indonesia current status of integrated community … daeng tb jayapura ctp padang pusako jakarta...
TRANSCRIPT

Indonesia
National TB Program
Current status of integrated community based TB service delivery and the Global Fund work plan to find missing TB cases

Country Profiles

3
Annual TB incidence in Indonesia reach 1,020,000 cases.
The incidence rate of TB is 391 per 100,000 population.
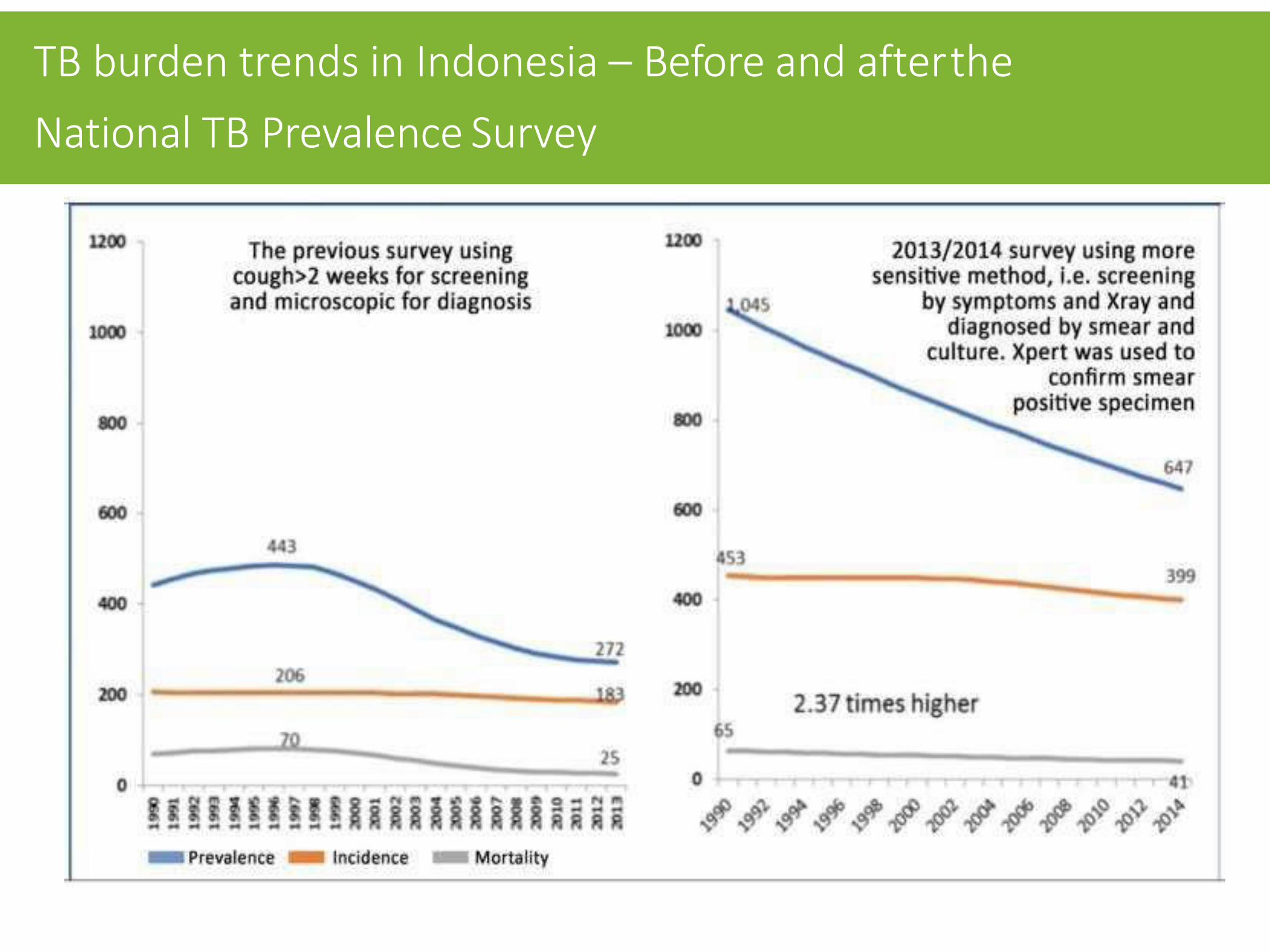
TB burden trends in Indonesia – Before and after the
National TB Prevalence Survey

• Contact Tracing • Screening in a Specific
Population (urban poor, underserved area, Remote area etc)
• Drop Out follow-up (DOFU) • Risk factor analysis
• Implementation of District Based PPM
• Mandatory Notification and Strengthening of surveillance
• Management of integrated TB services (HIV, DM, nutrition, smoking, elderly etc)
• Sync with National Insurance system

Case Detection Rate 2017

Treatment Success Rate 2017

Estimated of DR-TB burden (WHO 2017)
Incidence MDR+RR TB 32.000
Estimated MDR+RR-TB cases
among notified pulmonary TB
cases
11.000
Estimated %of TB cases with
MDR + RR-TB
2.8% (new)
16% (Prev.Tx)
Laboratory-confirmed cases 2.757
Patients started on treatment 1.931
Succes rate 51 %
Situation Burden
TB HIV incidence 45.000
Knowing HIV status 14%
TB HIV on ART 28%
Succes rate 60%

VISION An Indonesia free
of tuberculosis
MISSION TB Elimination in
Indonesia by 2030
NATIONAL STRATEGIC PLAN 2016 - 2020 Milestones toward TB elimination in Indonesia
02
03
04
05
06
Improving access to the quality TB services
Control of Risk Factors
Enhancing TB Partnership through
the Coordination Forum
Engaging Community in TB Control
Health System Strengthening
01 Strengthening Leadership in the District level Management

MAJOR TARGET
NATIONAL STRATEGIC PLAN 2016-2020
Milestones toward TB elimination in Indonesia
Indonesia END TB strategy key targets by 2030: • Increase case notification from 32% in 2016 to 70% in 2020 • Expand access to and utilization of Xpert MTB/RIF as primary diagnostic
tool for at least 75% of presumptive TB patients by 2020 • Ensure 80% of DR-TB patients are diagnosed and notified by 2020
Ensure 95% of diagnosed DR-TB patients are enrolled on treatment by 2020
Improve overall treatment success for DS-TB to 90% from 2017 onwards and for DR- TB to 75% by 2020
Increase proportion of TB patients with known HIV status from 15% to 50%, 60% and 75% in 2018, 2019, 2020 respectively, and ensure all co-infected patients are started on ART
Provide IPT to at least 50% of child (< 5 yrs.) contacts of TB patients

National Indicator on National Strategy
No Indicator Baseline
2015
Target
2016 2017 2018 2019 2020
Strategi 5: Increasing Community Participation to TB Control
5,1
Percentage of TB cases found and
referred by community or community
organizations
3,5%
8%
12%
16%
20%
20%

CSO Baseline 2018 2019 2020
Aisyiyah N/A
48.023 (35%)
75.749 (49%)
105.171 (63%)
Number of bacteriologically confirmed TB patients whose household contacts screened for TB
Number of notified TB cases (all forms) contributed by non-national TB program providers – community referral
CSO Baseline 2018 2019 2020
Aisyiyah N/A
40.109 (7,5%)
63.124 (10,5%)
87.643 (13,5%)
Performance Framework (PF) The Global Fund (Aisyiyah)

Challenges in Engaging Community in TB Control
Lack of public knowledge regarding TB symptoms and place to go for examination, diagnosis, and quality guaranteed treatment Limited involvement of the patients, former patients and families and the wider community in TB control
Limited geographical coverage of civil society organizations and other stakeholders
Socio-economic barriers TB patients to access TB care
Still Low public awareness about the rights and responsibilities of TB patients
High stigma among healthcare worker as well as in communities

Suspect finding by cadre
Cadre Counseling
Sputum Examination
Examinati on (+)
HIV Test
HIV + Monitor Cadre
HIV
HIV -
Training PMO- TB
Success TB ALL
Smear -
X-Ray Gen-X
TB +
TB -
TB - NOT Success
Cadre Training
Cadre Recruitment
Recruitment PS-MDR
PS-MDR
TB-MDR Care
Activity Flow Chart of“Community TB-HIV Care” (CST)
Cadre Monitoring Meeting (2 Monthly)
Coordination Meeting on District Level (3 Monthly)
Provincial Coordination Meeting (6 Monthly) - Rakorwil
Clinical Signs +
Contact Tracing by Cadre
FINISH
National Coordination Meeting (6 Monthly / Annual)
Monitor Cadre PMO

SR SSR
IMPLEMENTATION ARRANGEMENT MAPPING

MAPPING OF CSO
LKNU
AISYIYAH
PELKESI
PERDHAKI
SPIRITA
PAMALI TB INDONESIA
PPTI PUSAT
LKC
DMI Dewan Masjid
Indonesia
YKB Yayasan
Kusuma Buana
PARTISAN (Red Institute)
YAPARI Yayasan
Pembinaan Remaja
YARSI TB CARE
JKM Jaringan Kesehatan
Masyarakat
PKPU
JAPETI Jaringan Peduli TB Indonesia

MAPPING OF PATIENTS ORGANIZATION (PROVIDE SUPPORT AND CONTACT INVESTIGATION FOR DR TB PATIENTS)
MEDAN Pejuang Sehat
Bermanfaat (PESAT)
BATAM STORY
BANJARMASIN BEKANTAN
MAKASSAR Kami Rela Berjuang Bagi
Jiwa (KAREBABAJI)
GOWA DAENG TB
JAYAPURA CTP
PADANG PUSAKO
JAKARTA Pejuang Tangguh (PETA)
BANDUNG Terus Berjuang (TERJANG)
SEMARANG Semangat Membara
(SEMAR)
MADIUN PETIR
MALANG Pantang Menyerah
(PANTER)
SURABAYA Arek Nekat (REKAT)
JEMBER Syukur Sabar Semangat
Sukses (SEKAWANS)
DENPASAR GAMELAN
SIKA SIKA BERAKSI
• NTP develop guidelines and modules, • Training of Trainers will be supported by Global Fund and CTB
project • Training of Trainers focusing in high burden areas • 3 days training will be done in district level • Stepwise integrated supervision (NTP -> PHO -> DHO ->
Puskesmas) • Reporting and recording in case finding and case holding
• For DR TB will use mobile-based application called EMPATI (e-mobile for DR TB patient)
SUPPORT FOR IMPLEMENTATION

01
02
03
04
05
NTP
PHO
DHO
Puskesmas
Cadre
Reporting System
23
Presumptive TB Form
TB 06
TB 03
TB 07, 08, etc.

IMPLEMENTATION TOOLS (AISYIYAH CADRE)

IMPLEMENTATION TOOLS (AISYIYAH CADRE)

IMPLEMENTATION TOOLS (AISYIYAH CADRE)

IMPLEMENTATION TOOLS (MoH)

IMPLEMENTATION TOOLS (MoH)

IMPLEMENTATION TOOLS (MoH)

IMPLEMENTATION TOOLS (MoH)

IMPLEMENTATION TOOLS (MoH)

IMPLEMENTATION TOOLS (MOBILE)

• There is no formal coordination mechanism e.g. NTP-NGO coordination body
• Yet, there is an existing forum called Forum Stop TB Partnership Indonesia (FSTPI) consisting of CSO, Private Sector, Ministrials, Patient Organization, Professional Organization and individual
Mechanisms for coordination of community based TB Activities

Indonesia
National TB Program
Success story

36
Gancang Aron
• New innovation called “Gancang Aron” has been launched by the Local Government of Banyuwangi Regency to provide a wider access and comfortable services to TB patients by deploying the pharmacy team to deliver TB medicine to the patients’ homes in person. They also visited the patients’ homes to directly observe while the patients taking TB drug, assess the environment, behavior and give education the household member. “Gancang Aron” means “get well soon”. As an acronym, it means avoiding long queues.
• The local government also collaborated with online ride rents to deliver TB medicine. The drivers completed a training in a pharmacy service before joining.

Surakarta City
Jayapura City Community Coalitions

Family Health Approach: Indonesia's “Knock the Doors”

Knock the Doors

Indonesia
National TB Program
Country work plans for community based TB activities

SSR
Monitoring
Orientation of
PMO
Case reward
payment
Validasi oleh
SSR
Patient data
distribution by
SSR
Recruitment
and Cadre
selection
Investigation
by cadre
(index cases)
Cadre
Training
Data of
estimated
patient ratio
2017
Training
Module*
Patient Data
in Puskesmas
Drop-Out/
Death
Recapitulation
by Monev SSR
cured
Coordination
with sub-
district//village
head involving
cadre
Validation and repoting
to puskesmas by
subdistrict coordinator
coordination with department of health (dinkes)/healthcare center (puskes) each semester
Coordination with Provincial Department of Health
National Coordination
Monthly
Cadre
Mapping in
Sub District Suspect
reward
payment
Refer &
check at
puskesmas
Orientatio
n PMO
result +
(patient)
Child (<5 yo)
Elderly
suspect
Contact Investigation Suspect

Policy / service
changes and TB- HIV budget
improvements
Issue packing/campai
gn/public education
Lobby/negotiati
on/audiences
Legal drafting/counter
draft
FGD to Review regional policy
Meeting with philanthropy & private sector
Establishment of Alliance
(CSO Coordination
Meeting)
Development
of Policy Paper
Development
and updating of joint advocacy strategies for
HIV TB
Arrangement
and updating of situation analysis
/ public test
Workshop on Formation of
Academic Paper
Establishment of Advocacy
team
Preparation and
development of RAD
Monitoring of TB/HIV Services
Capacity building,
advocacy and fundraising
Advocacy Strategy

Indonesia
National TB Program
Thank You