impaired renal function is not associated with increased volume of intracerebral hemorrhage
TRANSCRIPT

Impaired Renal Function Is N
ot Associated with IncreasedVolume of Intracerebral HemorrhageShawna Cutting, MD,* Chloe Castro, BS,* Vivien H. Lee, MD,*
and Shyam Prabhakaran, MD, MS†
From *Department o
Medical Center; and †
University, Chicago, Illin
Received August 3,
accepted September 19, 2
Address corresponden
sity Medical Center, De
W Harrison St, Ste 1121,
rush.edu.
1052-3057/$ - see front
� 2014 by National Str
http://dx.doi.org/10.1
86
Background: Patients with low glomerular filtration rate (GFR) are at risk for hemor-
rhagic stroke and experience poor long-term outcomes after stroke. These associa-
tions may be mediated by hematoma volume. We investigated the relationship
between impaired renal function (GFR ,60 mL/min/1.73 m2) and hematoma
size. Methods: Consecutive patients admitted with spontaneous intracerebral hem-
orrhage (sICH) between August 2006 and January 2010 were evaluated; patients
with acute kidney injury or end stage renal disease were excluded. Data on patient
demographics, admission creatinine, size and location of bleed, and disposition at
discharge were collected. Hematoma size and location and discharge outcomes
were compared among those with normal and impaired renal function. Results:Among 573 patients admitted with sICH, 411 met our study criteria (mean age
61.4 years; 52.3% female; median ICH volume 11.2 mL). Mean GFR was 73.8 mL/
min/1.73 m2, and 99 patients (24.1%) had a GFR ,60 mL/min/1.73 m2. There
was no correlation between admission GFR and ICH volume (rs 5 0.014; P 5 .77);
those with GFR ,60 versus $60 mL/min/1.73 m2 also had similar ICH volumes
(median 10.8 v 11.4 mL; P5 .54). There was no association between in-hospital mor-
tality and admission GFR, although those with GFR ,60 mL/min/1.73 m2 were
more likely to die or be discharged to nursing homes (adjusted odds ratio 1.9;
P 5 .03). Conclusions: In a large sICH cohort, impaired renal function was not
associated with final hematoma volume. Additional study should focus on
the mechanism by which renal function impacts functional outcomes after
sICH.KeyWords: Cerebral hematoma—glomerular filtration rate—kidney disease.
� 2014 by National Stroke Association
There is increasing interest in the relationship between
abnormal kidney function and spontaneous intracerebral
hemorrhage (sICH). Patients with low glomerular filtra-
tion rate (GFR) are known to have endothelial and platelet
dysfunction and are at risk for both thrombotic and hem-
orrhagic events.1 Those with low GFR are at greater risk
f Neurological Sciences, Rush University
Department of Neurology, Northwestern
ois.
2012; revision received August 29, 2012;
012.
ce to Shawna Cutting, MD, Rush Univer-
partment of Neurological Sciences, 1725
Chicago, IL 60612. E-mail: shawna_cutting@
matter
oke Association
016/j.jstrokecerebrovasdis.2012.09.010
Journal of Stroke and Cer
for hemorrhagic than ischemic stroke and experience
poorer long-term outcomes after stroke.2 Previous studies
have suggested that patients with chronic kidney disease
have larger lobar hemorrhages and increased mortality.3,4
We sought to validate whether kidney function was asso-
ciated with hematoma volume and discharge outcomes in
a large cohort of patients with sICH.
Methods
With institutional review board approval, all patients
hospitalized at our institution with sICH between August
2006 and January 2010 were prospectively entered into
an acute stroke registry. Exclusion criteria included:
(1) patients ,18 years of age; (2) patients with vascular
anomalies, such as aneurysm, arteriovenous malforma-
tion, fistula, or venous sinus thrombosis; (3) patients
ebrovascular Diseases, Vol. 23, No. 1 (January), 2014: pp 86-90

RENAL FUNCTION AND INTRACEREBRAL HEMORRHAGE 87
taking anticoagulant medications with heparin or warfa-
rin at time of presentation; (4) patients who were trans-
ferred from community hospitals with only an initial
scan and death within 24 hours (because of the inability
to calculate final hematoma volume); and (5) patients
who were later determined to have an underlying mass
on follow-up contrast-enhanced imaging.
Data collected included age, sex, race, current use of
antiplatelet medications, hypertension, initial Glasgow
Coma Scale (GCS) score, blood urea nitrogen and creati-
nine levels at admission, current smoking status, length
of hospital stay, and disposition at discharge. Data were
not consistently available regarding duration of antiplate-
let drug use before presentation or dose of aspirin. ICH
score was calculated using the previously published scor-
ing system.5 We defined poor outcome as discharge to
skilled nursing facility, hospice care, or in-hospital death.
Patients with end stage renal disease were excluded be-
cause of the potential confounder of heparin use during
dialysis. Patients with acute kidney injury were also ex-
cluded from our analysis because accurate measurements
of renal function were difficult to determine in this set-
ting. We defined acute kidney injury as a rise in creatinine
of 0.3 mg/dL over baseline, a definition based on ac-
cepted definitions for acute kidney injury.6 We used dis-
charge creatinine as a surrogate marker for baseline in
the absence of other data points, such as previous preho-
spitalization values. GFR was calculated using the Modi-
fication of Diet in Renal Disease (MDRD) equation.7
Impaired renal function was defined as ,60 mL/min/
1.73 m2.
The 24-hour computed tomography (CT) scan obtained
at our institution was reviewed by 1 study neurologist
(Dr. Lee), and final hematoma volume was calculated us-
ing the ABC/2 method as previously described.8 Hemor-
rhages were grouped into 4 locations: basal ganglia or
thalamus, lobar, infratentorial, or other (including multi-
ple locations or intraventricular hemorrhage). For our pri-
mary hypothesis, we performed correlational statistics
using the Spearman coefficient for the relationship be-
tween GFR and final intracerebral hemorrhage (ICH) vol-
ume and compared median hematoma volumes in
patients with normal versus impaired renal function us-
ing theMann–Whitney test. The relationships between re-
nal function and clinical factors, hematoma size, and
outcomes were assessed using the Student t or Mann–
Whitney test (for continuous variables) and the Chi-
square or Fisher exact test (for categorical variables).
Multivariable logistic regression analyses assessedwhether
kidney function was a predictor of poor discharge out-
come independent of known predictors, including the
ICH score and its individual elements. Adjusted odds ra-
tios (ORs) and 95% confidence intervals (CIs) were esti-
mated from the final model.
Data analysis was performed using SPSS software (ver-
sion 16.0; SPSS Inc, Chicago, IL). P , .05 was considered
statistically significant in all analyses. With our sample
size, we had .90% power to detect hematoma volume
differences of at least 5 mL between those with normal
and impaired renal function and 80% power to detect
an increased OR of early mortality of at least 1.72.
Results
Five hundred seventy-three patients were identified
with sICH. We excluded a total of 162 patients because
of end-stage renal disease (n 5 36), acute kidney injury
(n 5 104), missing data (n 5 11), or death before the final
CT scan (n 5 11). The remaining 411 patients ranged in
age from 25 to 96 years (mean 61.4 6 14.7 years); 52.3 %
were female. The median volume of hemorrhage was
11.2 mL (interquartile ratio 3.5-33.9 mL); 117 patients
(28.5%) had a large (.30 mL) hemorrhage volume. Two
hundred eight (50.6%) hemorrhages were located in the
basal ganglia or thalamus; 64 (15.6%) were infratentorial;
and 139 (33.8%) were lobar. Intraventricular extension
was observed in 179 (43.6%) patients. Mean GFR was
73.8 6 23.6 mL/min/1.73 m2, and 99 patients (24.1%)
had a GFR ,60 mL/min/1.73 m2. Table 1 summarizes
the patient demographic, clinical, and hemorrhage char-
acteristics.
On univariable analysis, patients with impaired renal
function were older (mean age 66.1 vs 59.9 years;
P , .001) and more likely to have hypertension (83.8%
vs 66.3%; P , .01) and diabetes (28.3% vs 18.3%). There
was no linear correlation between admission GFR and
volume of hemorrhage (r2 5 0.014; P 5 .77). Those with
GFR ,60 versus $60 mL/min/1.73 m2 also had similar
median ICH volumes (11.4 vs 10.8 mL; P 5 .54) and had
similar proportions with large (.30 mL) volume (31.3%
vs 27.6%; P 5 .47). In stratified analyses, GFR was lower
in patients with infratentorial hemorrhages (66.8 vs 75.0
mL/min/1.73 m2; P 5 .01) compared to other sites. GFR
did not differ in the presence or absence of intraventricu-
lar hemorrhage (74.1 vs 73.5 mL/min/1.73 m2; P 5 .80).
There was no association between in-hospital mortality
and GFR analyzed as a continuous variable (74.2 vs 72.1
mL/min/1.73 m2; P 5 .54) or when GFR was dichoto-
mized (,60 mL/min/1.73 m2 [24.2%] vs $60 mL/min/
1.73 m2 [17.3%]; P 5 .125) or trichotomized ($60 mL/
min/1.73 m2 [17.3%] vs 45-60 mL/min/1.73 m2 [20.3%]
vs ,45 mL/min/1.73 m2 [30.0%]; P 5 .150). Those with
low GFR were less likely to be discharged to home or to
acute rehabilitation facilities (45.5% vs 62.8%; P 5 .002;
Fig 1).
Using multivariable logistic regression to determine
predictors of poor discharge outcome by adjusting for
ICH score (model 1—all elements of ICH score included
separately; model 2—ICH score dichotomized as ,2
and $2), GFR ,60 mL/min/1.73 m2 was independently
associated with greater odds of poor discharge outcome
(Table 2).
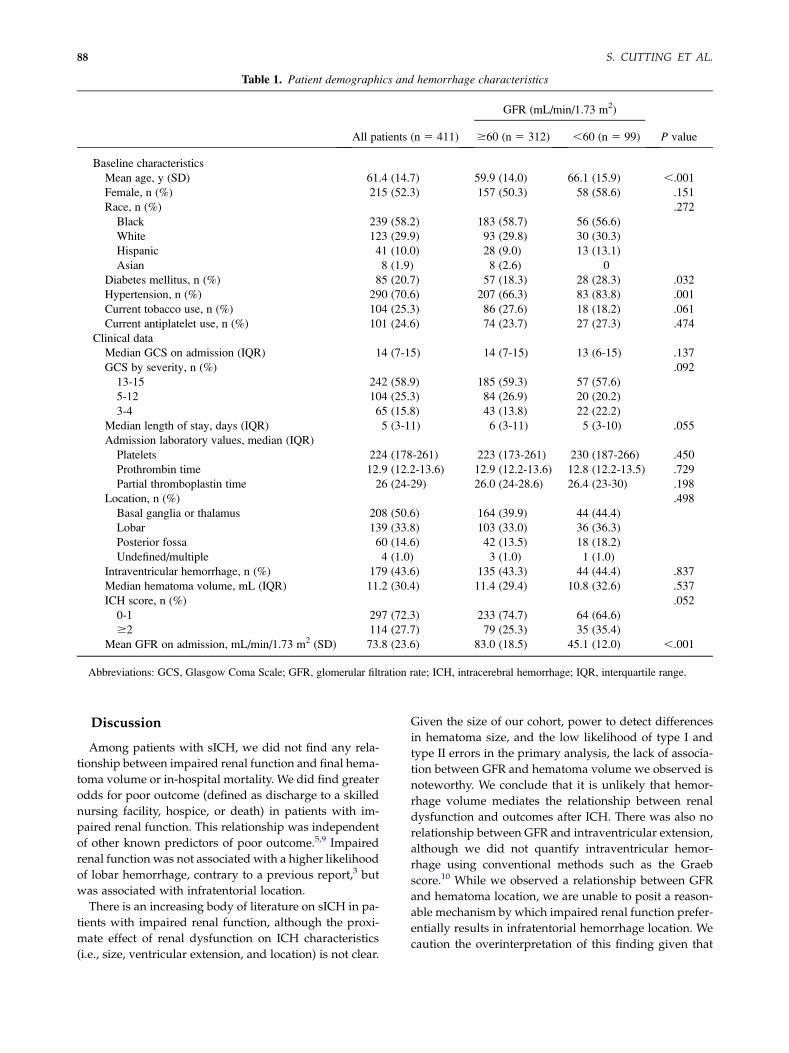
Table 1. Patient demographics and hemorrhage characteristics
All patients (n 5 411)
GFR (mL/min/1.73 m2)
P value$60 (n 5 312) ,60 (n 5 99)
Baseline characteristics
Mean age, y (SD) 61.4 (14.7) 59.9 (14.0) 66.1 (15.9) ,.001
Female, n (%) 215 (52.3) 157 (50.3) 58 (58.6) .151
Race, n (%) .272
Black 239 (58.2) 183 (58.7) 56 (56.6)
White 123 (29.9) 93 (29.8) 30 (30.3)
Hispanic 41 (10.0) 28 (9.0) 13 (13.1)
Asian 8 (1.9) 8 (2.6) 0
Diabetes mellitus, n (%) 85 (20.7) 57 (18.3) 28 (28.3) .032
Hypertension, n (%) 290 (70.6) 207 (66.3) 83 (83.8) .001
Current tobacco use, n (%) 104 (25.3) 86 (27.6) 18 (18.2) .061
Current antiplatelet use, n (%) 101 (24.6) 74 (23.7) 27 (27.3) .474
Clinical data
Median GCS on admission (IQR) 14 (7-15) 14 (7-15) 13 (6-15) .137
GCS by severity, n (%) .092
13-15 242 (58.9) 185 (59.3) 57 (57.6)
5-12 104 (25.3) 84 (26.9) 20 (20.2)
3-4 65 (15.8) 43 (13.8) 22 (22.2)
Median length of stay, days (IQR) 5 (3-11) 6 (3-11) 5 (3-10) .055
Admission laboratory values, median (IQR)
Platelets 224 (178-261) 223 (173-261) 230 (187-266) .450
Prothrombin time 12.9 (12.2-13.6) 12.9 (12.2-13.6) 12.8 (12.2-13.5) .729
Partial thromboplastin time 26 (24-29) 26.0 (24-28.6) 26.4 (23-30) .198
Location, n (%) .498
Basal ganglia or thalamus 208 (50.6) 164 (39.9) 44 (44.4)
Lobar 139 (33.8) 103 (33.0) 36 (36.3)
Posterior fossa 60 (14.6) 42 (13.5) 18 (18.2)
Undefined/multiple 4 (1.0) 3 (1.0) 1 (1.0)
Intraventricular hemorrhage, n (%) 179 (43.6) 135 (43.3) 44 (44.4) .837
Median hematoma volume, mL (IQR) 11.2 (30.4) 11.4 (29.4) 10.8 (32.6) .537
ICH score, n (%) .052
0-1 297 (72.3) 233 (74.7) 64 (64.6)
$2 114 (27.7) 79 (25.3) 35 (35.4)
Mean GFR on admission, mL/min/1.73 m2 (SD) 73.8 (23.6) 83.0 (18.5) 45.1 (12.0) ,.001
Abbreviations: GCS, Glasgow Coma Scale; GFR, glomerular filtration rate; ICH, intracerebral hemorrhage; IQR, interquartile range.
S. CUTTING ET AL.88
Discussion
Among patients with sICH, we did not find any rela-
tionship between impaired renal function and final hema-
toma volume or in-hospital mortality. We did find greater
odds for poor outcome (defined as discharge to a skilled
nursing facility, hospice, or death) in patients with im-
paired renal function. This relationship was independent
of other known predictors of poor outcome.5,9 Impaired
renal function was not associated with a higher likelihood
of lobar hemorrhage, contrary to a previous report,3 but
was associated with infratentorial location.
There is an increasing body of literature on sICH in pa-
tients with impaired renal function, although the proxi-
mate effect of renal dysfunction on ICH characteristics
(i.e., size, ventricular extension, and location) is not clear.
Given the size of our cohort, power to detect differences
in hematoma size, and the low likelihood of type I and
type II errors in the primary analysis, the lack of associa-
tion between GFR and hematoma volume we observed is
noteworthy. We conclude that it is unlikely that hemor-
rhage volume mediates the relationship between renal
dysfunction and outcomes after ICH. There was also no
relationship between GFR and intraventricular extension,
although we did not quantify intraventricular hemor-
rhage using conventional methods such as the Graeb
score.10 While we observed a relationship between GFR
and hematoma location, we are unable to posit a reason-
able mechanism by which impaired renal function prefer-
entially results in infratentorial hemorrhage location. We
caution the overinterpretation of this finding given that

Figure 1. Histogram of patient discharge disposition.
RENAL FUNCTION AND INTRACEREBRAL HEMORRHAGE 89
it was derived from stratified analyses andmay be subject
to type I errors. The causal link between renal disease,
platelet dysfunction, and hematoma characteristics re-
quires additional supporting evidence.
Decreased GFR is a risk factor for the development of
hemorrhagic stroke11 and has been linked to higher
odds of in-hospital mortality after ischemic and hemor-
rhagic stroke, particularly when severe disease (GFR
,15 mL/min/1.73 m2) or end-stage renal disease is pres-
ent.12,13 In a study of acute stroke patients, GFR,45 mL/
min/1.73 m2 was associated with an increased OR for
death at 1 month and 1 year, particularly after hemor-
rhagic stroke.2 However, the subset with hemorrhage
was small (112 patients), and patients with end-stage re-
nal disease were included. Proteinuria on admission
may be associated with poorer discharge functional activ-
ity and a lower likelihood of being discharged home di-
rectly for patients with ischemic stroke.14 A more recent
study involving 94 patients with ICH found that those pa-
tients discharged home were less likely to have a reduced
GFR or proteinuria on admission, although with multi-
variable analysis these associations were not statistically
significant.15 We confirm the impact of renal function
on discharge outcomes, although the relationship with
Table 2. Multivariate logistic regression analysis for poor
outcome (defined as skilled nursing, hospice, or death)
Adjusted OR (95% CI) P value
Model 1
GFR ,60 1.954 (1.074-3.555) .028
Age .80 y 2.743 (1.323-5.687) .007
IVH 2.972 (1.757-5.029) ,.001
ICH .30 mL 3.790 (2.145-6.695) ,.001
GCS ,12 3.458 (1.921-6.224) ,.001
Model 2
GFR ,60 1.802 (1.044-3.110) .034
ICH score $2 15.575 (8.979-27.017) ,.001
Abbreviations: CI, confidence interval; GCS, Glasgow Coma
Scale; GFR, glomerular filtration rate; ICH, intracerebral hemor-
rhage; IVH, intraventricular hemorrhage; OR, odds ratio.
short-term mortality was not present. Our study, despite
its larger size, focused on moderate renal disease, and
therefore the effect of severe dysfunction on volume
could not be robustly assessed.
We speculate that other factors, such as medical comor-
bidities and secondary insults (i.e., ischemic injury, sei-
zures, and infections), may indirectly drive outcomes in
patients with renal dysfunction. Moderate to severe renal
disease is included in the Charlson comorbidity index,
which independently influences outcome after ICH.16
Long-term outcomes may also be influenced by elevated
risk of recurrent ischemic and hemorrhagic stroke in
this high-risk population. Therefore, impaired renal func-
tion likely represents an important, albeit indirect, marker
of long-term outcomes after ICH, but its proximate effect
on immediate or short-term outcomes is unclear.
Our study has some notable limitations. CT scans at
standardized intervals (i.e., 6 hours) were not routinely
obtained, and so hematoma expansion could not be con-
sistently evaluated. We therefore evaluated the relation-
ship between GFR and final ICH volume, which may be
a more important surrogate of the effect of renal function
on platelet function than hematoma growth. Functional
outcome measures (i.e., modified Rankin Scale scores)
were also not available at baseline, discharge, or at long-
term follow-up. We were unable to establish with cer-
tainty baseline renal function or duration of chronic
kidney disease before hospitalization and using discharge
renal function as a surrogate measure of baseline renal
function may be inaccurate.17
We could not show a relationship between GFR and he-
matoma volume, implying that other mechanisms may
explain the impact of renal function on outcome after
ICH. Given previous reports implicating the role of renal
function on risk of ICH, early and late mortality, and func-
tional outcomes,3,8 additional studies should investigate
whether these are mediated by acute hematoma expan-
sion, location of hemorrhage, risk of recurrent hemor-
rhage, medical complications, and long-term functional
outcomes.
References
1. Jalal DI, Chonchol M, Targher G. Disorders of hemostasisassociated with chronic kidney disease. Semin ThrombHemost 2010;36:34-40.
2. YahalomG, Schwartz R, Schwammenthal Y, et al. Chronickidney disease and clinical outcome in patients withacute stroke. Stroke 2009;40:1296-1303.
3. Molshatzki N, Orion D, Tsabari R, et al. Chronic kidneydisease in patients with acute intracerebral hemorrhage:Association with large hematoma volume and poor out-come. Cerebrovasc Dis 2011;31:271-277.
4. Rhoney DH, Parker D Jr, Millis SR, et al. Kidney dysfunc-tion at the time of intracerebral hemorrhage is associatedwith increased in-hospital mortality: A retrospective ob-servational cohort study. Neurol Res 2012;34:518-521.

S. CUTTING ET AL.90
5. Hemphill JC, Bonovich DC, Besmertis L, et al. The ICHscore: A simple, reliable grading scale for intracerebralhemorrhage. Stroke 2001;32:891-897.
6. Mehta RL, Kellum JK, Shah SV, et al. Acute Kidney InjuryNetwork: Report of an initiative to improve outcomes inacute kidney injury. Crit Care 2007;11:1-8.
7. Nephron Information Center web site. Fadem SZ,Rosenthal B. CKD EPI and MDRD GFR Calculator: 4variable MDRD CKD EPI equation (with SI units) usingstandardized serum creatinine, age, race, gender. Avail-able at http://www.nephron.com/MDRD_GFR.cgi. Ac-cessed April 3, 2012.
8. Kothari RU, Brott T, Broderick JP, et al. The ABCs of mea-suring intracerebral hemorrhage volumes. Stroke 1996;27:1304-1305.
9. Chanderraj R, Schwab K, FitzMaurice E, et al. Predictionof functional outcome in patients with primary intracere-bral hemorrhage: The FUNC score. Stroke 2008;39:2304-2309.
10. Graeb DA, Robertson WD, Lapointe JS, et al. Com-puted tomographic diagnosis of intraventricular hem-orrhage. Etiology and prognosis. Radiology 1982;143:91-96.
11. Bos MJ, Koudstaal PJ, Hofman A, et al. Decreased glo-merular filtration rate is a risk factor for hemorrhagicbut not for ischemic stroke: The Rotterdam study. Stroke2007;38:3127-3132.
12. Hojs Fabjan T, Hojs R, Tetickovic E, et al. Ischaemicstroke—Impact of renal dysfunction on in-hospital mor-tality. Eur J Neurol 2007;14:1351-1356.
13. Ovbiagele B. Chronic kidney disease and risk of deathduring hospitalization for stroke. J Neurol Sci 2011;301:46-50.
14. Ovbiagele B, Sanossian N, Liebeskind DS, et al. Indices ofkidney dysfunction and discharge outcomes in hospital-ized stroke patients without known renal disease. Cere-brovasc Dis 2009;28:582-588.
15. Ovbiagele B, Pineda S, Saver JL. Renal dysfunction anddischarge destination in patients with intracerebral hem-orrhage. J Stroke Cerebrovasc Dis 2011;20:145-149.
16. Bar B, Hemphill JB. Charlson comorbidity index ad-justment in intracerebral hemorrhage. Stroke 2011;42:2944-2946.
17. Haider DJ, Ferrari J, Mittermayer F. A transient improve-ment in renal function occurs after ischemic stroke. RenFail 2012;34:7-12.