infection prevention and control breakfast for hospitals ... · infection prevention and control...
TRANSCRIPT

© J
oint
Com
mis
sion
Res
ourc
es
Infection Prevention and Control Breakfast for Hospitals
September 14, 2017
Karen Martin RN, MPH, CICConsultant, Infection Prevention Services
Joint Commission Resources

© J
oint
Com
mis
sion
Res
ourc
es
Disclosure Statement
Disclosure StatementThe following staff and speakers have disclosed that they do not
have any financial arrangements or affiliations with corporate organizations that either provide educational grants to this program or may be referenced in this activity:• Karen Martin• Leslie LaBelle• George Riccio• Steve Chinn
The listed staff and speakers have verbally disclosed their arrangements and affiliations: Not Applicable to this presentation
Furthermore, each of the previously named speakers has also attested that their discussions will not include any unapproved or off-label use of products.
2

© J
oint
Com
mis
sion
Res
ourc
es
Publications and Record Restrictions
The program may be electronically recorded by JCR and is subject to the protection of the copyright laws of the US. No individual or entity other than JCR may electronically record any portion of these programs for any purpose without the written permission of JCR. Any and all reproduction or publication of these proceedings and programs for commercial purposes by anyone other than JCR is prohibited.
3

© J
oint
Com
mis
sion
Res
ourc
es
Publications and Record Restrictions
Copyright © 2017 by Joint Commission Resources, Inc. All rights reserved. No part of this publication may be reproduced in any form or by any means without written permission from the publisher. Request for permission to make copies of any part of this work should be mailed to: Publication and Education Resources, Joint Commission Resources, 1515 West 22nd StreetSuite 1300W, Oak Brook, Illinois 60523.
4
© J
oint
Com
mis
sion
Res
ourc
es
Objectives for Hospital Briefings: The Participant will be able to:
• Discuss most cited Standards IPC challenges and solutions.
• Discuss changes to the 2018 standards as it relates to NPSG.07.03.01
• Discuss changes to the 2018 standards as it relates to NPSG.07.04.01
5

© J
oint
Com
mis
sion
Res
ourc
es
Most Frequent Non-Compliant Standards For 2016
6

© J
oint
Com
mis
sion
Res
ourc
es
What’s Wrong With This Picture
7

© J
oint
Com
mis
sion
Res
ourc
es
It’s Headed In The Wrong DirectionIC.02.02.01
From 60%
To 70%

© J
oint
Com
mis
sion
Res
ourc
es
CDC Progress Report For HAI’s
9

© J
oint
Com
mis
sion
Res
ourc
es
CDC Progress Report 2016
Among national acute care hospitals, the report found:
50 percent decrease in CLABSI between 2008 and 2014
No change in overall CAUTI between 2009 and 2014 • However, there was progress in non-ICU
settings between 2009 and 2014, progress in all settings between 2013 and 2014, and even more progress in all settings towards the end of 2014
17 percent decrease in SSI related to the
10

© J
oint
Com
mis
sion
Res
ourc
es
10 select procedures tracked in previous reports • 17 percent decrease in abdominal hysterectomy
SSI between 2008 and 2014• 2 percent decrease in colon surgery SSI
between 2008 and 2014 8 percent decrease in C. difficile infections
between 2011 and 2014 13 percent decrease in MRSA bacteremia
between 2011 and 2014
11

© J
oint
Com
mis
sion
Res
ourc
es
HAI Prevalence Survey
HAI Estimates Occurring in US Acute Care Hospitals, 2011
Major Site of Infection Estimated No.
Pneumonia 157,500
Gastrointestinal Illness 123,100
Urinary Tract Infections 93,300
Primary Bloodstream Infections 71,900
Surgical site infections from any inpatient surgery 157,500
Other types of infections 118,500
Estimated total number of infections in hospitals 721,800
12
© J
oint
Com
mis
sion
Res
ourc
es
What Does This Mean For Us
13
This Photo by Unknown Author is licensed under CC BY-NC-SA
© J
oint
Com
mis
sion
Res
ourc
es
14
Effective Infection Prevention and Control (IPC) Program
Goal: Reduce the risk of acquisition and transmission of healthcare associated infections (HAI)• Input and support of hospital leadership• Communication and collaboration• Everyone involved in the daily operations of the
facility knows their role in preventing infection• Culture of patient and staff safety

© J
oint
Com
mis
sion
Res
ourc
es
Joint Commission Infection Prevention and Control Standards
l. PlanningA. Responsibility (IC.01.01.01)B. Resources (IC.01.02.01)C. Risks (IC.01.03.01)D. Goals (IC.01.04.01)E. Activities – Plan (IC.01.05.01)F. Influx (IC.01.06.01)
ll. ImplementationA. Activities (IC.02.01.01)B. Medical Equipment, Devices and Supplies (IC .02.02.01)C. Transmission of Infections (IC.20.03.01)D. Influenza Vaccinations (IC.02.04.01)
III. Evaluation (IC.03.01.01)
15

© J
oint
Com
mis
sion
Res
ourc
es
IPC Standards Are Supported By Other Chapter’s Standards
• Leadership• Management of the Environment of Care• Management of Human Resources• Improving Organization Performance• Emergency Preparedness
See Examples in Slides at the end of the presentation
16

© J
oint
Com
mis
sion
Res
ourc
es
2017 IC Standards Non Compliance
17

© J
oint
Com
mis
sion
Res
ourc
es
What are the Most Challenging Infection Prevention and Control Standards for Hospitals?
18

© J
oint
Com
mis
sion
Res
ourc
es
Top Cited Standards From 4/17 –8/17
19

© J
oint
Com
mis
sion
Res
ourc
es
IC.02.01.01 Non-Compliance
EP 1 - Implements infection control activities (407/1445)
EP 2 – The hospital uses standard precautions ( 93/ 1445)
EP 3 – The hospital uses transmission based precautions ( 20/1445)
EP 6 – The hospital minimizes risk of infectious waste (10/1445)

© J
oint
Com
mis
sion
Res
ourc
es
The Hospital Implements It’s Infection Prevention Activities
· Soiled ceiling tiles in central sterile department (CSD) · Patient care items stored within three feet of sinks · Unclear processes for separation of clean/dirty · Lack of solid surfaces on storage shelves · Drink found in patient care areas· Commingling of clean and dirty supplies
21

© J
oint
Com
mis
sion
Res
ourc
es
The Hospital Implements Standard Precautions
22

© J
oint
Com
mis
sion
Res
ourc
es
Hospital Implements Transmission Based Precautions
23
© J
oint
Com
mis
sion
Res
ourc
es
Minimizes the Risk of Infection When Storing and Disposing of Medical Waste
24
© J
oint
Com
mis
sion
Res
ourc
es
25

© J
oint
Com
mis
sion
Res
ourc
es
IC.02.02.01The hospital reduces the risk of infections associated with medical equipment, devices and supplies
26

© J
oint
Com
mis
sion
Res
ourc
es
Noncompliance Findings Sterilization
Quality monitoring parameters (physical, chemical, and biological) not being consistently conducted or documented per manufacturer’s instructions, or use of evidence based guidelines
Approximating use of cleaning products not measuring per manufacturer’s instructions
No documentation of routine cleaning or preventative maintenance of the sterilizer
27

© J
oint
Com
mis
sion
Res
ourc
es
Non compliance Continued
Not following sterilization evidence-based guidelines
28

© J
oint
Com
mis
sion
Res
ourc
es
Non compliance High Level Disinfection
Use of a low-level disinfectant wipe instead of a high level disinfectant to reprocess a vaginal ultrasound probe between patient use
Lack of quality monitoring documentation( temperature, time. Minimal effective concentration of high-level disinfectant per manufacturers’ instructions or evidence based guidelines
29

© J
oint
Com
mis
sion
Res
ourc
es
Noncompliance Continued
Reusable brushes to clean endoscopes not being cleaned or disinfected between each use or at the end of the day per evidence –based guidelines or manufactures’ instructions
Not following device manufacturer instructions for use or high level disinfection evidence-based guidelines for endoscopes or probes (vaginal,rectal)
30

© J
oint
Com
mis
sion
Res
ourc
es
IC.02.02.01 Medical equipment, devices and supplies. Surveyors have found:
Failure to properly:• Clean• Disinfect• Sterilize• Use • Store
Medical equipment, devices, and supplies
31

© J
oint
Com
mis
sion
Res
ourc
es
What Needs TO Be Done TO Improve
Training
Clear concise policies
Standardization of process
Follow manufacturers’ direction for use
32

© J
oint
Com
mis
sion
Res
ourc
es
IC.02.02.01 Medical equipment, devices and supplies
Orientation, training, and competency of health care workers who are processing medical equipment, devices, and supplies
Levels of staffing and supervision of the health care workers who are processing medical equipment, devices, and supplies
33
© J
oint
Com
mis
sion
Res
ourc
es
IC.02.02.01 Medical equipment, devices and supplies
Standardization of process regardless of whether it is centralized or decentralized
Reinforcing the process
Ongoing quality monitoring
34

© J
oint
Com
mis
sion
Res
ourc
es
Training and Competency
Training and Competency• Upon hire• At least annually• Whenever new item or equipment
– borrowed – leased– purchased
• Whenever new policies and procedures are implemented
35
© J
oint
Com
mis
sion
Res
ourc
es
Training and Competency
Training should include*• Principles of cleaning, disinfection and sterilization• Inspection, preparation, and packaging of
instruments• Worker safety and use of personal protective
equipment (PPE)• Manufacturer’s instructions for use• Quality control of processes• Endoscope model specific cleaning and
disinfection, if applicable
* Abbreviated list for presentation purposes
36

© J
oint
Com
mis
sion
Res
ourc
es
Training and Competency
Training is NOT equivalent to demonstrated competency
Competency is ability of the individual to perform specific tasks in accordance to the standards that are required
37

© J
oint
Com
mis
sion
Res
ourc
es
Policies and Procedures
Clear – no room for interpretation (creativity and work-a-rounds not appropriate)
Based on• scientifically based standards• manufacturer’s instructions for use• infection control and prevention practices
Apply to all locations and staff Readily accessible to staff
38

© J
oint
Com
mis
sion
Res
ourc
es
IC.02.02.01
39

© J
oint
Com
mis
sion
Res
ourc
es
Low Level Disinfection
40
Slideshare.net

© J
oint
Com
mis
sion
Res
ourc
es
Findings of Noncompliance
Lack of clear policy
Separation of Clean /Dirty
Identifying what is clean
Proper wet contact time
Not following policy
41

© J
oint
Com
mis
sion
Res
ourc
es
Use of Supplies
42
© Sylvia Garcia-Houchins
Must be able to clearly differentiate clean from dirty

© J
oint
Com
mis
sion
Res
ourc
es
Performing Intermediate and High Level Disinfection and Sterilization
43

© J
oint
Com
mis
sion
Res
ourc
es
Personal Protective Equipment
Donned by all persons entering decontamination areas
• fluid-resistant gown or jump suit
• hair and shoe covering Individuals performing
decontamination of instruments or equipment
• heavy duty gloves• fluid-resistant mask • eye protection
© Sylvia Garcia-Houchins
44

© J
oint
Com
mis
sion
Res
ourc
es
Endoscopy: Processing Room
Pre-cleaning must be done at bedside Endoscope processing may not occur in a
room that is used for any other purpose, and it should never occur in the procedure room• area physically separated from locations where
clean items are handled and patient care activities are performed.
10 air changes (local regulations or manufacturers recommendations may require more)
45Source: Perspectives March 2012

© J
oint
Com
mis
sion
Res
ourc
es
Pre-Cleaning
Should start as soon as possible after use to prevent drying• Flush lumens with sterile water • Wipe instruments with a moistened sponge
Immediately after the procedure, cover with • A compatible enzymatic spray, gel or foam, • Compatible detergent • Cloth moistened with water
Transport as soon as possible Some endoscopes require reprocessing within 1
hour
Ref: AORN and AAMI
46

© J
oint
Com
mis
sion
Res
ourc
es
Decontamination
Follow manufacturer’s instructions May require
• Manual• Mechanical• Combination of both
Ensure entire instrument is disassembled, cleaned and rinsed including valves, channels, connectors and all detachable parts in accordance with manufacturer’s instructions
© Sylvia Garcia-Houchins
47
© J
oint
Com
mis
sion
Res
ourc
es
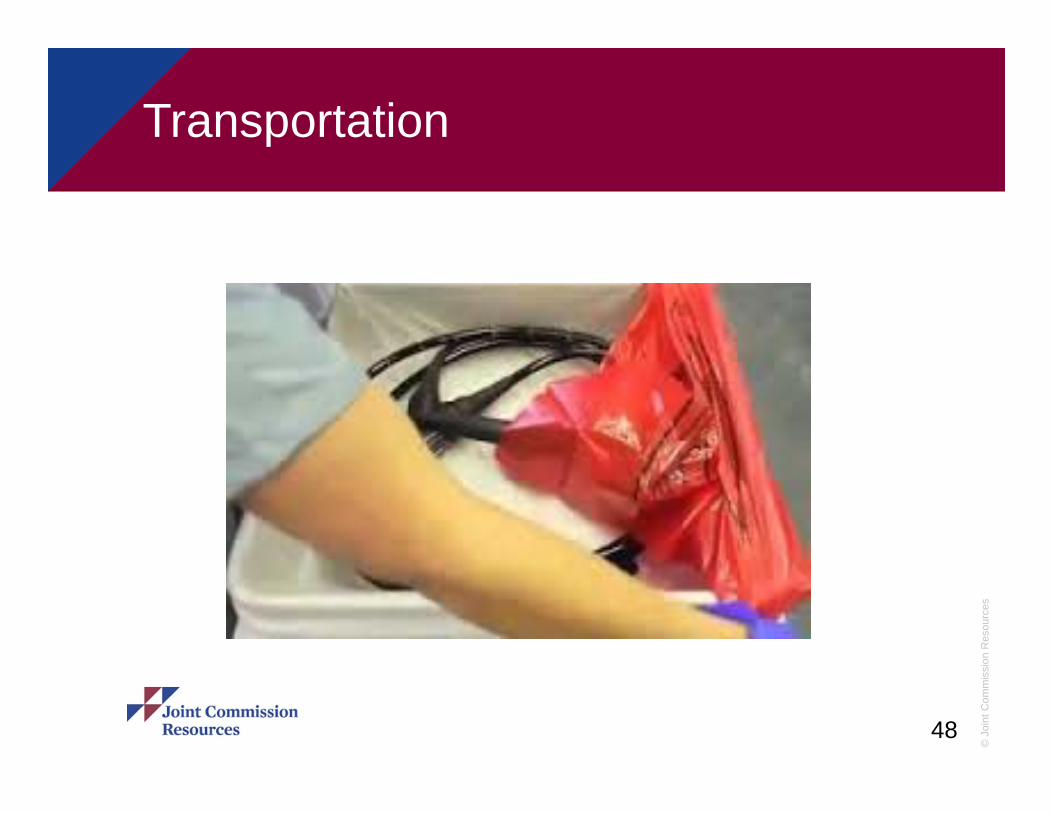
Transportation
48
© Sylvia Garcia-Houchins

© J
oint
Com
mis
sion
Res
ourc
es
Transporting Supplies, Equipment, Specimens
49
© Sylvia Garcia-Houchins
© Sylvia Garcia-Houchins

© J
oint
Com
mis
sion
Res
ourc
es
50

© J
oint
Com
mis
sion
Res
ourc
es
Decontamination
Follow recommended dilution of cleaning chemicals and soak times
Rinse according to cleaning agent manufacturer’s instructions
Brushes • may be labeled as single or
multiple use• reusable brushes should be
disinfected• In accordance with device
instructions
51

© J
oint
Com
mis
sion
Res
ourc
es
Equipment
Use in accordance to manufacturer’s instructions
Test at installation and at least weekly, if applicable © Sylvia Garcia-Houchins
52
© Sylvia Garcia-Houchins
© Sylvia Garcia-Houchins

© J
oint
Com
mis
sion
Res
ourc
es
Monitoring and Documentation
If the device includes a printout, staff should verify that all sterilization parameters were met by initialing the printout
If no recording device is part of the device, the operator should verify in writing that sterilization parameters as indicated by the manufacturer were met
© Sylvia Garcia-Houchins
53
© J
oint
Com
mis
sion
Res
ourc
es
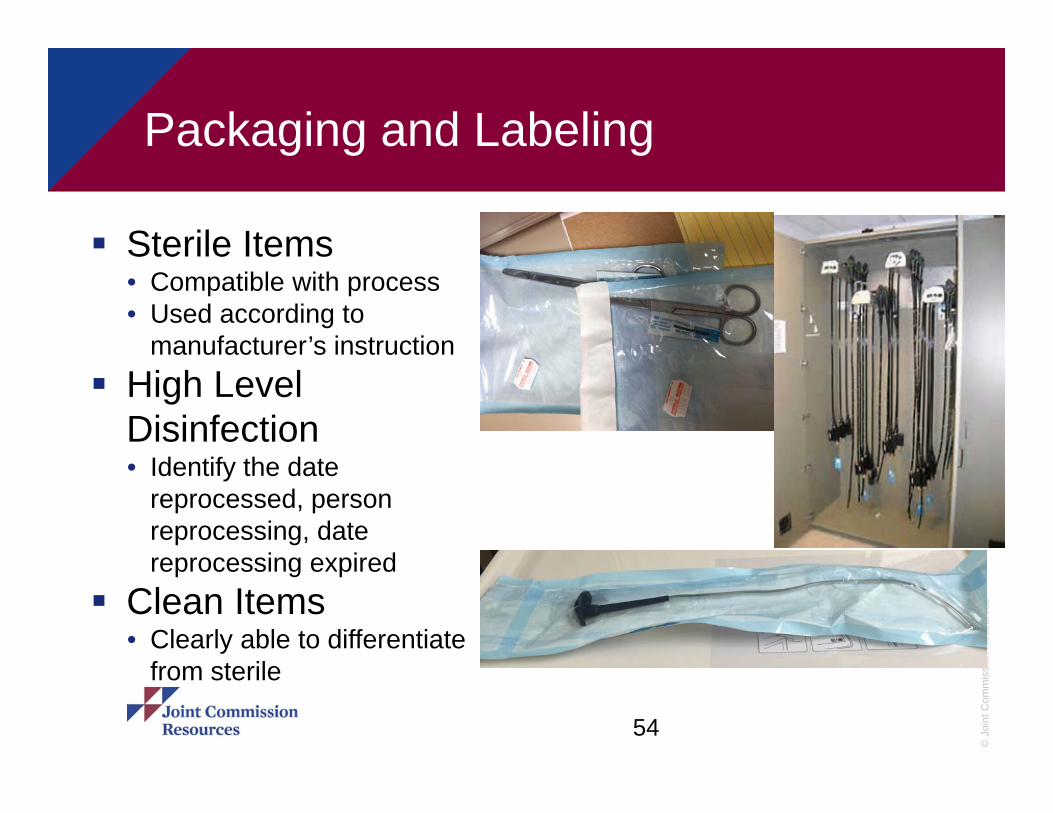
Packaging and Labeling
Sterile Items• Compatible with process• Used according to
manufacturer’s instruction High Level
Disinfection• Identify the date
reprocessed, person reprocessing, date reprocessing expired
Clean Items• Clearly able to differentiate
from sterile
54

© J
oint
Com
mis
sion
Res
ourc
es
Labeling Sterile Products
Label should • Not compromise
the barrier Include
• Contents• Date sterilized• Identifier that
allows the item to be tracked back to the sterilization load
© Sylvia Garcia-Houchins
© Sylvia Garcia-Houchins
© Sylvia Garcia-Houchins
© Sylvia Garcia-Houchins
55

© J
oint
Com
mis
sion
Res
ourc
es
Storage of Sterile Devices
AAMI: sterile items be stored • at least 8 inches of the floor• 18 inches below ceiling or sprinkler• 2 inches from outside wall• away from any location where they
could become wet Dust covers may be used to
protect sterilized items that could be subjected to environmental challenges or excessive handling before use
No corrugated boxes (external shipping boxes)
Does not damage packaging
© Sylvia Garcia-Houchins
56

© J
oint
Com
mis
sion
Res
ourc
es
Storage of Sterile Devices
If open shelves are used, traffic control, ventilation, and housekeeping should be monitored
• Bottom shelves should be solid to prevent soiling when floors are cleaned
• Covered or closed cabinets limit dust and are preferred for seldom used items
© Sylvia Garcia-Houchins
57

© J
oint
Com
mis
sion
Res
ourc
es
Essential References for Endoscopy
Society of Gastroenterology Nurses and Associates (SGNA)
American Society for Gastrointestinal Endoscopy (ASGE)
Gastrointestinal Society of Australia (GESA)
58

© J
oint
Com
mis
sion
Res
ourc
es
Essential References
AAMI AORN CDC Guidelines OSHA Bloodborne
Pathogens Standard State Regulations
59

© J
oint
Com
mis
sion
Res
ourc
es
Immediate Jeopardy ?
60
© J
oint
Com
mis
sion
Res
ourc
es
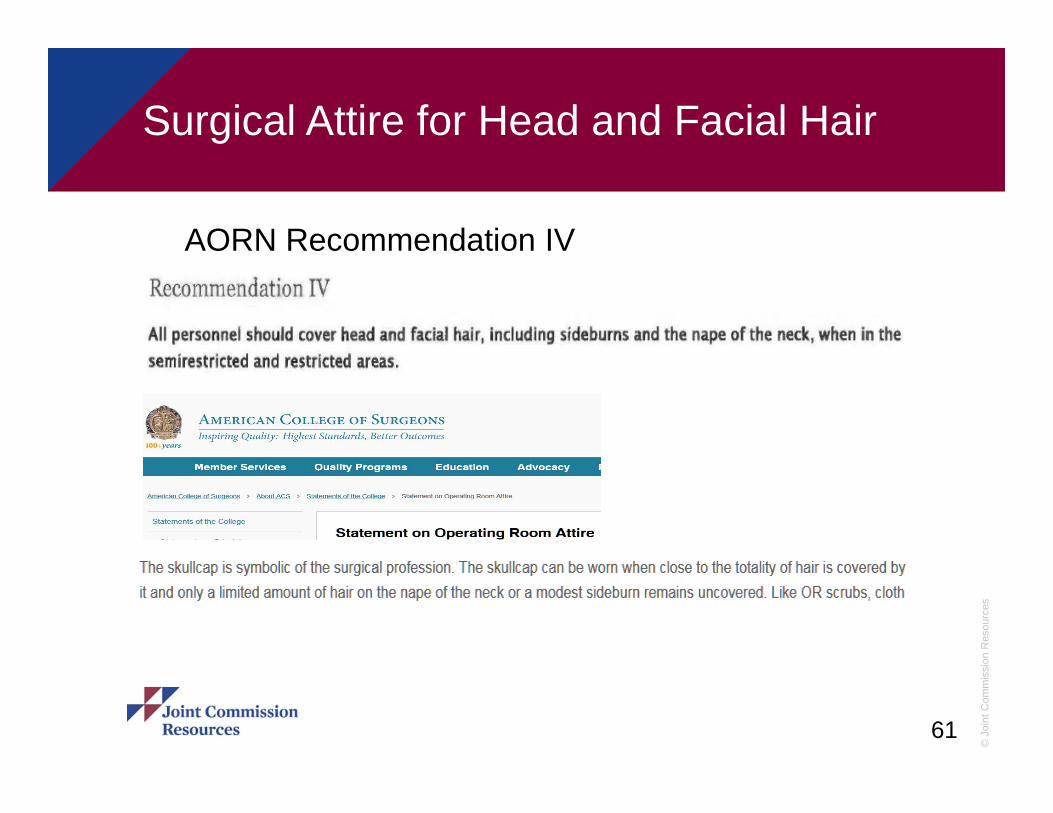
Surgical Attire for Head and Facial Hair
61
AORN Recommendation IV

© J
oint
Com
mis
sion
Res
ourc
es
What’s On The Horizon 2018
No changes for IC standards
Modifications to National Patient Safety Goal 7
NPSG.07.03.01
NPSG.07.04.01
62

© J
oint
Com
mis
sion
Res
ourc
es
NPSG.07.03.01 MDRO’s
Although this goal already exists for hospitals, Carbapenem-resistant enterobacteriaceae (CRE) as one of the organisms covered by the goal
Organizations can determine timeframe for education to staff
Surveillance may be targeted rather than house wide
63

© J
oint
Com
mis
sion
Res
ourc
es
NPSG.07.04.01 Central Lines
Organizations can determine time-lines for education
Maximum sterile barrier no more protocol for
Chlorhexidine antiseptic for skin preparation
64
© J
oint
Com
mis
sion
Res
ourc
es
Thank You
Questions !
65