improving quality of newborn care in hoima...
TRANSCRIPT
IMPROVING QUALITY OF NEWBORN CARE IN HOIMA REGION THROUGH A REGIONAL LEARNING NETWORK
A collaborative effort of Uganda ministry of Health, Save the Children
and University Research Company
IHI Africa Forum for Quality and Safety Durban, South Africa
February 20th 2018
Cutting Edge MNCH programming from across Africa
University Research Co., LLC
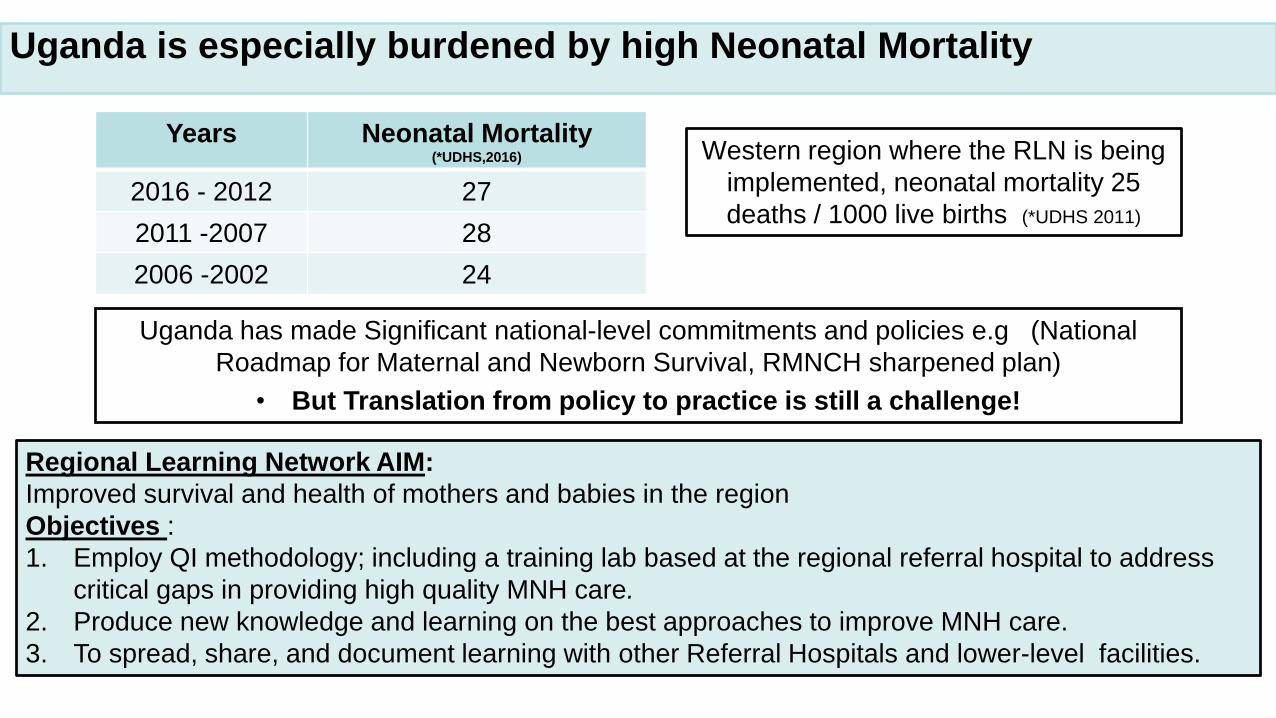
Uganda is especially burdened by high Neonatal Mortality
Years Neonatal Mortality (*UDHS,2016)
2016 - 2012 27
2011 -2007 28
2006 -2002 24
Western region where the RLN is being
implemented, neonatal mortality 25
deaths / 1000 live births (*UDHS 2011)
Regional Learning Network AIM:
Improved survival and health of mothers and babies in the region
Objectives :
1. Employ QI methodology; including a training lab based at the regional referral hospital to address
critical gaps in providing high quality MNH care.
2. Produce new knowledge and learning on the best approaches to improve MNH care.
3. To spread, share, and document learning with other Referral Hospitals and lower-level facilities.
Uganda has made Significant national-level commitments and policies e.g (National
Roadmap for Maternal and Newborn Survival, RMNCH sharpened plan)
• But Translation from policy to practice is still a challenge!
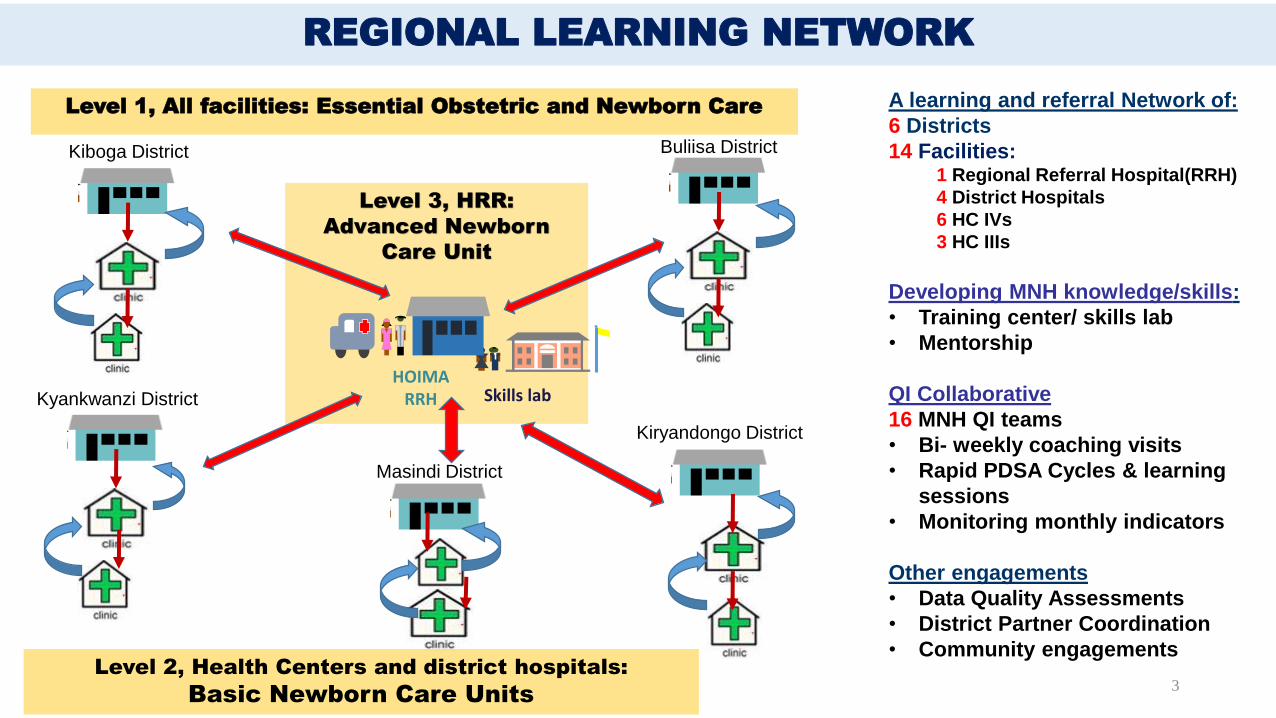
Level 1, All facilities: Essential Obstetric and Newborn Care
Level 3, HRR:
Advanced Newborn
Care Unit
REGIONAL LEARNING NETWORK
3
Skills lab HOIMA
RRH
Kiboga District
Masindi District
Kiryandongo District
Buliisa District
Kyankwanzi District
A learning and referral Network of:
6 Districts
14 Facilities:1 Regional Referral Hospital(RRH)
4 District Hospitals
6 HC IVs
3 HC IIIs
Developing MNH knowledge/skills:
• Training center/ skills lab
• Mentorship
QI Collaborative
16 MNH QI teams
• Bi- weekly coaching visits
• Rapid PDSA Cycles & learning
sessions
• Monitoring monthly indicators
Other engagements
• Data Quality Assessments
• District Partner Coordination
• Community engagementsLevel 2, Health Centers and district hospitals:
Basic Newborn Care Units

THE TRAINING/SKILLS LAB.
AIM:
• Provide for practical in-service and pre-service training for health workers, medical and nursing students
Model:
• Practical setting with hands-on skills combined with theoretical session
Curriculum:
• Comprehensive context specific to MNH
98% (151/157) of MNH health workers trained in the region
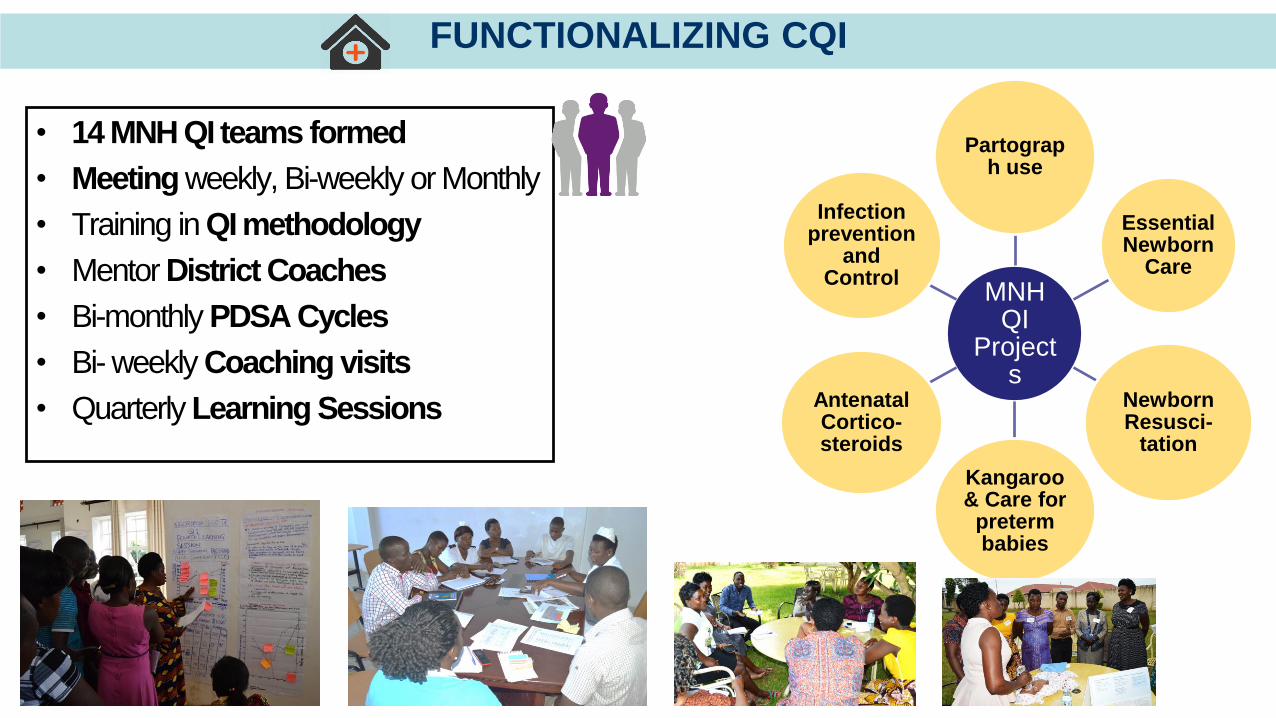
FUNCTIONALIZING CQI
• 14 MNH QI teams formed
• Meeting weekly, Bi-weekly or Monthly
• Training in QI methodology
• Mentor District Coaches
• Bi-monthly PDSA Cycles
• Bi- weekly Coaching visits
• Quarterly Learning Sessions
MNH QI
Projects
Partograph use
Essential Newborn
Care
Newborn Resusci-
tation
Kangaroo & Care for
preterm babies
Antenatal Cortico-steroids
Infection prevention
and Control

6
Basic Drugs and Supplies Basic EquipmentKnowledge Check
Topic Baseline Endline
Components
of ENC73% 96%
KMC 31% 62%
Infection
control84% 100%
Resuscitation Equipment Baseline Endline
Adequate surface 21% (3/14) 100%
Oxygen cylinder 31% (4/14) 62%
Bag & Mask 71% (10/14) 100%
Penguins 0% 85 % (12/14)
64 64
14 14
77
92
38
93
Incubator OxygenConcentrator
oxygenCylinder
infantwarmer
Baseline Endline
64
86
43 50
7
72 64
0
7792
38
93
8
100 100 100
Baseline Endline
Pre-term Care Baseline Endline
# cases Identified 30 275
Gestation Age Assessed 0 40%
KMC 0% 100%
Referred 40% 3%
Progress in Key inputs and processes of Care June 2016 (Baseline) –June 2017 (Endline)
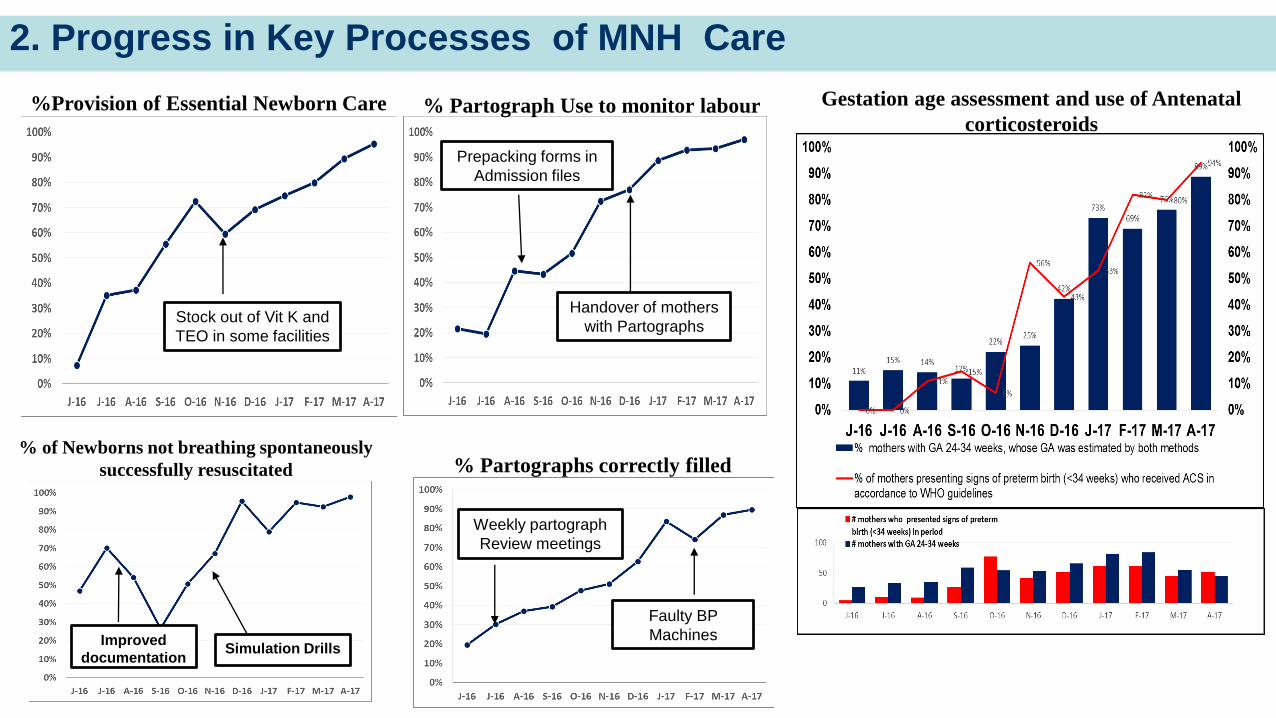
2. Progress in Key Processes of MNH Care
7
Stock out of Vit K and
TEO in some facilities
Handover of mothers
with Partographs
Weekly partograph
Review meetings
Faulty BP
Machines
Prepacking forms in
Admission files
Improved
documentationSimulation Drills
%Provision of Essential Newborn Care % Partograph Use to monitor labour
% of Newborns not breathing spontaneously
successfully resuscitated % Partographs correctly filled
Gestation age assessment and use of Antenatal
corticosteroids

3. Progress in outcome indicators in 14 Facilities of the RLN
8
Reduction
in Referrals
Identify space within or close to the maternity ward
Equip the unitwith essential
equipment and supplies
Provide Newborn caretrainings for
staff
Improvedocumentation.
Set up of Newborn Care Units
Early Institutional Newborn mortality Fresh Still Births and Partographs
correctly filledDeaths due to prematurity and
Provision of KMC

Reflections
1. Improvements in the availability of essential inputs, knowledge of evidence-based
care among health care providers, and delivery of key MNH services can make a
substantial difference to improving the outcomes of mothers and newborns
2. Improving health worker knowledge, skills and work environment boosts confidence,
reduces on unnecessary referrals and is a big motivator for health workers
3. The experience of the Regional Learning Network in using QI techniques and
hands-on skills training to improve MNH care by tackling the above dimensions of
quality demonstrates evidence of this and provides useful insight for spread tp other
facilities seeking to improve MNH care in similar settings.
9
A collaborative effort of Ministry of Health Uganda, Save the Children and University Research Co., LLC