hyperkalaemia case study
TRANSCRIPT
The pathology lab calls on a Friday night to advise a patient has
hyperkalaemia?
What next….
Dr Chris Arden
GP, Chandlers Ford
GPSI Cardiology, Southampton
Issues & Answers in Issues & Answers in Cardiovascular DiseaseCardiovascular Disease
1717thth November 2012 November 2012
WarwickWarwick
G e o rg e
7 2 y e a r o ld re tire d s a le s m an
PH - LVSD HTN Typ e 2 DM O A
Rx - Ena la p ril 1 0 m g o d Bis o p ro lo l 5 m g o d Sp iro no la c to ne 2 5 m g o d Nap ro x e n 2 5 0 m g i-ii bd Co -Co dam o l 8 /5 0 0 p rn
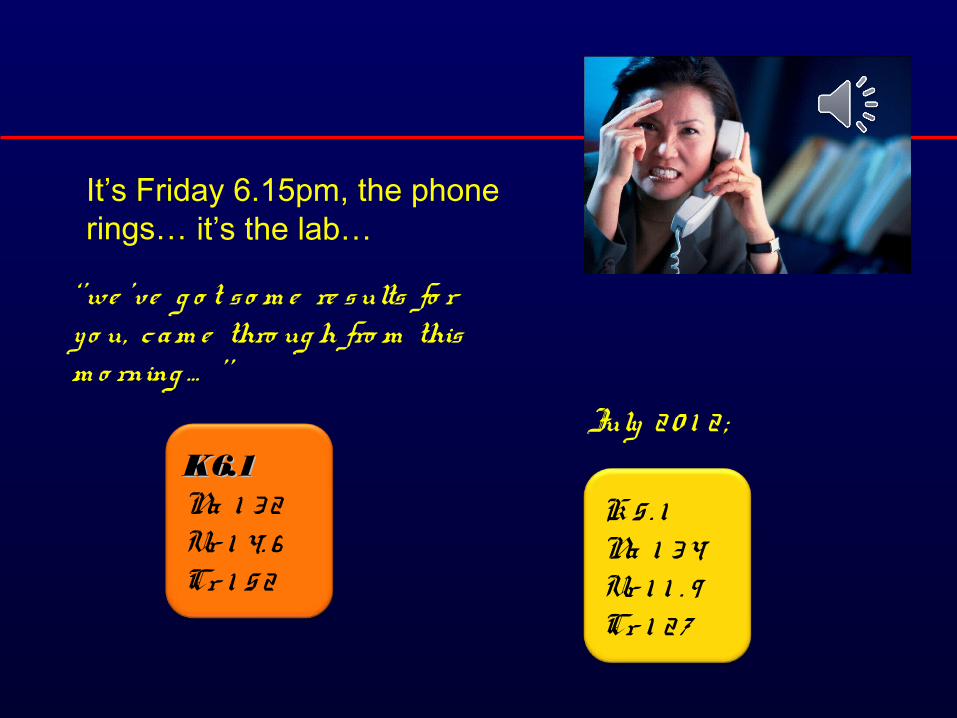
It’s Friday 6.15pm, the phone rings…
K 6.1K 6.1Na 1 3 2Ur 1 4. 6Cr 1 5 2
July 2 0 1 2 ;
K 5 . 1Na 1 3 4Ur 1 1 . 9Cr 1 2 7
it’s the lab…
‘ ’we ’v e g o t s o m e re s ults fo r y o u, c am e thro ug h fro m this m o rning … ’ ’
Po ta s s ium p a tho phys io lo g y
No rm a l ra ng e - 3 . 5 -5 . 0 m m o l/l
Hyp e rka la e m ia - > 5 . 5 m m o l/l
Hyp e rka la e m ia is a p o te ntia lly life -thre a te ning m e ta bo lic p ro ble m c a us e d by ;
•inability of the kidneys to excrete potassium•impairment of the mechanisms facilitating potassium movement from circulation into cells•or a combination of these factors
Co m m o n c a us e s o f hyp e rka la e m ia
Incre a s e d inta ke
• + Po ta s s ium s up p le m e nts
• d ie ta ry e x c e s s
• s a lt s ubs titute s
Incre a s e d p ro duc tio n
• ha e m o ly s is• tra um a• inte ns e phys ic a l a c tiv ity• e x te ns ive burns
Co m m o n c a us e s o f hyp e rka la e m ia
Im pa ire d e x c re tio n
• re duc e d G FR (a cute o r ESRF)
• Drug s• ACE-I• potassium sparing diuretics• NSAID’s• cyclosporin
• d e fe c t in tubula r s e c re tio n (e . g . re na l tubula r a c id o s is )
Co m m o n c a us e s o f hyp e rka la e m ia
Re d is tributio n
‘shift from intracellular to extracellular fluid’
•a c id o s is (m e ta bo lic o r re s p ira to ry )
•ins ulin d e fic ie nc y
•Drug s• Digoxin• Beta blockers• Scoline (suxamethonium)
Co m m o n c a us e s o f hyp e rka la e m ia
Ps e udo hyp e rka la e m ia
• ha e m o ly s is (in la b tube !) most common• thro m bo c y to s is
• ve ne p unc ture te chniq ue• (e . g . p ro lo ng e d to uniq ue t a p p lic a tio n)
Sig ns & Sym p to m s o f hyp e rka la e m ia
• Clinic a l fe a ture s o fte n non-specific• Lethargy• Confusion• Weakness• Palpitations
• G e ne ra lis e d m us c le we a kne s s
• Pa ra e s the s ia o f ha nds & fe e t
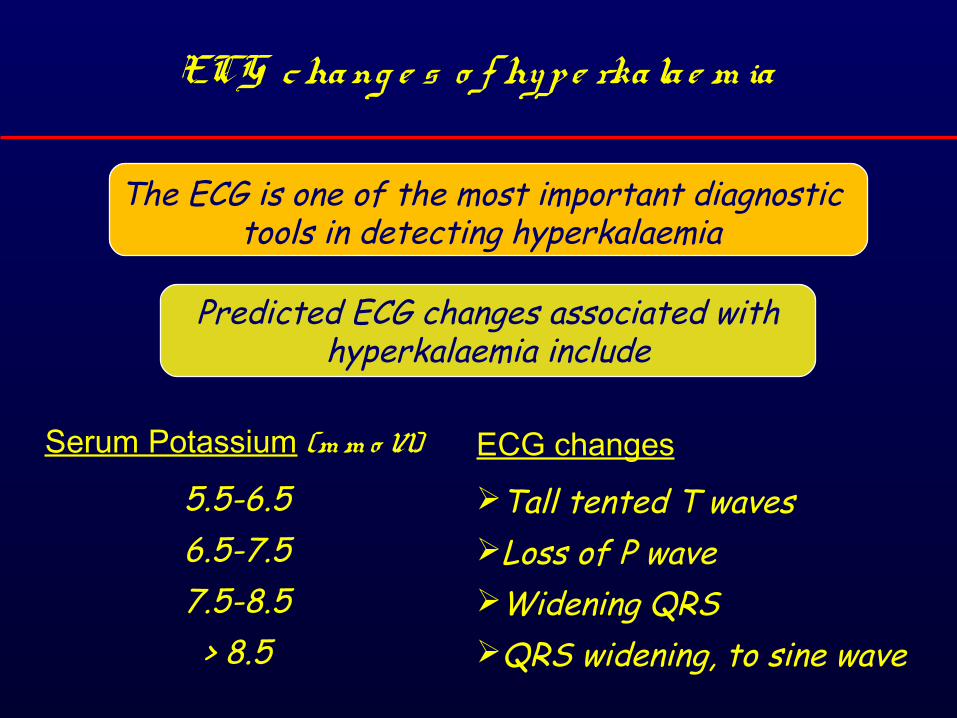
ECG cha ng e s o f hyp e rka la e m ia
The ECG is one of the most important diagnostic tools in detecting hyperkalaemia
Predicted ECG changes associated with hyperkalaemia include
Serum Potassium (m m o l/l)
5.5-6.56.5-7.57.5-8.5
> 8.5
ECG changes
Tall tented T wavesLoss of P waveWidening QRSQRS widening, to sine wave
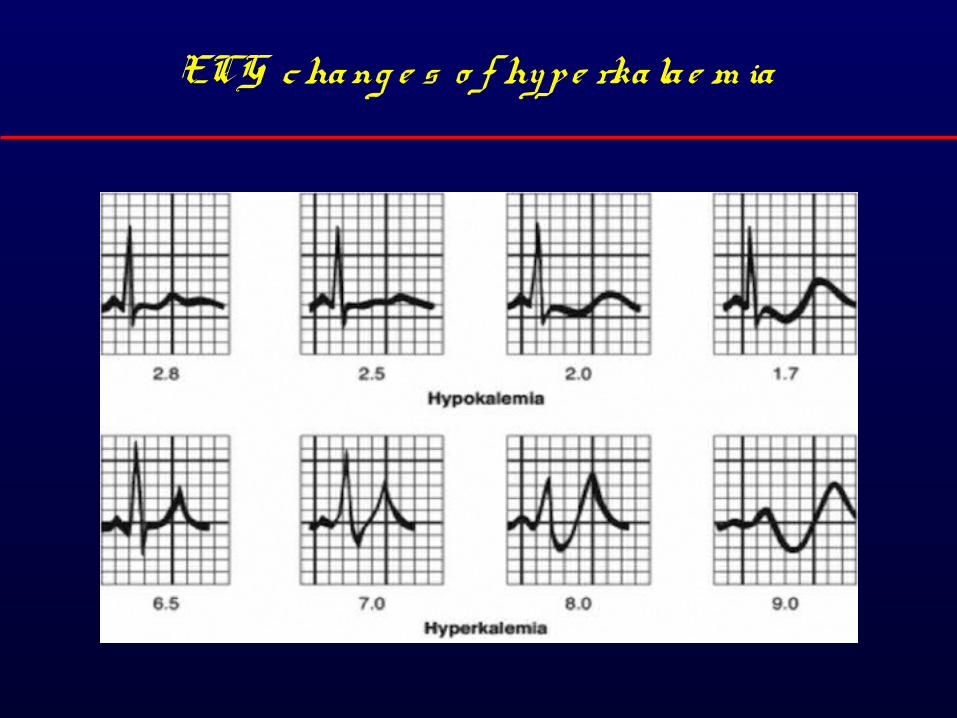
ECG cha ng e s o f hyp e rka la e m ia
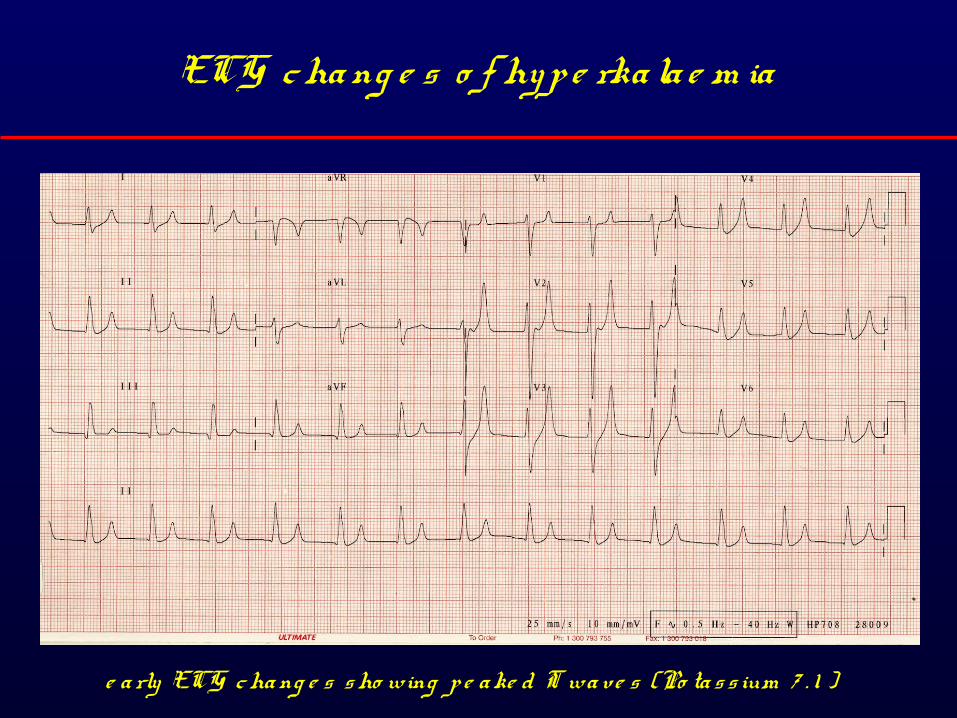
ECG cha ng e s o f hyp e rka la e m ia
e a rly ECG cha ng e s s ho wing p e a ke d T wa ve s (Po ta s s ium 7 . 1 )
You’re on duty, the clock’s ticking, wha t d o y o u d o ne x t… ?
•phone patient..•assess symptoms
• a cute• s y s te m ic a lly unwe ll• Rx c o m p lia nc e ? O TC• inte r-c urre nt illne s s
•review previous results – trend ? ARF•vulnerable/alone?•options include;
• admit• d/w medics• No thing• none of the above…• Or…?