idiopathic intracranial hypertension - peacehealth hills... · idiopathic intracranial hypertension...
TRANSCRIPT

IDIOPATHIC INTRACRANIAL HYPERTENSION
William L Hills, MD Neuro-ophthalmology
Oregon Neurology Associates Affiliated Assistant Professor
Ophthalmology and Neurology Casey Eye Institute, OHSU
No disclosures
CASE - 19 YO WOMAN WITH HEADACHES X 3 MONTHS
Headaches frontal Worse lying down Wake from sleep Pulsatile tinnitus x
1 month. Vision blacks out
transiently when she bends over or sits down
PMHx: obesity Meds: takes ibuprofen
for headaches

EXAMINATION
Vision: 20/20 R eye, 20/25 L eye. Neuro: PERRL, no APD, EOMI, VF full
to confrontation. Dilated fundoscopic exam: 360 degree
blurring of disc margins in both eyes, absent SVP.
Formal visual field testing: Enlargement of the blind spot, generalized constriction both eyes.
Posterior flattening of the globes
Empty sella otherwise normal
Opening pressure 39 cm H20
Normal CSF studies Headache improved
after LP
MRI brain: Lumbar puncture:
IDIOPATHIC INTRACRANIAL HYPERTENSION
SYNDROME:
Increased intracranial pressure without ventriculomegaly or mass lesion
Normal CSF composition

NOMENCLATURE Idiopathic intracranial hypertension (IIH) Benign intracranial hypertension Pseudotumor cerebri Intracranial hypertension secondary to…

DIAGNOSTIC CRITERIA Original criteria have been updated to reflect
new imaging modalities: Symptoms and signs reflect only those of
increased ICP or papilledema Documented increased ICP during LP in lateral
decubitus position Normal CSF composition No evidence of mass, hydrocephalus, structural
or vascular lesion on MRI or CT with contrast in typical patients and on MRI with MRV for all others.
No other cause of elevated ICP identified
Friedman and Jacobsen. N
eurology 2002; 59: 1492-1495
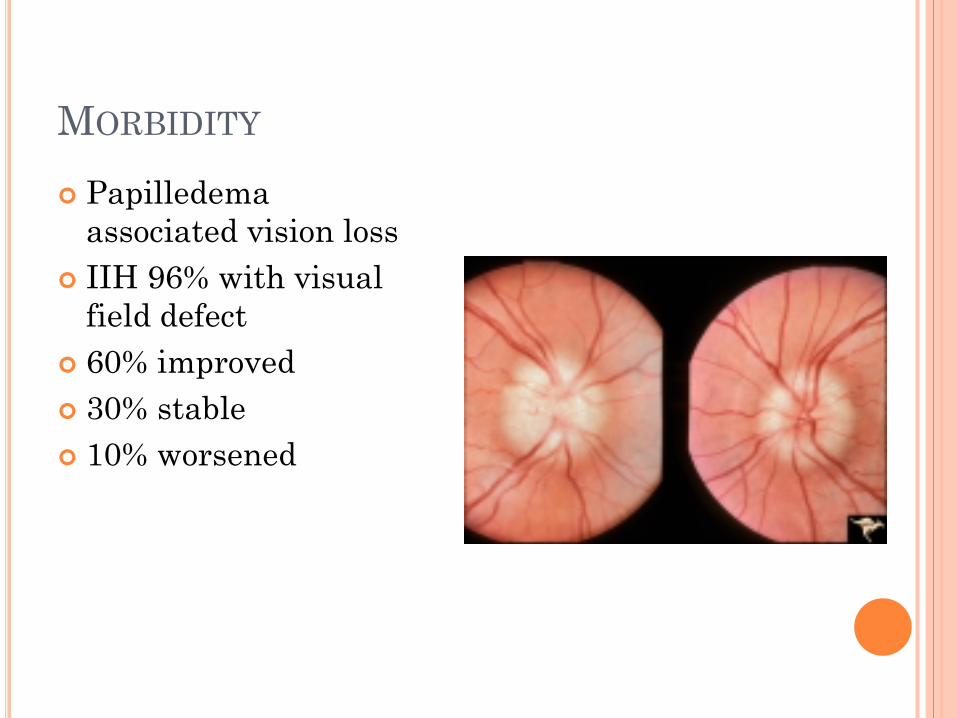
MORBIDITY Papilledema
associated vision loss IIH 96% with visual
field defect 60% improved 30% stable 10% worsened
EPIDEMIOLOGY Annual incidence General population 0.9/100,000 Women 15 to 44 3.5/100,000 Women 20-44 and 20% above ideal body weight
19.3/100,000

EPIDEMIOLOGY Before puberty boys = girls After puberty women affected 9 times as often as
men Rarely develops in patients over 45
CLINICAL MANIFESTATIONS Headache Transient visual obscurations Visual loss Pulse synchronous tinnitus Diplopia
HEADACHE Almost all patients with IIH Daily, retro-bulbar Neck pain can be prominent features Throbbing, nausea, vomiting, photophobia Often worse supine
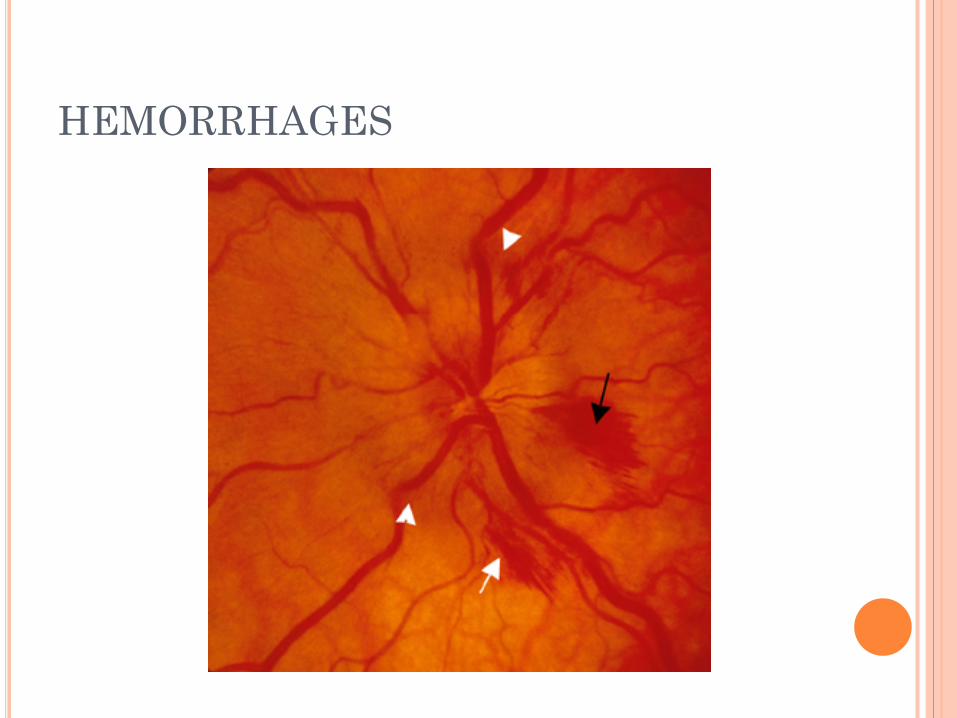
HEMORRHAGES

TRANSIENT VISUAL OBSCURATIONS Brief episodes of monocular or binocular vision
loss Partial or complete Likely due to disc edema leading to ischemia of
the optic nerve head

VISUAL LOSS Blurred vision Metamorphopsia Temporal dark spot Tunnel vision Profound or complete blindness Tempo variable: as soon as days

PULSE SYNCHRONOUS TINNITUS Pulsatile tinnitus 60% Unilateral or bilateral Typically worse when lying down Abolished with LP or jugular venous compression Transmission of intensified vascular pulsations
via CSF
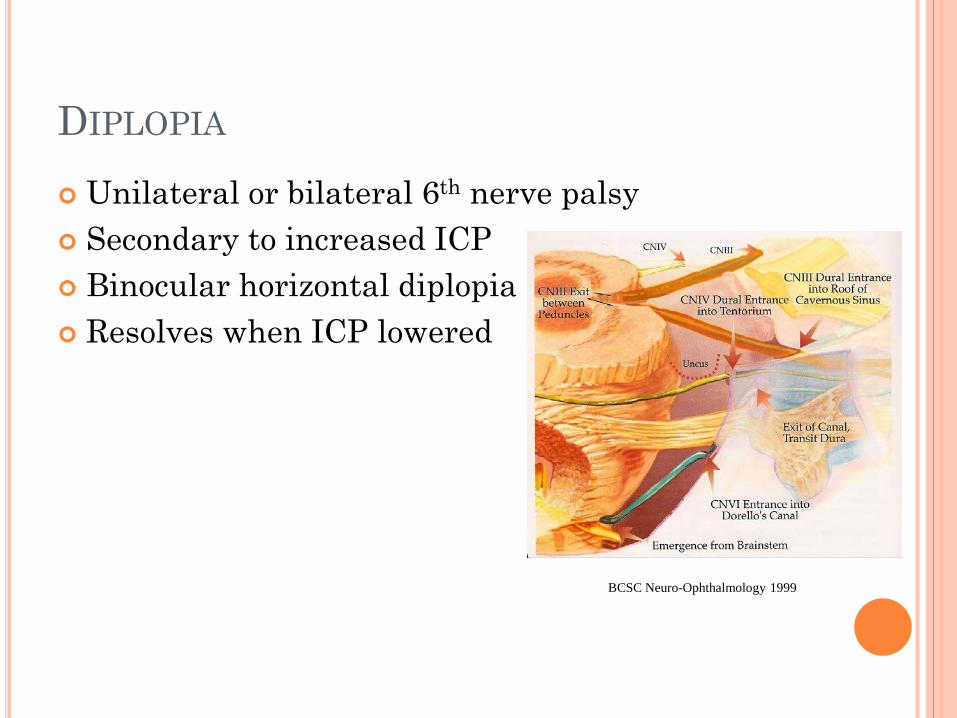
DIPLOPIA Unilateral or bilateral 6th nerve palsy Secondary to increased ICP Binocular horizontal diplopia Resolves when ICP lowered
BCSC Neuro-Ophthalmology 1999
OTHER SYMPTOMS: Paresthesias Neck stiffness Arthralgia shoulders, wrists, knees Ataxia Facial palsy- rare Radicular pain Depression
EVALUATION FOR SUSPECTED IIH History and neurologic exam Dilated fundoscopic exam Evaluation of optic nerve function- color vision,
visual acuity Neuroimaging- usually MRI (?MRV) Lumbar puncture with opening pressure and
CSF analysis Referral to confirm papilledema and for formal
visual field testing (perimetry)
PAPILLEDEMA: WHAT TO LOOK FOR 1. Disc Elevation Focus on the retina, then focus on the top of
the disc (not the cup) 2. Blurring of the margins The lower pole blurs first, then the upper
pole, then the nasal aspect. The temporal aspect of the disc is the last portion to blur.
3. Vessel obscuration As the nerve fiber layer swells, the retinal
vessels at the edge of the disc get obscured.

NORMAL OPTIC DISC

BLURRED MARGINS

PAPILLEDEMA CONTINUED 4. Can you see the cup? The cup is the last part of the disc to become
elevated. 5. Look at the veins- can you see pulsations? Venous pulsations are lost with elevated
ICP, so will not be present in true papilledema. Veins become dilated and tortuous. This is
easier to see if you compare them with the arteries.
6. Look for things that shouldn’t be there- -hemorrhages. Usually at the border of the disc. -dilated capillaries forming a “hairnet” on the
disc. This occurs in chronic papilledema -exudates- may look like drusen but will go away
when papilledema resolves.

Hair net cappillaries Vessel contour Obscuration of vessels Loss of physiologic cup
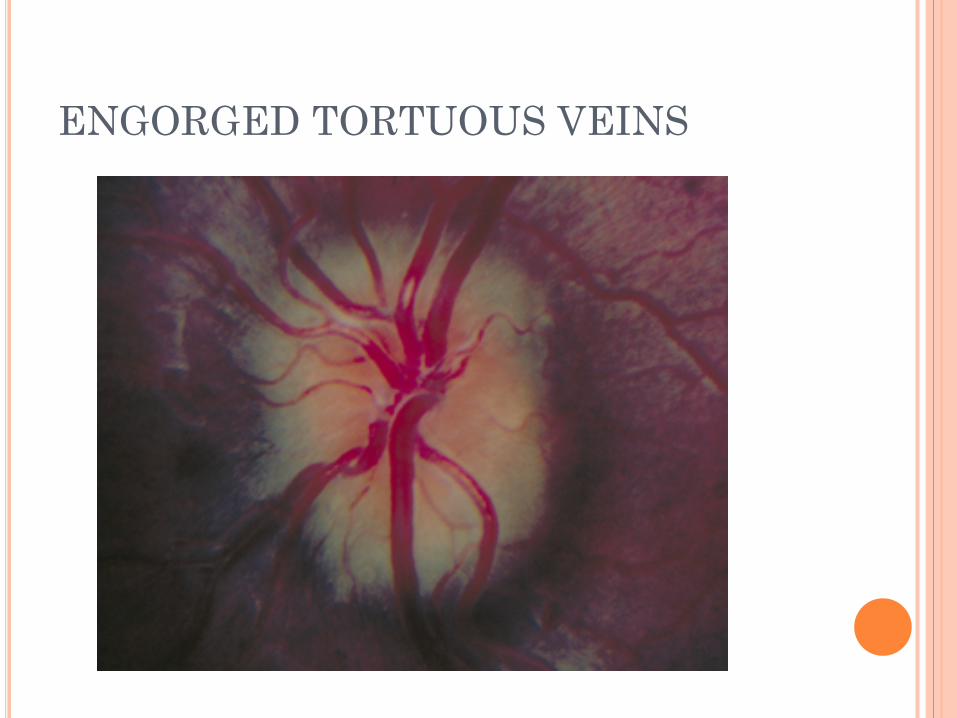
ENGORGED TORTUOUS VEINS

EXUDATES
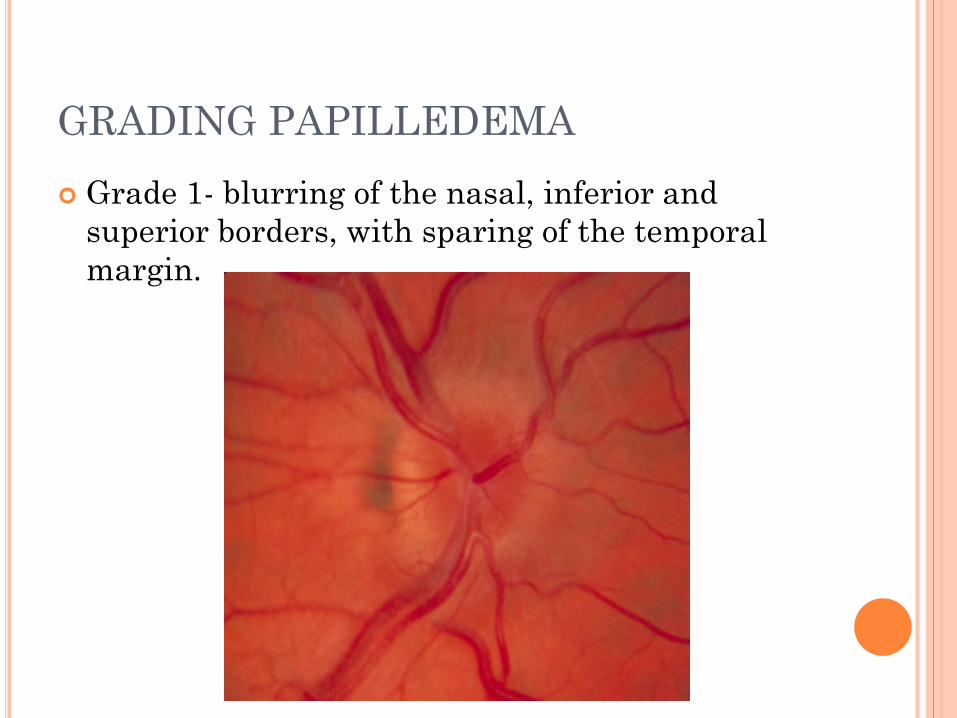
GRADING PAPILLEDEMA Grade 1- blurring of the nasal, inferior and
superior borders, with sparing of the temporal margin.
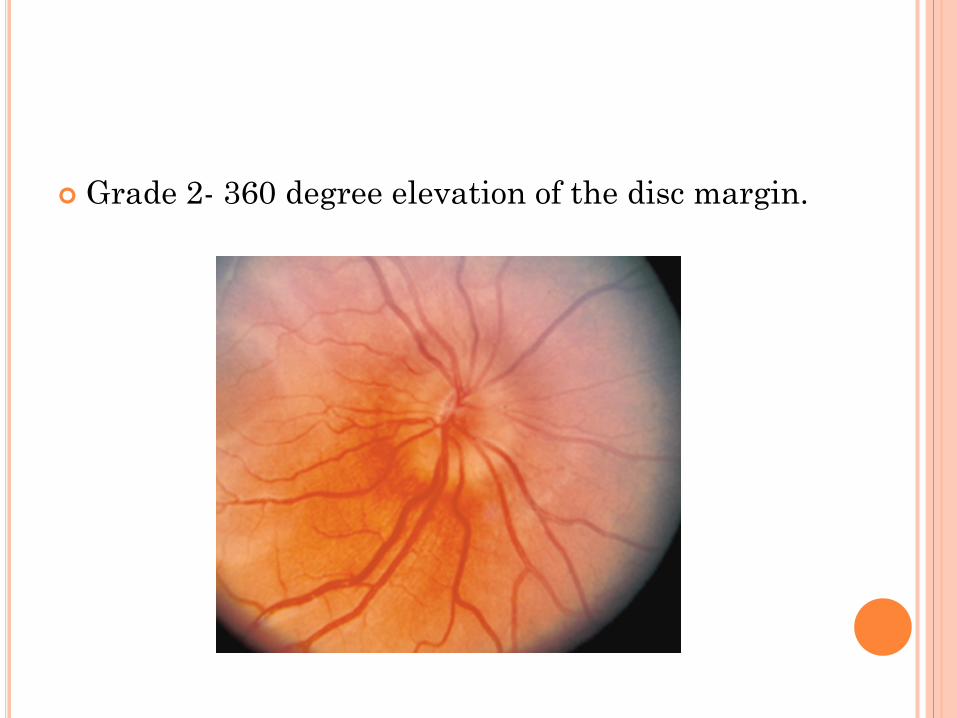
Grade 2- 360 degree elevation of the disc margin.

Grade 3- elevation of the entire disc with partial obscuration of the vessels at the margin.

Grade 4- complete obliteration of the cup and
disappearance of at least some of the vessels on the disc’s surface
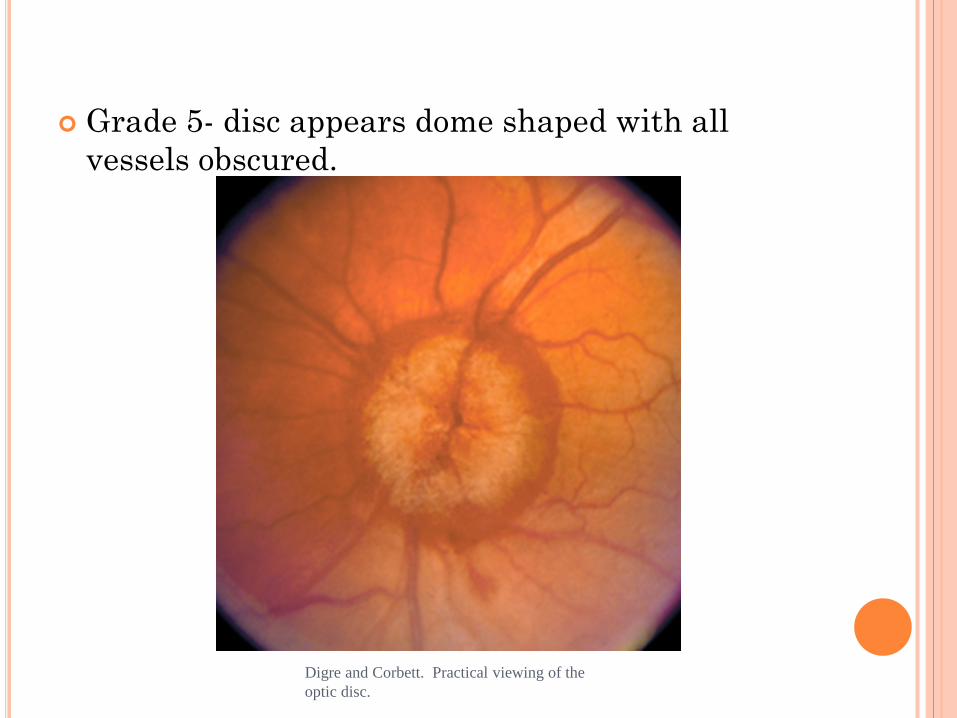
Grade 5- disc appears dome shaped with all vessels obscured.
Digre and Corbett. Practical viewing of the optic disc.
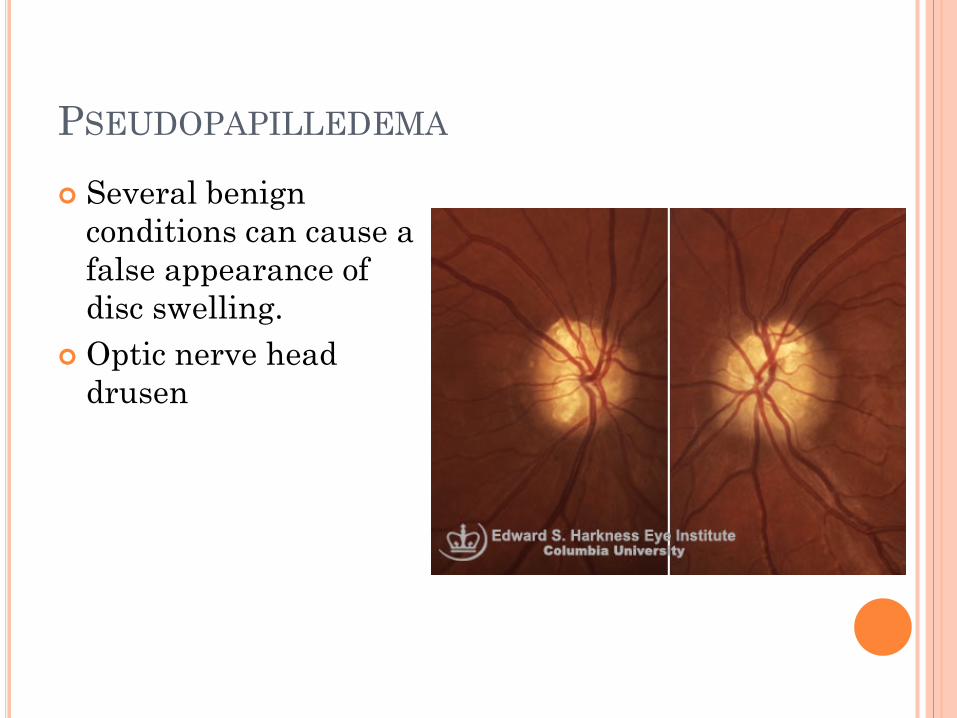
PSEUDOPAPILLEDEMA Several benign
conditions can cause a false appearance of disc swelling.
Optic nerve head drusen
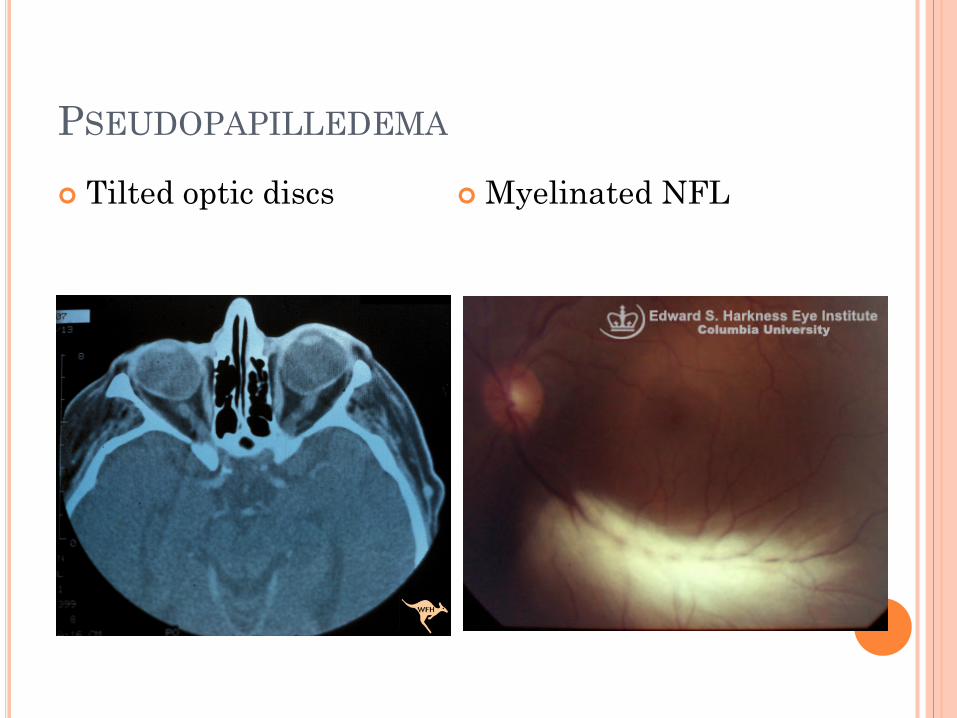
PSEUDOPAPILLEDEMA Tilted optic discs
Myelinated NFL
OPTIC NERVE FUNCTION Visual acuity < 20/20 in 15% at initial visit Contrast sensitivity is early indicator of
dysfunction Color vision is insensitive to loss; unlike in optic
neuritis RAPD – if there is an asymmetry
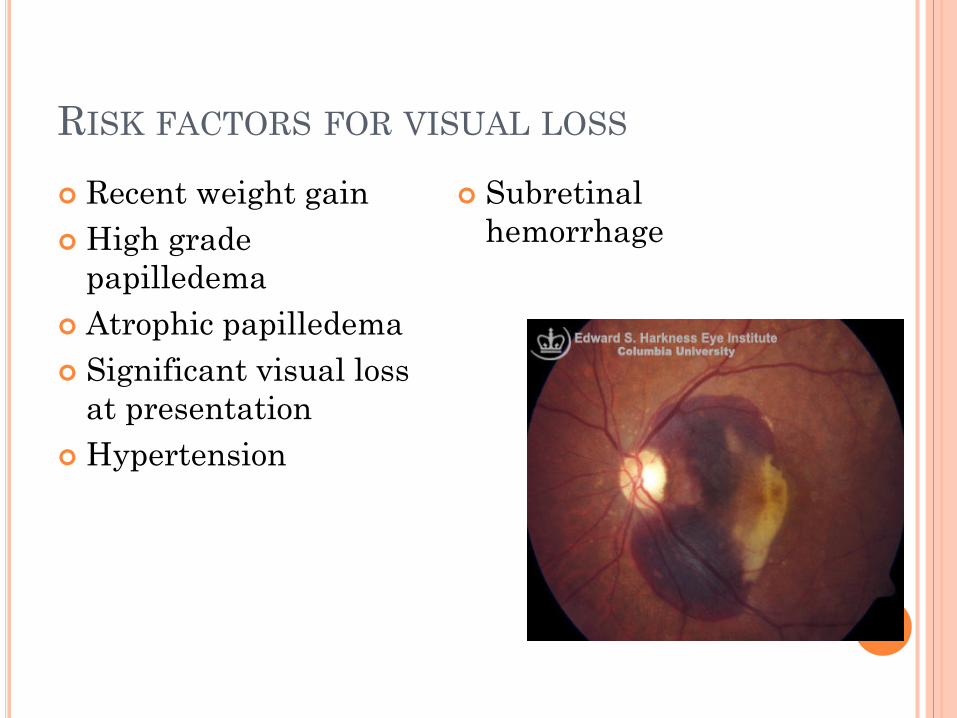
RISK FACTORS FOR VISUAL LOSS Recent weight gain High grade
papilledema Atrophic papilledema Significant visual loss
at presentation Hypertension
Subretinal hemorrhage
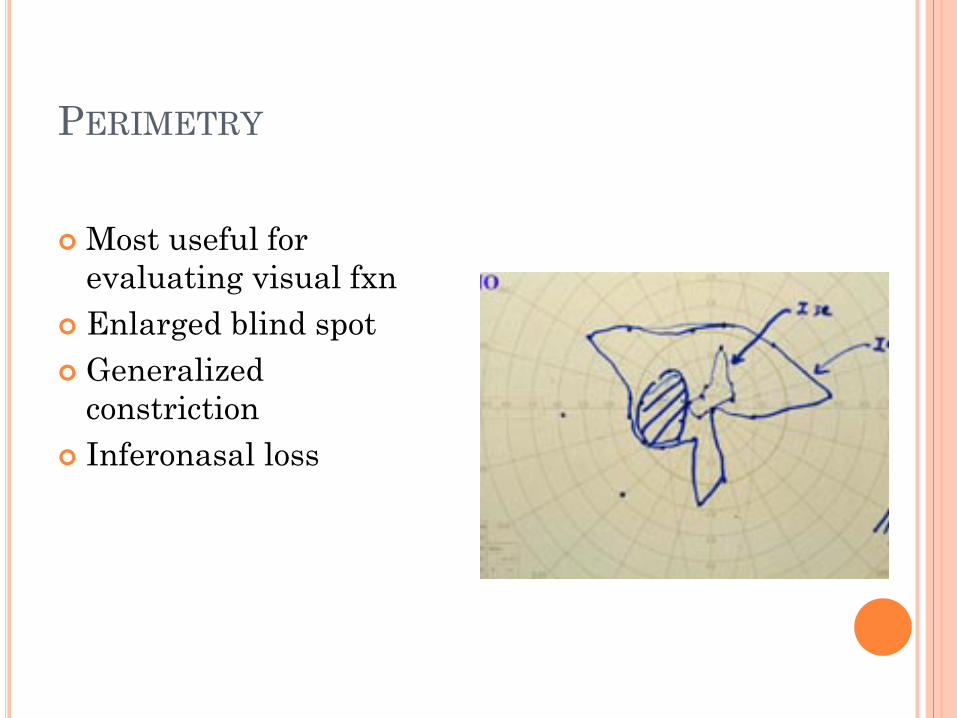
PERIMETRY
Most useful for evaluating visual fxn
Enlarged blind spot Generalized
constriction Inferonasal loss

PERIMETRY: GENERALIZED CONSTRICTION

FACTORS NOT PREDICTIVE OF VISUAL LOSS Duration of symptoms Transient visual obscurations Diplopia Pulsitile intracranial noises Degree of headache Opening pressure Pregnancy
NEUROIMAGING Primary role is to rule out other causes of elevated
ICP other than IIH Rule out hydrocephalus, mass lesion, venous sinus
thrombosis Need to image (at least a CT) before LP Traditional recommendation is MRI or contrast-
enhanced CT in typical patients and MRI with MRV in all others.
Some authors recommend MRI/MRV for all patients with suspected IIH

TYPICAL MRI FINDINGS OF IIH Flattening of the posterior globe at the insertion
of the optic nerve- 80% patients Empty sella- 70% Distension of the perioptic nerve sheath- 45% Chiari malformation- small, asymptomatic, not
seen in most patients
Remember, the primary reason for imaging in IIH is to EXCLUDE other diagnoses
Diagnostic criteria for idiopathic intracranial hypertension. Friedman and Jacobson. Neurology v 59 p. 1492-1495

IDIOPATHIC INTRACRANIAL HYPERTENSION
Hassan et al. Teaching N
euroImages: Idiopathic
intracranial hypertension. Neurology. v 74 (7)
Feb 2010, p e 24
VENOUS SINUS THROMBOSIS Dangerous diagnosis to miss Treatment is anticoagulation Lin et al. obtained MRI/MRV in 106 patients
with suspected IIH (patients with bilateral papilledema without mass lesions, meningitis or hydrocephalus).
10/106 (9.4%) of paients were found to have cerebral venous sinus thrombosis
Four of these patients were “typical” IIH patients (young, obese, female) and previous guidelines would not have recommended MRV for them.
Therefore the authors recommend obtaining MRV in all patients with suspected IIH
Lin et al. Occurrence of Cerebral Venous Sinus Thrombosis in Patients with Presumed Idiopathic Intracranial Hypertension. Ophthalmology 2006; 113: 2281-2284
LUMBAR PUNCTURE
Lateral decubitus position with legs relaxed
18- to 20- gauge spinal needle Document elevated CSF pressure Opening pressure > 250mm H20 201 – 249 mm H20 are nondiagnostic Repeat LP may be necessary if initial OP
nondiagnostic Rarely need 24 hour transducer
monitoring through lumbar drain to diagnose
DIAGNOSTIC PERILS OF LUMBAR PUNCTURE Opening pressure is normally higher in the obese
(cutoff 300 mm H20 not 250 mmH20) Radiologists usually position patient prone for
fluoroscopic guided LP. Prone measurements are unsatisfactory!
Legs need to be straightened and patient relaxed. Hyperventilation can artificially lower opening
pressure Valsalva can artificially raise opening pressure
as high as 47 cm H20!
Frequency and amplitude of elevation of cerebrospinal fluid resting pressure by the Valsalva manuever. Neville and Egan. Can J Ophthalmol. 2005; 40: 775-7
WORKUP FOR CONTRIBUTING FACTORS/MIMICS Vital signs- r/o hypertensive encephalopathy Medications Medical history Consider sleep study to eval for OSA Labs
Hct- anemia TSH, free T4- hypothyroidism Vitamin D level Parathyroid level- hypoparathyroidism CMP Specific tests for suspected conditions suggested by
the history
MEDICATIONS ASSOCIATED WITH IIH Tetracyclines Nalidixic acid Fluoroquinolones OCPs Danaxol Progesterone Lithium Vitamin A, isotretinoin Sulfamethoxazole Steroids or steroid withdrawal Growth hormone
Dhungana et al. Idiopathic intracranial
hypertension. Acta N
eurol Acan: 121: 71-82
CONDITIONS ASSOCIATED WITH IIH Obesity and recent weight gain are the only
conditions shown to be associated with IIH in case-control studies. But many conditions are reported to be associated with IIH.
SLE OSA Behcet’s disease Iron deficiency anemia Addison’s disease Hypothyroidism, hypoparathyroidism PCOS Obstruction to venous drainage
-sp thrombosis, elevated R heart pressure
Dhungana et al. Idiopathic intracranial
hypertension. Acta N
eurol Scan: 2010: 121: 71-82

RED FLAGS Atypical demographic Rapid development of
symptoms Explosive onset CN palsies other than
VI AMS Other focal signs Abnormal CSF
Global ophthalmoparesis
INO Vertical gaze d/o

TREATMENT Medical
Diet and weight loss Medications
Surgical Optic nerve sheath decompression CSF shunting

DIET AND WEIGHT LOSS
Retrospective studies of significant weight loss demonstrated Resolution of papilledema improvement in headaches and pulsatile
tinnitus Retrospective study demonstrating
papilledema grade and visual fields improved more rapidly in those that lost at least 2.5 kg over 3 months

MEDICATIONS TO DECREASE ICP Carbonic anhydrase
inhibitors Acetazolamide Topiramate
Other diuretics Furosemide Thiazides Spironolactone triamterene
Corticosteroids
ACETAZOLAMIDE Effective in 75% with IIH Effective dose 1 g to 4 g daily divided Start at 500 mg daily x 1 week, then 500 mg BID Most patients cannot tolerate beyond 2 g/day Side effects – patients SHOULD get these
Paresthesias Unpleasant taste with carbonated beverages Altered taste of food Low serum bicarbonate level
ACETAZOLAMIDE Severe reactions
Allergic rash Aplastic anemia Renal stones
Contains sulfa moiety
TOPIRAMATE Inhibits carbonic anhydrase Causes weight loss Also beneficial for migraines Recent study compared topiramate with
acetazolamide: Open label, 40 patients, randomized Acetazolamide started at 500 mg/day and titrated
up to1000-1500 mg/day Topiramate started at 50 mg/day and titrated up
to 100-150 mg/day Endpoint was visual field grade Result: topiramate and acetazolamide equally
efficacious

TOPIRAMATE: SIDE EFFECTS Distal paresthesias Cognitive impairment (dope-amax) Rare serious side effects: acute myopia, angle
closure glaucoma, kidney stones

CORTICOSTEROIDS Rapidly decrease ICP Not suitable for chronic use Used in emergencies while awaiting surgery Corticosteroid use and steroid withdrawal are
both associated with IIH May rebound when tapered

HEADACHE Persistent or recurrent headaches may indicate
elevated ICP However, many patients have persistent
headache even after normalization of intracranial pressure.
These headaches may be different from their initial “high pressure” headache.
In one study, 68% patients with IIH that was well controlled (resolution of papilledema and visual field abnormalities) developed new headaches.
30% had tension type headache, 20% had migraine without aura
Headache diagnoses in patients with treated idiopathic intracranial hypertension. Friedman and Rausch. Neurology v58 (10). 2002. p 1551-1553
HEADACHE MANAGEMENT First determine whether headache is due to
elevated ICP. History and exam, fundoscopic exam, perimetry. Recognize analgesic overuse headache. Treatment similar to migraine management.
TCA Depakote CCB B blockers Topamax NSAIDS

SURGICAL TREATMENT Indicated for visual loss or worsening of vision
attributable to papilledema that fails to respond to medication or is advanced at presentation.
NOT indicated for headache management Optic nerve sheath decompression CSF shunting Repeated LP????
OPTIC NERVE SHEATH DECOMPRESSION Mechanism not well understood
Filtering procedure Perineuronal scarring shifts pressure gradient
posteriorly Increases blood flow to the optic nerve

OPTIC NERVE SHEATH DECOMPRESSION Retrospective study
Improvement in visual field in 36% Stabilization in 32% Deterioration in 32%
Probability of failure 3 to 5 year post op 35%
Complications Failure Ischemic optic neuropathy Transient blindness
CSF SHUNTING In the past, lumboperitoneal shunting
preferred over ventricular shunting due to small ventricular size in IIH.
Improved surgical methods (stereotactic localization) has led to increased VP shunting.
In practice, decision is up to the surgeon. Both VP and LP shunts are highly
effective in the short term but have very high long-term failure and revision rates.
For example, retrospective series of 30 patients receiving LP shunt.
All patients experienced relief of symptoms. 30 patients required 126 revisions (average of 4.2
revisions per patient!)
Surgery for idiopathic intracranial hypertension. Brazis. J Neuro-ophthalmol. Vol 29, n, 4, 2009
COMPLICATIONS Common Complications --Shunt obstruction --Shunt infection --Overdrainage of CSF --Catheter migration
In-Hospital Mortality Rate of 0.9% for VP shunt
and 0.3% for LP shunt
Uretsky. Surgical interventions for idiopathic intracranial hypertension. Current opinion in ophthalmology. 2009; 20: 451-455
ENDOVASCULAR STENTING Still experimental Patients with IIH commonly have narrowing of
the transverse sinuses on MRV. Debatable whether this is causative or not. May
be secondary.
DONNET ET AL.
10 consecutive patients with refractory IIH
underwent direct retrograde cerebral venography and manometry.
All had morphologic obstruction of the transverse sinuses.
All underwent stenting of the venous sinuses All had resolution of papilledema and
normalization of CSF pressure at 3 month followup.
Donnet et al. Endovascular treatment of idiopathic intracranial hypertension. Neurology 70, p. 641-647
MONITORING AND FOLLOW-UP OF IIH Obtain formal visual fields at time of starting
therapy. This needs to be done in a timely manner.
If no visual field abnormalities on initial testing, no visual complaints and just mild grade one papilledema probably don’t need repeat visual fields unless symptoms worsen.
All other patients: repeat visual fields after three months on treatment.
Sooner if symptoms get worse. After three months repeat fields if papilledema
worsens or symptoms worsen.
IF PATIENT DOESN’T RESPOND TO DIURETICS… Obtain MRV/CTV if you have not already done so Look for secondary causes of IIH Reconsider diagnosis Consider sending for shunting or ONSF
PREGNANCY IIH may develop or worsen during
pregnancy. Occurrence rate is similar to age matched
controls No increased risk of fetal loss Diagnostic criteria same Acetazolamide – use after 20 weeks
gestation Avoid thiazide diuretics and TCA Corticosteroids indicated with vision loss ONSD or LP shunt
MEN Constitute about 10% patients with IIH Less likely to report headache More likely to report visual disturbances Twice as likely as women to develop severe visual
loss Visual function should be followed more closely
because less likely to experience and report other symptoms of elevated ICP
Bruce et al. Idiopathic intracranial hypertension in men. Neurology v72 p. 304-309

FULMINANT IIH Defined as acute onset of symptoms and signs of
IIH (less than 4 weeks between onset of initial symptoms and severe visual loss) with rapid worsening of visual loss over a few days and normal MRI/MRV
All have severe loss of visual acuity and severe bilateral papilledema at presentation.
Usually have very elevated opening pressure (mean 54.1 but range 29-70 cm H20)

Need MRV to rule out CVST Urgent surgery is usually required. Visual outcome correlates directly with time from
presentation to surgery Temporizing measures include IV corticosteroids,
IV acetazolamide, lumbar drain In one study of 16 patients, 8 patients remained
legally blind, these had surgery between 3-37 days after presentation. 8 patients recovered vision, these had surgery between hours to 4 days after presentation.
Thambisetty et al. Fulm
iant idiopathic intracranial hypertension. N
eurology v68, p. 229-232


IIH WITHOUT PAPILLEDEMA? Does it really exist? IIHWOP is recognized in the International
Headache Society criteria Digre et al. reviewed records of all patients with
diagnosis of IIH at a neuro-ophthalmology clinic from 1990-2003
353 patients 20 (5.7%) were without papilledema
PATIENTS WITHOUT PAPILLEDEMA Had lower opening pressures (309 vs 373 mm
H20) Most (75%) had spontaneous venous pulsations 73% had normal visual fields (vs. 13% in patients
with papilledema) 20% had nonphysiologic constriction of visual
fields None had enlarged blind spot (vs. 59% in patients
with papilledema) 55% had auras (vs. 20%) Had poorer response to diuretics (30% vs 55%)