardation understood and complied with this response set. The
intermediate scores produced by subjects faking "insanity" tends to
support to the accumulation of anecdotal evidence that persons
malingering "insanity" are likely to erroneously assume that they should
present themselves as somewhat mentally deficient, as well.
Major Findings
A discriminant function analysis was executed in order to
determine how effectively the obtained test results would predict each
subj ect 's group membership. The specific procedure is described by
Klecka (1975) and was executed on a Cyber 65 computer at the University
of Arizona. The mathematical objective of discriminant analysis is to
weight and linearly combine a set of discriminating (predictive)
variables so that two or more groups of cases are forced to be as
statistically distinct as possible. In the present analysis, a total of
13 predictive variables were entered in a stepwise fashion according to
their discriminating power, as measured by each variable's contribution
to the overall separation of groups (Rao's V criterion). The use of

Table 7
Mean Number of Correct Responses on Each
Malingering Scale Subtest
Group Arith Info Vocab Abstract
Control 18.6
Psychotic 19.0
Fake Insanity 13.6
Retarded 2.4
Fake Retarded 7.8
21.0
22.7
15.3
7.0
9.8
25.5
25.8
18.1
16.6
15.8
19.4
19.0
15.5
15.8
12.5
Total
84.4
86.4
62.6
38.9
45.8
58

59
this procedure results in an optimal set of variables being selected.
The maximum number of discriminant functions that may be derived is
equal to one less than the number of groups, or a maximum of four in the
present study. These functions are derived in such a way that the first
functions separates the groups as much as possible. Then, each
subsequent function separates them as much as possible in an orthogonal
direction given the prior functions. Finally, the functions were
rotated according to the VARIMAX criterion to allow for an examination
of the standardized discriminant function coefficients. These
coefficients represent the relative contribution of each predictor to
that function.
The predictor variables entered into the analysis included the F
and F-K raw scores from the MMPI, the four subscales (Vocabulary,
Arithmetic, Information, Abstraction) as well as the MgI and MgR scores
from the Malingering Scale, and five of the Bender Gestalt malingering
features (Diminished size, Distorted relationship, Complex additions,
Gross simplifications, Inconsistent form quality). The data indicate
that eight test scores proved to be remarkably powerful predictors of
membership in the five groups. Each of these variables resulted in a
highly significant change in Rao' s V. Listed in descending order of
importance, they are as follows: 1) MgR score from the Malingering
Scale, 2) Gross Simplification of Bender drawings, 3) F-K raw score
difference on the MMPI, 4) MgI score from the Malingering Scale, 5)
Inconsistent Form Quality on Bender drawings, 6) Abstraction subtest of
the Malingering Scale, 7) Arithmetic subtest of the Malingering Scale,
and 8) Distorted Relationships on Bender drawings. The five remaining

60
scores entered into the discriminant analysis (F raw score from the
MMPI, Information and Vocabulary from the Malingering Scale as well as
Complex Additions and Diminished Size from the Bender Gestalt) made
trivial contributions to the predictive power of the first eight.
The five-group design used in this study allowed for the
computation of four discriminant functions. Table 8 and Table 9 present
information regarding the discriminating power and statistical
significance of these functions. The eigenvalue showen in Table 8 is a
measure of the relative importance of the function. The canonical
correlation squared may be interpreted as the proportion of variance in
the discriminant function explained by the groups. Table 9 shows the
changes in Wilk's lambda, and their associated chi-square tests, as the
information in successive discriminant functions is removed. As each
function is derived, starting with no (zero) functions, Wilk's lambda is
computed. Lambda is an inverse measure of the discriminating power in
the original variables which has not yet been removed by the
discriminant functions. Thus, the larger lambda is, the less
information remaining. As shown in the table, lambda can be transformed
into a chi-square statistic for a test of statistical significance.
Before any functions were removed, lambda was .0165, indicating that a
tremendous amount of discriminating power exists in the predictor
variables being used. In fact, (by using I-lambda to estimate eta) over
98% of the variance in grouping was accounted for by these eight
predictors •
.. - ---_._-_._------.----------- ------------------

Table 8
Discriminating Power of the Discriminant Functions
Function
1
2
3
4
Eigenvalue
7.9445
2.0917
.9153
.1477
Percent of
Variance
71.67
18.85
8.25
1.29
Table 9
Canonical
Correlation
.9424
.8225
.6913
.3541
Significance of the Discriminant Functions
After Wilks' Chi-
Function
o
1
2
3
Lambda
.0165
.1477
.4566
.8746
Square
379.58
176.91
72 .51
12.39
D.F.
32
21
12
5
Significance
p <.0001
p <.0001
p <.0001
p <.05
61

62
Another way of evaluating the discriminating power of the
obtained functions is to examine the classification results. These
results are presented in Table 10. It should be noted that, although
the "hit rate" for group membership was found to be 84% across all five
groups, the hit rate for making an accurate determination of faking vs
not faking is 96%. This estimate is easily calculated by adding the
number of not-faking subjects accurately identified as not-faking (60 or
100%) to the number, of faking subjects who were accurately indentified
as faking (36 -or 90%) and dividing this sum by the total number of
subjects (ie, 96/100).
Table 11 presents a listing of the standardized discriminant
function coefficients associated with each variable on all four
functions. The interpretation of these coefficients is analogous to
beta weights in multiple regression. Each coefficient represents the
relative contribution of its associated variable to that function, while
the sign merely denotes whether the variable made a positive or negative
contribution. Thus, inspection of Table 11 reveals that the four test
scores: Gross Simplification, MgR, F-K and Inconsistent Form Quality
contribute most to the predictive power of Function 1. Most heavily
weighted on Function 2 were the scores: MgI, Arithmetic and MgR, all
three of which are derived from the Malingering Scale. On Functions 3
and 4, most variables loaded quite heavily; however, these two functions
contribute less than ten percent of the total explained variance.

Table 10
Discriminant Function Analysis Classification Results
Predicted Group Membership
Fake
63
Actual
Group
No. of
Cases
Fake
Control Insane Psychotic Retarded Retarded
Control
Fake Insanity
Psychotic
Fake Retarded
Retarded
20
20
20
20
20
17 0
o 14
4 0
1 1
o 0
300
240
16 0 0
1 17 0
o 0 20

64
Table 11
Standardized Discriminant Function Coefficients
Predictor Variable Func 1 Func 2 Func 3 Func 4
F-K raw score .4906 -.2970 .6179 .5330
Arithmetic subtest .1043 .5898 1.2389 -.7326
Abstraction subtest -.4034 -.1049 .3586 -.9026
Distorted Relation -.1737 .0795 .5256 .1468
Gross Simplification -.8224 .0653 .1814 -.1577
Inconsistent Quality .4601 -.0166 -.6364 .4352
MgI scoring key .1363 .7696 -.7346 1.5803
MgR scoring key .6130 -.5868 -.6967 -.3657

65
Finally, a description of the discriminant functions evaluated
at the group means is presented in Table 12. By averaging the scores
for cases within a particular group, one arrives at the group mean on
the respective function. For a single group, the means on all the
functions are referred to as the group centroid, which is the most
typical location of a case from that grou.p in the discriminant function
space. A comparison of the group means of each function tells how far
apart the groups are along that dimension. As shown in Table 12,
Function 1 sharply distinguishes mentally retarded subjects from the
other four groups, but it also distinguishes quite well between control
subjects and the other four groups. Function 2 appears to provide
considerable separation between all of the groups, with the exception
that it does not distinguish between control and psychotic subjects.
Function 3 appears to chiefly differentiate subjects faking "insanity"
from the others, while Function 4 seems to chiefly separate genuinely
psychotic subjects from the other four groups.
Tests of Specific Hypotheses
It was first hypothesized that subjects in the two malingering
conditions would obtain significantly higher scores on the F and F-K
indices than genuine psychotics and the inmate controls (recall that the
mentally retarded subjects did not take the MMPI). To test these
hypotheses, a series of planned comparisons using one-way analyses of
variance (ANOVA). Specifically, the first planned contrast compared the
F raw scores of subjects in the two malingering conditions with subjects
in the control and genuine psychotic groups. This contrast indicated

Table 12
Discriminant Functions Evaluated at Group Means (Centroids)
Group Funct 1 Funct 2 Funct 3 Funct 4
Fake Insanity
Control
Fake Retarded
Retarded
Psychotic
1.82
.75
1.26
-5.45
1.62
-1.02
1.57
-1.99
-.12
1.56
1.57
-.58
-1.23
.18
.06
-.16
-.56
.09
.06
.57
..... -.-._ ......... _ ........ ~----.---... -----------------
66

67
that malingerers did obtain significantly higher F raw scores than the
non-malingerers, F(1,76)=9.39, p < .01. The same procedure applied to
the F-K raw scores also indicated that malingerers obtained higher
scores on this index than did non-malingerers, F (1,76)=6.83, p < .05.
Next it was hypothesized that subj ects in the two malingering
conditions would produce significantly higher scores on each of the six
"malingering criteria" for the Bender Gestalt. To test these hypotheses
a series of six planned comparisons using one-way ANOVAs contrasted the
scores of subjects in the two malingering groups with the scores of
subj ects in the other three conditions. Three of these, involving
scores on Diminished Size, Changed Position and Complex Additions,
revealed no significant differences between malingering and
non-malingering subjects. A surprising finding was that the malingering
subjects scored significantly lower than non-malingering subjects on two
Bender criteria, namely Gross Simplification F(I,95)=30.88, p <.01 and
Distorted Relationship F(I,95)=6.56, p < .05. On the final Bender
criterion, Inconsistent Form Quality, each subject's protocol is scored
either +1 or O. Therefore the planned comparison in this case was based
on a chi-square statistic, using Yates correction, which revealed no
significant association between experimental condition (malingering vs.
non-malingering) and scores of Inconsistent Form Quality,
(1, N=100)=0.52. The group means and standard deviations on which these
analyses were based are shown in Table 13.
Third, it was hypothesized that a discriminant analysis based on
scores derived from all three instruments (MMPI, Bender Gestalt and
Malingering Scale) would yield a higher hit rate than any single test.
--------------------------------- ----_._-----_ ...

68
This hypothesis was evaluated by means of a series of discriminant
analyses that predicted group membership by using subsets of the
predictor variables that were used in the previously described analysis.
As in the previous analysis, predictor variables were entered in
stepwise fashion and the derived functions were rotated according to the
VARIMAX criterion. The results showed that use of the test battery
provided more predictive power than any single instrument. It was also
shown that the Malingering Scale was superior to the other malingering
indices. These results are summarized in Table 14.
Finally, it was hypothesized that subjects faking retardation
would obtain scores on the Goldberg Psychoticism Index that are higher
than those obtained by inmate controls. As shown in Table 6, subjects
malingering mental retardation produced significantly higher scores on
the Psychoticism Index than inmate controls, when this difference was
evaluated by a one-tailed ! test for independent groups (p < .001).
Conversely, it was hypothesized that subjects faking "insanity" would
obtain lower total scores on the Malingering Scale (an intelligence
test) than the inmate controls. This hypothesis was tested by means of
a one-tailed t test for independent groups. This analysis revealed that
subj ects malingering "insanity" did score significantly lower than the
inmate controls. (p <.001).
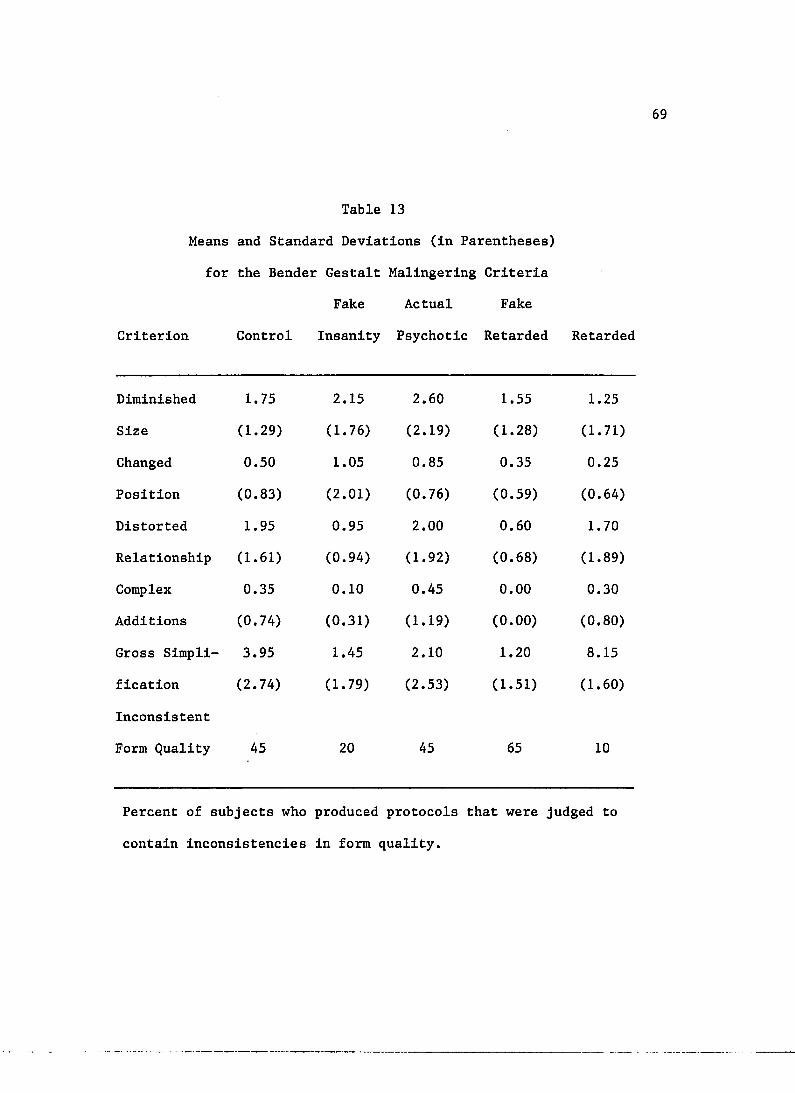
Table 13
Means and Standard Deviations (in Parentheses)
for the Bender Gestalt Malingering Criteria
Fake Actual Fake
Criterion Control Insanity Psychotic Retarded Retarded
Diminished 1. 75 2.15 2.60 1.55 1.25
Size (1.29) (1.76) (2.19) (1. 28) (1.71)
Changed 0.50 1.05 0.85 0.35 0.25
Position (0.83) (2.01) (0.76) (0.59) (0.64)
Distorted 1.95 0.95 2.00 0.60 1. 70
Relationship (1.61) (0.94) (1.92) (0.68) (1.89)
Complex 0.35 0.10 0.45 0.00 0.30
Additions (0.74) (0.31) (1.19) (0.00) (0.80)
Gross Simpli- 3.95 1.45 2.10 1.20 8.15
fication (2.74) (1.79) (2.53) (1.51) (1.60)
Inconsistent
Form Quality 45 20 45 65 10
Percent of subjects who produced protocols that were judged to
contain inconsistencies in form quality.
. _ .. __ ... _--_._- .•... -.-._-------_ .•. _---------------
69

70
Table 14
Comparison of Hit Rates (Percent of Group Correctly Classified) for
Discriminant Analyses Based on Individual Tests Versus the Test Battery
Discriminant Function Analysis
Group
Control
Fake Insanity
Psychotic
Fake Retarded
Retarded
Overall Hit Rate
Restricted
Hit Rate
MMPI
F raw
65
70
50
20
NA
41
76
MMPI
F-K raw
65
75
35
20
NA
39
74
Bender
Gestalt
60
30
30
60
100
36
74
Malingering
Scale
55
40
75
70
95
48
89
Entire
Battery
85
70
80
85
100
84
96
Summed percent of subjects in malingering conditions who were correctly
classified as malingering and subjects in non-malingering conditions
correctly classified as not malingering.
- -- -------------- ----------------------------------- - --- - --- -

CHAPTER IV
DISCUSSION
The present study provides compelling support for the hypothesis
that a battery of psychological tests permits the identification of
subjects faking either "insanity" or mental retardation with greater
accuracy than any single test. This finding is consistent with (and
augments) previous reports that a battery of tests is more accurate than
a single test for identifying subjects suspected of faking schizophrenia
(Bash & Alpert, 1980) and subjects instructed to fake neurological
deficits (Heaton, et al., 1978). The battery used in this study
classified subjects into each of five groups with 84% accuracy, nearly
twice the accuracy shown by the most effective single test, the
Malingering Scale, which produced a hit rate of 48%. When the
determination is restricted to the discrimination of faking versus
not-faking, the battery accurately classified 96% of the cases. This
increase in accuracy obtains from the fact that some subjects faking one
disorder produced results which resembled those produced by subjects
faking another disorder. For example, the test battery precisely
identified 70% of the subjects who faked "insanity;" it identified
another 20% of these subj ects as faking the other condition, mental
retardation. Similarly, the battery identified 85% of the subjects
faking retardation with complete accuracy; it identified another 5% of
them as faking "insanity." The same principle applies to the single
71

72
test predictors, and the increase in accuracy for each is shown in Table
14, where it is referred to as the "restricted hit rate."
Of the single tests, the Malingering Scale proved to be most
effective overall, the most effective for differentiating subjects
faking retardation from genuine retardates, and the most accurate for
identifying genuine psychotics. However, for differntiating subjects
faking "insanity" from genuine psychotics, the F raw score was superior.
The F raw score was also superior to the F-K raw score index.
This finding may seem peculiar since the F-K index was introduced as an
improvement over the F raw score, yet a close examination of Table 1
reveals that Anthony (1971), Gough (1947) and Grow, et a1. (1980)
obtained similar results. Sepcifically, these investigators found the F
raw score superior to the F-K index for differentiating malingerers from
genuinely impaired subjects, while the reverse was true for
differentiating malingerers from control subjects. For the sake of
comparison with previous research, it as found that Hunt's (1948)
recommended F-K cutoff score of +11 produced a hit rate of 90% for
subjects faking "insanity" in the present study, although the associated
false positive rates for psychotics and controls (misidentified as
faking) were 40% and 15% respectively. Alternatively, the optimal F-K
cutoff score was found to be +15, which accurately identified 80% of the
subjects faking "insanity" with associated false positive rates of 15%
for genuine psychotics and 0% for inmate controls.
In the present study an F raw score of +27 proved to be the
optimal cutoff score for differentiating subjects faking "insanity" from
genuine psychotics. Scores of 27 or greater correctly identified 80% of

73
the subj ects faking "insanity," with 15% false positives. This cutoff
score is nearly identical to that obtained by Gough (1947), who found
that an F raw score of +26 or more differentiated 73% of his malingerers
from genuine psychotics (no false positive rate was reported). This
similarity is not surprising. Nor is it surprising that the F and F-K
raw score indices proved to be somewhat less effective in the present
study than in many previous studies. As noted earlier, inspection of
Table 1 reveals that it is far more difficult to differentiate
malingerers from genuinely impaired subjects than from normal controls.
One explanation for these findings is the possibility that, by reducing
analog factors in the experimental design, one makes it more difficult
to differentiate malingering from non-malingering subjects.
Reducing analog factors could make such a differentiation more
difficult in several ways. First, it is likely that the prison inmate
population includes a greater proportion of persons with antisocial
personality disorder, who are more skilled at deception, and therefore
more difficult to identify, than the general population.
Second, it is also possible that, despite our efforts to screen
out psychotics from among the inmates who agreed to participate in the
study, some of the inmate controls may well have suffered from severe
psychiatric impairments. In fact, none of the inmates who consented to
be in the study were found to carry the diagnosis of a psychotic
disorder at the time of his participation. However, it was found that
the test battery "misclassified" three inmate controls as psychotic;
only two subjects faking "insanity" were similarly misclassified. As
shown in Table 6, it was also found that the inmate controls obtained a

74
mean score of 69 on ther Goldberg Psychoticism Index, well above the
cut-off score for a diagnosis of psychosis. Clearly, the inclusion of
psychotic subjects in the control group would reduce the apparent
accuracy of a diagnostic test, even one with "perfect validity."
Third, it is entirely possible that some of the genuine
psychotics may have exaggerated their symptoms, or conversely, not have
been psychotic at all. Suspicion of the latter is raised by the fact
that 20% of the genuine psychotics were classified as control subjects
by the discriminant analysis based on the test battery; none of the
genuine psychotics were misclassified as malingering. The inclusion of
nonpsychotic subj ects or malingerers in the genuine psychotic group
would also compromise the apparent accuracy of any diagnostic test, even
one with "perfect validity."
Fourth, the present study offered a real, monetary incentive for
successful, non-detected simulation of the stipulated condition. Prison
inmates at the facility used in this study were able to earn no more
than $1.60 per day working in the prison. Therefore, the prospect of
obtaining $15.00 by successfully faking mental retardation or "insanity"
was found to represent a powerful incentive, as evidenced by the
inmates' remarks to this effect. Such a powerful incentive, combined
with the explicit statement that only non-detected malingering would be
rewarded, might reasonably be expected to assure that the malingering
subjects would exert greater efforts to conceal their deception than
subjects not provided with these conditions, and thereby make their
detection more difficult.

75
One strength of the present study is that most analog factors
were eliminated from the experimental design. Several previous studies
have limited the reliance on analog factors by using genuinely impaired
subjects in comparison groups (e.g., Anthony, 1971; Gough, 1947; and
Pollaczek, 1952). Others have used subjects actually suspected of
malingering (Bash & Alpert, 1980) or drawn subjects for their
malingering group from a clinically relevant population, such as prison
inmates (Gendreasu, et al., 1973). However, very few have combined more
than one of these strategies to limit analog factors, and none have
offered a real incentive for successful, non-detected faking to the
subjects who were instructed to malinger. Consequently, the design
employed in the present study allows for maximal generalizability of
findings. Such generalization extends to those clinical situations in
which a criminal defendant, pleading Incompetent to Stand Trial or Not
Guilty by Reason of Insanity, is suspected of malingering "insanity" or
mental retardation.
The present study explicitly addressed the question of which
tests would be most effective for identifying each malingered condition.
Examination of the standardized discriminant function coefficients
(Table 11) together with the discriminant function group means (Table
12) serves to answer this question. For example, examination of
Function 1 reveals that the absence of Gross Simplifications on Bender
drawings and elevated MgR scores on the Malingering Scale were
particularly useful for identifying subjects who faked retardation.
Examination of the standardized coefficients and group means for
Function 2 shows that depressed MgI, MgR and Arithmetic scores on the
. -.- - -- -.-.. --. ---_._._---- _ .. _.-._-------------- -~----------------

76
Malingering Scale were particularly useful for identifying subjects who
faked "insanity." On every function it can be seen that elevations on
the F-K raw score index are modestly predictive of subj ects who faked
either condition.
The present study also produced some evidence in support of the
hypotheses that subjects instructed to fake "insanity" would present
themselves as unintelligent, while those instructed to fake mental
retardation would present themselves as emotionally disturbed.
Specifically, subjects who faked "insanity" obtained significantly lower
total scores on the Malingering Scale than controls, while subjects who
faked retardation obtained significantly higher scores on the Goldberg
Psychoticism Index of the MMPI than inmate controls. These findings are
consistent with previous reports that subjects faking mental deficiency
may produce bizarre responses to test questions (Hunt & Older, 1943),
while subjects suspected of faking psychotic disorders may present
themselves as unintelligent (Wachspress, et al., 1953).
The present study revealed that three aspects of Bender Gestalt
drawings, namely: Gross Simplifications, Inconsistent Form Quality and
Distorted Relationships made significant contributions to the test
battery's discrimination of malingerers from non-malingerers. However,
close examination of Table 13 indicates that the data directly
contradict Bender's (1938) original assertion. Subjects in both
malingering conditions produced fewer --- instances of Distorted
Relationships and of Gross Simplification than the controls or the
genuinely impaired subjects. Mentally retarded subjects produced the
fewest instances of Inconsistent Form Quality, principally because very
-- .. -.------.---------------------------------~--

77
few of these subjects were able to produce even one "high level"
drawing, which is necessary to score for inconsistency in the protocol.
The highest proportion of protocols characterized by inconsistency in
form quality was observed in the drawings of subjects faking
retardation. This is not surprising; it reflects their efforts to
simplify the drawings as they thought a retarded person might. It also
reflects the difficulty of consistently accomplishing this. Further, it
was shown that subjects who faked "insanity" evidenced Inconsistent Form
Quality less than half as often as genuine psychotics or inmate
controls. Thus, while several Bender scores made significant
·contributions to the overall predictive power of the discriminant
analysis, the precise manner in which they proved useful did not support
Bender's original observations.
The question arises as to whether the use of a single test,
especially given prior awareness of an individual's clinical
presentation, may be more efficient than the use of an entire test
battery for making the determination of malingering. As shown in Table
14, the Malingering Scale is clearly superior to any other single test
in terms of overall hit rate, and especially for differentiating between
genuine and faked retardation. Further, the MMPI F raw score appears to
be slightly better than the Malingering Scale for differentiating
between genuine psychosis and faked "insanity. " Comparison of the
restricted hit rates for each single test and the battery, as shown in
Table 14, also indicates that the Malingering Scale, by itself, is
nearly as effective as the complete battery.

78
I believe that there are compelling reasons to use the battery,
rather than an abbreviated subset of tests. First, administration and
scoring of the Malingering Scale takes no more than 15 minutes of the
examiner's time, while the Bender Gestalt and MMPI require even less,
and all three may be administered by a technician. In short, very
little saving of time accrues to the elimination of any individual test,
so that even marginal increases in diagnostic accuracy justify using the
battery as a whole. But use of the entire battery yields far more than
marginal increases in diagnostic accuracy. Examination of Table 14
shows that, although use of the battery only increased the restricted
hit rate by 7% over that produced by the Malingering Scale alone (from
89% to 96%), it increased the overall hit rate by 38% (from 48% to 84%).
This finding indicates that only the entire battery permits the
clinician to draw accurate conclusions about the exact diagnostic
category to which a given subject belongs. This is to be expected; the
discriminant function analysis, by definition, combines the various test
scores in a manner which maximizes their predictive power.
A limitation of the present study is worthy of mention. As
noted in the results, our efforts to match subjects were successful on
all demographic variables except age. Psychotic inpatients drawn from
the Tucson VAMC were found to be significantly older than subjects in
the other four conditions. Since this represents a possible source of
confound, it is recommended that future research, especially research
designed to cross validate the Malingering Scale or the test battery
used in the present study, take precautions to insure careful matching
for age.
--_. __ . __ ._--- .. _.--------------------------------

79
Finally, several leads for future research emerge from the
present study. First, it should be emphasized that the Malingering
Scale developed for this validation study shows promise as a clinical
and research instrument. However, clinical use of this test, alone or
in conjunction with the other instruments which comprise the complete
battery, cannot be justified until it has been cross validated. Cross
validation might be undertaken with a variety of related populations.
In the present study, for example, the subjects who received
instructions to fake either mental retardation or "insanity" were not
provided with any information about how persons with these conditions
present clinically. It is possible that better informed subjects would
evade detection with greater success. In order to test this hypothesis
it would be necessary to select subjects for malingering conditions from
a clinically sophisticated population, such as mental health
professionals, or to provide less clinically sophisticated subjects with
information about the clinical presentation of persons suffering from
the malingered conditions.
Using a similar design and similar experimental incentives to
that employed in this study, subjects malingering various mental
disorders might be drawn from hospital patients, Army recruits, college
students, as well as prison inmates, and compared with genuinely
impaired subj ects from comparable populations. As data from further
research accumulates, they should lead to the development of robust
equations for differentiating between persons with genuine psychiatric
impairment and those making fraudulent claims of illness for some
desired end.
- - _._ ... - .... - -_._. --_. __ ._---- ._._---_._--_._---------------------

Appendix A
Group I Subject's Consent (Mentally Retarded)
I understand that David J. Schretlen would like to invite my ward,
80
to participate as a subject in an experiment being conducted to devise and validate a psychological test of intelligence. I understand that each subject will be asked to complete two psychological tests which. will require between 45 minutes to one hour of time, and that each subject will be paid $2.00 upon completion of the tests. I have also been informed that the principal investigator will require the following information about each subject: age, education, occupation, ethnic background, and medications being taken and psychiatric diagnoses, if any.
I understand that each subject's participation in this study is entirely voluntary, and that he may withdraw at any time. I understand that there are no foreseeable risks associated with participating in the study, and that all information gathered in the course of this research will be kept confidential, will be coded by number rather than name, and will be stored in a locked cabinet in the Psychology Clinic at the University of Arizona. I understand that each subject's participation will not in any way affect his treatment at any institution of the Department of Economic Security.
As the legal guardian of , I hereby give my consent that he be invited to participate as a subj ect in the experiment described above.
Guardian's Signature
David J. Schretlen, M.A. Principal Investigator
Date
Date
... _ ...•......... ------.-- .... -.-.-------~---.---------------

Group II Subject's Consent (Psychotic Inpatient)
81
You are invited to participate in an experiment that is being conducted in order to collect information about how different types of people answer a recently-developed psychological test. Your participation is voluntary, and you are free to withdraw from the study at any time.
The principal investigator will need to obtain certain information from your file, including your age, race, occupation, and highest grade of school completed. However, any information gathered in the course of this study will be kept strictly confidential. Your participation in this study will not in any way affect your treatment at this institution. Neither your identity nor your test responses will be made available to any person other than the principal investigator. All information gathered in the course of this study will be coded by number, rather than by name, and will be stored in a locked file in the Psychology clinic at the University of Arizona.
You will be asked to take two psychological tests which require approximately 10-15 minutes each, for a total of 20-30 minutes of your time. There are no foreseeable risks associated with participating in this experiment. Should you decide to participate, you will be making a contribution to our understanding of human behavior that will be greatly appreciated. Although you will not be given feedback about your test results, you may obtain information about the results of the study once it is completed, if you wish.
I understand what my participation in this study involves, and understand that I am free to withdraw from the project at any time. I am aware that my test results will be kept confidential, and give permission to the principal investigator to examine my life for the specified information. I hereby volunteer to participate in the study.
Subject's Signature
Witness' Signature
David J. Schretlen, M.A. Principal Investigator
Date
Date
._._-_ .. _-----_._--------_._-------------------------

82
Group III & IV Subject's Consent (Malinger Mental Retardation and Insanity, respectively)
This study will attempt to find out whether or not we can detect people who are trying to fake mental retardation (insanity). You will be given some psychological tests, and you are to answer them the way that you think a mentally retarded (insane) person would. The tests will require about two hours to complete. A doctor will compare your tests results with those given by truly retarded (insane) people. If you can give test results that look like those of a mentally retarded (insane) person, without being detected, you will receive $15. If you are detected, you will receive only $2.
* * * * * * * * * I understand what my participation in this study involves, and understand that I am free to withdraw from the study at any time, but will be paid only if I complete the tests. I am aware that my test results will be kept confidential, and give my permission to the principal investigator to examine my file for the following information: age, race, years of school completed, occupation, the results of any previous psychological testing since the time of my admission to the Department of Corrections, and present psychiatric diagnoses, if any. I hereby volunteer to participate in the study.
Subject's Signature
Witness' Signature
David J. Schretlen, M.A. Principal Investigator
Date
Date

Group V Subject's Consent (Inmate Controls)
83
You are invited to participate in a psychological experiment that is being conducted to collect information about how different types of people answer a recently-developed psychological test. Your participation is voluntary, and you are free to withdraw from the study at any time, although you must complete the testing to be eligible for payment.
The principal investigator will need to obtain certain information from your file, including your age, race, years of school completed, current psychiatric diagnoses, if any, and the results of any previous testing since the time of your present admission to the Department of Corrections. However, any information gathered in the course of this study will be kept confidential. Your participation in this study will not in any way affect your treatment at this institution. Neither your identity nor your test results will be made available to any person other than the principal investigator. All information gathered in the course of this study will be coded by number, rather than by name, and will be stored in a locked file in the Psychology Clinic at the University of Arizona.
In this study you will be asked to take some psychological tests so that we can learn more about the particular difficulties experienced by prison inmates. The test will require about 2 hours to complete. You are simply asked to answer test questions honestly and to the best of your ability. At the end of testing, you will be paid $2.00.
I understand what my participation in this study involves, and understand that I am free to withdraw from the project at any time. I am aware that my test results will be kept confidential, and give my permission to the principal investigator to examine my file for the specified information. I hereby volunteer to participate in the study.
Subject's Signature
Witness' Signature
David J. Schretlen, M.A. Principal Investigator
Date
Date
-----------------------~--------------

84
Appendix B
Instructions read to subjects in Groups III and IV
In this experiment you will be taking some psychological tests. But we do not want you to take them in the usual way. Instead, we want you to pretend that you are "insane" (mentally retarded), that is, crazy (very dumb). In other words, you are to answer the test questions in the way that you think an "insane" (mentally retarded) person would. If you can produce test results that look like those of an "insane" (mentally retarded) person, without being caught, you will receive $15. But if you are caught, you will receive nothing. It is like a game. We expect that you have about one chance in five of not being caught. However, it is possible for everyone to get $15 if nobody gets caught.
It may be helpful for you to think of your job this way: Pretend that you have committed a felony, and that you want to avoid trial or conviction by faking "insanity" (mental retardation). That is, you have decided to plead Incompetent to Stand Trial or Not Guilty by Reason of Insanity. A psychologist is going to evaluate you with some psychological tests. You should respond in the way that you think a person suffering from "insanity" (mental retardation) would. If you can convince the doctor that you are too "insane" (mentally retarded) to be tried or convicted for your crime, then you will not have to do time in jail. Since you do not want to go to jail, you are to answer the test questions in the way that you think an "insane" 'tmentally retarded) person might.

Appendix C
Malingering Scale
Arithmetic
1. A woman has two pairs of shoes. How many shoes does she have altogether?
2. How much is 50 cents plus one dollar? 3. If you have three books and give one away, how
many will you have left? 4. If you have 18 dollars and spend seven dollars
and 50 cents, how much will you have left? 5. How much is 20 cents plus five cents? 6. A boy had 12 newspapers and he sold 5 of them.
How many did he have left? 7. How much is four dollars plus five dollars? 8. If I cut an apple in half, how many pieces will
I have? 9. Raffle tickets cost 25 cents each. How much will
6 tickets cost? 10. If you buy six dollars worth of gasoline, and pay
for it with a 10 dollar bill, hou much change should you get back?
11. How many hours will it take a person to walk 24 miles at the rate of three miles per hour?
12. A girl had one dollar in change. She lost 50 cents. How much did she have left?
13. How much does three times nine equal? 14. How much does 10 minus five equal? 15. How much does one plus one plus three equal? 16. How much does six divided by three equal? 17. How much does seven plus four equal? 18. How much does one times eight equal? 19. How much does 19 minus five equal? 20. How much is six divided by three?
85
Score ---

Malingering Scale
Information
1. What are the colors in the American flag? 2. How many months are there in a year? 3. How many things make a dozen? 4. What must you do to make water boil? 5. Who discovered America? 6. How many pennies make a nickel? 7. From what animal do we get bacon? 8. Why does oil float on water? 9. What is the capital of Italy? 10. What is a thermometer? 11. How many days make a week? 12. Where does the sun rise? 13. Name the two countries that border the
United States? 14. Who wrote Hamlet? 15. Name the four seasons of the year? 16. Who invented the electric light bulb? 17. Name the month that comes next after March? 18. What does the stomach do? 19. What is the shape of a ball? 20. In what direction would you travel if you
went from Chicago to Panama? 21. How many weeks are there in a year? 22. Who runs a courtroom? 23. Who was president of the United States
during the Civil War? 24. How many legs does a dog have?
86
Score

87
Malingering Scale
Vocabulary
Underline the word that means the same thing as the word in CAPITAL letters.
LAW book rule
Score
1. PENNY money candy --2. STEP write walk 3. STREET road path --4. SAUCER spoon dish 5. COUCH sofa glass 6. FABRIC cloth shirt 7. ENORMOUS huge gentle --8. FIDDLE story violin --9. REMEMBER recall number --10. EVIDENT separate obvious 11. RAT coat cap --12. DONKEY dreadful mule 13. THIEF robber driver --14. REPAIR fix rest 15. TUMBLE dress fall --16. FURIOUS angry noisy 17. SHIP jump boat --18. MANY several coins 19. FRY cook eat --20. APPLE fruit berry 21. PARDON divide forgive --22. IMMUNE diseased protected 23. TALK speak sleep --24. GAMBLE join bet 25. DIAMOND follow jewel 26. LIKE new same

88
Malingering Scale
Abstraction
Circle the answer that should go in the blank ( --) space.
Score
1. A B C D R --2. 1 2 3 5 4
3. SCAPE CAPE APE CA PE --4. North South East Winter West
5. A AB ABC DEF ABCD
6. 65/56 24/42 73/ 37 10 --7. Mouth/eat Eye/see Hand/ smell touch --8. AB AC AD AE BC
9. Over/under In/out Above/ below behind -- --10. Al B2 C3 E5 D4
11. White/black Fast/slow UP/ __ side down --12. Bus Car Ship Table Truck
13. 2 4 6 5 8
14. Red Blue Green Yellow Chair
15. Monday Friday Sunday March Tuesday --16. 5 10 15 50 20
17. Candy/bar In/side Light/ __ bulb ball --18. Dog Bird Cat Tree Horse
19. Bread Fruit Meat Cheese Fork
20. * ** *** **** *
_.- _ .... -----..... -------.. ----.-~-----------------

Appendix D
Malingering Scale Scoring Key for Subjects Faking "Insanity" (MgI)
Sum the correct scores for all of the following:
ARITHMETIC ITEMS: 1, 9, 10, 11, 15, 16, 18
INFORMATION ITEMS: 3, 7, 8, 9, 10, 12, 13, 16, 18, 20, 22, 23, 24
VOCABULARY ITEMS: 3, 4, 6, 8, 9, 10, 11, 12, 14, 16, 18, 19, 20, 21, 22, 25
ABSTRACTION ITEMS: 15, 18, 19
Malingering Scale Scoring Key for Subjects Faking Mental Retardation (MgR)
Sum the correct and incorrect scores (as indicated) for all of the following:
ARITHMETIC ITEMS (Correct): 2, 5, 6, 7, 14, 17, 18
INFORMATION ITEMS (Correct): 2, 11, 15, 18 (Incorrect): 1, 4, 7, 17, 23
VOCABULARY ITEMS (Correct): 5, 7, 23 (Incorrect): 11
ABSTRACTION ITEMS (Correct): 8, 17 (Incorrect): 5, 10
89

90
Appendix E
Means and Standard Deviations (in Parentheses) of Each
Group on the Nine Clinical Scales of the MMPI
Experimental Condition
MMPI Malinger Malinger Genuine
Scale Control Retardation Insanity Psychotic
Hs 59.8 78.2 80.0 73.0 (13.5) (15.0) (15.5) (20.4)
D 60.1 73.2 78.5 82.0 (12.3) (14.5) (12.4) (29.3)
Hy 56.4 65.2 68.9 69.7 (8.4) (15.3) (11. 9) (14.5)
Pd 72.0 74.2 81.7 80.4 (8.8) (13.9) (12.0) (10.5)
Mf 60.9 70.7 66.7 65.1 (7.1) (9.1) (8.5) (12.1)
Pa 64.6 80.3 93.2 77 .9 (11. 2) (12.9) (16.7) (14.5)
Pt 65.5 79.8 86.6 84.1 (14.4) (15.4) (27.3) (19.5)
Sc 72.9 106.2 116.5 97.0 (18.8) (18.9) (19.1) (18.9)
Ma 67.9 73.8 79.4 73.2 (8.5) (14.1) (12.5) (28.0)

REFERENCES
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). Washington, DC: Author.
Anderson, E.W., Trethowan, W.R. & Kenna, J.C. (1956). An experimental approach to the problem of simulation in mental disorder. Proceedings of the Royal Society of Medicine, 49, 513-520.
Anthony, N. (1971). Comparison of clients' standard, exaggerated, and matching MMPI profiles. Journal of Clinical Psychology, 36, 100-103.
Asher, R. (1951). Munchausen's syndrome. Lancet,!, 339-341.
Bash, I.Y. &, Alpert, M. (1980). The determination of malingering. Annals of the New York Academy of Sciences, "':347, 86-99.
" ... ~" ",
Bender, L. (1938). A visual motor gestalt test and its clinical use. New York: The Orthopsychiatric Association.
Bleuler, E.P. (1951). Textbook of psychiatry (A.A. Brill, Ed. and Trans.) • New York: The Macmillan Company. (Original work published 1924).
Bruhn, A.R. & Reed, M.R. (1975). Simulation of brain damage on the Bender-Gestalt test by college students. Journal of Personality Assessment, 39, 244-255.
Cofer, C.N., Chance, J. & Judson, A.J. (1949). A Study of malingering on the Minnesota Multiphasic Personality Inventory. The Journal of Psychology, 27, 491-499.
Crowley, M.E. (1952). malingering.
The use of the Kent EGY for the detection of Journal of Clinical Psychology, ~, 332-337.
Dahlstrom, W.G., Welsh, G.S. & Dahlstrom, L.E. An MMPI handbookvolume 1: clinical interpretation (rev. ed.) Minneapolis: University of Minnesota Press.
Davidson, R.A. (1965). Forensic psychiatry (2nd ed.). New York: The Ronald Press Company.
Eissler, K.R. (1951). Malingering. In G.B. Wilbur & W. Muenstenberger (Eds.), Psychoanalysis and culture. New York: International Universities Press.
91

92
Exner, J.E., McDowell, E., Pabst, J., Stackman, W. & Kirk, L. (1963). On the detection of willful falsifications of the MMPI. Journal of Consulting Psychology, 27, 91-94.
Flicker, D.J. (1956). Malingering - a symptom. Journal of Nervous and Mental Diseases, 123, 23-31.
Garner, J.R. (1939). Malingering. American Journal of Jurisprudence, 1, 173-177.
Goldberg, L.R. (1965). Diagnosticians vs. diagnostic signs: diagnosis of psychosis vs. Neurosis from Psychological Monographs, 79(9, Whole No. 602).
Goldstein, H. (1~45). A malingering key for mental tests. Psychological ilulletin, 42, 215-255.
The the MMPI.
Gough, H.G. (1946). Personality 23-37.
Diagnostic patterns on the Minnesota Multiphasic Inventory. Journal of Clinical Psychology, 1,
Gough, H.G. (1947). Simulated patterns on the Minnesota Multiphasic Personality Inventory. Journal of Abnormal and Social Psychology, 42, 215-255.
Gough, H.G. (1950). The F minus K dissimulation index for the Minnesota Multiphasic Personality Inventory. Journal of Consulting Psychology, 14, 154-156.
Gough, H.G. (1954). Some common misconceptions about neuroticism. Journal of Consulting Psychology, ~, 287-292.
Grow, R., McVaugh, W. & Eno, T. (1980). Faking and the MMPI. Journal of Clinical Psychology, 36, 910-917.
Harvey, M.A. & Sipprelle, C.N. (1976). Demand characteristic effects on the subtle and obvious subscales of the MMPI. Journal of Personality Assessment, 40, 539-544.
Heaton, R.K., Smith, H.H., Lehman, R.A. & Vogt, A.T. (1978). Prospects for faking believable deficits on neuropsychological testing. Journal of Consulting and Clinical Psychology, 46, 892-900.
Hofling, C.K. (1975). Philadelphia:
Textbook of psychiatry for medical practice. J.B. Lippincott Company.
Hunt, H.F. (1948). The effect of deliberate deception on Minnesota Multiphasic Personality Inventory performance. Journal of Consulting Psychology, 11, 396-402.
Hunt, W.A. (1946). The detection of malingering: a further study. Naval Medical Bulletin, 46, 249-254 •
. _._ ..... _. _____ L ____________ _

Hunt, W.A. & Older, H.J. (1943). Detection of malingering through psychometric tests. Naval Medical Bulletin, 41, 1318-1323.
93
Ireland, P., Shapira, J.D. & Templeton, B. (1967). Munchausen's syndrome: Review and report of an additional case. American Journal of Medicine, 60, 1236-1239.
Jones, A.B. & Llewellyn, L.J. (1917). Malingering. Philadelphia: P.
Klecka,
Blackiston's Son & Co.
W.R. (1975). Discriminant analysis. In Nie, N.H., Hull, C.H., Jenkins, J.G., Steinbrenner, K. & Bent, D.H. (Eds.), Statistical package for the social sciences (2nd ed.). New York: McGraw Hill Book Company.
Meehl, P.E. & Hathaway, S.R. (1946). The K factor as a supressor variable in the Minnesota Multiphasic Personality Inventory. Journal of Applied Psychology, 30, 525-564.
Menninger, K.A. (1935). Psychology of a certain type of malingering. Archives of Neurology and Psychiatry, 33, 507-515.
Merrikin, K.J., Overcast, T.D. & Sales, B.D. (1982). Worker's compensation law and compensability of mental injuries. Health Psychology, 1, 373-387.
Miller, M., Overcast, T., & Sales, B.D. (1984). Damages for emotional distress in tort law. Unpublished manuscript.
Moersch, F.P. (1944). Malingering; with reference to its neuropsychiatric aspects in civil and in military practice. In The Medical Clinics of North America, the Mayo Clinic Number 928-944. Philadelphia: W.B. Saunders.
Paulson, M.J. & Lin, T. (1970). Predicting WAIS IQ from ShipleyHartford scores. Journal of Clinical Psychology, 26, 453-461.
Pollaczek, P.P. (1952). A study of malingering on the CVS Abbreviated Intelligence Scale. Journal of Clinical Psychology, ~, 77-81.
Steadman, H.J., Monahan, J., Hartstone, E., Davis, S.K. & Robbins, P.C. (1982). Mentally disordered offenders: A national survey of patients and facilities. Law and Human Behavior, ~, 31-38.
Szasz, T.S. (1956). Malingering: "diagnosis" or social condemnation? Archives of Neurology and Psychiatry, 76, 432-443.
Wachspress, M., Berenberg, A.N. & Jacobson, A. (1953). Simulation of psychosis. Psychiatric Quarterly, 27, 463-473.
Wertham, F. (1969). The show of violence. New York: Greenwood Press •
.. .... _ ... _ .. L ___ ... ________ .. _ .. _______ .. _________________ _ ... _ ........••. ---

94
Wiener, D.N. (1948). Subtle and obvious keys for the Minnesota Multiphasic Personality Inventory. Journal of Consulting Psychology, ~, 164-170.
_ .. _._~.1 ______________ _