in the name of god history and physical examinations hassan ghobadi md assistant professor of...
TRANSCRIPT

In the name of GOD
History and Physical Examinations
Hassan Ghobadi MD
Assistant Professor of Internal Medicine
Ardabil University of Medical Science

MEDICAL INTERVIEW
CHIEF COMPLAINT AND PRESENT ILLNESS MAJOR PULMONARY SYMPTOMS FAMILY AND SOCIAL HISTORIES PAST HISTORY SYSTEMS REVIEW QUESTIONNAIRES
PHYSICAL EXAMINATION

Symptoms & Signs
Dyspnea (Breathlessness) Cough Chest pain Hemoptysis Palpable mass Audible wheeze An abnormal chest finding on imaging

Dyspnea( Breathlessness )
History and Physical Examinations

Dyspnea
Unpleasant sensation of breathing.
Dyspnea implies that the awareness is disproportionate to the stimulus and, the sensation is abnormally uncomfortable.
The sensation experienced by normal subjects during physical exertion is described as “ shortness of breath," not as dyspnea .
Many patients describe their breathing discomfort as: "breathlessness," "tightness," "choking," "inability to take a deep breath," "suffocating," and simply "can't get enough air.

Dyspnea
Dyspnea occurs in healthy subjects under stress (e.g., exercise, altitude).
In patients with an underlying disorder it may occur with little or no exertion.
Dyspnea is a term used to characterize a subjective experience of breathing discomfort
Mechanisms of Dyspnea
There are no known specialized dyspnea receptors. The mechanisms of dyspnea are incompletely understood . Mechanisms are multifactorial. Interactions between the efferent motor output from the brain
to the ventilatory muscles and the afferent. Disorders of the ventilatory pump are associated with
increased work of breathing or a sense of an increased effort to breathe
A discrepancy or mismatch between the feed-forward message to the ventilatory muscles and the feedback from receptors that monitor the response of the ventilatory pump increases the intensity of dyspnea.

Mechanisms of Dyspnea
Dyspnea may occur when there is :
1- Increased central respiratory drive secondary to hypoxia, hypercapnia, or other afferent input;
2- Augmented requirement for the respiratory drive to overcome mechanical constraints or weakness; and
3- Altered central perception.

Mechanisms of Dyspnea
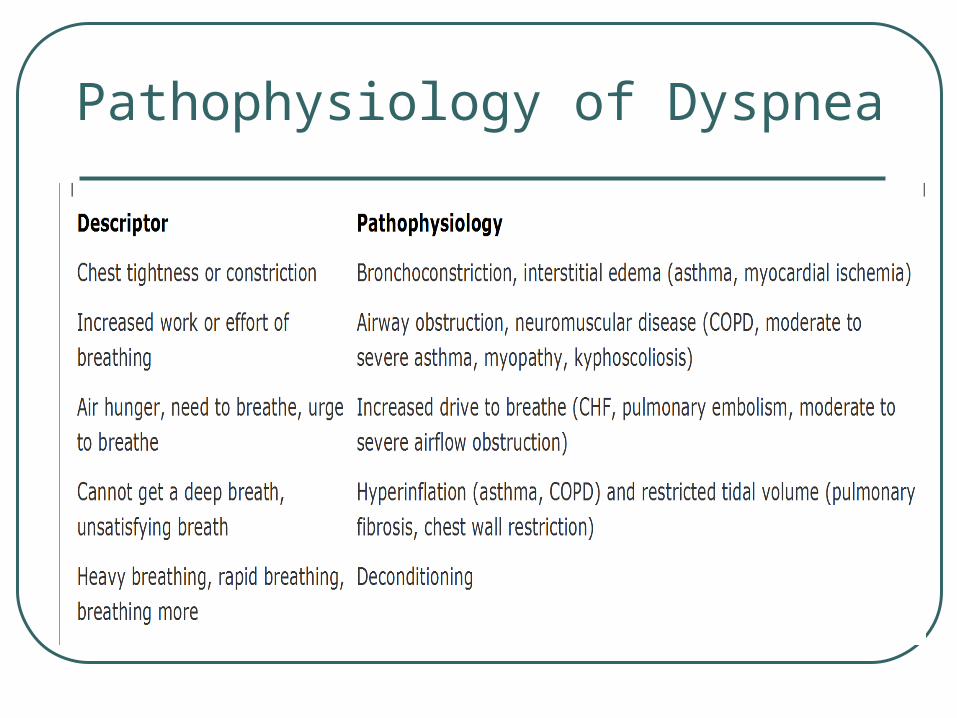
Pathophysiology of Dyspnea

Pathophysiology of Dyspnea

Intensity of Dyspnea
Clinicians generally rely on a combination of patients' reports and physiologic measurements (e.g., FEV1) to evaluate dyspnea
Modified Borg scale Visual analogue scale Chronic Respiratory Disease Questionnaire

Diseases Causing Dyspnea
1- Mechanical Interference with Ventilation Obstruction to airflow (central or peripheral) Asthma, emphysema, bronchitis, Endobronchial tumor ,Tracheal or laryngeal stenosisResistance to expansion of the lungs ("stiff lungs") Interstitial fibrosis of any cause , Left ventricular failure ,
Lymphangitic tumorResistance to expansion of the chest wall or diaphragm
Pleural thickening or "peel" (e.g., empyema) Kyphoscoliosis , Obesity ,
Abdominal mass (e.g., tumor, pregnancy)

Diseases Causing Dyspnea
2 - Weakness of the Respiratory Pump
Absolute Prior poliomyelitis, Neuromuscular disease (e.g.,
Guillain-Barré syndrome, muscular dystrophy, systemic lupus erythematosus, hyperthyroidism)
Relative
(i.e., muscles at a mechanical disadventage ) Hyperinflation (e.g., asthma, emphysema) ,
Pleural effusion ,Pneumothorax

Diseases Causing Dyspnea
3 - Increased Respiratory Drive
a- Hypoxemia of any causeb- Metabolic acidosis Renal disease (failure or tubular acidosis) Decreased effective hemoglobin (e.g., anemia, hemoglobinopathy) Decreased cardiac outputc- Stimulation of intrapulmonary receptors
infiltrative lung disease, pulmonary hypertension, pulmonary edema

Diseases Causing Dyspnea
4 -Increased Wasted Ventilation
Capillary destruction
(e.g., emphysema, interstitial lung disease)
Large-vessel obstruction
(e.g., pulmonary emboli, pulmonary vasculitis)

Diseases Causing Dyspnea
5 - Psychological Dysfunction
Bodily preoccupation ( somatization)
Anxiety ( hyperventilation syndrome)
Depression
Involvement in litigation
( alleged respiratory injury)

Respiratory System Dyspnea
1- ControllerAcute hypoxemia and hypercapnia, bronchospasm (asthma),
interstitial edema, pulmonary embolism, High altitude, high progesterone states (pregnancy), drugs (aspirin).
2- Ventilatory PumpIncreased airway resistance (e.g., asthma, emphysema, chronic
bronchitis, bronchiectasis).increased airway resistance and work of breathing (kyphoscoliosis, Guillain-Barré syndrome, pleural effusions).
3- Gas ExchangerPneumonia, pulmonary edema, ILD, Pulmonary vascular disease.
Cardiovascular System Dyspnea
1- High Cardiac Output Anemia, Left-to-right intracardiac shunts, obesity .
2- Normal Cardiac Output
Deconditioning, Diastolic dys., Pericardial disease 3- Low Cardiac Output coronary artery disease, cardiomyopathies

Approach to Dyspnea
HISTORY. A comprehensive medical history is important for a diagnosis
of dyspnea PHYSICAL EXAMINATION. Pattern of breathing , body habitus (e.g., cachexia, obesity),
posture (e.g., leaning forward on elbows as in COPD), skeletal deformity, Cough on deep inspiration or expiration suggests asthma or interstitial lung disease
DATABASE. Anemia , Polycythemia , chest radiography, spirometry, and
possibly electrocardiography SPECIAL STUDIE. Pulmonary function tests , Pulse oximetry , Spiral CT scanning ,
Gallium CT scanning , cardiac catheterization .

Approach to Dyspnea
Orthopnea is a common indicator of congestive heart failure,
mechanical impairment of the diaphragm associated with obesity,
Asthma triggered by esophageal reflux.
Nocturnal dyspnea suggests congestive heart failure or asthma. Acute, intermittent episodes of dyspnea are more likely to reflect
episodes of myocardial ischemia, bronchospasm, or pulmonary embolism,
Chronic persistent dyspnea is typical of COPD and interstitial lung disease.

Approach to Dyspnea
Severity of dyspnea
Inability of the patient to speak in full sentences
Evidence for increased work of breathing (supraclavicular retractions, use of accessory muscles of ventilation, and the tripod position) is indicative of disorders of the ventilatory pump.
When measuring the vital signs, an accurate assessment of the respiratory rate should be obtained and examination for a pulsus paradoxus ; if it is >10 mm Hg, consider the presence of COPD.
During the general examination, signs of anemia (pale conjunctivae), cyanosis, and cirrhosis (spider angiomata, gynecomastia) should be sought.

Dyspnea: Treatment
Correct the underlying problem responsible for the symptom and its complications .
If this is not possible, one attempts to lessen the intensity of
the symptom and its effect on the patient's quality of life .
Supplemental O2 should be administered if the resting O2 saturation is < 90% .
For patients with COPD, pulmonary rehabilitation programs have demonstrated positive effects on dyspnea, exercise capacity, and rates of hospitalization .

Dyspnea: Treatment (1)
Reduce Sense of Effort and “ Improve Respiratory Muscle Function “
Energy conservation (e.g., pacing) Breathing strategies (e.g., pursed-lip breathing) Position (e.g., leaning forward) Correct obesity or malnutrition Inspiratory muscle exercise Respiratory muscle rest (e.g., cuirass, nasal
ventilation, transtracheal oxygen) Medications (e.g., theophylline)

Dyspnea: Treatment (2)
Decrease Respiratory Drive
Oxygen Opiates and sedatives Exercise conditioning Vagal nerve section (not done) Carotid body resection (not done)

Dyspnea: Treatment (3)
Alter Central Nervous System Function
Education Psychological interventions (e.g., coping
strategies, psychotherapy, group support) Opiates and sedatives

Dyspnea: Treatment (4)
Exercise Training (Pulmonary Rehabilitation)
Enhance self-esteem and self-confidence in ability to performImprove efficiency of movementDesensitization to dyspnea
(i.e., from repeated exercise)

چنان کن سرانجام کار تو خشنود باشی و خدایاما رستگار