hydrocele seminar - a comprehensive review of literature
TRANSCRIPT
D R . H A R M A N D E E P S I N G H
G U I D E D B Y – D R . D . D . W A G H S I R
P R O F E S S O R & H E A D ,
D E P T . O F G E N E R A L S U R G E R Y ,
D . M . I . M . S . , S A W A N G I ( M )
HYDROCELE

INTRODUCTION
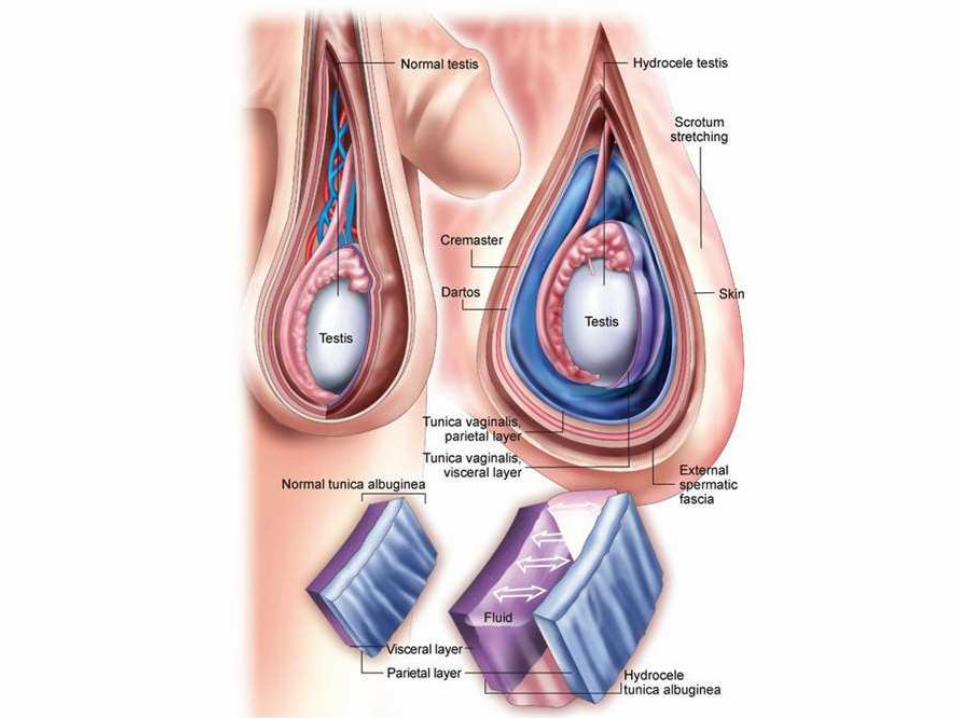
Hydrocele is an abnormal fluid collection between the visceral and parietal layers of the tunica vaginalis.
In infants it is usually the result of incomplete closure of the processus vaginalis. It may or may not be associated with inguinal hernia. In older boys and men it may be idiopathic but more likely to be secondary to another pathologic process in the scrotum or adjacent structures
DEVELOPMENTAL ANATOMY
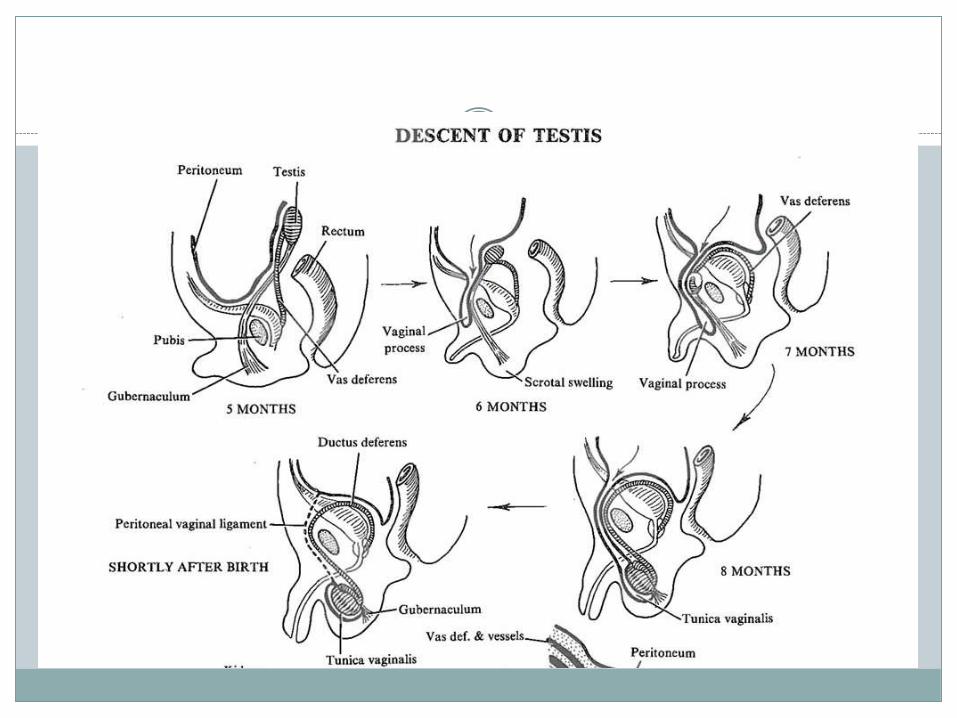
Testis descends from the posterolateral genitourinary ridge at the beginning of the third trimester of fetal gestation, a saclike extension of peritoneum descends in concert with the testis. As descent progresses, the sac envelops the testis and epididymis. The result is a serosal-lined tubular communication between the abdomen and the tunica vaginalis of the scrotum.
The peritoneum-derived serosal communication is the processus vaginalis, and the serosa of the hemiscrotumbecomes the tunica vaginalis.

At term, or within the first 1-2 years of life, the processus vaginalis of the spermatic cord fuses, obliterating the communication between the abdomen and the scrotum. The processus fuses distally as far as the lower epididymal pole and anteriorly to the upper epididymal pole. Failure of complete fusion may result in communicating hydroceles, indirect inguinal hernias, and the bell-clapper deformity of abnormal testicular fixation in the scrotum.


Layers of Scrotum
SKIN
DARTOS MUSCLE
EXTERNAL SPERMATIC FASCIA
CREMASTRIC MUSCLE
INTERNAL SPERMATIC FASCIA
TUNICA VAGINALIS
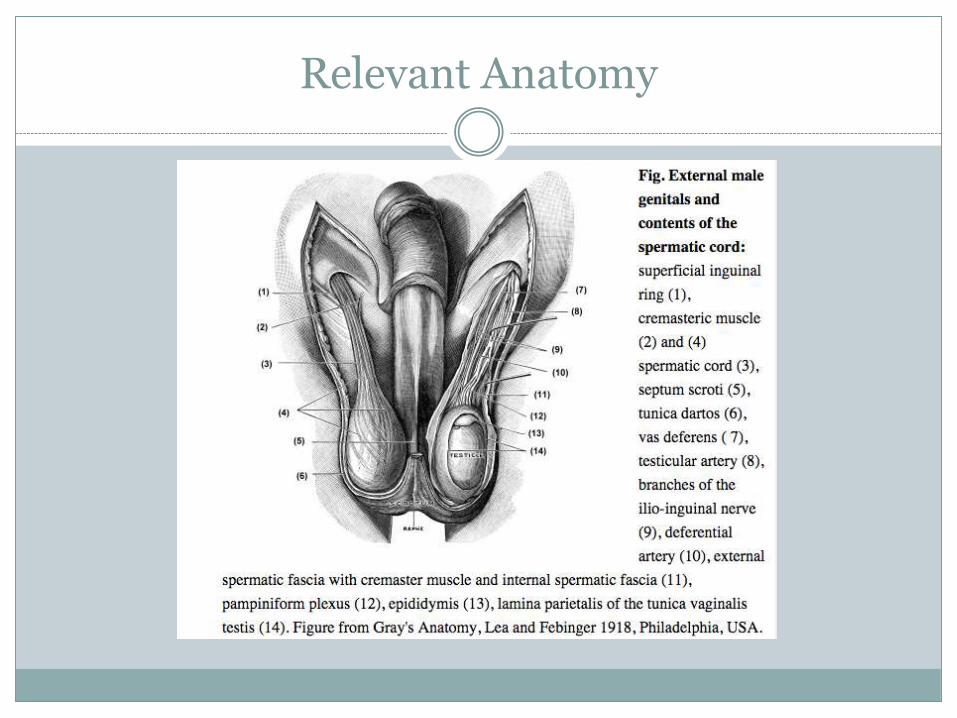
Relevant Anatomy


Lymphatic Drainage
Scrotal lymphatics drain into the corresponding superficial inguinal lymph nodes.
Anastomoses to the lymphatics of the contralateral network across the median raphe occur.
Testicular lymphatics via the spermatic cord drain to the paraaortic nodes.
Risk factors
Most hydroceles are present at birth (congenital), and babies who are born prematurely have a higher risk of having a hydrocele.
Incidence : 3.5 to 5.0% in full term infants and 44 to 55% in premature and Low birth weight babies (Groff D, Nagaraj HS, Pietsch JB, Inguinal hernias in premature infants who were operated on before their discharge from the neonatal intensive care unit Arch Surgery 1985)
Risk factors for developing a hydrocele later in life include: Scrotal injury (Traumatic/Iatrogenic), Infection including sexually transmitted infections, Tumours.

CLASSIFICATION
CONGENITAL
ACQUIRED
I) PRIMARY
II) SECONDARY

CONGENITAL HYDROCELE
NONCOMMUNICATING HYDROCELE - patent processus vaginalis obliterates but fluid remains.
COMMUNICATING HYDROCELE - the sac remains open in communication with the peritoneal cavity.
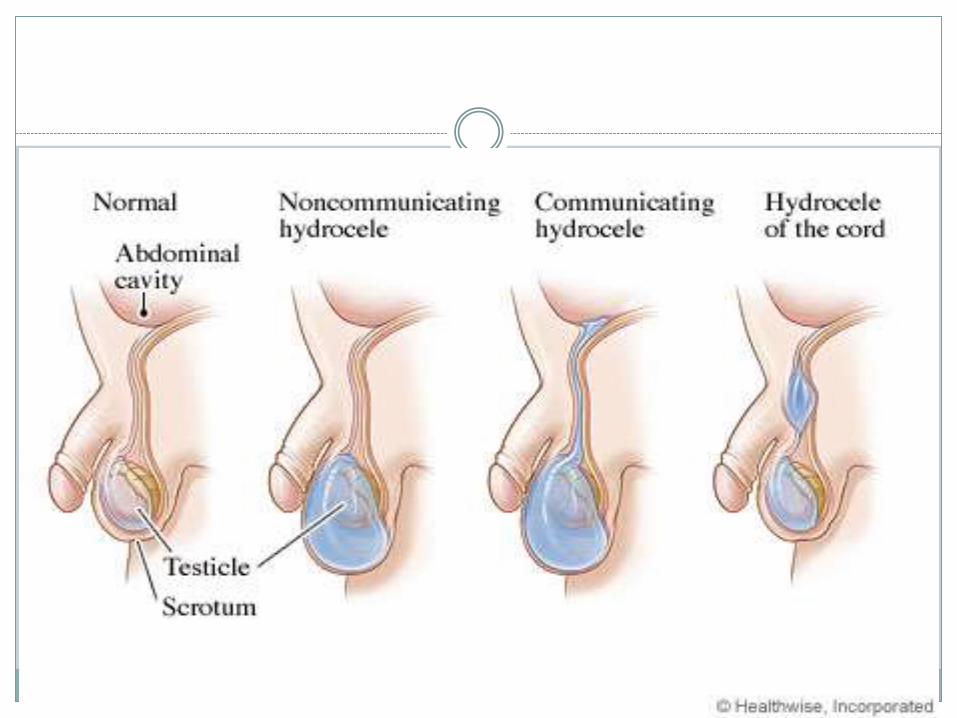
CONGENITAL HYDROCELE:
PROCESSUS VAGINALIS COMMUNICATES WITH PERITONEAL CAVITY

INFANTILE HYDROCELE:
TUNICA &PROCESSUS VAGINALIS DISTENDED UPTO INTERNAL RING BUT SAC HAS NO CONNECTION WITH PERITONEAL CAVITY

ENCYSTED HYDROCELE OF CORD:
PART OF FUNICULAR PROCESS PATENT, & IS CLOSED FROM
THE TUNICA VAGINALIS BELOW & PERITONEAL CAVITY ABOVE.
SMOOTH,OVAL SWELLING ASSOCIATED WITH SPERMATIC CORD.
TRACTION TEST

HYDROCELE EN BISSAC
TWO INTERCOMMUNICATING SACS ABOVE & BELOW NECK OF SCROTUM
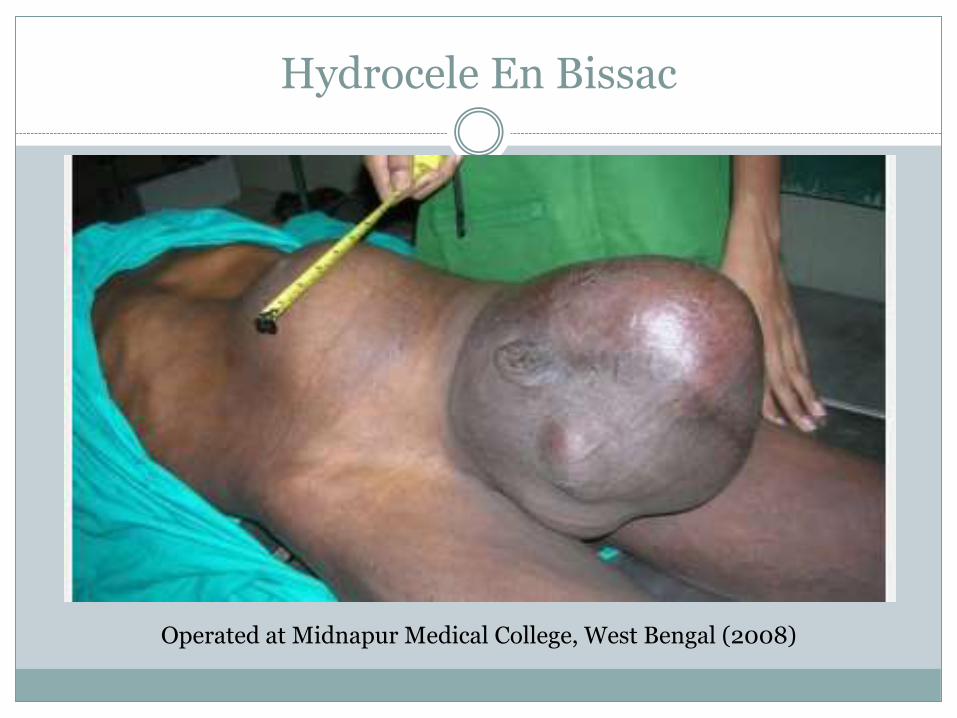
Hydrocele En Bissac
Operated at Midnapur Medical College, West Bengal (2008)

HYDROCELE OF CANAL OF NUCK:
OCCURS IN FEMALES IN RELATION ROUND LIGAMENT
ALWAYS IN THE INGUINAL CANAL

HYDROCELE OF HERNIAL SAC:
NECK OF THE HERNIAL SAC BECOMES CLOSED BY ADHESIONS OR PLUGGED BY OMENTUM.
RESULTS IS RETENTION OF FLUID SECRETED BY PERITONEUM OF HERNIAL SAC

INFECTIONS:FILARIASISTUBERCULOSIS OF EPIDIDYMISSYPHILIS
INJURYPOST HERNIORRHAPHY HYDROCELEPOST VARICOCELECTOMY HYDROCELETRAUMA
TUMOURMALIGNANCY
SECONDARY HYDROCELE
ETIOLOGY
In older men, any process that acts to stimulate increased production of watery fluid by the tunica or decrease the absorption of this fluid by the scrotal lymphatics or venous system will result in the formation of a hydrocele.
Increased production of fluid could be due to:Inflammation of the testis (orchitis) or epididymis (epididymitis) caused by tuberculosis and by tropical infections such as filariasis.Testicular torsion (rotation of the testis) may cause a reactive hydrocele in 20% of cases.Tumors of the testis, especially germ cell tumors or tumors of the testicular adnexa may cause hydrocele.
Decreased resorption of fluid could be due to:Surgery in the inguinal region or a renal transplantation can affect the lymphatics or venous system causing decreased absorption.Radiation therapy is associated with cases of hydrocele.Peritoneal dialysis and ventriculoperitoneal shunts.
COMMON IN COASTAL/TROPICAL REGIONS , ACCOUNTS FOR 80 % OF ALL HYDROCELES IN TROPICAL REGIONS, CAUSED BY Wucheria bancrofti
REPEATED ATTACKS OF FILARIAL EPIDIDYMITIS
SIZE- LARGE SIZE WITH THICKENED SAC
OCCASIONALLY CONTAINS CHOLESTEROL RICH FLUID – CHYLOCELE
DUE TO RUPTURED LYPMH VARIX WITH DISCHARGE OF CHYLE IN TO THE HYDROCELE
RESEMBLES PRIMARY HYDROCELE
MAY BE ASSOCIATED WITH FILARIAL ELEPHANTIASIS.
FILARIAL HYDROCELE
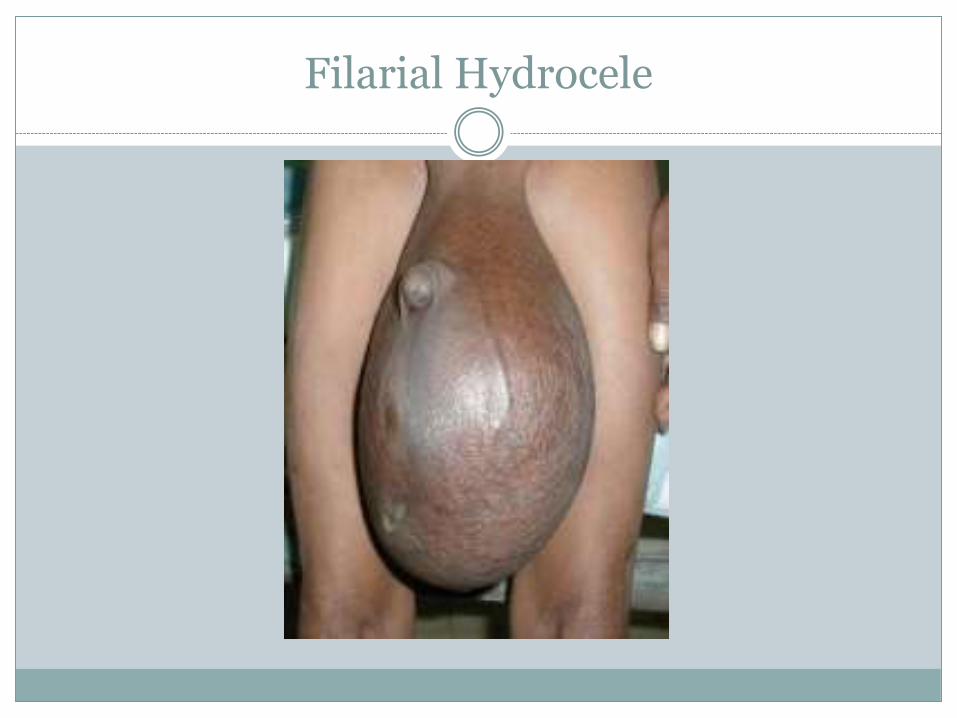
Filarial Hydrocele

SIGNS & SYMPTOMS
In the early stages hydroceles are usually asymptomatic. As they enlarge they bulge out and can become a cosmetic problem.
Symptoms can develop, as the swelling increases in size, which include: Heaviness, fullness, or dragging sensations due to an enlarged scrotum.
There may be mild discomfort radiating along the inguinal area to the mid portion of the back.
If pain develops in a Hydrocele it is usually an indication of acute epididymal infection or due to overstretched scrotal skin in huge hydroceles.
The size may decrease with recumbency or increase in the upright position.
Fever, chills, nausea, or vomiting indicate an infection of a hydrocele.
1. INFECTION
2. PYOCELE,HEMATOCELE/CLOTTED HEMATOCELE
3. CALCIFICATION OF SAC (D/D FOR TESTICULAR
TUMOUR)
4. INFERTILITY
5. ATROPHY OF TESTIS
6. HERNIATION OF HYDROCELE SAC (rare)
7. RUPTURE (rare)
COMPLICATIONS OF HYDROCELE:
PHYSICAL ASSESSMENT
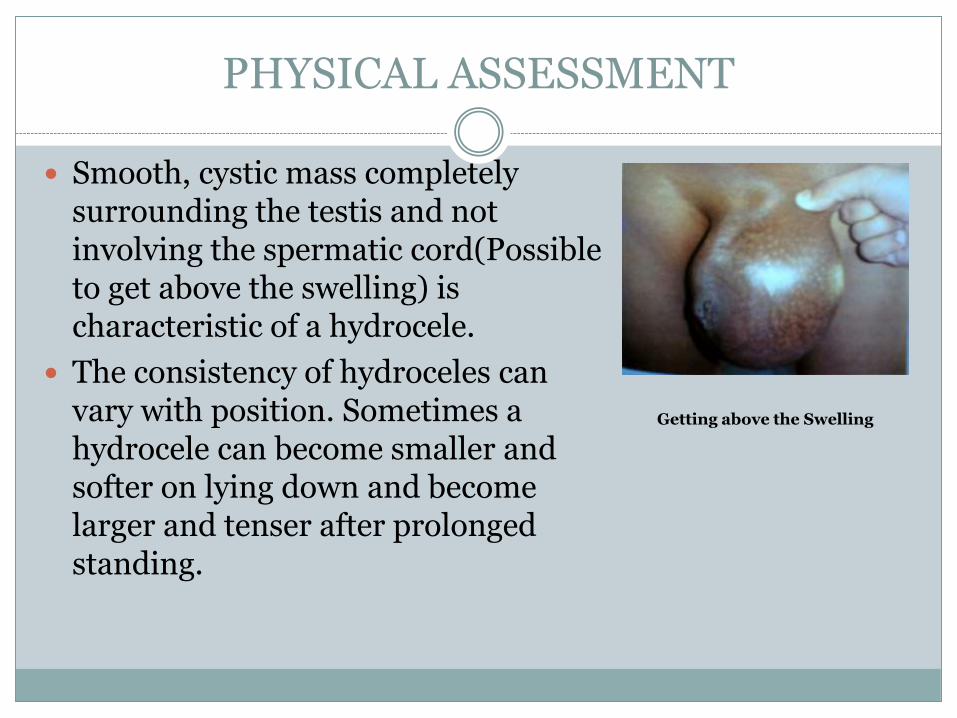
Smooth, cystic mass completely surrounding the testis and not involving the spermatic cord(Possible to get above the swelling) is characteristic of a hydrocele.
The consistency of hydroceles can vary with position. Sometimes a hydrocele can become smaller and softer on lying down and become larger and tenser after prolonged standing.
Getting above the Swelling

When the fluid in the hydrocele is clear, Transillumination is positive.
Transillumination may be negative in filarial hydrocele due to prescence of chyle, calcification or in complicated hematocele/pyocele
Hydroceles are generally painless. The presence of pain, redness and edema with loss of the normal scrotal rugae is suggestive of an inflammatory lesion like epididymitis or epididymo-orchitis or filarial relapses.

PRIMARY
TESTIS NOT PALPABLE
TENSE,FLUCTUANT
TRANSILLUMINANT
CAN GET ABOVE SWELLING
FEATURES : PRIMARY VS SECONDARY HYDROCELE
SECONDARY
TESTIS MAY BE PALPABLESOFT,FLUCTUANT, MAYBE TENSE IN CASE OF FILARIAL SCROTUMTRANSILLUMINANTCAN GET ABOVE SWELLING
LABORATORY STUDIES
Laboratory evaluation is generally not essential to the evaluation of hydroceles.
Leukocytosis with a higher percentage of neutrophils suggests an infectious and/or inflammatory process (eg, epididymo-orchitis).
IMAGING STUDIES
Uncomplicated hydroceles do not require radiographic studies. Findings from USG can help evaluate for an underlying process, such as a tumour or torsion.
1. TESTICULAR TUMOUR
2. EPIDIDYMAL CYST
3. SPERMATOCELE
4. SCROTAL EDEMA
5. IRREDUCIBLE INGUINAL HERNIA
DIFFERENTIAL DIAGNOSIS

In Children,
A Non-communicating Hydrocele usually resolves spontaneously by the time the child reaches the age of 1 year.
A hydrocele that persists longer than 12 to 18 months is usually a Communicating Hydrocele & requires Herniotomy
TREATMENT

TREATMENT
In Adults,
Treatment depends upon the age of the patient and the degree of discomfort caused by the hydrocele. Surgical excision forms the definitive therapy for hydroceles.
When they are small and asymptomatic, hydroceles require no treatment other than reassurance.
Indications for surgery –
Scrotal discomfort or pain
Cosmetic - disfigurement due to the sheer size of the hydrocele.

Principle of Surgery
Techniques include – LORDS PLICATION
used for small to medium hydroceles with thin sac. Benefits - reduced risk of hematoma.. Some articles suggest a slight incidence of recurrence of the hydrocele following this procedure.
JABOULEYS OPERATION
the sac & everted and sutured behind the testis, associated with a reduced risk of recurrence, may have an increased risk of hematoma.
SUBTOTAL EXCISION or HYDROCELECTOMY
In cases of large sac, where there is risk of a large redundant swelling post operatively, excision of the sac with 1 cm margin around the testis & epididymis. ?Filarial Sac
SHARMA & JHAWERS TECHNIQUE
ASPIRATION WITH/WITHOUT INJECTION OF SCLEROSING AGENT
CONGENITAL HYDROCELE ARE TREATED BY HERNIOTOMY.
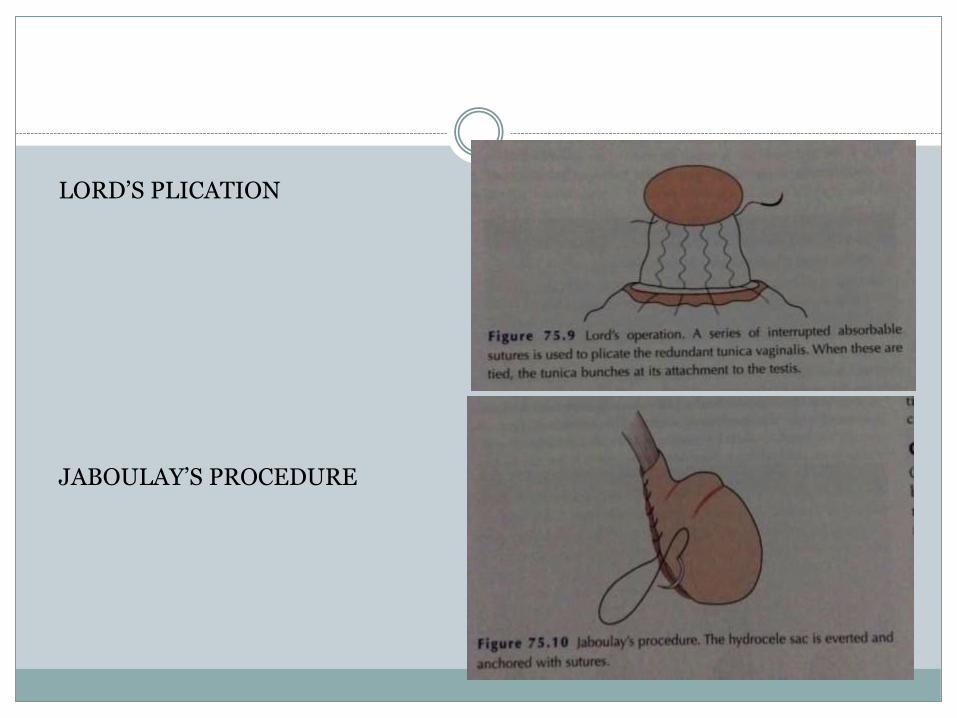
LORD’S PLICATION
JABOULAY’S PROCEDURE
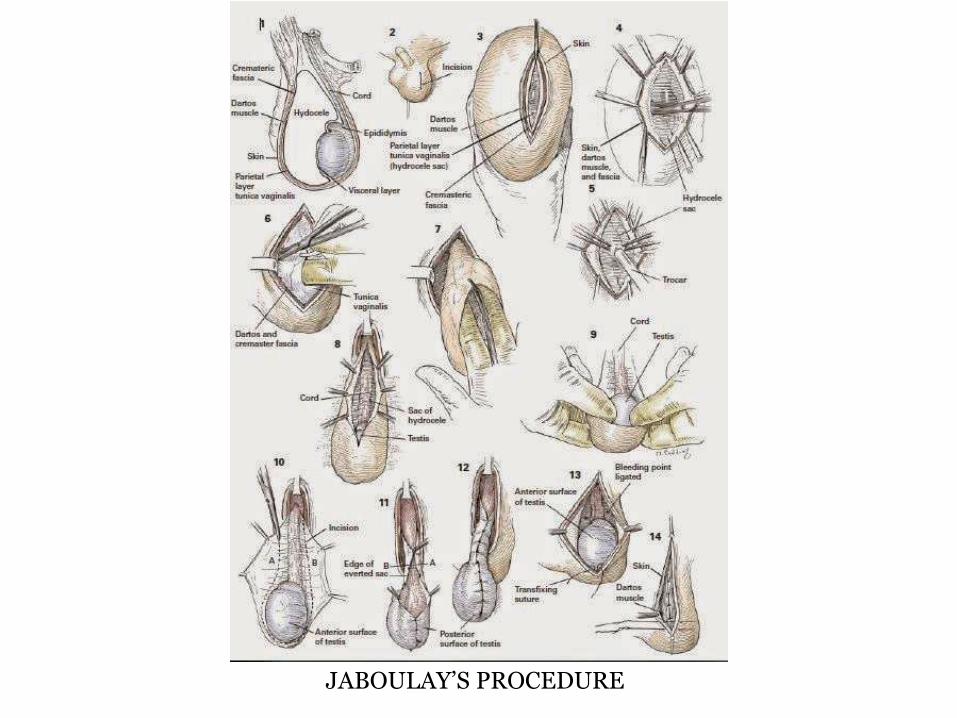
JABOULAY’S PROCEDURE

INJURY TO VAS DEFERENS
INJURY TO URETHRA
INJURY TO TESTIS/EPIDIDYMIS
REACTIONARY HAEMORRHAGE
INFECTION
SINUS FORMATION
RECURRENT HYDROCELE
COMPLICATIONS OF SURGERY
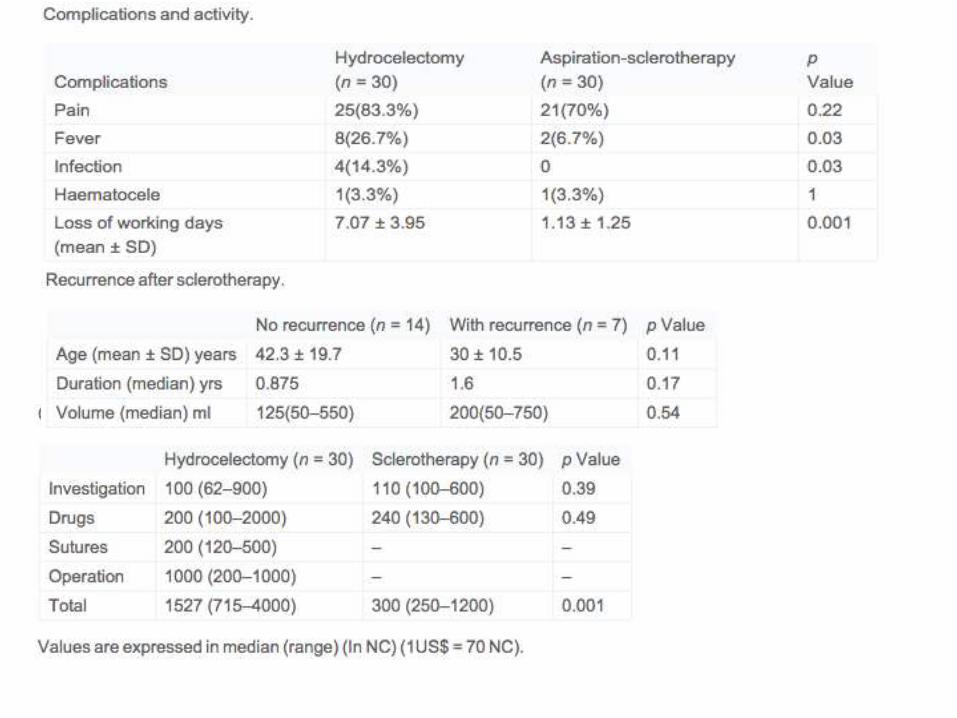
COMPARISON

COMPARISON