humanitarian support for conflict affected persons...
TRANSCRIPT

Humanitarian Support for Conflict Affected Persons and Communities in South Darfur
Final Results Report DFD-G-00-06-00076-00 U.S. Agency for International Development, Office of Foreign Disaster Assistance
Report: October 1st 2006 to July 31st 2007
1. EXECUTIVE SUMMARY
Since February 2004, ARC has been facilitating life saving and protection activities for IDPs and host community members in relatively safe corridors in south Darfur. The overall goal of the 2006/7 OFDA proposal was to improve the well being of war-affected persons by addressing immediate humanitarian needs and at the same time contributing to long-term community stabilization. The specific objectives included: improved access to basic health care services; increased access to improved water and sanitation services and hygiene practices; improved household incomes and strengthened livelihoods; and improved access to quality primary education.
Needs assessments were carried out along side program implementation. Needs in health, nutrition, water and sanitation and agricultural livelihoods were assessed in the target communities, including the Gereida camp. All assessment reports pointed to inadequate service provision in these areas and the need for urgent intervention. Programming flexibility made it possible for some of the findings to be addressed within this reporting period. For instance, all five supplementary feeding centers were formed in response to findings of various nutrition assessments. One such assessment conducted in November 2006 indicated 14.3% acute malnutrition (severe 0.9% and moderate 13.3 %) among the 1709 children screened. Results of a joint multi-sector assessment of the Gereida camp in May 2007 prompted program review in relation to prevailing needs. Among some of the key priority areas that came out as crucial were the need to increase health education coverage, urgent need to train community health providers (Midwives and TBA’s) in reproductive health, and the need to provide specialized health services like dental and psychiatric care. The assessment also influenced ARC to start considering the possibility of increased involvement in hygiene promotion in the camp.
With exception of the education objective that was not fully pursued because of funding constraints, the other three objectives were largely achieved leading to significant accomplishment of the overall goal, notwithstanding the overall fluid security situation. Increased access to preventive and curative health services, water, sanitation facilities, improved knowledge and practice of hygiene, and improved household food and income availability, all contributed to improving the overall well being of the targeted populations.
In collaboration with the State Ministry of Health, UNICEF, WHO, UNFPA and UNCHF, integrated basic health care services, including reproductive health, treatment of minor ailments, nutrition, and health education, were routinely provided to over 200,000 vulnerable people, particularly women and children. This was accomplished by rehabilitating and running twelve community clinics, operating mobile clinic services to five locations, including the women’s wing of the Nyala prison, and by setting up and operating a large clinic in the Gereida IDP camp with an average daily caseload of 250. Support continued to be provided for the El Wihda clinic in Nyala town. In collaboration with WFP, five clinic-based
1

and community supplementary feeding centers were established and operated in response to the nutrient needs of identified malnourished children. By end of the reporting period 1,259 cases were admitted to these centers.
The rehabilitation/construction of 18 water yards, 21 boreholes and 4 hand-dug wells increased access to water for an estimated 300,000 beneficiaries including nomads. Daily per capita water consumption increased from 12.52 liters (baseline) to 18.4 liters. The percentage of beneficiaries with water sources within 400m walking distance increased from 20 (baseline) to 59.9. In addition, the construction of 2,080 household latrines and 114 institutional latrines increased the percentage of the target population using latrines from 25 to 56.
Through a seed voucher scheme jointly implemented by ARC, World Vision and CHF under the technical advice of a Consultant and with support from FAO, 1,000 poor farming households had access to quality seeds of their choice and within easy reach. Participating farmers expressed happiness over receiving quality seed supplies in time for planting for the first time. In collaboration with FAO, a variety of seeds, including vegetable seeds and sweet potato vines, were distributed to 6,000 additional farming households. In collaboration with FAO, low technology irrigation foot pumps were distributed to 85 farming households. Harvests and the use of farm proceeds were not assessed to determine the extent to which these interventions contributed to increased household food and income availability. However, access to quality seeds and their timely distribution coupled with extension services are surrogate indicators of improved farm productivity.
ARC proposed to reactivate the defunct education program during this reporting period. In coordination with UNICEF, a Consultant evaluated the old program – attributing failure of the program to poor management, recommending resumption of the program as soon as possible and drafting a new proposal. Funding was still being pursued with a potential donor by the end of this reporting period.
The program was implemented in a very fluid security context and amidst bureaucratic impediments posed by various departments of the government of Sudan. These impediments seriously constrained program implementation resulting in: certain target communities, particularly in the Gereida corridor, not being covered or activities relocated to other communities; certain program activities, like anti-GBV initiatives, not being pursued; occasional restrictions on staff movements and suspension of program activities; and a generally delayed implementation of activities making it necessary to request a no-cost extension.
With the depressing security context vis-à-vis strong desire to save and protect lives, ARC learnt to use safer and more sustainable field methodologies: supplies of drugs and other consumables were pre-positioned in large quantities and in advance; local capacities were built and empowered to carry out certain activities including community mobilization, maintenance of water facilities, etc; a large number of both technical staff and auxiliaries were recruited from within their communities. These innovative ideas made it possible for ARC supported clinics to continue to operate even after expatriates and staff recruited from Nyala were withdrawn during moments of insecurity.
2. DETAILED SECTOR REPORTS
2.1 HEALTH
2.1.1 Narrative
OVERALL SECTOR OBJECTIVE “To improve access to basic health care services in South Darfur through capacity building, provision of material support and emergency preparedness and response”.
2

ARC continued to support 12 existing MOH primary health care facilities in the Nyala Tulus- Nyala- Gereida corridor (Birkatulli, Abujabra, Sanam el Naga, Ditto, Bulbul Tembsko, Bulbul Abujazo, Abu Ajura, Safya, Abu Selala, Dimso, Eltomat and an RH unit in Tulus) as well as a large PHCC in Gereida camp. ARC also supported a large PHC (ElWihda West) in Nyala town and a small service delivery point in Nyala Women's Prison. Donnki dressa which had earlier been closed in May 2006 remained closed while Birkatuli and Sanam alnaga suspended their services in January 2007 due to escalation in insecurity.
ARC’s health program provided primary health care services in these facilities with integrated services inclusive of all health components including but not limited to consultations, curatives, RH (including pre- and post-natal care and training on basic emergency obstetric care), nutrition screening, preventives (including EPI and health education). In December 2006, a major security incident saw the evacuation of INGO from Gereida camp and suspension of some operations. ARC continued to provide basic primary health care services in the Gereida camp clinic as most of the essential staff had been recruited from Gereida and this did not interfere with service provision. However, supervision was done from Nyala on regular basis.
ACCOMPLISHMENTS A. Needs assessments
In November 2006, ARC carried out a rapid nutrition screening in selected communities along Nyala - Gereida and Tulus corridors. The result of the screening showed a total of 14.3% acute malnutrition (severe 0.9% and moderate 13.3 %) among the 1709 children screened. This prompted the establishment of various SFP in selected sentinel sites and was followed by a nutrition survey in April 2007.
Owing to the suspension of most services as a result of the withdrawal of various INGO’s in the Gereida camp, there was need to assess the gaps and the coping mechanisms of the population in relation to health. An assessment of the camp was conducted from 22- 29 May, 2007 in order to determine the then prevailing health situation of the IDP population and the health needs in terms of time, place and person. The evaluation was also aimed at determining the areas which needed to be enhanced to meet the needs of the camp population after the pull out of many NGOs. Results from this assessment helped adjust programming in relation to the needs. Among some of the key priority areas that came out as crucial was the need to increase health education coverage, urgent need to train community health providers (Midwives and TBA’s) in reproductive health, and provide specialized health services like dental and psychiatric care.
A health staff assessment completed in August –September of 2006 saw a great need to undertake various capacity building trainings with a view of improving performance of health staff in various practical areas. A series of trainings were done to address this based on the recommendations in the staff assessment report.
The continuous nutrition surveillance within the community has resulted in the timeliness of intervention and introduction of new ideas in addressing the nutritional needs of communities.
B. Reproductive Health
ARC's RH team continued implementation of MISP activities as well as supervision and on-the-job training in Antenatal and Postnatal Care, Safe Motherhood, Family Planning, Breast Feeding, Growth Monitoring and Nutrition, Oral Rehydration Therapy (ORT), Infection prevention, and clinical consultations in MCH Units at the PHCCs.
The reproductive health trainings focused on management of emergency obstetrical complications (EMOC), IP, family planning, some GBV issues especially on management of post rape cases, and refresher on the basics of safe motherhood.
3
As an annual activity, ARC sponsored students this reporting period to the Nyala midwifery school and once they graduate they go back to the communities to give their services. This is done in collaboration with community leaders and village health committees in candidate selection and the MOH for the training. Seven midwives graduated during this period.
External trainers from USA organization, JHPIEGO, trained key health providers both from the MOH and ARC on various RH topics such as use of a partogram in monitoring labor, management of 3rd stage of labor, infection prevention, family planning, STI and HIV/AIDS, facilitation skills and management of common EMOC. A total of 14 participants were trained on this and follow-up supervision continued on an ongoing basis.
Reproductive health awareness sessions were also carried out within the communities focusing mainly on the importance of ante natal care post natal care, early referral and family planning. This resulted in more appropriate health seeking behavior among women of the reproductive age.
A total of 9016 clean delivery kits were distributed to all visibly pregnant women in the catchment population. These kits were produced by a local NGO supported by ARC.
Referral mechanisms through pre-arranged transportation to referral points or services as needed were among two top priorities of the RH program. Pre-arranged transportation in rural areas is a more difficult issue, due to lack of communication services and the long distances between outlying villages, clinics, and referral hospitals. Currently, an ambulance is on call 24 hours to transport referral cases from Elwihda Clinic to Nyala Teaching Hospital. An ARC vehicle is available at the Gereida Clinic to transport referral cases to the Gereida Hospital when necessary.
Owing to the deterioration of the existing structures in most of the health facilities, rehabilitation work was carried out on the Al Safia, Gereida, Eltomat, Abusalala, Abuajoura health facilities.
C. Health education
ARC provides Health Education programs in health facilities, communities and in selected schools in the ARC area of operation. Eight schools received health education sessions. In the next planning period 6 new schools are expected to be added targeting female schools as currently more male schools are in the program. Community volunteers and village health committees have been recruited and trained in all areas of ARC programs to support ARC activities (e.g. community education, referral system, early warning system, GBV focal points) and to help collect data.
So far 270 community health volunteers from both corridors have been trained to carry out health education in their communities. This includes sites with static as well as mobile clinics. During this reporting period, 415 health education sessions have been held in both the communities and the health facilities while 54,911 beneficiaries have received health education messages. Of these, 34,710 were female. A key activity planned after this period will be a knowledge, attitudes and practice (KAP) survey to assess the impact of health education in these communities. Extensive health education in anticipation of an acute water diarrhea outbreak that happened in the same season the previous year (June -August) resulted in no incidents of acute watery diarrhea by the time of writing this report. No incidents of outbreaks of communicable epidemic diseases were also reported. This has resulted in more appropriate health seeking behavior among communities.
D. EPI The gap in the provision of EPI services in South Darfur is immense. MOH has expressed the need to have this supported by partners in various ways that can ensure coverage either through static routine EPI services or through vaccination acceleration campaigns.
4

ARC supported vaccination coverage in collaboration with UNICEF, MoH, and WHO by participating in National Immunization Days through the provision of logistical support. ARC has continued to provide vehicles to be used to reach targeted populations in this exercise to ensure proper coverage. In 2007, the SMOH EPI department, in coordination with UNICEF and WHO, planned 3 acceleration campaigns targeting 127,000 children through out South Darfur. ARC supported all these campaigns by provision of vehicles for each corridor.
EPI services are ongoing in Gereida, Bulbul Tembsco and Elwihda clinics. Currently, these are the only three out of the 12 PHC that ARC is supporting that have a fully functional EPI activity.
ARC and other partner agencies in health are looking at ways of supporting MOH efforts by installing cold chain facilities and training staff on maintenance. (This includes support for transport of necessary machinery to the sites, purchase of spare parts, and coverage of labor costs for repairs while still training local technicians on maintenance). Two such cold chain facilities have been placed in Ditto and Alsafia clinics. Efforts are still underway to put everything in place including the staff, in order to make this operational.
E. EWARN/Emergency Preparedness and Response
Early warning system is in place. ARC is conducting EWARN and submitting reports to WHO and MOH from the 12 clinic sites. Surveillance on morbidity and mortality continues in collaboration with the MOH. ARC coordinates closely on reports of outbreaks or impending outbreaks with the MOH and other agencies.
Diseases with epidemic impact are monitored and the occurrences reported to WHO and MOH. Notifiable diseases like acute watery diarrhea, acute jaundice syndrome, meningitis, measles, and acute flaccid paralysis are among some of the morbidities that are monitored very closely.
ARC works closely with the MOH, OCHA, and other agencies in carrying out relevant assessments geared at identifying areas of need during outbreaks or impending outbreaks. This involves activities like training staff and pre-positioning of supplies. One of the key approaches ARC has been involved with in relation to emergency preparedness and response has been putting in store all the necessary stock for emergency response as well as conducting activities aiming at diagnosing, monitoring and averting humanitarian concerns (i.e. nutrition surveys, exploration of new areas, lobbying for other actors and actively participating in MOH-led task forces during epidemics. In July this year, ARC in collaboration with Merlin, MOH, and ICRC pre-positioned supplies at the MOH Gereda hospital in preparation for anticipated acute watery diarrhea outbreak.
A basic mobile clinic team was formed to be able to respond to the provision of emergency health care, especially in areas within ARC catchment areas that ARC was unable to provide static health services. The team provides services on a regular basis to the host communities and IDPs in Gereiga, Tokumaya, Fuluamnuara, and Tabaldiat in the Nyala Gereida corridor and Twal in the Nyala tulus corridor. The team has been able to access its mobile locations in the Nyala tulus corridor regularly with the exception of a few occasions while in the Nyala Gereda corridor of restrictions due to insecurity that consequently prevented them from making regular trips.
F. Nutrition The main objective of the nutrition program has been to carry out nutritional monitoring and rehabilitation of children <5yrs of age with global acute malnutrition, and pregnant and lactating women (PLW) with MUAC < 22 cm, among IDPs and host populations in ARC areas of operation. This is accomplished through assessing for specific nutrition needs regularly, nutrition monitoring and surveillance and starting nutrition interventions in sentinel areas of both corridors by implementation of supplementary feeding centers. In March 2007, the SFP was integrated into 3 health facilities - Al
5

Safia, Abu Salalah and El-Wehda West centers - while Abuajura opened in May 07 in the Tulus corridor. In July a fifth SFP was opened in Abujabra in the Nyala tulus corridor.
In Gereida, ICRC is running a big nutrition program. The ARC clinic in Gereida screens children under five and refers the cases that qualify for nutrition rehabilitation to the ICRC clinic. ARC implemented 5 SFP in these selected health facilities to treat beneficiaries with moderate acute malnutrition without complications and those with special nutrient requirements. The SFP admission criteria is MUAC < 125 cm and or weight for height percentage from 70 to 79%. Pregnant and lactating women are admitted based on MUAC < 21.0 cm. Also, recent discharges from TFC / OTP facilities are eligible to continue treatment till 85% weight for height percentage is reached. All cases of severe malnutrition were referred to Nyala or ICRC clinic at Gereida. So far a total of 1259 beneficiaries have been admitted in this program which started in March 2007. Activities in the nutrition program included nutrition education, micro-nutrient supplementation, and capacity building through training of Community Health Volunteers, Community Nutrition workers and Nutrition staff as well as lobbying for other actors to become involved. Nutrition education was organized at all the five SFP locations during SFP sessions. Eight thousand eight hundred and thirty-seven (8,837) participants were involved in the sessions. Topics discussed included exclusive breast feeding, home management of diarrhea conditions, household consumption of iodized salt and food preparation and storage. Post partum Vitamin A supplementation was done at 10 PHCs (76.9% of the expected reporting units) targeting post-natal mothers. Beneficiaries in the SFP received micronutrients (Vitamin A, Iron and folic) and deworming pills.
Community nutrition volunteers also received training on surveillance, hygiene, SFP organization, defaulter tracing, childcare practice, dissemination of simple and appropriate messages during household home visits to promote child health and to encourage mothers’ return. Four SFP staff had training on SFP data compilation and analysis. ARC continued to lobby for other actors to become involved in the nutrition interventions. WFP provided food for the SFP while UNICEF supported some of the interventions (provision of essential drugs to the SFP, support staff training, support assessments/ survey) in line with UNICEF nutrition priorities.
ARC remained active in the nutrition coordination meetings. The Nyala-tulus final survey report that was done by ARC in collaboration with UNICEF in April was shared with other partners through UNICEF. A mid-term activity review was done with UNICEF to identify gaps, challenges and remedies. South Darfur Nutrition activity mapping was done with UNICEF and other partners to avoid duplication.
G. HIV/AIDS/GBV issues
HIV/AIDS has been a subject little understood by most communities in South Darfur. A team of facilitators was trained which in turn trained various target groups within the communities on awareness. Religious and community leaders were the main change centers in the inception of these workshops. Other target groups that followed were teachers, youth, women, TBA’s, other national NGO staff, CHV’s. MOH and UNICEF were actively involved in working closely with ARC on this. They provided support through facilitation and provision of IEC materials on HIV/AIDS.
GBV has been a difficult subject matter in Darfur. However, ARC focused mainly on community sensitization with an emphasis on health seeking behavior following incidents of rape. GBV focal points in communities are trained on how to advise victims of rape to seek medical care at the health facilities. H. Community involvement/participation
6

ARC’s approach of working with communities has seen wider community involvement through close collaboration and communication in working towards providing more sustainable health services. Community leaders and village health committees have been instrumental in the involvement of communities in selection of their own health resource persons, identification of their priority health needs, and collaboration between the communities and the health facilities that serve them.
Capacities within these communities have been enhanced by training of the selected members on various health issues so that they can make a wholesome contribution toward attaining maximum health awareness. Among some training sessions that have been carried out are health education, nutrition education and surveillance, reproductive health issues, management issues, and a few elements of gender based violence focusing mainly on health seeking behavior following such incidents.
This has resulted in the communities having their own resource persons such as community health volunteers, trained birth attendants (before they were traditional birth attendants), community nutrition workers and last but not least, village health committees which have been key in spearheading this process. The village health committees in regard to their terms of reference have supported gender mainstreaming, as ARC emphasizes the importance of gender balance in the service provision structure.
I. Capacity building of health staff Capacity building of health staff through trainings, refresher trainings, on the job trainings, and supervision has made considerable achievements towards bettering their skills and performance on the job. A health staff assessment that was carried out between August and September was a key element in helping determine the main areas of need in regards to carrying out these trainings. These trainings captured all the key areas of primary health services that are provided touching on areas of preventive and curative services.
MOH/WHO protocols as well as Sphere standards were employed during the training and service provision process. Follow-up supervision and on-the-job training were carried out as a follow-up to these trainings. The health program had staff trained on key areas such as integrated management of childhood illnesses (IMCI), management of Oral Rehydration Therapy (ORT), Infection Prevention (IP), HIV/AIDS awareness, data collection and Health Information Systems (HIS), refresher trainings for nurses, clinical consultations, emergency preparedness and response.
2.1.2 PROJECT ACHIEVEMENT ON INDICATORS
Objective 1: To improve access to basic health care services in South Darfur through capacity building, provision of material support and emergency preparedness and response
Results/Indicators Cumulative (October 2006 to July 31st 2007)
Comments
Results 1.1: Improved access to basic health care services for the population in ARC operational areas of South Darfur # of PHC facilities functioning in ARC operation areas (Target: 17)
12 4 more were planned and two were opened only to be closed again due to insecurity and lack of qualified staff. Other areas that were earmarked for establishment did not get approval from the MOH.
# of consultations/month 242,899 These are the number of utilizations of the health facilities.
# of PHC kits distributed/PHC facility
2 Per month
Result 1.2: Essential services in place to treat common illnesses • % of malaria cases treated
with paracheck Target: Not achieved As reported previously, ARC had originally envisioned
that paracheck monitoring would be feasible, however,
7

70%
due to inaccessibility of certain areas and lack of sufficient paracheck facilities throughout South Darfur, this indicator became less viable than originally envisioned.
• % of antibiotics prescribed in all prescriptions (Target: 50%)
Not achieved This indicator was envisioned as a proxy indicator for morbidity and was difficult to measure in the emergency setting, as it does not increase surveillance of disease and disease pattern.
% of patients with common illness treated according to WHO/MOH protocols (Target: 60%)
85% ARC’s extensive focus on capacity building trainings conducted with health staff allowed for exceeding the target.
% of knowledge of drug usage among patients (Target: 50%)
85% The focus on health staff training allowed ARC to exceed the target, and positively impacted overall performance.
# of supervisory visits by relevant supervisors /PHC facility/month (Target: at least 1)
1 Clinics in the Nyala Tulus corridor received extra supervisory visits while the Nyala Gereida corridor had minimal due to travel restrictions as a result of insecurity.
Result 1.3: Enhanced management of children <5yrs by health workers through Integrated Management of Childhood Illnesses (IMCI) # of health workers / facility trained on IMCI (Target: 3)
3 Target achieved
# of facilities where health workers are incorporating IMCI in the management of children (Target: 17)
12 Only 12 clinics were established as explained in result 1.1 above.
Result 1.4: Major causes of morbidity and mortality are monitored and reported. Established EWARN system in place and reports handed in weekly for each site.
Monitoring of all morbidities done each week with high alert on AWD, malaria, bloody diarrhea & acute jaundice syndrome.
EWARN reports are shared with UNICEF, MOH and WHO
Result 1.5: Each ARC PHCC has a functional RH unit. # of PHC facilities with RH units (Target: 17)
12 As in result 1.1 above.
# of first antenatal visits 13,359 # of repeat antenatal visits % of repeat ante natal visits (target 30%)
11567 86%
Target exceeded due to effective health education and outreach efforts highlighting the importance of ANC(micronutrients, TT and anti- malaria prophylaxis and issuance of CDK) by the midwives in the health facilities.
# of deliveries in RH unit or in the home by ARC midwife
2647
# of post natal check ups by ARC midwife % of post natal check ups by ARC midwife (target 30%)
3198 120%
Target exceeded due to effective health education and outreach efforts on the importance of PNC (micronutrients postnatal vitamin A and immunization for the baby) by the trained TBAs and midwives in the communities and health facilities. The target of 30% was exceeded because deliveries done by trained TBAs warranted increased ARC PN checkups, thus the 120% increase.
# of basic EmOC cases treated at the clinic
2916
8

# of referrals to secondary facilities
1063 3 referral hospitals were available. Nyala, Tulus and Gereida Hospitals.
Result 1.6: Every visibly pregnant woman in ARC operational areas is supplied with a clean delivery kit # of clean delivery kits distributed
9016 Some supplied by ARC and others by UNFPA.
Result 1.7: At least 75% of ARC medical staff receive relevant capacity building trainings # of trainings (Target: 8) 13 More trainings were initiated as a response to
recommendations from the staff assessment in August-September 2006.
# of participants (Target: 50) 141 Target exceeded due to the reason above. # of follow-up supervision visits (Target: 20)
46 Target exceeded due to the reason above.
Result 1.8: TBAs and CHVs are trained and supplied # Of trainings. (Target: 24) 12 Insecurity made it impossible to deliver CHV trainings
in the Nyala Gereida corridor. # of participants (Target: 60 TBAs and 70 CHVs)
CHV 75 TBA 80 Exceeded target due to a May need assessment which indicated a dire need for training in Gereida. TBA’S are given a basic kit with essential items which are replenish able after training while CHV are given posters and other IEC materials to distribute in the communities as they give health education messages.
# of midwives supplied per site
2 All the midwives in the RH units were supplied with necessary equipments and consumable supplies.
# of TBAs supplied per site (Target: 3/site)
3 Target achieved
Result 1.9: Increased access to information on HIV/AIDS in ARC areas of operation # of HIV/AIDS workshops held. (Target: 4)
10 Target exceeded due to collaboration and support from other partners.
# of participants (Target:80) 190 Target exceeded due to collaboration and support from other partners.
#of target groups who participate in the workshops
10
Result 1.10: Community volunteers and youth are trained and supervised in each village of ARC operation. # Of trainings for CHVs and youth. (Target: 2)
3 There was a need for CHV in one new clinic site since the previously trained ones had relocated.
# of participants trained (Target: 80)
105 The increase is due to the additional needs that were identified as a result of the relocation of some of the CHV who had been earlier trained. They relocated due to insecurity and did not return even when the security situation improved.
# of follow-up visits (Target 12)
17 See above
Result 1.11: CHVs conduct independent health education activities in their communities. # of health education sessions conducted independently by CHVs (Target: 1/site/month)
1 Target achieved
# of participants (Target: 20/site/month)
20 Target achieved
Result 1.12: A GBV focal point exists in every community of ARC operation. # Of GBV focal point trainings. (Target: 4)
2 GBV is a very political issue in Darfur while some locations in the Nyala Gereida corridor did not receive trainings for GBV focal point due to insecurity.
# of participants (Target: 40) 20 See above # of existing GBV focal 8 See above
9

points (Target: 14) # of follow-up visits with GBV focal points (Target: 10)
7 See above
GBV attitudes survey results (Target: awareness increase of 50% or more)
No survey done Unfortunately, severe bureaucratic obstacles prevented ARC from hiring a Coordinator to oversee this activity. The GoS, through HAC, discouraged GBV programming and denied the GBV Coordinator entry visa. Although ARC was unable to conduct the survey, ARC did implement the following GBV activities as a part of RH activities: • Community awareness and sensitization on GBV
issues. • Clinical management of post rape cases. • Periodic reports to UNFPA. • Supported a local NGO for workshop on GBV issues
Result 1.13: IEC materials are produced and distributed in strategic sites in ARC areas of operation (i.e. clinics, schools, locality centers, markets, etc). # of posters distributed (Target 200)
1155 ARC collaborated with UNICEF, UNFPA, MOH, and ARC HQ to increase the amount of IEC materials received and distributed.
# of posters on display in each PHC facility and other identified sites (Target: 3 per site)
16 See above
# of T-shirts and aprons distributed to target groups (Target: 200)
276 Extras were received from the WATSAN sector.
Result 1.14: Nutritional monitoring and rehabilitation of children<5yrs of age with global acute malnutrition and pregnant and lactating women (PLW) with MUAC < 22 cm among IDPs and host populations in ARC areas of operation. # of admissions 1259 SFP started in March 2007 Recovery rate (Target: >75%) 68.3% Some distribution days were missed because of
inaccessibility due to insecurity, especially in the Nyala Gereida corridor.
Defaulter rate (Target: <10%) 31% Garden preparation season in May to July resulted in a higher default rate due to children being relocated to assist with family/community farming.
Attendance rate (Target: >75%)
82.2%
Death rate (Target: < 2%) 0.8% Mean length of stay (Target: <60 days)
60.3
Average weight gain (Target: 3-6g/kg/day)
2.7kg/day Due to high defaulter rates.
Measles immunization (Target: 100%)
85.8% The SFP had difficulty in acquiring vaccines from the MoH in June and July reducing the measles coverage.
Vitamin A coverage (Target: 100%)
100% All admissions eligible for vitamin A received the drug.
# of PLW presenting with MUAC <22cm
109
Amount of food used CSB-11.9MT OIL-1.2MT SUGAR-1.2MT
% of beneficiaries getting designated NFIs (Target:
4259 ( cumulative) representing 100%
All beneficiaries received soap
10

100%) Result 1.15: SFC staff and community nutrition workers are trained # of SFC staff and community nutrition workers trained/site (Target: 20/site)
4 SFC STAFF 25 CNV(5 PER SITE)
The number remained below target based on the lower number of beneficiaries.
Result 1.16: Caretakers of targeted children have access to information on health, hygiene and essential nutrition issues. # of health and nutrition education sessions carried out per site (Target: 24)
35 Community nutrition volunteers gave nutrition education messages both in the SFP’s and in the community.
# of participants attending education sessions (Target: 3000)
8,837 Community nutrition volunteers gave nutrition education messages both in the SFP’s and in the community.
Result 1.17: Close monitoring of the nutritional status in communities in ARC program catchments areas Prevalence of global acute malnutrition rate among children under 5 years (Target: reduced from its current rate of 13.5% to below 10%)
GAM: 14.1% (April 07 survey) SAM: 1.0%
The nutritional status of the target population rose during the implementation period primarily due to the decreasing security situation. The survey was carried out during the hunger season which also coincides with the onset of the rainy season. Household food security is usually threatened at this time. The impact due to ARC’s intervention has not yet been fully realized in part due to the late start up of the program (resulting from a delay in receipt of food stocks from WFP). ARC will conduct a follow-up assessment at a later date to measure the impact of the later interventions
Result of new Community Nutrition Workers (CNW) screenings of <5 years and PLW/site/month
Cumulative of 57.8% of the total referrals are from CNV
# of CNW referrals to SFC/PHCC % of CNW referrals to SFC/PHCC
728 57.8%
Result 1.18: Humanitarian concerns of IDPs and host populations in ARC areas of operation are monitored, action is lobbied for, new areas are explored, and emergencies are responded to in a timely manner. Time interval for project area surveys for CMR and malnutrition (Target: every 6 months or as necessary)
Carried out only once in April 2007 because of late start-up of nutrition activities.
Another CMR and malnutrition survey will be conducted in the next phase of this program.
Mortality and morbidity during epidemics as reported by WHO and MoH (Target: within Sphere standard rates)
No epidemic of any sort has been reported by WHO/MoH
No epidemic of any sort has been reported by WHO/MoH.
2.2 WASH
2.2.1 NARATIVE OVERALL SECTOR OBJECTIVE
11

“To increase access to improved water and sanitation services and practices by providing sustainable facilities and community education”.
ACCOMPLISHMENTS
A. Summary In the absence of an end of program assessment, data from the quarterly reports were analyzed and they indicate that the overall WASH objective was largely achieved. The percentage of beneficiaries with water sources within 400m walking distance was increased from 20 % to 59.9 %. Water consumption was increased from 12.52 l/p/d to 18.4 l/p/d and the percentage of beneficiaries using latrines was increased from 25 to 56. Beneficiary community members attended several training sessions, thus, building their capacity to manage water and sanitation issues.
ARC was able to drill 21 boreholes and fit them with hand pumps, sink 4 hand dug wells, rehabilitate 12 water yards, construct 6 new water yards, replace 8 generators and 9 submersible pumps in water yards, take and test 147 water samples from different water sources. Two thousand and eighty household and 114 institutional latrines were constructed. 3,558 beneficiary community members participated in various hygiene promotion campaigns. In addition, 23 village health committees were formed, 90 hand pump operators trained and 2133 pupils were sensitized on hygiene and sanitation. These accomplishments contributed to increased access to water and sanitation facilities and improved hygiene practice among the target population.
B. Needs Assessment Two WASH needs assessments were carried out during this reporting period – one in the Tulus corridor in April 2007 and another in the Gereida IDP camp in May 2007. The Tulus corridor assessment findings indicated the following: a. About 30 % of population (11,250) using water yards walked less than 400m to water yards. b. About 50% of population (12,500) using boreholes with hand pumps walked less than 400m to the
boreholes. c. About 70% of population (1,050) using hand dug wells walked less than 400m to hand dug well. d. 55% of water points constructed were clean 3 months after completion e. 45 % of people practiced correct hand washing.
The Gereida camp assessment findings indicated the following: a. Poor sanitation as latrines were inadequate. There were not enough latrines in all sectors and an alarming percentage
of constructed latrines had caved in. For instance, only 27% of 382 latrines in four sectors were in use and only 19% of those in use were in good condition.
b. Only 22 (44%) out of 50 sectors in the camp had hygiene committees. c. Only 75,076 (61%) of the camp inhabitants had been sensitized at one time or another on hygiene promotion. d. 78% of the 1,250 camp inhabitants interviewed indicated they had access to adequate water supply. e. There were no bathrooms in the camp. f. There were no places for washing clothes.
These findings influenced programming decision towards more emphasis on sanitation and hygiene promotion in the communities and the Gereida camp.
C. Water
12

In addition to the needs assessments carried out, extensive assessments were also conducted for all the new water projects that were implemented. These were aimed at finding out the feasibility and sustainability of the projects. In particular, studies were done to find out the soil formations in order to inform the design and the potential catchments population. For boreholes, data was collected on the type and thickness of geological materials, the occurrence of ground water, the flow in pores and /or fractures, direction of flow and the possible quality of ground water in each locality.
Twenty-one boreholes were drilled and fitted with hand pumps to increase access to water in Umlaota, Barkatule, Tokomaya, Almura, Babanosya, Shawera, Kateel, Tabaldia, Selgassa, Afona I, AfonaII, Bani Hussein, Abuaujala, Amashu, Abuajura, Talybay, Aumarad and Shedani.
Four hand-dug wells were sunk in Amashu, Mattio, Tchururu and Marega. The target of 8 could not be met because the actual cost of sinking the wells was higher than budgeted for. The increase in cost was due largely to high insecurity. A total of 148 hand pumps were rehabilitated. This activity surpassed its target because the program used trained repairmen in the villages to carry out the rehabilitation, especially in Greida corridor. Eight generators and 9 submersible pumps were installed.
Twelve water yards were rehabilitated in Girba, Elnakhara, Barkatule, Delbedyat, Safiya, Aumkherein, Kuezy, Sergeila Damboloya, Giwegin, Gidad, and Almashro. The proposed target was surpassed because the actual cost was lower than the budget. Six water yards were constructed in Akroup, Wadajam, Gibebish Gereiga, Tokomaya and Abugatati.
One hundred and forty-seven water samples were tested from a combination of new and old water sources. All new water sources were tested.
D. Sanitation
A total of 750 household latrines were constructed out of a target of 1000. This brings the cumulative total to 2080 building on the previous grant - 900 of these were constructed in the Gereida camp and the rest in various villages. A total of 114 institutional latrines were constructed in schools in Alfarug Domaya, Gerba, Nakhara, Wadhajam, Gidad, Rajaj Abusalala, Abujabra, Ditto, Gerieda A, Gereida B, Sany Fandu Selaha and Yassin and Allsalam, Abuajura, Safia, Dimo, Tokomaya, Barkatule, Safia and at the PHCCs in Greida and Abujabra.
A total of 3,558 sanitation and hygiene promotion training sessions were facilitated for community members, Community volunteers, school children and community leaders. The number is much higher than planned because the communities showed a lot of enthusiasm in being trained and the costs for the training turned out to be lower than budgeted in the proposal.
A total of 10,975 sanitation and hygiene inspection visits were conducted by Community Hygiene Volunteers (CHV) to sensitize households on issues of sanitation and at the same time collect vital information on the sanitation and hygiene status of the households, including availability of drinking water storage facilities. The visits surpassed the planned number because of the high number of people that attended trainings.
Twenty-seven Village Health Committees were formed, 383 CHVs, 90 pump operators and 80 hand pump technicians were trained and 2133 children were sensitized on hygiene and sanitation during this grant period. The number of children is below the planned target because of security related disruptions in schools.
2.2.2 ACHIEVEMENT ON INDICATORS
13

Objective 2: “To increase access to improved water and sanitation services and practices by providing sustainable facilities and community education”.
Result 2.1: To increase access to improved water and sanitation services by providing sustainable facilities and community education Specific Objective 2.1: To improve hygiene, sanitation and water % of targeted population with water source within 400m walking distance (Current situation is 20%: Target: 50%)
• 21 boreholes were drilled and fitted with hand pumps serving 10500 people with 5250 of them walking less than 400m to the borehole)
• 4 hand dug wells were sunk serving 1600 people with 1120 of them walking less than 400m to the water point.
• 148 hand pumps were rehabilitated serving 74000 people with 37000 of them walking less than 400m to water point.
• 12 water yards were rehabilitated serving 90,000 people with 27000 of them walking less than 400m to water yard
• 6 water yards were constructed serving 45,000 people with 13,500 of them walking less than 400m to water yard
This brings the additional people walking less than 400m to water yards to 83,870.This is 59.9% of the target population of 140,000.
Target is successfully accomplished
100% increase in amount of water consumed per person per day. # liters per person per day among target population. Current situation is 12.52 liters per person per day (from our OFDA Feb 06-Sep 06 grant report) Target: minimum 20 liters per person per day.
• 21 boreholes were drilled and fitted with hand pumps and are giving an additional supply of about 168 m3/day.
• 4 hand dug wells were sunk and are giving an additional supply of about 12m3/day
• 148 hand pumps were rehabilitated and are giving an additional supply of about 572 m3/day
• 12 water yards were rehabilitated and are giving an additional supply of about 34.56 m3/day
• 6 water yards were constructed and are giving an additional supply of 47.8m3/day
The total additional supply from all these activities is 834.3 m3/day. This added to the baseline amount of 1752.8 3/day brings the cumulative total to 2587.1
Slightly below target, but a significant improvement.
14
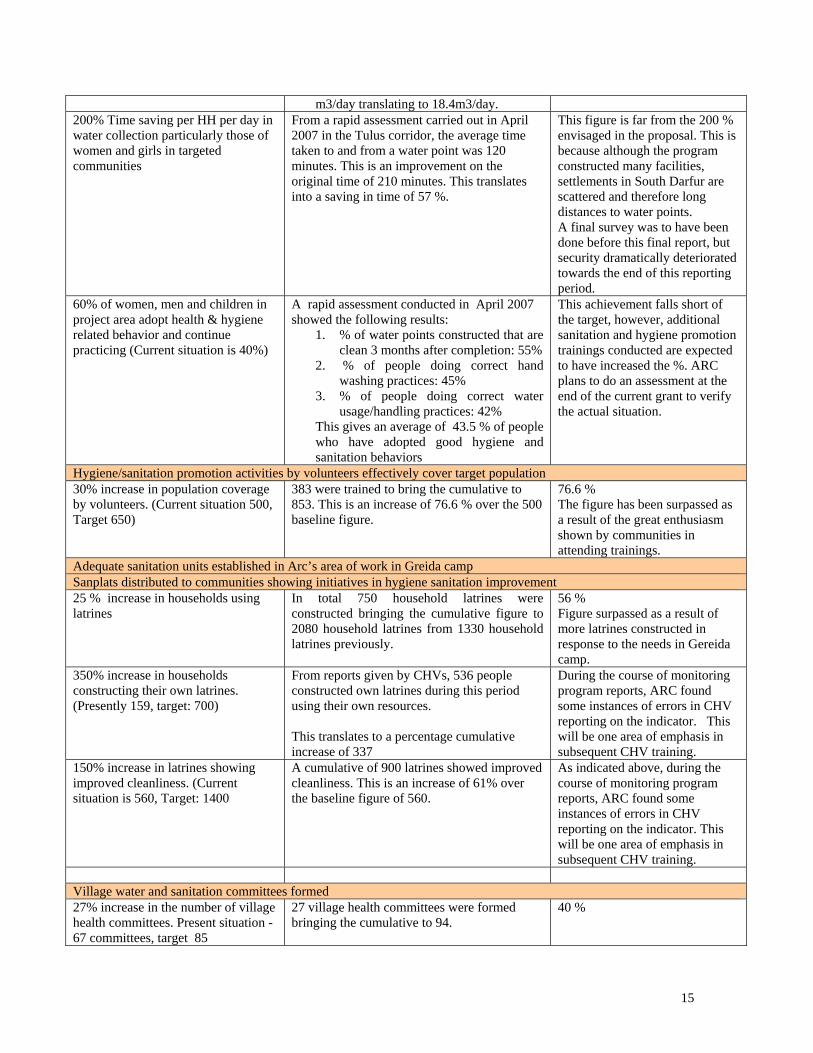
m3/day translating to 18.4m3/day. 200% Time saving per HH per day in water collection particularly those of women and girls in targeted communities
From a rapid assessment carried out in April 2007 in the Tulus corridor, the average time taken to and from a water point was 120 minutes. This is an improvement on the original time of 210 minutes. This translates into a saving in time of 57 %.
This figure is far from the 200 % envisaged in the proposal. This is because although the program constructed many facilities, settlements in South Darfur are scattered and therefore long distances to water points. A final survey was to have been done before this final report, but security dramatically deteriorated towards the end of this reporting period.
60% of women, men and children in project area adopt health & hygiene related behavior and continue practicing (Current situation is 40%)
A rapid assessment conducted in April 2007 showed the following results:
1. % of water points constructed that are clean 3 months after completion: 55%
2. % of people doing correct hand washing practices: 45%
3. % of people doing correct water usage/handling practices: 42%
This gives an average of 43.5 % of people who have adopted good hygiene and sanitation behaviors
This achievement falls short of the target, however, additional sanitation and hygiene promotion trainings conducted are expected to have increased the %. ARC plans to do an assessment at the end of the current grant to verify the actual situation.
Hygiene/sanitation promotion activities by volunteers effectively cover target population 30% increase in population coverage by volunteers. (Current situation 500, Target 650)
383 were trained to bring the cumulative to 853. This is an increase of 76.6 % over the 500 baseline figure.
76.6 % The figure has been surpassed as a result of the great enthusiasm shown by communities in attending trainings.
Adequate sanitation units established in Arc’s area of work in Greida camp Sanplats distributed to communities showing initiatives in hygiene sanitation improvement 25 % increase in households using latrines
In total 750 household latrines were constructed bringing the cumulative figure to 2080 household latrines from 1330 household latrines previously.
56 % Figure surpassed as a result of more latrines constructed in response to the needs in Gereida camp.
350% increase in households constructing their own latrines. (Presently 159, target: 700)
From reports given by CHVs, 536 people constructed own latrines during this period using their own resources. This translates to a percentage cumulative increase of 337
During the course of monitoring program reports, ARC found some instances of errors in CHV reporting on the indicator. This will be one area of emphasis in subsequent CHV training.
150% increase in latrines showing improved cleanliness. (Current situation is 560, Target: 1400
A cumulative of 900 latrines showed improved cleanliness. This is an increase of 61% over the baseline figure of 560.
As indicated above, during the course of monitoring program reports, ARC found some instances of errors in CHV reporting on the indicator. This will be one area of emphasis in subsequent CHV training.
Village water and sanitation committees formed 27% increase in the number of village health committees. Present situation -67 committees, target 85
27 village health committees were formed bringing the cumulative to 94.
40 %
15

This translates to an increase of 40%. 30 % increase in people reporting health and sanitation issues to VHC
Many community people attended hygiene sanitation promotion sessions and there was a corresponding increase in awareness leading to more people reporting on water and sanitation issues either to the village sanitation volunteers or to ARC staff in the field. From VHC records, 150 such reports were received. There was no available baseline for this indicator. Therefore, percentage increase cannot be calculated.
20 hygiene promotion trainings conducted for 800 participants by the end of the project 80% of participants are able to state at least 1 way of keeping proper personal and environmental hygiene
Training evaluations indicated that all participants trained in hygiene promotion were able to state at least two ways of keeping proper personal and environmental hygiene
# of people attending hygiene/sanitation sessions (Current situation is 2400, Target: 3200)
1119 people attended hygiene sanitation sessions bringing the cumulative to 3519
3,519 The figure has been surpassed as a result of the great enthusiasm showed by communities in attending trainings.
# of house hold visits done by volunteers-(Current situation is 9000, Target: 15,000)
10,975 house hold visits were done bringing the cumulative total to 19,975
19,975
Pupils have information on hygiene and sanitation issues 80% of pupils are able to state at least 10 ways of keeping proper personal and environmental hygiene.
2133 pupils were sensitized on water, sanitation and hygiene and 1803 of them were able to state 10 ways of keeping proper personal and environmental hygiene (84.5%).
84.5%
# of teachers given water/sanitation awareness sessions (current: 30; target 130)
Schools in target areas have adequate sanitation facilities 60% increase in school population having access to latrines in target area. (Current situation is 45,Target: 67)
24 schools were provided with latrines increasing the number of schools with latrines to 69. This translates to a percentage increase of 53.
53.3% Within target
Water sources in our area of operation are considered safe No faecel coliforms per 100ml at the point of delivery for all water sources tested
In collaboration with the Water, Environment and Sanitation project, water samples were collected from 147 water points across the program area and tested for bacteriological and chemical elements. Samples from only 2 sources were found to be contaminated.
2 sources contaminated
100% of contaminated water sources chlorinated after testing.
Out of 147 samples taken only 2 samples showed contamination beyond the acceptable limit and were chlorinated.
100%
Specific Objective 2.2: To improve access to adequate potable water from water supply systems owned, operated, maintained and managed in a sustainable manner by either communities or government. 12 water yards repaired/constructed and fully functioning in the target area by the end of the project 100 % in crease in liters of water produced per person per day in target area (Current situation is 9, target:20)
• 21 boreholes were drilled and fitted with hand pumps and are giving an additional supply of about 168 m3/day.
2587.1m3/d = 2,587,100 liters per day over a target population of 140,000 = 18.47
16

• 4 hand dug wells were sunk and are giving an additional supply of about 12m3/day
• 148 hand pumps were rehabilitated and are giving an additional supply of about 572 m3/day
• 12 water yards were rehabilitated and are giving an additional supply of about 34.56 m3/day
• 6 water yards were constructed and are giving an additional supply of 47.8m3/day
The total additional supply from all these activities is 834.3 m3/ day. This added to the baseline amount of 1752.83m3/day brings the cumulative total to 2587.1 m3/day translating to 18.4m3/day.
200 % reduction average walking distance to facilities (Current situation is 21km.,target: 700m)
• 21 boreholes were drilled and fitted with hand pumps
• 4 hand dug wells were sunk • 6 water yards were constructed
These 31 new projects were spread all over the project area and from assessments done reduced the average walking distance to water points from 21 km to about 10 km. This is a reduction of about 52.4%
52.4 % As project activities progressed, ARC came to realize the target of 200% may have been over-ambitious and could not be reached within such a short period given the level of insecurity and logistical requirements that were hampered as a result of the increased insecurity.
80% increase in people using water facilities: (Current situation: 73,944 , Target: 133,100)
• 21 boreholes were drilled and fitted with hand pumps serving 8,400 more people
• 4 hand dug wells were sunk serving 1,600 more people
• 148 hand pumps were rehabilitated serving 29,600 more people
• 12 water yards were rehabilitated serving 36,000 more people
• 6 water yards were constructed serving 45,000 more people
This brings the additional people using water facilities to a cumulative of 120,600. This makes a percentage increase of 163 % over the 73,944.
163 %%
40% of existing un rehabilitated water yards rehabilitated (Current situation is 13 rehabilitated already, Target: 7 more)
12 new water yards were rehabilitated bringing the cumulative figure to 25 and a percentage of 92.
92 % Target surpassed because cost turned out to be lower than planned in the budget.
# of water yards constructed (Current situation is 2, Target: 5)
6 water yards were constructed
6
10 boreholes rehabilitated and fully functioning in the target areas by the end of the project
17

600 % of boreholes rehabilitated and fully functioning. (Current situation is 2 Target: 12)
148 boreholes were rehabilitated
7,400 % Target surpassed because local repairmen were used to carry out the work even when ARC staff were not able to go to the field due to insecurity. Another reason was that during the planning, it was envisaged that ARC would do complete overhauling of the boreholes but this in the end was done as part of the rehabilitation of water yards thus leaving a significant amount of funds to do minor hand pump/ borehole rehabilitation/repairs that required local expertise.
6 hands dug wells sunk and fully functioning and 4 shallow boreholes with hand pumps sunk by project end. 50% increase in shallow boreholes with hand pumps sunk and functioning (Current is 8, Target: 12)
21 boreholes with hand pumps were drilled
162.5 % Target surpassed because cost turned out to be lower than planned in the budget.
# of fully functioning hand dug wells constructed (Current none, Target: 6)
4 hand dug wells were sunk and are fully functioning.
4 Target not reached because some funds for this activity were diverted to construct latrines in Gereida camp. This was done at a time when there was a very huge influx of IDPs into Gereida camp ( An arrival of about 60,000 people in a space of 5 weeks) without a corresponding increase in service provision to them. This was in an ARC area of operation and apart from ICRC and OXFAM, ARC was the only other NGO in the area by that time. UNICEF appealed to other NGOs for support in putting up latrines in the camp but none was forthcoming. ARC was obliged to support the IDPs after the need for hand dug wells in host communities was assessed to be secondary to the need for latrines for the new IDPs in the camp. ARC sought and received permission from OFDA for this diversion of funds.
At least 30 hand pumps rehabilitated and functioning 37% of hand pumps rehabilitated and functioning (Current situation is 81 Target:111)
148 hand pumps were rehabilitated This activity has surpassed its target because we utilize trained repairmen in the villages to carry out rehabilitation using tools provided by ARC.
113.5%
18

180 % increase in water facilities built and functioning in schools(current situation 5 target 14)
Only 1 (20%) school was provided with an extension of a pipeline from an existing water yard.
This is one of the activities that ARC had anticipated to receive funding from other donors, specifically CHF through UNICEF. Unfortunately ARC did not receive the CHF funding and had to resort to internal funding for this activity, hence the low output.
Specific Objective 2.3:To improve the capacity of community, water operators and ARC’ Water and Sanitation staff through training No. of ARC WASH staff attending at least 1 course and scoring at least 50 % marks in training evaluation ( Current situation is none target 12 )
None attended 0% -No funding was provided for this activity in the proposal and other funding sources (CHF/UNICEF) that had been identified were not forthcoming. Although this activity was not funded by OFDA and other donors, ARC intended to use own resources. However, there were problems in the implementation. Prominent among them being the difficulties in accessing qualified facilitators in Darfur. Even where we made arrangements to train staff in water testing and sampling through a local organization, the organization could not honor the deal as it turned out that it’s schedules could not allow training for other organizations.
No. of staff from water department (and community managed water yards) facilitated to have a course and scoring at least 50 % Marks in training evaluation (current situation is 25 target : 50)
30 water yard operators 30 Water yard operators were trained in April and scored at least 50% in training evaluations.
71% increase in village hand pump mechanics trained and able to fix hand pumps on their own (current situation84 target 144)
90 new hand pump mechanics were trained. This represents an increase of 107 % over the 84 who had been trained earlier.
107 %
2.3 AGRICULTURAL LIVELIHOODS 2.3.1 NARATIVE OVERALL SECTOR OBJECTIVE “To improve household incomes and strengthen livelihoods of resettled IDPs, the war-affected and resident poor households”.
19

The objective for this sector remained the same, but the activities changed significantly in relation to donor (FAO) priorities. Following is a summary of accomplishments on the revised program: Through a seed voucher scheme jointly implemented by ARC, World Vision and CHF under the technical advice of a Consultant and with support from FAO, 1,000 poor farming households had access to quality seeds of their choice and within easy reach. Participating farmers expressed happiness over receiving quality seed supplies in time for planting for the first time. In collaboration with FAO, a variety of seeds, including vegetable seeds and sweet potato vines, were distributed to 6,000 additional farming households. In collaboration with FAO low technology irrigation foot pumps were distributed to 85 farming households. Harvests and the use of farm proceeds were not assessed to determine the extent to which these interventions contributed to increased household food and income availability. However, access to quality seeds and their timely distribution coupled with extension services are surrogate indicators of improved farm productivity. 2.3.2 ACHIEVEMENTS ON INDICATORS Objective 3: “To improve household incomes and strengthen livelihoods of resettled IDPs, the war-affected and resident
poor households”.
Objective 3: To improve household incomes and strengthen livelihoods of resettled IDPs, the war-affected and resident poor households. # Community Animal Health Workers trained on animal vaccination
None The focus of the Agricultural livelihoods program completely changed due to preference of the donor (FAO). No funds were requested of OFDA for this objective. The proposed livestock scheme was not undertaken. See above description for additional information.
# of animals vaccinated
None The focus of the Agricultural livelihoods program completely changed due to preference of the donor (FAO). No funds were requested of OFDA for this objective. The proposed livestock scheme was not undertaken. See above description for additional information.
# persons trained in chicken care
None The focus of the Agricultural livelihoods program completely changed. The proposed livestock scheme was not undertaken.
# of families who receive crop seeds and tools. Target: 3000
7,000 households With support from FAO assorted vegetable seeds were distribute to 6,000 household and seed vouchers were given to 1,000 households for the principal grain seeds.
# of families who receive kitchen garden seeds.
Same as above Same as above
2.4 BASIC PRIMARY EDUCATION
20

2.4.1 NARRATIVE OVERALL SECTOR OBJECTIVE “To ensure access to quality primary education for war-affected children in ARC’s areas of operation in
South Darfur”.
The proposal to reactivate the education program did not materialize because of lack of funding. Only minimal support was requested from OFDA to support this objective (10,800 USD) for general program supplies. However, in coordination with UNICEF, a Consultant evaluated the old program and concluded that failure of the program was attributable to poor management as a result of ARC’s inability to find suitably qualified staff. A recommendation was made to resume the program as soon as possible and a new proposal was drafted. Funding was still being pursued with a potential donor by the end of this reporting period.
3. COORDINATION WITH OTHER PARTNERS
ARC continued to coordinate work with other international organizations (WV, CARE, IRC, IMC, Mercy Corps, Concern World Wide, Samaritan Purse, ICRC, OXFAM-GB, Merlin, GOAL, NCA etc.),UN agencies (UNICEF, WHO, FAO, UNFPA, UNHCR, WFP), local NGOs (including Alham and Al Massar), and local authorities (MoH , HAC and WES). ARC continued to actively participate in strategic health and nutrition annual planning meetings and the development of work plans in partnership and collaboration with key partners in health like MOH, UNICEF, WFP and WHO. More specifically, ARC participated in the 2006/7 UNCHF work plan and grant for health during the first half of this reporting period. A Partners Cooperation Agreement was signed with UNICEF for the supply of PHC kits and an agreement was signed with WFP to supply needed food items for the supplementary feeding program. An agreement was also signed with UNICEF for the supply of hygiene promotion materials, including soap. ARC collaborated with JHPIEGO of the Columbia University, USA and Marie Stopes International in UK in setting up a comprehensive reproductive health program and in supporting the quality training of both MOH and ARC staff in improved reproductive health service delivery. Weekly or bi-weekly meetings are held with all these actors to discus common issues that pertain to common areas of interest. An average of 7 meetings are held every month.
4. CHALLENGES/CONSTRAINTS
1. Insecurity rendered most facilities especially in the Gereida corridor inaccessible thus hindering supervision and
regular supply of materials like equipment and drugs. Some target communities were inaccessible for long periods of time, activities were relocated from some and regular supervision of field activities was interrupted on several occasions. Insecurity resulted in cancellation of the establishment of new clinic sites.
2. Low literacy level of most of the RH service providers, thus, rendering them incapable of documenting their work
(most midwives cannot read and write).This contributed in deficiencies in imparting of basic skills that are need in enabling them perform better.
3. The competency level of some national staff is very low as there is a general shortage of qualified health staff in
South Darfur.
4. Limited availability of professional service providers like geologists, laboratory technologists/chemists, electrical engineers, drillers etc. meant that it was sometimes difficult to follow procurement procedures where bids must be
21

received from at least 3 suppliers or service providers. Also, some contracted service providers were in most cases reluctant to go to work in some areas and if they did accept to go, they charged exorbitant fees/costs.
5. South Darfur is a semi-desert environment. When it rains most roads are rendered impassable and pit latrines and
other constructed facilities are undermined or they actually cave in. When it does not rain for long the heat loosens the soil and renders it difficult to dig pits for latrines and water wells. Existing latrines also collapse when the soil is too loose.
5. LESSONS LEARNT
1. The most important lesson learnt relates to the appropriate recruitment and deployment of local capacities as a
strategy. The use of this strategy ensured that program activities continued to be implemented even when key staff were withdrawn or prevented from going to certain locations because of insecurity. When all expatriates and staff recruited from Nyala were withdrawn from the Gereida clinic following the December 19 2006 security incident, staff recruited from among the IDPs and host community in Gereida continued operating the ARC supported clinic. Also, all 12 PHCCs in the communities continued to function even when these communities were not accessible to Nyala. All that was missing was technical supervision for quality control.
2. The hiring of local Contractors for construction work also enabled program implementation in communities that
Contractors from Nyala or other locations could not venture into because of security considerations. Sometimes fees charged were even lower.
3. Community involvement/participation is vital in the provision of basic community services. When key community
members are involved, acceptance gradually ripples from them and makes implementation of programs easier. A classical example of involving key community members is the establishment and strengthening of village committees – be it for health WASH or Agriculture. Another example is the training of community health volunteers to deliver hygiene and sanitation messages in their respective communities. This practice proved to be more cost-effective than using directly employed staff. The volunteers had a wider reach and some took their work as a prestige and therefore a motivation to work even harder.
4. Building capacities of local NGO’s in various income generating activities contributes to local capacity enhancement.
ARC contracted a local NGO owned and operated by women to produce clean delivery kits.
5. Collaboration and coordination with other partners is important. ARC, ICRC, Merlin and MOH were able to put up emergency preparedness system in place in Gereida.
6. Involvement of MOH in all aspects the health program contributed significantly to the establishment of health
facilities in the communities and to staff recruitment. ARC is supporting MOH clinics in the communities and using largely MOH staff. Phase-out from these facilities is likely to be easier than if ARC were to establish new clinics.
6. SECURITY
Security in Darfur generally continued to deteriorate during this program period irrespective of international pressure and intervention. While the US-brokered peace agreement between the SLA Minawi faction and the GoS appeared to be holding, emerging internal frictions questioned the integrity of the agreement.
The GoS continued to be generally accused of deliberately prolonging the conflict and conducting indiscriminate air raids on positions held by the warring factions - leaving several civilian casualties and displaced populations in their trail. GoS fighter planes bombed rebel controlled community in west and south Darfur killing and/or further displacing innocent civilians.
22

23
Bureaucratic processes introduced by the GoS restricted and delayed movement of humanitarian workers, including ARC staff. Relations between the GoS and the humanitarian community worsened when in January 2007 GoS security personnel invaded one ARC residence in Nyala, arrested, detained and later prosecuted 20 humanitarian workers including AU and UN personnel. The UN personnel were exempted form court charges because of their diplomatic immunity, but the NGO workers were later tried in court and some were fined minimal charges for organizing a party without police clearance.
The overall humanitarian space in Darfur corroded dramatically during this reporting period with increased attacks on aid agencies. In addition to factional and tribal fighting that limited access, there was a systematic increase in the number of assaults on aid agencies. More vehicles were hijacked and more physical assaults were inflicted on humanitarian workers with impunity. A number of aid agencies had cause to close, suspend or relocate operations to other areas.
The office of the UN Humanitarian Coordinator described the Darfur situation as follows:
• Access levels are their lowest level since the start of the conflict whilst need has almost doubled and this trend looks like it will continue to worsen.
• Violence against civilians by all parties to the conflict continues. Violence against humanitarian agencies has reached unprecedented levels and the position of humanitarian, especially NGO, workers is bordering on untenable. Morale amongst aid workers is at an all time low.
• Despite the extension of the moratorium, bureaucratic impediments remain in place. Restrictions on visas, recruitment, travel and importation of goods continue to severely impede the ability of aid agencies to do their job and assist the beneficiaries in Darfur.
The general situation described above continued to hold in different degrees in the three regions of Darfur. West Darfur was, in general, notably the worst in terms of atrocities and instability, particularly along the border with Chad. North Darfur, particularly the El Fasher area, followed next. South Darfur was generally more stable with safe corridors for recovery work although inter-tribal conflicts in the Tulus corridor and attacks on the humanitarian community by an alleged SLA breakaway faction registered the worst security incident in the Gereida corridor. However, the GoS later appeared to be yielding to pressure regarding the deployment of AU/UN hybrid forces and there were commendable improvements in the processing of visas, permits and other official relations with the humanitarian community.
ARC operations in Darfur continue to be confined to the Nyala-Gereida and Nyala-Tulus corridors and Nyala town. These are GoS and SLA Minawi controlled areas. The Tulus corridor is partly flanked by the Janjaweed, but no threatening security incidents were recorded from them during this reporting period.
On December 19 2006, residences of aid workers were attacked by a breakaway faction from SLA Minawi. Twelve vehicles, radio equipment and a large sum of money were taken away. An expatriate female aid worker was raped. These brutal acts led to the withdrawal of all aid agency staff and suspension of activities in the Gereida camp. Only ARC and ICRC remained operational in the camp.
ARC has a Security Officer to manage program security and security information in the field. The Officer maintains links with other aid agencies, the UNOCHA and AMIS and advises ARC staff on security matters. All ARC vehicles and office bases in Nyala and Gereida are fitted with communication radios for security checks and incident reporting. Thuraya phones with appropriate contact numbers are made available for all field travels.
With support from the HQ based Security Manager, security in the Tulus and Gereida corridors and other pockets was reviewed twice during this reporting period and the security manual was adjusted accordingly.