infocus the dangers of dust devils - australian … officer while submitting the flight plan. the...
TRANSCRIPT

The Dangers of Dust DevilsInvestigation AO-2012-056
An accident in the Northern Territory that left two pilots injured has demonstrated the major hazard that dust devils can pose to light aircraft during landing. It also shows the virtues of conducting an early go-around, should an approach become unstable.
On 18 April 2012, at about 1200, a Cessna 210 was attempting to land at the Nyirripi aircraft landing area in the Northern Territory. Although there were dust devils forecast, the supervisory pilot reported that there were none observed at Nyirripi.
The supervisory pilot reported that, during the landing flare, the aircraft had not been slowed sufficiently. As a result, the aircraft ballooned twice. The supervisory pilot took control of the aircraft with the intent of recovering to a normal landing. A gust of wind, however, caused the aircraft to yaw significantly to the left. The supervisory pilot applied full power to go-around but the aircraft did not climb. He then rolled the aircraft into a thirty-degree right bank to remain over clear ground, closer to the runway.
Realising that the aircraft was going to impact the ground, the supervisory pilot rolled the wings level. The aircraft impacted fairly hard and skidded about 100 m before coming to rest north of the runway and about 600 m from the threshold. The supervisory pilot was seriously injured and the pilot in command under supervision sustained minor injuries.
The aircraft operator has since issued guidance notes to all flight crew regarding windshear recognition and recovery, as well as a reminder of information in the procedures manual.
ATSB’s full report AO-2012-056 is available at: www.atsb.gov.au
For more information on the impact that dust devils can have on aircraft operations, the following ATSB investigations provide some useful examples: 200605133, AO-2007-060.
The Bureau of Meteorology Research Centre Report No. 20, A Survey of Australian Dust Devils.
InFocus Social media is offering new opportunities to interact with our stakeholders in a more dynamic way. The ATSB already uses Twitter to alert our followers of the release of our reports and to distribute important safety messages. I am now launching a new information outlet—the Chief Commissioner’s blog.
Titled InFocus, the new blog will provide me with an opportunity to highlight issues, events, concerns and developments. Of course, this is not going to replace our traditional communication channels, but it will augment the ATSB’s message, and promote greater stakeholder discussion.
Most importantly, it will provide an avenue for public feedback. From time to time the ATSB and its work draw a great deal commentary and discussion, much of it informed. And while there are already forums where members of the transport community can discuss their views and their concerns, I think it is timely that I and my colleagues at the ATSB start to engage more openly with stakeholders through social media. All constructive messages and opinions that are shared in the comments section of this blog will be read and taken into account by the ATSB.
Inevitably, there will be some restrictions and policies surrounding the blog (this is the Government, after all), but I am looking forward to this opportunity to speak a little more directly with the transport community, and for you to speak to us.
The InFocus blog can be found on the ATSB website.
Martin Dolan Chief Commissioner
24 Hours 1800 020 616
Web www.atsb.gov.au
Twitter @ATSBinfo
Email [email protected]

Ditching highlights the need for good flight planning and monitoring
On 30 August 2012, the ATSB released its investigation report into the ditching of an Israel Aircraft Industries Westwind 1124A that occurred off Norfolk Island on 18 November 2009. The report found that the need to ditch the aircraft arose from incomplete pre-flight and en route planning and the failure to assess that a safe landing could not be assured before it was too late to divert. The investigation also confirmed the benefit of clear in-flight weather decision-making guidance and its timely application by pilots in command.
The flight was an aeromedical retrieval from Apia, Samoa bound for Melbourne via Norfolk Island. It was carrying a pilot in command (PIC), copilot, a doctor, a nurse, a patient and one passenger. The pilot submitted a flight plan to leave Apia bound for Norfolk Island, a journey of four and a half hours.
The PIC received the latest aerodrome forecast (TAF) for Norfolk Island from the briefing officer while submitting the flight plan. The forecast was valid beyond the period of the flight and indicated that the weather conditions would be suitable for landing. Based on that forecast, there was no requirement to plan or to carry fuel for the possibility of a diversion to an alternate airport.
Various weather reports and forecasts, both routine and special, were available en route through air traffic control. Special weather reports (or SPECIs) are issued when there is significant deterioration or improvement in airport weather conditions. The flight crew did not realise the significance of the changed conditions reported in a SPECI
for Norfolk Island until after they had committed to landing on Norfolk Island. By this time they had insufficient fuel reserves to divert to another destination.
The crew attempted a night approach and landing on Norfolk Island, but the weather conditions prevented them from seeing the runway or its visual aids, and therefore, from landing. After four failed attempts, the PIC elected to ditch the aircraft in the sea 3km south-west of Headstone Point on Norfolk Island, before its fuel was exhausted. The aircraft broke in two after ditching. All the occupants escaped from the aircraft and were rescued by boat, although two sustained serious injuries.
The report found that the operator’s procedures and flight planning guidance managed risks consistent with regulatory provisions but did not minimise the risks associated with aero-medical operations
to remote islands. Clearer guidance on the in-flight management of previously unforecast, but deteriorating destination weather might have assisted the crew to consider and plan their diversion options earlier.
As a result of this accident, the operator changed its guidance for the management of previously unforecast deteriorating destination weather. Satellite communication has been provided to crews to allow more reliable remote communications and its flight crew oversight systems and procedures have been enhanced. CASA is also developing a number of Civil Aviation Safety Regulations covering fuel planning and in-flight management, the selection of alternate destinations and extended diversion time operations.
ATSB’s full report AO-2009-072 is available at: www.atsb.gov.au
Wreckage of the aircraft off Norfolk Island

The ATSB’s investigation into an incident on 8 October 2011 has once again highlighted the risks of pilots becoming distracted during the critical stages of flight preparation. It also emphasises the importance of good flight crew communication to ensure a shared understanding of an aircraft’s systems status.
The incident occurred when the flight crew of a Qantas Airbus A380-800, was preparing for departure from Los Angeles International Airport. Before takeoff, the captain changed the departure runway that was entered in the aircraft’s flight management system. The procedure for completing that task was not followed exactly, resulting in the take-off speeds not being displayed on the flight instruments.
During the take-off roll, the flight crew, became aware that the take-off speeds were not displayed. Instead, they called out the speeds from their notes and proceeded with the takeoff. At all times during the takeoff, the crew were aware of how fast they were going. However, the take-off speeds that are normally displayed on the airspeed indicator were not visible for this takeoff.
The ATSB found that the captain had been distracted from updating the runway change in the aircraft’s navigation systems before the aircraft taxied for the runway. Twice, before takeoff, the aircraft’s systems displayed a message to check take-off data. The first officer cleared the first message on the understanding that the take-off data would be checked and in the second instance, believing that it had been checked. There were no other warnings
to alert the crew that they were commencing the takeoff without the take-off speeds in the aircraft’s navigation systems.
Following this incident the aircraft manufacturer has updated the aircraft’s warning systems as part of a planned upgrade program. This upgrade will issue a warning if takeoff is commenced without the take-off speeds having been entered into the aircraft’s systems. Qantas advised that their standard operating procedures have been updated to avoid any misinterpretation of the required actions in the case of a runway change.
ATSB’s full report AO-2011-151 is available at: www.atsb.gov.au
The ATSB found that the captain had been distracted from updating the runway
change in the aircraft’s navigation systems before the aircraft taxied for the runway.
Flight Crew Licence Information Many readers would be aware the ATSB requires details of flight crew involved in safety occurrences to be included in mandatory notifications.
The ATSB collects this information in accordance with the Transport Safety Investigation Act 2003 (the TSI Act) and its regulations. The information is used, where relevant, to assist the ATSB with its investigations and safety research.
Personal information collected by the ATSB is protected by the Privacy Act 1988. Under the Information Privacy Principles (IPPs) of that Act, the ATSB is obliged to make personal information it holds available to the individual. One of the ways we do that is a process called a flight crew licence check.
A flight crew licence check allows an individual to request a summary of all instances where that individual’s details have been included in a mandatory occurrence notification under the TSI Act and regulations. Some operators and recruitment agencies request copies of a flight
crew licence check from prospective employees as part of their recruitment process. The ATSB has become aware that there have been instances whereby that information may unintentionally or unfairly act to a job applicant’s disadvantage.
The ATSB has been reviewing the TSI Regulations and has been consulting on possible changes to those regulations. As a part of that process, the ATSB is considering the issue of what information is collected by the ATSB and how, consistent with the ATSB’s legal obligations, it may be provided in the future.
The ATSB is always interested in receiving comments and feedback on its processes from interested persons. If you wish to know more about either the existing flight crew licence check process or proposed amendments to the TSI regulations, we encourage you to visit the ATSB website, www.atsb.gov.au
We also welcome any feedback at [email protected]
The continuing risk of pilot distraction

Web atsb.gov.au
Twitter @ATSBinfo
Help keep aviation safe
1800 011 034www.atsb.gov.au/mandatory.aspx
To confidentially report safety concerns
call REPCON 1800 020 505
report all aviation accidents and incidents to the ATSB
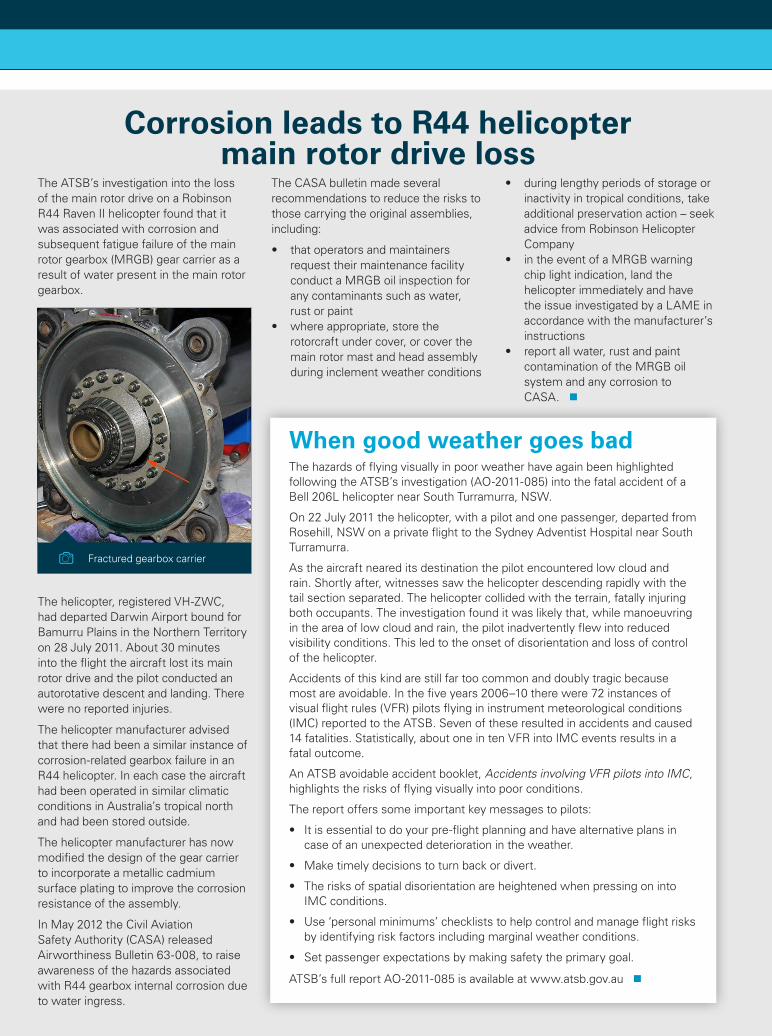
The ATSB’s investigation into the loss of the main rotor drive on a Robinson R44 Raven II helicopter found that it was associated with corrosion and subsequent fatigue failure of the main rotor gearbox (MRGB) gear carrier as a result of water present in the main rotor gearbox.
The helicopter, registered VH-ZWC, had departed Darwin Airport bound for Bamurru Plains in the Northern Territory on 28 July 2011. About 30 minutes into the flight the aircraft lost its main rotor drive and the pilot conducted an autorotative descent and landing. There were no reported injuries.
The helicopter manufacturer advised that there had been a similar instance of corrosion-related gearbox failure in an R44 helicopter. In each case the aircraft had been operated in similar climatic conditions in Australia’s tropical north and had been stored outside.
The helicopter manufacturer has now modified the design of the gear carrier to incorporate a metallic cadmium surface plating to improve the corrosion resistance of the assembly.
In May 2012 the Civil Aviation Safety Authority (CASA) released Airworthiness Bulletin 63-008, to raise awareness of the hazards associated with R44 gearbox internal corrosion due to water ingress.
The CASA bulletin made several recommendations to reduce the risks to those carrying the original assemblies, including:
• thatoperatorsandmaintainersrequest their maintenance facility conduct a MRGB oil inspection for any contaminants such as water, rust or paint
• whereappropriate,storetherotorcraft under cover, or cover the main rotor mast and head assembly during inclement weather conditions
• duringlengthyperiodsofstorageorinactivity in tropical conditions, take additional preservation action – seek advice from Robinson Helicopter Company
• intheeventofaMRGBwarningchip light indication, land the helicopter immediately and have the issue investigated by a LAME in accordance with the manufacturer’s instructions
• reportallwater,rustandpaintcontamination of the MRGB oil system and any corrosion to CASA.
Corrosion leads to R44 helicopter main rotor drive loss
When good weather goes bad The hazards of flying visually in poor weather have again been highlighted following the ATSB’s investigation (AO-2011-085) into the fatal accident of a Bell 206L helicopter near South Turramurra, NSW.
On 22 July 2011 the helicopter, with a pilot and one passenger, departed from Rosehill, NSW on a private flight to the Sydney Adventist Hospital near South Turramurra.
As the aircraft neared its destination the pilot encountered low cloud and rain. Shortly after, witnesses saw the helicopter descending rapidly with the tail section separated. The helicopter collided with the terrain, fatally injuring both occupants. The investigation found it was likely that, while manoeuvring in the area of low cloud and rain, the pilot inadvertently flew into reduced visibility conditions. This led to the onset of disorientation and loss of control of the helicopter.
Accidents of this kind are still far too common and doubly tragic because most are avoidable. In the five years 2006–10 there were 72 instances of visual flight rules (VFR) pilots flying in instrument meteorological conditions (IMC) reported to the ATSB. Seven of these resulted in accidents and caused 14 fatalities. Statistically, about one in ten VFR into IMC events results in a fatal outcome.
An ATSB avoidable accident booklet, Accidents involving VFR pilots into IMC, highlights the risks of flying visually into poor conditions.
The report offers some important key messages to pilots:
• Itisessentialtodoyourpre-flightplanningandhavealternativeplansincase of an unexpected deterioration in the weather.
• Maketimelydecisionstoturnbackordivert.
• TherisksofspatialdisorientationareheightenedwhenpressingonintoIMC conditions.
• Use‘personalminimums’checkliststohelpcontrolandmanageflightrisksby identifying risk factors including marginal weather conditions.
• Setpassengerexpectationsbymakingsafetytheprimarygoal.
ATSB’s full report AO-2011-085 is available at www.atsb.gov.au
Fractured gearbox carrier

Frequency congestion at Emerald
Report narrative:The reporter expressed a safety concern about the congestion on the radio experienced by pilots operating in the Emerald area.
The reporter stated that the Emerald CTAF is very busy due to the number of airports in close proximity using the same frequency. This is compounded by having to monitor the Area Frequency as well. This frequency is itself busy, but as the Area Frequency is combined with the adjacent Area Frequencies, which are retransmitted on each of the frequencies, the level of congestion is unacceptably high.
The levels of radio congestion create a difficult environment for crews to maintain a good situational awareness and to communicate with conflicting traffic to arrange mutual separation.
Response/s received:REPCON supplied Airservices Australia with the de-identified report. The following is a version of their response:
In relation to the combining of area frequencies, most Air Traffic Control (ATC) Sectors containing Class G airspace encompass more than one VHF frequency. A frequency retransmission facility is provided to avoid repeated aircraft over-transmissions resulting in garbling and/or jamming of aircraft calls. While it is recognised that frequency congestion can sometimes be an issue, use of the retransmission facility assists ATCs and pilots to ensure continuity of communications.
The reporter’s concern in respect of the CTAF should be referred to Civil Aviation Safety Authority (CASA).
REPCON supplied CASA with the de-identified report and a version of Airservices Australia’s response. The following is a version of the response that CASA provided:
The process for determining the need for, and allocation of, a discrete CTAF at a particular aerodrome, or aerodromes group is:
• applicationtoCASAtoassessthesituation (local Field Office);
• adviseRAPAC,throughRAPACSecretariat, of the proposal for industry consultation; and
• ifachangeisdetermined,forwardthe decision to the Office of Airspace Regulation in CASA to facilitate the change(s).
CASA, as part of our relevant safety action, will raise this issue at the next local RAPAC meeting for discussion and resolution as appropriate.
Use of personal electronic devices
Report narrative:The reporter expressed a safety concern about the use of mobile devices onboard a domestic flight. The reporter observed that passengers are using these devices frequently, texting and using internet connectivity during flight. The reporter believes that cabin crew do not take this safety matter seriously and often do not adequately warn passengers to turn off electronic devices or that the devices should be in flight mode.
Response/s received:REPCON supplied the operator with the de-identified report. The following is a version of their response:
We can advise that a review of our occurrence database from 1 January 2011 shows that on over 500 occasions cabin crew have reported the hazard of passengers using their mobile phones and personal electronic devices (PEDs) onboard. It is felt that the volume of reports received illustrates that cabin crew are very aware of the regulatory requirements and company policies on this matter and are vigilant in ensuring compliance, particularly as the cabin is being secured for takeoff.
In addition, it’s possible that passengers writing text messages are constructing them while their phones are in flight mode. It is also not possible to manage passenger use of PEDs during takeoff and/or the descent phase as the cabin crew must be seated. The reports we receive highlight passenger reluctance and attitudes towards PED usage and the belief it is the operator’s policy and not a regulatory requirement. However, the operator believes the hundreds of reports each year show that our cabin crew take passenger use of PEDs at inappropriate times very seriously.
In addition, the PED policy is currently part of the cabin crew recurrent emergency procedures curriculum and is covered in the “Standard Operating Procedures” section of the training day. The proliferation of PEDs has made the potential much higher for non-compliance but it is not possible for cabin crew to check that all PEDs are switched to flight mode and then off. In this respect cabin crew act in good faith that passengers are compliant, responsible and accountable themselves.
REPCON supplied CASA with the de-identified report and a version of the operator’s response. The following is a version of the response that CASA provided:
CASA has reviewed this matter with internal subject matter experts and has examined the operator’s procedures and, is satisfied with the operator’s response.
Australia’s voluntary confidential aviation reporting schemeREPCON allows any person who has an aviation safety concern to report it to the ATSB confidentially. All personal information regarding any individual (either the reporter or any person referred to in the report) remains strictly confidential, unless permission is given by the subject of the information.
The goals of the scheme are to increase awareness of safety issues and to encourage safety action by those best placed to respond to safety concerns.
How can I report to REPCON?Online: www.atsb.gov.au/voluntary.aspx
REPCON BRIEFS