improving health systems the role of design thinking and ... · improving health systems – the...
TRANSCRIPT

Improving Health Systems –
The Role of Design Thinking and
Operations Research
Dr Mark Mackay
Mr Keith Stockman
Professor Robert Adams
Professor Don Campbell
10 May 2016

Questions?
Use the Ask a Question Box to type in
Questions at any time during our presentation
We may answer it when we see it or at the end
of the presentation
Remember - if you don’t know, it’s likely
others don’t know too, so please ask your
questions.

The Cumberland Initiative
• Cumberland Initiative – promotes the
use of operational research and
systems thinking in health
• Aim to save 20% of annual NHS budget
by 2020 (ok a stretch target)!
• See www.cumberland-initiative.org
• Australian “branch” cumberland.au

4
A multi-D and
multi-country
Group!
Plus authors from UK CI!

Cumberland.au
• The Australian arm of the UK
Cumberland Initiative
• Most recently a joint piece in “The
Conversation”
• Various grant activities e.g., Adelaide
we are modelling RAH ICU and
embarking on other modelling
• Monash has been applying this work for
some time
5

Politicians and Media…& Health
6

Sustained Period of Costs Increasing
For every dollar spent in health it means it’s one
dollar not spent elsewhere or on additional patients.
7
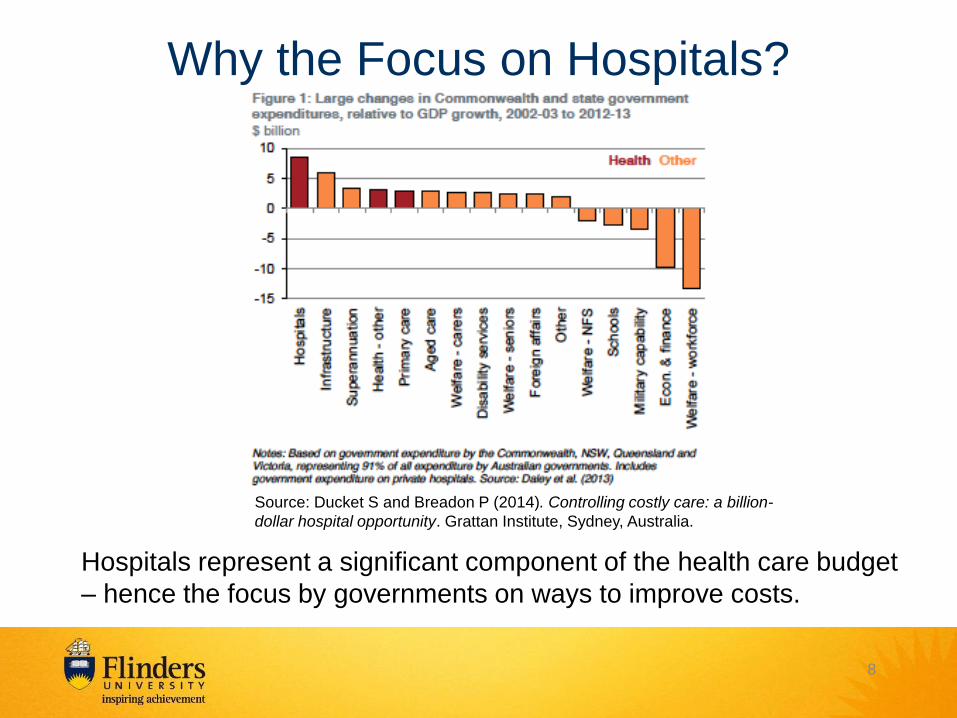
Why the Focus on Hospitals?
Hospitals represent a significant component of the health care budget
– hence the focus by governments on ways to improve costs.
Source: Ducket S and Breadon P (2014). Controlling costly care: a billion-
dollar hospital opportunity. Grattan Institute, Sydney, Australia.
8

Getting Ready for Change!
9
First published in The health advocate Oct 2013

What’s a System?
10

Critical Systems Thinking and Practice
1. A system is an organized assembly of elements and special
relationships between the elements. If the elements or
relationships change the system changes.
2. Each element contributes to the system’s behaviour and is
affected by it.
3. A system exhibits emergent properties that none of its
components have individually. Emergence is a characteristic of the
particular case.
4. Sub-groups of a system may have the above properties – they
form sub-systems.
5. A system has an outside – its environment and boundaries that
determine what is in the system or not in the system. [A system
can influence but not control its environment.]
6. A system transforms inputs from the environment to outputs to
the environment Slide by Dr Don Houston, Centre for
University Education, Flinders University

A hospital – a systems dynamics view
12

Complicated
• A plane is
complicated
• But it has
reliable
performance –
you can
expect the
same result
each time
14

Mapping patient flow across the hospital system
15
There has been
many attempts to
improve patient
flow – usually
based upon
simple “fixes”.
For every
complex problem
there is an
answer that is
clear, simple, and
wrong. H. L.
Mencken
Hospitals are Complex Service Environments

Design and Health
Every system is perfectly designed to
achieve the results it achieves Berwick
(1996, pg 619). [highlight is my emphasis]
Berwick DM (1996). A primer on leading the improvement of systems. BMJ,
312: 619-22.
So all the bugs in the system – they’re design
outcomes.
They may be planned or unintended
consequences of design problems.
16

Design Thinking
1. How we got to here
2. What is it
3. Some key properties
4. Our experiences
17

How we
got to here

19
Every system is
perfectly designed
to achieve the
results it achieves
Berwick
Berwick DM (1996). A primer
on leading the improvement of
systems. BMJ, 312: 619-22.

http://www.systemdynamics.org/DL-IntroSysDyn/bwb.htm
Painful lessons learnt

Horses for courses
Diagram by Dave Snowden, Cynefin 21

22

We are
not
alone
23

What is DT?


26

27

Diagram by Hugh Dubberly 28

Diagram by Hugh Dubberly 29

Designing Thinking Process
Diagram by Jeanne Liedtka 30
“It’s a
systematic
approach to
problem
solving”
Liedtka & Ogilvie
2011 Designing for
Growth, Columbia
Business School,
New York, pg. 5

Some Key
Properties

• Human Centred
–Experience, needs & desires
–Empathy
–Multiple perspectives
• Constraints part of the fun!
32

• Divergence
then
convergence +
synthesis
• Systems
Thinking in
action!
33

34
Extensive
use of
models &
visualisation
Large set of
methods &
tools

Diagram by Hugh Dubberly 35

• Prototyping
• Test user
insights &
experience
interactively
• “Fail often,
fail early”
36

How is DT different from the re-design
we have been doing for years?
• Complementary to other system design approaches
such as LEAN, TOC, Six Sigma
• Useful in the Complex Domain in which there are
many ”Wicked Problems”
• More emphasis on understanding consumer
experience and needs from multiple perspectives
• Less prone to “picking from our favourite solutions –
again!”
• Encourages creativity
• User co-design goes well beyond asking “What do
you want”
37

Our experiences
• Avoidable hospitalisation
• Hand Hygiene
• Make-a-thon series
• Long-stays
• Arrival at hospital
• Mental Health
• Community care
38
Pain points - implementation needs good design
- all design has a political dimension

Challenges for DT
• Health staff understanding and skills
• Adequate time and “creative energy”
• Mixing it more with the Designers
outside health
• Organizational nurturance
• Evidence of value
39
Outcomes from Design Thinking can
only be judged via scientific
evaluation. Ultimately that is the only
way to judge Design Thinking itself
Evaluation needs to include
consumer experience which is in the
end how value manifest
40


A Definition & Implications
“Planning and control of processes that
transform inputs into outputs”
(Vissers and Beech, 2005)
Really it brings together many areas that you
study – knowledge of organisations, people and
$ - and combines them with some tools.
While the tools may have an engineering,
operations research or similar basis –
application is a matter of judgment and/or art.

Simulation and Health Care
• While you may not have encountered it - it’s
not new!
• Discrete event simulation (useful for
modelling processes) has been used for:
– Planning new capacity (ED, outpatients, etc.)
– Improving patient flow or workflow
• There are many papers
• As Fone et al. (2003) highlighted – little
evaluation of such work & to date this is still
true.
43

So What is Simulation Modelling?
• Simulation is one of
OR’s tools
• It’s a means of
creating a
computerised model
of a real system
• Various uses –
asking “what-if”
questions,
understanding, etc.
44

We’re not talking about simulation for
training health professionals e.g., “smart”
manikins for training purposes
45


The Point of Simulation
• Given that the system is complex and isn’t
perfect, how should “bugs” be fixed or
improvements tested… without causing more
harm?
• Simulation is the answer!
• It provides a mechanism to pre-test ideas –
many more ideas than could be tried in real
life – without investing in any real change.
47

Systems Thinking & Design Thinking &…
48
Operations
Management
Design Thinking
Systems Thinking Best Solutions –
takes it all
Giving Some Context to
Operations Management

Ambulance Ramping
50

ED Overcrowding
51

Enough Beds?

Waiting for Services
53

Logistics
54

10/05/2016 55
Logistics (cont.) - Work Time Lost
Valuable time spent on logistics – waiting for things to be found or
provided
Proportion of Time Spent by Function
100 Service Delivery
62%
200 Administrative Duties
9%
300 Logistic Support
8%
400 Workforce Management
16%
500 Research
0%
600 Rostered & other breaks
5%

Forecasting
56

Variation
Not all hospitals are the same!
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
0 1 2 3 4 5
Cost$
Hospital
Re-crea onofDucke andBreadon2014Figure11:Costoflaparoscopiccholecystectomies,highvolumehospitals,2010-11
cost.of.procedure
median_cost
57

58
Case Study: Stroke Care

Modelling stroke care systems :
Evidence of the benefits in the NHS*
• Simulation to test-drive options for managing suspected stroke patients – minimise time to treat and maximise the benefit to patients.
• Two process changes following the modelling. – First, ambulances by-pass A&E with all suspected stroke patients.
• The acute stroke team are instead alerted to pending arrivals as patients are transported to hospital.
– Second, senior A&E nurses alert the acute stroke team of any suspected strokes that have self-presented as they are triaged.
• This by-passes any lengthy wait for physicians in A&E.
• As a result of this, the Royal Devon and Exeter Foundation Trust now treats four times as many stroke patients in half the time.
*cumberland-initiative.org

Results
60

Results (cont.)
61

Do We Really Need to Model? From Cumberland Initiaitve and the Stroke Model:
The question is why did we need to model it? The trouble is that
many ‘obvious’ improvements are simply not implemented
successfully or sustainably. You need to convince a lot of people
to change their practice and the model helped to do just that. In
this case modelling translated the evidence of the clinical
effectiveness of rtPA into a local context. The magnitude of the
improvement predicted by the model both in terms of treatment
rates and post-stroke disability made it more real for clinicians in
the hospital and convinced them to implement the changes.
Benefits (Monks T, (2015) Modelling stroke care systems : Evidence of the
benefits. www.cumberland-initiative.org date accessed 2 September 2015).
62


The flaw of averages • In 1950s USAF accidents were very common
• Problem thought to be cockpit design and size
• Initial solution- measure 4000 pilots and get average
dimensions and use in design
• Then someone asked, “How many pilots are actually
average?”
• So, calculated average of 10 physical dimensions
– Average was defined as middle 30% of range on each
• Found-
– not 1 of 4,063 pilots were within the average range on all 10
dimensions
– Less than 3.5% were average on any 3 dimensions

Implications • There was no such thing as an average pilot. If you’ve designed
a cockpit to fit the average pilot, you’ve actually designed it to fit
no one.
• “The tendency to think in terms of the ‘average man’ is a pitfall
into which many persons blunder,”
Lt. Gilbert S. Daniels
1952
• “any system designed around the average person is doomed to
fail
• environments need to fit the individual rather than the average”
The End of Average
L Todd Rose
65

Other Uses?
66

Duckett’s Advice
• Although anecdotes help to sell policies, they
shouldn’t be the basis of policy development. If they
are, they will almost certainly distort policymakers’
perceptions and start them down the wrong paths.
• Data should be used to … model the effects of new
policies.
• Organisations need to invest in the mindset and skills
to use data in policy, and have the mandate to do so.
Duckkett, S (2014). Forget the co-payment… Seven tips for an
affordable, quality health system. The Conversation, 19 August
2014.

68
Making it Happen
It starts with a good question!

Do Good Questions Matter? • Yes!
• Jeff Foote (NZ) – set out to determine an
algorithm for improving hospital capacity
(PhD) – determined it couldn’t be done
• SA Health simulation project – project leader
realised that they’d been asking the wrong
questions
• Researchers also ask the question e.g., • Fackler, J., & Spaeder, M. (2011, December). Why doesn't healthcare
embrace simulation and modeling? What would it take?. In Simulation Conference (WSC), Proceedings of the 2011 Winter (pp. 1137-1142). IEEE.
69

So What Does it Take to Ask A Good
Question?
Understanding:
• Constraints
• Politics
• Methods
• Timing
• Stakeholders
• Knowing what the real problem is
• Appreciation of the system
• Understanding your biases

Context Alters the Frame or Perspective
71

Consideration of the systemic characteristics
of an operation management project
should lead to a better question and method
Context & boundaries
Participants perspectives
YOU
knowledge
Context & boundaries
Participants’ perspectives
Issue/problem
methodology
purpose
Politics
power ethics
Action Learning Projects – Understanding the Characteristics of the Project
Alternative – start with the method and make
the situation fit the method. Reduce
probability of delivering what’s needed – but
happens.
Based on a slide by Dr Don Houston, Centre for
University Education, Flinders University

And of course … it takes a variety of people
73
Making it
Happen
Computer Scientists
Medical Officers
Allied Health
Patients Process
Improvement Teams
Economists
Statisticians
Nurses Mathematicians
Social Scientists
Psychologists
It’s multi-disciplinary

74
So What is Happening
Locally?

Want to Learn More
• A Cumberland.au website coming soon
– email us if you want to be on a contact
list
• A conference is planned for later this
year – keynote speakers include Hugh
Dubberly (USA) and Terry Young (UK)
• Take some courses (e.g., MHA at
Flinders includes a subject on
operations management)
75

76
And Finally…

Know Your Business
To manage a business or any part of
that business you need to … know your
business. This means understanding:
• How it functions
• What resources it has, and
• Its strengths and weaknesses.
And have some tools to help improve it!
Simulation is one of these tools!
77

It’s Time to Address the Streetlight Effect
And… health services research has a role to play in improving
health care management
